Recommendations for Prevention and Control of Influenza in Children, 2011-2012 - Pediatrics
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

FROM THE AMERICAN ACADEMY OF PEDIATRICS
Organizational Principles to Guide and Define the Child
Health Care System and/or Improve the Health of all Children
POLICY STATEMENT
Recommendations for Prevention and Control of
Influenza in Children, 2011–2012
COMMITTEE ON INFECTIOUS DISEASES
KEY WORDS abstract
influenza, immunization, live-attenuated influenza vaccine,
trivalent inactivated influenza vaccine, vaccine, children,
The purpose of this statement is to update recommendations for rou-
pediatrics tine use of trivalent seasonal influenza vaccine and antiviral medica-
ABBREVIATIONS tions for the prevention and treatment of influenza in children. The key
AAP—American Academy of Pediatrics points for the upcoming 2011–2012 season are that (1) the influenza
HCP—health care personnel vaccine composition for the 2011–2012 season is unchanged from the
CDC—Centers for Disease Control and Prevention
TIV—trivalent inactivated influenza vaccine 2010 –2011 season, (2) annual universal influenza immunization is in-
LAIV—live-attenuated influenza vaccine dicated, (3) a simplified dosing algorithm for administration of influ-
This document is copyrighted and is property of the American enza vaccine to children 6 months through 8 years of age has been
Academy of Pediatrics and its Board of Directors. All authors created, (4) most children presumed to have egg allergy can safely
have filed conflict of interest statements with the American
Academy of Pediatrics. Any conflicts have been resolved through
receive influenza vaccine in the office without need for an allergy con-
a process approved by the Board of Directors. The American sultation, and (5) an intradermal trivalent inactivated influenza vaccine
Academy of Pediatrics has neither solicited nor accepted any has been licensed for the 2011–2012 season for use in people 18
commercial involvement in the development of the content of
through 64 years of age. Pediatricians, nurses, and all health care
this publication.
personnel have leadership roles in the prevention of influenza through
vaccine use and public education. In addition, pediatricians should
promptly identify influenza infections to enable rapid treatment, when
indicated, to reduce childhood morbidity and mortality. Pediatrics
2011;128:000
INTRODUCTION
The American Academy of Pediatrics (AAP) recommends annual triva-
lent seasonal influenza immunization for all children and adolescents 6
months of age and older during the 2011–2012 influenza season. Spe-
www.pediatrics.org/cgi/doi/10.1542/peds.2011-2295
cial outreach efforts should be made to vaccinate people in the follow-
doi:10.1542/peds.2011-2295
ing groups:
All policy statements from the American Academy of Pediatrics
automatically expire 5 years after publication unless reaffirmed, ● All children, including infants born prematurely, 6 months of age
revised, or retired at or before that time. and older with conditions that increase the risk of complications
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). from influenza.
Copyright © 2011 by the American Academy of Pediatrics ● All household contacts and out-of-home care providers of
● children with high-risk conditions and
● children younger than 5 years.
● All health care personnel (HCP).
● All women who are pregnant, considering pregnancy, or breastfeed-
ing during the influenza season.
KEY POINTS RELEVANT FOR THE 2011–2012 INFLUENZA SEASON
1. All people 6 months of age and older should receive trivalent sea-
sonal influenza vaccine each year, especially those who are at high
PEDIATRICS Volume 128, Number 4, October 2011 from www.aappublications.org/news by guest on February 18, 2020 1
Downloaded
risk of influenza complications immunization status to the pri- demic period, at least 114
(eg, children with chronic medical mary care provider. Immunization laboratory-confirmed influenza-
conditions such as asthma, diabe- of close contacts of children at associated pediatric deaths were
tes mellitus, immunosuppression, high risk of influenza-related com- recorded during the 2010 –2011
or neurologic disorders). In the plications is intended to reduce season. Seventy-one deaths were
United States, more than two- their risk of contagion (ie, “co- associated with influenza A virus
thirds of children younger than 6 cooning”). The concept of cocoon- subtypes: 30 influenza A (2009
years and almost all children ing is particularly important for H1N1), 21 influenza A (H3N2), and
older than 6 years spend signifi- helping to protect infants younger 20 undetermined subtypes. Forty-
cant time in child care and school than 6 months, because they are three deaths were associated with
settings outside the home. Expo- too young to be immunized with influenza B viruses. More than half
sure to groups of children in- influenza vaccine. The risk of of all hospitalized pediatric pa-
creases the risk of infectious dis- influenza-associated hospitaliza- tients (51.8%) did not have any
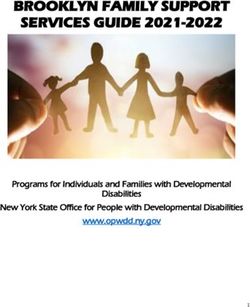
eases. Children younger than 2 tion in healthy children younger known underlying conditions (Fig
years are at an increased risk of than 24 months has been shown to 1). Although children with certain
hospitalization and complications be greater than the risk of hospi- conditions are at higher risk of
attributable to influenza. School- talization in previously recognized complications, substantial pro-
aged children bear a large influ- high-risk groups such as the el- portions of seasonal influenza
enza disease burden and have a derly. Children 24 through 59 morbidity and mortality occur
significantly higher chance of months of age have had increased among healthy children.
seeking influenza-related medical rates of outpatient visits and anti- 5. The recommended trivalent vaccine
care compared with healthy microbial use. for the 2011–2012 influenza season
adults. Therefore, reducing influ- 3. The 2009 pandemic influenza A contains the following 3 virus strains:
enza transmission among chil- (H1N1) virus emerged in March ● A/California/7/2009 (H1N1)–like
dren who attend child care or 2009 and was associated with 2 antigen (derived from 2009 pan-
school should decrease the bur- significant waves of influenza ac- demic influenza A [H1N1] virus);
den of childhood influenza and tivity during 2009 and 2010, as de- ● A/Perth/16/2009 (H3N2)–like
transmission of influenza to fined by the World Health Organi- antigen; and
household contacts and commu- zation. This virus strain
● B/Brisbane/60/2008–like antigen.
nity members. Most egg-allergic disproportionately affected the
children can now receive influ- pediatric population compared 6. On the basis of ongoing global
enza vaccine safely. with the usual seasonal influenza surveillance data, for only the
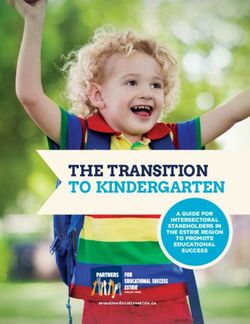
strains. It was 1 of 3 circulating fourth time in 25 years there is
2. Annual trivalent seasonal influ-
influenza viruses during the no need to change any of the in-
enza vaccine is recommended for
2010 –2011 influenza season, and fluenza vaccine strains (Fig 2).
household members and out-of-
it is expected to circulate again The number of trivalent seasonal
home care providers of children
during the 2011–2012 influenza influenza vaccine doses to be ad-
and adolescents at high risk of
season in combination with 1 or ministered this year depends on the
complications of influenza and
more of the other seasonal influ- child’s age at the time of the first
healthy children younger than 5
enza strains. During the 2010 – administered dose and his or her
years, especially infants younger
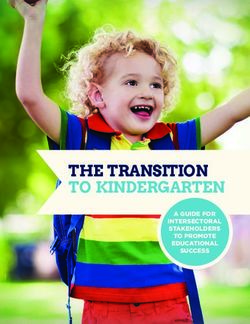
2011 season, influenza A (H3N2) vaccine history (Fig 3):
than 6 months. Pediatric offices
was the predominant circulating ● Infants younger than 6 months
should consider serving as an al-
ternate venue for parents and strain, but weekly virus subtype are too young to be immunized
other adults who care for children activity varied regionally. with influenza vaccine.
to receive influenza vaccine, if this 4. Although the number of hospital- ● Children 9 years of age and
approach is acceptable to both the izations for younger persons and older need only 1 dose.
pediatrician and the adult to be outpatient visits for influenza-like ● Children 6 months through 8
immunized. Clinicians should still illness overall was lower during years of age should receive 2
encourage adults to have a medi- the 2010 –2011 season compared doses of vaccine if they did not
cal home and communicate their with the influenza A (H1N1) pan- receive any dose of vaccine last
2 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from www.aappublications.org/news by guest on February 18, 2020
FROM THE AMERICAN ACADEMY OF PEDIATRICS
FIGURE 1
Selected underlying medical conditions in patients hospitalized with influenza, FluSurv-NET 2010 –2011. Reprinted from: Centers for Disease Control and
Prevention. FluView 2010 –2011 influenza season week 15 ending April 16, 2010. Available at: www.cdc.gov/flu/weekly.
H1N1-like strain H3N2-like strain B-like strain
1986-'87 A/Chile/1/83 and A/Christchurch/4/85- B/Ann Arbor/1/86 seasonal influenza vaccine last
A/Singapore/6/86 A/Mississippi/1/85 season need only 1 dose of the
1987-'88 A/Singapore/6/86 A/Leningrad/360/1986 B/Ann Arbor/1/86
1988-'89 A/Singapore/6/86 A/Sichuan/2/87 B/Beijing/1/87 2011–2012 influenza vaccine this
1989-'90 A/Singapore/6/86 A/Shanghai/11/87 B/Yamagata/16/88
1990-'91 A/Singapore/6/86 A/Guizhou/54/89 B/Yamagata/16/88
season.
1991-'92 A/Singapore/6/86 A/Beijing/353/89 B/Yamagata/16/88
1992-'93a A/Singapore/6/86 A/Beijing/353/89 B/Yamagata/16/88
In most influenza seasons, children
1993-'94 A/Singapore/6/86 A/Beijing/32/92 B/Panama/45/90 who received influenza vaccine for the
1994-'95 A/Singapore/6/86 A/Shangdong/9/93 B/Panama/45/90
1995-'96 A/Singapore/6/86 A/Johannesburg/33/94 B/Beijing/184/93 first time the previous season but who
1996-'97 A/Singapore/6/86 A/Wuhan/359/95 B/Beijing/184/93 received only 1 dose are recom-
1997-'98 A/Bayern/7/95 A/Wuhan/359/95 B/Beijing/184/93
1998-'99 A/Beijing/262/95 A/Sydney/5/97 B/Beijing/184/93 mended to receive 2 doses of vaccine
1999-2000a A/Beijing/262/95 A/Sydney/5/97 B/Beijing/184/93
2000-'01 A/New Caledonia/20/99 A/Moscow/10/99 B/Beijing/184/93 in the current season, because the
2001-'02 A/New Caledonia/20/99 A/Moscow/10/99 B/Sichuan/379/99 first vaccine dose primes the immune
2002-'03 A/New Caledonia/20/99 A/Moscow/10/99 B/Hong Kong/330/2001
2003-'04a A/New Caledonia/20/99 A/Moscow/10/99 B/Hong Kong/330/2001 system, but no significant protection
2004-'05 A/New Caledonia/20/99 A/Fujian/411/2002 B/Shanghai/361/2002
2005-'06 A/New Caledonia/20/99 A/California/7/2004 B/Shanghai/361/2002
against disease is achieved until 1
2006-'07 A/New Caledonia/20/99 A/Wisconsin/67/2005 B/Malaysia/2506/2004 week after the second dose. How-
2007-'08 A/Solomon Islands/3/2006 A/Wisconsin/67/2005 B/Malaysia/2506/2004
2008-'09 A/Brisbane/59/2007 A/Brisbane/10/2007 B/Florida/4/2006 ever, because the vaccine strains for
2009-'10 A/Brisbane/59/2007 A/Brisbane/10/2007 B/Brisbane/60/2008 the 2011–2012 season are un-
Pandemic A/California/07/2009
2010-'11 A/California/07/2009 A/Perth/16/2009 B/Brisbane/60/2008 changed from last season, 1 dose
2011-'12a A/California/07/2009 A/Perth/16/2009 B/Brisbane/60/2008
this season coupled with the 1 dose
FIGURE 2 of last season will provide adequate
World Health Organization vaccine composition recommendations 1986 to present. a No change in
influenza vaccine strains from previous influenza season. Data source: World Health Organization, protection (Fig 4). Previous recom-
Global Alert and Response. Recommendations for influenza vaccine composition. Available at: www. mendations for 2 doses of vaccine will
who.int/csr/disease/influenza/vaccinerecommendations1/en/index.html (for data from 1998 to pres-
ent; previous years’ data were obtained from Weekly Epidemiologic Record). resume for seasons in which 1 or more
of the vaccine strains change.
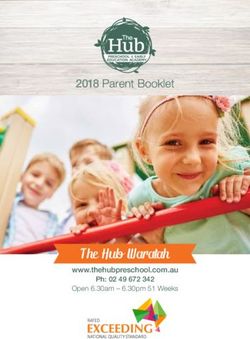
season. The second dose should ● Children 6 months through 8 7. Optimal protection is achieved
be administered at least 4 years of age who received at least through annual immunization. An-
weeks after the first dose. 1 dose of the 2010 –2011 trivalent tibody titers wane to 50% of their
PEDIATRICS Volume 128, Number 4, October 2011 from www.aappublications.org/news by guest on February 18, 2020 3
Downloaded
date. Protective immune responses
persist throughout the influenza
season, which can have ⬎1 dis-
ease peak and often extends into
March or later. Prompt initiation
of influenza immunization and
continuance of immunization
throughout the influenza season,
regardless of whether influenza is
circulating (or has circulated) in
the community, are critical com-
ponents of an effective immuniza-
FIGURE 3 tion strategy. This approach pro-
Number of 2011–2012 seasonal influenza vaccine doses for children 6 months through 8 years of age. vides ample opportunity to
● This simplified approach is only possible because the 2011–2012 influenza vaccine contains the
administer a second dose of vac-
identical 3 influenza virus strains used last year in the 2010 –2011 vaccine.
● The number of doses to be given is determined on the basis of the child’s age at the time of the first dose.
cine, because children younger than
9 years might require 2 doses to
confer optimal protection.
9. HCP, influenza campaign organiz-
ers, and public health agencies
should collaborate to develop im-
proved strategies for planning,
communication, and administra-
tion of vaccines.
● Plan to make trivalent seasonal
influenza vaccine easily acces-
sible for all children. Examples
of such action include creating
walk-in influenza clinics, ex-
tending office hours beyond
routine times during peak vac-
cination periods, considering
FIGURE 4 how to immunize parents and
Percentage of children with titers greater than 1:32 during seasons with no change in vaccine antigen. adult caregivers at the same
* One dose administered in the spring; the second dose administered in the fall. ** Two doses
administered 4 weeks apart in the fall. (Reprinted with permission from Englund JA, Fairchok MP, time in the same office setting
Monto AS, Neuzil KM. Pediatrics. 2005;115[4]:1039 –1047.) as children, and working with
other institutions (eg, schools,
child care centers, and reli-
original levels 6 to 12 months after ents and caregivers, and begin gious organizations) or alterna-
vaccination. Because the vaccine immunization of all children 6 tive care sites, such as emer-
strains for the 2011–2012 season months of age and older, espe- gency departments, to expand
are unchanged from last season, a cially children at high risk of venues for administering vac-
repeat dose this season is critical complications from influenza. cine while providing appropri-
for maintaining protection in all HCP endorsement plays a major ate documentation of immuni-
populations. role in vaccine uptake. A strong zation for the child’s medical
8. As soon as the trivalent seasonal correlation exists between HCP home.
influenza vaccine is available lo- endorsement of influenza vac- ● Concerted efforts among the
cally, health care personnel cine and patient acceptance. Pro- aforementioned groups, plus vac-
(HCP) should be immunized, pub- viders should continue to offer vac- cine manufacturers, distributors,
licize vaccine availability to par- cine through the vaccine expiration and payers, are also necessary to
4 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from www.aappublications.org/news by guest on February 18, 2020FROM THE AMERICAN ACADEMY OF PEDIATRICS
TABLE 1 Antiviral Drug Sensitivities of Influenza Strains Expected to Circulate During the 2011– ommended for children 6 months of
2012 Influenza Season
age and older and adults, including
Seasonal Influenza Vaccine Amantadine (Symmetrela)/ Oseltamivir Zanamivir
people with and without chronic med-
Strain (2011–2012) Rimantadine (Flumadineb) (Tamifluc) (Relenzad)
ical conditions. The most common ad-
Seasonal influenza A (H1N1) virus Resistant Susceptible Susceptible
(derived from 2009 pandemic verse events after administration are
influenza A [H1N1] virus) local injection-site pain and tender-
Seasonal influenza A (H3N2) virus Resistant Susceptible Susceptible ness. Fever might occur within 24
Seasonal influenza B virus Resistant Susceptible Susceptible
For current recommendations about treatment and chemoprophylaxis of influenza, see www.cdc.gov/flu/professionals/
hours after immunization in approxi-
antivirals/index.htm or www.aapredbook.org/flu. Circulating strains in local communities may vary from those found in the mately 10% to 35% of children younger
vaccine; antiviral sensitivities of these strains are reported weekly at www.cdc.gov/flu/weekly/summary.htm. than 2 years but rarely in older chil-
a Endo Pharmaceuticals (Chads Ford, PA).
b Forest Pharmaceuticals (St Louis, MO). dren and adults. Mild systemic symp-
c Roche Laboratories (Nutley, NJ).
d GlaxoSmithKline (Research Triangle Park, NC).
toms such as nausea, lethargy, head-
ache, muscle aches, and chills might
occur after administration of TIV.
appropriately prioritize distribu- Control and Prevention (CDC) Web An intradermal formulation of TIV has
tion to the primary care office set- site (www.cdc.gov/flu/index.htm). been licensed for the 2011–2012 sea-
ting, especially when vaccine sup- 11. As the 2011–2012 influenza sea- son for use in people 18 through 64
plies are delayed or limited. son unfolds, it is critically impor- years of age. This method of delivery
● Vaccine safety, effectiveness, tant for HCP to be aware of new involves a microinjection with a needle
and indications must be com- or changing recommendations 90% shorter than needles used for in-
municated properly to the pub- from the CDC or their local and state tramuscular administration. The most
lic. HCP should act as role mod- health departments. Up-to-date infor- common adverse events are redness,
els by receiving influenza mation can be found on the AAP induration, swelling, pain, and itching
immunization annually and rec- Web site (www.aap.org or http:// at the site of administration at a
ommending annual immuniza- aapredbook.aappublications.org/flu), slightly higher rate than occurs with
tions to both their colleagues through state-specific AAP chapter the intramuscular formulation of TIV.
and patients. Web sites, or on the CDC Web site Headache, myalgia, and malaise might
(www.cdc.gov/flu/index.htm). occur and tend to occur at the same
10. The neuraminidase inhibitors os-
rate as that with the intramuscular
eltamivir (Tamiflu [Roche Labora-
TRIVALENT SEASONAL INFLUENZA formulation of TIV. There is no prefer-
tories, Nutley, NJ]) and zanamivir
VACCINES ence for intramuscular or intradermal
(Relenza [GlaxoSmithKline, Re-
Tables 2 and 3 summarize information immunization in people 18 years of age
search Triangle Park, NC]) are the
on the 2 types of 2011–2012 trivalent or older; therefore, pediatricians may
only antiviral medications rou-
tinely recommended for chemo- seasonal influenza vaccines licensed choose to use either the intramuscular
prophylaxis or treatment during for immunization of children and or intradermal product in their late ad-
the 2011–2012 season. All strains adults: injectable trivalent inactivated olescent and young adult patients.
of influenza currently anticipated influenza vaccine (TIV) and intrana- Increased reports of febrile seizures in
to circulate are susceptible to sally administered live-attenuated in- the United States were noted by the
neuraminidase inhibitors but have fluenza vaccine (LAIV). Both vaccines Vaccine Adverse Event Reporting Sys-
high rates of resistance to aman- contain the identical strains of influ- tem (VAERS) and were associated with
tadine and rimantadine (Table 1). enza A subtypes (ie, H1N1 and H3N2) TIV manufactured by Sanofi Pasteur
Resistance characteristics might and influenza B anticipated to circulate (Fluzone), mainly in children in the 12-
change rapidly; clinicians should during the 2011–2012 influenza through 23-month age group (the peak
verify susceptibility information at season. age for febrile seizures), and included
the start of the influenza season and TIV is an inactivated vaccine that con- some who concurrently had received
monitor it during the season tains no live virus and cannot produce 13-valent pneumococcal conjugate
through either the AAP Web a viral infection. TIV formulations are vaccine (PCV13). All children fully re-
site (www.aap.org or http:// now available for intramuscular and covered. On the basis of current data,
aapredbook.aappublications.org/ intradermal use. The intramuscular prophylactic use of antipyretic agents
flu) or the Centers for Disease formulation of TIV is licensed and rec- in TIV-immunized children is not indi-
PEDIATRICS Volume 128, Number 4, October 2011 from www.aappublications.org/news by guest on February 18, 2020 5
DownloadedTABLE 2 Recommended Trivalent Seasonal Influenza Vaccines for Different Age Groups: United States, 2011–2012 Influenza Season
Vaccine Trade Name Manufacturer Presentation Ovalbumin Content, Thimerosal Mercury Age
g of Ovalbumin Content, g of Hg Group
per 0.5-mL Dose per 0.5-mL Dose
Inactivated
TIV Fluzone Sanofi Pasteur, Swiftwater, PA 0.25-mL prefilled syringe ⬃0.1a 0.0 6–35 mo
0.5-mL prefilled syringe ⬃0.1a 0.0 ⱖ36 mo
0.5-mL vial ⬃0.1a 0.0 ⱖ36 mo
5.0-mL multidose vial ⬃0.1a 25.0 ⱖ6 mo
TIV Fluzone intradermal Sanofi Pasteur, Swiftwater, PA 0.1-mL prefilled Not cited 0.0 18–64 y
microinjection
TIV Fluzone HD Sanofi Pasteur, Swiftwater, PA 0.5-mL prefilled syringe ⬃0.1a 0.0 ⱖ65 y
TIV Fluvirin Novartis, East Hanover, NJ 0.5-mL prefilled syringe ⱕ1.0b ⬍1.0 ⱖ4 y
5.0-mL multidose vial ⱕ1.0b 25 ⱖ4 y
TIV Fluarix GlaxoSmithKline, King of Prussia, PA 0.5-mL prefilled syringe ⱕ0.05b 0.0 ⱖ3 y
TIV FluLaval GlaxoSmithKline, King of Prussia, PA 5.0-mL multidose vial ⱕ1.0b 25.0 ⱖ18 y
TIV Afluria CSL Biotherapies, King of Prussia, PA 0.5-mL prefilled syringe ⱕ1.0b 0 ⱖ9c
5-mL multidose vial ⱕ1.0b 25.0 ⱖ9c
Live-attenuated
LAIV FluMist MedImmune, Gaithersburg, MD 0.2-mL sprayer Not cited 0.0 2–49 y
a Data obtained from Sanofi Pasteur (personal communication, 2011) suggests that the residual egg protein (expressed as ovalbumin) in Fluzone vaccine or in Fluzone High-Dose vaccine is
typically on the order of 0.1 g per dose.
b Data are from the package inserts, many of which have been updated for the 2011–2012 season.
Data sources: American Academy of Pediatrics, Committee on Infectious Diseases. Pediatrics. 2010;126(4):816 – 826; Centers for Disease Control and Prevention. MMWR Recomm Rep.
2010;59(RR-8):1– 62; and Centers for Disease Control and Prevention. Morb Mortal Wkly Rep. 2011;60 (Early Release):1– 6.
c Age indication per package insert is ⱖ5 years; however, the ACIP recommends Afluria not be used in children aged 6 months through 8 years because of increased reports of febrile
reactions noted in this age group. If no other age-appropriate, licensed inactivated seasonal influenza vaccine is available for a child aged 5 through 8 years of age who has a medical
condition that increases the child’s risk for influenza complications, Afluria can be used; however, providers should discuss with the parents or caregivers the benefits and risks of influenza
vaccination with Afluria before administering this vaccine.
cated, and current AAP and Advisory and Drug Administration for healthy tions using several different clinical
Committee on Immunization Practices people 2 through 49 years of age. It is end points. In 1 study that compared
(ACIP) recommendations for adminis- not recommended for people with a LAIV with TIV in infants and young
tration of TIV in this age group are un- history of asthma or other high-risk children without severe asthma or a
changed. Febrile seizures can occur medical conditions associated with recent history of wheezing, LAIV
anytime a child has a fever, but the typ- an increased risk of complications showed significantly better efficacy
ical child who has a febrile seizure re- from influenza (see “Contraindica- than TIV; results of other studies sug-
covers quickly and fully. tions and Precautions”). LAIV has the gest that TIV might be more effective
Previous febrile seizures or seizure potential to produce mild symptoms in young adults.
disorders are not a contraindication including rhinitis, headache, wheez- A large body of evidence demonstrates
to use of TIV or LAIV in otherwise eli- ing, vomiting, muscle aches, and fe- that thimerosal-containing vaccines
gible children. Use of antipyretic ver. LAIV should not be administered are not associated with increased risk
agents in febrile children does not to people with copious nasal conges- of autism spectrum disorders in chil-
reduce the incidence of febrile sei- tion that would impede vaccine dren. However, some people might
zures; therefore, routine use of anti- delivery. raise concerns about the minute
pyretic agents for avoiding febrile Both TIV and LAIV are cost-effective amounts of thimerosal in TIV vaccines,
seizures in children who receive in- strategies for preventing influenza and in some states, there is a legis-
fluenza vaccine is not recommended. among children and their families lated restriction on the use of
Approximately 2% to 5% of children 6 when circulating and vaccine strains thimerosal-containing vaccines for in-
months through 5 years of age will are matched closely, but efficacy var- fants and/or children. The benefits of
have at least 1 febrile seizure not as- ies according to the age of the recipi- protecting children against the known
sociated with vaccines in their ent. Current data from direct compar- risks of influenza are clear. Therefore,
lifetime. isons of the efficacy or effectiveness children should receive any available
LAIV is a live-attenuated influenza of these 2 vaccines are limited, be- formulation of TIV rather than delay
vaccine that is administered intrana- cause the studies were conducted in immunization while waiting for vaccines
sally and is licensed by the US Food a variety of settings and in popula- with reduced thimerosal content or for
6 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from www.aappublications.org/news by guest on February 18, 2020FROM THE AMERICAN ACADEMY OF PEDIATRICS
TABLE 3 LAIV Compared With TIV cine administration to people with egg
Vaccine Characteristic LAIV TIV allergy can happen without the need
Route of administration Intranasal spray Intramuscular or intradermal for referral. Data indicate that only ap-
injectiona proximately 1% of children have immu-
Type of vaccine Live virus Killed virus
Product Attenuated, Inactivated subvirion or noglobulin E–mediated sensitivity to
cold-adapted surface antigen egg, and of those, a very small minority
No. of included virus strains 3 (2 influenza A, 1 3 (2 influenza A, 1 influenza B) have a severe allergy.
influenza B)
Vaccine virus strains updated Annually Annually Standard immunization practice
Frequency of administrationb Annually Annually should include the ability to respond
Approved age groups All healthy persons aged All persons aged ⱖ6 mo
to acute hypersensitivity reactions.
2–49 y (intradermal 18–64 y)
Interval between 2 doses in children 4 wk 4 wk Therefore, influenza vaccine should be
Can be given to persons with medical risk No Yes given to people with egg allergy with
factors for influenza-related the following preconditions (Fig 5):
complications
Can be given to children with asthma or Noc Yes ● Appropriate resuscitative equip-
children aged 2–4 y with wheezing in ment must be readily available.1
the previous year
Can be simultaneously administered with Yesd Yesd ● Ovalbumin content up to 0.7 micro-
other vaccines grams/0.5 mL per vaccine dose
If not simultaneously administered, can No, prudent to space 4 Yes
has been well tolerated (Table 2).
be administered within 4 wk of another wk apart
live vaccine ● After immunization, the vaccine re-
Can be administered within 4 wk of an Yes Yes cipient should be observed in the of-
inactivated vaccine
a
fice for 30 minutes, the standard
The preferred site of TIV intramuscular injection for infants and young children is the anterolateral aspect of the thigh.
b See Fig 4 for decision algorithm to determine the number of doses of 2011–2012 seasonal influenza vaccine recommended observation time after receiving
for children this year. immunotherapy.
c LAIV is not recommended for children with a history of asthma. In the 2- through 4-year age group, there are children who
have a history of wheezing with respiratory illnesses in whom reactive airways disease is diagnosed and in whom asthma ● For children who need a second dose,
may later be diagnosed. Therefore, because of the potential for increased wheezing after immunization, children 2 through
4 years of age with recurrent wheezing or a wheezing episode in the previous 12 months should not receive LAIV. When
the same product brand is preferred, if
offering LAIV to children in this age group, a clinician should screen those who might be at higher risk of asthma by asking possible, but it does not need to be from
the parents/guardians of 2-, 3-, and 4-year-olds (24- to 59-month-olds) the question, “In the previous 12 months, has a health
the same lot as the first dose.
care professional ever told you that your child had wheezing?” If the parents answer “yes” to this question, LAIV is not
recommended for these children.
d LAIV coadministration has been evaluated systematically only among children 12 to 15 months of age with measles-
VACCINE STORAGE AND
mumps-rubella and varicella vaccines. TIV coadministration has been evaluated systematically only among adults with
pneumococcal polysaccharide and zoster vaccines.
ADMINISTRATION
Data sources: American Academy of Pediatrics, Committee on Infectious Diseases. Pediatrics. 2010;126(4):816 – 826; and
Fiore AE, Fry A, Shay D, Gubareva L, Bresee JS, Uyeki TM; Centers for Disease Control and Prevention. MMWR Recomm Rep. Intramuscular Vaccine
2011;60(RR-1):1–24.
The intramuscular formulation of TIV is
shipped and stored at 2°C to 8°C (35°F–
thimerosal-free vaccine. Although some have egg allergy. More conservative 46°F). It is administered intramuscu-
formulations of TIV contain only a trace approaches, such as skin testing or a larly into the anterolateral thigh of in-
amount of thimerosal, certain types can 2-step graded challenge, are no longer fants and young children and into the
be obtained with no thimerosal. LAIV recommended. deltoid muscle of older children and
does not contain thimerosal. Vaccine adults. The volume of vaccine is age
As a precaution, clinicians should de- dependent; infants and toddlers older
manufacturers are delivering increas-
ing amounts of thimerosal-free influenza termine if the presumed egg allergy is than 6 months but younger than 36
vaccine each year. based on a mild or severe reaction. months should receive a dose of 0.25
Mild reactions are defined as hives mL, and all people aged 3 years (36
Administration to Egg-Allergic alone; severe reactions involve cardio- months) and older should receive 0.5
Individuals vascular changes, respiratory and/or mL per dose.
Although both TIV and LAIV are pro- gastrointestinal tract symptoms, or
duced in eggs, recent data have shown reactions that require the use of epi- Intradermal Vaccine
that influenza vaccine administered in nephrine. Clinicians should consult The intradermal formulation of TIV
a single, age-appropriate dose is well with an allergist for children with a also is shipped and stored at 2°C to
tolerated by nearly all recipients who history of severe reaction. Most vac- 8°C (35°F– 46°F). The package insert
PEDIATRICS Volume 128, Number 4, October 2011 from www.aappublications.org/news by guest on February 18, 2020 7
Downloadedsecretions or can increase the risk
of aspiration, such as neurodevel-
opmental disorders, spinal cord in-
juries, seizure disorders, or neuro-
muscular abnormalities.
Although universal immunization for
all people 6 months of age and older
is recommended for 2011–2012, par-
ticular immunization efforts with ei-
ther TIV or LAIV should be made for
the following groups to prevent
transmission of influenza to those at
risk, unless contraindicated:
● Household contacts and out-of-
home care providers of children
younger than 5 years and at-risk
children of all ages (healthy con-
tacts 2– 49 years of age can receive
FIGURE 5 either TIV or LAIV).
Precautions for administering influenza vaccine to presumed egg-allergic recipients.
● Any female who is pregnant, consid-
ering pregnancy, or breastfeeding
should be reviewed for full adminis- dren 2 years of age and older can re- during the influenza season (TIV
tration details of this new product, ceive either TIV or LAIV. Particular fo- only). Studies have found that in-
which is licensed for the 2011–2012 cus should be on the administration of fants born to immunized women
season for persons 18 through 64 TIV for all children and adolescents have better influenza-related health
years of age. outcomes. However, data suggest
who have underlying medical condi-
that no more than one-half of preg-
tions associated with an increased
Live-Attenuated (Intranasal) nant women receive seasonal influ-
Vaccine risk of complications from influenza,
enza vaccine, although both preg-
including:
The cold-adapted LAIV formulation cur- nant women and their infants are at
● Asthma or other chronic pulmonary higher risk of complications. In ad-
rently licensed in the United States
diseases including cystic fibrosis. dition, there is limited evidence that
must be shipped and stored at 2°C to
8°C and administered intranasally in a ● Hemodynamically significant car- influenza vaccination in pregnancy
prefilled, single-use sprayer contain- diac disease. might decrease the risk of preterm
ing 0.2 mL of vaccine. A removable ● Immunosuppressive disorders or
birth.
dose-divider clip is attached to the therapy. ● HCP or health care volunteers. De-
sprayer to administer 0.1 mL sepa- spite the recent AAP recommenda-
● HIV infection.
rately into each nostril. Any of the influ- tion for mandatory influenza immu-
● Sickle cell anemia and other nization for all HCP,2 many HCP
enza vaccines can be administered at
the same visit with all other recom- hemoglobinopathies. remain unvaccinated. As of January
mended routine vaccines. After ad- ● Diseases that require long-term as- 2010, the CDC estimated that only
ministration of any live-virus vac- pirin therapy, including juvenile id- 62% of HCP received the seasonal
cine, at least 4 weeks should pass iopathic arthritis and Kawasaki vaccine and only 37% received the
before another live-virus vaccine is disease. 2009 H1N1 monovalent vaccine. HCP
administered. ● Chronic renal dysfunction.
frequently come into contact with
patients at high risk of influenza ill-
CURRENT RECOMMENDATIONS ● Chronic metabolic disease includ- ness in their clinical settings, so it is
Trivalent seasonal influenza immuniza- ing diabetes mellitus. paramount that HCP protect them-
tion is recommended for all children 6 ● Any condition that can compromise selves against influenza to remain
months of age and older. Healthy chil- respiratory function or handling of influenza free, to prevent disease
8 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from www.aappublications.org/news by guest on February 18, 2020FROM THE AMERICAN ACADEMY OF PEDIATRICS
transmission to patient populations should be balanced against the po- in the previous 12 months of age
at high risk, and to avoid lost work- tential morbidity and mortality as- should not receive LAIV.
place productivity. sociated with influenza for that indi- When offering LAIV to children 24
● Close contacts of immunosup- vidual child. through 59 months of age, the clinician
pressed people. ● Children who have received other should screen them by asking the par-
live-virus vaccines within the previ- ent/guardian the question, “In the pre-
CONTRAINDICATIONS AND
ous 4 weeks; however, other live- vious 12 months, has a health care pro-
PRECAUTIONS
virus vaccines can be given on the fessional ever told you that your child
Minor illnesses, with or without fe- same day as LAIV. had wheezing?” If a parent answers
ver, are not contraindications to the “yes” to this question, LAIV is not rec-
● Children with asthma, children with
use of influenza vaccines, particu- ommended for the child. TIV would be
other chronic disorders of the pul-
larly among children with mild upper recommended for the child to whom
monary or cardiovascular systems,
respiratory infection symptoms or LAIV is not given.
allergic rhinitis. or children 2 through 4 years of age
with a history of recurrent wheezing In addition, TIV is the vaccine of choice
Children Who Should Not Be or a medically attended wheezing for anyone in close contact with a sub-
Vaccinated With TIV episode in the previous 12 months. set of severely immunocompromised
people (ie, people in a protected envi-
● Infants younger than 6 months. ● Children with chronic underlying medi-
ronment). TIV is preferred over LAIV for
● Children who have a moderate-to- cal conditions including metabolic dis-
contacts of severely immunocompro-
severe febrile illness, on the basis of ease, diabetes mellitus, renal dysfunc-
mised people (ie, in a protected envi-
clinical judgment of the provider. tion, and hemoglobinopathies.
ronment) because of the theoretical
● Children who are known to have ex- ● Children who have known or sus- risk of infection in an immunocompro-
perienced Guillain-Barré syndrome pected immunodeficiency disease mised contact of an LAIV-immunized
(GBS) within 6 weeks after a previ- or who are receiving immunosup- person. Available data indicate that
ous influenza vaccination; whether pressive or immunomodulatory there is a very low risk of transmission
influenza vaccination specifically therapies. of the virus in both children and adults
might increase the risk of recur- ● Children who are receiving aspirin vaccinated with LAIV. HCP immunized
rence of Guillain-Barré syndrome is or other salicylates. with LAIV may continue to work in most
unknown; the decision not to immu- units of a hospital, including the NICU
● Any female who is pregnant or con-
nize should be thoughtfully bal- and general oncology wards, while us-
anced against the potential morbid- sidering pregnancy.
ing standard infection-control tech-
ity and mortality associated with ● Children with any condition that can niques. As a precautionary measure,
influenza for that individual child. compromise respiratory function or people recently vaccinated with LAIV
handling of secretions or can in- should restrict contact with severely
Children Who Should Not Be crease the risk for aspiration, such as
Vaccinated With LAIV immunocompromised patients (eg, he-
neurodevelopmental disorders, spi- matopoietic stem cell transplant recip-
● Children younger than 2 years. nal cord injuries, seizure disorders, ients during periods that require a
● Children who have a moderate-to- or neuromuscular abnormalities. protected environment) for 7 days af-
severe febrile illness. ter immunization, although there have
● Children with copious nasal conges- PRECAUTIONS been no reports of LAIV transmission
tion that would impede vaccine LAIV is not recommended for children from a vaccinated person to an immu-
delivery. with asthma. In the 2- through 4-year nocompromised person. In the theo-
● Children who are known to have ex- age range, many children have a his- retical scenario in which symptomatic
perienced Guillain-Barré syndrome tory of wheezing with respiratory tract LAIV infection develops in an immuno-
within 6 weeks after a previous in- illnesses and are eventually diagnosed compromised host, oseltamivir or
fluenza vaccination; whether influ- with asthma. Therefore, because of the zanamivir could be prescribed, be-
enza vaccination specifically might potential for increased wheezing after cause LAIV strains are susceptible to
increase the risk of recurrence of immunization, children younger than 5 these antiviral medications.
Guillain-Barré syndrome is un- years with recurrent wheezing or a Information about influenza surveil-
known; the decision not to immunize medically attended wheezing episode lance is available through the CDC
PEDIATRICS Volume 128, Number 4, October 2011 from www.aappublications.org/news by guest on February 18, 2020 9
DownloadedTABLE 4 Recommended Dosage and Schedule of Influenza Antiviral Medications for Treatment and Chemoprophylaxis for the 2011–2012 Influenza
Season: United States
Medication Treatment (5 d) Chemoprophylaxis (10 d)
Oseltamivira
Adults 75 mg twice daily 75 mg once daily
Children ⬎12 mo
Body weight
ⱕ15 kg (ⱕ33 lb) 30 mg twice daily 30 mg once daily
⬎15 to 23 kg (33 to 51 lb) 45 mg twice daily 45 mg once daily
⬎23 to 40 kg (⬎51 to 88 lb) 60 mg twice daily 60 mg twice daily
⬎40 kg (⬎88 lb) 75 mg twice daily 75 mg once daily
Children 3 to ⬍12 mob 3 mg/kg per dose twice daily 3 mg/kg per dose once per day
Children 0 to ⬍3 moc 3 mg/kg per dose twice daily Not recommended unless situation
judged critical because of limited
data on use in this age group
Zanamivird
Adults 10 mg (two 5-mg inhalations) twice daily 10 mg (two 5-mg inhalations) once daily
Children (ⱖ7 y for treatment, 5 y for 10 mg (two 5-mg inhalations) twice daily 10 mg (two 5-mg inhalations) once daily
chemoprophylaxis
a Oseltamivir is manufactured by Roche Laboratories (Nutley, NJ) and is administered orally without regard to meals, although administration with meals may improve gastrointestinal
tolerability. Oseltamivir is available as Tamiflu in 30-, 45-, and 75-mg capsules and as a powder for oral suspension that is reconstituted to provide a final concentration of 6 mg/mL. The
volume of oral suspension is being changed from 12 mg/mL to 6 mg/mL this year to reduce frothing when shaken. Oral suspensions in 12 mg/mL concentrations will remain available
until supplies run out. For the 6-mg/mL suspension, a 30-mg dose is given with 5 mL of oral suspension, 45-mg dose is given with 7.5 mL oral suspension, 60-mg dose is given
with 10 mL oral suspension, and 75-mg dose is given with 12.5 mL oral suspension. If the commercially manufactured oral suspension is not available, the capsules may be opened
and the contents mixed with a sweetened liquid to mask the bitter taste, or a suspension can be compounded by retail pharmacies (final concentration: 15 mg/mL). For patients with renal
insufficiency, the dose should be adjusted on the basis of creatinine-clearance rate. For treatment of patients with a creatinine-clearance rate of 10 to 30 mL/min: 75 mg once daily for 5 days.
For chemoprophylaxis of patients with a creatinine-clearance rate of 10 to 30 mL/min: 30 mg once daily for 10 days after exposure or 75 mg once every other day for 10 days after exposure
(5 doses). (See www.cdc.gov/flu/professionals/antivirals/antiviral-drug-resistance.htm.)
b Weight-based dosing is preferred; however, if weight is not known, dosing according to age for treatment (give 2 doses per day) or prophylaxis (give 1 dose per day) of influenza in term
infants younger than 1 year may be necessary: 0 to 3 months (treatment only), 12 mg (2 mL of 6 mg/mL commercial suspension); 4 to 5 months, 17 mg (2.8 mL of 6 mg/mL of commercial
suspension); 6 to 11 months, 24 mg (4 mL of 6 mg/mL commercial suspension). Although Emergency Use Authorization recommendations for use of oseltamivir in children younger than 1
y expired on June 23, 2010, this drug remains appropriate for use when indicated.
c Current weight-based dosing recommendations are not intended for preterm infants. Preterm infants may have slower clearance of oseltamivir because of immature renal function, and
doses recommended for term infants may lead to very high drug concentrations in this age group. Limited data from a cohort of preterm infants who received an average dose of 1.7 mg/kg
twice daily revealed drug concentrations higher than those observed with the recommended treatment dose in term infants (3 mg/kg twice daily). Observed drug concentrations were highly
variable among preterm infants. These data are insufficient to recommend a specific dose of oseltamivir for preterm infants.
d Zanamivir is manufactured by GlaxoSmithKline (King of Prussia, PA) and is administered by inhalation using a proprietary “Diskhaler” device distributed together with the medication.
Zanamivir is a dry powder (not an aerosol) and should not be administered by using nebulizers, ventilators, or other devices typically used for administering medications in aerosolized
solutions. Zanamivir is not recommended for persons with chronic respiratory diseases such as asthma or chronic obstructive pulmonary disease that increase the risk of bronchospasm.
Data source: Fiore AE, Fry A, Shay D, Gubareva L, Bresee JS, Uyeki TM; Centers for Disease Control and Prevention. MMWR Recomm Rep. 2011;60(RR-1):1–24.
Voice Information System (influenza VACCINE IMPLEMENTATION ward that strain. For example, during
update, 888-232-3228) or at www.cdc. These updated recommendations for the 2010 –2011 season, only 1.3% of in-
gov/flu/index.htm. Although current in- prevention and control of influenza in fluenza viruses tested were resistant
fluenza season data on circulating children will have considerable opera- to oseltamivir, and none were resis-
strains do not necessarily predict tant to zanamivir. High levels of resis-
tional and fiscal effect on pediatric
which and in what proportion strains tance to amantadine and rimantadine
practice. Therefore, the AAP has devel-
will circulate in the subsequent season, persist, and these drugs should not be
oped implementation guidance on sup-
it is instructive to be aware of 2010 –2011 used in the upcoming season unless
ply, payment, coding, and liability is-
influenza surveillance data and use them resistance patterns change signifi-
sues; these documents can be found at
as a guide to empiric therapy until cur- cantly (Table 1).
www.aapredbook.org/implementation.
rent seasonal data are available from
the CDC. Information is posted weekly ● Oseltamivir is available in capsule
USE OF ANTIVIRAL MEDICATIONS and oral-suspension formulations.
by the CDC (www.cdc.gov/flu/weekly/
fluactivitysurv.htm). During the 2010 – Antiviral resistance can emerge The manufactured liquid formulation
2011 season, most activity was attrib- quickly from one season to the next. If has a concentration of 6 mg/mL. Oral
utable to influenza A; approximately local or national influenza surveillance suspensions in 12 mg/mL concentra-
66% was attributable to influenza A data indicate a predominance of a par- tions will remain available until sup-
(H3N2) activity, and 34% was attribut- ticular influenza strain with a known plies run out. If the commercially
able to 2009 (H1N1) activity. Activity antiviral-susceptibility profile, then manufactured oral suspension is not
varied widely on a local level. empiric treatment can be directed to- available, the capsule might be
10 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from www.aappublications.org/news by guest on February 18, 2020FROM THE AMERICAN ACADEMY OF PEDIATRICS
TABLE 5 Persons at Higher Risk Treatment should be considered for: People with suspected influenza who
Recommended for Antiviral
Treatment for Suspected/Confirmed ● Any otherwise healthy child with in- present with an uncomplicated febrile
Influenza fluenza infection for whom a de- illness typically do not require treatment
Children ⬍2 y of age crease in duration of clinical symp- with antiviral medications unless they
Adults ⱖ65 y of age are at higher risk of influenza complica-
toms is felt to be warranted by his
Persons with chronic pulmonary (including
asthma), cardiovascular (except hypertension or her provider if treatment can be tions, especially in situations with lim-
alone), renal, hepatic, hematologic (including initiated within 48 hours of illness ited antiviral medication availability.
sickle cell disease), or metabolic (including onset. Should there be a shortage of antiviral
diabetes mellitus) disorders or neurologic and
Earlier treatment provides more opti- medications, local public health authori-
neurodevelopmental conditions (including
disorders of the brain, spinal cord, peripheral mal clinical responses, although treat- ties might provide additional guidance
nerve, and muscle, such as cerebral palsy,
ment after 48 hours of symptoms in about testing and treatment. Rapid
epilepsy [seizure disorders], stroke,
the child with moderate-to-severe dis- antigen tests are not helpful in the
intellectual disability [mental retardation],
moderate-to-severe developmental delay, ease or with progressive disease management of children with sus-
muscular dystrophy, or spinal cord injury)
might still provide some benefit. Dos- pected influenza.
Persons with immunosuppression, including that
caused by medications or by HIV infection ages for antiviral agents for both treat- Recommendations for chemoprophy-
Women who are pregnant or in the postpartum ment and chemoprophylaxis in children laxis during an influenza outbreak:
period (within 2 wk after delivery)
Persons aged ⬍19 y who are receiving long-term
can be found in Table 4 and on the ● For children at high risk of compli-
aspirin therapy CDC Web site (antivirals/index.htm;/ cations from influenza for whom in-
American Indian/Alaska Native persons Border [0 0 0]?⬎www.cdc.gov/flu/ fluenza vaccine is contraindicated.
Persons who are morbidly obese (ie, BMI ⱖ 40) professionals/antivirals/index.htm).
Residents of nursing homes and other chronic ● For children at high risk during the 2
care facilities Children younger than 1 year are at weeks after influenza immunization.
Data source: Fiore AE, Fry A, Shay D, Gubareva L, Bresee JS, increased risk of influenza-related
● For family members or HCP who are
Uyeki TM; Centers for Disease Control and Prevention. complications. Although there are no
MMWR Recomm Rep. 2011;60(RR-1):1–24.
antiviral medications licensed by the unimmunized and are likely to have
Food and Drug Administration for ongoing, close exposure to:
opened and the contents mixed with a this age group and the 2009 H1N1 ● unimmunized children at high
sweetened liquid by retail pharma- pandemic Emergency Use Authoriza- risk; or
cies to a final concentration of 15 tion has expired, recommendations ● infants and toddlers who are
mg/mL (Table 4, footnote “a”). for use of oseltamivir in this young younger than 24 months.
● Current treatment guidelines (Table age group can still be followed and ● For control of influenza outbreaks
4) are applicable to infants and chil- are provided in Table 4. for unimmunized staff and children
dren with suspected influenza when Clinical judgment (based on underly- in a closed institutional setting with
known virus strains are circulating ing conditions, disease severity, time children at high risk (eg, extended
in the community or when infants or since symptom onset, and local influ- care facilities).
children are confirmed to have sea- enza activity) is an important factor in
● As a supplement to immunization
sonal influenza. treatment decisions for pediatric pa-
among children at high risk, includ-
● Continuous monitoring of the epide- tients who present with influenza-
ing children who are immunocom-
miology, change in severity, and likeillness. Antiviral treatment should
promised and might not respond to
resistance patterns of influenza be started as soon as possible after
vaccine.
strains might lead to new guidance. illness onset and should not be de-
layed while waiting for a definitive in- ● As postexposure prophylaxis for
Treatment should be offered for: family members and close contacts
fluenza test result. Currently available
● Any child hospitalized with pre- rapid antigen tests have low sensitiv- of an infected person if those people
sumed influenza or with severe, ity, particularly for the 2009 pandemic are at high risk of complications
complicated, or progressive illness, influenza A (H1N1) virus strain and from influenza.
regardless of influenza immuniza- should not be used to rule out influ- ● For children at high risk and their
tion status. enza. Negative results from rapid anti- family members and close contacts,
● Influenza infection of any severity in gen tests should not be used to as well as HCP, when circulating
children at high risk of complica- make treatment or infection-control strains of influenza virus in the com-
tions of influenza infection (Table 5.) decisions. munity are not matched with triva-
PEDIATRICS Volume 128, Number 4, October 2011 from www.aappublications.org/news by guest on February 18, 2020 11
Downloadedlent seasonal influenza vaccine home. However, medical homes might immunization programs. Optimal pre-
strains, on the basis of current data have limited capacity to accommodate vention of influenza in the health care
from the CDC and local health all patients (and their families) who setting depends on coverage of at
departments. seek influenza immunization. Because least 90% of HCP. Finally, efforts are
These recommendations apply to rou- of the increased demand for immuni- underway to improve the vaccine-
tine circumstances, but it should be zation during each influenza season, development process to allow for a
noted that guidance might change on the AAP and the CDC recommend vac- shorter interval between identification
the basis of updated recommenda- cine administration at any visit to the of vaccine strains and vaccine
tions from the CDC in concert with medical home during influenza season production.
antiviral-agent availability, local re- when it is not contraindicated, at spe-
sources, clinical judgment, recom- cially arranged “vaccine-only” ses- COMMITTEE ON INFECTIOUS DISEASES,
mendations from local or public health sions, and through cooperation with 2011–2012
community sites, schools, and child Michael T. Brady, MD, Chairperson
authorities, risk of influenza complica- Carrie L. Byington, MD
tions, type and duration of exposure care centers to provide influenza vac- H. Dele Davies, MD
contact, and change in epidemiology cine. If alternate venues are used, a Kathryn M. Edwards, MD
system of patient record transfer is Mary P. Glode, MD
or severity of influenza. Mary Anne Jackson, MD
Chemoprophylaxis should not be con- beneficial for ensuring maintenance Harry L. Keyserling, MD
sidered a substitute for immunization. of accurate immunization records. Yvonne A. Maldonado, MD
Immunization-information systems Dennis L. Murray, MD
Influenza vaccine should always be of- Walter A. Orenstein, MD
fered when not contraindicated, even should be used whenever available. Gordon E. Schutze, MD
when influenza virus is circulating in Cost-effectiveness and logistic feasibil- Rodney E. Willoughby, MD
Theoklis E. Zaoutis, MD
the community. Antiviral medications ity of vaccinating everyone continue to
currently licensed are important ad- be concerns. With universal immuniza- FORMER COMMITTEE MEMBER
juncts to influenza immunization for tion, particular attention is being paid Margaret C. Fisher, MD
control and prevention of influenza to vaccine supply, distribution, imple-
mentation, and financing. Potential LIAISONS
disease, but indiscriminate use might Marc A. Fischer, MD – Centers for Disease
promote resistance and/or limit avail- benefits of more widespread child- Control and Prevention
ability (Table 1). Providers should in- hood immunization among recipients, Bruce Gellin, MD – National Vaccine Program
their contacts, and the community in- Office
form recipients of antiviral chemopro-
Richard L. Gorman, MD – National Institutes of
phylaxis that risk of influenza is clude fewer influenza cases, fewer out- Health
lowered but still remains while taking patient visits and hospitalizations for Lucia Lee, MD – Food and Drug Administration
medication, and susceptibility to influ- influenza infection, and a decrease in R. Douglas Pratt, MD – Food and Drug
Administration
enza returns when medication is the use of antimicrobial agents, absen- Jennifer S. Read, MD – National Vaccine
discontinued. For recommendations teeism from school, and lost parent Program Office
about treatment and chemoprophy- work time. Joan Robinson, MD – Canadian Paediatric
Society
laxis against influenza, see Table 4. Up- Continued evaluation of the safety, im- Jane Seward, MBBS, MPH – Centers for
dates will be available at www. munogenicity, and effectiveness of in- Disease Control and Prevention
aapredbook.org/flu and www.cdc. Jeffrey R. Starke, MD – American Thoracic
fluenza vaccine, especially for children
Society
gov/flu/professionals/antivirals/index. younger than 2 years, is important. De- Jack Swanson, MD – Committee on Practice
htm. velopment of a safe, immunogenic vac- Ambulatory Medicine
cine for infants younger than 6 months Tina Q. Tan, MD – Pediatric Infectious Diseases
FUTURE NEEDS Society
is essential. Consideration of how best
Manufacturers anticipate being able to offer to immunize parents and adult EX OFFICIO
to provide adequate supplies of vac- child care providers in the pediatric Carol J. Baker, MD – Red Book Associate Editor
Henry H. Bernstein, DO – Red Book Associate
cine. Efforts should be made to create office setting continues to be investi-
Editor
adequate outreach and infrastructure gated. Mandatory annual influenza im- David W. Kimberlin, MD – Red Book Associate
to ensure an optimal distribution of munization has been implemented Editor
vaccine so that more people are immu- successfully at pediatric institutions, Sarah S. Long, MD – Red Book Associate Editor
H. Cody Meissner, MD – Red Book Associate
nized. Health care for children should and future efforts should include Editor
be provided in the child’s medical broader implementation of mandatory Larry K. Pickering, MD – Red Book Editor
12 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from www.aappublications.org/news by guest on February 18, 2020You can also read