Resident Brown Recluse Spider Bites - EMRA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Resident
Official Publication of the Emergency Medicine Residents’ Association
June/July 2020
Brown Recluse
VOL 47 / ISSUE 3
Spider Bites
Pitfalls of US-guided
IV Placement
ITP Beyond
the Boards
Maintaining
Wellness in
Residency
Exciting opportunities at
our growing organization
• Adult and Pediatric Emergency Medicine Faculty positions
• Medical Director
• Vice Chair, Clinical Operations
• Vice Chair, Research
• Medical Student Clerkship Director
Penn State Health, Hershey PA, is expanding our health system. We What the Area Offers:
offer multiple new positions for exceptional physicians eager to join our We welcome you to a community that
dynamic team of EM and PEM faculty treating patients at the only Level I emulates the values Milton Hershey
Adult and Level I Pediatrics Trauma Center in Central Pennsylvania. instilled in a town that holds his name.
Located in a safe family-friendly setting,
What We’re Offering:
Hershey, PA, our local neighborhoods boast
• Salaries commensurate with qualifications
a reasonable cost of living whether you
• Sign-on Bonus
prefer a more suburban setting or thriving
• Relocation Assistance
city rich in theater, arts, and culture. Known
• Retirement options, Penn State University Tuition Discount, and so
as the home of the Hershey chocolate
much more!
bar, Hershey’s community is rich in history
What We’re Seeking: and offers an abundant range of outdoor
• Emergency Medicine trained physicians with additional training in any activities, arts, and diverse experiences.
of the following: Toxicology, Ultrasound, Geriatric Medicine, Pediatric We’re conveniently located within a
Emergency Medicine, Research short distance to major cities such as
• Completion of an accredited Residency Program. Philadelphia, Pittsburgh, NYC, Baltimore,
• BE/BC by ABEM or ABOEM and Washington DC.
FOR MORE INFORMATION PLEASE CONTACT:
Heather Peffley, PHR FASPR at: hpeffley@pennstatehealth.psu.edu
Penn State Health is committed to affirmative action, equal opportunity and the diversity of its workforce. Equal Opportunity Employer – Minorities/Women/Protected Veterans/Disabled.
Time for Gratitude
Hello EMRA Family, “When I was a boy, and I would see exhaustion, and unrelenting body aches.
I
will be honest; the past few months scary things in the news, my mother Pre-coronavirus, I was a very active person
have been difficult, as I am sure it has would say to me, ‘Look for the helpers. — mentally and physically. I worked out
been for a lot of you as well. It has been You will always find people who are several times a week, read most days out of
a rollercoaster of emotions riddled with helping’ “ — this quote by Mr. Rogers the week, and felt motivated to continuously
guilt, fear, and frustration, often leaving rings truer than ever today. During the progress upward in my career. The STOP
me feeling emotionally exhausted and pandemic, even while witnessing so many the virus placed on my body and life was
physically unmotivated. horrid things, I have also been blessed to jarring. A week and a half flew by while I
COVID-19, the novel virus that forever see so many helpers. mostly moved between my bed and chair.
changed the landscape of medicine I have been inspired by medical I felt unmotivated and discouraged. I felt
and society. Globally and nationally, it students who have used social media to guilty about missing my shifts while I
brought out and highlighted our gross gather PPEs to donate. Encouraged by recovered. I felt saddened, by proxy, when I
shortcomings as a medical institution. everyday folks pooling their spoke to my parents on video chat, who had
It has stripped us of some of life’s most resources to provide for a struggling to stay away from their sick daughter. I felt
joyous moments: weddings, graduation, neighbor. Astonished by the physician let-down that I was getting behind on my
concerts, baby showers. mothers and fathers living outside their residency and EMRA tasks.
It has taken lives. Countless of homes, isolating themselves from their
Now, close to 2 months post-recovery, I
colleagues/family members/friends have family and children, while they proudly
am THANKFUL.
succumbed to this virus, sometimes at the continue their mission of care and service
I am thankful for that ‘down-time’: time
peak of their lives. to others.
to stop and focus on just myself helped me
It has robbed us of humanity. We’ve I have also formed more profound
re-prioritize my life. I have used this time
had to tell patients’ family members, while connections with friends and colleagues
to reach out to friends from college and
they are crying in front of us, that they will who have only existed in a superficial
medical school that I have not spoken to in
not be able to visit their loved ones in the realm until now. We have had more time
a few months. I used the lack of distractions
hospital once admitted. And we’ve had to to open up and speak vulnerably and
to reconnect with my husband and friends
see our patients die in an empty room. honestly, and connections have been
and helped strengthen friendships and
This has created an incredible mental forged and strengthened by relating to
relationships.
and spiritual strain on all of us. This is a collective trauma. One of my favorite
trauma we will be dealing with for the rest questions that prompted many of these I am filled with newfound gratitude
of our lives. connections/conversations has been: when I go for a run on a warm day, and I
But let’s not let this virus take What’s one positive you have can breathe in the air deeply without the
anything more from us. learned from this time? dyspnea I had felt for weeks. Speaking with
Let’s not let it take our ability to This has led to some of the most family members on video chat has taken on
connect emotionally, even if it’s through authentic answers. I witnessed melancholy a new sense of joy as I am lucky enough to
our phones and laptops. Let’s not let it take colleagues light up when answering. This be present at this moment to be able to do it.
our ability to open up and be vulnerable to question truly makes us re-frame the To my #EMRAFamily, times are tough.
others as we share our valleys and peaks. situation at hand. But don’t let this virus take away
Let’s let it serve as a reminder to prioritize I implore you all to ask this question anything more than it already has. Take
ourselves and the people we care about AND share authentically yourself. I will the time to talk to our colleagues, friends,
most. Friends, our careers are important, help start the conversation: family. Do not repress your thoughts.
but the connections we create in this world I contracted COVID-19 in March. Journal and self-reflect authentically. It’s
with our fellow humans are what makes What I thought was just nasal congestion ok not to be ok. Reach out when you need
life meaningful. turned into dyspnea on exertion, extreme to. We are all in this together. ¬
Facing COVID-19
together on the
front lines.
Stronger
Togeth
Together
Stronger together means leadership by front-line physicians and
advanced providers. We are a physician-led and -owned partnership
united by compassion and collaboration. Our clinicians deliver
integrated acute care at practice sites across the nation, working
together to achieve our greatest goal: saving lives.
Learn how Vituity’s clinicians are fighting
the epidemic at vituity.com/COVID-19.
Vituity ® is a registered trademark of CEP America, LLC.
© CEP America, LLC, All Rights Reserved.
TABLE OF CONTENTS
5 Transition, Not
Competition 28 DIY: CI
Tips for Getting into
EDITORIAL STAFF
PRESIDENT’S MESSAGE EDITOR-IN-CHIEF
Clinical Informatics Priyanka Lauber, DO
INFORMATICS,
6 Update from the ACGME
Review Committee for
CAREER PLANNING
Lehigh Valley Health Network
EDITORIAL TEAM
Emergency Medicine
LEADERSHIP REPORT 32 Until Help Arrives –
Prehospital Emergency
Marc Cassone, DO
Geisinger Medical Center
Brian Freeman, DO
Education All Citizens
8 Systemic Ioxoscelism
TOXICOLOGY Should Have
Lakeland Health
Sean Hickey, MD
PREHOSPITAL/DISASTER
11 The Phenomenon
of Tumor Neglect
MEDICINE
Mount Sinai Hospital
Whitney Johnson, MD
MENTAL HEALTH 34 Maintaining Wellness
as an EM Resident
UCSF-Fresno
Jeremy Lacocque, DO
12 Atypical Hemolytic
Uremic Syndrome
WELLNESS UCSF EMS Fellow
Jason Silberman, MD
CRITICAL CARE
36 A Letter to Graduating
Residents & Fellows
University of Tennessee
14 Recognition and
Management of Nerve
During the COVID-19
Pandemic
Samuel Southgate
University of Connecticut
Agent Exposure CAREER PLANNING MSC Editor
TOXICOLOGY David Wilson
16 Reviewing Accidental 38 Room 16 Right
HEART OF EM
Sidney Kimmel Medical College
Thomas Jefferson University
Hypothermia ECG Faculty Editor
WILDERNESS MEDICINE
39 Dexamethasone
in ARDS
Jeremy Berberian, MD
ChristianaCare
18 ITP Beyond the Boards
HEMATOLOGY
CRITICAL CARE/PULMONARY
PEM Faculty Editor
41 A Resident’s Intro to Billing
Yagnaram Ravichandran, MBBS, MD, FAAP
20 A Case of Severe
Malaria in the ED
ADMIN & OP
Dayton Children’s Hospital Pediatric ED
Clinical Asst. Professor of Pediatrics
43 What
Wright State University
INFECTIOUS DISEASE is Surprise Billing…
and Why Should I Care? Toxicology Faculty Editor
22 A Pause to Consider
Strongyloides Stercoralis
HEALTH POLICY David J. Vearrier, MD, MPH, FACMT,
FAACT, FAAEM
in the ED
INFECTIOUS DISEASE
44 Not Your Mother’s
AAWEP…
EM Resident (ISSN 2377-438X) is the
CAREER PLANNING
24 Common Pitfalls of bi-monthly magazine of the Emergency
49 News & Notes
Medicine Residents’ Association (EMRA).
Ultrasound-Guided The opinions herein are those of the
Peripheral IV Placement NEW GUIDES, HEALTH POLICY, authors and not of EMRA or any institutions,
ULTRASOUND ABEM, AND MORE organizations, or federal agencies. EMRA
encourages readers to inform themselves
26 Implicit Bias Is Both
Helpful and Harmful,
51 ECG Challenge
INTERPRET AND DIAGNOSE
fully about all issues presented. EM Resident
reserves the right to edit all material and does
So What Can We Do? not guarantee publication.
ADMIN & OPS 53 Board Review
Questions
© Copyright 2020
Emergency Medicine Residents’ Association
PEER ASSISTANCE
June/July 2020 | EM Resident 3
INTRODUCING
MobilEM
Free content and in-app purchases
Top 5 reasons why you
should download this
awesome app!
• Comprehensive digital library
of EMRA’s most popular
clinical resources
• Continual updates that require no
action on your part (simply open the
app to get up-to-the-minute content)
• 2 types of search
(targeted and universal)
• Bookmarking
• New resources added constantly
All of this for only
links
$333/month
Get direct Annual subscription $3999
and
to iTunes
y at
Google Pla s!
app
emra.org/
Emergency Medicine Residents’ Association
4 EMRA | emra.org • emresident.org www.emra.org | emra@emra.org | @emresidents |
PRESIDENT’S MESSAGE
Transition,
Not
Competition
Hannah R. Hughes, MD, MBA electives, and fluctuating patient volumes. out of the imposter syndrome spiral:
President, EMRA Pre-coronavirus, we would have had time 1. Don’t be afraid to say, “I don’t
Chief Resident, to reflect on the year we just finished, know.”
University of Cincinnati Emergency Medicine
prepare for the year ahead, maybe even Regardless of where you are in train-
@hrh_approved
T
take that vacation we’ve been dreaming ing, no one expects you to know it all,
wo months into my intern year,
about forever. and this is especially true for early
I had my first case presented at
But now? interns who are just getting used to
Morbidity & Mortality conference.
Now, we’ve endured weeks of being called “Doctor.” As my chief
An elderly man with metastatic prostate
unremitting high alert. We’ve been, resident told me early in my intern
cancer came in with back pain and known
by turns, overwhelmed by volume and year, “If you were expected to enter
spinal lesions. While his neurologic driven to distraction by eerily empty training already knowing everything,
exam was initially normal, he developed ED waiting rooms. Our students are residency wouldn’t be a thing.” It’s OK
paraplegia within hours, and it was sidelined, our graduates are facing to not know; we’re all here to learn.
missed. I was crushed. Ten years of unexpected unemployment, and we don’t 2. Demonstrate vulnerability.
undergraduate and graduate education know what this year will bring. Failure is inevitable, whether it’s your
spent aiming to be at the top of my It doesn’t make for the first patient of intern year or well into
game, only to fail a patient so early in smoothest transition of all time. being an attending. We all are or will
my residency training? It made for a As I shift from running our Shock be #BAFERDs, but we are also human
tough transition from medical student to and Resuscitation Unit as a third-year and bound to make mistakes. Sharing
physician. resident to supervising interns as a fourth those with others requires vulnerabil-
And here we are again, on the brink of year, I worry. Have my extracurricular ity, a demonstration of bravery, not
another transition. interests pulled me away from keeping weakness.
The start of a new academic year up with evidence-based medicine? Have I 3. Support one another.
is full of anxiety as we all step into our run enough resuscitations of critically ill Life is not a competition. There is no
new roles, regardless of what level we’ve patients? What if my interns know more race – and in EM, no finish line (every
reached in training. It’s part of the than me when I’m supposed to be the one empty waiting area fills up again).
medical maturation process. But this teaching them? All those frantic footsteps you hear
year, it just feels… different. The spiral always ends with the same are not people trying to outrun you;
Being on the front lines of COVID-19, question: Am I good enough? they’re your fellow caregivers, making
it seems as though we’ve matured years Having an early M&M case shook my sure you and your patients are not
in just a matter of months, in many ways. confidence, and the same can be true for alone. And heads-up: You’re doing the
Yet there’s still this uneasiness as we role transitions. Self-doubt can be either same for them, whether you realize it
step into our new roles, particularly in debilitating or harnessed as a tool for or not. EM is a team endeavor, not a
the setting of delayed rotations, canceled growth. Here are 3 reminders that get me solo sprint. ¬
References available online June/July 2020 | EM Resident 5
LEADERSHIP REPORT
Update from the ACGME Review
Committee for Emergency Medicine
Breanne Jaqua, DO, MPH
ACGME Review Committee for Emergency Medicine
Mercy St. Vincent Medical Center
@BreanneJaqua
A
s the resident representative to ACGME’s Review Committee for Emergency Medicine, it is my pleasure and honor to provide
an RC-EM update to EMRA and the readers of EM Resident magazine.
Please read on for updates in 5 key areas affecting emergency medicine residents:
Hospital closures Parental leave
Diversity in medicine Single Accreditation System
COVID-19
Ohio Valley Medical Center’s hospital standardized approach to parental leave
1. Hospital Closures
closure was announced in August policies for resident and fellow parents
Excluding the global pandemic, 2019.1 All 15 internal medicine and 17 by certifying boards, accreditation
the most well-known issue in graduate emergency medicine residents were able requirements, Sponsoring Institutions,
medical education over the past year to transfer to other training programs, and programs.”4
was the sudden closure of Hahnemann and a total of 325 positions were offered Final recommendations are expected
University Hospital in the summer of to the displaced residents.1 This closure in 2020.
2019.1 A total of 553 residents and fellows was different than Hahnemann’s
from 35 programs were affected by this 3. Diversity
because Ohio Valley Medical Center did
abrupt announcement, including 55 not declare bankruptcy, therefore tail Diversity is an important topic at the
residents and fellows on J-1 visas.1 ACGME. The revised common program
coverage was provided to these residents.1
The response from the medical requirements that went into effect in July
The February 2020 ACGME Annual
community was overwhelming and 2019 included a new core requirement,
Educational Conference included
supportive; the ACGME, AMA, AOA, item I.C., that codifies diversity in
excellent discussion and recognition of
AAMC, ECFMG, NRMP, FSMB, ABMS, graduate medical education.
the lessons learned from these events and
and many other medical organizations “The program, in partnership
plans for how to be better prepared for
came together to support the trainees with its Sponsoring Institution, must
future hospital closures.1
affected.1 A total of 1,530 available engage in practices that focus on
positions were offered to the displaced 2. Parental Leave mission-driven, ongoing, systematic
trainees, representing a total of 190 recruitment and retention of a diverse
sponsoring institutions in 39 states.1 Parental/family leave is a topic that and inclusive workforce of residents,
Ultimately, 100% of the displaced has gained a lot of attention in recent fellows (if present), faculty members,
residents and fellows transferred to new months, thanks to the advocacy of the senior administrative staff members, and
programs, and 60% were able to stay in ACGME’s Council of Review Committee other relevant members of its academic
the Philadelphia metro area.1 Hahnemann Residents.4 In the fall of 2019, the community.”5
University Hospital declared bankruptcy ACGME created a multi-disciplinary task The ACGME hired William A. McDade,
in addition to closing the hospital, which force dedicated to this topic. Parental/ MD, PhD, as its first Chief Diversity
left 1,400+ trainees and alumni without family leave is a multifaceted issue that and Inclusion Officer in March 2019.6
medical liability “tail” coverage.2 A has ramifications for board eligibility, Dr. McDade comes to the ACGME from
$9.3 million settlement was reached in which is why the task force includes direct Ochsner Health System in New Orleans,
March 2020, ensuring liability coverage collaboration with the American Board of where he was executive vice president
for Hahnemann residents, fellows, and Medical Specialties (ABMS).4 and chief academic officer. Prior to his
alumni.3 “This work will lead to a more appointment at Ochsner, Dr. McDade was
6 EMRA | emra.org • emresident.org
a professor of anesthesia and critical care All GME programs can apply for proposed language closed March 25.11
at the University of Chicago. osteopathic recognition, which provides If approved by the ACGME Board of
On Feb. 20, 2020, the ACGME osteopathic training in graduate medical Directors, the new language will take
announced Bonnie Mason, MD, as the education.8 effect July 2020.
Vice President of Diversity and Inclusion.7 As of March 2020, 89% of the 62
Prior to joining the ACGME, Dr. Mason previously AOA-accredited emergency 6. COVID-19
was the founder and executive director medicine programs have an accreditation These are unprecedented times.
of Nth Dimensions. She is also the co- status with the ACGME; 28 programs are The ACGME has suspended several
founder/chief executive officer of Beyond on continued accreditation, 23 on initial accreditation-related activities to allow for
the Exam Room, where she has developed accreditation, 4 on initial accreditation the prioritization of patient care, including
a comprehensive, continuing medical with warning, 1 had accreditation self-study activities, accreditation site
education (CME)-accredited business withdrawn, and 6 closed.8 visits, CLER program site visits, and
of medicine, career development, resident, fellow and faculty surveys.12
leadership, and financial curriculum for 5. Faculty Protected Time Additionally, the telemedicine
young physicians at the undergraduate In the 2019 July revised common supervision requirements that were
and graduate medical education levels. program requirements, the stipulation scheduled to go in to effect in July of 2020
regarding core faculty protected time was were fast tracked to help the medical
4. Single Accreditation System
removed. The subsequent outcry from the community respond to the pandemic.13
The single accreditation system will emergency medicine9 and family medicine The ACGME president and CEO noted
conclude its 5-year transition this year. communities inspired the ACGME to in March that 3 areas of priority include
After the completion of the transition, create a task force dedicated to this issue. maintenance of duty hour requirements,
all GME programs in the United States The task force recommended adequate resources and training related to
will be accredited by the ACGME.8 This including language that protects COVID-19, and adequate supervision for
brought unique changes to the GME core faculty non-clinical time which residents and fellows.13
landscape, including a single match prompted the emergency medicine review This is a constantly evolving situation;
through the National Resident Matching committee to add language to this effect.10 please check the ACGME’s Newsroom
Program (NRMP).8 The open comment period for the online for the latest updates. ¬
The COVID-19 pandemic has changed how OCTOBER 26-29•2020
D A L L A S • T E X A S
we live, we connect...and how we learn.
Right now, we are fully committed to holding REGISTRATION OPENING JULY 1
ACEP20 in Dallas October 26-29.
But we know that might not be an option for all, so we also plan to offer
a virtual event to allow anyone to participate remotely. This is a dynamic
situation, no matter what happens you will be covered by our worry-free
registration guarantee.
We know you look forward to the networking, education, and fun that
comes along with ACEP’s annual meeting. We will do everything we can D A L L A S
to ensure the safety of our attendees, presenters, vendors and staff while
following the recommendations of our communities’ health officials.
For updates, sign up for our ACEP20 interest list at
We are excited to share with you a freshly re-designed event experience
that will meet you where you are - whether in Dallas for the live event
Start Planning,
Book Your acep.org/acep20
or remotely for a virtual connection. ACEP20 will deliver the world class
Hotel Now!
faculty, education and innovation you have come to expect from the Book only through onPeak,
world’s largest gathering for emergency medicine. our official hotel provider,
to secure your room.
EMR_0620_MC94_0520 Approved for AMA PRA Category 1 Credit ™
References available online June/July 2020 | EM Resident 7
TOXICOLOGY
ITSY BITSY
SPIDER, BIG
TIME DANGER
Systemic
Ioxoscelism
Michael Simpson, MD to as brown recluses and black widows, basements and attics. Outside, they can
EMRA Toxicology Committee Chair-elect though there are other relevant species be commonly found underneath rocks
Vanderbilt University Medical Center within each genus. In this article, we and the bark of dead trees. They have
Monisha Veerapaneni will cover Loxosceles specifically, but 6 eyes arranged in dyads, while most
Burrell College of Osteopathic Medicine
would encourage readers to familiarize other spiders have 8, and the markings
Class of 2023
@monieeehearts themselves with Lactrodectus as well. on their torso are said to resemble a
A
The Elusive Recluse violin or fiddle, though the markings
20-year-old woman presents to
are less reliable and have led to the
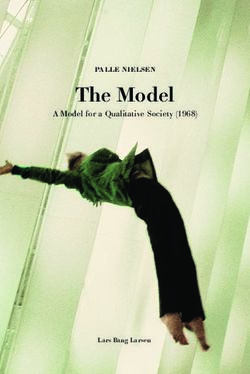
the emergency department with Loxosceles spiders are found in
misidentification of harmless spiders in
a painful ulcer to her proximal certain endemic areas in North and South
non-endemic areas as brown recluses.
thigh that she says has grown in size and America, especially the South, Southeast,
While definitive epidemiological
become necrotic over the last 3 days. She and Southwest United States (Figure 1).
data is lacking due to the difficulty in
also reports fever, malaise, and dark Location in an endemic area is a
confirming a bite, retrospective data of
urine for the past day. She has been strong predictor of a spider belonging to
359 patients over 11 years from Brazil,
helping her parents renovate their old the Loxosceles genus, as these spiders
where Loxosceles envenomation is
house in the countryside and believes she are rare outside of these described
a significant public health concern,4
may have been bitten by a spider. regions.2,3 These spiders are nocturnal
demonstrates bites in children and adults
hunters who are not aggressive but
“Is this a spider bite?” will bite if threatened, typically found up to 59 years of age, with males and
The ED chief complaint of “spider females equally represented, and the
inside homes in dark, quiet areas such as
bite” is a common one, and as most most common sites of injuries being the
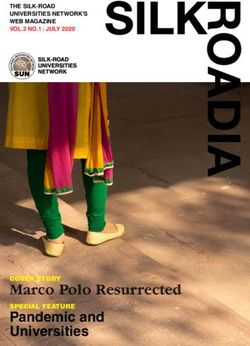
residents will realize, the majority (as FIGURE 2. Brown Recluse Bite thigh and the trunk.5 A similar study from
high as 84% in one study) of these will Chile demonstrated that 73.6% of bites
have a final diagnosis of a skin and soft occurred during the summer months of
tissue infection like abscess or cellulitis.1 the year.6
Even in actual cases of spider bites, Local Toxicity
the spider will rarely be available for The stereotypical cutaneous lesion
definitive identification, so the treating in Loxosceles bites is characterized by
physician must be aware at least of the central necrosis, a middle ring of blanched
clinical presentation of the two most skin, and an outer ring of surrounding
common venomous spiders in North erythema. This pattern is known as the
America: those of the genus Loxosceles “red, white, and blue” lesion and is highly
and Lactrodectus, frequently referred PHOTO BY MICHAEL SIMPSON suggestive of envenomation. The likely
8 EMRA | emra.org • emresident.orgpathophysiology for this necrosis involves As mentioned previously, appropriate Systemic Illness
the cytotoxic effects of sphingomyelinase identification of an offending spider In addition to localized necrosis, some
D found in Loxosceles venom.7 is unlikely to be of much use to ED patients will develop systemic effects of
Over the 14 days following the bite physicians treating patients with possible Loxosceles envenomation, collectively
(Figure 2), an eschar will develop over the spider bites. Because the differential for a referred to as “loxoscelism.” The most
site and then slough off spontaneously. necrotic wound is large and the diagnosis well-described elements of loxoscelism
The rate of healing past these first 2 weeks is often a clinical one, dermatologists and include fever and chills, nausea and
often depends on the location and size of entomologists have published a memory vomiting, arthralgias, intravascular
the wound, but most patients recover from aid for when to consider a diagnosis other hemolysis with hemoglobinuria,
the cutaneous effects of envenomation and than brown recluse spider bite (BRSB): rhabdomyolysis, disseminated
do not progress to systemic toxicity. NOT RECLUSE (Table 1).8 intravascular coagulation (DIC) and
TABLE 1. BSRB — NOT RECLUSE acute kidney injury.9 Sphingomyelinase
Numerous If multiple lesions, consider bites by blood-feeding arthropods D has also been implicated in systemic
loxoscelism, damaging the erythrocyte
Occurrence If occurs outside, consider fungal infection or insect bite
cell membrane and recruiting
Timing Loxosceles bite very unlikely in October and March inflammatory mediators leading to a
Red center If red center, consider cellulitis or insect bite systemic inflammatory reaction.10
Elevated If raised > 1 cm, consider abscess or cellulitis Again due to the difficulty of
Chronic If persists > 3 months, consider skin cancer confirming cases of BRSB, the true
Large If > 10 cm, consider pyoderma gangrenosum rate of loxoscelism is unknown; while
it appears to be rare in North America,
Ulcerates If ulcerates in < 7 days, consider pyoderma gangrenosum
the condition is potentially life-
Swelling If causes swelling below the neck, consider abscess or cellulitis threatening and can affect otherwise
Exudate If wound is weeping, consider abscess or purulent cellulitis healthy individuals,7 so it must be on
FIGURE 1. Brown Recluse Habitats
deserta
apachea
arizonica reclusa
blanda
devia
REPRODUCED WITH PERMISSION OF RICK VETTER
June/July 2020 | EM Resident 9TOXICOLOGY
the differential when appropriate. In concerning for loxoscelism, including to the medical ICU and although she
particular there are reports of children hematuria, should be admitted to required a single transfusion of packed
developing severe systemic loxoscelism the hospital and closely monitored, red blood cells during her admission, she
prior to the appearance of the classic skin likely in the ICU.14 Severe hemolysis recovered over the next 5 days and was
findings.11,12 While there are lab tests that should be transfused as necessary, discharged home with wound care for
can differentiate Loxosceles bites from and coagulopathy/DIC may need her necrotic ulcer. ¬
the necrotic wounds of several other to be reversed in the setting of life-
spider species, these tests are not readily threatening bleeding. Those experiencing
available to most ED physicians.13 Instead
TAKE-HOME POINTS
rhabdomyolysis, hemoglobinuria, or
the best way to diagnose loxoscelism is acute kidney injury require intravenous ü The diagnosis of BRSB is a clinical
to be aware of and monitor for the feared fluid hydration.5 Antivenom is currently one, as spider identification is
systemic complications themselves. not available in the United States, so often not possible and definitive
ED physicians should turn their treatment is aimed at supportive care of lab testing is not widely available.
attention initially toward the airway, the complications as they arrive. ü BRSB are extremely uncommon
breathing, circulation, and mental
status of the patient. Once any needed
Case Conclusion outside of endemic areas.
resuscitation is complete and the In the setting of a necrotic lesion ü Using the NOT RECLUSE
patient is determined to be at risk for concerning for BRSB, the ED team mnemonic, consider a broad
loxoscelism, relevant labs include serum identified the dark urine as concerning differential diagnosis.
creatinine, hemoglobin/hematocrit, for hemoglobinuria from loxoscelism. ü Systemic loxoscelism is rare
platelets, Coombs test, prothrombin Urinalysis was positive for blood, but deadly – screen suspected
time and partial thromboplastin time, confirming suspicion for hemoglobinuria patients for hemolysis, rhabdo
D-dimer, fibrinogen, and creatine kinase, and intravascular hemolysis. The myolysis, and acute kidney injury.
with additional testing dictated by the patient’s hematocrit was 35%, platelets
ü As antivenom is unavailable in
patient’s presentation. Urinalysis is also were 163,000/mcL, her Coombs test
the United States, treatment
indicated, as hematuria is an ominous was positive, and her creatine kinase,
for systemic loxoscelism is ICU
predictor of intravascular hemolysis. PT, PTT, D dimer, and fibrinogen were
Patients with diagnostic testing within normal limits. She was admitted
admission and supportive care.
Because
motorcycles
will never
have
seatbelts. You’re there for them, we’re here for you.
AC EP AN D EM R A’ S O FFI C I AL O N LI N E C AR EER C EN T E R
POWERED BY HEALTH ECAREERS
10 EMRA | emra.org • emresident.orgMENTAL HEALTH
DENIAL
OF DEATH
The Phenomenon
of Tumor Neglect
Rebecca Kreston, MD, MSPH Little research is available on this diagnosis and its potential financial
University of Illinois-Chicago phenomenon, with only a few isolated burden may also be contributing factors.
@thebodyhorrors case studies. The incidence is unknown. Patients seek to maintain control and
Payal Patel, MD Cancers that appear to be most commonly independence as their deteriorating
University of Illinois-Chicago
associated with tumor neglect include health threatens the status quo.3 Those
Shana Ross, DO, MS
those that are visible to the patient, larger suffering from tumor neglect do not see
Assistant Professor,
Department of Emergency Medicine than 1 cm, and especially malignancies their behavior as a form of denial and
Assistant Director, EM Residency Program of the skin and breast, though cases of can feel suspicious of and threatened
University of Illinois-Chicago testicular and some solid organ cancers by the perceived interference of family
@ShanaElisha have been reported. It is estimated that a and medical personnel who seek to
A
56-year-old male with a past third of women with symptoms of breast help. Understandably, patients with
medical history of active tobacco cancer will delay seeking professional tumor neglect can inadvertently become
use and remote intravenous care by > 3 months.1 A 2018 report details alienated by their behavior and the
heroin use presents to the ED complaining a case of a 37-year-old woman with a presence of a visible malignancy.
of a 2-month history of a rapidly growing breast lump for 4 months who Emergency physicians are uniquely
enlarging mass on his right cheek. He presented to the ED with pain at the site.2 positioned to offer support, as potentially
states the lesion began as a “small pimple” Imaging confirmed the 16 cm by 13 cm the first point of contact when a patient
and rapidly expanded. Exam reveals a fungating mass had metastasized to the seeks help. Often, the most meaningful
10 cm by 10 cm exophytic and indurated lung and liver. Shortly after admission, the impact relates less to immediate
mass protruding from the right face, patient developed spontaneous tumor lysis management than referral to a specialist.
extending from the preauricular area syndrome and died of multiorgan failure. Establish rapport, try to overcome the
and zygoma to his proximal neck with Several case studies describe patient’s distrust of physicians, and
a necrotic and purulent central region. individuals ignoring their tumors for eliminate barriers to health care when
CT imaging shows a necrotic infiltrative months or even decades, resisting the possible. Preserve the patient’s autonomy
malignant mass of the right cheek with efforts of family and friends to persuade by seeking their input on key decisions in
extensive right neck neovascularity and them to seek medical care.2 Such neglect their care, while providing an informed
adenopathy at all cervical levels. can lead to unchecked tumor growth, perspective on their condition.
Tumor neglect is a maladaptive disfigurement, metastasis, and death.2 Case Resolution
response to grossly evident cancers that Management of such advanced cases Our patient was admitted with
are disfiguring and life-threatening. The depends on several factors and often oncology and otolaryngology consults.
phenomenon, uncommon and largely requires a multidisciplinary team that Biopsies revealed HPV-negative, poorly
unstudied, involves patients ignoring may include surgeons for resection and differentiated squamous cell carcinoma
tumors in order to “cope with the reconstruction in challenging cases.1 of the face. A PET scan demonstrated
obvious, outward and clearly visible signs The reasons for this unusual significant metastases to the spine, liver,
of cancer.”1 Denial is a common coping phenomenon are multifactorial: distrust and lungs. Three weeks later, the patient
mechanism that grants individuals time of the health care system, poor medical underwent resection of the facial mass
to come to terms with stressful situations. literacy, low socioeconomic status, with modified radical neck dissection and
However, it has the potential to become psychosocial stressors, and the tendency pectoralis flap placement. Three months
pathological, particularly when one’s own to overlook the hazard of slow-growing later, he was transitioned to hospice care
health is at stake. tumors. A patient’s fear of a formal cancer and died under unclear circumstances. ¬
References available online June/July 2020 | EM Resident 11CRITICAL CARE
Atypical Hemolytic Uremic
Syndrome
Peter Brooks, DO gluconate, 1 amp sodium bicarbonate, dialysis was started, the remainder of the
Carolinas Medical Center Ultrasound Fellow 10 U insulin, 25 g D50, and nebulized laboratory studies results were:
Eastern Virginia Medical School EM Residency albuterol. The QRS immediately narrowed • BMP: Na 131, K 9.4, Cl 85, CO2 6,
Martin D. Klinkhammer, MD, MPH, FACEP on telemetry and on a subsequent ECG BUN >186, Creatinine 48.3, Glucose
Assistant Program Director
Assistant Professor, Emergency Medicine
(Figure 3) that was obtained. 117, (Anion gap 39.6)
Eastern Virginia Medical School Results of a CBC with manual • Path review of smear: Moderate
A
n 18-year-old African American differential showed a platelet count of schistocytes
female presented to the ED 75 and 2+ RBC fragments. Hemolysis • Total bilirubin 0.3; LDH 1,328;
complaining of a 3-week history labs and DIC screen were ordered. The haptoglobin < 10. PT; pTT and
of generalized fatigue, nausea, vomiting, patient’s repeat BMP was reported as fibrinogen were within normal limits
heavy vaginal bleeding, lightheadedness. hemolyzed once again. All are consistent with
Given the clinical scenario of microangiopathic hemolytic anemia.
On the day prior to arrival in the ED,
anemia with evidence of hemolysis, The patient was admitted to the
she developed progressively worsening
thrombocytopenia, and presumed medical intensive care unit, where she
dyspnea with exertion. She had been
hyperkalemia likely due to acute renal required endotracheal intubation for
to several urgent care centers and
failure, thrombotic microangiopathy was acute hypoxic respiratory failure. Four
EDs without receiving a diagnosis.
considered with differential diagnoses hours of dialysis were completed with
She denied any fever, rash, diarrhea,
including thrombotic thrombocytopenic transfusion of 2 units of packed RBCs,
or hematochezia. She denied alcohol,
purpura, hemolytic uremic syndrome, or and shortly afterwards PLEX was started.
cigarettes, or other drug use and was not
complement-mediated hemolytic uremic Discussion
taking any medications. On presentation,
syndrome. Nephrology and oncology
her VS were as follows: 98.6 T, 140 HR, Microangiopathic hemolytic
were consulted for emergent dialysis
22 RR, 180/90 mmHg BP, 96% oxygen anemia (MAHA) is a condition defined
and plasma exchange therapy (PLEX).
saturation on room air. The patient by microvascular hemolysis with
A bedside istat was drawn showing a
appeared tired with pale conjunctiva. anemia and schistocyte formation.
potassium of 7.5 and immeasurable
There was no rash or evidence of active Thrombotic microangiopathy (TMA)
creatinine. Telemetry showed recurrence
bleeding. Pelvic exam showed minimal is a condition characterized by MAHA
of QRS widening requiring additional
blood at the cervical os, and rectal exam and thrombocytopenia due to platelet
treatment for hyperkalemia, with
showed normal brown stool in the rectal activation and consumption. End-organ
improvement. The decision was made
vault, which was hemoccult negative. damage is caused by microvascular
to place an emergent UDALL catheter
Initial lab work demonstrated WBC thrombi and occlusion leading to tissue
to initiate dialysis and PLEX. After
23.6, Hb 5.1, HCT 14.9. The platelet count ischemia.1,2
was indeterminate due to clumping. All The major types of TMA are shiga
other labs were marked as hemolyzed. toxin-mediated hemolytic uremic
Two units pRBCs were ordered for critical syndrome (ST-HUS, also known as classic
anemia. A bedside echo showed no HUS), complement-mediated TMA (also
pericardial effusion, no right heart strain, known as atypical HUS or aHUS), and
and normal ejection fraction. A FAST thrombotic thrombocytopenic purpura
exam was negative for intraperitoneal (TTP). TMA is a hematologic emergency
fluid. A chest x-ray was obtained requiring prompt diagnosis and treatment.
(Figure 1) with a radiology interpretation It should be suspected in any patient
reporting, “Cardiomegaly with bilateral with evidence of hemolytic anemia and
basilar opacities concerning bilateral thrombocytopenia. The initial treatment
pneumonia vs pulmonary hemorrhage.” of TMA includes supportive care,
An ECG was obtained (Figure 2) corticosteroids, and antibody removal
showing a wide-complex rhythm with with plasma exchange or plasmapheresis.
peaked T-waves. While awaiting BMP FIGURE 1. A Chest X-ray Demonstrated Treatment should be started before
results, the patient was empirically Cardiomegaly and Bilateral Basilar definitive diagnosis is made, which can
treated for hyperkalemia with 3 g calcium Opacities take several days.
12 EMRA | emra.org • emresident.orgAIRWAY
Comparing TTP, ST-HUS, with PLEX should not be delayed, as 50% TTP, patients with complement-mediated
complement-mediated TMA of deaths from TTP occur in the first 24 TMA are more likely to have severe renal
TTP is caused by decreased activity hours.2 In cases where access to PLEX is dysfunction and pulmonary involvement
of ADAMTS13, most commonly due delayed, FFP can be started, as it contains (eg, pulmonary hemorrhage) and are less
to inhibitory autoantibodies against ADAMTS13, but PLEX has been shown likely to have severe neurological changes.
ADAMTS13. ADAMTS13 is a protease to improve survival over FFP infusion Prognosis of complement-mediated
that cleaves von Willebrand Factor alone.4 An ADAMTS13 level should be TMA is highly variable depending on
(vWF) from large multimers to shorter drawn before the initiation of PLEX or which complement regulatory protein is
molecules. Normally, endothelial FFP to avoid a false-negative result. mutated.6 Eculizumab is a monoclonal
cells produce long chains of vWF, and ST-HUS is caused by shiga antibody used in the treatment for
ADAMTS13 binds to cleavage points and toxin, commonly produced by complement-mediated TMA. Eculizumab
cleaves the long molecules into shorter enterohemorrhagic Escherichia coli binds to the complement protein C5 and
fragments. Without ADAMTS13, large (EHEC) (usually O157:H7) and is prevents conversion into C5a and C5b,
chains of vWF accumulate in arterioles associated with diarrhea. It is diagnosed ultimately preventing the production
and capillaries, subsequently causing by the identification of the shiga toxin
of membrane attack complex (MAC)
platelets to clump onto vWF, leading to or EHEC in the stool. Treatment with
and protecting RBCs from intravascular
microangiopathic occlusion causing end- antibiotics may worsen the disease, and
hemolysis.7,8
organ damage.3 TTP is most commonly ST-HUS usually resolves with supportive
care such as fluid resuscitation and blood Conclusion
seen in young women. The classic pentad
transfusion.5 In the ICU, our patient underwent
of TTP (found in only 5% of patients)
Complement-mediated TMA is an daily hemodialysis and PLEX with clinical
is fever, microangiopathic hemolytic
anemia, thrombocytopenia, renal failure, autoimmune-mediated HUS caused by and biochemical improvement and was
and neurologic symptoms (FAT RN). The complement dysregulation. The diagnosis extubated on hospital day 3. Workup
hallmark of TTP is TMA with a severely is suspected in any patient with TMA with revealed an ADAMTS13 antibody activity
reduced ADAMTS13 level ofTOXICOLOGY
Feeling Nervous?
Recognition and Management
of Nerve Agent Exposure
Garrett Cavaliere, DO
University of Maryland Medical Center
Emergency Medicine Residency
Gregory Jasani, MD
University of Maryland Medical Center
Emergency Medicine Residency
Reem AlFalasi, MBChB
University of Maryland Medical Center
Emergency Medicine Residency
A
patient presents to your urban
emergency department via EMS
with shortness of breath, copious
secretions, nausea, vomiting, and stool
incontinence. His symptoms began
abruptly at a concert and progressively
worsened. During transport, he develops
signs of increased work of breathing,
coarse lung sounds, and hypoxia. You
then receive a box call from the concert
Incident Command regarding multiple
casualties en route to your facility with
similar symptoms. What do you do next?
Who do you call, what procedures need
to be initiated? (GD), and cyclosarin (GF). They have agents.2 They add a sulfur group to the
the designation “G” because they organophosphates thereby making these
Introduction were initially synthesized by German agents less volatile as well as more fat/
Nerve agents are one of the most scientists in the early 20th century.2 oil soluble. They act through direct skin
terrifying weapons of war. With many contact and persist in the environment
Originally, tabun was designed as an
direct pathophysiologic effects, the for up to several weeks due to their
organophosphate pesticide. However,
psychological terror they instill is often hydrophobic nature. The most notable
its utility as a weapon was quickly
the intent of their use.1 Often tasteless
realized and the additional agents were example is VX which is highly toxic and
and colorless, they can be dispersed over
developed. These agents are all liquids can cause death within a few minutes to
a wide area to inflict as many casualties
at room temperature but can easily be hours.2
as possible. Although banned from use in
conventional war, there have increased
aerosolized by either a dispersal device Pathophysiology
concerns that terrorist organizations or or by an explosive blast. They are all Nerve agents are very similar
other non-governmental organizations soluble in both fat and water, meaning to organophosphates; they bind to
may seek to use these weapons anyways.1 they can readily be absorbed through and inhibit acetylcholinesterase.
While the United States has fortunately the eyes, skin, and respiratory tract. This produces a toxic accumulation
never seen a nerve agent attack on its soil, They are all considered non-persistent of acetylcholine at the peripheral
the possibility remains high. Emergency compounds meaning that they evaporate muscarinic, nicotinic receptors as well
medicine providers must be able to quickly.2 as the CNS synapses. Additionally, nerve
recognize and treat victims of nerve agent The second generation of nerve agents appear to activate the NMDA
attacks. agents with the designation “V” are much receptors in the brain and inhibit GABA
The 4 most common nerve agents more stable and potent compared to the transmission.3
are tabun (GA), sarin (GB), soman “G” agents and are considered persistent Overstimulation of muscarinic
14 EMRA | emra.org • emresident.orgreceptors causes miosis, hypersecretion, SLUDGE: Salivation, Lacrimation, an event has been identified. All
bronchoconstriction, vomiting, diarrhea, Urination, Defecation, GI upset, Emesis emergency notifications to staff and
urinary and fecal incontinence, and In addition to atropine, providers local government agencies should be
bradycardia. Over-activating nicotinic should also administer Pralidoxime made. This includes the state health
receptors in the skin cause sweating, and Chloride (2-PAM chloride). department to begin mobilizing
in skeletal muscle, they cause weakness 2-PAM works by reactivating the resources.7
and flaccid paralysis.3 At CNS cholinergic acetylcholinesterase by scavenging the The specific level of personal
receptors, nerve agents produce fatigue, phosphoryl group and attaching it to protective equipment (PPE) is dictated
lethargy, amnesia, ataxia, seizures, coma, the functional hydroxyl group of the by the type of release and air vapor
and respiratory depression.3 acetylcholinesterase.4,5 Delays in the concentrations. At a minimum level,
Symptoms administration of 2-PAM can render it coveralls, gloves, steel toe, shank boots
ineffective because of the aging of the [chemical-resistant], should be used
The clinical presentation of patients
agent cholinesterase complex. if no air involvement.8 It is unrealistic
exposed to nerve agents depends on
to expect ED staff to be trained for
the route and duration of exposure. TABLE 2. Dosing of 2-PAM for
higher levels of PPE; however, the
Exposure to lower concentrations of Cholinergic Toxicity
decontamination group should at
vapor leads to relatively mild symptoms
Route Dose minimum be operating in level B PPE
such as miosis, ocular pain and
IV 30 mg/kg (typically 1-2 g), (SCBA. Chemical-resistant gloves
rhinorrhea followed by gastrointestinal
over 15-30 min. Followed by [double-layered], clothing, steel-toe,
and respiratory symptoms with extended
4-8 mg/kg/hr IV infusion and boots) if operating within the
durations of exposure.3
OR hot or warm zone.8 Specific federal
Exposure to high concentrations 500 mg/h infusion decontamination teams are able to
of vapor induces convulsions, flaccid
IM Mild Symptoms: 600 mg x3 be mobilized; however, for the initial
paralysis, loss of consciousness, and
every 15 minutes incident response, decontamination
ultimately respiratory failure. The
Severe Symptoms: 600 mg will fall on the local institution and
severity is due to nerve agent vapor being
in rapid succession not to local emergency response resources.
easily absorbed in the respiratory tract. It
exceed 1800 mg total initial Personal provider safety is
is so potent that it exerts its effects within
dose. paramount! You cannot treat others if
seconds of exposure.3
For persistent symptoms you become a casualty!
Treatment repeat the series of three
Conclusion
Initial therapy should focus on injections 1 hr after the last
injection Nerve agent attacks have the
removing the patient’s clothes and
potential to quickly inflict a high
decontamination to avoid further
The only class of antiepileptics number of casualties. As emergency
skin absorption followed by assessing
effective in the management of medicine providers, we will be some
the patient’s airway, breathing, and
seizures induced by nerve agents are of the first providers to treat victims of
circulation. The priority MUST be
benzodiazepines. The management of such an attack. Our ability to recognize
decontamination.7
status epilepticus due to nerve agent and properly treat these patients is
Atropine remains the cornerstone of
exposure requires higher doses of paramount to mitigating the damage
cholinergic toxicity treatment since its
anti-epileptic agents than conventional from such an event. Of course, providers
mechanism of action works as an
seizure therapy. Animal studies that must always be mindful to protect
acetylcholine receptor antagonist. The
have been extrapolated to humans themselves first and foremost. ¬
dose of atropine is based on the severity
of symptoms. 4,5 estimate that doses as high as 30-40 mg
of diazepam may be required to break TAKE-HOME POINTS
TABLE 1. Dosing of Atropine for
seizures due to nerve agent exposure.1
Cholinergic Toxicity ü Symptoms: Salivation,
Provider Considerations
Symptoms Dose lacrimation, urination,
Your safety and the safety of
1 Mild 0.8 mg IM defecation, GI upset, emesis
the ED must be the No. 1 priority
Definite SLUDGE 2 mg IM q1hr during any nerve agent attack. Proper ü Treatment: Decontamination,
1 or more Mild
decontamination and disaster planning Atropine and 2-PAM Chloride
1 mild symptom with
at a hospital-level must be performed on
no effect in 30 min ü Personal safety and
a regular basis to ensure preparedness
Be aware that you may have to utilize for such an event.7 decontamination are the most
2-3 times this dose in severe poisoning The ED (and hospital) should important considerations for
situations (4-6 mg) titrated to decrease in be immediately locked down with nerve agent attacks.
symptoms.5 controlled entry and exit once
References available online June/July 2020 | EM Resident 15WILDERNESS MEDICINE
Winter Is Still Coming!
Reviewing
Accidental
Hypothermia
Brendan A. Mulcahy, DO, PHP, PA include the extremes of age, who have a Respiratory status may become
Chief Resident, Emergency Medicine weakened ability to thermoregulate. tenuous as the initial tachypnea settles
Allegheny General Hospital and eventually leads to respiratory
Clinical Manifestations
S
ince the dawn of time, biological depression as core temperature continues
Cold exposure can lead to an
life has been affected by the to drop. Pulmonary edema and aspiration
incredibly variable clinical presentation.
extremes of temperature. pneumonia are common findings in the
As the body temperature begins to
Militarily, wars have been won and profoundly hypothermic patient.
decrease — breathing, circulation, and
lost due to the devastation brought on Prehospital Management
level of consciousness are affected.
by hypothermia. Hannibal lost nearly Below 95°F, patients will begin to The prehospital management of a
half his men in the Second Punic have decreased cognitive function and suspected hypothermic patient can be
War. Napoleon’s army was crippled difficulty with fine motor dexterity. broken down to careful movement, basic
in the harsh winter of Russia in 1812. Hypertension and tachycardia quickly and advanced life support, passive and
Arguably the greatest American progress to cardiac instability with active rewarming, and transportation to
generation suffered through the associated hypotension, bradycardia, an appropriate center. There is a concept
infamous European winters of WWII. and ultimately dysrhythmia. EKG known as Rescue Collapse, which refers
Unfortunately, accidental hypothermia findings can consist of bradycardia, to the cardiac instability that is caused
remains a substantial cause of death in QRS widening, prolonged PR and QT by the sheer movement of a patient
our developed nation with nearly 1500 intervals, as well as the classic Osborn suffering from severe hypothermia. Even
people dying yearly. In 1999, a Swedish wave. basic movements can cause ventricular
physician suffered from one of the lowest disturbance leading to fatal arrhythmia.
FIGURE 1. Osborn Wave
recorded hypothermia cases, with a core
Emergency Department
temperature of 13.7°C after 9 hours of
Management
resuscitation — including initiating of
Determining an accurate core body
ECMO.
temperature can often be difficult but
Pathophysiology remains paramount in the management
Accidental hypothermia refers to of the hypothermic patient. An
an involuntary drop in the body’s core esophageal probe is a preferred method
temperature below 35°C (95°F). As the in your intubated patients. This is closely
body cools with cold exposure, there is followed by the bladder probe. If unable
a natural response to maintain a normal to obtain an esophageal or bladder
core temperature, with involuntary temperature, then rectal temperature
shivering and active movement. The becomes the ideal method. Modified
ability to regulate temperature and advanced life support should be initiated
respond appropriately is multifactorial as soon as possible, with the first and
depending on age, exposure, health, foremost focus remaining on rewarming
nutrition, medications, and intoxicating the patient. Pharmacologic interventions,
substances. In the urban setting, the such as epinephrine and other vasoactive
majority of patients presenting with agents, can be arrhythmogenic while
accidental hypothermia are the homeless having little to no effect, and thus should
and alcoholics. Other at-risk populations generally be avoided. Most arrhythmias
16 EMRA | emra.org • emresident.orgconvert spontaneously into normal until the temperature is above 30°C. potassium greater than 12 mmol
sinus rhythm during rewarming. Transvenous pacing is considered per liter (10 mmol per liter in some
Defibrillation can be attempted if hazardous for hypothermia-induced institutions) may be used as a hard stop
necessary but is typically unsuccessful bradydysrhythmias. for whether or not CPR may provide
until the core temperature is above 28- Serum potassium levels have been benefit. There is no consensus on how
30°C. If defibrillation is unsuccessful, a controversial marker of non-survival. hyperkalemia is best treated in levels
then further attempts should be delayed Research has suggested that serum less than 12mmol per liter in the non-
cardiac arrest patient.
TABLE 1. Staging and Management of Accidental Hypothermia Disposition
Typical Core The disposition of the patient
Stage Clinical Symptoms Temperature Treatment is highly variable depending on the
HT I Conscious, shivering 32 – 35°C Warm environment and clothing, degree of hypothermia and response to
warm sweet drinks, and active
therapies administered. Patients who
movement (if possible)
are classified as mild to moderate may
HT II Impaired consciousness, 28 –You can also read