Putting oneself in the other person's shoes: Effects of guided parent-child observations on
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Putting oneself in the other person’s shoes:
Effects of guided parent-child observations on
Theory of Mind abilities in adults
Masterarbeit
zur Erlangung des Mastergrades, MSc.
an der Naturwissenschaftlichen Fakultät
der Paris-Lodron Universität Salzburg
Eingereicht von
JASMIN DIETL, BSc.
01521433
Gutachter: Mag. Dr. BA. Beate Priewasser,
O. Univ.-Prof. Dr. Josef Perner
Fachbereich: Psychologie
Salzburg, Juni, 2020PUTTING ONESELF IN THE OTHER PERSON´S SHOES 1
Abstract
The present study investigates whether a guided parent-child observation training
enhances Theory of Mind abilities in adults. Thirty-two future psychologists participated in
the study and their ToM skills were evaluated at the beginning and the end of one semester.
All participants were trained in the CARE-Index interaction-analysis technique and the
experimental group additionally received a slightly modified version of the prevention
program B.A.S.E Babywatching (Brisch, 2007) validated for children. The participants
showed a significant improvement in their Theory of Mind abilities after completion of the
parent-child observation trainings. Findings indicate the possibility of such trainings to
improve Theory of Mind skills in adulthood, which in turn provides promising indications for
the future training of people in the social field (e.g. psychologists).
Number of words: 121
Keywords: Theory of Mind, empathy, Babywatching, mental states, parent-
child observation training
Abstrakt
In der vorliegenden Studie sollte untersucht werden, ob es möglich ist, die Theory of
Mind Fähigkeiten von Erwachsenen durch angeleitete Eltern-Kind-Beobachtungstrainings zu
verbessern. An der Studie nahmen 32 angehende Psychologen/Innen teil und wurden zu
Beginn und am Ende eines Semesters evaluiert. Alle Versuchspersonen wurden in der CARE-
Index-Interaktionsanalyse Technik geschult und eine Gruppe erhielt zusätzlich eine leicht
modifizierte Version des bereits validierten Präventionsprogramms B.A.S.E. Babywatching
(Brisch, 2007) für Kinder. Die Versuchspersonen zeigten eine signifikante Verbesserung in
ihren Theory of Mind Fähigkeiten nach Abschluss der Eltern-Kind Beobachtungstrainings.
Die Ergebnisse deuten darauf hin, dass es möglich ist, die Theory of Mind Fähigkeiten bei
Erwachsenen durch Eltern-Kind Interaktionstrainings zu verbessern, was wiederum
vielversprechende Ansatzpunkte für die zukünftige Gestaltung der Ausbildung von Personen
im sozialen Bereich (z.B. Psychologen) liefert.
Anzahl der Wörter: 124
Keywords: Theory of Mind, Empathie, Babywatching, mentale Zustände,
Eltern-Kind BeobachtungstrainingPUTTING ONESELF IN THE OTHER PERSON´S SHOES 2
For our daily social interaction it is crucial that we can put ourselves in the other
person's shoes and understand how they think and feel. In this matter our social perception of
situations plays an important role. In social situations we perceive a variety of information
(e.g. facial expressions, gestures), which are then processed by our brain. In the social
neurosciences, two routes are postulated that can be used to understand others (Kanske,
Böckler & Singer, 2015a). The affective route (empathy, empathizing) describes how we
directly share the affect of another person. This sharing can be triggered by observation or
imagination of another person’s emotional state. It involves the knowledge that the source of
one’s own affective state is the state of the observed person. The cognitive route (Theory of
Mind, mentalizing) describes the understanding of mental states of others like their thoughts
and goals. For this purpose the person infers beliefs, thoughts and emotions of others.
Contextual factors influence which route (cognitive or affective) we take to understand others
and to what extent we engage in empathy or Theory of Mind (ToM). Stietz, Jauk, Krach &
Kanske (2019) were able to show that empathy and perspective taking indeed employ
different neural circuits. Both interact and facilitate in complex situations because both routes
are addressed (Stietz et al., 2019).
Empathy can be divided into cognitive and affective empathy. In the literature ToM is
often equated with cognitive empathy. The separation of the two constructs is difficult both
theoretically and practically. Nevertheless, it can be said that empathy refers more to affective
understanding and ToM describes cognitive understanding for which one does not need to be
emotionally involved oneself (Engelen & Röttger-Rössler, 2012). The importance of empathy
and ToM often only becomes apparent when people are limited in these competencies, e.g. by
an autism spectrum disorder (e.g. Baron-Cohen & Wheelright, 2004). Both skills are key
components of interpersonal relationships and are necessary to understand and empathize
with others. These skills allow us to build and maintain relationships and also support pro-
social behavior (Berkhout & Malouff, 2016). Furthermore these are essential competences in
health and social professions. In this context, a focused and differentiated perception is crucial
for the interaction with patients. ToM and empathy are needed to recognize and understand
the motivation, thoughts and feelings of clients and are important competencies of
psychologists and therapists (Schuster, 2015). ToM is important to ensure a trusting
relationship between psychologist and patient, which is the basis for the therapeutic process
and progress (Kaufer et al., 2015). Above-average skills in empathy and ToM are found in
psychologists and psychotherapists (Schuster, 2015; Hassenstab et al, 2007) and are
associated with a positive therapeutic outcome (Berkhout & Malouff, 2016). Especially sincePUTTING ONESELF IN THE OTHER PERSON´S SHOES 3
interactions are usually very variable and unforeseeable, a flexible use of ToM is important.
Professionals need to be able to observe social situations very precisely in order to put
themselves into the situations of the patients and the patients per se. Machado, Beutler and
Greenberg (1999) examined the influence of professional experience and the awareness of
one's own emotions on the ability to recognize the emotional states of others. In their study,
psychotherapists, compared to psychology students, were better at interpreting verbal cues.
This illustrates the importance of above-average skills in social perception, empathy and
ToM. Since these are core qualifications for social professions, it would be beneficial to be
able to intensify them through training. In this master thesis the main focus is on ToM, for a
more detailed focus on empathy see Freismuth (2020). A training that focuses on both,
observation techniques as well as ToM skills, could be an effective training program for
social professions and will be the central question of this study. Therefore the question arises
whether a specific training can enhance the ToM ability of psychology students.
There are already various training studies, which examined the improvement of ToM
skills in different individuals. In various mental illnesses e.g. schizophrenia, the illness causes
deficiencies in the social and emotional domains of everyday life. Many studies have
therefore investigated whether social cognition (especially ToM or empathy) can be improved
through specific trainings. For example, Turner-Brown, Perry, Dichter, Bodfish & Penn
(2008) showed that an adapted social cognition and interaction training significantly
improved ToM skills in high functioning autism adults and even found a trend towards
improved social communication skills. The training mainly focused on emotion training and
figuring out social situations. The same training was also used in schizophrenic patients and
also showed an improvement in ToM ability and emotional perception (Voutilainen, Kouhia,
Roberts & Oksanen, 2016). Golan and Baron-Cohen (2006) evaluated the effectiveness of the
training program "Mind Reading" in adult subjects with Asperger syndrome or high-
functioning autism. With the help of an interactive guide participants learned about emotions
and mental states through video and voice recordings over a period of 10 weeks. Compared to
people in the control group who received no training, the participants of the training group
improved their performance in recognizing complex emotions and mental states in faces and
voices (Golan & Baron-Cohen, 2006).
Another group of healthy participants that was investigated are children and
adolescents. A meta-analysis by Hofmann et al. (2016) revealed that various ToM training
programs for children effectively improve ToM abilities and that these effects can be
considered moderately strong. There is also evidence (Devine & Hughes, 2013; Grazzani &PUTTING ONESELF IN THE OTHER PERSON´S SHOES 4
Ornaghi, 2012) that ToM skills continue to develop in middle childhood and early
adolescence. A training study by Goldstein and Winner (2012) showed, that ToM skills in
RMET task increased in children as well as adolescents after receiving weekly acting and
role-playing training lessons, compared to the control group who received art lessons.
Furthermore Goldstein, Wu and Winner (2009) observed that adolescents who had received
drama-play training achieved significantly higher values in ToM assessed by RMET and
MASC. This leads to the conclusion that ToM can also be improved in young adulthood and
for that purpose trainings, which only indirectly train ToM (e.g. acting trainings) can be used.
Another important focus in training programs is the improvement of ToM skills
among older people. Reiter, Kanske, Eppinger and Li (2017) were able to show that ToM and
metacognition were worse in older people than younger, whereas abilities like empathy and
compassion were less affected by age. Lecce, Bottiroli, Bianco, Rosi and Cavallini (2015)
conducted a training study with subjects aged 58-85 with three training groups: ToM
conservation training, which included guided conversations about mental states, physical
conversation training, which focused on physical inferences, and social contact training,
which included conversations about aging. Only in the ToM training group their ToM
abilities increased significantly. Cavallini et al. (2015) and Rosi, Cavallini, Bottiroli, Bianco
and Lecce (2015) continued the study with older subjects. Again, subjects showed improved
ToM performance in the strange stories task (Happé, 1994) as well as improved transfer
performance at the animation task (Castelli et al., 2000). They showed better mentalizing
descriptions and less observational descriptions in the animation task. The researchers
concluded that they became more aware of mental states through training and suggested a
high plasticity of ToM even a long time after childhood.
But there only a few studies of training programs in healthy adults and non for social
profession so far. One study was conducted by Kanske, Trautwein, Böckler and Singer
(2015b), in which the adult subjects received either a training for socio-cognitive abilities
(perspective), socio-affective abilities (affective) or mindfulness-based attentioning
(presence). In the three-month perspective taking training they learned to identify and classify
their own mental states. In a novel fMRI task they measured compassion, empathy and ToM
and investigated training effects on both, behavioral and neuronal levels. The more they
improved their understanding of their mental states in the perspective modul, the higher their
ToM skills, measured by EmpaToM, became. This was also replicated by Böckler, Herrmann,
Trautwein and Holmes (2017) and Valk et al. (2017). The better the test persons were able to
put themselves in the mind of their counterpart in the EmpaToM (ToM condition), thePUTTING ONESELF IN THE OTHER PERSON´S SHOES 5
stronger the neural network, associated with ToM was activated (increased neural plasticity
and thickness; Valk et al., 2017). This illustrates the plasticity of ToM abilities that can be
found not only behaviorally but also neuronally. Preckel, Kanske and Singer (2018) explained
the improvement of ToM by postulating that the distinction between self and others is
important for the greater use of ToM. The only other study, which examined ToM training in
healthy adults, is the study by Schröder (2013). She showed that four weeks of ToM training
in adults improved automaticity and flexibility in the use of ToM (i.e. use of more mental
explanations) in the FASC task (Hayward, Homer & Sprung, 2016).
In summary, it can be stated that most studies have shown that ToM can be improved
by training in different groups of people. Nevertheless, there are no studies on the
effectiveness of ToM training in professional fields (e.g. social) where a particularly
pronounced ability for the job is required. In addition it is often criticized that the trainings are
too unspecific or very complex and not precisely defined (in terms of what was exactly
trained). Therefore, there is a strong appeal for specific and uniform training content. In the
existing training studies a realistic implementation of the training is also missing, as they are
very abstract and trained in a laboratory context. A program which is close to everyday life
(e.g. watching parent child interaction) and uses a specific, recurring questioning technique to
train affective and cognitive empathy skills already exists: the prevention program B.A.S.E. ®
- Babywatching training program for children by Karl Heinz Brisch (2007). It stands for
Babywatching (B) against Aggression and Anxiety (A) and for sensitivity (S) and empathy
(E). In the original setting a mother/father visits a preschool group or school class every week
with her/his baby for about half an hour. Children observe the interaction between parent and
child and are part of the babies’ development. The B.A.S.E. group leader acts as a facilitator
and through a special questioning technique, the children are encouraged to be mindful and
learn to put themselves in the shoes of mother and baby and empathize with them (Brisch,
Hollerbach & Quehenberger, 2016). There are already promising studies on the effects of
Babywatching in children. The studies investigated in a pre-post design the differences
between an experimental group (receiving one school year of Babywatching) and a control
group (treatment as usual) in terms of empathy (e.g. with the GEM) and behavioral changes
(e.g. with CBCL, SET, SEVV) collected from the children, parents and teachers. In a
longitudinal study it was shown that B.A.S.E Babywatching improved affective and cognitive
empathy, better speech production (singular – plural formations) as well as a decrease in
anxiety and aggression (Brisch et al., 2016). There is also some evidence from school children
such as the study by Haneder (2011). She was able to show that empathy, sensitivity, socialPUTTING ONESELF IN THE OTHER PERSON´S SHOES 6
skills and prosocial behavior improved in children in an Austrian primary school and that they
showed less fear and aggression. Another Babywatching study in a primary and junior school
likewise revealed that Babywatching promotes positive prosocial skills and reduces conduct
and emotional problems (Lionetti, Snelling & Pluess, 2017). Brisch, Hollerbach, Kellie-
Smith, Perry and Driessen (2014) described the observed improvements and experiences with
Babywatching: increased capacity to empathize, transferring this capacity to everyday
situations, increase in calmness, concentration and readiness to request and accept help from
adults, development of a realistic view of demands and joys of parenting; concluding that
there are positive effects for both home and institution.
The special feature of this program is the questioning technique with which the group
leader guides the children through the interaction every week. There are five levels of
questions. Questions on levels 1 to 3 invite children to explore behavior, motivation and
emotions of the dyad. With these questions the children learn to perceive precisely (fine
signals through facial expressions and gestures), to reflect on them and to describe behavior in
detail. In doing so, the goals/intentions of behavior and emotional states of others are
explored. In levels 4 and 5 they are prompted to explore their own emotional world by
imagining what one would do or how one would feel in the other person's shoes. Thereby
perspective taking and emphatic sensitivity are addressed quite explicitly. The questions are
intended to encourage empathy, sensitivity and the adoption of perspectives and to facilitate
the recognition of emotions and reactions. Besides the unique questioning technique, another
feature is the exceptional setting. The whole process is a live observation and through the
group you receive immediate observations from the other participants, which could differ
from your own. In this way it can be experienced that one's own point of view and feelings
can be different from those of others.
Due to these special characteristics of baby observation, the goal of this study was to
adapt, apply and evaluate B.A.S.E. Babywatching for adults. Empathy and ToM are strongly
promoted through this training, which is close to everyday life (observing parent-child
interactions) and can be easily implemented. Therefore we asked ourselves whether this
parent-child observation training could intensify the empathy and ToM ability in psychology
students. We conducted a study with psychology students (master’s degree) to evaluate if the
empathy and ToM skills in psychology students could be improved in general through
trainings with regular parent-child observations and especially with an adapted version of
Babywatching. All students participated in the lecture ‘Interaction and Attachment’, in which
they learned an interaction analysis technique. In addition, some subjects participated also inPUTTING ONESELF IN THE OTHER PERSON´S SHOES 7
the practical exercise 'Observation of Parent-Child Dyads', in which they received weekly
Babywatching. In both techniques the ToM ability is addressed by the need to put oneself in
the position of a particular dyad and to assess different emotional states and intentions
through close observation of behavior. The students were assessed in their empathy and ToM
skills both at the beginning of the semester (T1) and at the end of the semester (T2) with the
SPF (Paulus, 2009), RMET (Baron-Cohen, Wheelright, Hill, Raste & Plumb, 2001) and
EmpaToM task (Kanske, Böckler, Trautwein & Singer, 2015b) to identify possible
improvements through the trainings. The experimental group (EG) learned the very precise
observation technique (B.A.S.E. ® Babywatching) in addition to the evaluation technique
(CARE Index; Crittenden, 2005). The control group (CG), on the other hand, was only trained
in interaction evaluation and in the recognition of important indicators for assessment (CARE
Index). Based on the presented research it is presumed, that the described parent-child
observation trainings (Babywatching and CARE Index) can contribute to the strengthening of
ToM by repeatedly addressing them through watching and reflecting over parent child
interactions and therefore will increase these abilities in both groups. We anticipated that the
EG should show more increase in their ToM abilities in RMET and EmpaToM task from the
beginning (T1) to the end of the semester (T2) compared to the improvement of the control
group (CG). In the EG empathy and ToM are being addressed more by training the ability to
observe and identify with the dyad, the EG learns to empathize and understand reasons for
action. Finding positive results would support the use of parent child observation trainings as
ToM trainings and extend the application of baby observation trainings to adults and social
professions e.g. psychologists. Furthermore the explicit findings of B.A.S.E. ® Babywatching
would contribute to the possible use of this prevention program in adults. This could have an
important impact for the education of psychologists and psychotherapists, and perhaps even
an outlook for parent-child interaction trainings in educational settings.
Method
Participants
Thirty-three master psychology students of the University of Salzburg participated in
our study, one subject in the EG (n = 1) dropped out of the study after T1 and was therefore
excluded from the analysis. Leaving a sample of 32 psychology students (M = 25.34 years;
SD = 6.63; 30 female) with an age range from 21 to 57 years with German (25) or Austrian
nationality (7). The experimental group consisted of 15 subjects (M = 26.67 years; SD = 9.22)PUTTING ONESELF IN THE OTHER PERSON´S SHOES 8
with an age range from 21 to 57 years and the control group of 17 subjects (M = 24.18; SD =
2.77) with an age range from 21 to 31 years. All test persons filled out a written informed
consent and received 20 € expense allowance after T2.
An a priori power analysis was performed to determine the necessary sample size. The
power analysis was conducted using G*Power 3.1 to test the improvement of ToM skills from
T1 and T2 and the interaction between test time and group. As a reference for the power
analysis, the medium effect size (f = .211; Ellis, 2010) for experimental and control group
comparison for social cognitive training from the meta-analysis (Butters, 2010) was used.
Results showed that a total sample of 62 participants (each group n = 31) would be required to
achieve a power of .90. We are aware that the present study did not meet the required sample
size.
Study Design
In our study both, the experimental as well as the control group attended a standard
lecture on ‘Interaction and Attachment’ (four block appointments). The experimental group
additionally received an interaction observation training (based on B.A.S.E Babywatching)
over a period of eight weeks (twelve appointments) which was embedded in the practice
lecture ‘Observation of Parent-Child Dyads’. Both groups were tested at the beginning (T1)
and at the end of the semester (T2) with the SPF, the RMET and the EmpaToM to measure
empathy and ToM. Resulting in a mixed study design with between-subject (group
differences regarding enhancement in empathy and ToM) and within-subject (improvements
from T1 to T2 regarding empathy and ToM) factors.
Procedure
With the start of the lecture ‘Interaction and Attachment’, the test subjects received a
short introduction to the CARE Index and were then given three videos to rate the interaction
quality of parent and child (VR1). The first testing phase (T1) at the beginning of the semester
took place in the children's laboratory of the University of Salzburg. After a consent form was
explained and signed, the examination began with a computerized questionnaire (for a
segment of the questionnaire see appendix A). First of all, sociodemographic data such as age,
nationality, etc. were asked. Then the Saarbrücker personality questionnaire (SPF), the
Reading the Mind in the Eyes Test (RMET) and the Scales for Experiencing Emotions (SEE ;
Behr & Becker, 2004) questionnaire were answered. The SEE is not relevant for this thesis
(see Kosztolanyi, 2020). Afterwards the EmpaToM task was launched, which lasted about 30
minutes including instructions, hearing test, a practice task and the test task. During thePUTTING ONESELF IN THE OTHER PERSON´S SHOES 9
semester the participation of the Adult Attachment Projective by George, West and Pettem
(1999; AAP) took place (TX), which is also not relevant (see Pross, 2020). At testing phase 2
(T2) in addition to the repeated implementation of SPF, RMET and EmpaToM (different
stimulus set) subjective assessments of the effects of parent-child interactions and the lectures
were collected (see appendix B). At about the same time the video rating (VR2) was repeated
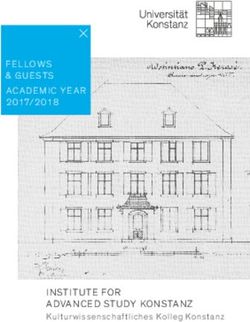
with the same three videos as at the beginning. For a systematic illustration of the study´s
procedure see Figure 1.
Figure 1. Systematic illustration of study procedure. SPF, Saarbrücker personality questionnaire; RMET, Reading
the Mind in the Eyes test; SEE, Scales for Experiencing Emotions; AAP, Adult Attachment Projective
Training Module Babywatching. For the exercise lecture four mothers and their
babies were recruited via our website, Facebook or the mailing list of the University of
Salzburg. Each session started with a short meditation or mindfulness exercise in the group to
create a calm atmosphere. Then a mother with her baby came into the group and spent about
30 minutes in the middle of the group circle. The mothers were instructed to interact as usual,
e.g., playing, feeding or sleeping. The group leader asked questions according to the B.A.S.E.
questioning technique, starting on the behavioral level with questions like what is the mother
doing right now, how does the baby react to it or how does the mother/baby feel right now.
This was followed by questions why mother or baby behaved in a certain way inviting
participants to think about reasons and justify their thoughts. Questions relate solely to
observations of the interacting dyad. In a next step questions are asked about one's own
identification with the behavior (e.g. What would you do if you were in Mom's shoes?) and
feelings (e.g. How would you feel if you were in the baby's place?). The group leader adjusted
questions each week individually and spontaneously to the observations and ideas of thePUTTING ONESELF IN THE OTHER PERSON´S SHOES 10
group. After observing the dyad, in the last 20 minutes of the lecture, students reflected on
their observations and their thoughts and feelings related to it, first in written form and then
discussed them in the group.
Training Module CARE Index. The CARE Index (Crittenden, 2005) is a tool to
evaluate the quality of adult-infant interactions in a dyadic context. All participants got to
know the procedure in the course of the lecture and learned how to apply it by watching and
evaluating many practical video examples. The students had to code interactions videos on
seven aspects of the adult and the infant with 14 points each. Furthermore, the behavior
patterns of the mother (sensitive, controlling and unresponsive) and the child (cooperative,
compulsive, passive and difficult) can be classified. The behavior is evaluated separately for
child and adult and then scores are summed for the relationship quality. The total score could
range from 0-14, with 0 being dangerously insensitive, 7 being average sensitive and 14 being
above average sensitive (Crittenden, 2005).
Measurements
Adult Attachment Projective (AAP). The AAP by George, West and Pettem (1999)
is a projective method for identifying the attachment representation of adults. The AAP took
about 30 minutes and was individually administered over the semester (TX)
Scales for Experiencing Emotions (SEE). The SEE by Behr and Becker (2004) is a
questionnaire with 42 items for assessing how people perceive, evaluate and deal with their
own emotions. The test takes about 10-15 minutes and was presented at T1.
Video rating (VR). At the beginning and the end of the semester, students rated three
parent-child interactions videos according to the guidelines of the Infancy CARE Index
(Crittenden, 2005; for video rating sheet see appendix C). The same three interactions were
rated at T1 and T2 and lasted about 45 minutes.
Saarbrücker personality questionnaire (SPF). The SPF from Paulus (2009) is the
German version of the interpersonal reactivity index (Davis, 1983) and a self-report
questionnaire with 16 items for measuring empathy. On a 5-level likert scale (never - rarely -
sometimes - often - always) the extent to which a statement applies to the individual is
assessed. Four dimensions are recorded: Perspective taking, Fantasy, Empathic concern,
Personal distress. The completion of the questionnaire took about 15 minutes and was
presented in the same version at both T1 and T2.PUTTING ONESELF IN THE OTHER PERSON´S SHOES 11
Reading the Mind in the Eyes Test (RMET). The Reading the Mind in the Eyes
Test: Revised Version by Baron-Cohen et al. (2001) was used in the German version (Bölte,
2005). It is a research tool for measuring cognitive empathy (described as ToM) using 36
items. The test person sees a black and white photograph of an eye area (balanced male and
female eyes). The expression of the eyes should be used to identify what the person is
thinking or feeling. One of four complex emotions (e.g. disappointed) must be assigned to the
eye expression. The descriptions of emotions do not contain basic emotions but rather
complex mental states. In RMET the total score is the number of correctly answered items.
The questionnaire takes about 15 minutes to complete and was submitted in the same version
at both T1 and T2.
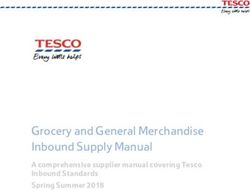
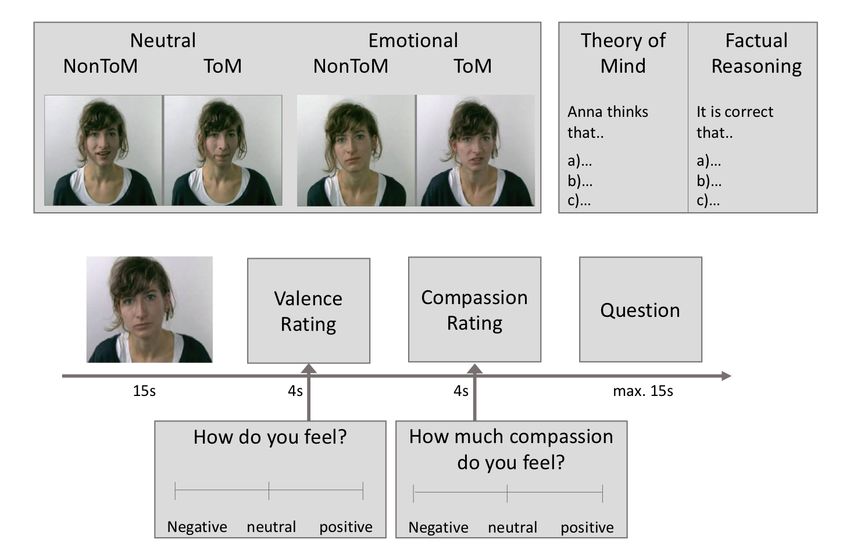
EmpaToM. With the EmpaToM (Kanske et al., 2015b) it is possible to measures
empathy, compassion and ToM in the same person. The task consists of 48 video trials (each
approx. 15 s) of actors telling autobiographic episodes. For systematic illustration of trial
sequence see Figure 2. An episode had either a high emotional (negative) or low emotional
(neutral) content and demanded ToM or NonToM capacities. After each video the participants
had to rate how they are feeling (empathic response) ranging from very negative to very
positive (-3 to +3). Then they should also estimate how much compassion they feel for the
current person and situation (from none to very much, 1-7). Afterwards a question about the
content of the video was presented, in which one of three answers had to be chosen within 14
seconds. For the answer either perspective taking (ToM) or factual reasoning had to be
applied. For example questions see Appendix D. The EmpaToM task was presented via
presentation software (Neurobehavioral Systems, Berkeley, USA) and performed on both T1
and T2, using different sets of video stimuli.
Figure 2. Trial sequences EmpaToM (adapted from Kankse et al., 2015).PUTTING ONESELF IN THE OTHER PERSON´S SHOES 12
Results
In this thesis the main focus of the analysis is on ToM (RMET and EmpaToM). For a
more detailed analysis of empathy see Freismuth (2020).
EmpaToM
The data were processed using MATLAB_R2019b (MathWorks Inc., Natick, USA).
The accuracy in ToM questions describes the average percentage of correctly solved ToM
questions, whereby it is rated as incorrect if either the wrong answer option was selected or no
answer was selected within the 14 seconds. The data was not normally distributed according
to Shapiro-Wilk test, p> .05. The Mann-Whitney U test showed no statistical difference
between the two groups at T1 (U = 126,50, Z = -.038, p = .970, r = .007) or T2 (U = 106.00, Z
= -.82, p = .413, r = .15), meaning the groups did not differ in the amount of correctly
answered questions at T1 (Md_EG = 79.17; Md_CG = 79.16) or T2 (Md_EG = 79.17;
Md_CG = 83.33). In contrast, the Wilcoxon signed-rank test showed a significant
improvement in EG from T1 to T2 (Z = -1.96, p = .05, r = .51) in correctly answered ToM
questions and a marginally significant improvement in CG (Z = -1.85, p = .064, r = .45). For
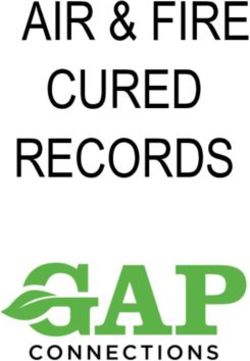
descriptive overview of the improvements in accuracy from T1 to T2 see Figure 3. Here one
can see that both groups solved more percent of the ToM questions at T2 correctly.
Figure 3. Mean percentage of accuracy in EmpaToM task for both test times subdivided into EG and CG. The
error bars represent the 95 % CI.
The reaction time reflects the speed at which the ToM questions are answered,
whereby it only refers to correctly answered questions. The Shapiro-Wilk test showed a
normal distribution (p > .05) of the reaction time data, therefore a mixed ANOVA wasPUTTING ONESELF IN THE OTHER PERSON´S SHOES 13
calculated. There was no statistically significant interaction between test time and group
(F(1, 30) = 1.22, p = .278, partial η² = .04) as well as no significant main effect for test time
(F(1, 30) = 2.86, p = .101, partial η² = .09) or group (F(1, 30) = 0.22, p = .645,
partial η² = .01). Looking at the data descriptively one can see a slight decrease in reaction
times. The EG decreased from 8.18 seconds (95% CI [7.56;8.80] to 8.02 seconds (95% CI
[7.43;8.62]) and the CG from 8.34 seconds (95% CI [7.93;8.75] to 7.60 seconds (95% CI
[7.16;8.08]).
The ToM performance is calculated by the response time and accuracy in ToM
questions, the values were z-transformed and combined to a mean value according to Kanske,
Böckler, Trautwein, Lesemann & Singer (2016). ToM performance was not approximately
normally distributed according to the Shapiro-Wilk test, p > .05. Neither the Wilcoxon
signed-rank test showed a significant improvement from T1 to T2 of the groups (EG: Z = -
.23, p = .820, r = .06; CG: Z = -.21, p = .831, r = .05) nor did the Mann-Whitney U test show
a significant group difference at T1 (U = 127.00, Z = -.02, p = .985, r = .00) or T2 (U =
119.00, Z = -.32, p = .748, r = .06) in their ToM performance.
RMET
One point can be scored for each item, so that a maximum score of 36 can be
achieved.
As RMET was normally distributed for both groups, as assessed by the Shapiro-Wilk
test (p > .05), we performed a mixed ANOVA. There was no statistically significant
interaction between test time and group, F(1, 30) = 0.004, p = .951, partial η² = .00. But there
was a significant main effect for test time F(1, 30) = 7.10, p = .012, partial η² = .19, meaning
they identified more correct mental states in the eyes at T2 than T1. For the descriptive mean
value distribution from T1 to T2 sorted by groups, see Figure 4. The main effect for the group
was not statistically significant F(1, 30) = 0.02, p = .894, partial η² = .00. The groups did not
differ in their RMET total scores neither on T1 (M_EG = 27.07; M_CG = 27.18) nor T2
(M_EG = 28.13; M_CG = 28.29).PUTTING ONESELF IN THE OTHER PERSON´S SHOES 14
Figure 4. Mean values of RMET total score for both test times subdivided into EG and CG. The error bars
represent the 95 % CI.
The correlations between RMET and EmpaToM (n = 32) are not significant, except
the correlation between RMET at T2 and reaction time as (rs = .48, p = .005) well as ToM
performance at T1 (rs = .454, p = .009) for all correlations see Table 1.
Table 1
Correlation between RMET task and EmpaToM task
Measure M SD 1 2 3 4 5 6 7
1.RMET_T1 27.13 3.08 -
2.RMET_T2 28.22 2.96 .74** -
3.Acc_ToM_T1 76.56 8.18 .15 .26 -
4.Acc_ToM_T2 81.51 8.33 .05 .01 .34 -
5.RT_ToM_T1 8.26 1.08 .27 .48** .09 -.21 -
6.RT_ToM_T2 7.80 1.12 -.02 -.16 -.13 -.25 -.03 -
7.Perf_ToM_T1 .00 .73 .27 .45** .77** .12 .66** -.11 -
8.Perf_ToM_T2 .00 .64 .09 -.08 .04 .55** -.16 .59** -.05
Note. Spearman correlation, n = 32, two tailed significance niveau, * p < .05, ** p < .01.
Discussion
The aim of the study was to investigate the possible improvement of ToM skills in
psychology students through the implied lectures to train parent-child interaction observation
competencies. For this purpose we examined two groups of future psychologists regarding
their ToM enhancement from T1 to T2 using the EmpaToM Task and RMET. The wholePUTTING ONESELF IN THE OTHER PERSON´S SHOES 15
group was taught how to observe and evaluate interactions using the CARE index, while the
experimental group additionally received a specific parent-child observation training based on
B.A.S.E Babywatching.
Our study showed a clear improvement in ToM ability through the training techniques
applied in both groups. Both groups showed better ToM abilities in the RMET after the
training (Figure 4). This is specifically interesting as the psychology students in our study
already achieved high scores in the baseline measure; e.g., even higher than in the study by
Kaufer et al. (2015), who also investigated German psychology and medicine students. In
addition, the mean values of our subjects were generally higher than those found in a study by
Hassenstab et al. (2007), who examined psychotherapists using the RMET. This indicates that
RMET performance can be improved even at high baseline levels, and that it can differentiate
training effects accurately.
In the EmpaToM Task, a significant increase from T1 to T2 in the EG regarding the
percentage of correctly answered ToM questions was found (Figure 3). In the CG the increase
was only marginally significant. The reaction time in answering the ToM questions showed
no improvement in speed between the test times. However, both groups descriptively showed
a slightly faster reaction time. The combination of reaction time and accuracy calculated
according to Kanske et al. (2016) also showed no significant differences in test time. Thus our
results are not in line with other training studies using the EmpaToM, who had found
significant increases in both variables and stated their practicability to assess ToM
enhancement (e.g. Böckler et al., 2014; Kanske et al., 2015b). The non-significant results in
ToM performance in our study are probably due to the lack of a significant increase of
reaction time, since performance is composed of accurcay and reaction time. However,
reaction time may not be considered as so important in this study. It is unclear how relevant a
significant speedup within the given 14 seconds really is for the evaluation of the
effectiveness of ToM trainings. Schröder (2013) also found in her study that the speed in a
ToM task did not differ significantly between the groups and only decreased slightly. This is
in line with our results and can also be interpreted as a simple training effect of the EmpaToM
tasks and might not reflect the improvement in ToM. However, the fact that the results of
EmpaToM and RMET do not show a clear correlation (see Table 1) could be additionally
problematic in terms of the interpretation of the EmpaToM task. It might be an indication that
the two tasks do not measure the same abilities in terms of ToM. RMET is already a very
commonly used research tool for measuring ToM skills in adults (e.g. Bölte & Pforte, 2007;
Kaufer et al., 2015) and measured trainings effects well, so that it can be assumed that the taskPUTTING ONESELF IN THE OTHER PERSON´S SHOES 16
reliably measures ToM abilities. The EmpaToM, on the other hand, is a relatively new
research tool for measuring ToM. According to Böckler, Kanske, Trautwein and Singer
(2014) the EmpaToM allows differentiated training effects to be measured. But the task was
originally designed as an fMRI task and was mainly used in brain imaging studies. We used
the task only as a behavioral measurement. So it may require further evaluation of this task
before it can be reliably used at the behavioral level as a measurement tool for ToM. Another
difference between these two tasks is the way how the given information is processed. The
EmpaToM task enables the simultaneous processing of verbal and non-verbal information,
however, the verbal information is more in the spotlight. RMET requires non-verbal
information (eye expression) processing. Both training techniques (CARE Index and baby
observation) mainly focus on identifying nonverbal cues between parent and child, which
would explain the stronger results in RMET in both groups. RMET measures ToM
capabilities more passively and EmpaToM more actively. Mar, Oatley, Hirsch, dela Paz and
Peterson (2006) also found a passive effect for ToM, i.e., people who read novels are
significantly better at empathizing with others (ToM skills tested with RMET), just as people
who mainly read non-fiction.
Concerning our hypothesis that ToM capabilities should improve significantly more in
the EG compared to CG, as they were trained not only in evaluation but also in a deeper
observation technique, our current results cannot confirm this. There was no apparent
difference between the two groups regarding the increase of ToM in any dimension, neither in
the EmpaToM task nor in the RMET. In this context the differences and similarities between
our two interaction trainings should be addressed to explain this result. It could be criticized
that the trainings both train perspective taking (ToM) and were too similar to highlight group
differences. In order to assess if both interaction analysis techniques could be considered as
trainings we compared them to Marshall's guidelines for an effective training. Marshall
(1995) postulates that a training should teach the following aspects to be effective: (1) skills
to recognize non-verbal signals; (2) skills to recognize subtle body language and facial
expressions; (3) skills to decipher the emotional states of others. If you compare these
suggestions with the concept of baby observation and CARE-Index, you will notice that both
concepts fulfill these demands. The main difference one can immediately see in the intention
of the techniques: The goal of baby observation is precise perception and the goal of the
CARE Index is evaluation. For example with the CARE Index you ask yourself how the child
experiences the behavior of the mother, whereas with baby observation you ask yourself how
would you feel as a baby if the mother did this or that. The CARE Index is a scientificallyPUTTING ONESELF IN THE OTHER PERSON´S SHOES 17 validated video-based screening tool, microanalysing the quality of an infant-adult relationship for risk assessment and counseling (Svanberg et al., 2010). Its proposed that the CARE Index can be used in a psychotherapeutic context with parents. In this case, inner representations can be read by analyzing facial expressions or tone of voice (Letourneau & Tryphonopoulos, 2012). This suggests that the CARE Index technique also could have contributed to better ToM performance insofar, as it also included training of analyzing facial expressions and/or pitch and then attributing mental states in our tasks. In baby observation, the focus was not on evaluating the interaction but on experiencing and reflecting on feelings while observing the interaction on its different levels. Furthermore, it was about the self- reflection of the group members, which plays a special role in baby watching (Haneder, 2011). It is not about finding the one correct solution for assessing the interaction, but about the fine observation of the unique interaction between a mother/father and child. Another important difference between the two methods is that CARE Index is video-based, i.e. the video is analyzed in detail several times and can be repeatedly played back. Baby observation, on the other hand, takes place live, so you have to learn to observe quickly in order to catch as much as possible. One could argue that a direct observation of parent-child interactions like baby observation is more important for everyday life. Live observations better reflect real processes and are more consistent and tangible (Aspland & Gardner, 2003). McDaniel and Bugs (2012) suggested that a large variation of different aspects during training leads to a greater transfer of ToM abilities in everyday life. When a person is invited to reflect on personal experiences, the task becomes more meaningful for the participants, which makes a transfer into everyday life easier (Cavallini et al., 2015). This point was definitely met in the EG is supported by the subjective assessment of what the test subjects were able to absorb through baby watching for themselves. The expected stronger improvement of EG compared to CG may have been less evident due to the fact that the 12 units of Babywatching were not sufficient enough. In the original setting, children receive about one year of this training (Haneder, 2011). Despite the differences, both training methods helped the participants to better put themselves in the position of others, regardless of whether they evaluate the dyad (CARE-Index) or not (baby observation). Based on participants subjective assessment, the EG stated a deeper engagement with the teaching concepts than the CG, which was marginally significant. Secondly, participants in the EG subjectively ascribed themselves a higher improvement of their skills in analyzing parent-child interactions than the CG. Indeed, a positive correlation between the performance in RMET at T2 and the subjective evaluation of improvement was evident in the EG. Thirdly, participants of the EG stated that they dealt
PUTTING ONESELF IN THE OTHER PERSON´S SHOES 18
more with their personal attachment experience. Babywatching activates the own attachment
system by perceiving the interaction and own emotional reactions with the dyad. Crooks et al.
(2019) postulated that attachment plays a central role in Babywatching, which could explain
these results. Altogether, these points suggest that there is a greater growth of expertise in the
EG through baby observation due to a higher personal engagement.
It should be noted that our study had some methodological limitations. Our sample
consisted mostly of female individuals (n = 30). The gender distribution is far from evenly
balanced, which means that general assumptions for the adult population should be made with
caution. However, according to American Psychology Association (2016) findings, women
are still overrepresented in psychology (about 75%). A population with this proportion should
therefore be representative, this should be taken into account in the follow-up of the study.
Another limitation of the validity of our study is the quasi-experimental design. There
was no random assignment to experimental and control group. The composition of the sample
should also be reconsidered. In our study, all master psychology students attended the lecture
‘Interaction and Attachment’, which leads one to conclude that self-selective processes played
a role in that all subjects had a general interest in parent-child interactions and attachment. As
we had no other control group this limits the generalizability to other psychological
specializations. Hall, Davis and Connelly (2000) for example showed that female practicing
psychologists (e.g. psychotherapists) differed from academic psychologists (e.g. scientists) in
their ability of perspective taking and empathy. In follow-up studies control groups with
master's degree students with other specializations as well as master's degree students from
other academic fields should be included. This could be used to check whether ToM can also
be improved through parent-child observation training in other groups of people and to
investigate the effect of baby observation in more detail.
An important point regarding the explanatory power of our results is the very small
sample size. The power analysis revealed that we would have needed 62 participants (each
group consisting of 31). Our study may have produced false-negative results because the
groups are not large enough to sufficiently produce significant mean differences. Hackshaw
(2008) postulates that a small sample leads to large standard errors, making the 95%
confidence intervals large, resulting in an imprecise estimate of the effect and no firm
conclusion. As a conclusion, the results of our study should be classified as preliminary and
further research is required to make generalizable claims. A randomized design with a larger
sample as well as additional control groups would be needed in order to be able to draw better
conclusions regarding the effectiveness of our guided parent-child observation trainings.PUTTING ONESELF IN THE OTHER PERSON´S SHOES 19
Nevertheless we could prove some evidence for effects. Two special features of our
study should be highlighted: firstly, the initial implementation of parent-child interactions as
part of a ToM training. Secondly the first-time application of B.A.S.E. ® Babywatching for
healthy adults. Thirdly, the successful attempt to improve ToM in social professions that
already exhibit high ToM skills (Schuster, 2015).
Highly developed ToM abilities are of importance for social interactions, especially in
social and health professions (Kaufer et al., 2015). Hildebrandt, McCall & Singer (2018) even
point out that emotion regulation strategies (e.g. reappraisal, acceptance, etc.) can be
increased through training of perspective taking. These abilities play an important role for
maintaining a good patient-therapists relationship and therefore influence the outcome of a
therapy (Rogers, 1957; Rogers, 1959). The evaluation of interactions can also be an important
part of a psychologist's work e.g. parent-child interactions in a clinical context. For this
purpose it is essential to recognize nuances of communication between parent and child. But
not only in the professional context but also in the personal context an improvement of ToM
and therewith also the analyzing skills are of enormous advantage. In our study, almost all of
the students reported a possible transfer to their future work as well as to their personal lives.
It should be particularly highlighted that all students in the baby observation stated that they
think that they have benefited from this for their future work. So it seems to be a promising
approach to train ToM in future psychologists. This approach could be extended to other
health and social professions like social workers, pedagogues, midwives or medical staff.
With further research, it could even be achieved that parent-child observation training will be
included in the curriculum of these professions, so that they can intensify their skills and are
more prepared for their future work and ensure better outcomes of their treatment.PUTTING ONESELF IN THE OTHER PERSON´S SHOES 20
References
American Psychological Association. (2016). Summary Report, Graduate Study in
Psychology 2017: Student Demographics. Retrieved from
http://www.apa.org/education/grad/survey-data/2017-student-demographics
Aspland, H., & Gardner, F. (2003). Observational Measures of Parent-Child Interaction: An
Introductory Review. Child and Adolescent Mental Health, 8(3), 136-143.
doi.10.1111/1475-3588.00061
Baron-Cohen, S., Wheelwright, S., Hill, J., Raste, Y., & Plumb, I. (2001). The „Reading the
Mind in the Eyes“ Test Revised Version: A study with normal adults, and adults with
Asperger Syndrome or High-Functioning Autism. Journal of Child Psychology and
Psychiatry, and Allied Disciplines, 42, 241-251.
Baron-Cohen, S., & Wheelwright, S. (2004). The empathy quotient: An investigation of
adults with Asperger syndrome or high functioning autism, and normal sex
differences. Journal of Autism and Developmental Disorders, 34(2), 163-175.
Behr, M., & Becker, M. (2004). Manual: Skalen zum Erleben von Emotionen, Hogrefe:
Göttingen
Berkhout, R. T., & Malouff, J.M. (2019). The Efficacy of Empathy Training: A Meta-
Analysis of Randomized Controlled Trials. Journal of Counseling Psychology, 63(1),
32-41. doi.10.1037/cou0000093
Böckler, A., Herrmann, L., Trautwein, F.-M., Holmes, T., & Singer, T. (2017). Know thy
selves: Learning to understand oneself increases the ability to understand others.
Journal of Cognitive Enhancement, 1, 197-209. doi:10.1007/s41465-017-0023-6
Böckler, A., Kanske, P., Trautwein, F.-M., & Singer, T. (2014). The EmpaToM: A novel
fMRI-task separating affective and cognitive routes to social cognition. Poster
presented at 20th Annual Meeting of the Organization for Human Brain Mapping
(OHBM), Hamburg, Germany.
Bölte, S., & Pforte, S. (2007). Der Test „Reading Mind in the Eyes” veranschaulicht
kognitive Empathie – Die Kunst, in Gesichtern zu lesen, Special Personalführung, 4,
72-79.
Brisch, K. H. (2007). Prävention von emotionalen und Bindungsstörungen. In von
Suchodoletz (Hrsg.), Prävention von Entwicklungsstörungen (pp. 167-181). Göttingen:
Hogrefe.PUTTING ONESELF IN THE OTHER PERSON´S SHOES 21
Brisch, K. H., Hollerbach, J., Kellie-Smith, G., Perry, A., & Driessen, A. (2014). B.A.S.E. -
Babywatching in England, New Zealand and Germany: A prevention program to
counter aggression and anxiety and to promote empathy and sensitivity. Poster
presented at the World Association of Infant Mental Health Conference, Edinburgh,
England.
Brisch, K.H, Hollerbach, J., & Quehenberger, J. (2016). Impact of an attachment-based
prevention program B.A.S.E-Babywatching: A program to counter aggression and
anxiety and to promote empathy and sensivity. Poster presented at the World
Association of Infant Mental Health Conference, Prag, Czech Republic.
Butters, R. P. (2010). A Meta-Analysis of Empathy Training Programs for Client Populations.
Unpublished Dissertation, University of Utah, Salt Lake City, USA.
Castelli, F., Happe, F., Frith, U., & Frith, C. (2000). Movement and mind: a functional
imaging study of perception and interpretation of complex intentional movement
patterns. Neuroimage, 12, 314-325. doi: 10.1006/nimg.2000.0612
Cavallini, E., Bianco, F., Bottiroli, S., Rosi, A., Vecchi, T., & Lecce, S. (2015). Training for
generalization in theory of mind: a study with older adults. Frontiers in Psychology,
6(1123). doi:10.3389/fpsyg.2015.01123
Crittenden, P. M. (2005). Der CARE-Index als Hilfsmittel für Früherkennung, Intervention
und Forschung. Frühförderung interdisziplinär (early interdisciplinary intervention).
Specialissue: Bindungsorientierte Ansätze in der Praxis der Frühförderung, 24, 99-
106.
Crooks, M., Kellie-Smith, G., & Perry, A. (2019). An introduction to B.A.S.E. Babywatching
as a whole-class nurture intervention in primary schools, contributing to a therapeutic
school culture. International Journal of Nurture in Education, 5(1), 66-69.
Davis, M. (1983). Measuring individual differences in empathy: Evidence for a
multidimensional approach. Journal of Personality and Social Psychology, 44, 1114-
1126.
Devine, R.T., & Hughes, C. (2014). Relations between false belief understanding and
executive function in early childhood: A meta-analysis. Child Development, 85(5),
1777-1794. doi.10.1111/cdev.12237
Engelen, E.-M., & Röttger-Rössler, B. (2012). Current Disciplinary and Interdisciplinary
Debates on Empathy. Emotion Review, 4(1), 3-8. doi:10.1177/1754073911422287PUTTING ONESELF IN THE OTHER PERSON´S SHOES 22
Ellis, P. D. (2010). The essential guide to effect sizes: Statistical power, meta-analysis, and
the interpretation of research results. Cambridge, New York: Cambridge University
Press.
Freismuth, S. (2020). Baby, teach me empathy! Angeleitete Eltern-Kind-Beobachtungen zur
Förderung von Empathie bei angehenden Psychologen (Unpublished master thesis).
Department of Psychology, University of Salzburg, Salzburg, Austria
George, C., West, M., & Pettem, O. (1999). The Adult Attachment Projective -
disorganization of Adult Attachment at the level of representation. In J. Solomon, C.
George (Eds.), Attachment disorganization (pp. 462-507). New York: Guilford.
Golan, O., & Baron-Cohen, S. (2006). Systemizing empathy: Teaching adults with Asperger
syndrome or high-functioning autism to recognize complex emotions using interactive
multimedia. Development and Psychopathology, 18(2), 591-617.
Goldstein, T. R., & Winner, E. (2012). Enhancing empathy and theory of mind. Journal of
Cognition and Development, 13(1), 19-37. doi:10.1080/15248372.2011.573514
Goldstein, T. R., Wu, K., & Winner, E. (2010). Actors are skilled in Theory of Mind but not
empathy. Imagination, Cognition and Personality, 29, 115-133. doi.10.2190/IC.29.2.c
Grazzani, I., & Ornaghi, V. (2012). How do use and comprehension of mental-state language
relate to theory of mind in middle childhood? Cognitive Development, 27(2), 99-111.
doi.10.1016/j.cogdev.2012.03.002
Hackshaw, A. (2008). Small Studies: Strengths and Limitations. The European Respiratory
Journal, 32(5), 1141-1143. doi.10.1183/09031936.00136408
Hall, J. A., Davis, M. H., & Connelly, M. (2000). Dispositional empathy in scientist and
practitioner psychologists: Group differences and relationship to self-reported
professional effectiveness. Psychotherapy, 37(1), 45-56. doi.10.1037/h0087758
Haneder, A. (2011). B.A.S.E Babywatchig – ein Programm für Empathie und Feinfühligkeit
& gegen Angst und Aggression – Implementierung und Evaluierung an Tiroler
Volksschulen (Unpublished Diplomarbeit). Department of Psychology, University of
Innsbruck, Innsbruck, Austria
Happé, F. G. (1994). An advanced test of theory of mind: Understanding of story character’s
thoughts and feelings by able autistic, mentally handicapped, and normal children and
adults. Journal of Autism and Developmental Disorders, 24 (2), 129-154.
Hassenstab, J., Dziobek, I., Rogers, K., Wolf, O. T., & Convit, A. (2007). Knowing what
others know, feeling what others feel. A controlled study of empathy inPUTTING ONESELF IN THE OTHER PERSON´S SHOES 23
psychotherapists. The Journal of Nervous and Mental Disease, 195, 277-281.
doi.10.1097/01.nmd.0000253794.74540.2d
Hayward, E., Homer, B., & Sprung, M. (2016). Developmental Trends in Flexibility and
Automaticity of Social Cognition. Child development, 89(3), doi.10.1111/cdev.12705.
Hildebrandt, L. K., McCall, C., & Singer, T. (2019). Socioaffective versus sociocognitive
mental trainings differentially affect emotion regulation strategies. Emotion, 19(8),
1329-1342. doi.10.1037/emo0000518
Hofmann, S. G., Doan, S. N., Sprung, M., Wilson, A., Ebesutani, C., Andrews, L. A., Curtiss,
J., & Harris, P. L. (2016). Training children’s theory-of-mind: A meta-analysis of
controlled studies. Cognition, 150, 200-212. doi.10.1016/j.cognition.2016.01.006
Kanske, P., Böckler, A., & Singer, T. (2015a). Models, Mechanisms and Moderators
Dissociating Empathy and Theory of Mind. In M. Wöhr, & S. Krach (Eds.), Current
Topics in Behavioral Neurosciences - Social Behavior from Rodents to Humans:
Neural Foundations and Clinical Implications (pp. 1-14). Luxemburg: Springer.
Kanske, P., Böckler, A., Trautwein, F.-M., & Singer, T. (2015b). Dissecting the social brain:
Introducing the EmpaToM to reveal distinct neural networks and brain-behavior
relations for empathy and Theory of Mind. NeuroImage, 122, 6-19.
doi.10.1016/j.neuroimage.2015.07.082.
Kanske, P., Böckler, A., Trautwein, F.-M., Lesemann, F. H. P., & Singer, T. (2016). Are
strong empathizers better mentalizers? Evidence for independence and interaction
between the routes of social cognition. Social Cognitive and Affective Neuroscience,
11, 1383-1392. doi.10.1093/scan/nsw052
Kanske, P., Trautwein, F.-M., Böckler, A., & Singer, T. (2015). Training Compassion and
Theory of Mind separately: Differential effects on socio-affective & socio-cognitive
abilities, Poster presented at Bi-Annual Conference of the International Society for
Research on Emotion, Genf, Swiss.
Kaufer, K., Oddo, S., Kraus, M., Thiel, A., Wicker, S., & Stirn, A. (2015).
Empathiefähigkeiten (Theory of mind) bei deutschen Medizin- und
Psychologiestudierenden. Hessisches Ärzteblatt. Retrieved from
https://www.laekh.de/images/Hessisches_Aerzteblatt/2015/Studie_Empathiefaehigkeit
en_Kaufer_Oddo_et_al.pdf
Kellie-Smith, G., & Perry, A. (2016). Hello, baby!. Nursery world, 3-16, 30-31.You can also read