Parents Who Supply Sips of Alcohol in Early Adolescence: A Prospective Study of Risk Factors
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Parents Who Supply Sips of
Alcohol in Early Adolescence: A
Prospective Study of Risk Factors
Monika Wadolowski, PhD,a Delyse Hutchinson, PhD,a,b Raimondo Bruno, PhD,a,c Alexandra Aiken, BS,a Jackob
M. Najman, PhD,d Kypros Kypri, PhD,e Tim Slade, PhD,a Nyanda McBride, PhD,f Richard P. Mattick, PhDa
BACKGROUND: Parents are a major supplier of alcohol to adolescents, often initiating use with abstract
sips. Despite harms of adolescent alcohol use, research has not addressed the antecedents
of such parental supply. This study investigated the prospective associations between
familial, parental, peer, and adolescent characteristics on parental supply of sips.
METHODS: Participants were 1729 parent–child dyads recruited from Grade 7 classes,
as part of the Australian Parental Supply of Alcohol Longitudinal Study. Data are from
baseline surveys (Time 1) and 1-year follow-up (Time 2). Unadjusted and adjusted logistic
regressions tested prospective associations between Time 1 familial, parental, peer, and
adolescent characteristics and Time 2 parental supply.
RESULTS: In the fully adjusted model, parental supply was associated with increased parent-
report of peer substance use (odds ratio [OR] = 1.20, 95% confidence ratio [CI], 1.08–1.34),
increased home alcohol access (OR = 1.07, 95% CI, 1.03–1.11), and lenient alcohol-specific
rules (OR=0.88, 95% CI, 0.78–0.99).
CONCLUSIONS: Parents who perceived that their child engaged with substance-using peers
were more likely to subsequently supply sips of alcohol. Parents may believe supply of a
small quantity of alcohol will protect their child from unsupervised alcohol use with peers.
It is also possible that parental perception of peer substance use may result in parents
believing that this is a normative behavior for their child’s age group, and in turn that
supply is also normative. Further research is required to understand the impacts of such
supply, even in small quantities, on adolescent alcohol use trajectories.
aNational Drug and Alcohol Research Centre, Faculty of Medicine, University of New South Wales, Sydney, New
WHAT’S KNOWN ON THIS SUBJECT: Adolescent
South Wales 2052, Australia; dQueensland Alcohol and Drug Research and Education Centre, University of alcohol use is associated with major long-term
Queensland, Brisbane, Queensland 4072, Australia; eCentre for Clinical Epidemiology and Biostatistics, School of
Medicine and Public Health, University of Newcastle, Newcastle, New South Wales 2308, Australia; and fNational
harms. Parents are a major supplier of alcohol to
Drug Research Institute, Curtin University, Perth, Western Australia 6845, Australia bSchool of Psychology, adolescent children, often initiating their child’s
Faculty of Health, Deakin University, Burwood, Victoria, Australia cSchool of Psychology, Faculty of Health, alcohol use with sips. However, no research has
University of Tasmania, Hobart, Tasmania, Australia addressed the antecedents of such supply.
Dr Wadolowski contributed to the conceptualization and design of the study, contributed to the WHAT THIS STUDY ADDS: Parental factors (parental
design of the data collection instruments, coordinated and supervised data collection, wrote the perception of substance-using peers, home alcohol
statistical analysis plan, conducted and interpreted the statistical analyses, drafted and revised access, lenient alcohol-specific rules, and initial
the manuscript, and approved the final draft of the manuscript; Dr Hutchinson contributed to
parental supply of alcohol sips) and previous child
the conceptualization and design of the study, contributed to the design of the data collection
sipping predicted subsequent parental supply of
instruments, critically reviewed the manuscript, and approved the final draft of the manuscript;
Asst Prof Bruno contributed to the conceptualization and design of the study, coordinated and alcohol sips.
supervised data collection, assisted with analysis planning, contributed to the interpretation
of the statistical analyses, critically reviewed the manuscript, and approved the final draft of
the manuscript; Ms Aiken coordinated and supervised data collection, critically reviewed the To cite: Wadolowski M, Hutchinson D, Bruno R, et al.
manuscript, and approved the final draft of the manuscript; Prof Najman contributed to the Parents Who Supply Sips of Alcohol in Early Adolescence:
A Prospective Study of Risk Factors. Pediatrics. 2016;
137(3):e20152611
Downloaded from www.aappublications.org/news by guest on February 9, 2021
PEDIATRICS Volume 137, number 3, March 2016:e20152611 ARTICLEEarly adolescent alcohol initiation supply of sips. The lack of such from parent–child dyads. Of these
is associated with increased risk prospective research runs the risk 1896 dyads, complete data were
of: delinquent behavior1; physical that the reasons for supply provided available for 1840 adolescent and
injury2; poor adolescent health by parents are post hoc explanations 1870 parent T1 surveys, resulting in
and well-being3,4; and alcohol- and may obscure some antecedents a total of 1808 parent–child dyads
use disorders.1 Alcohol use often of supply. with complete data. Data were
commences with a sip(s)/taste(s) Our aim was to comprehensively imputed for T1 surveys in 15 cases,
of alcohol, rather than consuming investigate how parental supply of using the PRELIS application in the
whole drinks.5–7 By age 13, up to sips of alcohol to adolescent children LISREL program.26 When a case was
60% of adolescents have had a at age 14 years was prospectively missing a single item on a scale, the
sip/taste of alcohol5,8–14; sipping associated with a range of: (1) dataset was searched for the same
is more prevalent than drinking familial, parental, and adolescent pattern of responses on that specific
in this age group.5,6,10,15 Sipping demographic characteristics; (2) scale within other cases. When
is associated with increased risk parent behaviors including alcohol multiple response patterns matched
of early adolescent drinking and consumption, alcohol availability, in the dataset, a reliability estimate
binge drinking,12,16 but the area of alcohol-specific rules, and parenting was generated. Only imputations
sipping is under-researched. Despite practices; (3) peer substance use and with high reliability (0.999, ie, a
recommendations that parents avoid alcohol attitudes; and (4) individual LISREL variance ratio = 0.001)
providing alcohol to children,15 adolescent psychological behaviors. were accepted. This in turn assured
parents remain a major supplier These factors were selected based confidence in the accuracy of the
of alcohol to adolescent children, on several theoretical perspectives imputed data.27 This provided a total
including sips.17,18 Reasons for this identifying their importance in of 1823 parent–child dyads at T1. Of
early supply are particularly poorly understanding adolescent alcohol these 1823 dyads, 1752 adolescents
studied, with a recent exception,9 use, including problem behavior and 1746 parents (87.0% were
where 60% to 70% of mothers theory, socialization theory, the mothers) returned follow-up surveys
disagreed that supplying access to social development model, and social 1 year later (Time 2 [T2]), resulting
sips was beneficial. Those authors learning theory.24,25 in 1729 (94.8% of dyads with
note9 that what remains unstudied complete data at T1) T2 dyads, the
are the antecedents associated sample used in the present analyses.
with parental supply of sips. METHODS
Understanding these reasons may The sample was similar to the
inform on ways to advise parents Sample Australian population on important
about reducing alcohol access. Grade 7 adolescents and 1 parent demographic factors. Males
were recruited for the Australian comprised 55% of the adolescent
Although the characteristics Parental Supply of Alcohol sample (51% of 12- to 13-year-
predicting parental supply of alcohol Longitudinal Study, and methods olds in the Australian adolescent
are poorly documented, some are described elsewhere.15 Families population),28 and 81% of children
observers suggest parents supply came from 49 Independent (49.0%), lived in 2-parent households
sips to inoculate their children Government (38.8%), and Catholic (80.0% of 2-parent households in
against heavy drinking,19 while also (12.2%) secondary schools across 3 the Australian population),29 and
acknowledging that little is known states: New South Wales, Tasmania, socioeconomic status (SES)30 showed
about the antecedents of children and Western Australia. A total of our sample was very similar to the
sipping.6,8,20 Recent research on why 2017 families expressed interest Australian population.31 Rates of
parents provide alcohol suggests it is in the study, but 90 families were alcohol use in our sample (parents
to decrease consumption and teach ineligible, as 16 adolescents were not and adolescents) were also similar
children to resist peer pressure.9 in Grade 7 and 74 parents did not to those in Australian population
However, the limited research on sign informed consent, yielding 1927 surveys. In a school-based population
factors associated with parental eligible parent–adolescent dyads. Of survey, any lifetime alcohol use
supply has focused on parental the surveys sent, 1910 adolescents was reported by 67.3% of 12- to
attitudes, used only cross-sectional (99.1%; mean age = 12.9-years- 13-year-olds,32 compared with 67.8%
designs, or focused on supply of old, SD = 0.5), and 1913 parents of adolescents in our sample at T1
whole drinks.9,21–23 There are no (99.3%) returned baseline surveys (mean age = 12.9 years). Parents
prospective studies investigating (Time 1 [T1]), which included reported the following frequencies
what parent and adolescent written consent. Of the returned of T1 alcohol use: 2.7% daily, 48.5%
characteristics predict parental T1 surveys, 1896 (98.4%) were weekly, 39.2% less than weekly,
Downloaded from www.aappublications.org/news by guest on February 9, 2021
2 WADOLOWSKI et aland 9.6% not in the past 12 months. scoring 10% of areas.30 For the Adolescents responded to 10 items
This was similar to the Australian analyses, deciles were collapsed into on their parents’ rules about drinking
population aged >18-years-old: 7.7% 3 categories: low SES (deciles 1–3), and binge drinking frequency and
daily, 41.7% weekly, 33.0% less than medium SES (deciles 4–7), and high quantity, and whether drinking
weekly, and 7.7% not in the past SES (deciles 8–10). Parent religiosity: was permitted in supervised and
12-months.33 One item asked how important unsupervised contexts.36 Family
religion was to them (very important, conflict: Parents responded to 3
Families completed surveys either
pretty important, and not/only a items about the frequency of family
via paper hardcopy or online. To
little important). disagreements.37 Positive family
maintain privacy, all paper surveys
relations: Parents responded to
were sent individually to parents Parental Alcohol Use another 3 items regarding family
and adolescents, and each survey
Consumption was based on the relationship quality.37 Parental
included its own reply-paid envelope
Alcohol Use Disorders Identification monitoring: 6 items assessed
for returning surveys. Where
Test short-form scale, AUDIT-C: adolescent report of monitoring,
available, links to online surveys
quantity, frequency, and heavy such as whether parents knew about
were e-mailed directly to parents
episodic use.34 Seven responses their peers, plans with peers, and
and adolescents. Participants were
measured quantity, ranging from 1–2 unsupervised activities.38 Parenting
reimbursed 10 AUD for their time
drinks to 13 or more drinks. These consistency: Parents responded to
completing each survey. Paper and
options were then collapsed into 5 10 items assessing the consistency of
online surveys each had 3 reminders,
categories: 1–2 drinks to 10 or more using discipline and enforcing rules.39
including resending surveys and
drinks. Frequency of alcohol use was
telephone calls. Approval to conduct Peers
measured with 8 categories, which
this research was received by the
were collapsed into: never, less often Substance-using peers: Parents
University of New South Wales
(than monthly), monthly or less, 2–4 were asked whether they thought
Human Research Ethics Committee
times a month, 2–3 times a week, and their child’s friends: had tried
(approval number 10144), and
4 or more times a week. Frequency alcohol; drank alcohol regularly;
this study is registered at www.
of heavy episodic use (more than and drank to get drunk. Adolescents
clinicaltrials.gov (identification
four standard drinks on a single also reported peer alcohol and
number NCT02280551).
occasion) was measured with 8 tobacco use, responding to 6 items,
Variables categories, collapsed into: never, less including whether their friends
than monthly, monthly, weekly, daily smoked cigarettes, drank alcohol,
Outcome Variable: Parental Supply of a
or almost daily. These 3 items were and the frequency of drunkenness.40
Sip at T2
then summed, with higher scores Peer disapproval of substance use:
At both T1 and T2, parents were indicating increased parental alcohol Four items asked adolescents about
asked: “In the last 12-months, did use. Cronbachs α for this measure, whether their friends disapproved of
you/your partner give your child a and the other scales and variables tobacco use and alcohol use.40
sip or taste of alcohol?” The response included in the analyses, are available
option was a dichotomous yes or no. elsewhere.6 Individual Adolescent Behaviors
Alcohol use: Adapted from the
Familial Demographics Parenting Practices Australian National Drug Strategy
Household composition: Adolescents Context of parental suppy: If parents Household Survey, adolescents were
were asked whether they lived had supplied a sip, they were also asked: “In the last six months, on a
in 1- or 2-parent households asked “In the last 12 months, when day that you have an alcoholic drink,
(including step-parents). SES: you/your partner have given your how many standard drinks do you
Family geographical locations were child alcohol, how many times have usually have?” There were 7 response
categorized into deciles from a you provided it in these situations…” options, including a sip/taste of
standardized Australian population with response options being: with alcohol. At T1, 14.1% of adolescents
measure, the Index of Relative family on a holiday or special reported sipping and 5.5% reported
Socioeconomic Advantage and occasion; with family at dinner; and consuming a whole drink. At T2,
Disadvantage. The deciles were at parent-supervised parties. Home sipping increased to 25.2%, whereas
distributed between 10 equal groups, alcohol access: Parents completed 5 7.8% of adolescents reported
with the first decile representing the items about access and availability of drinking. The 7 response options were
lowest scoring 10% of Australian alcohol in the family home, such as collapsed into 3 categories: abstainer,
geographical areas, and the tenth whether they kept track of, or locked sipper (only sip[s]), and drinker (at
decile representing the highest up, alcohol.35 Alcohol-specific rules: least 1 whole drink). Externalizing
Downloaded from www.aappublications.org/news by guest on February 9, 2021
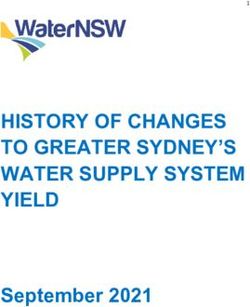
PEDIATRICS Volume 137, number 3, March 2016 3behaviors: Adolescents completed the TABLE 1 Descriptive Statistics for Time 2 Parental Supply by Time 1 Familial, Parental, Adolescent
rule-breaking and aggressive behavior and Peer Characteristics (N = 1729)
subscales from the Achenbach youth Time 1 Characteristics (Score Range) Time 2 Parental Supply Mean (SD) or %
self-report.41 Internalizing behaviors: No Supplya (n = 1279) Supplyb (n = 450)
Adolescents also completed the
Familial demographics
withdrawn-depressed and anxious- Age (years) 12.4 (0.5) 12.5 (0.6)
depressed subscales from the youth Adolescent sex, %
self-report.41 Male 75.2 24.8
Female 72.6 27.4
Data Analyses Household composition, %
Two-parent household 74.1 25.9
Planned logistic regression One-parent household 73.4 26.7
analyses first tested for unadjusted Importance of religion, %
associations between T1 variables Very important 76.4 23.6
Pretty important 76.2 23.8
and T2 parental supply of a sip. A
Not, or only a little, important 73.0 27.0
multivariate, logistic regression Socioeconomic status, %
analysis, adjusting for all T1 High 75.6 24.4
covariates (regardless of the Medium 74.3 25.7
significance of their associations with Low 67.4 32.6
Parental supply of sips of alcohol, %
T2 supply), was then conducted to
Noa 86.1 13.9
test for associations with T2 supply. Yesb 43.2 56.8
The adjusted model also controlled Parent alcohol use
for clustering at the school level and Total consumption (Score: 0–12) 3.8 (2.2) 4.3 (1.9)
tested for multicollinearity. Analyses Parenting practices
Home alcohol access(P) (Score: 6–30) 16.8 (3.7) 17.7 (3.3)
were conducted in Stata/SE 11.2,42
Alcohol-specific rules(A) (Score: 10–50) 49.6 (1.3) 48.9 (2.2)
using logistic and cluster commands. Family conflict(P) (Score: 3–6) 3.7 (0.9) 3.8 (0.9)
Positive family relations(P) (Score: 3–6) 5.9 (0.5) 5.9 (0.4)
Parental monitoring(A) (Score: 6–30) 27.8 (3.0) 27.5 (3.4)
RESULTS Parenting consistency(P) (Score 5–25) 21.4 (2.7) 21.3 (2.7)
Adolescent peers
Descriptive Analyses Peer substance use(P) (Score: 3–15) 4.3 (1.3) 5.0 (1.4)
Peer substance use(A) (Score: 6–30) 7.9 (2.6) 8.9 (3.0)
Supply was reported by 24.4% of Peer disapproval of substance use(A) (Score: 4–12) 10.9 (1.9) 10.5 (2.1)
parents (95% CI, 22.3826.43) at T2. Adolescent behaviors
Supply typically occurred in familial Adolescent alcohol use(A), %
contexts, such as holidays and Abstainerc 80.8 19.2
Sipperd 41.8 58.2
special occasions (68.0%, 95% CI,
Drinkere 56.8 43.2
63.53–72.16), family dinners (50.0%, Externalizing behaviors(A) (Score: 0–60) 5.3 (5.9) 6.2 (6.3)
95% CI, 45.38–54.62), and parties Internalizing behaviors(A) (Score: 0–40) 4.3 (5.1) 4.6 (5.5)
(10.4%, 95% CI, 7.93–13.64). Table 1 (A), Adolescent report; (P), parent report.
presents the means and proportions a Parent, and/or their partner, did not supply sips of alcohol in the past six months.
b Parent, and/or their partner, supplied sips of alcohol on at least one occasion in the past 6 months.
of T2 supply in relation to T1 familial, c Did not consume any alcohol in the past 6 months.
parental, peer, and individual d Consumed only a sip(s) of alcohol.
adolescent characteristics. e Consumed at least a whole drink in the past 6 months.
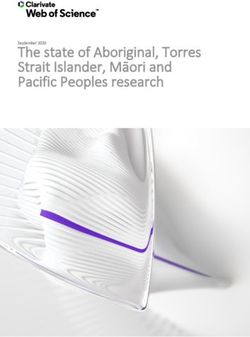
Unadjusted Analyses associated with decreased T1 reports increases, and in turn become more
Compared with no supply, T2 supply of: parental alcohol-specific rules pronounced when examining larger
was associated with increased T1 (OR = 0.73, P < .001); and perceived increases in the respective scales.
reports of: parental alcohol use (OR = peer disapproval of substance use
1.12, P < .001), home access to alcohol (OR = 0.91, P < .001). Notably, T2 supply Adjusted Analyses
(OR = 1.08, P < .001), perceived peer had no unadjusted associations with The multivariate logistic model was
substance use among both parents parenting factors such as monitoring, significant (χ2(22) = 1158.40, P < .001)
and adolescents (parent-report OR = parenting consistency, relationship (Table 2). Notably, in adjusting for all
1.37, P < .001; and adolescent-report quality, family conflict, or household familial demographic, parental, peer,
OR = 1.13, P < .001), and externalizing composition. While some of these ORs and individual adolescent factors,
problems (OR = 1.02, P = .009) (Table appear small, ORs for scales represent only a few T1 variables retained
2). Conversely, T2 supply was also differences based on single unit significant associations with T2
Downloaded from www.aappublications.org/news by guest on February 9, 2021
4 WADOLOWSKI et alsupply. Compared with no supply, TABLE 2 Unadjusted and Adjusted Associations Between Time 2 Parental Supply and Time 1 Familial,
these factors were: increased home Parental, Adolescent, and Peer Characteristics (N = 1729)
alcohol access (OR = 1.07, P < .001), Time 1 Characteristics Time 2 Parental Supply of Sips of Alcohol
the effect of which did not change from Unadjusted Adjusted
unadjusted analyses; increased parent
OR 95% CI OR 95% CI
perception that their child engaged
Familial demographics
with substance-using peers (OR =
Adolescent age 1.26* 1.05–1.52 0.98 0.82–1.17
1.20, P < .001); and decreased parental Adolescent sex
alcohol-specific rules (OR = 0.88, P = Male 1.00a — 1.00a —
.033). Adjusting for the type 1 error Female 1.14 0.92–1.42 1.25 0.97–1.62
rate (Bonferroni adjusted α = 0.05/28 Household composition
Two-parent household 1.00a — 1.00a —
= 0.0018), the association of alcohol-
One-parent household 1.04 0.79–1.37 0.92 0.69–1.23
specific rules was no longer significant, Importance of religion
but the other associations remained Very important 1.00a — 1.00a —
significant atexternalizing problems, peer alcohol access and lenient parental alcohol be relevant, but we have conducted
use, and alcohol use approval by rules (which was nonsignificant a comprehensive adjustment
peers.8,11,14 In our unadjusted after adjusting for capitalization on using variables known to predict
analyses, externalizing problems, chance). Although parental alcohol drinking, so the effect of unmeasured
adolescent perception of substance- use predicted parental supply in unobserved covariates is likely to be
using peers, and parent perception unadjusted analyses, this association small. Fourth, we have not been able
of substance-using peers, each disappeared in the adjusted model. It to assess the long-term associations
predicted subsequent parental supply. is possible that home alcohol access of early exposure to sips, which is a
However, after adjusting for a wide and lenient alcohol rules accounted matter for our ongoing work on this
range of familial, parental, peer, and for parental alcohol use. In previous cohort and not the focus of this paper.
adolescent factors, only parent factors studies8,9,12 and our present sample,
(parental perception of substance- parental supply occurred mostly in
using peers, home alcohol access, and familial social contexts. To this end,
lenient alcohol-specific rules) retained parental alcohol use may provide CONCLUSIONS
significant predictive associations. access and opportunity for parents
Compared with parents who did not to introduce alcohol to their child in The findings of this study are
supply alcohol, parents were more supervised, familial contexts. Likewise, important because we identify
likely to supply it if they perceived that the associations between lenient prospective predictors of parental
their child was mixing with substance- alcohol rules and home alcohol access supply of sips of alcohol, one of the
using peers and were more lenient on parental supply may increase first stages of drinking. The results
about alcohol access. This result is adolescent perception of parental show that parental perceptions of
consistent with recent longitudinal alcohol permissiveness, which whether their child engages with
findings, where the strongest increases the risk of early drinking substance-using peers are a significant
antecedents of sipping were parenting initiation.16 predictor of parental supply of
factors, whereas child psychosocial sips, along with home access and
proneness (such as externalizing) This study has a number of strengths. lenient alcohol rules. Parents may be
had no association.10 It seems The sample comprised a large-scale supplying sips of alcohol in response
parents may supply a sip of alcohol in cohort of young adolescents and 1 of to believing their child will be exposed
response to perceiving that their child their parents, recruited across a range to unsupervised alcohol use with their
has substance-using peers and are of sites, and Australia is a multicultural peers. However, they may be wrong in
motivated to inoculate their children country increasing generalizability of their belief, and may be prematurely
from the potential risk of unsupervised the results. The prospective design introducing their children to a
alcohol use and binge drinking with accounted for a wide range of different behavior that may have marked risks.
peers.9 In that regard, parents may be parent and child characteristics, Replication is needed, and research
reacting to a perceived risk of their using both adolescent- and parent- is required on whether supply of
adolescent child’s peers’ likelihood of report. Some limitations should sips quickly transitions to supply of
drinking, which may not be manifest; be considered. First, participants whole drinks, and whether predictors
they may be trying to inoculate against were not randomly selected from of supply differ with increasing
a nonexistent threat. the population, increasing the risk adolescent age and alcohol experience.
of self-selection and nonresponse Turning from the transitions of
Parental supply of sips may be biases. However, as outlined earlier parental behaviors to the transitions
motivated by the belief that smaller and elsewhere,15,28,29,33 the sample in actual adolescent drinking, it is also
quantities will protect their child reported many similarities on a necessary to better understand how
from unsupervised alcohol use with range of demographic and alcohol parental supply, even sips, relates to
peers and associated harms, such as use variables with the Australian the trajectories of adolescent from
binging.9 Sipping has been associated population, suggesting selective sipping to drinking and to binging.
with parental alcohol socialization nonresponse biases were minimized.
and lenient alcohol rules,8,10,11,14 and Second, self-report of parental supply
described as an opportunistic behavior may have resulted in social desirability ABBREVIATIONS
for parents to introduce alcohol in bias, where parents may have under-
CI: confidence interval
supervised contexts.8 Consistent with reported supply, fearing negative
OR: odds ratio
these notions, the only parenting social consequences, but this should
SES: socioeconomic status
practices associated with supply in reduce associations, so the results
T1: time 1
the present unadjusted and adjusted found are likely to be robust. Third,
T2: time 2
analyses were increased home alcohol other unmeasured covariates may
Downloaded from www.aappublications.org/news by guest on February 9, 2021
6 WADOLOWSKI et alconceptualization and design of the study, contributed to the design of the data collection instruments, critically reviewed the manuscript, and approved the final
draft of the manuscript; Prof Kypri contributed to the conceptualization and design of the study, contributed to the design of the data collection instruments,
critically reviewed the manuscript, and approved the final draft of the manuscript; Asst Prof Slade contributed to the conceptualization and design of the study,
contributed to the design of the data collection instruments, critically reviewed the manuscript, and approved the final draft of the manuscript; Dr McBride
coordinated and supervised data collection, critically reviewed the manuscript, and approved the final draft of the manuscript; and Prof Mattick contributed
to the conceptualization and design of the study, contributed to the design of the data collection instruments, coordinated and supervised data collection,
contributed to revising the manuscript, and approved the final draft of the manuscript.
This trial has been registered at www.clinicaltrials.gov (identifier NCT02280551).
Dr Bruno’s current affiliation is School of Psychology, Faculty of Health, University of Tasmania, Hobart, Tasmania, Australia.
DOI: 10.1542/peds.2015-2611
Accepted for publication Dec 2, 2015
Address correspondence to Dr Monika Wadolowski, National Drug and Alcohol Research Centre, Faculty of Medicine, University of New South Wales, Sydney, New
South Wales 2052, Australia. E-mail: m.wadolowski@unsw.edu.au.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2016 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have no financial relationships relevant to this article to disclose.
POTENTIAL CONFLICT OF INTEREST: The authors have no potential conflicts of interest to disclose.
FUNDING: Supporteded by: a 2010–2014 Australian Research Council Discovery Project grant (DP:1096668) to Prof Mattick, Prof Najman, Prof Kypri, Asst Prof
Slade, and Dr Hutchinson; an Australian Rotary Health Mental Health Research grant to Prof Mattick, Dr Wadolowski, Prof Najman, Prof Kypri, Asst Prof Slade, Dr
Hutchinson, and Asst Prof Bruno; an Australian Rotary Health Whitcroft Family PhD Scholarship Mental Health Research Companion grant to Dr Wadolowski; a
University of New South Wales Australian Postgraduate Award to Dr Wadolowski; a National Health and Medical Research Council Principal Research Fellowship
grant to Prof Mattick (APP1045318) and Prof Kypri (GNT0188568, APP1041867); National Health and Medical Research Council project grants to Prof Mattick for the
Longitudinal Cohorts Research Consortium (GNT1009381 and GNT1064893); and a Research Innovation grant from the Australian Foundation for Alcohol Research
and Education to Prof Mattick, Prof Najman, Prof Kypri, Asst Prof Slade, Dr Hutchinson, Asst Prof Bruno, and Dr Wadolowski. The National Drug and Alcohol
Research Centre at the University of New South Wales Australia (Dr Wadolowski, Dr Hutchinson, Asst Prof Bruno, Ms Aiken, Asst Prof Slade, and Prof Mattick) is
supported by funding from the Australian Government under a Substance Misuse Prevention and Service Improvements grant.
REFERENCES
1. Ellickson PL, Tucker JS, Klein DJ. sipping and drinking distinct? Alcohol through adolescence. J. Adolesc.
Ten-year prospective study of Clin Exp Res. 2015;39(9):1805–1813 Health. 2013;53(4):453–459
public health problems associated
7. Donovan JE. The burden of alcohol use: 13. Ward BM, Snow PC. Factors affecting
with early drinking. Pediatrics.
focus on children and preadolescents. parental supply of alcohol to underage
2003;111(5):949–955.
Alcohol Res. 2013;35(2):186–192 adolescents. Drug Alcohol Rev.
2. Hingson RW, Zha W. Age of drinking 2011;30(4):338–343
onset, alcohol use disorders, 8. Donovan JE, Molina BSG. Children’s
frequent heavy drinking, and introduction to alcohol use: sips 14. Jackson KM, Barnett NP, Colby SM,
unintentionally injuring oneself and and tastes. Alcohol Clin Exp Res. Rogers ML. The prospective association
others after drinking. Pediatrics. 2008;32(1):108–119 between sipping alcohol by the sixth
2009;123(6):1477–1484 grade and later substance use. J Stud
9. Jackson C, Ennett ST, Dickinson DM,
Alcohol Drugs. 2015;76(2):212–221
3. Gore FM, Bloem PJN, Patton GC, et al. Bowling JM. Letting children sip:
Global burden of disease in young people understanding why parents allow 15. Aiken A, Wadolowski M, Bruno R, et al.
aged 10-24 years: a systematic analysis. alcohol use by elementary school-aged Cohort profile: The Australian parental
Lancet. 2011;377(9783):2093–2102 children. Arch Pediatr Adolesc Med. supply of alcohol longitudinal study
2012;166(11):1053–1057 (APSALS) [published online ahead of
4. Patton GC, Coffey C, Cappa C, et al.
print May 6, 2015. Int J Epidemiol.
Health of the world’s adolescents: 10. Kypri K, Dean JI, Stojanovski E.
a synthesis of internationally Parent attitudes on the supply of 16. Donovan JE, Molina BSG. Childhood risk
comparable data. Lancet. alcohol to minors. Drug Alcohol Rev. factors for early-onset drinking. J Stud
2012;379(9826):1665–1675 2007;26(1):41–47 Alcohol Drugs. 2011;72(5):741–751
5. Wadolowski M, Bruno R, Aiken A, 11. Jackson C, Ennett S, Dickinson 17. Henderson H, Nass L, Payne C, Phelps
et al. Sipping, drinking, and early D, Bowling JM. Attributes that A, Ryley A. Smoking, drinking and drug
adolescent alcohol consumption: a differentiate children who sip alcohol use among young people in England in
cautionary note. Alcohol Clin Exp Res. from abstinent peers. J. Youth Adolesc. 2012. London: NHS Information Centre
2015;39(2):350–354 2013;42(11):1687–1695 for Health & Social Care; 2013
6. Wadolowski M, Hutchinson D, Bruno R, 12. Donovan JE, Molina BSG. Types of 18. White V, Bariola E. Australian
et al. Early adolescent alcohol use: Are alcohol use experience from childhood secondary school students’ use
Downloaded from www.aappublications.org/news by guest on February 9, 2021
PEDIATRICS Volume 137, number 3, March 2016 7of tobacco, alcohol, and over-the- 27. Joreskog K, Sorbom D. LISREL 8: an effective brief screening test
counter and illicit substances in Structural equation modeling with the for problem drinking. Ambulatory
2011. Melbourne, Victoria: Centre for SIMPLIS command language. Chicago, Care Quality Improvement Project
Behavioural Research in Cancer, The IL: Scientific Software International Inc; (ACQUIP). Alcohol Use Disorders
Cancer Council Victoria; 2012 1993 Identification Test. Arch Intern Med.
1998;158(16):1789–1795
19. Donovan JE. Really underage drinkers: 28. Australian Bureau of Statistics.
the epidemiology of children’s alcohol Australian demographic statistics, 35. Komro KA, Maldonado-Molina MM,
use in the United States. Prev Sci. June quarter 2012: Australian Tobler AL, Bonds JR, Muller KE. Effects
2007;8(3):192–205 demographic statistics tables. of home access and availability of
Canberra, Australian Capital Territory: alcohol on young adolescents’ alcohol
20. Donovan JE, Molina BSG. Antecedent use. Addiction. 2007;102(10):1597–1608
predictors of children’s initiation of Australian Bureau of Statistics; 2012
sipping/tasting alcohol. Alcohol Clin 36. van der Vorst H, Engels RCME, Meeus
29. Australian Bureau of Statistics. Family
Exp Res. 2014;38(9):2488–2495 W, Deković M, Van Leeuwe J. The
characteristics, Australia, 2009-10:
role of alcohol-specific socialization
21. Jones SC, Magee C, Andrews K. ‘I Households, families and persons,
in adolescents’ drinking behaviour.
think other parents might. …’: Using selected characteristics by state.
Addiction. 2005;100(10):1464–1476
a projective technique to explore Canberra, Australian Capital Territory:
parental supply of alcohol. Drug Australian Bureau of Statistics; 2011 37. Ary DV, Duncan TE, Duncan SC, Hops
Alcohol Rev. 2015;34(5):531–539 H. Adolescent problem behavior: the
30. Pink B. Information paper: An influence of parents and peers. Behav
22. Jackson KM, Colby SM, Barnett NP, introduction to Socio-Economic Indexes Res Ther. 1999;37(3):217–230
Abar CC. Prevalence and correlates of for Areas (SEIFA) 2006. Canberra,
Australian Capital Territory: Australian 38. Small SA, Kerns D. Unwanted sexual
sipping alcohol in a prospective middle
Bureau of Statistics, Commonwealth of activity among peers during early
school sample. Psychol Addict Behav.
Australia; 2008 and middle adolescence: Incidence
2015;29(3):766–778
and risk factors. J Marriage Fam.
23. Kaynak Ö, Winters KC, Cacciola 31. Australian Bureau of Statistics. Socio- 1993;55(4):941–952
J, Kirby KC, Arria AM. Providing economic Indexes for Areas (SEIFA),
39. Stice E, Barrera M Jr, Chassin L.
alcohol for underage youth: what Data cube, 2006. Canberra, Australian
Prospective differential prediction of
messages should we be sending Capital Territory: Australian Bureau of
adolescent alcohol use and problem
parents? J Stud Alcohol Drugs. Statistics; 2008
use: examining the mechanisms
2014;75(4):590–605 of effect. J Abnorm Psychol.
32. White V, Smith G. Australian secondary
24. Donovan JE. Adolescent alcohol school students’ use of tobacco, 1998;107(4):616–628
initiation: a review of psychosocial alcohol, and over-the-counter and 40. Johnston LD, Bachman JG, O’Malley PM.
risk factors. J Adolesc Health. illicit substances in 2008. Melbourne, Monitoring the Future: Questionnaire
2004;35(6):529.e7–529.e18 Victoria: Centre for Behavioural responses from the nation’s high
Research in Cancer, The Cancer school seniors, 2011. Ann Arbor,
25. Windle M, Spear LP, Fuligni AJ, et
Council Victoria; 2009 MI: Institute for Social Research,
al Transitions into underage and
problem drinking: Developmental 33. Australian Institute of Health & University of Michigan; 2013
processes and mechanisms Welfare. 2010 National Drug Strategy 41. Achenbac-h TM. Manual for the
between 10 and 15 years of age. Household Survey report. Canberra, youth self-report and 1991 profile.
Pediatrics. 2008;121(suppl 4): A: Australian Institute of Health & Burlington, VT: University of Vermont;
S273–S289 Welfare; 2011 1991
26. LISREL 8.8 for Windows [computer 34. Bush K, Kivlahan DR, McDonell MB, 42. Stata/SE 11.2 for Windows [computer
program]. Skokie, IL: Scientific Fihn SD, Bradley KA. The AUDIT alcohol program]. College Station, TX:
Software; 2006 consumption questions (AUDIT-C): StataCorp LP; 2012
Downloaded from www.aappublications.org/news by guest on February 9, 2021
8 WADOLOWSKI et alParents Who Supply Sips of Alcohol in Early Adolescence: A Prospective Study
of Risk Factors
Monika Wadolowski, Delyse Hutchinson, Raimondo Bruno, Alexandra Aiken, Jackob
M. Najman, Kypros Kypri, Tim Slade, Nyanda McBride and Richard P. Mattick
Pediatrics 2016;137;
DOI: 10.1542/peds.2015-2611 originally published online February 26, 2016;
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/137/3/e20152611
References This article cites 29 articles, 3 of which you can access for free at:
http://pediatrics.aappublications.org/content/137/3/e20152611#BIBL
Subspecialty Collections This article, along with others on similar topics, appears in the
following collection(s):
Adolescent Health/Medicine
http://www.aappublications.org/cgi/collection/adolescent_health:med
icine_sub
Substance Use
http://www.aappublications.org/cgi/collection/substance_abuse_sub
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on February 9, 2021Parents Who Supply Sips of Alcohol in Early Adolescence: A Prospective Study
of Risk Factors
Monika Wadolowski, Delyse Hutchinson, Raimondo Bruno, Alexandra Aiken, Jackob
M. Najman, Kypros Kypri, Tim Slade, Nyanda McBride and Richard P. Mattick
Pediatrics 2016;137;
DOI: 10.1542/peds.2015-2611 originally published online February 26, 2016;
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/137/3/e20152611
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2016
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
Downloaded from www.aappublications.org/news by guest on February 9, 2021You can also read