Have we got the right focus in asthma care in general practice?
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Research
Have we got the right focus in
asthma care in general practice?
A qualitative study
Maithri Rupasinghe, Jennifer Reath, IN AUSTRALIA, one in nine people reports Methods
Biljana Cvetkovski, Sheree Smith, having been diagnosed with asthma, with This was a qualitative study employing
Sinthia Bosnic-Anticevich, Vicky Kritikos, most asthma care delivered in general semi-structured interviews. The research
Penelope Abbott practice.1,2 However, opportunities team comprised GPs working in clinical
to optimise the control of asthma are practice and academic roles, and
Background and objective missed, including through poor adherence researchers with backgrounds in nursing,
Asthma presentations are common in to asthma guidelines.3–5 Structural and pharmacy, respiratory medicine and
general practice, but opportunities to knowledge barriers to asthma care qualitative research. All had experience in
control asthma are often missed. The delivered by general practitioners (GPs) delivering asthma care. Ethical approval
aim of this study was to explore how have been identified, including time was obtained from the Human Research
general practitioners (GPs) and practice
pressure, cost of spirometry and access Ethics Committee, Western Sydney
nurses (PNs) deliver asthma care, with
particular attention to perceived roles
to continuing medical education.4–6 University (H 13404).
and challenges, and ways to improve Some of these barriers may be Convenience and snowball sampling
management. overcome by improving team care in was used to recruit GPs and PNs. Email
asthma. Team work between GPs and invitations were sent to general practices
Methods
practice nurses (PNs) enhances healthcare affiliated with the teaching program of the
Using a qualitative approach, semi-
structured interviews were conducted delivery; however, this can be impeded Department of General Practice, Western
with GPs and PNs working in an area by a lack of clearly defined roles.7,8 Sydney University, and study participants
of cultural diversity and socioeconomic Expanding the PN role may be challenged referred by colleagues. Participants were
disadvantage in western Sydney. Inductive by the small business nature of Australian drawn from western Sydney, an area
thematic analysis was undertaken. general practice and funding that does of high cultural diversity and pockets
Results not support team care, and GPs not of social and economic disadvantage,
Nineteen interviews were conducted, with understanding PNs’ practice scope.9,10 where there is high use of general practice
nine GPs and 10 PNs. The main focus of To date, there has been little research services.11
asthma care was on acute presentations, examining GP and PN perspectives on All interviews were conducted by
with less emphasis on follow-up and delivering asthma care in general practice the lead researcher, who had no prior
preventive care and underuse of general
and how they could be supported to affiliation with participants, over a period
practice chronic disease models of care.
PN roles were generally limited to acute
optimise management. This study was of three months in 2019. An interview
asthma assessment and triage. GPs did conducted in western Sydney, Australia, guide was devised, based on the literature
not commonly use spirometry or access an urban region that includes some on asthma care and healthcare delivery
non-GP specialist input. of the most disadvantaged suburbs in general practice and research team
in the state and where the burden of expertise (Table 1). The interviews were
Discussion
Asthma care in general practice may be asthma is particularly high.1 This study semi-structured, with participant-led
improved by a greater focus on prevention explores how GPs and PNs deliver content encouraged. Focused probes were
and control, including through follow-up asthma care, with particular attention added as the data collection proceeded
after acute presentations, enhanced to their perceived roles and challenges, to further explore themes identified in
collaboration between GPs and PNs, and consideration of ways to improve the ongoing analysis. Interviews were
and supportive practice models.
management. recorded and then transcribed, and the
410 Reprinted from AJGP Vol. 50, No. 6, June 2021 © The Royal Australian College of General Practitioners 2021Have we got the right focus in asthma care in general practice? A qualitative study Research
de-identified data were managed using of asthma, using spirometry, accessing practices that I work, because I’m not
NVivo 12 software (QSR International). and updating knowledge, and accessing highly involved in the patients’ asthma
Reflexive, data-driven thematic additional medical opinion or care care – so that’s why that system is not
analysis12,13 was undertaken, underpinned in asthma. happening for them. (PN 8)
by a grounded theory approach and
recognition of the effect of the research Teamwork and discordant Focus on episodic acute asthma
team on the research. This included perceptions of roles in asthma care GPs and PNs reported that the practice
recognition that the research team Asthma care was reported to be led by team was well organised in episodic
members had a special interest in asthma GPs, with the PN role generally limited acute management. However, patients
care, and brought their understandings to assessing and triaging patients with with recurrent acute presentations were
to the research findings. The analysis acute asthma and performing spirometry. not usually engaged in preventive care.
involved multiple stages, including Asthma action plans were completed by It was suggested that this could be due
independent coding of early transcripts by GPs without involvement of PNs. Some to a lack of consideration of the dangers
three team members, subsequent iterative GP and PN participants recommended of acute asthma and value of prevention
coding of the whole dataset by MR, review PNs should have a broader role, including by patients.
of the dataset by multiple team members, delivering inhaler skill training and asthma
identification of themes and subthemes, education. PNs perceived they had limited People, they don’t take asthma disease
memo-writing, and refinement through time for this, given GP and practice as serious as the other chronic diseases …
group discussions into a finalised list of priorities, whereas GPs saw lack of PN because it’s a common disease, especially
themes. Interviews were conducted until skills as the main barrier. Several PNs felt from childhood, and I think, it’s more
the researchers observed data saturation GPs did not recognise the value of their about education, that people are not
for key themes. potential role in clinical management of adequately educated that asthma can
asthma and that teamwork was suboptimal, be very serious. (PN 8)
to the detriment of patient care.
Results It was reported that when patients
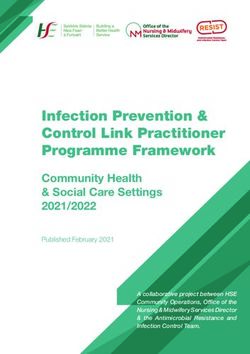
Nineteen interviews, face to face (16) GPs are the decision makers. When [a] presented to the practice with acute
or by telephone (three), were conducted decision is made, the nurses and the staff asthma symptoms, GPs and PNs generally
with GPs (nine) and PNs (10) from nine should be able to do it, but some can’t chose to use nebulisers instead of metered
different general practices. Participants do it; there are few nurses who are senior dose inhalers with spacers. This was
ranged in age from 25 to 59 years and nurses who know about these things but seen as more acceptable to the patient
varied in their engagement with asthma not the younger generation – it is very and more time-efficient to the practice.
patients and the frequency with which disappointing. (GP 3) GPs recognised this was a choice based
they saw people with asthma (Table 2). on convenience rather than adherence
Interviews ranged from 20 to 40 minutes, The services that GPs ask me to deliver to guidelines.
with a median duration of 32 minutes. The to the patient, that’s what I do. Practice
five themes identified in the analysis were nurses, they’re good at doing clinical I would probably say most of them don’t
the roles of GPs and PNs in asthma care, management. The more a PN is involved, even need that level of nebulisation to be
focusing on acute rather than chronic care the better that system gets … in the honest because they are only going to be
mild, moderate, and nebulisations are
usually reserved for the severe. But the
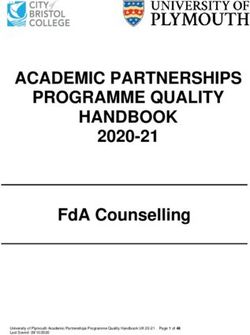
Table 1. Semi-structured interview guide problem, I guess, is convenience. (GP 1)
Topic Examples of probes
Nebuliser is easy for me. I give it to patients
General practitioner/practice nurse role Challenges, facilitators, expanding the role, very frequently because I’m used to giving
in asthma teamwork the nebuliser, not the spacer. [The] patient
also feels good after [the] nebuliser. (PN 4)
Approach to assessment/diagnosis Use of spirometry, challenges, facilitators,
strategies to improve
Most participants believed that health
Approach to management Acute asthma, chronic disease management, system and practice factors also
patient education encouraged the prioritisation of acute
Approach to updating knowledge Guidelines, pharmaceutical industry, education asthma management. Funding in general
preferences, challenges, facilitators practice was described as incentivising
short consultations, which contributes to
Seeking additional care, specialist opinion Processes, value, challenges less consultation time spent on prevention
or guidance for patient care
and patient education.
© The Royal Australian College of General Practitioners 2021 Reprinted from AJGP Vol. 50, No. 6, June 2021 411Research Have we got the right focus in asthma care in general practice? A qualitative study
The biggest problem that I face is people are
Table 2. Participant sociodemographic characteristics not accepting asthma, it is underdiagnosed,
Participant characteristics Number of participants (n = 19) a lot of, you know, [ethnic groups], they take
it as a social stigma, like they don’t want to
Role say I’ve got asthma. (GP 3)
GPs 9
Spirometry
PNs 10 A minority of general practices had
Gender Male Female spirometers, and spirometry was only
done if a PN was available. It was most
GPs 4 5 used in diagnosing chronic cough
PNs 0 10 and differentiating between chronic
obstructive pulmonary disease (COPD)
Years of experience range (years) and asthma. Facilitators of spirometry
GPs 1–30 use were good PN staffing, availability
through pathology collection centres,
PNs 1–20 linkage to clinical management software,
Less Every Usually Several and availability of PN training in asthma at
Frequency of asthma-related consultations often 2–3 days once/day times/day the primary health network. PNs reported
being interested in performing spirometry,
GPs 2 4 2 1 and found it assisted in patient education.
PNs 1 6 2 1
In the other practice … they booked
Practice billing characteristics Number of general practice clinics (n = 9) patients under me, I did spirometry for
Bulk billing (service covered by Medicare) 6 them … The challenge [is] non-availability
of spirometry, you know. I need to educate
Private fees (patient-claimed partial 3 and train them on treatment for the
reimbursement from Medicare)
asthma but I don’t know whether the
GPs, general practitioners; PNs, practice nurses patient has COPD or asthma … If we have
a spirometry I perform it here. (PN 1)
The government is rewarding short high we always recall the patient. Otherwise, Some GPs reported that they relied on
turnover, patient care rather than quality, for asthma, I think I did not. (PN 4) clinical features for diagnosis of asthma
comprehensive chronic conditions care. and did not perceive spirometry to be of
And if actually you spend half an hour The culturally and linguistically diverse value. Barriers to its use were the cost of the
and do your job really well, it will mean (CALD) backgrounds and poor health spirometer; perceived lack of benefit; poor
less flare-ups and they won’t come back as literacy of some patients regarding Medicare rebate; complexity of technique;
often because you would have dealt with asthma were reported to compromise and lack of trained nurses, clinic space and
it properly and it’s less cost to the health long-term management and adherence time required to perform spirometry.
system. (GP 8) to preventer medications. Participants
perceived that people from certain CALD We don’t use spirometry in our practice.
While used by some, chronic disease care backgrounds did not consider asthma as a We diagnose asthma clinically with a good
plans and follow-up systems for people chronic health problem, worried that they clinical history and clinical judgement. We
with asthma were not usual. Most practices would become dependent on preventer used to have a spirometer. But the problem
did not have a system for flagging and medications and found a diagnosis of is that you need a nurse to do that. And then
recalling patients with acute asthma asthma to be stigmatising. the other thing is that there is not enough
presentations. rebate for spirometry. It’s not enough, you
Most of them are first-time migrants, know, for the time spent. (GP 4)
There’s not a lot of incentive, financially, having grown up in different countries
either, for the practice to prioritise recall where the management of asthma might Accessing guidelines and updating
for asthma. (GP 5) be very sporadic and fragmented and, knowledge
with their own health literacy and ideas National Asthma Council online guidelines
For the other diseases, if they need to discuss and cultural beliefs, a number of them are were the main reference source described
it, there is a result with the doctor for the quite reluctant to use puffers because of the by GPs. However, the complexity of the
diabetes or other blood test results, [and] so-called dependence issue. (GP 2) guidelines, and difficulties in navigating
412 Reprinted from AJGP Vol. 50, No. 6, June 2021 © The Royal Australian College of General Practitioners 2021Have we got the right focus in asthma care in general practice? A qualitative study Research
them, meant that finding the required We use specialists just to reassure ourselves controlling asthma in general practice,
information was difficult. and to find out whether we’ve done consistent with previous research.15 This
everything right for the legal purpose. If appeared to be reinforced by patients
Guidelines, I guess because for different something goes wrong, you know, we can and the general practice team. The
age groups there’s a lot of different things get sued, so the only reasons why I send interviewees believed the lack of focus
there. Yes, I guess it is not as user friendly someone with asthma to a specialist is either on asthma control was driven to a large
as it could be because there’s a lot of, like, on parents’ request – or just to cover myself extent by their patients, who generally
multiple links for all the separate subsets. from legal problems, to check whether I have sought healthcare for acute presentations
It would be easy if you can have one done everything right for a legal issue. In only. Those from CALD backgrounds
simple, clear diagram. (GP 1) those instances only, I consult a specialist. were thought to be particularly likely
[Otherwise] there is no need. (GP 3) to disagree with the concept of asthma
GPs reported updating their knowledge as a chronic disease. Previous research
through a variety of channels including The patients, they’re happier to see [a] GP, into GP views about asthma and patients
pharmaceutical representative visits and not a specialist, because first, they can’t get from CALD backgrounds who were
workshops providing updates on asthma [a specialist] appointment early. Second, Arabic-speaking also identified decreased
guidelines and new inhaler devices. it’s the cost, it costs them much … It takes self-management as a concern, along
GPs believed that HealthPathways,14 an a long time to get to see a specialist, unless with the need to improve the cultural
online information portal that provides they [have a] very severe problem. (PN 9) competence of healthcare professionals in
clinical information to enhance patient managing asthma in CALD populations.16
management, was valuable. Long outpatient wait lists were seen People with asthma often overestimate
as a barrier to preventive asthma care. the degree to which their asthma is
The other things we use [in addition to However, GPs reported use of emergency controlled.17 Overuse of short-acting
on line guidelines] are pharmaceutical departments for acute asthma as a bronchodilators relative to preventer
[representatives] coming in from time pathway to respiratory specialist advice. medications appears common.18
to time, and … our usual resources in Promoting objective assessment
general practice, magazines, [and] [The] public hospital setting is difficult by patients of their own asthma,
HealthPathways, which is up there, which because of the waiting lists ... We do have self-management and understanding of
has very, very clear-cut guidelines. (GP 2) the asthma clinic there on hand for advice, the importance of controlling asthma is
and they will see the patient eventually, but needed.19,20 Acute asthma presentations
PNs described limited education and there is a bit of a waiting time. I guess there in general practice flag the need to review
training related to asthma, including would probably be more success [in timely and improve control. However, the present
spirometry, although they welcomed the access to specialist advice] if patients study suggests that opportunities for this
opportunity for further training. They end up more often in [the emergency may continue to be missed.
expressed interest in workshops and department]. (GP 1) The lack of follow-up after acute
practice-based education, and identified exacerbations of asthma in the present
that greater clinical responsibility for study accorded with previous research.6,21
asthma would drive PN education. Discussion In the present study, this appeared to be
GPs and PNs participating in this research exacerbated by lack of practice systems
I would say that I just follow whatever the reported multiple challenges in providing for asthma and suboptimal collaboration
doctors are telling to me to do, but they are quality asthma care, despite it being a within practice teams. Patients with
not telling me why I should do that. I would common condition in general practice.1 frequent exacerbations could ‘fall through
say that I have less knowledge on asthma. The present study provides insight into the cracks’ and not be adequately engaged
I believe that nurses need to organise their the challenges of managing asthma in in preventive care despite having unstable
education on asthma. Then we can help in an urban setting, in an area where a asthma. Asthma did not appear to be
diagnosis and management. (PN 4) high population of culturally diverse, usually managed as a chronic health
socioeconomically disadvantaged problem within existing chronic disease
Accessing additional medical opinion people receive asthma care in general models of care, such as care plans and
or care in asthma practice. These challenges related to scheduled recalls and reminders. PNs
GPs perceived that non-GP specialist lack of teamwork, focus on acute asthma have a pivotal role in managing other
referral is rarely required and almost all over chronic asthma care, low use of chronic conditions,22 yet in the present
asthma patients can be managed in general spirometry, inconsistent education and study were little used beyond acute
practices. Costs for private respiratory training access, and perceived limited management of asthma. Some GPs were
specialist consultations and waiting lists for need for non-GP specialist input. not confident in the skills and training of
hospital-based specialists were barriers to The study highlights the persistence PNs to take on a greater role; PNs spoke
accessing specialist advice. of a focus on treating acute asthma over of not being enabled to contribute beyond
© The Royal Australian College of General Practitioners 2021 Reprinted from AJGP Vol. 50, No. 6, June 2021 413Research Have we got the right focus in asthma care in general practice? A qualitative study
acute asthma triage and treatment, which study showed that cost and long waiting Sheree Smith BNursing, MSocPlanningDevelopment,
PhD (Public Health), PostGradCertHealthEcon,
decreased motivation for training despite lists inhibited referral to private and Professor, School of Nursing and Midwifery, Western
a perceived need. It appears that PNs may hospital non-GP specialists.27 However, the Sydney University, NSW
be a valuable resource to improve the study suggests there was also a perception Sinthia Bosnic-Anticevich BPharm (Hons),
PhD, Professor and Team Leader, Quality Use
systematic management of asthma within among GPs that non-GP specialist opinions of Respiratory Medicines Use Group, Woolcock
general practice and provide more patient were not commonly needed, which again Institute, University of Sydney, Sydney Local Health
District, NSW
education through role division. may reflect a focus on episodic acute
Vicky Kritikos BPharm, MPharm (Clinical), PhD,
The use of nebulisers for convenience asthma care. GradCertEdStudies (Higher Education), Clinical
in acute attacks – irrespective of severity A limitation of this study was that Lead, Quality Use of Respiratory Medicines Group,
Woolcock Institute of Medical Research, University of
and at variance with the guideline it was undertaken in general practices
Sydney, NSW; Department of Respiratory and Sleep
recommendation for use of spacers affiliated with an academic general Medicine, Royal Prince Alfred Hospital, NSW
and reliever inhalers – may further practice department, raising the possibility Penelope Abbott MBBS (Hons), MPH, PhD, Churchill
Fellow, GAICD, FRACGP, Associate Professor,
distract from a chronic disease focus that participant interview responses were
Department of General Practice, School of Medicine,
by reinforcing an emergency response. influenced by this relationship. This large Western Sydney University, NSW
The lack of value GPs appeared to place pool of practices is commonly contacted Competing interests: SBA reports an unrestricted
on opinions from non-GP specialists research grant on inhaler technique, and lecture
for different research opportunities, which
and advisory board fees from Teva Pharmaceuticals,
may be further evidence that they were may ameliorate that risk. Another potential advisory board and lecture fees from AstraZeneca
not thinking about asthma as a chronic limitation was that it was restricted to one and Boehringer Ingelheim, lecture fees from GSK and
consultancy fees from Sanofi and Mylan, outside the
disease. Additionally, spirometry was geographic region. However, this is also submitted work.
often seen by GP participants as being of a useful aspect of research as it provides Funding: Department of General Practice, Western
limited value and the rebate for spirometry information on what is occurring in an Sydney University, for payment of participants and
transcription of interviews. The lead researcher
as providing inadequate recompense. area where there is high burden of asthma, (MR) was supported by a scholarship for his
However, up to one-third of patients with high health needs, cultural diversity and post-MD overseas training in family medicine by
the Postgraduate Institute of Medicine, Sri Lanka,
doctor-diagnosed asthma do not have socioeconomic disadvantage, and yet good
and the Ministry of Health, Sri Lanka.
asthma when objectively measured,23 availability of general practice care. The Provenance and peer review: Not commissioned,
and guidelines promote the routine use of researchers have described the context externally peer reviewed.
spirometry in the diagnosis of asthma. of this region to assist readers to assess Correspondence to:
P.Abbott@westernsydney.edu.au
Education related to asthma was valued transferability of the findings.
by GPs and PNs. Both groups recognised Acknowledgements
the National Asthma Council guidelines24 The authors would like to acknowledge the general
as the benchmark, though found it Conclusion practitioners, practice nurses and practices who
participated in the study, and Vicki Bradley and
complex. The present study suggests This study has provided insight into the Sharon Lawrence, Western Sydney University, for
asthma education for healthcare providers challenges encountered by GPs and PNs administrative support.
needs to include strong messaging around in assessing and managing asthma in an
following up acute asthma presentations, Australian setting. The research suggests References
1. Australian Institute of Health and Welfare. Cat. no.
including within a chronic disease that increased messaging around asthma ACM 33. Canberra, ACT: AIHW, 2020. Available
model, to ensure optimal asthma control. as a chronic health issue to both patients at www.aihw.gov.au/reports/chronic-respiratory-
HealthPathways14 may be of assistance in and primary health care providers will conditions/asthma/contents/asthma [Accessed
2 February 2021].
this goal. Similar focus in patient education help improve outcomes. At the general
2. Britt H, Miller GC, Henderson J, et al. General
is needed, including the importance of practice level, this includes improvements practice activity in Australia 2014–15. General
preventing acute asthma and countering in flagging acute presentations; teamwork; practice series no. 38. Sydney, NSW: Sydney
University Press, 2015.
the perceived need for nebulisation. the use of existing practice systems; and
3. Barton C, Proudfoot J. Amoroso C, et al.
In terms of the healthcare system, the funding for chronic disease management Management of asthma in Australian general
Australian general practice funding model such as care plans and recall systems, which practice: Care is still not in line with clinical
practice guidelines. Prim Care Respir J
and barriers to accessing non-GP specialist encourage follow-up after acute asthma. 2009;18(2):100–05. doi: 10.3132/pcrj.2008.00059.
advice were seen to compromise quality in 4. Watkins K, Fisher C, Misaghian J, Schneider CR,
asthma care. Although longer consultations Clifford R. A qualitative evaluation of the
Authors implementation of guidelines and a support tool
are associated with better decision making for asthma management in primary care. Asthma
Maithri Rupasinghe MBBS, MRCGP (INT), MD
and resource usage, fee-for-service (Family Medicine), FCGP, Visiting Fellow, Department Res Pract 2016;2:8. doi: 10.1186/s40733-016-
of General Practice, Western Sydney University, NSW 0023-9.
funding may incentivise throughput and
Jennifer Reath MBBS, MMed, PhD, FRACGP, Dip 5. Heiner MM. Key barriers to optimal
inadequately support team-based care.25,26 RANZCOG, GAICD, Foundation Peter Brennan Chair management of adult asthma in Australia:
Further, GPs often saw themselves as of General Practice, Western Sydney University, NSW Physician and patient perspectives. Curr
Med Res Opin 2007;23(8):1799–803.
managing asthma without significant Biljana Cvetkovski BPharm (Hons), MPharm
(Research), PhD, Postdoctoral Research Fellow, doi: 10.1185/030079907X210714.
input from non-GP specialist colleagues. Quality Use of Respiratory Medicines Use Group, 6. Zwar NA, Comino EJ, Hasan I, Harris MF. General
Consistent with other research, the present Woolcock Institute, University of Sydney, NSW practitioner views on barriers and facilitators to
414 Reprinted from AJGP Vol. 50, No. 6, June 2021 © The Royal Australian College of General Practitioners 2021Have we got the right focus in asthma care in general practice? A qualitative study Research
implementation of asthma 3+ visit plan. Med J Available at www.ciap.health.nsw.gov.au/specialty- 21. Rudolphy S. Asthma management in general
Aust 2005;183(2):64–67. doi: 10.5694/j.1326- guides/nsw-healthpathways.html [Accessed practice – A chronic disease health priority.
5377.2005.tb06923.x. 27 April 2021]. Aust Fam Physician 2008;37(9):710–14.
7. Abbott P, Dadich A, Hosseinzadeh H, et al. Practice 15. Cvetkovski B, Armour C, Bosnic-Anticevich S. 22. Young J, Eley D, Patterson E, Turner C. A nurse-
nurse and sexual health: Enhancing team care Asthma management in rural New South led model of chronic disease management in
within general practice. Aust Fam Physician Wales: Perception of health care professionals general practice: Patients’ perspectives. Aust Fam
2013;42(10):729–32. and people with asthma. Aust J Rural Health Physician 2016;45(12):912–16.
8. Walker L. Practice nurses: Working smarter 2009;17(4):195–200. doi: 10.1111/j.1440- 23. Aaron SD, Vandemheen KL, FitzGerald JM, et al.
in general practice. Aust Fam Physician 1584.2009.01071.x. Reevaluation of diagnosis in adults with physician-
2006;35(1–2):20–2. 16. Alzaye R, Chaar BB, Basheti IA, Saini B. diagnosed asthma. JAMA 2017;317(3):269–79.
9. Halcomb EJ, Salamonson Y, Davidson PM, General practitioners’ experience of asthma doi: 10.1001/jama.2016.19627.
Kaur R, Young SA. The evolution of nursing management in culturally and linguistically
24. National Asthma Council. Australian asthma
in Australian general practice: A comparative diverse populations. J Asthma 2019;56(6):642–52.
handbook. South Melbourne, Vic: NAC, 2020.
analysis of workforce. BMC Fam Pract 2014;15:52. doi: 10.1080/02770903.2018.1472280.
Available at www.asthmahandbook.org.au
doi: 10.1186/1471-2296-15-52. 17. Kritikos V. Price D, Papi A, et al. A multinational [Accessed 2 February 2021].
observational study identifying primary care
10. Halcomb EJ, Salamonson Y, Cooper M, Clauson JL, 25. Heywood T, Laurence T. The general practice
patients at risk of overestimation of asthma
Lombardo L. Culturally and linguistically diverse nurse workforce: Estimating future supply. Aust J
control. NPJ Prim Care Respir Med 2019;29(1):43.
general practitioners’ utilization of practice nurses. Gen Pract 2018;47(11):788–95. doi: 10.31128/AJGP-
doi: 10.1038/s41533-019-0156-4.
Collegian 2013;20(3):137–44. doi: 10.1016/j. 01-18-4461.
colegn.2012.05.001. 18. Azzi EA, Kritikos V, Peters MJ, et al. Understanding
reliever overuse in patients purchasing over-the- 26. Sturmberg J, O’Halloran D, McDonnell G,
11. Australian Institute of Health and Welfare. Healthy Martin C. General practice work and workforce:
counter short-acting beta2 agonists: An Australian
community indicators. Canberra, ACT: AIHW, Independencies between demand, supply and
community pharmacy-based survey. BMJ Open
2020. Available at www.aihw.gov.au/reports- quality. Aust J Gen Pract 2018;47(8):507–13.
2019;9(8):e028995. doi: 10.1136/bmjopen-2019-
data/indicators/healthy-community-indicators doi: 10.31128/AJGP-03-18-4515.
028995.
[Accessed 2 February 2021].
19. Price D, David-Wang A, Cho SH, et al. Time for a 27. Chung LP, Hew M, Bardin P, McDonald VM,
12. Braun V, Clarke V. Using thematic analysis in Upham JW. Managing patients with severe asthma
new language for asthma control: Results from
psychology. Qual Res Psychol 2006;3(2):77–101. in Australia: Current challenges with existing
REALISE Asia. J Asthma Allergy 2015;8:93–103.
doi: 10.1191/1478088706qp063oa. model of care. Intern Med J 2018;48(12):1536–41.
doi: 10.2147/JAA.S82633.
13. Braun V, Clarke V. Reflecting on doi: 10.1111/imj.14103.
20. Bosnic-Anticevich S, Kritikos V, Carter V,
reflexive thematic analysis. Qual Res et al. Lack of asthma and rhinitis control
Sport Exerc Health 2019;11(4):589–97. in general practitioner-managed patients
doi: 10.1080/2159676X.2019.1628806. prescribed fixed-dose combination therapy
14. Clinical Information Access Portal. NSW in Australia. J Asthma 2018;55(6):684–94.
HealthPathways. Sydney, NSW: CIAP, 2021. doi: 10.1080/02770903.2017.1353611. correspondence ajgp@racgp.org.au
© The Royal Australian College of General Practitioners 2021 Reprinted from AJGP Vol. 50, No. 6, June 2021 415You can also read