Miss. N.Rai, MD, MRCOG - Consultant in Gynae Oncology Southend University Hospital, NHS Foundation Trust
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Miss. N.Rai, MD, MRCOG Consultant in Gynae Oncology Southend University Hospital, NHS Foundation Trust

Objective 2 WW referral criteria Overview of pathway Talking points Can we do better?
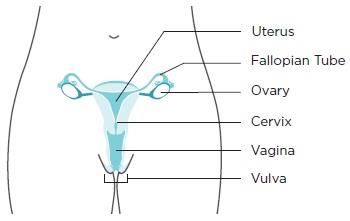
Gynaecological maliganacies Pic – courtesy CDC

Why 2WW clinic DOH recommendation since 2000 Patients in England have more advanced cancers at diagnosis (National audit 2004);older people, deprived areas more at risk Provides Rapid access Facilitates Prompt assessment Streamlines pathway Aims to improve putcomes
identifying patients needing urgent referral for suspected cancer a)symptoms, signs and other factors, taking into account variation in risk by age and ethnic group b) the initial investigations that contribute to the assessment of patients prior c)to, or in association with, urgent referral for suspected cancer d)interventions intended to help healthcare professionals appropriately
NICE Guideline-referrals for Gyn
cancers
•Lesions suspicious of cancer on cervix or
vagina on speculum examination (or smear
suspicious of invasive cancer)
•Lesions suspicious of cancer on clinical
examination of the vulva.
•Palpable pelvic mass not obviously fibroids.
•Suspicious pelvic mass on pelvic ultrasound.
•More than one or a single heavy episode of
postmenopausal bleeding (PMB) in women
aged >55 years who are not on HRT.
•Postcoital bleeding (PCB) in women age >55
that persists for more than 4 weeks.
•HRT - Unexpected or prolonged bleeding
persisting for more than 4 weeks after
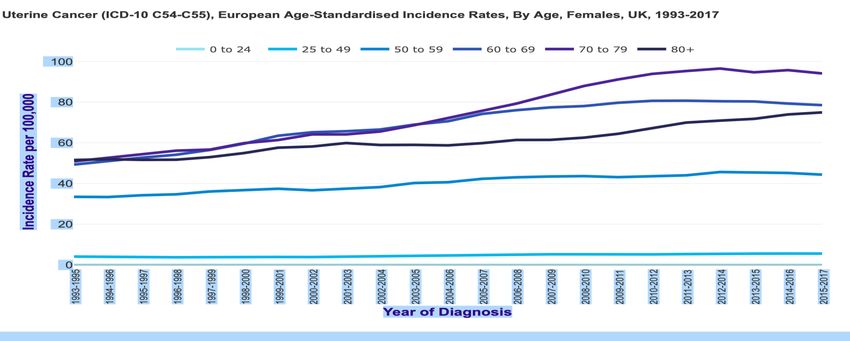
stopping HRT.Endometrial Cancer Commonest Early presentation is expressed as PMB triggering investigations 1 in 10 with PMB have endometrial cancer More than 9000 new cases a year (2015-2017 CRUK) Since 1990 55% increase in incidence 34% cases are preventable A full time GP is likely to diagnose approximately 1 person with endometrial cancer every 3-5 years (NICE).
Risk factors for Endometrial Ca Age Obesity Extraneous oestrogen in perimenopause/post menopause, tamoxifen, hormone producing ovarian tumours, and polycystic ovarian syndrome (PCOS) Type 2 diabetes Family history or personal history of endometrial or colorectal/breast cancer Background of endometrial hyperplasia current/past Previous radiation therapy to the pelvis as treatment for other cancers
2 WW Referral criteria - PMB
2 WW referral – criteria changed in 2015
Age (55) as a factor, Other non-PMB symptoms and tests
2 ww referral
If aged 55 and over with PMB
Consider
2 WW in under 55 with PMB [new 2015]
Suspected cancer: Recognition and referral
NICE Guideline June 20152 WW Referral criteria - PMB
Consider Direct access USS
if > = 55 with unexplained vaginal discharge
for first time or with thrombocytosis or report haematuria
visible haematuria with
low haemoglobin levels or thrombocytosis or high blood glucose
levels. [new 2015]
Suspected cancer: Recognition and referral
NICE Guideline June 2015Diagnostic Assessment TVS outpatient endometrial biopsy outpatient hysteroscopy+/- endometrial sampling+/- polypectomy GA hysteroscopy+/- endometrial curreting+/- polpectomy
Ovarian Cancer (OC) Early diagnosis is key. Five year survival is dependent upon the stage at diagnosis. Relative 5 year survival rates – 34 %, lower than European average, But stage 1, survival rates of 90% achieved over 7,000 new ovarian cancers A full time GP is likely to diagnose approximately 1 person with ovarian cancer every 3-5 years Non specific vague presenting symptoms
Symptoms suggestive of OC Common symptoms Bloating, distension Abdominal or pelvic pain/discomfort Feeling full quickly, loss of appetite, unintentional weight loss Urinary frequency or altered bowel habits Less common symptoms Persistent indigestion/nausea/vomiting PMB/discomfort during sex/pelvic fullness Feeling tired all the time
When to refer? (NICE guidance) Refer urgently if physical examination identifies ascites and or a pelvic or abdominal mass (which is not obviously a uterine fibroid If the ultrasound suggests ovarian cancer Raised CA 125 and abnormal USS For any woman who has normal serum CA125 (less than 35 IU/ml), or CA125 of 35 IU/ml or greater but a normal ultrasound -assess her carefully for other clinical causes of her symptoms and investigate if appropriate -if no other clinical cause is apparent, advise her to return to her GP if her symptoms become more frequent and/or persistent.
Cervical Cancer Cervical cancer — just below 3,000 new cervical cancers Since the 1990 reduction in cx ca cases by 25% 3/4ths are picked up with screening A full time GP is likely to diagnose one person with cervical cancer approximately every ten years
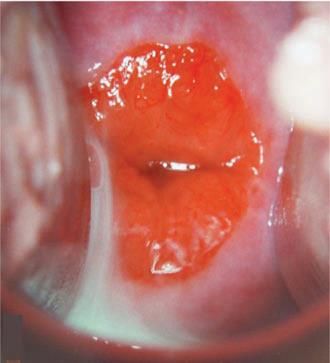
Suspicious Symptoms/and Signs (outside the screening framework) Persistent post coital bleeding Persistent intermenstrual bleeding Persistent contact bleeding Persistent foul smelling discharge> 6weeks Visible lesion or abnormal looking cervix Do not do a smear or be reassured by a smear in an abnormal looking cervix
Pause, think ?Premenopausal -IMB/PCB- Normal looking cervix Look for polyp, ectropion , warts Consider swabs/ Contraceptive change/smear if cx looks normal and not had a smear in line with guidelines Referral to Gyn/GU
19
20
21
22
25
Vulval/ Vaginal cancer Vulval cancers – Just over 1000 new vulval cancers A full time GP is likely to diagnose approximately one person with vulval cancer during their career Vaginal cancer- Just over 250 new vaginal cancers Most GPs will not encounter a woman with the disease during their career.
Recognition and referral Unexplained vulval lump, ulceration or bleeding In the vulva or vagina* *Familiarity with normal anatomy High risk factors -Age -Background of VIN/ Lichen sclerosus -Unremitting symptoms of vulval itching and soreness -Vulval symptoms not responding to diagnostic trail of treatment with steroids
Previous version of 2WW form
Proposed 2WW referral form
Evidence Rapid-access gynecological oncology clinic outcomes in North London, UK Bansal JK, Goldrick IG, Manchanda R, Olaitan A; 2017 Among 335 women referred to the RAC, 14 (4.2%) had cancer. Most women had benign pathology (80.6%). The same year, 13 cancers were diagnosed elsewhere, including in the emergency department. A total of 172 referrals did not fulfil the guidelines. Two week waits: What are we waiting for? Abdelraheim AR, Khairy M, Mohammed M, Lawrence A., 2017 The PP Vof referrals for diagnosing endometrial, ovarian, cervical and vulvo-vaginal malignancy was 8.1%, 9.5%, 5.98% and 13.64% and the overall predictive value for diagnosing gynaecological malignancy was 8.33%. The PPV of the 2WW referrals for diagnosis in premenopausal women are lower compared to postmenopausal women (1.86% and 9.89% respectively) Cancers diagnosed via non-urgent system was higher in comparison to 2WW (95 vs. 92%) Suggested incorporating risk factors to prioritise urgent appointments
Variation in use of the 2-week referral pathway for suspected cancer: A cross sectional analysis David Meechan, Carolynn Gildea, Louise Hollingworth, Mike A Richards, Di Riley and Greg Rubi, 2012 Examined use of the 2WW referral by GP practices in relation to all cancer diagnoses. Of all 2WW referrals, 11% resulted in a cancer diagnosis (conversion rate) Diagnoses resulting from 2WW referrals accounted for 43% of all first treatments for cancer recorded on the CWT database (detection rate). practices with higher conversion rates generally have higher detection rates and vice versa there is a consistent relationship between 2WW referral conversion rate and detection rate that can be interpreted as representing quality of clinical practice. Suggests the 2WW referral rate should not be a measure of quality of clinical care. Outcomes following implementation of symptom triggered diagnostic testing for ovarian cancer Nirmala Rai,James Nevin, Gabrielle Downey, Parveen Abedi, Moji Balogun, Sean Kehoe, Sudha Sundar; 2015 Secondary care received 2185 new referrals from primary care for women with suspected gynaecological cancer in post guideline cohort. Of these, 217 women were referred for suspected OC. 90% of primary care referrals were not compliant with guidance.
Patient and primary care delays in the diagnostic pathway of gynaecological cancers: a systematic review of influencing factors Pauline Williams, Peter Murchie and Christine Bond , 2019 Systematic narrative review evaluated Patient factors, Doctor factors and System factors identified certain specific factors that influence patient and primary care diagnostic delay and concluded Delayed diagnosis in the patient and primary care intervals of the diagnostic journey of gynaecological cancer is complex and multifactorial Differences in cancer awareness and beliefs between Australia, Canada, Denmark, Norway, Sweden and the UK (the International Cancer Benchmarking Partnership):do they contribute to differences in cancer survival? Forbes LJ, Simon AE, Warburton F, et al. 2013 UK had the ‘highest mean barriers to symptomatic presentation’, for example, embarrassment and worry about what the doctor might find, when compared with other high-income countries
Experience of symptoms indicative of gynaecological cancers in UK women E L Low, A E Simon, J Waller, J Wardle and U Menon , 2013 Noted occurrence of gynaecological symptoms potentially indicative of cancer in women in the UK is substantially higher than recorded in primary care. Just under half (44%) of the women in this study reported a symptom that may indicate a gynaecological cancer, and for a third (35%), the symptom was frequent and/or severe. 20% consulted GP for potential gynaecological cancer symptoms. Suggested targeting interventions towards older women who have a symptom that is frequent or severe could promote appropriate help-seeking without increasing consultations with the ‘worried well’. Intention-Behaviour Relations: A Conceptual and Empirical Review Paschal Sheeran , 2002 A study exploring health seeking behaviour estimates relation between intention-behaviour consistency of patients and explores related factors notes the “gap” between intentions and behaviour is significant and intention is not translated into behaviour.
Barriers summary information overload low awareness of practioners/patients Low incentives and inertia Acceptance and beliefs of primary care practioners/patients Organisational constraints Conflicting messages Secondary care attitude
Waiting Times for Suspected and Diagnosed Cancer Patients 2019-20 Annual Report Prepared by Joshua Richardson, Ana Rita Ubaldo, David Dai and Paul McDonnell A summary report* of the statistics on Waiting Times for Suspected and Diagnosed Cancer Patients within the English NHS for the period 2018-19 shows 213,773 patients were seen for Suspected Gynaecological Cancer 93.3% of patients seen within 14 days *an aggregate version of the provider-based revised final statistics available on the NHS England website https://www.england.nhs.uk/statistics/statistical-work-areas/cancer-waiting-times/
Effect of delays in the 2-week-wait cancer referral pathway during the
COVID-19 pandemic on cancer survival in the UK: a modelling study
Amit Sud et al August 2020
During the COVID-19 lockdown, referrals via the 2-week-wait urgent pathway for suspected
cancer in England, UK, are reported to have decreased by up to 84%.
In this modelling study, age-stratified and stage-stratified 10-year cancer survival was
estimated for patients in England .
Thee aggregate number of lives and life-years lost in England were estimated for per-
patient delays of 1–6 months in presentation, diagnosis, or cancer treatment, or a
combination of these for three scenarios of a 3-month period of lockdown during which
25%, 50%, and 75% of the normal monthly volumes of symptomatic patients delayed their
presentation until after lockdown.
Delays in presentation via the 2-week-wait pathway over a 3-month lockdown period (with
an average presentational delay of 2 months per patient) would result in 181 additional lives
and 3316 life-years lost as a result of a backlog of referrals of 25%, 361 additional lives and
6632 life-years lost for a 50% backlog of referrals, and 542 additional lives and 9948 life-
years lost for a 75% backlog in referrals.
Cancer Age group (years)
type 30-39 40-49 50-59 60-69 70-79 >80
Reduction in 10-
year net survival
incurred from a
Uterus 2·43% 2·43% 6·04% 8·68% 11·83% 14·43%
3-month delay
for the tumour
types, by age Ovary 7·24% 13·87% 17·38% 18·28% 17·08% 15·86%
group
Cervix 5·59% 9·03% 12·20% 15·73% 17·98% 15·52%Talking points
You can also read