MENTAL HEALTH PAYMENT BY RESULTS (PBR) - MARK RIDGE HEAD OF PBR
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Mental Health Payment by Results (PbR) Mark Ridge Head of PbR

• Payment by Results – money follows the patient • Commissioners pay providers for each patient seen / treated • Takes into account the complexity • Promotes efficiency • Supports patient choice • Increasingly incentivises for best practice

PbR In general healthcare • 1400+ separate types of activity • 40-50% of many hospital’s total income • £29 billion • ~¼ of total NHS budget • boosted activity: more for more • reduced lengths of stay • encouraged more day-cases vs. inpatient-work

• Payment-by-Results (PbR) for Mental Health is being introduced by the Department of Health to support funding for mental health services in the future. • It is an extension of the system that is in place across the acute sector but differs in many ways. • It focuses on a method of assessing need using an extension of the Health of the Nation Outcome Scales (HoNOS) • Mental Health Clustering Tool (MHCT), repeated at regular intervals

MH PbR will be underpinned by quality and outcome standards Payment is in three parts: 1. For the initial assessment 2. Each day a service user is in the service from assessment to discharge 3. For a achieving ‘successful’ quality and outcomes

Mental Health PbR Applies to adult and older peoples services in hospital and community There are versions for Learning Disabilities Services, Child and Adolescent Mental Health Services and Secure Care which are all in various stages of development

Mental Health Care Clusters Clustering is a method of undertaking a detailed assessment of the needs of each patient and then using the results of this assessment to allocate them to a needs-based “cluster” Clusters will be used as the national currency for Payment by Results (PbR) in Mental Health. They are a way of classifying service users that is intended to form the basis for payment, and are assigned using a care cluster decision tree

Non-
Psychotic
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
The current Care Clusters
The Care Clusters for Mental Health Payment by Results
Cluster 1 Common Mental Health Problems (Low Severity)
Cluster 2 Common Mental Health Problems (Low Severity with greater need)
Cluster 3 Non-Psychotic (Moderate Severity)
Cluster 4 Non-Psychotic (Severe)
Cluster 5 Non-Psychotic Disorders (Very Severe)
Cluster 6 Non-Psychotic Disorder of Over-valued Ideas
Cluster 7 Enduring Non-Psychotic Disorders (High Disability)
Cluster 8 Non-Psychotic Chaotic and Challenging Disorders
Cluster 9 Blank cluster
Cluster 10 First Episode Psychosis
Cluster 11 Ongoing or recurrent Psychosis (Low symptoms)
Cluster 12 Ongoing or recurrent Psychosis (High Disability)
Cluster 13 Ongoing or recurrent Psychosis (High Symptoms and Disability)
Cluster 14 Psychotic Crisis
Cluster 15 Severe Psychotic Depression
Cluster 16 Dual Diagnosis
Cluster 17 Psychosis and Affective Disorder - Difficult to Engage
Cluster 18 Cognitive Impairment (low need)
Cluster 19 Cognitive Impairment or Dementia Complicated (Moderate Need)
Cluster 20 Cognitive Impairment or Dementia Complicated (High Need)
Cluster 21 Cognitive Impairment or Dementia (High Physical or Engagement)
Following assessment the patient is directed to a service that is able to provide the appropriate package of care to meet the needs identified. These packages of care are the Clusters.
A patient with severe
Example psychotic symptoms and
unstable, chaotic lifestyle,
vulnerable & engages poorly,
may benefit from a care
package consisting of:
Assertive Outreach,
Substance misuse support,
Physical care monitoring,
Care coordination- multi-
agency referral
Possibly Mental Health ActThis care package is found in Cluster 17 and is most likely delivered in the following settings: Recovery Team Assertive Outreach Team Substance Misused Services Social Care Out Patient Clinics In-Patient Medical Home Visits Carer support
If a person has a crisis and requires admission or Home treatment they may transition into Cluster 14 or 15 for a temporary period before recommencing their care package in Cluster 17
Transition Step up
Cluster 14
Cluster 15
Cluster 16
Intervention
Package Little change
remain in Cluster
Assertive Outreach
17
Cluster 17 Dual Diagnosis
Initial Transition Step
Assessment - Psychosis Physical Care
Monitoring Down
HoNOS & On-going or Cluster 11
Cluster Recurrent Assertive Outreach
Cluster 12
Care Coordination Cluster 13
Multi Agency Referral
(Mental Health Act Unlikely Transition
e.g. CTO) Clusters 6, 7, 8 & 18
Rare Transition
Clusters 1, 2, 3, 4, 5,
10 19, 20 & 21Choosing the appropriate cluster Folio goes here
Assessment
In addition to the initial standard MH
assessment we also complete the
Mental Health Clustering Tool
comprising:
• Part 1HoNOS working age adults
score
• Part 2 Historical ScaleHoNOS PbR HoNOS PbR applies to adult and older peoples services It Comprises: HoNOS working age adults score and the Clustering Tool, which is the historical perspective
HoNOS is…..
A set of 12 scales with a 5-point rating scale which are
completed in
a few minutes by mental health professionals after routine
clinical assessment, CPA reviews etc
The scales:
• Are designed for use in any setting in secondary mental
health care services
• Are based on a rating of the worst symptoms/problems
within a specified time period
• Provide a numerical record of the clinical assessment
• Are ratings of mental health outcome, not health care
outcomes
The total score is used to measure health outcome. The MHCT is
all 18 Scales (1-13 then scales A-E). The score profile generated
at assessment is used to allocate to a Care Cluster.
© Royal College of Psychiatrists, 2010
6The MHCT
PART 1 (CURRENT SCALES)
SCALE SCALE DESCRIPTION
1 Overactive, aggressive, disruptive or agitated behaviour
2 Non-accidental self-injury
3 Problem drinking or drug-taking
4 Cognitive problems
5 Physical illness or disability problems
6 Problems with hallucinations & delusions
7 Problems with depressed mood
8 Other mental & behavioural problems
Please specify which problem- A – B – C – D – E – F – G – H - I or J,
NB if you choose ‘J’ (other problem then please specify the problem)
9 Problems with relationships
10 Problems with activities of daily living
11 Problems with living conditions
12 Problems with occupation & activities
TOTAL HoNOS SCORE FOR OUTCOME MEASUREMENT
13 Strong Unreasonable Beliefs occurring in non-psychotic disorders only
PART 2 (HISTORICAL SCALES)
SCALE SCALE DESCRIPTION
A Agitated behaviour/expansive mood (historical)
B Repeat self-harm (historical)
C Safeguarding children & vulnerable dependent adults (historic)
D Engagement (historical)
E Vulnerability (historical)
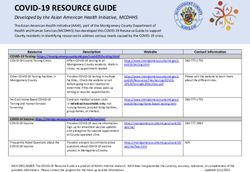
1Care Cluster 19: Cognitive Impairment or Dementia
Complicated (Moderate Need)
CARE CLUSTER 19: Cognitive Impairment or Dementia Complicated (Moderate Need)
Description Severity Score
No Item Description
0 1 2 3 4
People who have problems with their memory and / Current scales
or other aspects of cognitive functioning resulting in
1 Overactive, aggressive, disruptive or agitated behaviour
moderate problems looking after themselves and
2 Non - accidental self injury
maintaining social relationships. Probable risk of self-
neglect or harm to others and may be experiencing 3 Problem drinking or drug taking
some anxiety or depression. 4 Cognitive problems
5 Physical illness or disability problems
Diagnoses 6 Problems associated with hallucinations and delusions
Diagnoses likely to include F00-Dementia in 7 Problems with depressed mood *
Alzheimer's disease, F01 - vascular dementia, F02 - 8 Other mental and behavioural problems *
Dementia in other diseases classified elsewhere, F03 - 9 Problems with relationships
Unspecified Dementia, F09 - unspecified organic or 10 Problems with activities of daily living
symptomatic mental disoder, Dementia with Lewy 11 Problems with living conditions
bodies (DLB), Frontotemporal dementia (FTD)
12 Problems with occupation and activities
Impairment 13 Strong unreasonable beliefs
Impairment of ADL and some difficulty with Historic scales
communication and in fulfilling social and family A Agitated behavior / expansive mood
roles B Repeat self - harm
C Safeguarding children and vulnerable dependant adults
Risk D Engagement
E Vulnerability
Risk of self neglect, harm to self or others. May lack
awarness of problems. Must score
Expected to score
Course May score
Unlikely to score
Long term
Not used for clustering
* Either / OrOn completion of an initial assessment
a patient would be:
• Clustered - Only if the Trust is able
to offer the appropriate intervention
or
• Not clustered and discharged, or
signposted to alternative services.Assessment AA : Referred back to
GP/Primary Care
outcome options AB : Referred to DHCFT IAPT
AC : Referred to DHCFT
Assessed Not CAMHS
Clustered AD : Referred to DHCFT
Learning Disabilities
AE: Referred to DHCFT
Substance Misuse
Initial Assessed and AF: Referred to DHCFT
Assessment Clustered 4 - 21 Forensic/Low Secure
AG: Referred to Other
Discuss with:
Assessed and Clinical Director,
Clustered 1 – 3 Service Line Manager
or Service ManagerA patient would not be re-clustered on the basis of individual interventions, but only for complete care packages.
A patient would not be re-clustered on the basis of improvement or deterioration within a care package, unless there was need for a completely new care package, such as a Crisis Intervention
Quality Each Cluster has: • A definition of the relevant needs to be met • Information about the most appropriate treatment with references to NICE • A set of other tools to help with any specialist assessment needed • Information about how care win the cluster will be evaluated (outcomes) • A designated maximum review period ranging fro 4 week to a year Outcomes in each cluster will be measured. 4 outcomes: 2 clinician rated, 1 patient rated and 1 patient rated experience measure
2013 - 2014 Success of treatment evaluated using 4 measures: • 2 Clinician rated outcome measures (CROMS) HoNOS plus one other • 1 Patient rated outcome measure (PROM) • 1 Patient rated experience measure (PREM) To evaluate to what extent the clinical objectives outlined in the Care Plan were achieved Folio goes here
Service Objectives
Specialist skills
development
A
S
S Improved Patient
Information
E
S
S Service
M Benchmarking
E
N Improved Outcome
T Prediction
Improved Patient
SatisfactionAny Questions
You can also read