Harm Reduction in the Hospital: Preventing AMA Discharges and ED Bounce Backs - CAEP Conference
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Harm Reduction in the Hospital:
Preventing AMA Discharges and
ED Bounce Backs
Kathryn Dong MD, MSc, FRCP, DABAM
Director, Inner City Health and Wellness Program, Royal Alexandra Hospital
Associate Clinical Professor, Department of Emergency Medicine, University of Alberta
Faculty/Presenter Disclosure
Faculty: Kathryn Dong
Relationships with financial sponsors:
• Grants/Research Support: Royal Alexandra Hospital Foundation, Canadian Research
Initiative in Substance Misuse (CRISM), Edmonton Emergency Physicians Association
(EEPA), AHS Emergency Medicine Strategic Clinical Network
• Speakers Bureau/Honoraria: Canadian Institute for Health Research (CIHR), College of
Physicians and Surgeons of Alberta (CPSA), Covenant Health
• Consulting Fees: None
• Patents: None
• Other: Employee of Alberta Health Services (AHS)
Disclosure of Financial Support
The Addiction Recovery and Community Health (ARCH) Team has
received financial support from:
Royal Alexandra Hospital Foundation
Alberta Health Services
Alberta Health
I receive an administrative salary from Alberta Health Services.
Potential for conflict(s) of interest: • Speaker has not received an honorarium from CAEP • No sponsoring organization benefits from the sale of a product that may be discussed in this program

Mitigating Potential Bias None to declare.

HOSPITALS ARE HIGH RISK ENVIRONMENTS FOR PEOPLE WHO USE DRUGS

Drug Use in Hospital
• Contributes to patients leaving
against medical advice
• Leads to costly readmissions
• Patients unable to be abstinent
should not be penalized at the
expense of their health
Drug Use in Hospital
• 44% of people who were using drugs
prior to hospitalization continued to use
drugs while in hospital
• Drugs were most commonly used in
patient washrooms
• “Harm reduction programs (e.g. needle
syringe distribution programs and
supervised drug consumption facilities)
should be implemented in hospital
settings.”
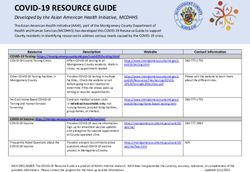
Against Medical Advice
• Patients who leave AMA are
12x more likely to be
readmitted within 14 days
• Doubles the risk of death
• Prevalence of AMA discharge
is 25-30% among people who
inject drugs
Hospitals Are High Risk “A key finding of this study is that patients who use illicit substances characterize the health care system as unsafe…"
Hospitals Are High Risk
Abstinence only policies, inadequate
pain & withdrawal management,
negative stereotypes
Inability to practice harm reduction,
involuntary discharge
Increased morbidity and mortality
McNeil R et al. “Hospitals as a ‘risk environment’: An ethno-epidemiological study of voluntary and involuntary
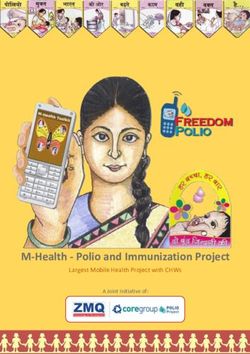
discharge from hospital against medical advice among people who inject drugs” Social Science & Medicine 105: 59-66.ED Presentations are Increasing Canadian Institute for Health Information. “Opioid-Related Harms in Canada” Chartbook, September 2017 https://www.cihi.ca/sites/default/files/document/opioid-harms-chart-book-en.pdf
Alcohol
“And while the opioid
crisis gripping many
provinces continues to
grab headlines, experts
warn that a looming
alcohol health crisis
should not be ignored.”
Canadian Institute for Health Information. “Alcohol Harm in Canada: Examining Hospitalizations Entirely Caused by
Alcohol and Strategies to Reduce Alcohol Harm” Ottawa, ON: CIHI; 2017.A FOCUS ON REDUCING HARM IS EVIDENCE-BASED AND ETHICAL.
Harm Reduction in Hospitals
• Focusing on reducing harm may be a more effective way of
managing substance use in acute care settings
• When abstinence is not possible, it is not ethical to ignore
other available means of reducing suffering
• It should not be easier to access evidence-based health
interventions in the community than in the hospital
Pauly B “Shifting moral values to enhance access to health care: Harm reduction as a context for ethical nursing
practice” International Journal of Drug Policy 19: 195-204.Royal Alexandra Hospital
Addiction Recovery and Community
Health (ARCH) Team
• Standardized intake and assessment procedure
• Comprehensive, evidence-based addiction management
• Interventions to Maximize Social Determinants of Health
– Housing, Income supports, ID
• Health Promotion
– STBBI screening, PAP smears, immunizations, fertility management
• Linkage to community and primary care directly from acute care or
via a Transitional ClinicARCH Team
• Comprehensive, evidence-based addiction management
– Treatment of complicated intoxication and/or withdrawal
– Initiation or maintenance of opioid agonist treatment
– Harm reduction including sterile injection equipment, overdose response
kits, supervised consumption
– Managed alcohol program
– Counseling, motivational interviewing, relapse prevention, treatment
referrals
– Identification and referral for co-morbid mental health conditionsARCH Team • Physicians • Nurse Practitioners • Social Workers • Peer Support Workers • Addiction Counsellors • Pharmacist • RNs / LPNs
Syringe Exchange
• Evidence is “overwhelming” that
syringe exchange programs
substantially reduce HIV rates
• Cost effective
• Can increase recruitment into drug
treatment and possibly into
primary health care
World Health Organization. “Effectiveness of Sterile Needle and Syringe Programming in Reducing HIV/AIDS Among
Injecting Drug Users” Geneva: WHO; 2004.Syringe Exchange
Patient M
• I: What do you think about our hospital
having a needle exchange program?
• P: I think that’s great.
• I: Why do you think it’s great?
• P: So, people don’t get infection when
they’re in the hospital. You’re trying to get
better when you come to the hospital so
having a needle exchange takes away
the risk for having another, or making it
worse.Syringe Exchange
Patient H
• I: What did you think when you first heard
about our needle exchange program?
• P: Oh, I wanted to come here when I got
sick. Told a few friends about it. Yeah.
• I: Do you think having a needle exchange
program here, does it make it?
• P: Easier, way easier. Yeah.
• I: It makes it easier to come here?
• P: Oh yeah. Yeah. Mm-hm. Very easy.Managed Alcohol Programs • Participants drank more days, but significantly fewer drinks per drinking day • Significantly reduced alcohol-related harms in the domains of health, safety, social, legal and withdrawal
Managed Alcohol Programs • Patient eligibility • Patients have to sign a ‘Patient Agreement’ • Assessed for intoxication prior to each dose
Supervised Consumption Services “Participants singled out hospital-based supervised drug consumption services as having the greatest potential to enable them to complete hospital treatment despite continued drug use.”
Supervised Consumption Services
Supervised Consumption Services
P: They should have a place to do it there. Especially if they’re
giving the supplies, they might as well supply a safe place. –
Patient Q
P: Yeah, it’s a little bit awkward, don’t want to get caught,
security guards, they’ll only let you stay in the bathroom for so
long and then they’ll come knocking on the door. Like why are
you taking so long, right. – Patient R
P: if you feel rushed you end up getting more and more
frustrated. And then if you draw blood, these things going to
gel up in you … I sometimes go there [to McDonald’s across
the street] and there’s a big line up ... when I’m in there … I
start hurrying, hurrying, missing. – Patient U
P: A lot of them can say they don’t care but I know that’s a lie.
Of course, we all care and of course it would be, if I was in
there and got caught sticking a needle in my arm and what
would happen is they would probably change my meds. –
Patient NSupervised Consumption Service • For inpatients only • Risks, benefits, alternatives and consequences of using the service are discussed • Patients sign: – Patient agreement – Consent form • Injection, intra-nasal and oral use are permitted
Supervised Consumption Service
Key Points
• Hospitals are high risk environments for people who use drugs
• A focus on reducing harm is evidence-based and ethical
• Syringe exchange, managed alcohol programs and supervised
consumption services have the potential to reduce AMA discharges
and the harms associated with ongoing drug and alcohol use in
hospital settingsThank you!
You can also read