Greece Country Health Profile - State of Health in the EU Conference on the Future of Healthcare in Greece, Athens, 22 March 2018 - OECD.org
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

State of Health in the EU Greece Country Health Profile Conference on the Future of Healthcare in Greece, Athens, 22 March 2018

1 Country Health Profiles 1. Highlights 2. Health status of the population 3. Risk Factors 4. Health System (description) 5. Performance of Health System 5.1 Effectiveness 5.2 Accessibility 5.3 Resilience (efficiency & sustainability) 6. Key Findings Released in November 2017 (in English and native language) This presentation focuses on sections highlighted in bold

What are the trends in the health status
of the population in Greece?
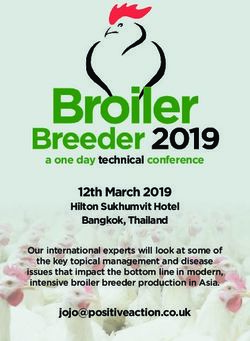
Life expectancy in Greece has increased less rapidly than in many other EU countries
Only ½ year higher now than EU average, 2 years lower than in Spain and Italy
Yea rs
Spain Greece EU
84
82
80
Yea rs (in 2015)
84
83.0 78
82.7
82.4 82.4 82.2
81.9 81.8
82 81.6 81.6 81.5 76
81.3 81.3 81.1 81.1
81.0 80.9 80.8
80.7 80.6
74
80
78.7 72
78.0
78 77.5 77.5 70
76.7
75.7
76
75.0 74.8
74.7 74.6
74
72
70
Source: Eurostat Database.People live longer, but less than half of remaining years of life at age 65
is free of health problem and disability
Healthy life expectancy Unhealthy life expectancy Number of working-age people (15-64) per person aged 65+
Greek men at 65 7.9 10.6 18.5
Greek women at 65 7.5 13.8 21.3
0 5 10 15 20 25
Years
Note: Healthy life expectancy: Number of years that people can expect to live free of disability.
Source: Eurostat Database (data refer to 2015).
Population ageing will increase the needs for health and long-term care,
while there will be fewer working-age people to respond to these needsHow to ensure universal access to
health care in a context of population
ageing, now and in the future?
(Access = Affordability + Accessibility to services)The 2016 Law to provide minimum public health insurance coverage for all the
population has been an important step towards universal health coverage
Before, 2016, Greece was lagging behind nearly all And a growing proportion of poor people was
EU countries in health insurance coverage… reporting unmet health care needs due to cost
Total public coverage Primary private health coverage
Croatia 100.0
Czech Republic 100.0
Denmark 100.0
% of population Poorest income quintile
Finland 100.0 20
Ireland 100.0 Richest income quintile 17.4
Italy 100.0 18 16.4
Latvia 100.0
Lithuania 100.0 16
Malta 100.0 13.9
Portugal 100.0
14
Slovenia 100.0
Sweden 100.0 11
12 10.1
United Kingdom 100.0
Austria 99.9
10
France
8.4
99.9 7.8
Spain 99.1 0.8 7
8
Germany 88.9 10.9
Netherlands 99.8
Belgium 99.0
6
Luxembourg 95.9 3.3 2.8
Hungary 95.0
4 2.2
Slovak Republic 94.2 0.9 0.6 0.8
Estonia 93.9
2 0.2 0
Poland 91.3
Bulgaria (2013) 88.2
0
Romania 86.0 2008 2009 2010 2011 2012 2013 2014 2015
Greece (2015) 86.0
Cyprus (2013) 83.0
70 80 90 100
% of population in 2015
Source: OECD (Health a t a Glance: Europe 2016). Source: Eurostat (EU-SILC).But it is also important to consider the comprehensiveness of health
insurance coverage: what is covered and what proportion is covered?
Only about 60% of health spending in Greece is
publicly funded, compared with about 80% in the EU
Source: OECD Health Statistics (data refer to 2015).Effective access to care also needs to address other barriers beyond coverage
Many Greek people report having difficulties accessing doctors or a health centre not only because of cost,
but also because of distance to the doctor’s office and waitings to get an appointment and see a doctor
Italy Spain EU Portugal Greece
Distance to doctor’s
office 0% 20% 40% 60%
Spain EU Italy Portugal Greece
Cost of seeing doctor
0% 20% 40% 60%
Spain Italy EU Portugal Greece
Delay in getting
appointment 0% 20% 40% 60%
Italy Spain EU Portugal Greece
Waiting time to see a
doctor on the day 0% 20% 40% 60%
Response to the question: “Thinking about the last time you needed to see or be treated by a GP, family doctor or health centre, to what extent
did any of the following make it difficult or not for you to do so?” (% of respondents answering “very difficult” or “a little difficult”).
Source: Eurofound (European Quality of Life Survey 2016).The main problem is not a lack of doctors, but a lack of generalists, the uneven
geographic distribution of doctors, and the lack of doctors in public facilities
Generalists,
6%
Other doctors
(not defined),
19%
Specialists,
75%
Greece
Note: In Portugal and Greece, data refer to all doctors licensed to practice, resulting in a large over-estimation of practising doctors (e.g. of around 30% in Portugal).
In Austria and Greece, the number of nurses is under-estimated as it only includes those w orking in hospital.
Sources: Eurostat Database and Health at a Glance 2017.Primary Care Plan launched in 2017 is another step in the right direction
• Creating an effective network of primary care services is one of the most urgent
priorities to respond effectively to the needs of (ageing) population and reduce
over-crowding of emergency departments and unnecessary hospital admissions
• Other EU countries can provide some inspiration to strengthen primary care:
• Portugal: Since 2007, a growing number of Family Health Units based on multi-
professional teams (with 3-8 GPs and same number of nurses) responsible for
delivering primary care to around 12000 people each (about 500 FHUs now)
• But there is probably “no one fits all” solution, and various primary care
models probably need to coexist and continue to evolve over time
• The success of the primary care reform in Greece will likely depend on:
Having sufficient financial resources to support creation and development
Supporting innovative ways to deliver services effectively (e.g. telemedecine)
Coordinating effectively the various primary care units (regional authorities)Universal and fairly comprehensive health coverage can be fiscally
sustainable in Greece, provided that…
Efforts continue to reduce waste in health spending to ensure
that resources are used effectively to respond to changing needs
and ensure continued support for publicly-funded system
The revenue base to finance public spending on health is
broadened to rely less on payroll taxes to raise sufficient
resources to meet future needsWasteful spending can occur at all levels of the system for many reasons
Patient
Ineffective/inappropriate (low value) care
Wasteful
Duplication of services
clinical care
Preventable adverse events
Clinician
Actors
Paying an excessive price
Discarding unused inputs Operational waste
Manager Overusing high-cost inputs (e.g. hospitals)
Governance-related
Ineffective administrative procedures
waste
Regulator and expenditure
Errors & poor Poor Poor Fraud and
Drivers
decisions organisation incentives corruption
Source: OECD, Tackling Wasteful Spending on Health.
Unintentional IntentionalDespite many recent efforts to reduce hospital and pharmaceutical cost, most health
spending in Greece continues to be allocated for these two big spending items
%
Inpatient care Outpatient care Long-term care Medical goods Collective services
100 4
5 8 6 7 5 5
9
90 12
20
21 19 14 22
28 20
80
2
70 18 9 26
10 15
2 12
A relatively small share of 60
spending is allocated to
25
outpatient care and long- 50
26 31
48
30 30 38
term care 40 34
30
20 40
33 32 30 29 26 26
10 23
0
Note: Countries are ranked by inpatient care as a share of health expenditure .
Source: OECD Health Statistics 2017 and Eurostat Database (data refer to 2015).A lot of efforts have been made in recent years to reduce pharmaceutical spending
Introduction of prescription guidelines,
coupled with country-wide prescription
system to monitor doctors’ prescribing and
Million (€) pharmacies’ dispensing
Introduction of reference pricing for
7 000 branded drugs based on the three lowest
EU prices and setting a maximum pricing
6 000
level for generics
5 000 Promoting use of generics in pharmacies and
4 000
hospitals (although there is still room for
further progress)
3 000
2 000 Share of generic market (in volume, 2015)
1 000 %
100
0
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 75
50
25
0
Note: The dotted line between 2007 and 2009 indicates estimates to fill missing data.
Source: OECD Health Statistics 2017.Broadening the revenue base to pay for growing public spending on health
• Payroll taxes have historically been the main source of public funding
in social health insurance systems, but:
Rationale to rely on employee and employer contributions is reduced when
health insurance coverage becomes universal (not linked to employment status)
Excessive reliance on payroll taxes reduces incentives for people to work and
employers to recruit (negative impact on employment)
May not provide sufficient revenue base to respond to future health care needs
given demographic changes (shrinking size of working-age population)
• In France, recent tax reform (since 1 January 2018) eliminated employee
contributions for health care and replaced it by increase in a more general
taxation covering broader revenue sources (capital gains, pensions, others)
• But tax reforms are never easy to implement (there are “winners” and “losers”)Key Findings from Greek Country Health Profile
• Life expectancy has continued to increase in Greece, but population ageing
will continue to add pressures on health and long-term care systems
• Despite difficult economic and budgetary context, recent important
reforms have started to address many barriers to access to care:
The 2016 Law has been an important step forward to provide minimum health
insurance coverage to previously uninsured people
The 2017 Primary Care plan has started to address an urgent priority to
strengthen access to primary care, but successful implementation will require
sufficient funding over several years and innovative ways to deliver primary care
services efficiently for the whole population
• Looking forward, universal and fairly comprehensive health coverage can be
financially sustainable, provided that efforts continue to be made to reduce
wasteful health spending and the revenue base to finance public spending
on health continues to be broadenedFor more information on State of Health in the EU
ec.europa.eu/health/state
oecd.org/health/health-systems/country-health-profiles-EU.htm
euro.who.int/en/about-us/partners/observatory/publications/country-health-profiles-EUYou can also read