Mediterranean Diet, Stroke, Cognitive Impairment, and Depression: A Meta-Analysis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ORIGINAL ARTICLE
Mediterranean Diet, Stroke, Cognitive
Impairment, and Depression:
A Meta-Analysis
Theodora Psaltopoulou, PhD,1 Theodoros N. Sergentanis, MD,1
Demosthenes B. Panagiotakos, PhD,2 Ioannis N. Sergentanis, MD,1,3
Rena Kosti, PhD,1 and Nikolaos Scarmeas, MD, MSc, PhD4,5
Objective: This meta-analysis aims to quantitatively synthesize all studies that examine the association between
adherence to a Mediterranean diet and risk of stroke, depression, cognitive impairment, and Parkinson disease.
Methods: Potentially eligible publications were those providing effect estimates of relative risk (RR) for the associa-
tion between Mediterranean diet and the aforementioned outcomes. Studies were sought in PubMed up to October
31, 2012. Maximally adjusted effect estimates were extracted; separate analyses were performed for high and mod-
erate adherence.
Results: Twenty-two eligible studies were included (11 covered stroke, 9 covered depression, and 8 covered cogni-
tive impairment; only 1 pertained to Parkinson’s disease). High adherence to Mediterranean diet was consistently
associated with reduced risk for stroke (RR 5 0.71, 95% confidence interval [CI] 5 0.57–0.89), depression (RR 5 0.68,
95% CI 5 0.54–0.86), and cognitive impairment (RR 5 0.60, 95% CI 5 0.43–0.83). Moderate adherence was similarly
associated with reduced risk for depression and cognitive impairment, whereas the protective trend concerning
stroke was only marginal. Subgroup analyses highlighted the protective actions of high adherence in terms of
reduced risk for ischemic stroke, mild cognitive impairment, dementia, and particularly Alzheimer disease. Meta-
regression analysis indicated that the protective effects of Mediterranean diet in stroke prevention seemed more
sizeable among males. Concerning depression, the protective effects of high adherence seemed independent of
age, whereas the favorable actions of moderate adherence seemed to fade away with more advanced age.
Interpretation: Adherence to a Mediterranean diet may contribute to the prevention of a series of brain diseases;
this may be of special value given the aging of Western societies.
ANN NEUROL 2013;74:580–591
“A ctive” aging and “healthy” aging are among
Western societies’ public health priorities, with
primary prevention playing a critical role. Maintaining
cognitive decline, reduced risk of progression from mild
cognitive impairment (MCI) to Alzheimer disease (AD),
lower risk of AD, and reduced crude mortality in AD
cognitive health in the elderly, as well as avoiding patients.1–3 In addition, adherence to a Mediterranean
brain vascular diseases and affective disorders, is a vital diet, as well as to DASH (Dietary Approaches to Stop
part of their well-being; otherwise, a heavy personal, Hypertension) and other prudent dietary patterns, seems
familial, public health, financial, and societal burden to protect from stroke, as food groups such as fish
emerges. intake, fruits and vegetables, and moderate alcohol intake
Prospective studies have provided evidence for a characterize this dietary pattern, too.4 The prevalence of
favorable relation of Mediterranean-type diet with slower affective disorders such as depression is increasing in
View this article online at wileyonlinelibrary.com. DOI: 10.1002/ana.23944
Received Mar 8, 2013, and in revised form May 8, 2013. Accepted for publication May 17, 2013.
Address correspondence to Dr Psaltopoulou, Department of Hygiene, Epidemiology, and Medical Statistics, School of Medicine, University of Athens,
75 M. Asias Str, Goudi 11527, Athens, Greece. E-mail: tpsaltop@med.uoa.gr
From the 1Department of Hygiene, Epidemiology, and Medical Statistics, University of Athens School of Medicine, Athens, Greece; 2Department of
Nutrition and Dietetics, Harokopio University, Athens, Greece; 3Hospital of Psychiatry, University Hospitals of Geneva, Geneva, Switzerland; 4Department
of Neurology, University of Athens Medical School, Athens, Greece; and 5Department of Neurology, Columbia University, New York, NY.
Additional Supporting Information can be found in the online version of this article.
580 V
C 2013 American Neurological Association
Psaltopoulou et al: Mediterranean Diet: Annals of Neurology
older age groups, and omega-3 intake is a promising fac- critical questions, such as whether the results are general-
tor for nonpharmacological treatment.5 izable in non-Mediterranean countries, the effect of the
Mediterranean diet has heterogeneous characteristics Mediterranean diet scale used, and the difference in out-
among countries residing in the Mediterranean basin.6 come when moderate as opposed to high adherence to
Precise definition, including appropriate characterization Mediterranean diet is followed.
of the food items or food groups and reference to its
macronutrient composition, as well as quantitative mea- Subjects and Methods
surement of its adherence, varies between studies,7 but in Search Strategy and Eligibility of Studies
general it is characterized by high intake of vegetables, This meta-analysis was performed in accordance with the
fruits, cereals, pulses, nuts, and seeds; moderate con- MOOSE (Meta-analysis Of Observational Studies in Epidemi-
sumption of dairy products, fish, poultry, eggs, and ology) guidelines.24 Eligible studies were sought in PubMed
unsaturated fats, such as olive oil as the primary source without any restriction of publication language; end-of-search
of monounsaturated fat for cooking and dressing; low to date was October 31, 2012. The details regarding search algo-
moderate intake of wine during meals; and low intake of rithm, eligibility criteria, and data extraction are provided in
the online-only Supplementary Methods.
red, processed meats and saturated fats.7,8 Mediterranean
diet is characterized as a healthy dietary pattern among
Statistical Analyses, Study Quality, Risk of Bias,
others, characterized by the United Nations as an intan- and Meta-Regression Analyses
gible cultural heritage of humanity,9 and related to a bet- Given that adherence to Mediterranean diet was quantified by
ter overall survival, as well as cardiovascular and cancer means of a variety of scores, a conceptual framework had to be
prevention,8,10 leading to a reduction of premature mor- constructed regarding the definitions of low, medium, and high
tality among middle-aged adults.11 adherence. To this end, the framework was principally based on
The protective role of Mediterranean diet in the the seminal work by Trichopoulou et al, according to whom a
ageing process could be multidimensional, encompassing scale of 0 to 9 represents the whole continuum of adherence,
anti-inflammatory functions,12 and protection from oxi- with low, medium, and high adherence levels corresponding to
dative stress13 and atherothrombosis,14 potentially by values of 0 to 3, 4 to 5, and 6 to 9.8 In light of this, the vari-
modulating the expression of proatherogenic genes.15 ous scores were proportionally converted to the 0 to 9 range,
and the midpoint of each exposure category was qualified as
Favorable results in cardiovascular risk factors have also
low when it fell within the 0 to 3 region, medium within the 4
been observed, such as reduction in total and low-density
to 5 region (ie, 3.5–5.4 prior to numerical rounding), and high
lipoprotein cholesterol as well as increase in high-density within the 6 to 9 region (ie, 5.5–9 prior to numerical round-
lipoprotein cholesterol levels,16 lower blood pressure,17 ing), respectively. For instance, the fairly frequent 0 to 29, 30
and protective association with metabolic syndrome,18 to 33, and 34 to 55 categories of the 0 to 55 score by Panagio-
and possibly with diabetes mellitus19 and obesity.20 takos et al25 represented low, medium, and high adherence, as
Among a multitude of suggested mechanisms, alterations their midpoints were equal to 2.37, 5.15, and 7.28 on the 0 to
in levels of biochemical mediators such as homocys- 9 scale, respectively. The conversion was deemed necessary, so
teine21 and adiponectin22 and improvement in endothe- as to maximize the statistical power of the quantitative synthe-
lial function and regenerative capacity23 have been sis; nevertheless, subanalyses by the type of score were always
named. performed, so that the reproducibility of the findings among
Data have accumulated from prospective, case–con- the various questionnaires could be examined.
trol, and cross-sectional studies concerning the relation Statistical analyses included pooling of studies at 2 sepa-
rate levels (high vs low adherence; moderate vs low adherence).
between adherence to Mediterranean diet and risk of
Random effects (DerSimonian–Laird) models were appropri-
stroke, cognitive impairment, depression, and Parkinson
ately used to calculate pooled effect estimates. Between-study
disease in the adult population. Several years after the heterogeneity was assessed through Cochran Q statistic and by
last quantitative synthesis,10 when only 4 papers were estimating I2.26 Details about subgroup analyses, assessment of
available in the field, the current number exceeds 20 study quality, evaluation of publication bias, alternative analy-
published studies. The scope of the present meta-analysis ses, and meta-regression analysis are provided in the online-only
is to quantitatively synthesize relevant literature, taking Supplementary Methods. Statistical analysis was performed
into account that different Mediterranean diet indices using Stata version 11.1 (Stata Corp, College Station, TX).
have been used and that these studies have been under-
taken in countries where Mediterranean diet is the tradi- Results
tional food pattern, as well as in countries distant from Description of Eligible Studies
the Mediterranean Sea. The number of the studies avail- Supplementary Figure 1 presents a flow chart describing
able will enable more subanalyses, in an effort to answer the subsequent steps of the selection of eligible studies.
October 2013 581
ANNALS of Neurology
The details regarding the selection of studies are pre- substantial modification of results (pooled effect
sented in the online-only Supplementary Results. estimate 5 0.68, 95% CI 5 0.54–0.86; ie, exactly equal
Twenty-two eligible studies were finally included in this to the main analysis).
meta-analysis1,27–47; 11 of them pertained to stroke (9
cohorts including 162,092 subjects, among whom 3,176 Meta-Analysis: Moderate Adherence to
cases of stroke were noted; 2 case–control studies with Mediterranean Diet
297 cases and 296 controls),30,31,36–38,40,41,43,44,46,47 9 Table 2 presents the results regarding moderate adherence
examined depression (8 cohorts including 16,719 sub- to Mediterranean diet. Similarly to the associations on
jects, among whom 2,092 cases of depression were noted; high adherence, the protective effects regarding depres-
1 case–control study with 111 cases and 345 con- sion (pooled effect estimate 5 0.77, 95% CI: 0.62–0.95)
trols),28,29,32,34,38,39,42,45,46 and 8 evaluated cognitive and cognitive impairment (pooled effect estimate 5 0.79,
impairment (7 cohorts including 8,291 subjects, among 95% CI: 0.67–0.94) emerged again. Conversely, the pro-
whom 1,278 cases of cognitive impairment were noted; tective trend concerning stroke was only marginal
1 case–control study with 194 cases and 1,790 con- (pooled effect estimate 5 0.90, 95% CI 5 0.81–1.00).
trols).1,27,28,30,33–35,44 The characteristics of the included Regarding depression as well as cognitive impairment,
studies are presented in Supplementary Table 1. Contact the protective effects were reproducible in the subanalyses
with the authors of the individual studies was particularly containing the larger number of studies, but analyses on
valuable, as 7 authors provided us with additional data smaller subgroups tended to be hampered by lower
on depression,28,29,34,38,39,42,45 2 on cognitive impair- power.
ment,28,34 and 1 on stroke.40 The evaluation of the qual- Supplementary Figures 2 to 13 present the forest
ity of included studies is presented in Supplementary plots underlying the associations summarized in Table 2;
Tables 2 and 3. specifically, Supplementary Figures 2 to 4 and 11 portray
the results for stroke, and Supplementary Figures 5 to 7,
12 and 8 to 10, 13 the results for depression and cogni-
Meta-Analysis: High Adherence to
tive impairment, respectively.
Mediterranean Diet
Significant publication bias was noted regarding
Table 1 illustrates the results of the meta-analysis regard-
stroke (p 5 0.024); conversely, no significant publication
ing high adherence to Mediterranean diet. At the overall
bias was detected with respect to depression (p 5 0.576)
analysis, high adherence was consistently associated with
and cognitive impairment (p 5 0.957). The alternative
reduced risk for stroke (pooled effect estimate 5 0.71,
analysis adopting the earlier wave 1 (instead of wave 2)
95% confidence interval [CI] 5 0.57–0.89; Fig 1),
of the study by Luciano et al45 was not necessary, as the
depression (pooled effect estimate 5 0.68, 95%
study provided exclusively data pertaining to high
CI 5 0.54–0.86; Fig 2), and cognitive impairment
adherence.
(pooled effect estimate 5 0.60, 95% CI 5 0.43–0.83; Fig
3). Regarding stroke, the protective effect was reproduci- Subcategories of Outcomes
ble among case–control and longitudinal cohort studies; The analyses regarding subcategories of stroke (ischemic,
a similar pattern was noted regarding cognitive impair- hemorrhagic, fatal, nonfatal) and cognitive impairment
ment. The protective effect of high adherence in terms of (mild, advanced) are presented in the Supplementary
depression risk was replicated upon the subsets of case– Results (Supplementary Tables 4–6 and Supplementary
control, longitudinal cohort, and cross-sectional studies, Figures 14–28).
as well as by region of origin and published/unpublished
status. Supplementary Figures 2 to 10 present the forest Meta-Regression Analysis
plots underlying the associations summarized in Table 1; Table 3 presents the results of meta-regression analyses.
specifically, Supplementary Figures 2 to 4 display the The protective effects mediated by high adherence to
results for stroke, and Supplementary Figures 5 to 7 and Mediterranean diet in terms of risk for stroke seemed
8 to 10 pertain to depression and cognitive impairment, more pronounced among males (exponentiated coef-
respectively. ficient 5 0.84, 95% CI 5 0.74–0.94; Supplementary Fig
No significant publication bias was detected by any 29A). The potentially protective effects mediated by
analysis of high adherence (p 5 0.112 regarding stroke, moderate adherence in terms of stroke risk (exponenti-
p 5 0.434 for depression, and p 5 0.229 for cognitive ated coefficient 5 0.94, 95% CI 5 0.88–0.99; see Supple-
impairment). Finally, the alternative analysis adopting the mentary Fig 29B) seemed to follow the same pattern.
earlier wave 1 (instead of wave 2) of the study by The protective association between moderate adher-
Luciano et al45 for depression did not result in ence and depression seemed to fade away with advanced
582 Volume 74, No. 4October 2013
TABLE 1: Results of the Meta-Analyses Examining the Association between the Examined Outcomes and High Adherence to Mediterranean Diet
Analysis Stroke Depression Cognitive Impairment
a a a
No. Effect Estimate Heterogeneity, No. Effect Estimate Heterogeneity, No. Effect Estimate Heterogeneity,
(95% CI) I 2, p (95% CI) I 2, p (95% CI) I 2, p
Overall analysis 12 0.71 (0.57–0.89)b 69.1%,ANNALS of Neurology
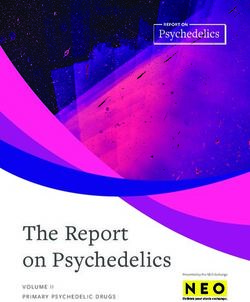
FIGURE 1: Forest plot describing the association between high adherence to Mediterranean diet and risk for stroke. Apart
from the overall analysis, the subanalyses on case–control (upper rows), longitudinal cohort (middle rows), and cross-sectional
studies (lower rows) are presented. CI 5 confidence interval; MeDi 5 score according to Trichopoulou et al.; MDS 5 score
according to Panagiotakos et al.; MD 5 other Mediterranean Diet score; OR 5 odds ratio; RR 5 relative risk. [Color figure can
be viewed in the online issue, which is available at www.annalsofneurology.org.]
age (exponentiated coefficient 5 1.13, 95% CI 5 1.01– moderate adherence to Mediterranean diet seemed also
1.26; Supplementary Fig 30); such a modifying effect to confer protection in terms of depression, as well as
was not observed regarding the effects mediated by high cognitive impairment risk, whereas its protective effects
adherence. regarding stroke remained only marginal; the pattern of
Supplementary Table 7 presents the results of the results may be indicative of a dose–response relationship.
post hoc meta-regression analysis examining effect modi- Interestingly, the protective effects of Mediterranean diet
fication by study quality measures and study characteris- in stroke prevention seemed more sizeable among males,
tics; no major effects were revealed, except for 2 cases. whereas the favorable actions of moderate adherence con-
First, regarding high adherence to Mediterranean diet cerning depression seemed to fade away with advancing
and cognitive impairment, multivariate adjustment was age.
associated with attenuation of the protective association. In an effort to describe in detail all relevant infor-
Second, regarding moderate adherence and depression, mation for cognitive impairment, the distinction between
longitudinal cohort studies seemed to yield more pro- MCI and advanced cognitive impairment (AD, cognitive
nounced protective effects. impairment ascertained through lower scores in Mini-
Mental State Examination [MMSE],48 and dementia
Discussion clinically diagnosed) was made. Mediterranean diet was
This meta-analysis shows that high adherence to a found to be protective for both subgroups (mild and
healthy dietary pattern, such as Mediterranean diet, advanced), and the finding was reproduced for AD,
seems beneficial along many central nervous system- which was the predominant condition among studies
related axes, as it was inversely associated with stroke, addressing advanced cognitive decline. Throughout the
cognitive impairment, and depression. To a lesser extent, studies, cognitive assessment was heterogeneous, done
584 Volume 74, No. 4Psaltopoulou et al: Mediterranean Diet: Annals of Neurology
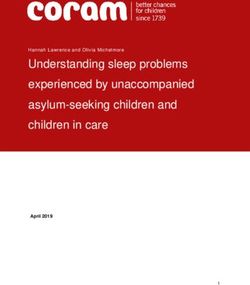
FIGURE 2: Forest plot describing the association between high adherence to Mediterranean diet and risk for depression. Apart
from the overall analysis, the subanalyses on case–control (upper panels), longitudinal cohort (middle panels), and cross-
sectional studies (lower panels) are presented. CI 5 confidence interval; MeDi 5 score according to Trichopoulou et al.;
MDS 5 score according to Panagiotakos et al.; OR 5 odds ratio; RR 5 relative risk. [Color figure can be viewed in the online
issue, which is available at www.annalsofneurology.org.]
either by neurologists though predefined batteries and in both longitudinal cohort and case–control studies, and
clinical examination, or through the MMSE question- in non-Mediterranean countries, the latter accounting for
naire, although there are inherent limitations regarding the majority of the sample. According to a recent review,
the latter, such as association with age and educational 70% of strokes could be avoided by healthy food choices
level.49 that are consistent with the traditional Mediterranean
Adherence to Mediterranean diet was found protec- diet.51 Gender emerged as a modifier in the relation of
tive for depression in all types of studies (longitudinal Mediterranean diet with stroke; our meta-regression anal-
cohort, case–control, and cross-sectional) both in Mediter- ysis showed that the protective effects seemed more size-
ranean and in non-Mediterranean countries. Depression able among males, regarding both high and moderate
was assessed with the Geriatric Depression Scale or with adherence. It would be tempting to hypothesize that
other relevant questionnaires (such as Center for Epide- males may particularly profit from the antioxidant, anti-
miologic Studies–Depression), which were interrelated to inflammatory, antithrombotic, and antiatherogenic prop-
an extent. According to meta-regression analysis, it was erties of Mediterranean diet in defense against stroke,
shown that gender was not a modifier in the relations, probably due to smoking and other lifestyle habits. Ische-
whereas age was. Specifically, it seems that the protective mic stroke had a statistically significant inverse associa-
effects of high adherence to Mediterranean diet were inde- tion with Mediterranean diet; however, the accumulation
pendent of age, whereas moderate adherence might lose its of further studies seems mandatory for the achievement
protective properties in older age. Interestingly, depression of statistical significance in subanalyses pertaining to the
is a risk factor for AD50; thus, the protective role mediated type of score used and Mediterranean region to guarantee
by Mediterranean diet in terms of both depression and AD the external generalizability of results. Interestingly, the
seems to point to the internal consistency of results. results of the present meta-analysis seem in accordance
Concerning stroke, the protective association of with the recently published, randomized multicenter
high adherence to Mediterranean diet has been replicated PREDIMED study, which showed that allocation of high
October 2013 585ANNALS of Neurology
FIGURE 3: Forest plot describing the association between high adherence to Mediterranean diet and risk for cognitive impair-
ment. Apart from the overall analysis, the subanalyses on case–control (upper panels), longitudinal cohort (middle panels), and
cross-sectional studies (lower panels) are presented. CI 5 confidence interval; MCI 5 mild cognitive impairment; MMSE 5 Mini-
Mental State Examination; OR 5 odds ratio; RR 5 relative risk. [Color figure can be viewed in the online issue, which is available
at www.annalsofneurology.org.]
cardiovascular risk participants to Mediterranean diet was meta-analysis, residual confounding can still exist. The
associated with protection from major cardiovascular analysis through diet scores can capture the extremes of
events (myocardial infarction, stroke, or death from car- the nutritional exposures and incorporate possible dietary
diovascular causes).52 confounding in the score.57 Two main indices, 1 with 9
Regarding the underlying mechanisms, studies dem- components with the use of sex-specific median as cutoffs
onstrating a protective relation between Mediterranean and a range from 0 (minimum adherence) to 9 (maxi-
diet and white matter hyperintensity53 as well as infarcts mum adherence) and another with positive and negative
detected on brain magnetic resonance imaging40 are sug- scoring of the components, have been used in most of
gestive of a vascular protective component of this diet. the articles synthesized herein. Moreover, all studies used
Conversely, it has been highlighted that, regarding AD, food frequency questionnaires, but the latter differed
other mechanisms such as inflammation and oxidation across studies, adding to the complexity of analyses;
could play a role, with vascular comorbidity having a sec- nevertheless, apart from reviewing single food groups or
ondary or no role.54 macro-/micronutrients, it is equally important to system-
Recent literature has shown that adherents to Medi- atically review the impact of nutritional patterns, as die-
terranean diet may be more health conscious,55 more tary components are not eaten in isolation and could
physically active, smoke less, or have more favorable exhibit synergistic and antagonistic interactions.58
social and lifestyle determinants.56 Notably, in many eli- The exclusion of studies that have not sent their
gible studies, these confounders have been taken into data is a potential limitation of this study, despite the
account, whereas meta-regression analysis in our study rigorous contact with authors, as appropriate.59 Cherbuin
did not reveal any sizeable modifying effects mediated by et al60 and Vercambre et al46 concluded that Mediterra-
them; although this may be considered an asset of this nean diet was not related to cognitive decline, whereas
586 Volume 74, No. 4October 2013
TABLE 2: Results of the Meta-Analyses Examining the Association between the Examined Outcomes and Moderate Adherence to Mediterranean Diet
Analysis Stroke Depression Cognitive Impairment
a a a
No. Effect Estimate Heterogeneity No. Effect Estimate Heterogeneity No. Effect Estimate Heterogeneity
(95% CI) I 2, p (95% CI) I2, p (95% CI) I2, p
Overall analysis 12 0.90 (0.81–1.00) 17.4%, 0.273 9 0.77 (0.62–0.95)b 54.4%, 0.025 9 0.79 (0.67–0.94)b 28.3%, 0.193
b
Case–control studies 1 0.50 (0.31–0.79) NC 1 0.71 (0.40–1.26) NC 1 0.48 (0.29–0.79)b NC
b
Longitudinal cohort studies 6 0.96 (0.87–1.05) 0.0%, 0.836 2 0.57 (0.43–0.77) 50.1%, 0.157 4 0.90 (0.75–1.08) 0.0%, 0.690
b
Cross-sectional studies 5 0.89 (0.74–1.09) 0.0%, 0.273 6 0.92 (0.78–1.09) 0.0%, 0.587 4 0.73 (0.56–0.97) 16.1%, 0.311
b b
Score according to 8 0.87 (0.74–1.02) 0.0%, 0.824 5 0.73 (0.56–0.94) 70.6%, 0.009 8 0.79 (0.66–0.94) 34.3%, 0.155
Trichopoulou et al8
Score according to 2 0.71 (0.37–1.38) 82.9%, 0.016 4 0.90 (0.64–1.27) 0.0%, 0.405 1 1.89 (0.18–19.82) NC
Panagiotakos et al25
Other scores 2 0.98 (0.87–1.09) 4.6%, 0.306 0 NC NC 0 NC NC
b
Mediterranean countries 3 0.66 (0.42–1.06) 55.3%, 0.107 8 0.71 (0.58–0.88) 36.0%, 0.142 3 1.02 (0.73–1.43) 0.0%, 0.803
b
Non-Mediterranean 9 0.95 (0.87–1.04) 0.0%, 0.775 1 1.00 (0.78–1.28) NC 6 0.74 (0.60–0.91) 39.4%, 0.143
countries
Data drawn from 11 0.91 (0.82–1.01) 16.8%, 0.284 3 0.69 (0.46–1.04) 84.9%, 0.001 7 0.77 (0.63–0.93)b 39.2%, 0.130
manuscriptsc
Data from reanalyses 1 0.67 (0.38–1.17) NC 6 0.83 (0.67–1.03) 0.0%, 0.666 2 0.98 (0.64–1.49) 0.0%, 0.576
provided after contact
with corresponding authors
a
Number of study arms.
b
Statistically significant associations.
c
Includes also effect estimates calculated by means of published 2 3 2 tables.
CI 5 confidence interval; NC 5 not calculable.
Psaltopoulou et al: Mediterranean Diet: Annals of Neurology
587588
ANNALS
of Neurology
TABLE 3: Results of the Meta-Regression Analyses Examining Whether Gender and Age Modified the Association between Adherence to Mediterranean
Diet and the Evaluated Conditions
Factor Stroke Depression Cognitive Impairment
a a a
No. Exponentiated p No. Exponentiated p No. Exponentiated p
Coefficient Coefficient Coefficient
(95% CI) (95% CI) (95% CI)
High adherence
Age, increments of 10 years 11 0.94 (0.67–1.33) 0.714 8 0.98 (0.71–1.36) 0.899 9 1.09 (0.31–3.83) 0.879
b
Percentage male, increments of 10% 12 0.84 (0.74–0.94) 0.008 8 0.91 (0.72–1.16) 0.388 9 1.00 (0.52–1.93) 0.997
Moderate adherence
Age, increments of 10 years 10 0.96 (0.81–1.14) 0.576 8 1.13 (1.01–1.26)b 0.038 9 1.06 (0.56–1.98) 0.841
b
Percentage male, increments of 10% 12 0.94 (0.89–0.99) 0.043 8 0.92 (0.80–1.07) 0.232 9 0.95 (0.69–1.31) 0.723
a
Number of study arms; the numbers are smaller than those in Tables 1 and 2, as some studies did not report the exact mean age and/or percentage male.
b
Statistically significant modification effects.
CI 5 confidence interval; NC 5 not calculable.
Volume 74, No. 4Psaltopoulou et al: Mediterranean Diet: Annals of Neurology
Tangney and colleagues47 showed that higher Mediterra- Apart from the limitations of the individual studies,
nean diet scores were associated with slower rates of cog- a core limitation regarding the synthesis of Mediterra-
nitive decline after correcting for age, sex, race, nean diet scores pertains to scores not using absolute cut-
education, participation in cognitive activities, and offs but rather relative cutoffs to identify adherence, so
energy. In addition, Gao and colleagues found that an someone could be differentially classified among studies.
alternate Mediterranean diet score was inversely related Nevertheless, subgroup analyses by type of score did not
to the development of Parkinson disease, in a nonsignifi- point to sizeable differences, underlining the consistency
cant way.61 Conversely, the inclusion of results obtained of effect estimates. Moreover, given that individual stud-
after the rigorous contact with authors59 seems to have ies did not present detailed dietary behavior characteris-
increased the statistical power, especially regarding tics and Mediterranean diet score components, neither a
depression. Regarding the latter, 7 of 9 study arms per- reclassification based on dietary behavior differences nor
taining to high adherence and 6 of 9 arms pertaining to detailed analyses by score components was feasible.
moderate adherence were obtained after contact with Another limitation pertains to the considerable heteroge-
authors; this may represent an asset of this meta-analysis, neity, especially regarding the analyses on high adherence
especially given that the effect estimates of the aforemen- to Mediterranean diet. Heterogeneity might be due to
tioned arms did not seem to differ from those published, differences in study design, variability in scores used, geo-
as attested by the respective subgroup analyses. On the graphical reasons, and other factors; in an attempt to
contrary, concerning stroke and cognitive impairment, trace its origins, detailed subgroup analyses have been
the majority of study arms stemmed from published presented for each outcome. The explanation underlying
studies. heterogeneity seeming to be more pronounced among
Moreover, limitations of the included studies were high adherence arms remains elusive, but may at a cer-
reflected upon their quality ratings. In longitudinal tain extent be associated with high adherence originally
cohort studies, median follow-up was oftenANNALS of Neurology
demonstration of dose–response effects and the achieve- Third National Health and Nutrition Examination Survey (NHANES
III), 1988–1994. Atherosclerosis 2010;210:630–636.
ment of statistical significance by the present synthesis of
studies may represent a reference dipole for future 15. Llorente-Cortes V, Estruch R, Mena MP, et al. Effect of Mediterra-
nean diet on the expression of pro-atherogenic genes in a
studies. population at high cardiovascular risk. Atherosclerosis 2010;208:
In conclusion, given the limited availability of phar- 442–450.
maceutical agents to treat cognitive impairment, cogni- 16. Vincent-Baudry S, Defoort C, Gerber M, et al. The Medi-RIVAGE
study: reduction of cardiovascular disease risk factors after a 3-mo
tive decline, and stroke, one could argue for the
intervention with a Mediterranean-type diet or a low-fat diet. Am
importance of preventive measures, such as a healthy die- J Clin Nutr 2005;82:964–971.
tary regime, to diminish the risk of mild and advanced 17. Psaltopoulou T, Naska A, Orfanos P, et al. Olive oil, the Mediter-
cognitive decline, AD, depression, and stroke. ranean diet, and arterial blood pressure: the Greek European
Prospective Investigation into Cancer and Nutrition (EPIC) study.
Am J Clin Nutr 2004;80:1012–1018.
Potential Conflicts of Interest 18. Kastorini CM, Milionis HJ, Esposito K, et al. The effect of Mediter-
ranean diet on metabolic syndrome and its components: a meta-
Nothing to report. analysis of 50 studies and 534,906 individuals. J Am Coll Cardiol
2011;57:1299–1313.
19. Romaguera D, Guevara M, Norat T, et al. Mediterranean diet and
type 2 diabetes risk in the European Prospective Investigation
References into Cancer and Nutrition (EPIC) study: the InterAct project.
Diabetes Care 2011;34:1913–1918.
1. Scarmeas N, Luchsinger JA, Schupf N, et al. Physical activity, diet,
and risk of Alzheimer disease. JAMA 2009;302:627–637. 20. Esposito K, Kastorini CM, Panagiotakos DB, et al. Mediterranean
diet and weight loss: meta-analysis of randomized controlled
2. Solfrizzi V, Frisardi V, Seripa D, et al. Mediterranean diet in trials. Metab Syndr Relat Disord 2011;9:1–12.
predementia and dementia syndromes. Curr Alzheimer Res 2011;
8:520–542. 21. Chrysohoou C, Skoumas J, Pitsavos C, et al. Long-term adherence
to the Mediterranean diet reduces the prevalence of hyperuricae-
3. Sofi F, Macchi C, Abbate R, et al. Effectiveness of the Mediterra-
mia in elderly individuals, without known cardiovascular disease:
nean diet: can it help delay or prevent Alzheimer’s disease? J Alz-
the Ikaria study. Maturitas 2011;70:58–64.
heimers Dis 2010;20:795–801.
22. Fragopoulou E, Panagiotakos DB, Pitsavos C, et al. The associa-
4. Sherzai A, Heim LT, Boothby C, et al. Stroke, food groups, and
tion between adherence to the Mediterranean diet and adiponec-
dietary patterns: a systematic review. Nutr Rev 2012;70:423–435.
tin levels among healthy adults: the ATTICA study. J Nutr
5. Appleton KM, Rogers PJ, Ness AR. Updated systematic review Biochem 2010;21:285–289.
and meta-analysis of the effects of n-3 long-chain polyunsaturated
fatty acids on depressed mood. Am J Clin Nutr 2010;91:757–770. 23. Esposito K, Marfella R, Ciotola M, et al. Effect of a
Mediterranean-style diet on endothelial dysfunction and markers
6. Bach-Faig A, Berry EM, Lairon D, et al. Mediterranean diet pyra- of vascular inflammation in the metabolic syndrome: a randomized
mid today. Science and cultural updates. Public Health Nutr 2011; trial. JAMA 2004;292:1440–1446.
14:2274–2284.
24. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observa-
7. European Food Safety Authority. Scientific opinion on the sub- tional studies in epidemiology: a proposal for reporting. Meta-
stantiation of health claims related to fruits and/or vegetables and analysis Of Observational Studies in Epidemiology (MOOSE)
to the “Mediterranean diet” pursuant to Article 13(1) of Regula- group. JAMA 2000;283:2008–2012.
tion (EC) No 1924/2006. EFSA J 2011;9:2245.
25. Panagiotakos DB, Pitsavos C, Stefanadis C. Dietary patterns: a
8. Trichopoulou A, Costacou T, Bamia C, et al. Adherence to a Med- Mediterranean diet score and its relation to clinical and biological
iterranean diet and survival in a Greek population. N Engl J Med markers of cardiovascular disease risk. Nutr Metab Cardiovasc Dis
2003;348:2599–2608. 2006;16:559–568.
9. UNESCO. Intangible heritage lists. Mediterranean diet. Available 26. Higgins JPT, Green S. Cochrane Handbook for systematic reviews
at: http://www.unesco.org/culture/ich/index.php?lg5en&pg50001 of interventions version 5.1.0. Updated March 2011. Available at:
1&RL500394 Accessed February 1, 2013. www.cochrane-handbook.org. Accessed on March 1, 2013.
10. Sofi F, Abbate R, Gensini GF, et al. Accruing evidence on benefits 27. Scarmeas N, Stern Y, Mayeux R, et al. Mediterranean diet,
of adherence to the Mediterranean diet on health: an updated Alzheimer disease, and vascular mediation. Arch Neurol 2006;63:
systematic review and meta-analysis. Am J Clin Nutr 2010;92: 1709–1717.
1189–1196.
28. Psaltopoulou T, Kyrozis A, Stathopoulos P, et al. Diet, physical
11. Martinez-Gonzalez MA, Guillen-Grima F, De Irala J, et al. The
activity and cognitive impairment among elders: the EPIC-Greece
Mediterranean diet is associated with a reduction in premature
cohort (European Prospective Investigation into Cancer and
mortality among middle-aged adults. J Nutr 2012;142:1672–1678.
Nutrition). Public Health Nutr 2008;11:1054–1062.
12. Panagiotakos DB, Dimakopoulou K, Katsouyanni K, et al. Mediter-
29. Bountziouka V, Polychronopoulos E, Zeimbekis A, et al. Long-term
ranean diet and inflammatory response in myocardial infarction
fish intake is associated with less severe depressive symptoms
survivors. Int J Epidemiol 2009;38:856–866.
among elderly men and women: the MEDIS (MEDiterranean
13. Dai J, Jones DP, Goldberg J, et al. Association between adher- ISlands Elderly) epidemiological study. J Aging Health 2009;21:
ence to the Mediterranean diet and oxidative stress. Am J Clin 864–880.
Nutr 2008;88:1364–1370.
30. Feart C, Samieri C, Rondeau V, et al. Adherence to a Mediterra-
14. Carter SJ, Roberts MB, Salter J, et al. Relationship between Medi- nean diet, cognitive decline, and risk of dementia. JAMA 2009;
terranean diet score and atherothrombotic risk: findings from the 302:638–648.
590 Volume 74, No. 4Psaltopoulou et al: Mediterranean Diet: Annals of Neurology
31. Fung TT, Rexrode KM, Mantzoros CS, et al. Mediterranean diet 46. Vercambre MN, Grodstein F, Berr C, et al. Mediterranean diet
and incidence of and mortality from coronary heart disease and and cognitive decline in women with cardiovascular disease or risk
stroke in women. Circulation 2009;119:1093–1100. factors. J Acad Nutr Diet 2012;112:816–823.
32. Sanchez-Villegas A, Delgado-Rodriguez M, Alonso A, et al. 47. Tangney CC, Kwasny MJ, Li H, et al. Adherence to a
Association of the Mediterranean dietary pattern with the inci- Mediterranean-type dietary pattern and cognitive decline in a
dence of depression: the Seguimiento Universidad de Navarra/ community population. Am J Clin Nutr 2011;93:601–607.
University of Navarra follow-up (SUN) cohort. Arch Gen Psychiatry
2009;66:1090–1098. 48. Christa Maree Stephan B, Minett T, Pagett E, et al. Diagnosing
mild cognitive impairment (MCI) in clinical trials: a systematic
33. Scarmeas N, Stern Y, Mayeux R, et al. Mediterranean diet and
review. BMJ Open 2013;3.
mild cognitive impairment. Arch Neurol 2009;66:216–225.
34. Chrysohoou C, Tsitsinakis G, Siassos G, et al. Fish consumption 49. Tombaugh TN, McIntyre NJ. The mini-mental state examination: a
moderates depressive symptomatology in elderly men and comprehensive review. J Am Geriatr Soc 1992;40:922–935.
women from the IKARIA study. Cardiol Res Pract 2010;2011:
50. Ownby RL, Crocco E, Acevedo A, et al. Depression and risk for
219578.
Alzheimer disease: systematic review, meta-analysis, and metare-
35. Roberts RO, Geda YE, Cerhan JR, et al. Vegetables, unsaturated gression analysis. Arch Gen Psychiatry 2006;63:530–538.
fats, moderate alcohol intake, and mild cognitive impairment.
Dement Geriatr Cogn Disord 2010;29:413–423. 51. Willett WC. The Mediterranean diet: science and practice. Public
Health Nutr 2006;9:105–110.
36. Agnoli C, Krogh V, Grioni S, et al. A priori-defined dietary pat-
terns are associated with reduced risk of stroke in a large Italian 52. Estruch R, Ros E, Salas-Salvado J, et al. Primary prevention of car-
cohort. J Nutr 2011;141:1552–1558. diovascular disease with a Mediterranean diet. N Engl J Med
2013;368:1279–1290.
37. Gardener H, Wright CB, Gu Y, et al. Mediterranean-style diet and
risk of ischemic stroke, myocardial infarction, and vascular death: 53. Gardener H, Scarmeas N, Gu Y, et al. Mediterranean diet and
the Northern Manhattan Study. Am J Clin Nutr 2011;94: white matter hyperintensity volume in the Northern Manhattan
1458–1464. Study. Arch Neurol 2012;69:251–256.
38. Kastorini CM, Milionis HJ, Ioannidi A, et al. Adherence to the
54. Gu Y, Scarmeas N. Dietary patterns in Alzheimer’s disease and
Mediterranean diet in relation to acute coronary syndrome or
cognitive aging. Curr Alzheimer Res 2011;8:510–519.
stroke nonfatal events: a comparative analysis of a case/case-
control study. Am Heart J 2011;162:717–724. 55. Knopman DS. Mediterranean diet and late-life cognitive impair-
39. Milaneschi Y, Bandinelli S, Penninx BW, et al. Depressive symp- ment: a taste of benefit. JAMA 2009;302:686–687.
toms and inflammation increase in a prospective study of older
56. Chrysohoou C, Panagiotakos DB, Pitsavos C, et al. Adherence to
adults: a protective effect of a healthy (Mediterranean-style) diet.
the Mediterranean diet attenuates inflammation and coagulation
Mol Psychiatry 2011;16:589–590.
process in healthy adults: the ATTICA Study. J Am Coll Cardiol
40. Scarmeas N, Luchsinger JA, Stern Y, et al. Mediterranean diet and 2004;44:152–158.
magnetic resonance imaging-assessed cerebrovascular disease.
Ann Neurol 2011;69:257–268. 57. Trichopoulou A, Orfanos P, Norat T, et al. Modified Mediterra-
nean diet and survival: EPIC-elderly prospective cohort study.
41. Yau WY, Hankey GJ. Which dietary and lifestyle behaviours may BMJ 2005;330:991.
be important in the aetiology (and prevention) of stroke? J Clin
Neurosci 2011;18:76–80. 58. Sofi F, Cesari F, Abbate R, et al. Adherence to Mediterranean
diet and health status: meta-analysis. BMJ 2008;337:a1344.
42. Antonogeorgos G, Panagiotakos DB, Pitsavos C, et al. Under-
standing the role of depression and anxiety on cardiovascular dis- 59. Mullan RJ, Flynn DN, Carlberg B, et al. Systematic reviewers com-
ease risk, using structural equation modeling; the mediating effect monly contact study authors but do so with limited rigor. J Clin
of the Mediterranean diet and physical activity: the ATTICA study. Epidemiol 2009;62:138–142.
Ann Epidemiol 2012;22:630–637.
60. Cherbuin N, Anstey KJ. The Mediterranean diet is not related to
43. Hoevenaar-Blom MP, Nooyens AC, Kromhout D, et al. Mediterra-
cognitive change in a large prospective investigation: the PATH
nean style diet and 12-year incidence of cardiovascular diseases:
Through Life study. Am J Geriatr Psychiatry 2012;20:635–639.
the EPIC-NL cohort study. PLoS One 2012;7:e45458.
44. Gardener S, Gu Y, Rainey-Smith SR, et al. Adherence to a Medi- 61. Gao X, Chen H, Fung TT, et al. Prospective study of dietary pat-
terranean diet and Alzheimer’s disease risk in an Australian popu- tern and risk of Parkinson disease. Am J Clin Nutr 2007;86:1486–
lation. Transl Psychiatry 2012;2:e164. 1494.
45. Luciano M, Mottus R, Starr JM, et al. Depressive symptoms and 62. McMillan L, Owen L, Kras M, et al. Behavioural effects of a 10-day
diet: their effects on prospective inflammation levels in the Mediterranean diet. Results from a pilot study evaluating mood
elderly. Brain Behav Immun 2012;26:717–720. and cognitive performance. Appetite 2011;56:143–147.
October 2013 591You can also read