Management of Common Sports Injuries of the Foot & Ankle - Simon Mordecai Consultant Trauma & Orthopaedic Surgeon Foot and Ankle Specialist ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Management of Common Sports Injuries of the
Foot & Ankle
Simon Mordecai
Consultant Trauma & Orthopaedic Surgeon
Foot and Ankle Specialist
www.footandanklespecialist.co.uk
6 July 2021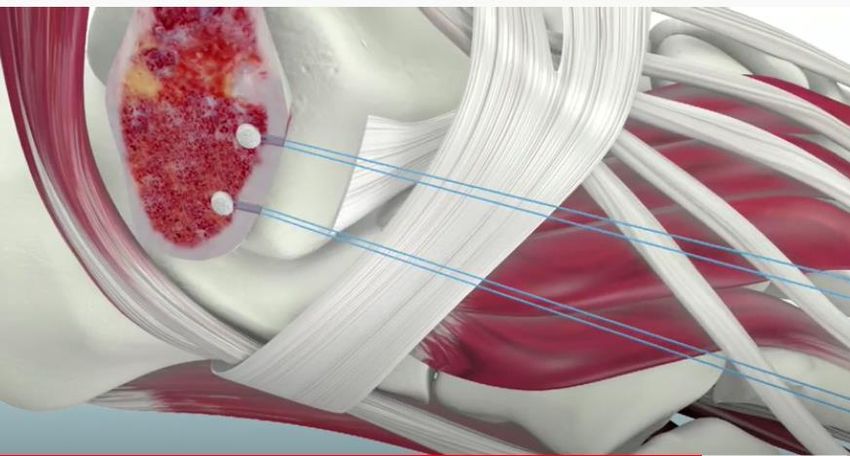
Introduction 1. Sports related injuries have been on the rise 2. Can be easily missed… 3. Recap common and important clinical signs 4. Management and when to refer 2
Case 1 1. 36Y F Police officer 2. Recurrent ankle pain / instability / swelling 3. Keeps ‘giving way’ 4. Significant inversion injury ~ 9 months ago 3

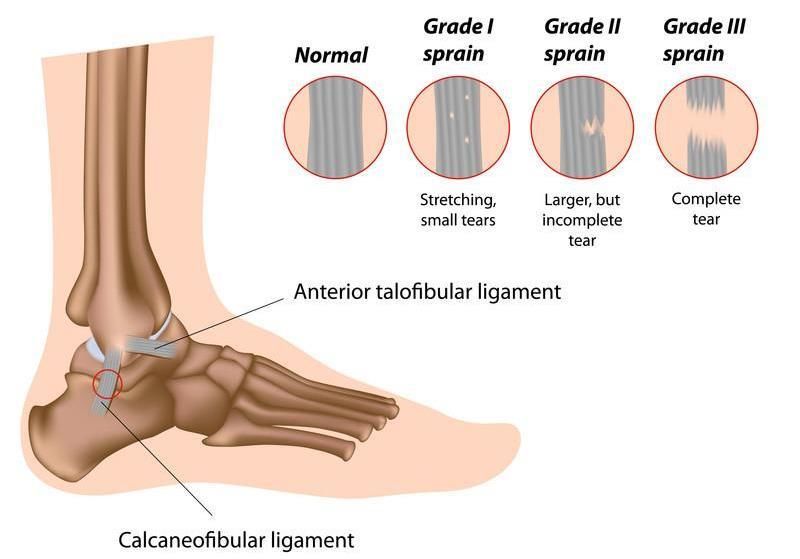
Ankle sprains 4

Grading 5
Presentation
1. Bruising / Swelling / difficulty bearing weight
2. Examination
• Tender distal to tip of fibular
• Anterior draw test
3. Investigations
• Radiographs
• MRI if persistent
6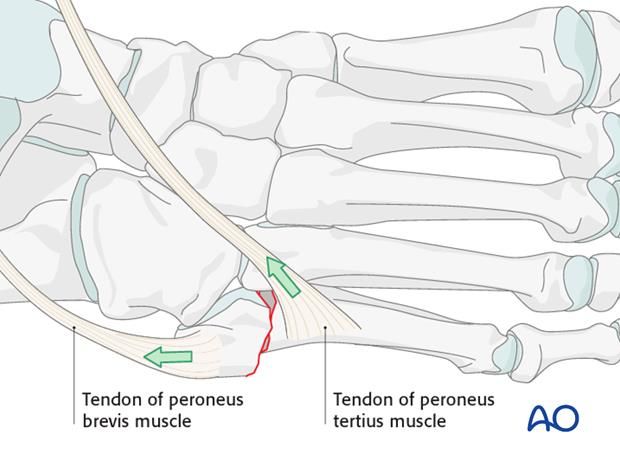
Management
1. RICE
2. Initial immobilisation - walking boot
3. Functional physiotherapy
4. Specialist referral after 3-6 months
• On going pain / swelling
• Recurrent instability
• Failure to return to baseline activity
• MRI scan +/- surgical stabilisation
• 2 weeks NWB in POP boot 4 weeks
Physiotherapy
7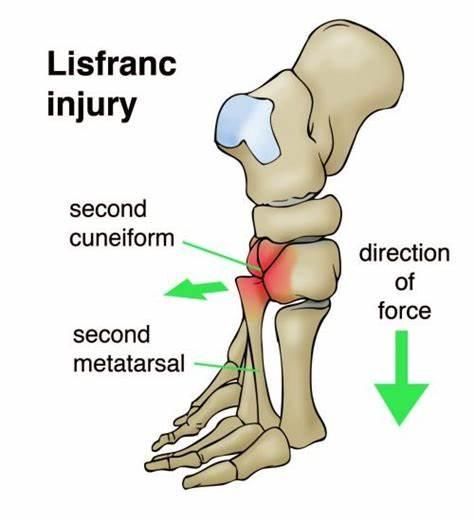
Take home messages
1. Initial management the same for all ankle sprains
2. Most commonly affects lateral ligaments with inversion injury
3. Stability examinations – compare to other side
4. Refer persistent pain and instability > 3 months
• MRI +/- surgery
8
Case 2
1. 61y M
2. Vague history – sudden pain in the back of the ankle
3. Able to continue walking but painful
4. Seen in UCC
• Noted full ROM
• Mildly swollen ankle
• Pain going up calf
• XR – no fractures
5. On going pain and swelling
• Referred for DVT scan negative
6. Referred to fracture clinic 6-7 weeks later
• Achilles tendon rupture
9
Achilles tendon rupture
1. Often misdiagnosed as an ankle sprain
2. May be missed in up to 20% of cases
3. 4500 cases per year
4. More common in men
5. Most common in ages 30-40 and 60yrs +
6. Risk factors
• episodic athletes, "weekend warrior“
• fluoroquinolone antibiotics
• steroid injections
10Symptoms 1. Pain in the back of heel 2. ‘kicked’ – turn around and no one there 3. Swelling 4. Bruising 5. People who think they have sprained their ankle MAY have ruptured their AT 6. Not always during sport 7. Difficulty walking with weakness - They can still often walk! 11
Signs 12
Investigations 13
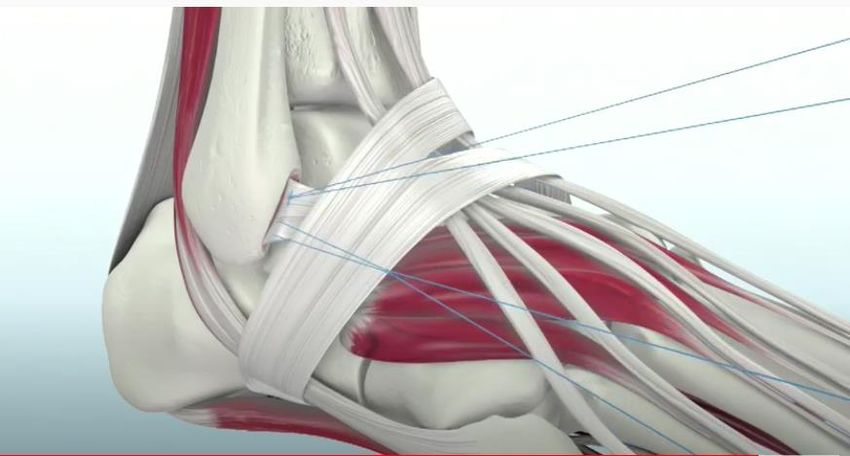
Treatment
Operative Non-operative
14Treatment
Surgery Conservative
Pros Predictable rehab Safer
MIS techniques Equal functional results at 1yr
Cons Wound complications Potential higher re-rupture
1. Flaws
• Different rehab regimes
• ? Gap size
• Different repair techniques
15Few usually go on to surgery 1. Patient choice 2. Elite athletes 3. Tendon gap size on USS (???? Magic figure) 16
Take home messages
1. Patients with rupture can still walk.
2. Patients with rupture can still actively move the ankle up and down.
3. Patients with rupture will not always have a palpable gap in the tendon.
4. Calf squeeze false negatives
• Ankle fusion
• Calf muscle wasting
• Ankle arthritis
5. Although still debate over operative vs. non-operative
• Prompt recognition and treatment is paramount
17Case 3 1. 28 F 2. Tripped over dog 3. Bruising and swelling of midfoot 4. Able to walk 5. Attended UCC – advised no acute bony injury 6. On going pain and discomfort – not quite right 18
Signs 19
Radiographs - WB 20
Radiographs - WB 21
Lisfranc Injures 1. Almost one-third are missed on initial review 2. These missed injuries are a common cause of litigation 3. Missed injuries cause pain, late deformity and significant morbidity 22
Lisfranc Anatomy 23
Role and importance
1. Role of Lisfranc ligament
• Transfer of load through midfoot
• Maintains medial longitudinal arch
• Main connection between medial column and rest of foot
2. Morbidity if missed
• Midfoot arthritis
• Midfoot collapse and deformity +/- ulceration
• Persistent pain
24Mechanism 1. Can be severe trauma, but also mild trauma 2. Mild trauma can be twisting, or landing awkwardly 3. Sometimes a history of tripping and plantarflexing the foot 25
Management – majority require fixation
1. Considerations
• Fix or fuse
• Plates or screws
26
• Purely ligamentous or bony injuryTake home messages
1. Can be from a trivial injury
2. Persistent midfoot pain and inability to bear weight properly
3. Plantar bruising is pathognomonic
4. Weight bearing XR crucial to aid diagnosis
5. Significant morbidity is missed
• Urgent referral to fracture clinic / On call team
27Case 4 1. 35 M basket ball player 2. Landed awkwardly on foot 3. Able to bear weight 4. Pain on lateral border of foot 28
Radiograph 29
5th Metatarsal base fracture 1. Most common foot fracture 2. Fracture position determines likelihood of healing 3. Athletes / manual labourers / military 4. Diagnoses made with plain radiograph 30
Injury zones 1. Zone 1 – avulsion 2. Zone 2 – Jones fracture 3. Zone 3 – shaft fracture 31
Zone 2 – blood supply 32
Mechanism
plantarflexion and hindfoot inversion Zone 1
forefoot adduction Zone 2
repetitive microtrauma Zone 3
33Management
Treatment Algorithm
Zone 1 WB as tolerated
Zone 2 Protected W/B 6/52 – monitor
Elite athlete fix
Zone 3 Protected W/B 6/52
34Fixation 35
Take home messages
1. 5th metatarsal base fracture very common
• Variety of mechanisms
2. Fracture location important for prognosis
3. All initially managed in the community
• >90% will go on to heal
4. Refer if still painful after 3 months.
36References
1. Orthopaedic Associates of St. Augustine’s, https://www.oastaug.com/ankle-sprains-high-vs-low/
2. https://www.bodyheal.com.au/blogs/sports-injuries/different-types-of-ankle-sprains-symptoms-treatment
3. Singh D, Acute Achilles tendon rupture, BMJ 351: h4722 (2015)
4. Maffulli N, Waterston SW, Squair J et al. Changing incidence of Achilles tendon rupture in Scotland: a 15-year study. Clin J
Sport Med. 1999 Jul;9(3):157-60
5. Bone Joint J. 2020 Nov;102-B(11):1535-1541. Does size of tendon gap affect patient-reported outcome following Achilles
tendon rupture treated with functional rehabilitation? Mohamed Yassin , Richard Myatt , William Thomas , Vatsal Gupta ,
Tagrit Hoque , Devendra Mahadevan
6. Achilles tendon rupture: how to avoid missing the diagnosis, Robert PR Boyd, Richard Dimock, Matthew C Solan, Edward
Porter, British Journal of General Practice 2015; 65 (641): 668-669.
7. https://orthoinfo.aaos.org/en/diseases--conditions/lisfranc-midfoot-injury/
8. https://www.orthobullets.com/foot-and-ankle/7030/lisfranc-injury
9. Jones Fracture, https://sportsclinicnq.com.au/jones-fracture/
10. 5th Metatarsal Injuries, https://www.biaphysio.com/treat/5th-metatarsal-injuries/
11. https://www.orthobullets.com/foot-and-ankle/7031/5th-metatarsal-base-fracture
37Questions 38
You can also read

















































