Making patient blood management the new norm(al) as experienced by implementors in diverse countries - BMC ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Hofmann et al. BMC Health Services Research (2021) 21:634
https://doi.org/10.1186/s12913-021-06484-3
RESEARCH ARTICLE Open Access
Making patient blood management the
new norm(al) as experienced by
implementors in diverse countries
Axel Hofmann1,2†, Donat R. Spahn1†, Anke-Peggy Holtorf3,4*† and PBM Implementation Group
Abstract
Background: Patient blood management (PBM) describes a set of evidence-based practices to optimize medical
and surgical patient outcomes by clinically managing and preserving a patient’s own blood. This concepts aims to
detect and treat anemia, minimize the risk for blood loss and the need for blood replacement for each patient
through a coordinated multidisciplinary care process. In combination with blood loss, anemia is the main driver for
transfusion and all three are independent risk factors for adverse outcomes including morbidity and mortality.
Evidence demonstrates that PBM significantly improves outcomes and safety while reducing cost by
macroeconomic magnitudes. Despite its huge potential to improve healthcare systems, PBM is not yet adopted
broadly. The aim of this study is to analyze the collective experiences of a diverse group of PBM implementors
across countries reflecting different healthcare contexts and to use these experiences to develop a guidance for
initiating and orchestrating PBM implementation for stakeholders from diverse professional backgrounds.
Methods: Semi-structured interviews were conducted with 1–4 PBM implementors from 12 countries in Asia, Latin
America, Australia, Central and Eastern Europe, the Middle East, and Africa. Responses reflecting the drivers, barriers,
measures, and stakeholders regarding the implementation of PBM were summarized per country and underwent
qualitative content analysis. Clustering the resulting implementation measures by levels of intervention for PBM
implementation informed a PBM implementation framework.
Results: A set of PBM implementation measures were extracted from the interviews with the implementors. Most
of these measures relate to one of six levels of implementation including government, healthcare providers,
funding, research, training/education, and patients/public. Essential cross-level measures are multi-stakeholder
communication and collaboration.
* Correspondence: anke.holtorf@health-os.com
†
Axel Hofmann, Donat R. Spahn and Anke-Peggy Holtorf contributed equally
to this work.
3
Health Outcomes Strategies GmbH, Colmarerstrasse 58, CH4055 Basel,
Switzerland
4
Faculty of the College of Pharmacy, University of Utah, Salt Lake City, UT,
USA
Full list of author information is available at the end of the article
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,
which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons
licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons
licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain
permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the
data made available in this article, unless otherwise stated in a credit line to the data.Hofmann et al. BMC Health Services Research (2021) 21:634 Page 2 of 19 Conclusion: The implementation matrix resulting from this research helps to decompose the complexity of PBM implementation into concrete measures on each implementation level. It provides guidance for diverse stakeholders to design, initiate and develop strategies and plans to make PBM a national standard of care, thus closing current practice gaps and matching this unmet public health need. Keywords: Patient blood management, Transfusion, Patient outcomes, Practice change, Culture change, Implementation Background calls for ‘Effective implementation of patient blood man- Of the millions of patients hospitalized yearly, a large agement’ [7]. proportion is anemic at admission. Preoperative anemia However, despite compelling evidence and ongoing rates range from 20 to 75% [1], and hospital acquired WHO policy drive, practical guidance for healthcare anemia often adds to the problem [2]. In most cases, providers and national authorities [16, 19–21] and clin- anemia is not considered a clinically significant condi- ical guidelines and recommendations across numerous tion, remains unnoticed, and therefore uncorrected in specialties and national health systems [17, 22–30], im- hospitalized patients. plementation of Patient Blood Management is still far However, a large body of evidence shows that anemia, behind the expectations for good and safe clinical blood loss, and transfusion are independent risk factors practices. for adverse outcomes including morbidity, mortality and The implementation of Patient Blood Management is average length of hospital stay [3–6]. Patient blood man- hampered by barriers mostly related to the difficulty of agement is defined by the WHO as ”a set of evidence- changing traditional “physicians’ attitudes” towards based practices to optimize medical and surgical patient transfusion [31] and “transfusion behavior” [32–34]. outcomes through preservation of the patient’s own Even hard-hitting crises such as the HIV-pandemic in blood” [7]. The International Foundation for Patient the 1970s and 1980s with tens of thousands infected Blood Mangement specifies, that “Patient Blood Man- from contaminated donor blood, the huge death toll, bil- agement (PBM) is an evidence-based bundle of care to lions of dollars in financial losses from lawsuits and optimize medical and surgical patient outcomes by clin- compensations and criminal charges [35] only had a ically managing and preserving a patient’s own blood” transient impact on changing long standing transfusion [8]. Patient blood management rests on three pillars: practice [36]. What was called at the time “transfusion diagnosis and treatment of anaemia (especially iron defi- alternative strategies” showed compelling results and ciency anaemia), minimization of blood loss, and avoid- could have been helpful to reduce overall blood ance of unnecessary transfusions. In addition to being a utilization with similar outcomes [37–40], but went fundamental element of good clinical practice in transfu- largely unnoticed [3]. Instead, the focus remained solely sion, it plays a key role in primary health care. The on improving blood product safety through introducing multi-professional, multimodal, and individualized ap- donor blood testing methods with unprecedented cost proach involves general practitioners, hematologists, an- per quality adjusted life year (QALY) between 4.7 and esthesiologists, intensive care specialists, surgeons, and 11.2 million US-$, representing 94–224 times the then others. The term ‘Patient Blood Management’ was commonly accepted threshold in public health decision coined in 2005 [9], but the concept has been emerging making (50,000 US-$/QALY) [41, 42]. Meanwhile, and since a much longer time [10, 11]. Meanwhile, large despite rapidly accumulating clinical evidence for ad- multicentric observational studies and randomized con- verse transfusion outcomes and favorable Patient Blood trolled trials demonstrated that Patient Blood Manage- Management outcomes [43], numerous Patient Blood ment significantly improves morbidity, mortality, and Management guidelines [17, 22–30], WHO endorsement average length of hospital stay, while reducing overall [18], call for Patient Blood Management [7], and several cost of care [12–15]. Clinical thought leaders urge that national policy recommendations, the global implemen- Patient Blood Management should be implemented as tation of Patient Blood Management is still alarmingly standard of care, and reduction of allogeneic blood prod- slow. Huge inter-center and inter-country transfusion uct utilization should serve as a marker for success [16, variability indicates, that blood utilization is rather 17]. In 2010, the World Health Organization (WHO) en- driven by culture and behavior than evidence [33, 34, dorsed Patient Blood Management [18] and the fourth 44–46]. Strategic Objective of the ‘WHO Action framework for Continuing to ignore the cumulative evidence puts life, blood products 2020-2023’ released in February 2020 well-being and safety of millions of hospitalized patients
Hofmann et al. BMC Health Services Research (2021) 21:634 Page 3 of 19
at risk. Delaying Patient Blood Management implemen- Patient Blood Management, and they were selected
tation also means that healthcare systems forego savings from the network of the authors, the International
of macro-economic magnitudes from a system-wide im- Foundation Patient Blood Management [50], and the
plementation of Patient Blood Management [15]. This is local networks of the industry or other interviewees.
even more alarming in countries striving towards Uni- The selection aimed to represent different clinical dis-
versal Healthcare Coverage and with severe resource ciplines (e.g., hematologists, anesthesiologists, sur-
constraints. In 2016, Eichbaum et al. compared the Pa- geons) and perspectives (e.g., clinical specialists, blood
tient Blood Management implementation status in four bank, policy, Patient Blood Management coordinator,
countries using a six-questions survey and observed con- industry). All interviews followed the structure of a
siderable variation between countries driven both by dif- newly developed questionnaire (Additional File 1).
ferences in health contexts and disparities in resources One question required rating of predefined barriers
[47]. They concluded that comparing Patient Blood between 0 (not important) and 4 (very important). To
Management strategies across low-, middle-, and high- allow the respondent to provide potentially unex-
income countries should foster mutual learning and pected answers, all other nine questions were formu-
implementing innovative, evidence-based strategies for lated open without prompting specific answers. The
improvement. survey was piloted with 11 interviewees and then fully
Following this recommendation, a more in-depth rolled-out after minor improvements in language and
questionnaire was developed in this study to gather, sequence of questions (survey flow). Most interviews
through interviews, the experiences of a diverse group of were conducted via web-communication (GoToMeet-
implementors of Patient Blood Management across ing™) by a single interviewer (AP Holtorf, Dr. rer. nat,
countries with different economic and healthcare con- female, without pre-existing relationship to the inter-
texts. The first aim was to describe the status-quo and viewees) in English language, two interviews were
chosen implementation approach in each of the surveyed conducted by a second qualified male interviewer in
countries, and to extract the drivers, barriers, measures, Chinese language after detailed briefing by the main
and stakeholders to be involved. The second aim of the interviewer. The interview questionnaire was provided
study was to analyze this information and synthesize it to the interviewees at least 1 week before the inter-
into an implementation framework for Patient Blood views. During the interviews, the interviewees verbally
Management which can serve as a comprehensive guid- consented to note-taking, recording, and publication
ance how to implement Patient Blood Management. of the results. The notes were revised using the re-
cordings and the interviewees had the opportunity to
review, correct or complement their initial responses.
Methods The COREQ checklist was applied to document
Semi-structured interviews mostly lasting 45–60 min transparent reporting of this interview-based qualita-
were conducted between November 2019 and May tive study and the completed form is available as
2020 with a multi-disciplinary group of 36 Patient Additional File 2 [51]. Qualitative content analysis
Blood Management implementors leading the imple- was performed for analysis and synthesis following
mentation of Patient Blood Management in their re- published guidance [52, 53]: 1.) Responses per coun-
spective environment. Ten countries from Latin try were extracted to a structured summary document
America, Central and Eastern Europe, Asia, Middle (from two to four interviews per country except for
East and Africa were selected to reflect experiences Switzerland with one). 2.) Responses from all coun-
from countries with different levels and types of tries regarding status-quo, approach of the implemen-
healthcare resources and system (national/ private tation, and 3.) drivers, barriers, measures, and
funders, public / private providers), and different de- stakeholders for Patient Blood Management were
velopmental stages of Patient Blood Management transferred in an electronic spreadsheet and coded
(from early stage to more advanced). In addition, guided by the items mentioned by the interviewees
Australia was chosen as a reference country, where (grounded theory approach). 4.) The coded responses
Patient Blood Management is adopted broadly and from step three were evaluated for the frequency of
supported through public health authorities since mentions (frequency analysis). 5.) Accelerating and
2008 and through National Patient Blood Manage- inhibiting factors were pooled and translated into im-
ment Guidelines since 2009 [15, 48, 49]. Likewise, a plementation measures (re-coding). 6.) Using an axial
Swiss reference case was included, where Patient coding approach [54], the measures were classified by
Blood Management is sustainably implemented across the interventional levels (policy/government, funding,
a leading hospital (University Hospital of Zürich). All research, healthcare provision, training/education, and
interviewees were actively involved in implementing public / patients). Steps 1 to 5 were conducted by theHofmann et al. BMC Health Services Research (2021) 21:634 Page 4 of 19
Table 1 Demographics of the interviewees. (1 expert could represent more than 1 perspectives. Therefore, the numbers in the
columns can add up to more than the number of experts). The survey was piloted with representatives of pharmaceutical
companies being actively involved in Patient Blood Management (Abdi Ibrahim, Genesis Pharma, Hikma, Sandoz Pharma, Takeda,
Vifor Pharma)
main interviewer and step 6 collaboratively by the Service and supported by a national Patient Blood Man-
authors. agement expert group [21].
Croatia, Greece and Lebanon seek the dual pathway,
Results although the current political situation in Lebanon has
Demographics put all governmental support to a halt. Brazil, Saudi Ara-
Thirty-six Patient Blood Management implementors, bia, and Switzerland currently rely on local clinician-led
named “Patient Blood Management Implementation initiatives (bottom-up).
Group” with 15 women and 21 men from 12 countries,
were interviewed following 11 pilot interviews (total of Drivers for the implementation of patient blood
47). The respective perspectives are depicted in Table 1. management (question 7A)
Of the 11 drivers mentioned unprompted during the in-
Current status and approach in implementing patient terviews (Fig. 1), patient outcomes (26 mentions), cost
blood management (question 3) savings (23 mentions), preventing or better dealing with
The country-level responses for the current level of Pa- blood shortages (16 mentions from Sth. Korea, Turkey,
tient Blood Management implementation and the ap- Mexico, China, Brazil), improving patient safety or redu-
proaches (top-down, bottom-up, or both approaches cing complications (15 mentions from Brazil, China, Sth.
simultaneously) are summarized in Table 2. Australia, Korea, Saudi Arabia, Turkey) were quoted most fre-
after initial bottom-up implementation in several leading quently. Several experts also mentioned national policy
public and private institutions, has fully implemented [8], education and awareness (concerning the risks of
Patient Blood Management supported by national insti- transfusion and benefits of Patient Blood Management)
tutions including the National Blood Authority (NBA), [7], and a quality assurance system [6].
the Australian Commission on Safety and Quality in Shorter length of hospital stays, better use of resources,
Healthcare, the Western Australia Department of and reduction of waste were only mentioned once each.
Health, and the Australian Red Cross Blood Service. In Patient demand was considered to become a driver once
South Korea, Patient Blood Management was imple- the risks related to transfusion and the benefits Patient
mented in few institutions about a decade ago, followed Blood Management were recognized more broadly in
by a broader strategic approach supported by national the general population.
authorities. In China, Turkey and Mexico, Patient Blood
Management implementation originated with leading Barriers for the Implementation of patient blood
clinicians (“champions”) of large national institutions management (question 6)
and is now increasingly recognized by the authorities. In Except for Australia, where Patient Blood Management
South Africa, the implementation of Patient Blood Man- is already widely adopted into practice, the need to
agement is led by the South African National Blood change work practice was rated as the most prominentTable 2 Summary of interview responses to the questions relating to the current status and approach to implementing Patient Blood Management on the national or local level
Australia Brazil China Croatia Greece Lebanon Mexico Saudi South South Korea Switzerland Turkey
Arabia Africa
AUS BRA CHN HRV GRE LBN MEX SAU ZAF KOR CHE TUR
Hofmann et al. BMC Health Services Research
Stage MATURE; INITIATION; ADVANCED; INITIATION; INITIATION; INITIATION; INITIATION; INITIATION; INITIATION; ADVANCED; INITIATION / ADVANCED;
National Policy; Scattered National Drive Specialist National individual national in some individual implementa-tion ADVANCED; Broad
Broad uptake individual society drive drive initiatives project and hospitals / initiatives. project; strong in some awareness
leadership through BB coordinator institutions PBM society hospitals / through cross-
institutions specialty
implementation
project
(2021) 21:634
Approach
Top NBA; States N.A. National Health MoH National BB Original National National N.A. National drive: Limited due EU Project for
Down Legal Commission, informed (with MoH) political project with interest collaboration to strong PBM
framework, PBM as part of Some and in drive Quality group, but program for federal implement-
standards & blood supply & coordination cooperation suspended certification not much pilots, data healthcare tation
guidance demand by specialist with hospital due to coordination collection, and policy
Quality strategy society managers political setting standards structure
certification (network) situation
Bottom Initially driven Individual Clinical Clinical/ de- Individual Individual Coordinated Introduced Individual Individual Strong in a Leading
up by individual Leadership champions in partmental initiatives in initiatives in bottom up in some initiatives initiatives in few leading institutions,
leadership and leading pilot champions some some hospitals / single hospitals hospitals broad
multi- hospitals hospitals / hospitals / institutions over past 10 based on awareness
disciplinary institutions institutions years individual through
teams in leadership specialist
hospitals societies
‘Mature’ describes a high level of implementation; ‘Advanced’ denotes a strategic, coordinated approach towards general implementation; ‘Initiation’ describes the occurrence of few individual initiatives with low level
of coordination
Abbreviations: BB Blood Bank, EU European Union, MoH Ministry of Health, N.A. Not available, NBA National Blood Authority, PBM Patient Blood Management
Page 5 of 19Hofmann et al. BMC Health Services Research (2021) 21:634 Page 6 of 19
barrier for the implementation of Patient Blood Manage- mentioned being low awareness, no funding for set-up
ment as shown in Table 3. The need for collaboration cost, education gaps, and stickiness of the old practice
and communication was rated equally important across (even stronger if combined with the responses for the
the countries, followed by the lack of experience with Pa- closely related resistance against change), lack of inter-
tient Blood Management, the feasibility to integrate Pa- disciplinary commitment, and resistance against change.
tient Blood Management into the current processes, and
strong belief in transfusion. Stakeholders (question 7B)
Sixty-three percent of the interviewees (29 of 46) identi-
Accelerators and inhibitors for the implementation of fied policy makers (National Health Council, Ministry of
patient blood management (question 7E) Health, etc.) as important stakeholders in Patient Blood
The responses for factors accelerating or supporting Management implementation. As shown in Fig. 3, the
Patient Blood Management implementation fell into majority also listed either specialists in general [22], or
24 categories as shown in Fig. 2 (left part). Gener- specific specialists (12 x anesthesiologists, 7 x hematolo-
ation of local data and evidence, education and gists, 5 x surgeons), 35% (16 of 46) included the hospital
training for Patient Blood Management, a national management. Other stakeholders (professional societies,
Patient Blood Management policy, and strong national or regional blood banks, payers, nursing staff,
thought leadership, were the most frequently men- enthusiastic champions, hospital pharmacists, patients/
tioned factors. Blood scarcity, funding, awareness of patient organizations, pharmaceutical companies, re-
transfusion risks, incentives for Patient Blood Man- searchers/academics, hospital champion, general practi-
agement engagement, belief and commitment of care tioners were mentioned less frequently or only in other
personnel, and quality assurance obligation were also parts of the interview (medical schools, non-
frequently mentioned. During the final six interviews governmental organizations, or the public at large).
between February and May 2020, the COVID-19
pandemic was newly mentioned as potential acceler- Coding and clustering of implementation measures
ator due to increased blood scarcity and potential After translating accelerators and inhibitors into action-
blood safety issues. able measures and clustering these measures by the type
The inhibitors or delaying factors fell into 22 categor- (level) of intervention, six levels for intervention were
ies (see Fig. 2, right part) with the most frequently identified: government/policy, funding, research,
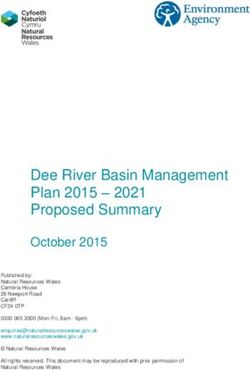
Fig. 1 Drivers for Patient Blood Management. Quantitative evaluation of all drivers mentioned by the interviewees when asked the question”
What could be the main drivers for Patient Blood Management – Why is Patient Blood Management needed?”. The responses were spontaneous
and unprompted. (N = 46) The driving factors were sorted by the total number of mentions (top to bottom decreasing). Note: The number of
mentions is not a measure for the strength of a specific driver. Education & Awareness is abbreviated for ‘education and awareness relating to
the risks of transfusion and the benefits of Patient Blood Management’Hofmann et al. BMC Health Services Research (2021) 21:634 Page 7 of 19
Table 3 Rating of Barriers for Implementation by perceived severity of the barrier. The rating was between 0 (is no barrier) and 4
(high barrier). The barriers were sorted by the average rating (top to bottom decreasing). (N = 35) Color coding: red for average
country values of 3 or higher, white for values between 2.01 and 2.99, and green for values of 2 or lower
healthcare providers, education/training, and public/pa- centered model of Patient Blood Management is that
tients. On each of the six levels specific measures can most diverse stakeholders need to communicate, collab-
contribute to the implementation of Patient Blood Man- orate and overcome the complexity of the Patient Blood
agement as reflected in Table 4 with reference to the Management implementation process. This starts with
concrete examples reported by the implementors. their specific contribution to the systemic implementa-
tion as summarized into the implementation matrix dis-
Discussion played in Fig. 4, which was derived from the full and
The challenge detailed collection of measures identified from the inter-
Unless translated into the daily routine and views (Table 4). We will discuss each level of the table in
organizational culture, evidence is of limited value [71]. more detail in the passages following below.
To bridge the gap and effectuate the necessary culture
change, it is essential to understand the drivers and bar- Using the Implementation matrix to develop patient
riers for Patient Blood Management as well as the stake- blood management strategies
holders’ roles and responsibilities. An essential challenge The Patient Blood Management-implementation matrix,
in replacing the long-standing, well-organized, product- as derived from the interviews, guides Patient Blood
centered culture of transfusion medicine by the patient- Management implementors in systematically identifying
Fig. 2 Accelerators and Inhibitors for Patient Blood Management. Quantitative evaluation of factors mentioned by the interviewees when asked
for the factors which would accelerate (Accelerators) or delay or inhibit (Inhibitors) the implementation of Patient Blood Management from their
perspective. The responses were spontaneous and unprompted. (N = 46) The items were sorted by the total number of mentions (top to bottom
decreasing). Note: The number of mentions is not a measure for the strength of a specific accelerator or inhibitorHofmann et al. BMC Health Services Research (2021) 21:634 Page 8 of 19
Fig. 3 Stakeholders Influencing Patient Blood Management Implementation. Quantitative evaluation of categories mentioned by the interviewees
to the question “Who in your opinion will be the essential stakeholders who will have to be involved / convinced?”. The responses were
spontaneous and unprompted. (N = 46) The stakeholder types were sorted by the total number of mentions (top to bottom decreasing). Note:
The number of mentions is not a measure for the importance of a specific stakeholder. Medical education, Non-governmental organization (NGO)
and the Public were not mentioned as important stakeholders specifically, but they were mentioned in other parts of the interview as important
groups and therefore were added for completeness
effective measures for Patient Blood Management imple- disciplinary national Patient Blood Management
mentation depending on the economic and healthcare guidelines form essential structural elements for driv-
context in their country. ing Patient Blood Management implementation
These measures will be discussed in more detail along nation-wide.
six implementation levels and consolidated in the final However, structural changes on government level
section into a Guided Implementation recommendation. usually require long time. One implementor stated “it
takes more than seven years to introduce a policy in
Government level our country”. Creating a sense of urgency through
Patient Blood Management is expected to improve qual- multiple stimuli, including success stories demon-
ity of care, reduce dependency on donor blood, and con- strated in pilots and the generation, publication, or
tribute to better access to healthcare and equity communication of the evidence, can help to overcome
(evidence-based blood preservation for all patients/citi- the inertness for introducing a new medical model
zens in the country). In Western Australia, hospital stays perceived as being complex [10].
were reduced by almost 70,000 days over 5 years [15].
Suchlike improvement enhances capacity of care and Healthcare provider level
consequently, patient access, and resource utilization. Patient Blood Management offers the rare opportunity
Likewise, the savings due to Patient Blood Management to improve patient outcomes while reducing resource
allow for better allocation of scarce resources, thus in- utilization and cost [15, 72, 73]. The healthcare provider
creasing productivity of the healthcare sector. This related measures reported by the implementors start
should motivate national policy makers to prioritize Pa- with the identification of local champions and allies from
tient Blood Management. clinical and non-clinical departments to create the suffi-
National policy makers and senior representatives of cient momentum and mass for the implementation. The
the Health Ministry are important stakeholders in co- securing of funding, information technology (IT) infra-
ordinating Patient Blood Management implementation structure and support to enable Patient Blood Manage-
nationally (see Fig. 3). Reporting and incentivization ment data collection, reporting and benchmarking was
of key performance indicators, accreditation of health- deemed equally necessary as establishing multi-
care providers for Patient Blood Management, Patient professional teams, Patient Blood Management commit-
Blood Management certification of clinicians, and tees, program coordinators and nurses. As recom-
funding and facilitating the development of multi- mended previously by others [19, 61] and aligned withHofmann et al. BMC Health Services Research (2021) 21:634 Page 9 of 19
Table 4 Summary of measures to consider for implementing PBM, sorted by level of intervention: Government (national and/or
regional), funding, research, healthcare provision, training/education, and patients
Measures Rational / Expectations Examples Points to consider
GOVERNMENT LEVEL (national or regional)
National Policy • National initiatives and guidance push • AUS: National policy for PBM and CHALLENGES
the hospitals towards PBM national measures to support • Changing of policy priorities; political
implementation implementation instability (LBN)
• TUR, KOR: Close collaboration of PBM • Policy priority of shifting from tertiary
leaders with MoH hospitals to primary care level
• TUR: qualification for a 3-yr EU grant antagonizes the pre-operative PBM in-
dedicated to a systematic country- terventions (CHN)
wide implementation of PBM [55] • National policy not a game changer in
• CHN: officially addressed the countries with decentralized healthcare
importance of PBM to improve clinical (CHE)
practice [56]
Blood Shortage • Actual and anticipated blood shortage is • ZAF, CHN, MEX: Frequent supply issues REMARK
recognized on a policy level and • HRV, GRE: Seasonal shortages • Impact of COVID-19 pandemic on
requires action; donation volume is • KOR, ZAF: Shortage and COVID-19 virus blood supply [58]
shrinking, the demand for blood is riska
increasing (aging population) • BRA: Zika-Virus [57]; supply issues in
• Donor deferrals due to new or re- public system
emerging pathogens; cancelled blood • AUS, TUR: Shortage predicted
collections due to lockdown during • LBN, GRE, MEX: Replacement modus
epidemics • CHN: 30% Reciprocal blood donation
• Family replacement schemes: mandatory
donations may increase risk and limit
access
Strong PBM • Fosters a broader country-wide accept- • KOR: Korean PBM Society with multi- REMARK
Thought ance and change disciplinary leadership function • May be difficult for few individuals to
Leadership • Liaise on policy level, engage with • TUR: EU-funded project for PBM imple- cover that scope and thus, formation
payers, engage specialist societies, and mentation across Turkey of a high-level work or interest group
introduce medical curricula may be advisable
PBM Incentives • Attract clinicians to become part of the • CRO: participation in international REMARKS
change clinical study • Involve practitioners actively in
• Increase level of experience and • TUR, KOR, MEX, ZAF: National pilots & research
familiarity with PBM research opportunities • Recognition of individual initiative
through active engagement and
authorship
National • Adapting international guidelines to • ZAF, TUR, KOR, MEX, BRA, HRV, CHN: RISK
Guidelines local healthcare context can be essential ongoing projects to locally adapt • Scattered / fragmented approaches
for acceptance international guidelines will make it difficult to consolidate in
• National guidance will facilitate best practice
coordinated and homogeneous activities
across the country
FUNDING LEVEL
Alignment of • Consensus for a reimbursement and • KOR: Center for Disease Control in the CHALLENGE
policy and funding solution MoH and the Health Insurance and • Heterogeneity in access to healthcare
funding Reimbursement Agency (HIRA) and its funding requires different
committed to PBM related projects (1) approaches for funding and
auditing the current level of reimbursement of PBM (MEX, LBN)
transfusion appropriateness in each
hospital, and (2) funding dedicated
projects on PBM implementation in
the country
Reimbursement • Increase the willingness to invest in • KOR, MEX, AUS, TUR: Funding national CHALLENGES
establishing PBM pilot or full implementation projects • Potential other sources of funding
• Adjust reimbursement systems to • BRA: volume-dependent reimburse- (NGOs, special international projects)
incentivize improved health outcomes ment to hospitals (fee for service) in- • Funding always compromised during
and efficiency and disincentivize centivizes a high use of transfusions; (economic) crises
transfusion volume [59, 60]. but first examples of capitation-based
hospital reimbursement emerge (sup-
portive for PBM)
Cost transparency • Mandate full cost transparency of • GRE, HRV: Not knowing the cost of REMARK
for blood; Cost transfusion and PBM to allow for cost- blood products or artificially low cost • Even if at zero cost to the hospital,
‘fairness’ effective allocation of (public) funds impedes adoption of PBM blood products are not for free from aHofmann et al. BMC Health Services Research (2021) 21:634 Page 10 of 19
Table 4 Summary of measures to consider for implementing PBM, sorted by level of intervention: Government (national and/or
regional), funding, research, healthcare provision, training/education, and patients (Continued)
Measures Rational / Expectations Examples Points to consider
societal perspective
Funding and • Secure funding necessary for setting up • HRV, GRE, LBN, MEX: Difficulties in REMARK
resources in the infrastructure (including point-of- securing funding despite principal • Use measures / local data to
hospital care testing devices, cell salvage equip- support for the concept demonstrate the realistic budget
ment, pre-operative anemia clinic, con- • BRA, LBN: Fee for service dis- needs, ROI, time frame required [61].
tinuous medical education (CME) and incentivizes PBM (imbalance between
training profitability and patient health)
• Identify and remove dis-incentives • Alignment across budgets: e.g.
pharmacy budget vs other cost
RESEARCH LEVEL
Quality • Use of quality measures, to track blood • KOR, MEX, CHE, AUS: pursuing quality REMARK
measurement/ use (i.e., units ordered, used, and and performance measurement • Performance measures empowers local
assurance discarded per hospital, ward, type of initiatives transfusion committees and PBM
intervention and individual specialists) to implementation task forces
shift focus to patient needs and
outcomes
Collecting and • Demonstrating impact of PBM with local • AUS, CHE, KOR: local data collection REMARKS
publishing local data on clinical outcomes, adverse systems initiated or established to • Local evidence helps to refute that the
data events or complications, enable reporting, benchmarking, or international experience may not be
• Capturing and reporting local performance analysis transferrable to the local context
epidemiology data (prevalence) • TUR: publication of local data [62] • Local research motivates participants
• Quantify opportunities, risks, and cost for to gain expertise and to become part
PBM in the local setting; ideally as multi- of the change
disciplinary intra- or inter-hospital
collaboration
Health-economic • To convince stakeholders of the cost- • Health-economic evidence from AUS, CHALLENGE
analyses effectiveness of PBM, analyses must be CHE, GER, and the USA [63, 64] • Current H/E evidence from countries
based on local data (cost / outcomes) with specific economic and health-
economic settings and may not be
generalizable
International • Cross-fertilize and share the learnings • International collaboration is frequent, REMARK
support and transnationally e.g. strong engagement of IFPBM & • Includes international teaching, web-
collaboration SABM, ZAF w. National Blood Authority based services, advisory exchange, or
in AUS, KOR w. AUS, BRA w. SABM. involvement of experts in another
country’s task forces.
HEALTHCARE PROVIDER LEVEL
Communication • Strengthen belief and commitment of • GRE: Generation of an intra-hospital A common vision and buy-in by those
clinical staff consensus and protocol with reporting who need to change their practice is es-
• Re-align all stakeholders around the system for restrictive blood use sential to achieve change [65]
transfusion process • MEX, ZAF, AUS: continuous
communication, involvement, and
feedback by coordinator / initiator in
hospital,
• ZAF, MEX: Chat-group in a social media
platform to report local experiences,
announce events, and post relevant
publications, questions. and
suggestions
Identify allies, • To increase clout and trust across • LBN: Expanding across specialties REMARKS
build teams specialties already in initial phase added great • PBM is a team effort [15, 21, 61]
• Foster multi-disciplinary collaboration, impetus MEX, TUR: Multidisciplinary • Supports forming a guiding coalition
mutual endorsement and support PBM Academies; LEB, KOR, ZAF: [65]
Multidisciplinary Iron Academies
Prior experience • Expand the knowledge and openness • Pilot projects in several hospitals/wards REMARK
with PBM for PBM by involving care personnel to involve and expose them to PBM • Overcome the stickiness of the old
from different disciplines in methods practice [66] and resistance to change
implementation projects
Ensure support • Design/align the organization to enable • Most initiatives reported that REMARKS
from hospital optimal and sustainable PBM across alignment with hospital administration • While small changes could be
administration specialties / CEO was improving chances for introduced individually or within one
• Secure funding for staff, systems support success specialty the full potential can only beHofmann et al. BMC Health Services Research (2021) 21:634 Page 11 of 19
Table 4 Summary of measures to consider for implementing PBM, sorted by level of intervention: Government (national and/or
regional), funding, research, healthcare provision, training/education, and patients (Continued)
Measures Rational / Expectations Examples Points to consider
(IT), other resources • HRV, GRE: Activities under achieved with multi-disciplinary
• Get approval to establish a multi- departmental responsibility may not change
disciplinary PBM committee need agreement by hospital • Understand the economic and system
management. incentives and to be in close
• LBN, SAU, HRV, LBN: To get funding for communication to collaboratively
establishing PBM was difficult and identify the path to implementation
therefore done within the existing (milestones, tasks, and responsibilities)
resources (overtime)
• BRA, MEX: dedicated project
management ensures planning and
roll out across specialties /
departments
Local champion • Responsible for planning, organizing and • HRV, GRE, MEX: general role in training, REMARK
(Medical Director directing PBM, supporting specialists, education, information, protocol • PBM coordinator can be a success
or project and ensuring continuous data collection, development factor for sustainability (AUS, CHE)
coordinator for reporting and benchmarking, • BRA: Change management
PBM) • AUS, CHE: organize PBM at patient
level (case management)
Hospital • Tailor PBM protocols to the specific • HRV, GRE, TUR, MEX, BRA: Several
protocols (SOPs) hospital context and routines interviewees reported the
• Increase local ownership across the development of local protocols before
disciplines, interdisciplinary commitment the availability of National Guidelines
Data collection, • Shows impact, measures gaps, and helps • ZAF, KOR: currently developing a
reporting & to improve quality of care monitoring system in hospital(s)
benchmarking
system
Nudging • Using IT or quality reporting systems to • AUS, CHF, MEX, ZAF reported use or REMARKS
clinicians & motivate and remind physicians to plan to use competitive forces or • Include IT and/or quality specialists in
stimulating practice PBM ‘nudging instruments’ to remind developing the local procedures for
competition • Using the competitive nature of people practitioners to improve their PBM mapping into data collection and
to motivate them to excel in PBM practices (reminders, league tables) analytical support tools
• Nudging = nonregulatory and
nonmonetary interventions that steer
people in a particular direction while
preserving their freedom of choice”
[67, 68]
Involving the • Alignment, participatory processes • ZAF: Importance of involving nurses REMARK
entire care team who have high influence on the • Includes nursing, hospital pharmacy,
patient care blood ordering process to ensure
• GRE: Importance of aligning the common goals
ordering of blood products.
Seizing local • Create momentum: Use opportunities in • HRV, LBN: Start within ward/ REMARK
opportunities for own environment for starting with department • Even small ‘wins’ will motivate people
improvement specific aspects of PBM • ZAF: start with communication &
• Move forward faster and prove success education of hospital specialists
• MEX, BRA: pilots
TRAINING & EDUCATION LEVEL
Education and • Identify and address knowledge gaps • AUS: Integration in medical school REMARKS
Training for PBM among specialists (University of Western Australia) • Training of all specialists concerned
• Update under-and postgraduate curriculum & exams (incl. anesthesiologist, intensive care
curricula • MEX, ZAF, TUR: PBM academies and/or specialists, surgeons, hematologists,
continued medical education (CME) for oncologists, gastroenterologists,
practitioners obstetricians & gynecologists) and
• AUS, ZAF: online training material [69] nursing staff in relation to benefits of
PBM,
• Avoid asymmetry in information to
prevent that ‘eminence wins over
evidence’ in the choice of therapy
Increase • Overcome eminence-based practice • Global: Many of the specialists who REMARKS
Awareness (“transfusion is always beneficial”) and in- administer transfusions during surgery • Necessitates re-education of all partici-
Transfusion Risks crease the knowledge about the associ- (surgeons, anesthesiologists) often pants in the transfusion decision
ated risks don’t see the mid- or long-term • Requires information, education, andHofmann et al. BMC Health Services Research (2021) 21:634 Page 12 of 19
Table 4 Summary of measures to consider for implementing PBM, sorted by level of intervention: Government (national and/or
regional), funding, research, healthcare provision, training/education, and patients (Continued)
Measures Rational / Expectations Examples Points to consider
complications (infections, immune re- reminders across specialties
actions, thrombosis). (publications and newsletters,
conferences, social media-channels)
Medico-legal • Strengthen the assertiveness of • BRA: Litigation is commonly used by
aspects and physicians relating to PBM patients to get access to procedures
protective which they perceive to be beneficial
measures as part
of PBM training
PATIENT & PUBLIC LEVEL
National • Develop awareness for PBM • KOR, LBN, ZAF: Initiated or conducted RISKS
information • Encourage patients to discuss PBM at national awareness campaigns through • If done too early, doctors might be
campaigns their doctor’s appointment important media channels overwhelmed by patient demand
• Prevent litigation against physicians • BRA: Litigation is commonly used by • Too much information on transfusion
following guideline-compliant restrictive patients to get access to procedures risks may negatively impact the
transfusion strategies which they perceive to be beneficial willingness of the public to donate
• Decrease patient demand blood blood
transfusion REMARK
• Involving patients, collaborating with
patients, and informing the public may
improve understanding and reduce
the risk for litigation
PAG initiatives • Co-create national information cam- • HRV, KOR: Initial contacts REMARKS
paigns (PBM thought leaders, politicians, • TUR: In contact with 5 NGO’s, who • PAG-patient interaction relating to
PAGs) receive regular information transfusion and/or PBM not yet
• Explore patient experiences and • GRE, LBN, HRV, KOR, BRA: increasing common
preferences demand for participatory medicine and • Co-creation / co-production: re-
• Engagement / advocating for PBM shared decision making by PAGs and/ searchers, practitioners and the public
insurance coverage or healthcare policy join efforts and share responsibilities to
• Achieve comprehensive patient develop, implement, monitor, evaluate
education on risks and benefits of all and re-develop interventions [70]
treatment options (including transfusion)
for anaemia, blood loss and
coagulopathy
• Ensure fully informed consent and/or
shared decision making
• PAGs to request PBM certification and/or
hospitals accreditation
Abbreviations: MoH Ministry of Health, SABM, https://sabm.org Society for the Advancement of Blood Management, ROI Return on Investment. Country
Abbreviations: AUS Australia, BRA Brazil, CHN Peoples Republic of China, HRV Croatia, GRC Greece, KOR Republic of Korea, LBN Lebanon, MEX Mexico, ZAF South
Africa, CHE Switzerland, TUR Turkey, PAG Patient Advocacy Group, IFPBM International Foundation Patient Blood Management, SABM Society for the Advancement
of Blood Management
a
The risk of COVID-19 viral infection only became apparent starting in January 2020. Hence, this threat was only mentioned in the last interviews (KOR, ZAF, SAU)
recognized approaches to change [74, 75], implementors ‘Nudging’ denotes “non-regulatory and non-monetary
preferred a piloting approach (“harvest low hanging interventions for changing behavior that steer people in
fruit”) accompanied by the development of internal cap- a particular direction while preserving their freedom of
ability, aiming to gain practical experience and to choice” [67, 68]. This includes automated or targeted re-
optimize the Patient Blood Management processes in minders, individual performance reviews based on local
the local context. Other important modules on the pro- data collection and analysis, or Patient Blood Manage-
vider level were developing Patient Blood Management ment dashboards as reported elsewhere [78].
standard operating procedures, defining key perform-
ance indicators, and measuring outcomes. Training and education level
Electronic clinical decision support systems for con- To avoid asymmetry of information and conflicting be-
trolling transfusions were deemed effective, also if com- haviors within the hospital, training, and communication
bined with systems to incentivize and reward the on Patient Blood Management needs to address the en-
progression towards Patient Blood Management. Elec- tire clinical staff including clinical specialists, nurses,
tronic transfusion decision support systems can effect- pharmacists, and others influencing decisions related to
ively reduce transfusion rate and index in the daily managing patients’ blood. Implementors suggested that
routine [76, 77] and serve as a ‘nudging’ mechanism. clinical knowledge and skills for Patient BloodHofmann et al. BMC Health Services Research (2021) 21:634 Page 13 of 19
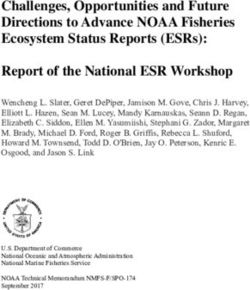
Fig. 4 Patient Blood Management Implementation Matrix. Implementation matrix summarizing the aims, measures, and expected outcomes of
comprehensive Patient Blood Management across six implementation levels. This implementation matrix is derived from the full table of
measures (Table 4). a) Equity: access to evidence-based blood preservation for all patients/citizens in the country
Management must be embedded in both under- and Management. Further research as well as national and
postgraduate education (curricula in medical schools, international exchange will help to improve Patient
accredited continuous medical education, Patient Blood Blood Management techniques as also highlighted by
Management academies, and e-learning- and international thought leaders [29, 61, 78, 79]. Most im-
information-platforms). However, except for Western portantly, as an essential prerequisite, the implementors
Australia, Patient Blood Management is currently not demanded to generate and communicate local evidence
part of the undergraduate curriculum of medical stu- (prove of outcomes and cost-effectiveness in the local
dents. Like Patient Blood Management preceptorships, context at local cost structures) to link the implementa-
educational and training activities for Patient Blood tion across hospitals and to foster policies on the na-
Management are currently organized for post-graduates, tional level.
often initiated by the implementors and local Patient
Blood Management champions, and mostly industry Funder level
sponsored. Implementors should liaise with the leader- Public funders may benefit from Patient Blood Manage-
ship of academia and medical schools to firmly integrate ment through reduced average length of hospital stay
Patient Blood Management into the undergraduate edu- and lower resource consumption, resulting in cost con-
cation in alignment with the federal Ministries of Health tainment and better resource use. Private funders may
and Education, where applicable. expect higher profitability, in particular with diagnosis
related groups (DRG) or value-based reimbursement sys-
Research level tems (e.g., accountable care): in DRGs with high anemia
Patient Blood Management offers a broad spectrum of prevalence and potentially high blood loss such as ob-
new experimental, clinical, epidemiological, and health- stetrics, cardiovascular surgery or oncology, the total
economic research opportunities, as evidenced by the cost per episode of care have shown to decrease over
growing number of research publications. Benchmarking time, thus leading to reduced tariffs [80]. For Germany,
and reporting of key performance indicators for Patient overall yearly cost-savings with elective surgery were cal-
Blood Management yield valuable insights concerning culated to be €1029 million - almost 1.58% of the total
clinical and economic outcomes related to Patient Blood national hospital budget [81].Hofmann et al. BMC Health Services Research (2021) 21:634 Page 14 of 19
Even in fee-for-service settings, funders may benefit potential for patient advocates to approach funders to
from Patient Blood Management: currently, they might incentivize and support Patient Blood Management.
reimburse hospitals for the number of transfusions ad- Potential risks were expected by one implementor
ministered, while patients pay for their anemia treatment when entering the public domain too early and thus,
out-of-pocket. Where transparent, implementors in the creating demand before physicians would be suffi-
interviews reported increasing cost of blood components ciently familiar with Patient Blood Management and
(per unit) due to increasing measures for quality and its benefit. Another implementor cautioned, that too
safety testing. Once funders begin incentivizing (pre-op- much information on transfusion risks may negatively
erative) anemia management as an essential part of Pa- impact on the willingness to donate blood. Involve-
tient Blood Management, they foster better outcomes, ment of patients or patient advocates should be
fewer complications, and shorter hospital stays, thus re- planned thoroughly within the country culture and
ducing the overall reimbursement cost per episode of context. However, the aim to involve patients more in
care as compared to the currently established transfu- their own care [87], the strive for ‘person-centered
sion preferences [15, 63]. The cost of quality assurance healthcare’ [88], and the priority of increased patient
and administering these blood products is a multifold of safety [89–91] conforms to physicians’ obligations to-
the actual acquisition cost and therefore, represents a wards educating and informing patients about all risks
substantial cost volume for the hospital and conse- and benefits of available treatment options. Medico-
quently for the funder, even where allogeneic blood legal experts increasingly caution that widespread dis-
products are covered by national funds and are consid- regard of transfusion associated risks for adverse out-
ered ‘free’ [82, 83]. comes may result in litigation against those neglecting
Appropriate reimbursement of Patient Blood Manage- physicians and specialists [92]. Informing the public
ment including anemia management was a strong re- and the patients in collaboration with patient advo-
quest in our interviews, and implementors even cacy groups can be a powerful element of the Patient
proposed to incentivize Patient Blood Management for Blood Management implementation strategy. Engaging
healthcare providers. Given the documented savings po- the public and patients will not only result in more
tential with Patient Blood Management [15, 64, 81, 84– demand for Patient Blood Management but also im-
86], it should be a priority for implementors to inform, prove patient satisfaction and foster participatory
educate and engage funders on this important issue. Fol- medicine.
lowing the example of the German health insurance
BARMER [80], insurers may even help underpinning the Guided Implementation
Patient Blood Management value using their own data In some of the countries described in this survey, Patient
to demonstrate savings with improved outcomes. Blood Management was implemented simultaneously
from bottom-up (e.g., from a department level or hos-
Patient level pital/clinical level) and top-down (driven by policy and/
According to the implementors, Patient Blood Manage- or hospital administrative leadership) (see Table 2) with
ment and its benefits are largely unknown to patients, large variation in the closeness of the interaction be-
despite being the ‘big winners’ from Patient Blood Man- tween policy and operational levels. In other countries,
agement with significantly improved clinical outcomes, implementation progresses just through the bottom-up
safety, and reduced average length of hospital stay. Pa- pathway, predominantly initiated, and led by individuals
tients usually seek medical treatment based on a proper or small groups with different clinical background or
diagnosis and expect to be treated with safe and effective innovation managers. To effectively coordinate and exe-
medical or surgical interventions. Unless being informed cute a statewide or even national implementation project
by their treating physician and being involved for shared across all six interdependent layers requires governance
decision making, they would not know that Patient [15, 20, 93]. Following the example of Western Australia
Blood Management improves their chances for earlier [15, 93], the EU Guide for Health Authorities [20] sug-
discharge from hospital and reduces their risk for hos- gests that National Patient Blood Management Steering
pital acquired infection or even mortality. Patient advo- Committees, preferably under the authority of the
cates could contribute by creating Patient Blood Health Ministry, should coordinate planning and provi-
Management awareness, but also by educating for and sioning of Patient Blood Management resources, struc-
defending patients’ rights. Collaborating and likewise, tural requirements, and national and international
supporting national campaigns to emphasize safety and Patient Blood Management research efforts. Transitional
the beneficial outcomes of Patient Blood Management, tasks forces were proposed to develop national Patient
could foster shared clinical decision making and in- Blood Management reimbursement schemes and man-
formed consent. Some implementors even saw the aging Patient Blood Management transition costs (i.e.You can also read