Key Concepts and Complications: Managing Cancer-Associated Thrombosis Disclosures - UNC Lineberger
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

UNC Lineberger Cancer Network Presented on January 19, 2022
Key Concepts and Complications:
Managing Cancer-Associated Thrombosis
Cassiopeia Frank, MMSc, PA-C
1
Disclosures
• Consultant for BMS/Pfizer x1
2
For Educational Use Only 1
UNC Lineberger Cancer Network Presented on January 19, 2022
Objectives:
• Define deep vein thrombosis (DVT) or pulmonary embolism (PE) based on
location, acuity, and severity.
• Implement an appropriate intervention for treatment.
• Identify risk factors for venous thromboembolism (VTE) and recurrence
and understand rationale for duration of anticoagulation.
3
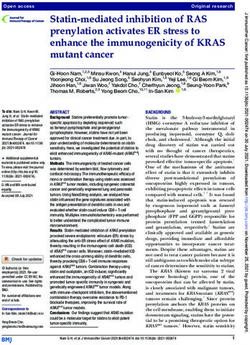
Defining the Clot - Location
• A venous clot can be superficial (superficial thrombophlebitis) or deep
(DVT).
• A DVT can be proximal (popliteal vein and above) or distal (below the
popliteal vein).
• In general, treatment duration and/or dosing is different depending on
these factors. There is somewhat less variation in the case of cancer-
associated thrombosis, as we will discuss.
This and other helpful material can be found at clotconnect.org
Illustrations courtesy of Dr. Stephan Moll, UNC Hematology
4
For Educational Use Only 2
UNC Lineberger Cancer Network Presented on January 19, 2022
Defining the Clot – Acute vs Chronic
• Venous Doppler can usually differentiate between acute and chronic features for DVT.
• It is less straightforward to determine the chronicity of PE, particularly if incidentally
found.
• In general, the appearance on imaging should be considered in conjunction with the
patient history.
• If questions arise, call radiology for clarification!
5
Pulmonary Embolism - 558 ESC Guidelines
European Heart Journal (2020) 41, 543"603
Definitions doi:10.1093/eurheartj/ehz405
RV RV LV
RV
IVC 2019 ESC Guidelines for
• Low-risk: No evidence of right heart strain. Ao RA
LV
LA RA
LV
management of acute p
• Submassive: evidence of right heart strain, B. Dilated RV with basal RV/LV C. Flattened intraventricle developed in collaborat
D. Distended inferior vena cava
A. Enlarged right ventricle,
parasternal long axis view ratio >1.0, and McConnell sign septum (arrows) parasternal with diminished inspiratory
without hemodynamic instability. (arrow), four chamber view short axis view
Respiratory Society (ER
collapsibility, subcostal view
• Massive: Hemodynamic instability, generally
Downloaded from https://academic.oup.com/eurheartj/article/41/4/543/5556136 by guest on 15 December 2021
RV RiHTh
M-Mode The Task Force for the diagnosis a
Tissue Doppler Imaging
S’
RV
hypotension/shock. RA TAPSE
pulmonary embolism of the Europ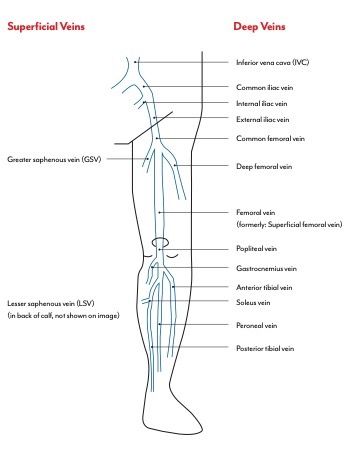
UNC Lineberger Cancer Network Presented on January 19, 2022
Case:
• 45 yo female with metastatic breast cancer and new left
lower extremity swelling and pain.
• Sent for lower extremity Doppler ultrasound:
• Acute obstruction of the left lower extremity femoral
vein at mid thigh, distal thigh, popliteal vein, posterior
tibial vein 1/2, and peroneal vein.
• No evidence of DVT in the RLE.
7
Step 1: Define the clot.
• Is this a proximal DVT or a
distal DVT?
• Is it acute or chronic?
Illustrations courtesy of Dr. Stephan Moll, UNC Hematology
8
For Educational Use Only 4UNC Lineberger Cancer Network Presented on January 19, 2022
552
... 3.3 Pathophysiology and d
Table 3 Predisposing factors for venous thromboembo- ..
lism (data modified from Rogers et al.23 and Anderson .. outcome
and Spencer24) ... Acute PE interferes with both circulation
..
Strong risk factors (OR > 10) .. ventricular (RV) failure due to acute pres
Fracture of lower limb
.. ered the primary cause of death in seve
..
Hospitalization for heart failure or atrial fibrillation/flutter .. pressure (PAP) increases if >30!50% of
.. area of the pulmonary arterial bed is oc
Step 2: Assess Risk Factors
(within previous 3 months) ..
Hip or knee replacement .. boli.57 PE-induced vasoconstriction, med
Major trauma ... thromboxane A2 and serotonin, contribu
.. in pulmonary vascular resistance (PVR)
Myocardial infarction (within previous 3 months) ..
Previous VTE .. obstruction and hypoxic vasoconstriction
.. lead to an increase in PVR, and a proport
Spinal cord injury ..
Moderate risk factors (OR 2!9) .. compliance.59
.. The abrupt increase in PVR results in RV
Arthroscopic knee surgery ..
.. contractile properties of the RV myocardiu
There are many risk factors with Autoimmune diseases
Blood transfusion
... mechanism. The increase in RV pressure
.. increase in wall tension and myocyte stretch
..
variable relevance.
Central venous lines
Intravenous catheters and leads
.. the RV is prolonged, while neurohumora
..
Chemotherapy .. tropic and chronotropic stimulation. Toge
.. constriction, these compensatory mec
Congestive heart failure or respiratory failure ..
Erythropoiesis-stimulating agents .. improving flow through the obstructed pu
.. thus temporarily stabilizing systemic blood
Cancer patients are more likely to be ... the extent of immediate adaptation
Hormone replacement therapy (depends on formulation)
In vitro fertilization ..
Oral contraceptive therapy .. preconditioned, thin-walled RV is unable
impacted by some of these risks due to
.. >40 mmHg.
Post-partum period ..
Infection (specifically pneumonia, urinary tract .. Prolongation of RV contraction time int
.. ventricle (LV) leads to leftward bowing of
illness and treatment –
infection, and HIV) .. 60
Inflammatory bowel disease .
.. tum. The desynchronization of the ventr
. by the development of right bundle branch
Cancer (highest risk in metastatic disease)
... ing is impeded in early diastole, and this m
i.e. infections, blood transfusions, Paralytic stroke
Superficial vein thrombosis
..
.. the cardiac output (CO), and contribute
.. and haemodynamic instability.61
trauma (surgery), etc. Thrombophilia
Weak risk factors (OR < 2)
..
.. As described above, excessive neurohum
.. be the result of both abnormal RV wall tens
..
Bed rest >3 days
.. The finding of massive infiltrates of inflamm
Diabetes mellitus .. cardia of patients who died within 48 h of a
Arterial hypertension ... by high levels of epinephrine released as a
Additionally, cancer itself is a risk factor Immobility due to sitting (e.g. prolonged car or air travel) ..
.. ‘myocarditis’.62 This inflammatory response
Increasing age .. dary haemodynamic destabilization that so
Laparoscopic surgery (e.g. cholecystectomy) ..
for VTE.1
.. after acute PE, although early recurrence o
Obesity .. ESC GUIDELINES
Pregnancy
.. explanation in some of these cases.
European Heart Journal (2020) 41, 543"603 .. Finally, the association between elevated
Varicose veins
doi:10.1093/eurheartj/ehz405 ..
. markers of myocardial injury and an advers
.
HIV = human immunodeficiency virus; OR = odds ratio; VTE = venous
.. that RV ischaemia is of pathophysiologica
thromboembolism.
Table – from ESC, citation... 1 phase of PE.63,64 Although RV infarction is
..
.. likely that the imbalance between oxygen
9
.. result in damage to cardiomyocytes, and f
2019 ESC Guidelines for the diagnosis andmellitus 44!47
—are shared with arterial disease, notably athe- ..
..
. forces. Systemic hypotension is a critical ele
. ing to impairment of the coronary driving p
rosclerosis.48!51 However, this may be an indirect association ..
management of acute pulmonary embolism mediated, at least in part, by the complications of coronary ..
. RV.
. The detrimental effects of acute PE on
artery disease and, in the case of smoking, cancer.52,53 ..
. the circulation are summarized in Figure 2.
developed in collaboration with the European
Myocardial infarction and heart failure increase the risk of ..
PE.54,55 Conversely, patients with VTE have an increased risk of ..
. Respiratory failure in PE is predomin
. haemodynamic disturbances.66 Low CO r
subsequent myocardial infarction and stroke, or peripheral arte- ..
Respiratory Society (ERS) rial embolization.56
.
..
the mixed venous blood. Zones of redu
The Task Force for the diagnosis and management of acute
pulmonary embolism of the European Society of Cardiology (ESC)
Authors/Task Force Members: Stavros V. Konstantinides* (Chairperson) (Germany/
Greece), Guy Meyer* (Co-Chairperson) (France), Cecilia Becattini (Italy), Héctor
Step 2: Assess Risk Factors Bueno (Spain), Geert-Jan Geersing (Netherlands), Veli-Pekka Harjola (Finland),
Menno V. Huisman (Netherlands), Marc Humbert1 (France),
Catriona Sian Jennings (United Kingdom), David Jiménez (Spain),
Nils Kucher (Switzerland), Irene Marthe Lang (Austria), Mareike Lankeit
(Germany), Roberto Lorusso (Netherlands), Lucia Mazzolai (Switzerland), Nicolas
!
Meneveau (France), Fionnuala N!ı Ainle (Ireland), Paolo Prandoni (Italy), Piotr
• This patient is receiving chemotherapy. Pruszczyk (Poland), Marc Righini (Switzerland), Adam Torbicki (Poland),
Eric Van Belle (France), and José Luis Zamorano (Spain)
• She was recently admitted (2 weeks ago) for 3 days for neutropenic fever, no source
identified.
* Corresponding authors: Stavros V. Konstantinides, Center for Thrombosis and Hemostasis, Johannes Gutenberg University Mainz, Building 403, Langenbeckstr. 1, 55131 Mainz,
Germany. Tel: þ49 613 117 6255, Fax: þ49 613 117 3456, Email: stavros.konstantinides@unimedizin-mainz.de; and Department of Cardiology, Democritus University of Thrace,
• She has not had a recent blood transfusion and she has not had surgery in 6 months.
68100 Alexandroupolis, Greece. Email: skonst@med.duth.gr. Guy Meyer, Respiratory Medicine Department, Hôpital Européen Georges Pompidou, 20 Rue Leblanc, 75015 Paris,
France. Tel: þ33 156 093 461, Fax: þ33 156 093 255, Email: guy.meyer@aphp.fr; and Université Paris Descartes, 15 rue de l’école de médecine 75006 Paris, France.
Author/Task Force Member Affiliations: listed in the Appendix.
• Risk factors for VTE:
ESC Committee for Practice Guidelines (CPG) and National Cardiac Societies document reviewers: listed in the Appendix.
1
Representing the ERS.
ESC entities having participated in the development of this document:
1) Active malignancy (metastatic breast cancer) Associations: Acute Cardiovascular Care Association (ACCA), Association of Cardiovascular Nursing & Allied Professions (ACNAP), European Association of Cardiovascular
Imaging (EACVI), European Association of Percutaneous Cardiovascular Interventions (EAPCI), Heart Failure Association (HFA).
Councils: Council on Cardiovascular Primary Care.
2) Recent hospitalization/immobility Working Groups: Aorta and Peripheral Vascular Diseases, Cardiovascular Surgery, Pulmonary Circulation and Right Ventricular Function, Thrombosis.
The content of these European Society of Cardiology (ESC) Guidelines has been published for personal and educational use only. No commercial use is authorized. No part of the
ESC Guidelines may be translated or reproduced in any form without written permission from the ESC. Permission can be obtained upon submission of a written request to Oxford
3) Recent infection University Press, the publisher of the European Heart Journal and the party authorized to handle such permissions on behalf of the ESC (journals.permissions@oxfordjournals.org).
Disclaimer. The ESC Guidelines represent the views of the ESC and were produced after careful consideration of the scientific and medical knowledge, and the evidence available
at the time of their publication. The ESC is not responsible in the event of any contradiction, discrepancy, and/or ambiguity between the ESC Guidelines and any other official recom-
4) Receiving Chemotherapy mendations or guidelines issued by the relevant public health authorities, in particular in relation to good use of healthcare or therapeutic strategies. Health professionals are encour-
aged to take the ESC Guidelines fully into account when exercising their clinical judgment, as well as in the determination and the implementation of preventive, diagnostic, or
therapeutic medical strategies; however, the ESC Guidelines do not override, in any way whatsoever, the individual responsibility of health professionals to make appropriate and accu-
rate decisions in consideration of each patient’s health condition and in consultation with that patient and, where appropriate and/or necessary, the patient’s caregiver. Nor do the
Risk factors for bleeding: None. ESC Guidelines exempt health professionals from taking into full and careful consideration the relevant official updated recommendations or guidelines issued by the competent public
health authorities, in order to manage each patient’s case in light of the scientifically accepted data pursuant to their respective ethical and professional obligations. It is also the health
professional’s responsibility to verify the applicable rules and regulations relating to drugs and medical devices at the time of prescription.
C The European Society of Cardiology 2019. All rights reserved. For permissions please email: journals.permissions@oup.com.
V
10
For Educational Use Only 5UNC Lineberger Cancer Network Presented on January 19, 2022
Step 3: Treatment
Do they have contraindications to anticoagulation?2
Absolute contraindications
Active bleeding (major)
Indwelling neuraxial catheters
Neuraxial anesthesia/lumbar puncture
Interventional spine and pain procedures
Relative contraindications
Chronic, clinically significant measurable bleeding >48 hours 6
Thrombocytopenia (platelet countUNC Lineberger Cancer Network Presented on January 19, 2022
Printed by Blanca Andino on 11/4/2021 8:53:29 PM. For personal use only. Not approved for distrib
Considerations for specific anticoagulants2: NCCN Guideline
Cancer-Associa
NCCN Guidelines Version 3.2021, Cancer- Associated Thromboembolic Disease
*Michael B. Streiff, MD/Chair ‡ Krishna Gu
The Sidney Kimmel Comprehensive Fred & Pam
Cancer Center at Johns Hopkins
Ibrahim Ibr
Bjorn Holmstrom, MD/Vice-Chair Þ UT Southwe
UFH Moffitt Cancer Center Center
DOACS: History of HIT
Dana Angelini, MD ‡ Eric Kraut,
LMWH: Case Comprehensive Cancer Center/
University Hospitals Seidman Cancer Center
Ohio State
Cancer Cen
and Cleveland Clinic Taussig Cancer Institute and Solove
Stage IV/V CKD: CrCl Andrew D.
CKD: Consider Aneel Ashrani, MD, MS ‡
UCSF HeleUNC Lineberger Cancer Network Presented on January 19, 2022
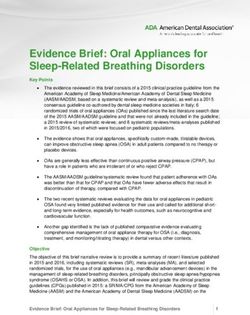
Case 2:
• 60 year old male with rectal cancer and new erythematous,
tender area with palpable cord along the medial thigh
• Sent for Doppler which demonstrate:
• Acute superficial vein thrombosis involving the great saphenous vein, 4cm
from the saphenofemoral junction.
15
Step 1: Define the clot
• Is the clot superficial or
deep?
• Is it acute or chronic?
Illustrations courtesy of Dr. Stephan Moll, UNC Hematology
16
For Educational Use Only 8UNC Lineberger Cancer Network Presented on January 19, 2022
Step 2: Assess risk factors
• This patient is receiving chemotherapy, has not recently been hospitalized, has not
had recent surgery, but has a BMI of 40. He has a family history of PE in his father.
• His risk factors:
1) Active malignancy (rectal cancer)
2) Obesity (BMI 40)
3) Family history of VTE
4) Receiving chemotherapy
17
Step 2: Assess Risk Factors - Bleeding
• This patient has rectal cancer and has a history of GI bleeding.
• He is not on any antiplatelet medications.
• He has normal platelets.
• He has normal renal function, CrCl 65ml/min
Risks for bleeding:
1) GI malignancy with history of GI bleeding
18
For Educational Use Only 9hypothesis generating and warrants attention in
90
15
future studies.
UNC Lineberger Cancer 80
Network Presented
Our trial has several on January
limitations. First, it was 19, 2022
Patients with Event (%)
70
10 Dalteparin an open-label trial to avoid the use of parenteral
60 placebo for 6 months. However, the numbers of
50 5
suspected recurrences of venous thromboembo-
Apixaban lism were similar in the two treatment groups,
40
0
and all suspected trial outcome events were cen-
30 0 30 60 90 120 150 180 trally adjudicated in a blinded manner. Second,
20 gastrointestinal bleeding was not a prespecified
10 trial outcome; however, after the publication of
0
results of studies of other direct anticoagulants,
0 30 60 90 120 150 180 such bleeding emerged as a relevant safety out-
Step 3: Treatment – Choice of Drug
No. at Risk
Days come. Third, patients with brain tumors, known
cerebral metastases, or acute leukemia were not
Dalteparin 579 507 462 417 383 352 217 enrolled for safety reasons, so our results cannot
Apixaban 575 522 481 453 424 399 241
be extrapolated to these patient groups. Finally,
• Recall
B Major – NCCN
Bleeding Guidelines caution against use of DOACs as with in the GI
large majority of studies regarding the
malignancies
treatment of venous thromboembolism, the sam-
• However… Caravaggio trial demonstrates similar bleeding
100 20
ple sizerisks of ourfor
trialapixaban
was poweredand
for the primary
dalteparin, 90 including in GI malignancies.4
outcome (recurrent venous thromboembolism)
15
80
T h e n e w e ng l a n d j o u r na l o f m e dic i n e and was not powered to make definitive conclu-
Dalteparin Apixaban
Patients with Event (%)
70
10 sions about bleeding.
60 Original Article Recurrent VTE The favorable 46/579 safety
(7.9%)profile that
32/576 (5.6%)for
we found
50 5 Dalteparin
Major Bleeding apixaban23/579 is in agreement
(4.0%) with the results
22/576 (3.8%) of
Apixaban for the Treatment of Venous Apixaban previous randomized trials of this drug with
40 Major GI Bleeding respect to10/579 (1.7%) of venous
the treatment 11/576 (1.9%)
thromboem-
Thromboembolism
30
0 Associated with Cancer
0 30 60 90 120 150 180 bolism in the general population. 10,17
Taken to-
Giancarlo Agnelli, M.D., Cecilia Becattini, M.D., Guy Meyer, M.D.,
20 M.D., Menno V. Huisman, M.D., Jean M. Connors, M.D.,
Andres Muñoz, gether, these findings may expand the propor-
Alexander Cohen, M.D., Rupert Bauersachs, M.D., Benjamin Brenner, M.D.,
10
Adam Torbicki, M.D., Maria R. Sueiro, M.D., Catherine Lambert, M.D., tion of patients with both cancer and venous
Gualberto Gussoni, M.D., Mauro Campanini, M.D., Andrea Fontanella, M.D.,
0 Giorgio Vescovo, M.D., and Melina Verso, M.D., thromboembolism who would be eligible for
0 for the30 60
Caravaggio Investigators* 90 120 150 180 treatment with apixaban, including patients with
Days gastrointestinal cancer. On the basis of these
A BS T R AC T
No. at Risk findings, we concluded that oral apixaban was
Dalteparin 579 510 473 430 387 355 222 noninferior to subcutaneous dalteparin for the
19 BACKGROUND
Apixaban
Recent 575recommend527
guidelines 490
consideration of the use of458 427or riva- The
oral edoxaban 402authors' affiliations
238 are listed in the
roxaban for the treatment of venous thromboembolism in patients with cancer. Appendix. Address reprint requests treatment
Dr. Agnelli at the Internal Vascular and
to of cancer-associated venous thrombo-
However, the benefit of these oral agents is limited by the increased risk of bleed- Emergency Medicine–Stroke Unit, Uni-
Figure 2. Recurrent
ing associated with their use.Venous Thromboembolism and Major Bleeding. embolism
versity of Perugia, Perugia 06124, Italy, or
without an increased risk of major
Shown
METHODS are cumulative percentages of patients with recurrent
at giancarlo.agnelli@unipg.it.
venous bleeding.
*A complete list of the investigators in
This was a multinational, randomized,
thromboembolism (Panel A) investigator-initiated,
and major bleeding open-label,
(Panelnoninfe-
B) who received
the Caravaggio trial is provided in the
riority trial with blinded central outcome adjudication. We randomly assigned Supplementary Appendix, available Supported at by the Bristol-Myers Squibb–Pfizer Alliance.
either
consecutive patients with cancer who had symptomatic or incidental acuteinsets
oral apixaban or subcutaneous dalteparin. The proxi- show
NEJM.org.the same Dr. Agnelli reports receiving lecture fees from Pfizer and
data on an thrombosis
mal deep-vein expanded or ypulmonary
axis. embolism to receive oral apixaban (at a This Bayer Healthcare and serving as chair of a registry for Daiichi
article was published on March 29,
2020, at NEJM.org.
dose of 10 mg twice daily for the first 7 days, followed by 5 mg twice daily) or
subcutaneous dalteparin (at a dose of 200 IU per kilogram of body weight once
Sankyo; Dr. Becattini, receiving lecture fees and consulting
N Engl J Med 2020;382:1599-607.
daily for the first month, followed by 150 IU per kilogram once daily). The treat- fees from Bayer Healthcare, Bristol-Myers Squibb, and Daiichi
DOI: 10.1056/NEJMoa1915103
Copyright © 2020 Massachusetts Medical Society.
ments were administered for 6 months. The primary outcome was objectively Sankyo; Dr. Meyer, receiving grant support and travel support
confirmed recurrent venous thromboembolism during the trial period. The prin-
assess the clinical benefit of a more extended from Leo Pharma, Bristol-Myers Squibb–Pfizer, Stago, and
Step 4: Treatment Duration2
cipal safety outcome was major bleeding.
Bayer Healthcare; Dr. Muñoz, receiving grant support, consult-
RESULTS treatment duration for venous thromboembo- ing fees, lecture fees, advisory board fees, and travel support
lism in these patients. In patients younger than from Sanofi and Celgene, lecture fees and advisory board fees
Recurrent venous thromboembolism occurred in 32 of 576 patients (5.6%) in the
apixaban group and in 46 of 579 patients (7.9%) in the dalteparin group (hazard
65interval
ratio, 0.63; 95% confidence years [CI], of
0.37 age,
to 1.07; apixaban was seen to be more from AstraZeneca, Servier, Bristol-Myers Squibb–Pfizer, Daiichi
P5cm
NCT03045406.)
1606
- SVT extends above knee n engl j med 382;17 nejm.org April 23, 2020
While the NCCN guidelines do not mandate longer-term
anticoagulationThe New England for Journal
this patient, his risk of recurrence and/or VTE
of Medicine
Anticoagulation
Downloaded from for at least
nejm.org at UNIV OF NC/ACQ is likely SRVCS on November
significant while 12, 2021.
he
1599
For personal to
continues usehave
only. No other uses
active without permission.
malignancy.
n engl j med 382;17 nejm.org April 23, 2020
3mo IF Copyright © 2020 Massachusetts Medical Society.
The New England Journal of Medicine
All rights reserved.
- SVT within Copyright 3cm ©of SFJ This
All rightssituation warrants discussion regarding risks and benefits of
Downloaded from nejm.org at UNIV OF NC/ACQ SRVCS on November 12, 2021. For personal use only. No other uses without permission.
2020 Massachusetts Medical Society. reserved.
anticoagulation considering both his episode of VTE/recurrence risk
Consider repeat ultrasound in and his bleeding risks.
7-10 days if SVTUNC Lineberger Cancer Network Presented on January 19, 2022
Case 3:
• 67 yo female with diffuse large B-cell lymphoma receiving chemotherapy
who presents with shortness of breath and pleuritic pain.
• Troponin negative, D-dimer 4,980
• Chest CTA:
• Acute pulmonary emboli involving bilateral lower lobe segmental and
subsegmental pulmonary arteries. No CT evidence of right heart
strain.
21
Step 1: Define the clot
• Acute pulmonary embolism, Low-Risk
• This episode was acute, with new sudden-onset symptoms.
• Her PE would be considered low-risk because:
• No evidence of right heart strain on CTA
• Negative troponin
22
For Educational Use Only 11UNC Lineberger Cancer Network Presented on January 19, 2022
Step 2: Assess Risk Factors
• This patient has DLBCL but is not obese (BMI 24), has no personal or family history of VTE, is
not on hormone therapy.
• Her risks:
1) Active malignancy (DLBCL)
2) Receiving chemotherapy
Risk factors for bleeding:
1) Thrombocytopenia associated with chemotherapy cycles
23
Step 3: Treatment – Choice of Drug
• Treatment for this episode would be the same as with proximal
DVT, as discussed above.
• However –
• This patient is receiving cytotoxic chemotherapy.
• On review of records, her platelets decline to 20-70 range with each cycle
of chemotherapy.
How do you manage her anticoagulation in the setting of recurrent
thrombocytopenia?
24
For Educational Use Only 12UNC Lineberger Cancer Network Presented on January 19, 2022
Printed by Cassiopeia Frank on 12/15/2021 3:44:00 PM. For personal use only. Not approved for distribution. Copyright © 2021 National Comprehensive Cancer Network, Inc., All Rights Reserved.
NCCN Guidelines Version 3.2021 NCCN Guidelines Index
Table of Contents
Cancer-Associated Venous Thromboembolic Disease Discussion
MANAGEMENT OF ANTICOAGULATION FOR VTE IN PATIENTS WITH CHEMOTHERAPY-INDUCED THROMBOCYTOPENIA
Venous Thr
ASCO
• Thrombocytopenia is a common occurrence in cancer patients receiving therapeutic anticoagulation for cancer-associated thrombosis.
decline below this threshold. Traditionally, physicians have transfused platelet concentrations to maintain platelet counts above 50,000/µL in Treatment i
special articles abstract
patients with thrombocytopenia on therapeutic anticoagulation, but this is not always feasible depending upon the duration and severity of
thrombocytopenia and availability of blood products.
Practice Gu
Management of Anticoagulation with
• When managing a patient with cancer-associated thrombosis with thrombocytopenia the provider should consider:
1. The patient’s risk for recurrent thromboembolism, and Nigel S. Key, MB ChB1; Alok A
Chemotherapy-Induced Thrombocytopenia2:
2. The patient’s risk of bleeding including the anticipated depth and duration of thrombocytopenia Juan I. Arcelus, MD, PhD6; Sa
Charles W. Francis, MD10; Lei
• For patients at high risk of recurrent thromboembolism (includes recent proximal DVT or PE [within 1 month], recurrent thromboembolism) Margaret A. Tempero, MD15; G
management options include:
• If high risk (i.e. within 1mo of VTE event, or history of recurrent VTE), consider PURPOSE To provide upd
transfusing to 50k or in rare cases, IVC filter.
• For patients at lower risk for recurrent thromboembolism (includes chronic DVT/PE [>1 month of treatment, central venous catheter-
associated DVT, upper extremity DVT, acute distal DVT) management options include:
(VTE) in patients with ca
Use lower dose anticoagulation as outlined below in table
METHODS PubMed and th
• For patients lower risk for recurrence, consider dose-reduction/holding
Remove central venous catheter in patients with central venous catheter-associated DVT analyses of RCTs publish
to review the evidence a
anticoagulation
as acute high-risk patient) as follows: RESULTS The systematic
on VTE risk assessment. T
Platelet Count Dose Adjustment Suggested Dose of Enoxaparin Alternative Once-Daily Dosing Regimen cancer reported that ed
>50,000/µL Full-dose enoxaparin 1 mg/kg twice daily 1.5 mg/kg daily compared
Printed by Blanca Andino on 11/4/2021 8:53:29 PM. For personal with
use only. Not low-molec
approved for distributio
Two additional RCTs repo
25,000–50,000/µL Half-dose enoxaparin 0.5 mg/kg twice daily — NCCN
risk of VTE. Guidelines
6 months) for patients with active
with metastatic disease or receiving Downloaded from ascop
rtainty in the evidence insertion for primary prevention or prophylaxis of pulmonary embolism (PE) or deep vein thrombosis due to its
cancer and VTE. RECOMMENDATION 32. For patients with active chemotherapy.
long-term harm concerns. It may be offered to patients with absolute contraindications to anticoagulant
Copyright © 20
cancer and VTE, the ASH guideline panel suggests long-term therapy in the acute treatment setting (VTE diagnosis within the past 4 weeks) if the thrombus burden was
ment of VTE (3-6 months) anticoagulation for secondary prophylaxis (.6 months) rather thanconsidered life-threatening. Further research is needed (Type: informal consensus; Evidence quality: low to
Downloaded from http://ashpublications.org/bloodadvances/article-pdf/5/4/927/1803860/a
deline panel suggests short-term treatment alone (3-6 months) (conditional recommen- intermediate; Strength of recommendation: moderate).
over VKA (conditional dation, low certainty in the evidence of effects ÅÅ◯◯). Recommendation 4.5. The insertion of a vena cava filter may be offered as an adjunct to anticoagulation in
ence of effects Å◯◯◯). patientsASH
with guidelines
progression of recommend
thrombosis (recurrent VTE or extension of existing thrombus) despite optimal
RECOMMENDATION 33. For patients with active cancer and VTE continued
anticoagulant therapy.anticoagulation
This is based on the inpanel’s expert opinion given the absence of a survival im-
reatment of VTE (3-6 receiving long-term anticoagulation for secondary prophylaxis, patients
provement, a limitedwith active
short-term cancer.
benefit, but mounting evidence of the long-term increased risk for VTE (Type:
ASH guideline panel the ASH guideline panel suggests continuing indefinite anti- informal consensus; Evidence quality: low to intermediate; Strength of recommendation: weak).
mmendation, moderate coagulation over stopping after completion of a definitive period
Recommendation 4.6. For patients with primary or metastatic CNS malignancies and established VTE, anti-
of anticoagulation (conditional recommendation, very low cer- coagulation as described for other patients with cancer should be offered, although uncertainties remain
ancer and incidental tainty in the evidence of effects Å◯◯◯). about choice of agents and selection of patients most likely to benefit (Type: informal consensus; Quality of
evidence: low; Strength of recommendation: moderate).
e ASH guideline panel RECOMMENDATION 34. For patients with active cancer and VTE
Recommendation 4.7. Incidental PE and deep vein thrombosis should be treated in the same manner as
ent rather than obser- requiring long-term anticoagulation (.6 months), the ASH guideline
symptomatic VTE, given their similar clinical outcomes compared with patients with cancer with symptomatic
low certainty in the 26 panel suggests using DOACs or LMWH (conditional recommen- events (Type: informal consensus; Evidence quality: low; Strength of recommendation: moderate).
dation, very low certainty in the evidence of effects Å◯◯◯). (continued on following page)
cer and subsegmental Values and preferences
gests short-term anti-
conditional recommen- The guideline panel rated mortality, PE, deep venous thrombosis
ects Å◯◯◯). (DVT), and major bleeding as critical for decision498
making
© 2019and placedSociety of Clinical Oncology
by American Volume 38, Issue 5
a high value on these outcomes and avoiding them with the
For Educational Use Only
cancer and visceral/
deline panel suggests
interventions that were evaluated.
Downloaded from ascopubs.org by 75.165.156.173 on December 10, 2021 from 075.165.156.173
13
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.
observing (conditional Explanations and other considerationsUNC Lineberger Cancer Network Presented on January 19, 2022
Case 5:
• 75 year old male with metastatic lung cancer who presents with newly
diagnosed left upper lobe and left lower lobe segmental pulmonary
emboli incidentally found on monitoring CT.
• Last prior CT was 3 months ago and no emboli were present
• He is asymptomatic.
27
Step 1: Define the clot
• CTA with PE, no evidence of right heart strain
• Troponin was not performed
• No echo
• Given no symptoms, incidentally found, and no CT evidence of right
heart strain, this would be considered a low-risk PE.
28
For Educational Use Only 14UNC Lineberger Cancer Network Presented on January 19, 2022
Key et al
THE BOTTOM LINE (CONTINUED)
of active bleeding or high bleeding risk (Type: evidence based; Evidence quality: intermediate; Strength of
recommendation: strong).
Recommendation 3.4. A combined regimen of pharmacologic and mechanical prophylaxis may improve ef-
ficacy, especially in the highest-risk patients (Type: evidence based; Evidence quality: intermediate; Strength
Step 2: Assess Risk Factors
of recommendation: moderate).
Recommendation 3.5. Pharmacologic thromboprophylaxis for patients undergoing major surgery for cancer
should be continued for at least 7 to 10 days. Extended prophylaxis with LMWH for up to 4 weeks post-
operatively is recommended for patients undergoing major open or laparoscopic abdominal or pelvic surgery
for cancer who have high-risk features, such as restricted mobility, obesity, history of VTE, or with additional
Venous Thromb
ASCO
Patient
risk•factors. is 72 years
In lower-risk old with
surgical settings, a BMI on
the decision ofappropriate
23. Non-smoker. No family should
duration of thromboprophylaxis
history of DVT. Has been receiving chemotherapy.
be made on a case-by-case basis (Type: evidence based; Evidence quality: high; StrengthHas a port
of recommen- Treatment in Pa
special articles abstract
which has been
dation: moderate to strong). present for 1 year without issues. No recent
travel. Last hospitalization for pneumonia 6mo ago.
Clinical Question 4. What is the best method for treatment of patients with cancer with established VTE to prevent
Practice Guidel
• Risk factors: Nigel S. Key, MB ChB ; Alok A. Khorana, 1
recurrence? Juan I. Arcelus, MD, PhD ; Sandra L. Won 6
Recommendation 4.1. Initial anticoagulation may involve LMWH, UFH, fondaparinux, or rivaroxaban. For Charles W. Francis, MD ; Leigh E. Gates 10 1
1) Active malignancy (metastatic
patients initiating treatment with parenteral
lung LMWH
anticoagulation,
cancer) is preferred overcancer
UFH for the
Margaret A. Tempero, MD ; Gary H. Lym 15
RECOMMENDATION 22. For patients with andinitial
VTE, 5 tothe ASH
continuing wit
10 2)
daysReceiving chemotherapy
of anticoagulation for the patient with cancer with newly diagnosed VTE who does not have severe
guideline panel suggests LMWH over
renal impairment (defined as creatinine clearance less than 30 mL/min) (Type: evidence based; Evidence
fondaparinux for initial
PURPOSE To very
providelow certa
updated reco
treatment of
quality: high; Strength of recommendation: VTE for patients with cancer (conditional recommen-
strong).
(VTE) in patients with cancer.
METHODS PubMed RECOMMEND
Risk factors
Recommendation forlong-term
4.2. For bleeding:
dation, 1) Age
very
anticoagulation, lowLMWH,certainty in the
edoxaban, evidenceforofateffects
or rivaroxaban Å◯◯◯
least 6 months are ).
and the Cochra
analyses of RCTs published from A
preferred because of improved efficacy over vitamin K antagonists (VKAs). VKAs are inferior but may be used to review the VTE despite
evidence and revisea
if LMWH or direct oral anticoagulants (DOACs) are
Short-term not accessible.
treatment forThere is an increase
patients withinactive
major bleeding
cancer risk (initial RESULTS suggests
The systematic not
review inc
on VTE risk assessment. Two RCTs
with DOACs, particularly observed in GI and potentially genitourinary malignancies. Caution with DOACs is a filter (condan
3-6 months). RECOMMENDATION 23. For the short-term treatment of
also warranted in other settings with high risk for mucosal bleeding. Drug-drug interaction should be checked
cancer reported that edoxaban
VTE (3-6
prior to using a DOAC (Type: evidence months)
based; Evidence forquality:
patientshigh; with
Strengthactive cancer, the ASH
of recommendation: strong).guideline
evidence of e
compared with low-molecular-weig
Two additional RCTs reported on DO
29Recommendation 4.3. Anticoagulation with LMWH, DOACs, or VKAs beyond the initial 6 months should be risk of VTE.
panel suggests DOAC (apixaban, edoxaban, or rivaroxaban) over
offered to select patients with active cancer, such as those with metastatic disease or those receiving Long-term
RECOMMENDATIONS Changes totr p
LMWH (conditional recommendation, low certainty in the evidence apixaban, rivaroxaban, or LMWH
chemotherapy. Anticoagulation beyond 6 months needs to be assessed on an intermittent basis to ensure have beencanceradded as options and for VT
a continued favorable risk-benefit of effects ÅÅ◯◯
profile (Type: ).
informal consensus; Evidence quality: low; Strength of treatment section; and the recom
Re-affirmed recommendations: V
cancer and M
recommendation: weak to moderate).
RECOMMENDATION 24. For the short-term treatment of VTE (3-6 months) anticoagulatio
require thromboprophylaxis throu
Recommendation 4.4. Based on expert opinion in the absence of randomized trial data, uncertain short-term for all outpatients with cancer. Pat
benefit, and mounting evidencefor patientsharm
of long-term with fromactive
filters, cancer,
the insertion theof aASH
vena cava guideline not besuggests
panel
filter should before surgeryshort-term
and continuingtre for
for VTE risk, and oncology profes
DOAC
offered to patients with established (apixaban,
or chronic thrombosisedoxaban, or rivaroxaban)
(VTE diagnosis more than 4 weeks over ago),
VKAnor (conditional
to
ASSOCIATED
of VTE. dation, low ce
Step 3: Treatment – Choice of Drug and
patients with temporary contraindications to anticoagulant
recommendation, verytherapy (eg, surgery).
low certainty There
in the also is no of
evidence
insertion for primary prevention or prophylaxis of pulmonary embolism (PE) or deep vein thrombosis dueData
forCONTENT
Appendix Å◯◯◯Additional
roleeffects
filter
toSupplement
its
). information is available
RECOMMEND
Step 4: Duration of Therapy
long-term harm concerns. It may RECOMMENDATION
be offered to patients25with . For the contraindications
absolute short-term treatment of
to anticoagulant
Author VTE
affiliations (3-6
and support
J Clin Oncol 38:496-520. © 2019 by Ameri
INTRODUCTION
receiving lon
therapy in the acute treatmentmonths)
setting (VTEfor diagnosis within the past 4 weeks) if
patients with active cancer, the ASH guidelinethe thrombus burden was
information (if
panel the ASH gui
• We have life-threatening.
considered reviewed drug Further options
research is – needed
DOAC,(Type: LMWH… informalbut…consensus; Evidence quality: low applicable) appear
to Venous thromboembolism (VTE)
suggests LMWH
intermediate; Strength of recommendation: moderate). over VKA (conditional recommendation, article.
moderate
at the end of this deep vein coagulation
thrombosis (DVT) and o
3,5
For incidentally
•Recommendation found
4.5. The insertionVTE,
certainty do
of a vena you
in cava treat
the filter
evidence at
may be ofall? effects
offered as anÅÅÅadjunct ◯ ).
to anticoagulationAccepted on June 4,
in
lism (PE), is an important cause
mortality of
among anticoagul
patients with canc
2019 and published at
cancer are significantly more like
patients with progression of thrombosis (recurrent VTE or extension of existing thrombus) despite optimal
RECOMMENDATION 26. For patients with cancer and
ascopubs.org/journal/
jco on incidental
August 5, than people tainty in the
without cancer 3
and e
anticoagulant therapy. This is based on the panel’s expert opinion given the absence of a survival 2019:im-DOI https://doi. rates of VTE recurrence and blee
provement, a limited short-term(unsuspected)
benefit, but mounting pulmonary
evidence of embolism
the long-term(PE),increasedtherisk
ASH guideline
for VTE (Type: panel
org/10.1200/JCO.19.
01461
during VTE treatment.RECOMMEND
4,5
informal consensus; Evidencesuggests
quality: low to short-term
intermediate;anticoagulation treatment
Strength of recommendation: ratherClinical
weak). than obser-
Practice Comprehensive requiring
management long- of V
Committee cancer includes both the identifica
Recommendation 4.6. For patients with primary or metastatic CNS malignancies and established VTE,Guideline anti- May
vation (conditional recommendation, very low certainty approval: in the are most panel sugges
likely to benefit from p
coagulation as described for other patients with cancer should be offered, although uncertainties remain 16, 2019.
phylaxis as well as the effective trea
evidence
about choice of agents and selection of effects
of patients Å◯◯◯
most likely ). (Type: informal consensus; Quality
to benefit Reprint
ofRequests:
2318 Mill Rd, Suite
dation, very
risk of VTE recurrence and mortal lo
lished a guideline on these topics in
evidence: low; Strength of recommendation: moderate). 800, Alexandria, VA
RECOMMENDATION 27. For patients with cancer and subsegmental in 20137 and 2015.8 The 2015
the 2013 Values and
22314; guidelines@
Recommendation 4.7. Incidental PE and deep vein thrombosis should be treated in the same manner as
asco.org. recommendations. Th
PE (SSPE),
symptomatic VTE, given their similar the compared
clinical outcomes ASH guideline with patients panel suggests
with cancer short-term anti-
with symptomatic
events (Type: informal consensus; coagulation treatment
Evidence quality: rather than
low; Strength observation (conditional
of recommendation: moderate). recommen- The guideline
(continued on following page) (DVT), and ma
dation, very low certainty in the evidence of effects Å 496 ).Volume 38, Issue 5 ◯◯◯
a high value
Downloaded from ascopubs.org by
Copyright © 2021 America
RECOMMENDATION 28.For patients with cancer and visceral/ interventions t
30 splanchnic vein thrombosis, the ASH guideline panel suggests
498 © 2019 by American Society of Clinical Oncology treating with short-term anticoagulation or observing
Volume 38,(conditional
Issue 5
Explanation
recommendation, very low certainty in the evidence of effects Å◯◯◯).
Downloaded from ascopubs.org by 75.165.156.173 on December 10, 2021 from 075.165.156.173
These recomm
RECOMMENDATION
Copyright © 2021 American 29. For
Society of Clinical Oncology. patients
All rights reserved. with cancer
with CVC-related effectiveness,
For Educational Use Only VTE receiving anticoagulant treatment, the ASH guideline panel 15
Good pract
suggests keeping the CVC over removing the CVC (conditionalUNC Lineberger Cancer Network Presented on January 19, 2022
Case 6:
• 55 year old female with uterine cancer presents with three days of
worsening left upper arm swelling, pain, and tenderness. She has
a PICC line in the left arm.
31
Step 1: Define the clot
• Venous Dopplers are obtained and confirm thrombosis:
• Acute obstruction in the left brachial vein, axillary vein. Other
veins fully compressible.
Is this a deep or superficial vein thrombosis?
32
For Educational Use Only 16UNC Lineberger Cancer Network Presented on January 19, 2022
Illustrations courtesy of Dr. Stephan Moll, UNC Hematology
33
Step 2: Assess the risk factors
• This patient has been receiving chemotherapy for her uterine cancer. She
had surgery 3 weeks ago as an outpatient. Her BMI is 32. She is not on any
hormone therapy. She has not recently traveled. She has not recently
traveled. She has no family history of VTE. She has not been on any recent
hormone therapies.
• Risk Factors for VTE:
1) Active malignancy (uterine cancer)
2) Chemotherapy
3) Recent surgery
4) Obesity
5) PICC line
Risk factors for bleeding: None.
34
For Educational Use Only 17UNC Lineberger Cancer Network Presented on January 19, 2022
Step 3 & 4: Treatment and Duration2
Printed by Cassiopeia Frank on 12/15/2021 3:44:00 PM. For personal use only. Not approved for distribution. Copyright © 2021 National Comprehensive Cancer Network, Inc., All Rights Reserved.
NCCN Guidelines Version 3.2021 NCCN Guidelines Index
Table of Contents
Acute Deep Vein Thrombosis (DVT) Discussion
If no contraindication to
CATHETER-RELATED DVT: DIAGNOSIS AND TREATMENT anticoagulation
• Choice of drug – as reviewed,
DIAGNOSIS WORKUP/IMAGING TREATMENT
DOAC or LMWH would be
• Anticoagulation for at least 3 months or as long as central
venous access device (CVAD) is in placec,e,k
recommended. No contraindication to • Consider catheter removal if symptoms persist or if the catheter
anticoagulationd is infected or dysfunctional or no longer necessary
• Consider catheter-directed therapy (pharmacomechanical
• With this patient, what is the thrombolysis or mechanical thrombectomy) in appropriate
candidatesf,h,l
appropriate management of DVT Anticoagulation
Contraindication
Clinical for at least 3
resolved
suspicion of Remove Follow for monthsc,e,k
the PICC line?
catheter-related • Venous US catheter change
DVT: • CT venogram or follow in contra-
Contraindication to
• Unilateral with contrast with indication
anticoagulation
arm/leg • MRV with serial as clinically
swelling contrast imaging indicated
• Pain in supra- • X-ray Re-evaluate for
Contraindication
clavicular venogram persists j
space or neck with contrast anticoagulation
Printed by Blanca Andino on 11/4/2021 8:53:29 PM. For personal use only. Not approved for distribution. Copyright © 2021 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Evaluate for other causes
If contraindication to
• Dysfunctional • Consider further diagnostic imaging/testing
catheter anticoagulation No DVT
if initial testing is unrevealing and clinical NCCN
NCCN Guidelines
Guidelines Version 3.2021, Version Cancer- 2.2021
suspicion remains high Associated
Cancer-Associated Thromboembolic Disease Venous Thromboembolic Dise
c See Therapeutic Anticoagulation for Venous Thromboembolism (VTE-D).
d See Contraindications to Therapeutic Anticoagulation (VTE-E). See
35 Management of Anticoagulation for VTE in Patients with Chemotherapy-Induced
Thrombocytopenia (VTE-F).
*Michael B. Streiff, MD/Chair ‡
h See Contraindications to Thrombolysis
The Sidney Kimmel
j See Elements
Krishna Gundabolu, MD ‡
Comprehensiveand Indications
Fred for Thrombolysis
& Pamela (VTE-I).
Buffett Cancer Center
Colleen Morto
Vanderbilt-Ing
Cancerfor Consideration
Center in Decision Not to Treat (VTE-J).
at Johns Hopkins
e See Therapeutic Anticoagulation Failure (VTE-G), if extension of VTE or new k Anticoagulation without catheter removal is the preferred
Ibrahimoption for MD
Ibrahim, initial
‡ Thomas L. Or
VTE while on recommended anticoagulation therapy. Bjorn
treatment, even Holmstrom, MD/Vice-Chair
for patients Þ
with symptomatic DVT,UT Southwestern
provided Simmons
that the catheterComprehensive
is Caner Duke Cancer
Moffitt Cancer Center
f Choice of regimen should be made based on institutional expertise/preferences necessary, functional, and free of infection. There isCentervery little clinical evidence Rita Paschal,
in conjunction with interventional radiology or vascular surgery colleagues. See regarding theAngelini,
Dana appropriate
MD ‡duration of anticoagulation. EricThe
Kraut, MD ‡
recommended duration O'Neal Compr
Thrombolytic Agents (VTE-H). Appropriate candidates may include: patients Case Comprehensive
of anticoagulation depends onCancer Center/
patient Ohio State University
tolerance of anticoagulation, Comprehensive
response to
University Hospitals Seidman Cancer Center Cancer Center - James Cancer Hospital Jordan Schae
at risk of limb loss (eg, phlegmasia cerulea dolens), patients who demonstrate anticoagulation, and catheter
and Cleveland status.
Clinic Taussig Consider
Cancer longer
Institute andduration anticoagulation
Solove Research Institute in University of M
central thrombus propagation in spite of anticoagulation, and those with moderate patients with poor flow, persistent symptoms, or unresolved thrombus. Consider
Aneel Ashrani, MD, MS ‡ Andrew D. Leavitt, MD ‡ Sanford Shat
to severely symptomatic proximal DVT. Candidates with high bleeding risk or shorter duration of anticoagulation if clot or symptoms UCSFresolve
Helen in response
Diller Family to
Mayo Clinic Cancer Centerremoval. UC San Diego
contraindication to fibrinolytic may be candidates for percutaneous mechanical anticoagulation and/or catheter Comprehensive Cancer Center
thrombectomy. l See Mechanical Thrombectomy Devices (VTE-H, 2 of 2). Tanya Siddiq
Amro Elshoury, MD ‡ Alfred Lee, MD, PhD ‡
Roswell Park Comprehensive Cancer Center City of Hope N
Yale Cancer Center/Smilow Cancer Hospital
Note: All recommendations are category 2A unless otherwise indicated. Deepak Sudh
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials and
Dana-Farber/Brigham is especially
Women’sencouraged. Jason T. Lee, MD ¶ Abramson Ca
Cancer Center Stanford Cancer Institute at the Univers
Take-home points:
DVT-3
Version 3.2021, 11/15/21 © 2021 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form withoutFertrin,
Kleber Yotsumoto the expressMD,
written ‡ of NCCN.Ming
permission
PhD Lim, MD ‡ Eliot Williams
Fred Hutchinson Cancer Research Center/ Huntsman Cancer Institute at the University of Utah University of W
Seattle Cancer Care Alliance Carbone Canc
Annemarie E. Fogerty, MD ‡ † Siteman Cancer Center at Barnes-Jewish Hospital
Massachusetts General Hospital and Washington Unviersity School of Medicine
Cancer Center
Karlyn Martin, MD ‡
Shuwei Gao, MD Þ Robert H. Lurie Comprehensive Cancer Center of
The University of Texas Northwestern University
MD Anderson Cancer Center NCCN
Brandon McMahon, MD ‡
Samuel Z. Goldhaber, MD University of Colorado Cancer Center Mai Nguyen,
Dana-Farber/Brigham and Women’s Liz Hollinger,
John Moriarty, MD
Steps in managing newly Cancer Center
UCLA Jonsson Comprehensive Cancer Center Cardiology
diagnosed DVT include: Renal function is a critical For most acute DVT/PE in ‡ Hematology/
consideration in choice of patients with active Hematology
1) Define the clot Anticoagulation with DOAC or anticoagulant.2 malignancy, recommendation
oncology
Þ Internal medic
2) Assess risks LMWH is preferred. Either is
usually appropriate.2,3 Cost is also an important
NCCN Guidelines Panel Disclosures is indefinite Continue
anticoagulation Interventional
radiology
3) Determine treatment factor. For DOACs, copay until no active malignancy/not † Medical oncolo
cards are widely available. receiving chemotherapy.3,5
4) Determine duration
Version 2.2021, 8/16/21 © 2021 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of
Anticoagulation must be
Incidentally found DVT/PE managed closely in patients Line-associated DVT can often
should be treated in patients with chemotherapy-induced be managed without removing
with active malignancy.3,5 CVAD.2
thrombocytopenia.2
36
For Educational Use Only 18UNC Lineberger Cancer Network Presented on January 19, 2022
UNC DVT Walk-In Program
• Rapid follow-up for patients with newly
diagnosed DVT.
• Ensure anticoagulation is started,
appropriate, affordable, and that patient
receives education.
• Located at UNC Eastowne
• 100 Eastowne Drive, Chapel Hill, NC
• Can place referral within the UNC system.
• Hope to expand to accept referrals outside
UNC in 2022.
37
Citations
1. Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP, Huisman MV, Humbert M, Jennings CS, Jiménez D, Kucher N, Lang IM, Lankeit M,
Lorusso R, Mazzolai L, Meneveau N, Ní Áinle F, Prandoni P, Pruszczyk P, Righini M, Torbicki A, Van Belle E, Zamorano JL; ESC Scientific Document Group. 2019
ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur
Heart J. 2020 Jan 21;41(4):543-603. doi: 10.1093/eurheartj/ehz405. PMID: 31504429.
2. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology, Cancer-Associated Venous Thromboembolic Disease. Version 3.2021 –
November 2021. NCCN.org
3. Lyman, G et al. American Society of Hematology 2021 guidelines for management of venous thromboembolism: prevention and treatment in patients with
cancer. Blood Advances, 5;4. February 2021.
4. Agnelli et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. New England Journal of Medicine. 282;17. April 23, 2020.
5. Key et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Clinical Practice Guideline Update. Journal of Clinical Oncology.
38;5. August 5, 2019.
6. Samuelson Bannow, BT, et al. Management of cancer-associated thrombosis in patients with thrombocytopenia: guidance from the SSC of the ISTH. Journal of
Thrombosis and Haemostasis. 16: 1246-1249. 2018.
38
For Educational Use Only 19You can also read