Mind-Body Treatments for the Pain-Fatigue-Sleep Disturbance Symptom Cluster in Persons with Cancer
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
126 Journal of Pain and Symptom Management Vol. 39 No. 1 January 2010
Review Article
Mind-Body Treatments for the Pain-Fatigue-
Sleep Disturbance Symptom Cluster in
Persons with Cancer
Kristine L. Kwekkeboom, PhD, RN, Catherine H. Cherwin, MS, RN, Jun
W. Lee, MS, RN, and Britt Wanta, MS, RN
School of Nursing, University of Wisconsin-Madison, Madison, Wisconsin, USA
Abstract
Context. Co-occurring pain, fatigue, and sleep disturbance comprise a common
symptom cluster in patients with cancer. Treatment approaches that target the
cluster of symptoms rather than just a single symptom need to be identified and tested.
Objectives. To synthesize evidence regarding mind-body interventions that
have shown efficacy in treating two or more symptoms in the pain-fatigue-sleep
disturbance cancer symptom cluster.
Methods. A literature search was conducted using CINAHL, Medline, and
PsychInfo databases through March 2009. Studies were categorized based on the
type of mind-body intervention (relaxation, imagery/hypnosis, cognitive-behavioral
therapy/coping skills training [CBT/CST], meditation, music, and virtual reality), and
a preliminary review was conducted with respect to efficacy for pain, fatigue, and sleep
disturbance. Mind-body interventions were selected for review if there was evidence of
efficacy for at least two of the three symptoms. Forty-three studies addressing five types
of mind-body interventions met criteria and are summarized in this review.
Results. Imagery/hypnosis and CBT/CST interventions have produced
improvement in all the three cancer-related symptoms individually: pain,
fatigue, and sleep disturbance. Relaxation has resulted in improvements in pain
and sleep disturbance. Meditation interventions have demonstrated beneficial
effects on fatigue and sleep disturbance. Music interventions have demonstrated
efficacy for pain and fatigue. No trials were found that tested the mind-body
interventions specifically for the pain-fatigue-sleep disturbance symptom cluster.
Conclusion. Efficacy studies are needed to test the impact of relaxation, imagery/
hypnosis, CBT/CST, meditation, and music interventions in persons with cancer
experiencing concurrent pain, fatigue, and sleep disturbance. These mind-body
interventions could help patients manage all the symptoms in the cluster with
a single treatment strategy. J Pain Symptom Manage 2010;39:126e138. Ó 2010 U.S.
Cancer Pain Relief Committee. Published by Elsevier Inc. All rights reserved.
Address correspondence to: Kristine L. Kwekkeboom, PhD, Highland Ave, Madison, WI 53792, USA. E-mail:
RN, School of Nursing, University of Wisconsin- kwekkeboom@wisc.edu
Madison, K6/336 Clinical Science Center, 600 Accepted for publication: June 17, 2009.
Ó 2010 U.S. Cancer Pain Relief Committee 0885-3924/10/$esee front matter
Published by Elsevier Inc. All rights reserved. doi:10.1016/j.jpainsymman.2009.05.022Vol. 39 No. 1 January 2010 Mind-Body Treatments 127
Key Words
Pain, fatigue, sleep disturbance, cancer, mind-body and relaxation techniques
Introduction a single symptom may have a broad spectrum
of effect and could also impact other symp-
Persons with cancer experience a range of symp-
toms in the cluster. Williams6 hypothesized
toms related to both the disease and its treat-
that a single intervention may impact the en-
ment. Recent evidence has demonstrated that
tire symptom cluster, noting that: (1) the symp-
certain symptoms tend to co-occur or ‘‘cluster’’
toms may share a common etiology, (2)
together, exacerbating the overall symptom ex-
diminishing one symptom may prevent exacer-
perience.1,2 In some cases, there may be shared
bations in others, and (3) single interventions
mechanisms causing each of the symptoms to
may be indicated for more than one symptom.
occur (e.g., cytokine-induced nausea and vomit-
She also noted possible benefits of using a sin-
ing). In other cases, having one symptom may
gle intervention in that it simplifies treatment,
cause or exacerbate another (e.g., uncontrolled
reduces the risk for side effects, and may re-
pain may interrupt one’s sleep). Finally, treat-
duce costs. In this article, the term ‘‘crossover’’
ment strategies used for a particular symptom
is used to describe treatments that have dem-
may produce side effects that manifest as new
onstrated efficacy for more than one of the
symptoms (e.g., using opioids to control pain
cluster component symptoms and may, there-
may leave one feeling fatigued). Most studies
fore, be beneficial in treating the symptom
have focused on identifying treatments for indi-
cluster as a whole. It is our position that such
vidual symptoms, but given new awareness of
crossover treatments should be given priority
symptom clusters, it now appears that this piece-
in symptom cluster management trials.
meal approach may be flawed. Treatment ap-
The most well-documented and studied
proaches may have greater effects if they target
symptom cluster is the combination of pain,
a cluster of symptoms rather than one single
fatigue, and sleep disturbance. Pain, fatigue,
symptom. This article will review evidence for
and sleep disturbance are among the most com-
mind-body interventions to identify those that
mon symptoms experienced by persons with
may be efficacious in treating the symptom clus-
cancer.7 Pain is reported by 59% of persons re-
ter of co-occurring pain, fatigue, and sleep dis-
ceiving anticancer treatment and 64% of those
turbance in cancer.
with advanced, metastatic, or terminal disease.8
Fatigue, the most common symptom experi-
Background enced by all the persons with cancer, impacts
The focus of cancer symptom management more than 75% of patients.9e11 Sleep problems,
research has recently shifted as investigators such as difficulty falling asleep, frequent night-
acknowledge that symptoms typically do not time wakening, waking too early in the morning,
occur in isolation. Symptom clusters are de- or excessive daytime sleeping, are reported by
fined as combinations of two or more co- up to 72% of persons with cancer.12,13 These
occurring symptoms that are related to each three symptoms have been found to cluster,
other and that are independent of other symp- co-occurring in more than 40% of patients, par-
toms or symptom clusters.3,4 Symptoms within ticularly those receiving cancer treatment.14e17
the cluster may share the same etiology, but Moderate positive correlations between the
are not required to do so. Some of the symp- three symptoms have been documented in per-
toms may be related to the cancer itself, sons with various cancer diagnoses and stages
whereas others are brought about by cancer of disease.14 If not adequately managed, the
treatment strategies. When occurring together, symptoms in this cluster may interfere with
the symptoms may have a greater impact on mood, role and social functions, ability to toler-
physical function, emotional distress, and over- ate and continue cancer therapies, and overall
all quality of life than was previously attributed quality of life.18e23
to symptoms occurring in isolation. Traditional medical management of pain,
Barsevick5 used the term ‘‘crossover’’ in sug- fatigue, or sleep disturbance has focused on
gesting that treatments shown to benefit the use of pharmaceutical treatments such as128 Kwekkeboom et al. Vol. 39 No. 1 January 2010 analgesics, psychostimulants, hematopoietic itself.17 Interventions to enhance coping, di- growth factors, or sedatives. Specific medications minish stress and anxiety, and improve mood prescribed for one symptom, however, may unin- may, therefore, help to improve the pain- tentionally worsen the other symptoms. For ex- fatigue-sleep disturbance symptom cluster.28 ample, opioid pain medications may cause Mind-body interventions may be useful in alter- feelings of tiredness and increase daytime nap- ing negative thoughts about cancer, the under- ping, which, in turn, leads to less restful night- lying cause of symptoms, or in reframing how time sleep. Disruptions in sleep may exacerbate the symptoms are interpreted. The interven- daytime fatigue, causing increased sensitivity to tions may improve mood and provide a more pain. Sleep disturbance related to steroid use optimistic attitude toward one’s ability to cope may result in inadequate rest and intensify fa- with pain, fatigue, and sleep disturbance. tigue. On the other hand, use of sedatives or Mind-body interventions may also enhance re- sleep enhancers may result in sensations of grog- laxation and reduce stress and anxiety related giness or lack of alertness throughout the day, to the symptom experience. The physical and which could intensify fatigue and contribute to mental effects of relaxation may reduce sensitiv- muscle aches and pain. It appears that the pain- ity to pain sensations, allow more restful sleep, fatigue-sleep disturbance symptom cluster cannot and reduce fatigue. be optimally managed with the use of medica- The purpose of this literature review was to tions alone. Nonpharmacologic, mind-body in- identify mind-body interventions for which terventions may provide a beneficial addition to evidence suggests beneficial effects on at least the treatment regimen. two of the three cluster component symptoms Mind-body interventions are techniques that (pain, fatigue, and sleep disturbance), and to ‘‘focus on the interactions among the brain, synthesize that evidence. These interventions mind, body, and behavior, and on the.ways may hold potential for use as treatment for in which emotional, mental, social, spiritual, the full symptom cluster. and behavioral factors can directly affect health.’’24 Examples of mind-body interven- tions include relaxation, hypnosis, imagery, Methods meditation, and cognitive or behavioral tech- CINAHL, Medline, and PsycINFO databases niques, among others. The goal of mind- were searched through March 2009 using se- body interventions is to provide patients with lected terms for mind-body interventions the knowledge and skills to cope with and (guided imagery, hypnosis, relaxation, biofeed- achieve personal control over their symptoms. back, cognitive-behavioral therapy, coping skills Mind-body interventions are particularly training, meditation, virtual reality, and music) appealing options to explore for the treatment combined with the term cancer and terms for of cancer symptom clusters as they are inex- any of the three symptoms of interest (pain, pensive, can be used in addition to pharmaco- fatigue, sleep disturbance, sleep difficulty, in- logic strategies, have relatively few negative somnia). We restricted our search to those side effects, and can be implemented by mind-body interventions that involve primarily patients independently with sufficient training. mental activity, as they can be performed by Pain, fatigue, and sleep disturbance share nearly all the patients, including those with a psychological component. Factors such as advanced disease. Although yoga is classified anxiety and meaning of the cancer symptoms as a mind-body intervention by the National may intensify how the symptoms are perceived Center for Complementary and Alternative and experienced.25 The Theory of Unpleasant Medicine,24 there is disagreement in the litera- Symptoms suggests that psychosocial factors ture, with some investigators describing the such as mental state, reaction to illness, and anx- intervention as physical exercise involving ‘‘vig- iety are antecedents to symptoms that help de- orous.aerobic activity’’ (p. 127).29 Thus, we fine the overall symptom experience.26,27 did not include ‘‘yoga’’ in our search. Results Depression is often noted as being related to were limited to English language, research, pain, fatigue, and sleep disturbance in cancer, and adults (age $ 18 years). and some investigators have included depres- Abstracts were reviewed and articles were se- sion as a component of the symptom cluster lected for inclusion if they tested one of the
Vol. 39 No. 1 January 2010 Mind-Body Treatments 129
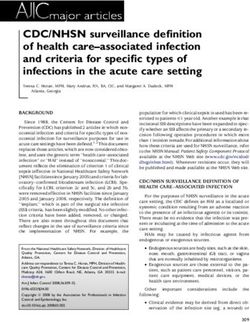
mind-body interventions in a sample of pa- Table 1
tients with cancer and if pain, fatigue, or sleep Evidence Supporting Effects of Mind-Body
Interventions on Pain, Fatigue, and Sleep
disturbance was among the dependent vari-
Disturbance
ables. We eliminated studies in which patients
Sleep
were undergoing diagnostic testing for cancer Mind-Body Intervention Pain Fatigue Disturbance
(i.e., a cancer diagnosis had not yet been estab-
CBT/coping skills training X X X
lished), as well as studies that included both Guided imagery or hypnosis X X
persons with and without cancer in their Meditation X X
samples. Music X X
Relaxation X X
Next, we placed studies into one of six Virtual reality X
categories by intervention type: 1) relaxation,
X ¼ Evidence of beneficial effects on the symptom.
2) imagery/hypnosis, 3) cognitive-behavioral
therapy/coping skills training [CBT/CST], 4) 2) imagery/hypnosis, 3) CBT/CST, 4) medita-
meditation, 5) music, and 6) virtual reality. tion, and 5) music are described and their
We categorized studies based on the descrip- findings synthesized in the following pages.
tion of the intervention provided in the re-
search report. If the study included more Relaxation. Studies were categorized as ‘‘re-
than one intervention, it was categorized based laxation’’ if they tested a technique designed
on the most complex intervention included in to elicit a state of relative freedom from mental
the study. For example, if a CBT intervention and/or physical tension.30 The use of relaxa-
was compared to a simple relaxation interven- tion as a therapeutic intervention dates back
tion, the study was categorized as a test of the many decades. In the early 1900s, Jacobsen de-
more complex intervention, CBT. Descriptions veloped the progressive muscle relaxation
of each type of intervention are provided in (PMR) technique to stimulate physical and
the Results section. mental relaxation by focusing attention on
We conducted a preliminary review and identi- the sensations associated with systematically
fied those mind-body interventions for which tensing and relaxing groups of muscles.31 A va-
beneficial effects were demonstrated on at least riety of other relaxation exercises have been
two of the three symptoms. Studies of those inter- developed, such as jaw relaxation (relaxing
ventions were then reviewed in detail using a sys- muscles of the face, mouth, and jaw), focused
tematic narrative approach. We did not compute breathing (focusing attention on a relaxing
study quality scores, as our intent was to cast word or phrase and slow, regular respirations),
a broad net for those mind-body interventions or abdominal breathing (slow deep breathing
that currently hold promise as treatment for using muscles of the abdomen). Relaxation
the symptom cluster. Those interventions can exercises minimize sympathetic nervous sys-
then be targeted for immediate study. tem response, which decreases oxygen de-
mand, slows heart rate and respirations, and
lowers blood pressure.32 Relaxation interven-
tions may improve symptoms by eliminating
Results physical tension and emotional stressors, and
Evidence for Crossover Mind-Body by facilitating the ability to become comfort-
Interventions able, rest, and fall asleep.25
A total of 47 published articles were identi- Relaxation interventions were implemented
fied that tested a mind-body strategy for pain, as the experimental treatment in six studies
fatigue, and/or sleep disturbance in persons (Supplementary Table 2). Pain was the most
with cancer. Of the six types of mind-body frequently studied outcome. It was the primary
interventions searched, all but virtual reality focus of four efficacy trials, with beneficial ef-
had studies supporting beneficial effects on fects demonstrated in three. Samples included
at least two of the three symptoms of interest hospitalized patients with cancer pain, outpa-
(Table 1). The four studies that tested a virtual tients with chronic cancer pain, and women
reality intervention provided evidence for with early stage breast cancer. Significantly
effects on fatigue only, and are not addressed greater pain relief was obtained with PMR
in this review. The 43 studies of 1) relaxation when compared to massage, treatment as130 Kwekkeboom et al. Vol. 39 No. 1 January 2010
usual,33 positive mood manipulation, distrac- or attention control conditions.39,46,47 Con-
tion, and a no-treatment control condition.34 versely, Haase et al.40 found no significant dif-
Biofeedback-assisted relaxation resulted in ferences in pain and no differences in fatigue
greater pain relief when compared to atten- between patients receiving an imagery
tion control (e.g., time spent with a nurse).35 intervention and those receiving standard
Domar et al.,36 however, found no significant care with colorectal surgery. Elkins et al.48
differences in pain between a daily relaxation tested a hypnosis intervention among women
exercise and a distraction condition among with breast cancer who were experiencing
patients having surgical skin cancer resection. hot flashes and reported a significant improve-
One study each explored the effect of relaxa- ment in sleep scores in the hypnosis group
tion training on fatigue and sleep disturbance. compared to a no treatment control condition.
Training in PMR did not improve fatigue in pa- Four additional studies used imagery inter-
tients receiving radiotherapy when compared ventions as comparison conditions in studies
to an informational intervention,37 but PMR of CBT/CST. All combined imagery with relax-
training did improve sleep in patients with in- ation instructions. One study reported no
somnia when compared to treatment as usual.38 change in pain or fatigue,49 but two reported
Two additional studies used relaxation inter- significant reductions in pain50,51 and one re-
ventions as comparison conditions in studies ported significant reductions in fatigue and
of imagery interventions. Both compared PMR sleep disturbance.52
to standard care in hospitalized patients. One
demonstrated a significant reduction in pain Cognitive-Behavioral Therapy/Coping Skills Train-
with PMR,39 but the other found no differences ing. Studies were categorized as ‘‘CBT/CST’’
in pain or fatigue.40 if the intervention aimed to change patients’
thoughts as a way to influence their feelings
Imagery/Hypnosis. Studies were categorized as and behaviors, helping patients to recognize
‘‘imagery/hypnosis’’ if they tested an interven- and subsequently control their response to
tion that asked participants to create specific symptoms using a programmed education or
mental images with the intent of bringing about counseling approach. Interventions that com-
positive physical or emotional effects.41 Despite bined training in more than two cognitive or
their different names, imagery and hypnosis behavioral coping strategies in a single treat-
have been noted to be quite similar in terms of ment group were also included in this category
practice. Both interventions focus on the crea- as coping skills training. What an individual
tion of mental representations, through recall thinks and believes about his/her symptoms,
of memories or creative imagination that including thoughts about the symptom’s
change the desired outcome (e.g., symptom meaning, controllability, and consequences,
experience).42 Pleasant images may be created influence how symptoms are experienced. In
to distract attention away from the noxious CBT/CST interventions, participants are
symptom. Alternatively, images of the unpleas- taught to understand how their thoughts influ-
ant symptom may be modified to change the ence their feelings and behavior, to recognize
symptom experience.43 Investigators have sug- and acknowledge when this is occurring, and
gested that the body mimics neurohormonal to use cognitive strategies and coping skills to
responses to the mental images, as if they were change their thoughts and behaviors. The in-
actually occurring.41,44 The mental images terventions are usually delivered over several
may also alter expectations for outcome, such weeks and involve assignments to practice
that the desired outcome occurs automatically what has been learned outside of the training
in response to the new image.44 sessions. If the patient experiences difficulty
Imagery/hypnosis interventions served as with the skills, problem solving and additional
the experimental intervention in six studies training are carried out at the next treatment
(Supplementary Table 3). Four studies tested session. As applied to symptom management,
imagery interventions in hospitalized patients CBT/CST interventions focus on helping par-
with cancer pain, and all reported beneficial ticipants to identify and change maladaptive
effects; one in a pretest-posttest design45 and cognitions about their symptoms and use
three when compared to treatment-as-usual various cognitive and behavioral copingVol. 39 No. 1 January 2010 Mind-Body Treatments 131 strategies that change how the symptoms are coping skills audio-recording before each che- perceived and experienced.53 motherapy cycle compared to treatment as A total of 21 studies (24 publications) tested usual. In one-group designs, both Quesnel a program of CBT/CST in persons with can- et al.64 and Berger et al.67,68 reported significant cer-related pain, fatigue, or sleep disturbance improvement in sleep with a four- to eight-week (Supplementary Table 4). Four studies tested CBT intervention, but only Quesnel also re- CBT/CST interventions for pain. Robb et al.54 ported improvement in fatigue. Espie et al.69 demonstrated a significant reduction in pain in- found greater improvements in sleep and less tensity among adults with chronic cancer pain fatigue after a five-session nurse-led CBT inter- after participating in a six-month pain-focused vention compared to treatment as usual. Savard CBT intervention. Syrjala et al.50,51 conducted et al.63 and Epstein and Dirksen reported two trials of a CBT intervention, comparing greater improvement in sleep, but no change the treatment to treatment as usual for mucosi- in fatigue when four to eight weeks of CBT was tis pain experienced by persons having a bone compared to treatment as usual or sleep educa- marrow transplant to treat hematologic malig- tion.65,66 Cohen and Fried52 reported no nancies. In the first study, pain reported by the improvement in either fatigue or sleep distur- CBT group was no different from pain reported bance with a nine-week CBT intervention com- by the control group. In the second study, CBT pared to standard treatment. resulted in significantly less pain than the con- Finally, four studies measured the effect of trol condition.51 Dalton55 tested a similar self- CBT/CST interventions on all the three symp- care program among adults with cancer-related toms concurrently: pain, fatigue, and sleep pain, but found no differences in pain ratings disturbance. One study documented improve- when compared to control. ment in two of the three symptoms. Davidson Cancer-related fatigue was the primary focus et al.70 tested an eight-week sleep focused of three studies of CBT/CST interventions; all CBT program in persons with cancer-related demonstrated beneficial effects. Samples in- insomnia using a one-group pretest-posttest cluded patients receiving chemotherapy, pa- design. Significant improvements were docu- tients who had completed treatment, and mented in both fatigue and sleep disturbance, patients with malignant melanoma. Signifi- but pain remained unchanged. Arving et al.71 cantly greater improvements in fatigue were and Dalton et al.72 both tested individually tai- achieved with a 6e12-week CBT/CST interven- lored CBT interventions. Arving et al. reported tion when compared to treatment as usual,56 significantly less sleep disturbance but no dif- wait-list control,57,58 and a no treatment control ferences in pain or fatigue among women condition.59 starting treatment for breast cancer following Three studies tested the effects of CST in a nurse-led CBT intervention compared to managing the combination of pain and fatigue. control. Dalton et al.72 reported significantly Samples included women with metastatic breast lower ratings of ‘‘worst’’ pain immediately after cancer experiencing pain,49 patients undergo- the tailored CBT program, and greater reduc- ing curative radiation therapy,60 and women un- tions in pain and fatigue six months after the dergoing bone marrow transplant for breast intervention compared to treatment-as-usual cancer.61 All the studies compared a one-session control. There were no differences in sleep. CST intervention to a treatment-as-usual con- Vilela et al.73 found no significant differences trol condition. No significant differences in in pain, fatigue, or sleep disturbance in pa- pain or fatigue were noted between groups in tients with head and neck cancer using any of these studies. a CST intervention compared to control. Seven studies evaluated the effects of CBT/ CST interventions on the combination of Meditation. Studies were categorized as ‘‘medi- fatigue and sleep disturbance. Six of these stud- tation’’ if they provided training in a self-directed ies involved samples of women with breast mental exercise to intentionally and continually cancer52,62e68 and one study included patients focus the mind on a single target perception. with a variety of cancer diagnoses.69 Williams Meditative techniques grew largely out of and Schreier62 found decreased incidence of Eastern religious practices such as Hindu, Bud- fatigue and sleep disturbance using a 20-minute dhist, and Taoist meditation.74 Mindfulness-
132 Kwekkeboom et al. Vol. 39 No. 1 January 2010
based stress reduction (MBSR), a meditative and emotional reactions based on its pitch, in-
technique that has grown in popularity over tensity, tone, and rhythms.84 Certain styles of
the last decade, involves awareness of body sensa- music may trigger relaxation, whereas others
tions and focused breathing to calm the mind enhance mood, and still others energize the
and give the individual a sense of nonjudgmen- mind and body. In general, music provides
tal awareness of bodily experiences.75 Some a source of distraction by holding one’s atten-
MBSR techniques include training in meditative tion on the specific musical qualities. Particu-
exercises such as gentle yoga poses to help bring larly engaging music may distract attention
about the meditative state.76 Symptoms such as from pain, relaxing music may release muscle
pain, fatigue, and sleep disturbance may be mod- tension and reduce pain, or stimulate muscle
ified through meditation by focusing attention relaxation to enhance sleep and rest.30,85
away from the symptom experience, by focusing Fast-paced, up-tempo, positive music may ener-
on strengths and positive thoughts, by eliminat- gize and elevate the mood of someone who is
ing the evaluation or judgment of sensations as- feeling fatigued.86,87
sociated with the symptom.77e79 Four studies evaluated the effects of music in-
Although no studies tested the effects of terventions on pain (Supplementary Table 6).
meditation on cancer-related pain, four stud- Cholburi et al.88 and Zimmerman et al.89
ies evaluated the impact of meditation inter- both reported significant pre- to post-treatment
ventions on fatigue and/or sleep disturbance reductions in pain using 30 minutes of pre-
(Supplementary Table 5). Three studies specif- ferred music among hospitalized patients with
ically identified the type of meditation as cancer pain. Beck90 and Kwekkeboom,91 how-
MBSR; one used similar techniques, but simply ever, found no differences in pain when music
described the intervention as meditation. Only listening was compared to a control condition
one study reported beneficial effects, and that (white noise, book on tape, or resting quietly).
study used a one-group pretest-posttest design. Two studies tested a music intervention on
Carlson and Garland77 reported a significant cancer-related fatigue. Ferrer92 compared live
improvement in both fatigue and sleep distur- music to a no treatment control condition
bance among outpatients with cancer who par- among cancer patients receiving chemotherapy
ticipated in an eight-week MBSR intervention. and reported significantly less fatigue in the mu-
Kieviet-Stijnen et al.80 studied an eight-week sic group. Burns et al.93 compared music with
MBSR intervention in patients with various standard care in a sample of hospitalized pa-
cancer diagnoses and found no within-group tients receiving intensive chemotherapy and
improvement in fatigue. Moadel et al.81 stud- found no significant difference in fatigue be-
ied a 12-week meditation intervention in a sam- tween groups.
ple of women with breast cancer and found no
significant differences in fatigue when com-
pared to a wait-list control condition. Similarly, Discussion
Shapiro et al.82 tested a six-week MBSR inter- A total of six mind-body interventions that
vention among women with breast cancer had been studied for cancer-related pain,
and found no differences in sleep disturbance fatigue, or sleep disturbance were initially
when compared to a choice of other self- identified in this review; all the interventions
directed stress management techniques. except virtual reality demonstrated beneficial
effects on at least two of the symptoms and
Music. Studies were categorized as tests of met criteria for review. Findings suggest there
‘‘music’’ interventions if they promoted health is at least some evidence to support the use
and well-being through listening to or partici- of CBT/CST interventions and imagery/hyp-
pating in music in some way.83 Music therapists nosis interventions for all the three symptoms.
sometimes involve persons in exploring Relaxation has demonstrated efficacy in man-
thoughts and beliefs through music or express- aging pain and sleep disturbance. Meditation
ing emotions by creating music, singing, or has been supported in the treatment of both
dancing, but simple music listening can also fatigue and sleep disturbance. Music has
be an efficacious strategy in managing symp- been efficacious in managing both pain and fa-
toms. Music can stimulate both physiologic tigue. This evidence suggests there is value inVol. 39 No. 1 January 2010 Mind-Body Treatments 133 exploring these five mind-body interventions was the primary treatment being tested, and as potential crossover treatments for the pain- three of four studies in which it was used as an fatigue-sleep disturbance symptom cluster in active comparison condition. The majority of persons with cancer. studies demonstrated support in relieving Of the 15 studies that measured multiple pain. Two studies documented improvement symptom outcomes, only six indicated im- in sleep and one study documented improve- provement in more than one symptom from ment in fatigue with an imagery intervention. the single intervention being tested. In each Most of these studies used randomized or cross- of those cases, the two symptoms improved over designs with treatment-as-usual control were fatigue and sleep disturbance. Three of conditions. The imagery/hypnosis studies six studies used pretest-posttest, within-group were conducted primarily with hospitalized designs. These studies did not control for the patients experiencing cancer-related pain. In- possibility of improvement simply due to terventions ranged from a one-time 12-minute passage of time rather than effects of the exercise to sessions of 50 minutes or more plus mind-body intervention. None of the studies daily practice over several weeks. demonstrated concurrent improvement in CBT/CST interventions were efficacious in pain and fatigue or pain and sleep distur- 14 of 21 studies. Studies demonstrated im- bance, and none demonstrated improvement provement in all the three symptoms, but the in all the three symptoms. It is important to most support was demonstrated for fatigue note, however, that none of these studies and sleep disturbance. Nearly half of the stud- specifically targeted a symptom cluster as their ies involved women with breast cancer either focus of treatment. They simply measured during or after completing treatment. All of other concurrent symptoms in addition to the studies that used experience of the symp- the primary symptom of interest. Most impor- tom(s) of interest as an inclusion criteria tantly, none of the studies used inclusion crite- demonstrated improvement in that symptom. ria to select patients who were experiencing Again, treatment as usual was the most fre- the pain-fatigue-sleep disturbance symptom quent control condition, although some used cluster. Thus, baseline symptom status may active comparison conditions. Two studies not have been sufficient to demonstrate signif- compared CBT/CST interventions to educa- icant improvement across the symptom cluster. tion and found greater effect of the CBT/ Relaxation interventions demonstrated effi- CST intervention in comparison;65,72 however, cacy in four of six trials in which relaxation three studies that used imagery interventions was the primary intervention, and one of the as a comparison found similar or stronger ef- two trials that used relaxation as a comparison fects in the imagery group.50e52 condition. The greatest evidence was for its Meditation interventions demonstrated effi- effect on cancer-related pain. No studies sup- cacy in only one of the four studies, and those ported effects on fatigue, but one study did findings were within group differences in suggest improvement in sleep disturbance. fatigue and sleep disturbance; a control or Both inpatients and outpatients were included comparison condition was not included.77 in the studies as well as patients on and off Populations studied included only outpatients, therapy (surgery, chemotherapy, radiation). most with early stage breast cancer and post- The most frequently studied intervention was treatment. The relatively healthy samples may PMR delivered over three or more training have precluded the ability to demonstrate im- sessions, facilitated with an audiotape and in- provement in symptoms. Both meditation dependent patient practice. Control condi- studies that used control conditions failed to tions were most often described as treatment demonstrate significant effects of the mind- as usual. When more active comparison condi- body intervention, regardless of whether the tions were used (i.e., education and counsel- control was a wait-list or an active comparison ing, distracting activity, imagery), effects of (patient-selected stress management tech- relaxation did not differ significantly from niques such as talking with a friend or those of the comparison group. exercising). Imagery/hypnosis interventions demon- Music interventions demonstrated greater strated efficacy in five of six studies in which it effects than control or comparison conditions
134 Kwekkeboom et al. Vol. 39 No. 1 January 2010 in three of the six studies. Evidence was stron- a common study population, a wide variety of pa- gest for effects on pain. One study docu- tients were studied, including inpatients and out- mented beneficial effects on fatigue. No patients, persons receiving treatment and those studies evaluated the effect of music on sleep who had completed it, as well as persons with var- disturbance. Patients studied were both inpa- ious diagnoses and stages of disease. Some of the tients and outpatients, with most experiencing studies required the presence of symptoms as an the symptom of interest as inclusion criteria inclusion criterion, reducing the possibility of for the study. The length of music interven- floor effects in these trials. tions were typically brief, 30e45 minutes deliv- The studies did, however, have some limita- ered either as a one-time intervention or twice tions. Sample sizes used in most trials were a day over two to three days. Four trials used small to moderate (n < 100 in 35 of 43 trials). randomized controlled designs with treatment Specific doses (timing, frequency of practice) as usual or ‘‘rest’’ as control conditions. Two of CBT/CST interventions varied across stud- used an active comparison condition involving ies. Relatively few studies tested meditation in- a distraction technique or white noise, which terventions. Most music interventions were did not differ from the effects of music. fairly brief (one to six sessions delivered over Few investigators used multisymptom inven-
Vol. 39 No. 1 January 2010 Mind-Body Treatments 135
interventions before they have been tested in designs and enhance the quality of evidence
treating the full symptom cluster. by using randomized controlled designs. Be-
cause active comparison conditions provide
a stringent test, and because patients are not
likely to be content ‘‘doing nothing’’ about
Conclusions bothersome symptoms, comparison/control
Mind-body interventions such as relaxation, groups should be given careful thought. Even-
CBT/CST, meditation, music, and imagery tually, effectiveness trials that make head-to-
may offer benefit to patients with co-occurring head comparisons among mind-body strategies
pain, fatigue, and sleep disturbance related to will be necessary to determine if one treatment
cancer. Most patients are capable of using is more effective than another for a particular
mind-body interventions. Age and advancing symptom cluster, or if one treatment can pro-
disease do not need to be barriers, as the strat- duce the same outcomes at a lesser cost.
egies reviewed here require some cognitive,
but very little physical effort. Many of the
mind-body interventions addressed in this re- Acknowledgments
view could be delivered by health-care pro-
The authors wish to thank Lars Bland for as-
viders, as social workers, health psychologists,
sistance with the initial literature search and
and oncology nurses receive training in cogni-
Kristen Abbott-Anderson for helpful com-
tive-behavioral coping strategies as part of
ments on manuscript drafts.
their educational preparation. Individualized
training along with written or audiotaped in-
structions could be used to evaluate effects
on co-occurring symptoms or on a specific References
symptom cluster. 1. Barsevick A. The concept of symptom cluster.
Although no studies tested mind-body inter- Semin Oncol Nurs 2007;23:89e98.
ventions specifically for the pain-fatigue-sleep 2. Gift A. Symptom clusters related to specific
disturbance symptom cluster, there is sufficient cancers. Semin Oncol Nurs 2007;23:136e141.
evidence to suggest that relaxation, imagery/ 3. Dodd MJ, Janson J, Facione N, et al. Advancing
hypnosis, CBT/CST, meditation, and music the science of symptom management. J Adv Nurs
interventions hold promise as crossover treat- 2001;33:668e676.
ments that may be efficacious for the full symp- 4. Kim H, McGuire DB, Tulman L, Barsevick AM.
tom cluster. Studies have shown that relaxation Symptom clusters: concept analysis and clinical im-
can improve pain and sleep disturbance, med- plications for cancer nursing. Cancer Nurs 2005;
itation can reduce fatigue and sleep distur- 28:270e282.
bance, music can reduce pain and fatigue, 5. Barsevick AM. The elusive concept of the symp-
and imagery/hypnosis and CBT/CST inter- tom cluster. Oncol Nurs Forum 2007;34:971e980.
ventions can produce improvements in all 6. Williams LA. Clinical management of symptom
the three symptoms. clusters. Semin Oncol Nurs 2007;23:113e120.
A number of unanswered questions about 7. Hoffman AJ, Given BA, von Eye A, Gift AG,
the effects of mind-body interventions on the Given CW. Relationships among pain, fatigue, in-
pain-fatigue-sleep disturbance symptom clus- somnia, and gender in persons with lung cancer.
Oncol Nurs Forum 2007;34:785e792.
ter need to be investigated. To adequately de-
termine if any of the mind-body interventions 8. van den Beuken-van Everdingen MHJ, de
can be recommended as treatment for the Rijke JM, Kessels AG, et al. Prevalence of pain in pa-
tients with cancer: a systematic review of the past 40
symptom cluster, investigators need to design years. Ann Oncol 2007;18:1437e1449.
efficacy studies that select participants based
9. Hickok JT, Morrow GR, Roscoe JA, Mustian K,
on their experiences of these three symptoms. Okunieff P. Occurrence, severity, and longitudinal
Researchers need to avoid floor effects by course of twelve common symptoms in 1129 consec-
establishing inclusion criteria that allow room utive patients during radiotherapy for cancer. J Pain
to demonstrate improvement in more than Symptom Manage 2005;30:433e442.
one clustered symptom. Studies need to 10. Stone P, Richards M, Hardy J. Fatigue in pa-
move away from one-group pretest-posttest tients with cancer. Eur J Cancer 1998;34:1670e1676.136 Kwekkeboom et al. Vol. 39 No. 1 January 2010
11. National Comprehensive Cancer Network. Can- symptoms: an update. ANS Adv Nurs Sci 1997;19:
cer-related fatigue: clinical practice guidelines in 14e27.
oncology. J Natl Compr Canc Netw 2003;1:308e331.
28. Parker PK, Kimble LP, Dunbar SB, Clark PC.
12. Davidson JR, MacLean AW, Brundage MD, Symptom interactions as mechanisms underlying
Schulze K. Sleep disturbance in cancer patients. symptom pairs and clusters. J Nurs Scholarsh
Soc Sci Med 2002;54:1309e1321. 2005;37:209e215.
13. Vena C, Parker K, Cunningham M, Clark J, 29. DiStasio SA. Integrating yoga into cancer care.
McMillan S. Sleep-wake disturbances in people Clin J Oncol Nurs 2008;12:125e130.
with cancer part 1: an overview of sleep, sleep regu-
lation, and effects of disease and treatment. Oncol 30. McCaffery M, Pasero C. Pain: Clinical manual,
Nurs Forum 2004;31:735e746. 2nd ed. St. Louis, MO: C.V. Mosby, 1999.
14. Beck S, Dudley WN, Barsevick AM. Using a me- 31. Jacobsen E. Progressive relaxation. Chicago, IL:
diation model to test a symptom cluster: pain, sleep University of Chicago Press, 1929.
disturbance, and fatigue in cancer patients. Oncol
32. Snyder M, Lindquist R. Complementary/alter-
Nurs Forum 2005;32:E48eE55.
native therapies in nursing, 3rd ed. New York:
15. Honea N, Brant J, Beck SL. Treatment-related Springer Publishing, 1998.
symptom clusters. Semin Oncol Nurs 2007;23:
142e151. 33. Hernandez-Reif M, Field T, Ironson G, et al.
Natural killer cells and lymphocytes increase in
16. Miaskowski C, Lee KA. Pain, fatigue, and sleep women with breast cancer following massage ther-
disturbance in oncology outpatients receiving radia- apy. Int J Neurosci 2005;115:495e510.
tion therapy for bone metastasis: a pilot study. J Pain
Symptom Manage 1999;17:320e332. 34. Anderson KO, Cohen MZ, Mendoza TR, et al.
Brief cognitive-behavioral audiotape interventions
17. Theobald DE. Cancer pain, fatigue, distress, for cancer related pain. Cancer 2006;107:207e214.
and insomnia in cancer patients. Clin Cornerstone
2004;6(Supp 1D):S15eS21. 35. Tsai PS, Chen PL, Lai YL, Lee MB, Lin CC. Ef-
fects of electromyography biofeedback-assisted re-
18. Barsevick AM, Dudley WN, Beck SL. Cancer-re-
laxation on pain in patients with advanced cancer
lated fatigue, depressive symptoms, and functional
in a palliative care unit. Cancer Nurs 2007;30:
status. Nurs Res 2006;55:366e372.
347e353.
19. Curt GA, Breitbart W, Cella D, et al. Impact of
cancer-related fatigue on the lives of patients: new 36. Domar AD, Noe JM, Benson H. The preopera-
findings from the fatigue coalition. Oncologist tive use of the relaxation response with ambulatory
2000;5:353e360. surgery patients. Hosp Top 1987;65(4):30e35.
20. Gupta D, Lis CG, Grutsch JF. The relationship 37. Decker TW, Cline-Elsen J, Gallagher M. Relaxa-
between cancer-related fatigue and patient satisfac- tion therapy as an adjunct in radiation oncology.
tion with quality of life in cancer. J Pain Symptom J Clin Psychol 1992;48:388e393.
Manage 2007;34:40e47. 38. Cannici J, Malcolm R, Peek LA. Treatment of in-
21. Payne R. Recognition and diagnosis of break- somnia in cancer patients using muscle relaxation
through pain. Pain Med 2007;8(S1):S3eS7. training. J Behav Ther Exp Psychiatry 1983;14:
251e256.
22. Serlin RC, Mendoza TR, Nakamura Y,
Edwards KR, Cleeland CS. When is cancer pain 39. Kwekkeboom KL, Wanta B, Bumpus M. Individ-
mild, moderate, or severe? Grading pain severity by ual difference variables and the effects of progres-
its interference with function. Pain 1995;61:277e284. sive muscle relaxation and analgesic imagery
interventions on cancer pain. J Pain Symptom Man-
23. Strang P. Existential consequences of unre-
age 2008;36:604e615.
lieved cancer pain. Palliat Med 1997;11:299e305.
24. National Center for Complementary and Alter- 40. Haase O, Schwenk W, Hermann C, Muller JM.
native Medicine. Mind-body medicine: an overview. Guided imagery and relaxation in conventional co-
Available from: http://nccam.nih.gov/health/back lorectal resections: a randomized controlled par-
grounds/mindbody.htm. Accessed June 2, 2008. tially blinded trial. Dis Colon Rectum 2005;48:
1955e1963.
25. Breitbart W, Gibson CA. Psychiatric aspects of
cancer pain management. Prim Psychiatry 2007;14: 41. Hart J. Guided imagery. Alternative and Com-
81e91. plementary Therapies 2008;14:295e299.
26. Gift AG, Jablonski A, Stommel M, Given CW. 42. Gay M, Hanin D, Luminet O. Effectiveness of an
Symptom clusters in elderly patients with lung can- hypnotic imagery intervention on reducing alexithy-
cer. Oncol Nurs Forum 2005;31:203e212. mia. Contemp Hypn 2008;25:1e13.
27. Lenz ER, Pugh LC, Milligan RA, Gift AG, 43. Lebovits A. Cognitive-behavioral approaches to
Suppe F. The middle-range theory of unpleasant chronic pain. Prim Psychiatry 2007;14:48e59.Vol. 39 No. 1 January 2010 Mind-Body Treatments 137
44. Milling LS. Recent developments in the study of 59. Fawzy FI, Cousins N, Fawzy NW, et al. A struc-
hypnotic pain reduction: a new golden era of tured psychiatric interventions for cancer patients.
research? Contemp Hypn 2008;25:165e177. Arch Gen Psychiatry 1990;47:720e725.
45. Kwekkeboom KL, Kneip J, Pearson L. A pilot 60. Clark M, Isaacks-Downton G, Wells N, et al. Use
study to predict success with guided imagery for can- of preferred music to reduce emotional distress and
cer pain. Pain Manage Nurs 2003;4:112e123. symptom activity during radiation therapy. J Music
Ther 2006;43:247e265.
46. Ebell H. The therapist as travelling companion
to the chronically ill: hypnosis and cancer related 61. Gaston-Johansson F, Fall-Dickson JM, Nanda J,
symptoms. Contemp Hypnosis 2008;25:46e56. et al. The effectiveness of the comprehensive coping
strategy program on clinical outcomes in breast can-
47. Sloman R, Brown P, Aldana E, Chee E. The use
cer autologous bone marrow transplantation. Can-
of relaxation for the promotion of comfort and pain
cer Nurs 2000;23:277e285.
relief in persons with advanced cancer. Contemp
Nurse 1994;3:6e12. 62. Williams SA, Schreier AM. The role of educa-
tion in managing fatigue, anxiety, and sleep disor-
48. Elkins G, Marcus J, Stearns V, et al. Randomized ders in women undergoing chemotherapy for
trial of a hypnosis intervention for treatment of hot breast cancer. Appl Nurs Res 2005;18:138e147.
flashes among breast cancer survivors. J Clin Oncol
2008;26:5022e5026. 63. Savard J, Simard S, Ivers H, Morin CM. Random-
ized study on the efficacy of cognitive-behavioral ther-
49. Arathuzik D. Effects of cognitive-behavioral apy for insomnia secondary to breast cancer, part I:
strategies on pain in cancer patients. Cancer Nurs sleep and psychological effects. J Clin Oncol 2005;
1994;17:207e214. 23:6083e6096.
50. Syrjala KL, Cummings C, Donaldson GW. Hyp- 64. Quesnel C, Savard J, Simard S, Ivers H,
nosis or cognitive behavioral training for the reduc- Morin CM. Efficacy of cognitive-behavioral therapy
tion of pain and nausea during cancer treatment: for insomnia in women treated for nonmetastatic
a controlled clinical trial. Pain 1992;48:137e146. breast cancer. J Consult Clin Psychol 2003;71:
51. Syrjala KL, Donaldson GW, Davis MW, 189e200.
Kippes ME, Carr JE. Relaxation and imagery and 65. Epstein DR, Dirksen SR. Randomized trial of
cognitive-behavioral training reduce pain during a cognitive-behavioral intervention for insomnia in
cancer treatment: a controlled clinical trial. Pain breast cancer survivors. Oncol Nurs Forum 2007;
1995;63:189e198. 34:E51eE59.
52. Cohen M, Fried G. Comparing relaxation train- 66. Dirksen SR, Epstein DR. Efficacy of an insomnia
ing and cognitive-behavioral group therapy for intervention on fatigue, mood and quality of life in
women with breast cancer. Res Soc Work Pract breast cancer survivors. J Adv Nurs 2008;61:
2007;17:313e323. 664e675.
53. Thorn BE. Cognitive therapy for chronic pain: 67. Berger AM, VonEssen S, Kuhn BR, et al. Feasi-
A step-by-step guide. New York: The Guilford Press, bility of a sleep intervention during adjuvant breast
2004. cancer chemotherapy. Oncol Nurs Forum 2002;29:
54. Robb KA, Williams JE, Duvivier V, Newham DJ. 1431e1441.
A pain management program for chronic cancer-- 68. Berger AM, VonEssen S, Kuhn BR, et al. Adher-
treatment-related pain: a preliminary study. J Pain ence, sleep, and fatigue outcomes after adjuvant
2006;7:82e90. breast cancer chemotherapy: results of a feasibility
55. Dalton JA. Education for pain management: intervention study. Oncol Nurs Forum 2003;30:
a pilot study. Patient Educ Couns 1987;9:155e165. 513e522.
56. Armes J, Chalder T, Addington-Hall J, 69. Espie CA, Fleming L, Cassidy J, et al. Random-
Richardson A, Hotopf M. A randomized controlled ized controlled clinical effectiveness trial of cogni-
trial to evaluate the effectiveness of a brief, behavior- tive behavior therapy compared with treatment as
ally oriented intervention for cancer-related fatigue. usual for persistent insomnia in patients with can-
Cancer 2007;110:1385e1395. cer. J Clin Oncol 2008;26:4651e4658.
57. Gielissen MF, Verhagen CA, Bleijenberg G. Cog- 70. Davidson JR, Waisberg JL, Brundage MD,
nitive behaviour therapy for fatigued cancer survi- Maclean AW. Nonpharmacologic group treatment
vors: long-term follow-up. Br J Cancer 2007;97: of insomnia: a preliminary study with cancer survi-
612e618. vors. Psychooncology 2001;10:389e397.
58. Gielissen MF, Vehagen S, Witjes F, Bleijenberg G. 71. Arving C, Sjödén P, Bergh J, et al. Individual psy-
Effects of cognitive behaviour therapy in severely chosocial support for breast cancer patients. Cancer
fatigued disease-free cancer patients compared with Nurs 2007;30:E10eE19.
patients waiting for cognitive behavior therapy: 72. Dalton JA, Keefe FJ, Carlson J, Youngblood R.
a randomized controlled trial. J Clin Oncol 2006;24: Tailoring cognitive-behavioral treatment for cancer
4882e4887. pain. Pain Manag Nurs 2004;51:3e18.138 Kwekkeboom et al. Vol. 39 No. 1 January 2010
73. Vilela LD, Nicolau B, Mahmud S, et al. Compar- 84. Magill L. The use of music therapy to address
ison of psychosocial outcomes in head and neck the suffering in advanced cancer pain. J Palliat
cancer patients receiving a coping strategies inter- Care 2001;17:167e172.
vention and control subjects receiving no interven- 85. Lai HL, Good M. Music improves sleep quality
tion. J Otolaryngol 2006;35:88e96. in older adults. J Adv Nurs 2006;53:134e144.
74. Kreitzer MJ. Meditation. In: Snyder M, 86. Szabo A, Small A, Length M. The effects of slow-
Lindquist R, eds. Complementary/alternative thera- and fast-rhythm classical music on progressive
pies in nursing, 3rd ed. New York: Springer Publish- cycling to voluntary physical exhaustion. J Sports
ing, 1998: 123e137. Med Phys Fitness 1999;39:220e225.
75. Ospina MB, Bond K, Karkhaneh MD, et al. Clin- 87. Siedliecki SL, Good M. Effects of music on
ical trials of meditation practices in health care: power, pain, depression, and disability. J Adv Nurs
characteristics and quality. J Altern Complement 2006;54:553e562.
Med 2008;14:1199e1213.
88. Cholburi JSN, Hanucharurnkul S, Waikakul W.
76. Carmody J, Baer RA. Relationships between Effects of music therapy on anxiety and pain in
mindfulness practice and levels of mindfulness, cancer patients. Thai J Nurs Res 2004;8:173e181.
medical and psychological symptoms and well-being 89. Zimmerman L, Pozehl B, Duncan K, Schmitz R.
in a mindfulness-based stress reduction program. Effects of music in patients who had chronic cancer
J Behav Med 2008;31:23e33. pain. West J Nurs Res 1989;11:296e309.
77. Carlson LE, Garland SN. Impact of mindful- 90. Beck SL. The therapeutic use of music for can-
ness-based stress reduction (MBSR) on sleep, cer related pain. Oncol Nurs Forum 1991;18:
mood, stress, and fatigue symptoms in cancer outpa- 1327e1337.
tients. Int J Behav Med 2005;12:278e285.
91. Kwekkeboom KL. Music versus distraction for
78. Tiexeira ME. Meditation as an intervention for procedural pain and anxiety in patients with cancer.
chronic pain: an integrative review. Holist Nurs Oncol Nurs Forum 2003;30:433e440.
Pract 2008;22:225e234. 92. Ferrer AJ. The effect of live music on decreasing
79. Ong JC, Shapiro SL, Manber R. Combining anxiety in patients undergoing chemotherapy treat-
mindfulness meditation with cognitive-behavior ment. J Music Ther 2007;44:242e255.
therapy for insomnia: a treatment-development 93. Burns DS, Azzouz F, Sledge R, et al. Music imag-
study. Behav Ther 2008;39:171e182. ery for adults with acute leukemia in protective en-
80. Kieviet-Stinjnen A, Visser A, Garssen B, vironments: a feasibility study. Support Care
Hudig W. Mindfulness-based stress reduction train- Cancer 2008;16:507e513.
ing for oncology patients: patients’ appraisal and 94. McNair DM, Loor M, Droppleman LF. Profile of
changes in well-being. Patient Educ Couns 2008; mood states. San Diego, CA: Educational and Indus-
72:436e442. trial Testing Service, 1971.
81. Moadel AB, Shah C, Wylie-Rosett J, et al. Ran- 95. Smets EM, Garssen B, Bonke B, DeHaes JC. The
domized controlled trial of yoga among a multieth- Multidimensional Fatigue Inventory (MFI): psycho-
nic sample of breast cancer patients: effects on metric qualities of an instrument to assess fatigue.
quality of life. J Clin Oncol 2007;25:4387e4395. J Psychosom Res 1995;39:315e325.
82. Shapiro SL, Bootzin RR, Figueredo AJ, 96. Buysse DJ, Reynolds CF, Monk TH, Berman SR,
Lopez AM, Schwartz GE. The efficacy of mindful- Kupfer DJ. The Pittsburgh Sleep Quality Index:
ness-based stress reduction in the treatment of sleep a new instrument for psychiatric practice and re-
disturbance in women with breast cancer: an explor- search. Psychiatry Res 1989;28:193e213.
atory study. J Psychosom Res 2003;54:85e91. 97. Aaronson NK. The EORTC-QLQ-30: a quality of
83. Chlan L. Music therapy. In: Snyder M, life instrument for use in international clinical trials
Lindquist R, eds. Complementary/alternative thera- in oncology. Qual Life Res 1993;2:51.
pies in nursing, 3rd ed. New York: Springer Publish- 98. Morin CM. Insomnia: Psychological assessment
ing, 1998:243e257. and management. New York: Guilford Press, 1993.
Supplementary Data
Supplementary data associated with this article can be found, in the online version, at doi:doi:10.
1016/j.jpainsymman.2009.05.022.You can also read