Individualisierte Nierenersatztherapie beim kritisch Kranken - Dialyseseminar Dezember 2020 Berlin
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Dialyseseminar Dezember 2020 Berlin
Individualisierte Nierenersatztherapie beim kritisch
Kranken
06.12.20 Dr. Mariam Abu-Tair 1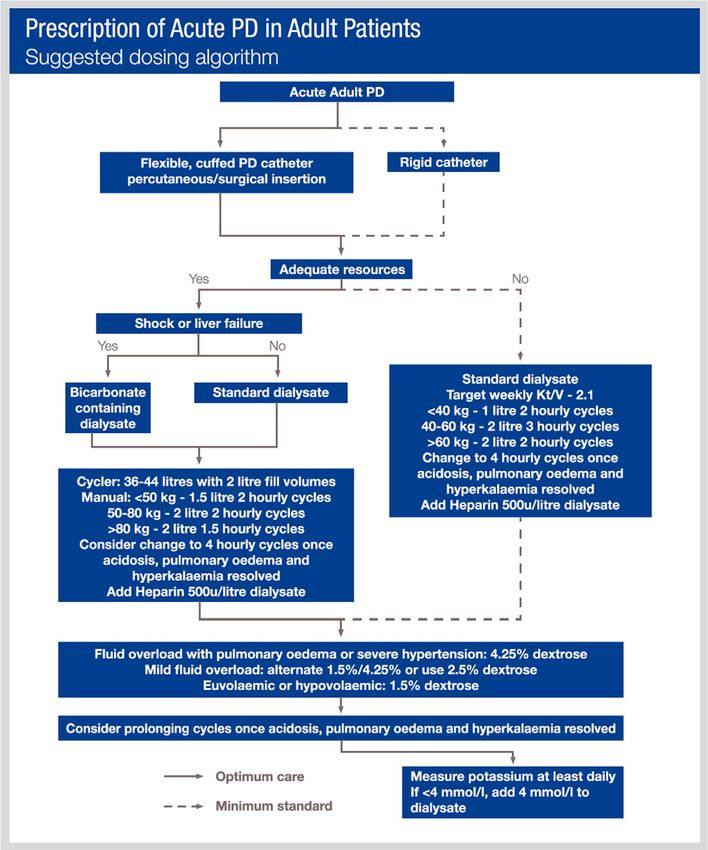
Dialyseseminar Dezember 2020 Berlin
Interessenskonflikte: keine
06.12.20 Dr. Mariam Abu-Tair 2
Dialyseseminar Dezember 2020 Berlin
KLINISCHER FALL
Übernahme eines anamnestisch 160 kg schweren 53 jährigen Patienten
Terminale Niereninsuffizienz unklarer Genese; V.a. hepatorenales Syndrom
Vordiagnosen: Leberzirrhose V.a. NASH; Ausschluss KHK bei leichtgradig eingeschränkter
Pumpfunktion; Diabetes mellitus Typ 2 ED 1995 (HbA1c aktuell 4,7%)
Auswärts tägliche UF bei nicht traktablen Ödemen, Pleuraergüssen, Aszites
Direkte Verlegung auf die Intensivstation bei respiratorischer Insuffizienz und schwerer Hypotonie
Versuch Volumenentzug mittels CiCaCVVHD ohne Erfolg bei steigendem Katecholaminbedarf
Implantation eines gecufften Tesiokatheters in den Bauch zur Durchführung einer PD; danach
kontinuierliche Negativbilanzierung möglich; nach Stabilisierung der Vitalparameter, Ausschleichen
der Katecholamine und Extubation Implantation eines Tenckhoff Katheters durch die Klinik für
Viszeralchirurgie
Entlassung des Patienten nach 2 Monaten und 60 kg Gewichtsverlust in die Häuslichkeit mit
fortgesetzter CAPD
06.12.20 Dr. Mariam Abu-Tair 3Dialyseseminar Berlin 2020 06.12.20 Dr. Mariam Abu-Tair 4
Search results Save
Review
Dialyseseminar Berlin 2020
Blood Purif Received: April 28, 2020
Accepted: September 5, 2020
Published online:Review Perit Dial Int. 2020 Sep;40(5):496-498. doi: 10.1177/0896860820953050.
DOI: 10.1159/000511390 October 5, 2020
Successfully treating three patients with acute
kidney injury secondary to COVID-19 by peritoneal
Peritoneal Dialysis Is an Option for Acute
dialysis: Case report and literature review
Kidney Injury Management in Patients
with COVID-19 Abdullah K Al-Hwiesh 1 , Abdelgalil Moaz Mohammed 1 , Mahmoud Elnokeety 1 ,
2, 3,
Amani Al-Hwiesh Nadia Al-Audah Syed Esam 1 , Ibrahiem Saeed Abdul-Rahman 1
José M. Rodríguez-Chagolla a Enzo Vásquez Jiménez b Leticia Herrera Arellano a Affiliations expand
Alberto Villa Torres a Nayeli Acosta García a Dolores Aleman Quimbiulco a PMID: 32998645 DOI: 10.1177/0896860820953050
Sergio Armeaga Aguilar a Magdalena Madero b
aNephrology Department, Centro Médico Issemym Toluca, Toluca de Lerdo, Mexico; bNephrology Department,
Instituto Nacional de Cardiología Ignacio Chávez, Ciudad de México, Mexico
Abstract
Coronavirus Disease 2019 (COVID-19) is a pandemic disease that increased the burden on heal
care system. In the Kingdom of Saudi Arabia, 74,795 cases have been reported until 26 May 20
and the number of cases is rapidly increasing. The mortality rate of COVID-19 worldwide is 6.37
Keywords Here wesyn-
nally shown to be caused by “severe acute respiratory report three cases of acute kidney injury (AKI) secondary to pneumonia of severe COV
COVID-19 disease · Peritoneal dialysis · Acute kidney injury drome coronavirus 2” (SARS-CoV-2) [3].19; Thethey were treated with automated peritoneal dialysis (PD) with full recovery. To the best of o
World
Health Organization recognized this disease as a pan- few reports in the literature have discussed the use of PD in AKI secondary to COVI
knowledge,
demic, and by April 2020, cases have been reported in 211
19.
Abstract countries, with more than 1.9 million confirmed cases
In December 2019, cases of acute respiratory illness of un- [4]. In Mexico, about 256,848 cases have been diagnosedAKI; COVID-19; automated peritoneal dialysis.
Keywords:
known origin were reported in Wuhan, China. The disease is in all of the states [5]. Since the beginning of the epidem-
caused by “severe acute respiratory syndrome coronavirus ic, kidney injury associated with COVID-19 disease has
2”. After identifying severe lung damage, injury to other or- been documented, in percentages as high as 15% [6].
gans, such as the kidney, has been identified. Peritoneal di- However, the available data suggest that Similar
the preva-articles
alysis is a renal replacement therapy (RRT) and is at least as lence of acute kidney injury (AKI) in patients with CO-
effective as other extracorporeal therapy options, with sig-
Acute peritoneal dialysis in COVID-19.
VID-19 is variable. In another cohort study (n = 1,099),
nificant06.12.20
cost-effective advantages. However, this strategy is Dr. Mariam
5.3% of patients required admission to theAbu-Tair
Parapiboon
intensive careW, Ponce D, Cullis B.
5
rarely used for the management of acute kidney injury in unit (ICU) and only 0.5% of patients had AKI [7].
Perit Dial Int. 2020 Jul;40(4):359-362. doi: 10.1177/0896860820931235. Epub 2020 Jun 19.Dialyseseminar Berlin 2020
Perit Dial Int. 2015 Jul-Aug; 35(4): 397–405
Peritoneal dialysis modalities used in acute kidney injury. Adapted from Ponce et al. (28). IPD =
intermittent peritoneal dialysis (PD); CEPD = chronic equilibrated PD; HVPD = high-volume PD; TPD
= tidal PD; CFPD = continuous-flow PD.
06.12.20 Dr. Mariam Abu-Tair 6Therapeutic Apheresis and Dialysis 2018
doi: 10.1111/1744-9987.12660
© 2018 The Authors. Therapeutic Apheresis and Dialysis published by John Wiley & Sons Australia, Ltd on behalf of International Society for Apheresis,
Dialyseseminar Berlin 2020 Japanese Society for Apheresis, and Japanese Society for Dialysis Therapy
Acute Kidney Injury in Critically Ill Patients: A Prospective
Randomized Study of Tidal Peritoneal Dialysis Versus
Continuous Renal Replacement Therapy
Abdullah Al-Hwiesh,1 Ibrahiem Abdul-Rahman,1 Fredric Finkelstein,2 Jose Divino-Filho,3
Hatem Qutub,1 Nadia Al-Audah,1 Abdalla Abdelrahman,4 Nazeeh El-Fakhrany,1
Mohammed Nasr El-Din,1 Tamer El-Salamony,1 Abdulsalam Noor,1
4 A Al-Hwiesh
Mohammed Al-Shahrani 1
, andetKhalid
al. Al-Otaibi1
1
Nephrology Division, King Fahd Hospital of the University, Al-Khobar, Imam Abdulrahman Bin Faisal
2
University, Saudi Arabia;2.andOutcome
TABLE Yale University,
of renalNewreplacement
Haven, CT, USA; and 3in
therapy Karolinska Institutet, CLINTEC,
the two groups
4
Division of Renal Medicine, Stockholm, Sweden; and Department of Electrical Engineering, Queens
University, Kingston,Group
ON, Canada
A Group B
Outcome N = 62 N = 63 P-value
Infectious complications related to dialysis, N (%) 11 (17.7) 6 (9.5) 0.0084
Time to prepare dialysis access and initiate dialysis, 0.2010
Abstract: Few studies have discussed the role of perito-
(min), median (IQR) between
35 (30–37)groups in regard to patients’
38 characteristics.
(32–40) The
neal function,
Recovery of kidney dialysis (PD) in managing acute kidney injury (AKI)
N (%) survival
22 (35.5)at 28 days was significantly38
better in the patients
(60.3) 0.0056
in critically ill patients. The present study compares the treated with TPD when compared to CVVHDF (69.8%
Resolution of AKI (days),
outcome median
of AKI (IQR) care unit (ICU) patients ran-
in intensive vs.8 46.8%,
(7–10)P < 0.01). Infectious complications
5 (4–6) were signifi- 0.0044
ICU stay (days),domized
medianto(IQR)treatment with tidal PD (TPD) or continuous cantly less (P < 0.01) in the TPD 9
19 (13–20) (7–11)
group (9.5%) when 0.0031
Need of chronic venovenous
dialysis, N hemodiafiltration
(%) (CVVHDF). One hundred 7 (11.3) to the CVVHDF group (17.7%).
compared 6 (9.5) Recovery of 0.3112
Mortality, N (%)and twenty-five ICU patients with AKI were randomly kidney function (60.3% vs. 35.5%), median
33 (53.2) time to resolu-
19 (30.2) 0.0028
allotted to CVVHDF, (Group A, N = 62) or TPD, tion of AKI and the median duration of ICU stay of
(group B, N = 63). Cause and severity of renal injury were 9 days (7–11) vs. 19 days (13–20) were all in favor of TPD
AKI, acute kidney injury; ICU, intensive care unit; IQR, interquartile(P
assessed at the time of initiating dialysis. The primary out-
range.
< 0.01). This study suggests that there are better out-
come was hospital mortality at 28 days, and secondary comes with TPD compared to CRRT in the treatment of
outcomes were time to recovery of renal function, dura- critically ill patients with AKI. Key Words: Acute kidney Therapeutic Apheresis and Dialysis 2018
tion of stay in the ICU, metabolic and fluid control, and injury, Acute tubular necrosis, Continuous venovenous doi: 10.1111/1744-9987.12660
and acidosis improvement
were deemed to have
of sensorial been achieved,
and hemodynamic parameters. CVVHDF (Group
hemodiafiltration, A, N =therapy,
Renal replacement 62) orSepsis,
TPD ©(Group B,
2018 The Authors. Therapeutic Apheresis and Dialysis pu
No statistically significant differences were observed Tidal peritoneal dialysis. Japanese Society for Apheresis, and Japanese Society for Dia
or when urine output had improved, or both. End- N = 63) (Fig. 2). Patient’s demographic and clinical
points included cessation of dialysis after improve- characteristics are shown in Table 1. There was no
06.12.20
ment and a minimum period of 3 days of not
requiring dialysis was necessary for the patients to
Acute kidney injury (AKI) is a common Dr. Mariam
compli-
statistically significant difference in age, gender, the
Abu-Tair
Hyman et al.(IQR)
(2) havesystolic
reported aand
transition of dialy-
Acute Kidney Injury in
median diastolic blood pressure, 7
cation in patients treated in the intensive
be classified as successfully withdrawn from dialysis, care unit sis methods prescribed for AKI from 1994–1995
median (IQR) baseline eGFR and the initial median
to
Randomized Study oDISCUSSION hemodialysis, CVVHD, CVVHDF or PD. Such a
BUN, blood urea nitrogen; Cr, serum creatinine; CVVHDF, continuous venovenous hemodiafiltration; HCO3, serum bicarbonate; IQR,
interquartile range; K,The
serum potassium; TPD, tidal peritoneal dialysis;requires,
decision is not always easy, taking into consider-
UF, net ultrafiltration.
management of AKI in ICU setting
ation the hemodynamic instability of the ICU
in addition to conservative treatment, a decision patients and the feasibility of implementing the dif-
Dialyseseminar Berlin 2020concerning when to start RRT. Once RRT
DISCUSSION is
hemodialysis, CVVHD,
ferent CVVHDF
modalities. or PD.
For the last Such a PD has
two decades,
needed, the treating physician should choose decision is been
not always easy, taking class
into treatment
consider- for ICU
considered a second
The management of AKI
between in ICU setting
its different requires,
modalities, i.e. intermittent
ation the patients who develop
hemodynamic AKI and
instability it hasICU
of the been rarely
in addition to conservative treatment, a decision patients and the feasibility of implementing the dif-might be
used in the developed world (2). This
concerning when to 4.
TABLE start RRT.
Adverse Once
events RRTto treatment
according is becauseFor
group modalities.
ferent of lack
the of
lastPDtwo
experience,
decades,and/or
PD has knowledge
needed, the treating physician should choose by intensivists and nephrologists working in ICU set-
CVVHDF TPD been
P-valueconsidered a second class treatment for ICU
between its different modalities, i.e. intermittent patients who tings, the limitations
develop AKI and attributed to PD,rarely
it has been and/or a lack
†
Hypotension 27 (43.5) 10 (15.9) 0.0016
Infections 11 (17.7) 6 (9.5) used
0.0036 in the developed world (2). This might be
‡
Catheter change
TABLE 4. Adverse events according 14 (22.6)
to treatment 5 (7.9)
group 0.0007
because of lack of PD experience,
TABLE 5. Causes ofand/or knowledge
death in the two groups
Bleeding events§ 17 (27.4) 4 (6.3) 0.0008
Arrhythmias ¶
CVVHDF 13
TPD(21.0) 5 (7.9)
P-value
by intensivists and nephrologists working
0.0023 in ICU
Group A
set-
Group B
Hypoglycemia 5 (8.1) 3 (4.8) tings,
0.0488 the limitations attributed
Cause of death to PD, and/or
N (%) a lack
N (%) P
Hypotension† Hypomagnesemia
27 (43.5) 106(15.9)
(9.7) 7 (11.1)
0.0016 0.3212
Infections Hypocalcemia
11 (17.7) 6 (9.7)
6 (9.5) 6 (9.5)
0.0036 — Sepsis 13 (20.9) 8 (12.7) 0.0232
Catheter change‡ Hypophosphatemia
14 (22.6) †† 5 5(7.9)
(8.1) 7 (11.1)
0.0007 0.1121 ARDS 5 (8.1) 2 (3.2) 0.0361
Bleeding events§ Thrombocytopenia
17 (27.4) 410 (16.1)
(6.3) 3 (4.8)
0.0008 0.0046TABLE DIC5. Causes of death in the5two (8.1)groups1 (1.6) 0.0066
¶ Hepatic failure 7 (11.3) 6 (9.5) 0.2344
Arrhythmias 13 (21.0) 5 (7.9) 0.0023 Group A 1Group
(1.6) B
†
All hypotensive episodes were recorded from initiation until Acute infective endocarditis 0 (0) 0.5454
Hypoglycemia end of RRT.5 (8.1)
Hypotension3 means
(4.8) at least0.0488 Cause
one hypotensive of deathMethanol toxicity N (%)
epi- 2N (%)
(3.2) P
2 (3.2) —
Hypomagnesemia sode during 6 (9.7) 7 (11.1)
RRT. ‡Catheter change due0.3212
to infection or mal- Total 33 (53.2) 19 (30.2) 0.0021
Hypocalcemia function. 6 (9.7)
§ 6 (9.5)reported when
Bleeding events — Sepsis is
transfusion 13 (20.9) 8 (12.7) 0.0232
Hypophosphatemiarequired. 5 (8.1)
¶
Arrhythmia 7means
(11.1) supraventricular
0.1121 ARDS
or ventricu- 5 (8.1) distress2 syndrome;
ARDS, acute respiratory (3.2) 0.0361
DIC, disseminated
††
Thrombocytopenialar. †† 10 (16.1)
Thrombocytopenia3related
(4.8) to the procedure.
0.0046 DIC 5 (8.1)
intravascular coagulopathy. 1 (1.6) 0.0066
Hepatic failure 7 (11.3) 6 (9.5) 0.2344
†
All hypotensive episodes were recorded from initiation until Acute infective endocarditis 1 (1.6) 0 (0) 0.5454
end of RRT. Hypotension means at least one hypotensive epi- © 2018 The Authors. Therapeutic Apheresis and Dialysis published by John
Methanol toxicity 2 (3.2) 2 (3.2) —
Wiley & Sons Australia, Ltd on behalf of International Society for Apheresis,
sode during RRT. ‡Catheter change due to infection or mal- Total 33 (53.2) 19 (30.2) 0.0021
§ Ther Apher Dial, Vol. ••, No. ••, 2018 Japanese Society for Apheresis, and Japanese Society for Dialysis Therapy
function. Bleeding events reported when transfusion is
¶
required. Arrhythmia means supraventricular or ventricu- ARDS, acute respiratory distress syndrome; DIC, disseminated
Therapeutic Apheresis and Dialysis 2018
lar. ††Thrombocytopenia related to the procedure. intravascular coagulopathy. doi: 10.1111/1744-9987.12660
© 2018 The Authors. Therapeutic Apheresis and Dialysis publ
Japanese Society for Apheresis, and Japanese Society for Dialy
© 2018 The Authors. Therapeutic Apheresis and Dialysis published by John
Wiley & Sons Australia, Ltd on behalf of International Society for Apheresis,
Ther Apher Dial, Vol. ••, No. ••, 2018 Japanese Society for Apheresis, and Japanese Society for Dialysis Therapy
Acute Kidney Injury in
Randomized Study o
06.12.20 Dr. Mariam Abu-Tair
Continuous Re
8Clinical and Experimental Nephrology
https://doi.org/10.1007/s10157-018-1598-7
Dialyseseminar Berlin 2020
ORIGINAL ARTICLE
Effect of peritoneal dialysis vs. haemodialysis on respiratory
mechanics in acute kidney injury patients
Clinical and Experimental Nephrology
https://doi.org/10.1007/s10157-018-1598-7
Cibele Puato Almeida1 · André Luís Balbi1 · Daniela Ponce1
ORIGINAL ARTICLE
Kein Unterschied zwischen beiden Gruppen bezügl. Ventilation, Weaning,
Received: 23 January 2018 / Accepted: 1 June 2018
© Japanese Society of Nephrology 2018
Oxygenierung
Abstract Effect of peritoneal dialysis vs. haemodialysis on respirator
mechanics in acute kidney injury patients
Background Peritoneal dialysis (PD) and hemodialysis (HD) are options for the treatment of acute kidney injury (AKI)
patients. The aim of this study was to compare the effects of PD and daily HD on respiratory mechanics of AKI patients
Zur Bauchlagerung
undergoing bei Peritonealdialyse
invasive mechanical ventilation (IMV). wenig Daten: mögliche Lösung multiple kleinvolumige
1 1 1
Zyklen unter intraabdomineller Druckmessung (18 – 20 cm H2O)
Methods A prospective cohort study evaluated 154 patients, 37 on continuous Cibele
PD Puato
and Almeida
94 on HD. · André Luís
RespiratoryBalbi · Daniela Ponce
mechanics
parameters such as pulmonary static compliance (Psc) and resistance of the respiratory system (Rsr) and oxygenation index
(OI) were assessed for 3 days. Patients were evaluated at moments 1, 2 and 3 (pre- and
Received: post-dialysis).
23 January 2018 / Accepted: 1 June 2018
Results The initial clinical parameters were similar in the two groups, except© the age
Japanese that
Society was higher
of Nephrology 2018 in continuous PD
group (70.8 ± 11.6 vs. 60 ± 15.8; p < 0.0001). In both groups, Psc increased significantly, with no difference between the
two groups—pre-dialysis (continuous PD 40 ± 17.4, 42.8 ± 17.2, 48 ± 19; HD 39.1 ± 21.3, 39. 5 ± 18.9, 45.2 ± 21) and post-
Abstract
dialysis (continuous PD 42.8 ± 7.2, 48 ± 19, 57.1 ± 18.3; HD 42 ± 19, 45 ± 18.5, 56 ± 24.8). Rsr remained stable among
Background Peritoneal dialysis (PD) and hemodialysis (HD) are options for the treatment
patients on continuous PD (pre-dialysis 10.4 ± 5.1, 13.3 ± 7.7, 13.5 ± 10.3, post-dialysis 13.3 ± 7.7, 13.5 ± 10.3, 11.1 ± 5.9)
06.12.20 Dr. Mariam Abu-Tair patients. The aim of this study was to compare the effects of PD and daily HD on respirator
9
and decreased among HD patients (pre-dialysis 10.4 ± 5.1, 10.4 ± 5.1, 10.4 ± 5, 1, post-dialysis 10.5 ± 6.8, 10 ± 4.9, 8.9 ± 4.2).
undergoing invasive mechanical ventilation (IMV).Dialyseseminar Berlin 2020
European Review for Medical and Pharmacological Sciences 2018; 22: 2432-2438
Peritoneal dialysis effectively removes toxic
substances and improves liver functions of
liver failure patients
W.-X. Zhao, X.-M. Liu, C.-M. Yu, H. Xu, J.-R. Dai, H.-Y. Chen, L. Li, F. Chen, Y.-L. Ou, Z.-K. Zhao
W.-X. ZHAO, X.-M. LIU, C.-M. YU, H. XU, J.-R. DAI, H.-Y. CHEN,
L. LI, F. CHEN, Y.-L. OU, Z.-K. ZHAO EurRevMedPharmacolSci 2018; 22:2432-2438
Table III.
Nephrology Department, People’s Hospital of Chuxiong Yi Autonomous Prefecture, Fourth
AffiliatedGroup TNF- (pg/ml)
Hospital of Dali University, Chuxiong, China IL-6 (pg/ml) PCT (ng/ml)
Abstract. – OBJECTIVE: Liver failure (LF) is Key Words:
a clinically complex disorder that characterizes Liver failure, Peritoneal dialysis, Plasma exchange,
with hepatic dysfunction. This study aimed at Toxic substances, Liver functions.
observing the therapeutic effects of peritoneal
dialysis on liver function in LF patients.
PATIENTS AND METHODS: This study in-
p < 0.01 vsIntroduction
volves 62 patients diagnosed as LF hospital-
conservative treatment.2005
ized from February pDialyseseminar Berlin 2020
PD Katheter Implantation
Laparoskopisch: unter Sicht weniger Risiko einer Verletzung des Darms
Katheter liegt an gewünschter Stelle
Verwachsungen können ggfs. gelöst werden
Perkutan: einfach und schnell, bettseitig
Nutzung unmittelbar
06.12.20 Dr. Mariam Abu-Tair 11Dialyseseminar Berlin 2020
adapted from ISPD guidelines
06.12.20 Dr. Mariam Abu-Tair 12Dialyseseminar Berlin 2020
adapted from ISPD guidelines
06.12.20 Dr. Mariam Abu-Tair 13Dialyseseminar Berlin 2020
adapted from ISPD guidelines
06.12.20 Dr. Mariam Abu-Tair 14Dialyseseminar Berlin 2020
Ggfs. zu ergänzen
Antibiotika
Insulin
adapted from ISPD guidelines
06.12.20 Dr. Mariam Abu-Tair 15Dialyseseminar Berlin 2020
Peritoneal Dialysis International: Journal of the International 1.768
Society for Peritoneal Dialysis Journal In
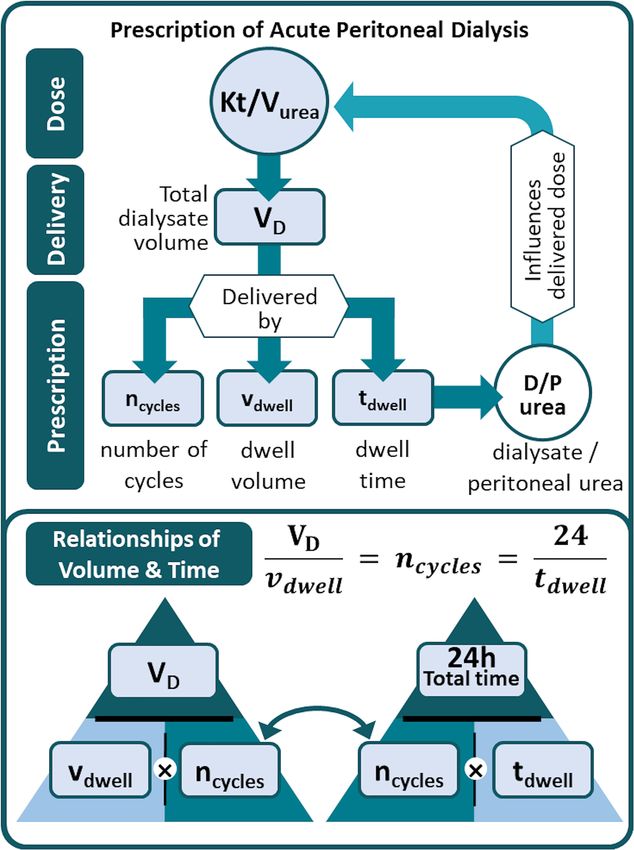
Peritoneal dialysis for acute kidney injury: Equations for dosing in pandemics,
disasters, and beyond
Chang Yin Chionh , Fredric O Finkelstein , Claudio Ronco
First Published November 11, 2020 Research Article
https://doi.org/10.1177/0896860820970066
Article information
Abstract
Background:
Peritoneal dialysis (PD) is a viable option for renal replacement therapy in acute kidney injury (AKI),
especially in challenging times during disasters and pandemics when resources are limited. While PD
techniques are well described, there is uncertainty about how to determine the amount of PD to be
prescribed toward a target dose. The aim of this study is to derive practical equations to assist with the
prescription of PD for AKI.
06.12.20 Dr. Mariam Abu-Tair 16Dialyseseminar Berlin 2020
Komplikationen bei Peritonealdialyse:
• Peritonitis/ intraabdominelle Abzedierungen
• Inadäquate Dialyse
• Exit- oder Tunnelinfekte
• Hernien und Leckagen
• Malnutrition durch Eiweissverluste
06.12.20 Dr. Mariam Abu-Tair 17Dialyseseminar Berlin 2020
Peritonealdialyse bei akutem Nierenversagen
Vorteile Nachteile
• techn. einfach • Bauchhöhle mit intakter
• kostengünstig Membranfunktion
• kein Gefäßzugang notwendig • nicht adäquat bei schwerem
• keine Blutverluste Lungenödem und
• biokompatibel lebensbedrohlicher
• schnellere renale Erholung Hyperkaliämie
• mehr kardiovask. Stabilität • UF kann nicht exakt bestimmt
• nicht nur für spezielle werden
Patientengruppen wie • mögliche Proteinverluste
Kinder, Pat. mit • mögliche Hyperglykämie und
Herzinsuffizienz, Hypernatriämie
Leberzirrhose, hämorrhagischer
Diathese
aus Seminars in Nephrology, Vol 37, NO1, Jan 2017,
pp103-112
06.12.20 Dr. Mariam Abu-Tair 18Dialyseseminar Berlin 2020
Peritonealdialyse ist
- einfach
- sicher und
- effizient, um metabolische Störungen, Elektrolytstörungen und Störungen des Säure
Basen und Volumen Haushalts zu beseitigen
In Kliniken mit PD Erfahrung sinken Mortalität und Komplikationsraten stetig.
Personalressourcen und Behandlungskosten sind geringer.
06.12.20 Dr. Mariam Abu-Tair 19Dialyseseminar Berlin 2020
PD als Alternative und sinnvolle Ergänzung auf der Intensivstation
Größer angelegte Studien zur Qualitätssicherung notwendig und damit
Eintrittskarte für die Nephrologie auf alle Intensivstationen
Vielen Dank für Ihre Aufmerksamkeit!
06.12.20 Dr. Mariam Abu-Tair 20You can also read

















































