Elective surgery without COVID-19 testing will lead to excess morbidity and mortality
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Elective surgery June 2021: 63:5
Pages 193–228
without COVID-19
testing will lead to
excess morbidity
and mortality
IN THIS ISSUE
Delay in diagnosis
and management of
adolescent ACL injuries
in patients with lower
socioeconomic status
Impacts of the COVID-19
pandemic on the
health and well-being
of young adults
Obesity as chronic
disease
Dr Jenn Tranmer:
Proust questionnaire
bcmj.org
June 2021
Volume 63 | No. 5
Pages 193–228
Emergency preparedness project in Kamloops. From left: Rhonda Eden, Graham Dodd, and Colin Swan. Article begins on page 220.
The BCMJ is published by Doctors of BC. The journal
provides peer-reviewed clinical and review articles 196 Editorials n Re: On the nature of being a
written primarily by BC physicians, for BC physicians,
Rights and freedoms professional, Brian S. Pound, MBBS
along with debate on medicine and medical politics in
David R. Richardson, MD
n Re: Managing vulnerable patients
editorials, letters, and essays; BC medical news; career
and CME listings; physician profiles; and regular columns. Restrictions on private health Roger Seldon, MBChB, MD
Print: The BCMJ is distributed monthly, insurance, Brian Day, MB
n Authors reply, Jennifer Laidlaw, MD,
other than in January and August. Leanne Lange, MPA,
Web: Each issue is available at www.bcmj.org. Erin Henthorne, MSW
Subscribe to print: Email journal@doctorsofbc.ca.
198 Letters
Single issue: $8.00 n Compliments to the artist
Canada per year: $60.00 Paul Thiessen, MD 200 President’s Comment
Foreign (surface mail): $75.00
n Value of family physicians Keeping you informed
Subscribe to notifications:
Robert H. Brown, MD during negotiations
To receive the table of contents by email, visit
www.bcmj.org and click on “Free e-subscription.” n Re: Lost art of physical examination Matthew C. Chow, MD
Prospective authors: Consult the Neil Finnie, MD
“Guidelines for Authors” at www.bcmj.org
for submission requirements.
n Re: The gender pay gap in medicine
Brenda Hardie, MD
Rita McCracken, MD
On the cover Editor Managing editor Proofreader Printing
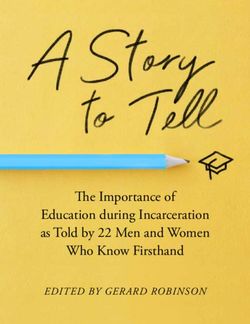
Elective surgery without COVID-19 David R. Richardson, MD Jay Draper Ruth Wilson Mitchell Press
testing will lead to excess
Editorial Board Associate editor Web and social media Advertising
morbidity and mortality
Jeevyn Chahal, MD Joanne Jablkowski coordinator Tara Lyon
Assuming 37 000 planned surgeries
David B. Chapman, MBChB Amy Haagsma 604 638-2815
are conducted per week in Canada Editorial and production
Brian Day, MB journal@doctorsofbc.ca
(excluding Quebec), and the prevalence coordinator Cover concept and
Caitlin Dunne, MD
of COVID-19 infection cases is 0.20%, the Tara Lyon art direction, Jerry Wong, ISSN: 0007-0556
David J. Esler, MD
number of avoidable deaths that could Peaceful Warrior Arts Established 1959
Yvonne Sin, MD Copy editor
occur is estimated to be 11.7 but could
Cynthia Verchere, MD Tracey D. Hooper Design and production
exceed 17.0. Article begins on page 208.
Laura Redmond, Scout Creative
194 BC Medical Journal vol. 63 no. 5 | june 2021
ElECtivE surgEry without CoviD-19 tEsting
201 News WIll leAD TO exCeSS MOrbIDITy AnD MOrTAlITy
n Book review: Dreamers, Skeptics, and
Healers: The story of BC’s medical school We are not routinely testing patients for COVID-19 prior to surgery.
n What is critical illness insurance? There are known morbidity and mortality dangers
to performing surgery on infected people.
n Grant to offset costs of recruiting
into team-based care practices
n Preventing symptom escalation
among mild COVID-19 patients
204 BCMD2B 0.20% 77%
Clicks, tweets, and likes Assumed active Risk of operating on at least
1 person with COVID-19
case prevalence
Faizan Bhatia, MD, Arman for every 500 surgeries
Mojtabavi, BSc, Azim Ahmed, BSc,
Vishal Varshney, MD, Alana M. As well as increased risk to patients, operating on COVID-19 patients risks transmission to hospital staff.
The authors recommend mandatory preoperative COVID-19 testing for planned operations.
Flexman, MD
TheA.A.
authors argue that
Karimuddin, patients should
J.M. Sutherland, be tested for COVID-19 prior to planned operations to prevent avoidable surgical
S.M. Wiseman
207 WorkSafeBC complications and mortality. Article begins on page 208.
BCMJ 2021;63:208-210
Workers Compensation Act
amended to include COVID-19
Michelle Vukelic
217 BCCDC 220 Shared Care
CLINICAL Last in line: Impacts of the Emergency preparedness project
COVID-19 pandemic on the health rises to the challenge with pandemic
208 Elective surgery without and well-being of young adults in response, Graham Dodd, MD
BC, Hasina Samji, PhD, Naomi
COVID-19 testing will lead
Dove, MD, Megan Ames, PhD, 221 CME Calendar
to excess morbidity and
Meridith Sones, MPH, Bonnie
mortality, Ahmer A. Karimuddin, 222 Obituaries
Leadbeater, PhD
MD, Jason M. Sutherland, PhD, Dr Robert Lachlan MacLeod Coupe
Sam M. Wiseman, MD 218 College Library
Hidden gems on the bookshelves 223 Classifieds
211 Delay in diagnosis and Karen MacDonell
management of adolescent 226 Proust
anterior cruciate ligament 219 Council on Health Promotion Dr Jen Tranmer
injuries in patients with lower Obesity as chronic disease
socioeconomic status Ilona Hale, MD, Priya Manjoo, MD
Lise Leveille, MD, Tessa Ladner,
BSc, Christopher Reilly, MD
Environmental impact Postage paid at Vancouver, BC. Canadian Publications Mail, Product Sales Agreement #40841036. Return undeliverable copies
The BCMJ seeks to minimize its negative impact on the to BC Medical Journal, 115–1665 West Broadway, Vancouver, BC V6J 5A4; tel: 604 638-2815; email: journal@doctorsofbc.ca.
environment by:
Advertisements and enclosures carry no endorsement of Doctors of BC or BCMJ.
• Supporting members who wish to read online with an
e-subscription to bcmj.org © British Columbia Medical Journal, 2021. All rights reserved. No part of this journal may be reproduced, stored in a retrieval system, or trans-
• Avoiding bag use, and using certified-compostable plant-based mitted in any form or by any other means—electronic, mechanical, photocopying, recording, or otherwise—without prior permission in
bags when needed writing from the British Columbia Medical Journal. To seek permission to use BCMJ material in any form for any purpose, send an email to
• Working with Mitchell Press, ranked third in North America for journal@doctorsofbc.ca or call 604 638-2815.
sustainability by canopy.org Statements and opinions expressed in the BCMJ reflect the opinions of the authors and not necessarily those of Doctors of BC or the
• Printing with vegetable-based inks institutions they may be associated with. Doctors of BC does not assume responsibility or liability for damages arising from errors or omis-
• Using FSC-certified paper sions, or from the use of information or advice contained in the BCMJ.
• Printing locally in British Columbia The BCMJ reserves the right to refuse advertising.
BC Medical Journal vol. 63 no. 5 | June 2021 195
Editorials
Rights and freedoms
4 May 2021
I
am writing this editorial as the provincial the powers that be made travel restrictions more receive increasingly suspicious glances thrown
government just announced sweeping re- stringent with the threat of roadblocks and in my direction as the belief grows that maybe
strictions preventing British Columbians fines. Tourism providers have been asked to I am part of “they.”
from moving between three defined regions. cancel and refund customers who are from out- A quick evaluation of our elected officials
Stuck between a rock and a hard place, the side their regions. All recreational vehicles have should be enough to doubt the government
government made this difficult decision due to been banned on BC Ferries. conspiracy idea. In addition, if you have ever
rising COVID-19 case numbers with hospi- As soon as these re- had to deal with any
talizations and ICU admission levels reaching strictions were announced, government body, you’ll
all-time pandemic highs. Despite pleas from angry comments began Despite pleas from recognize that the level
our provincial health officer, people contin- to appear on social me- our provincial health of organization required
ue to travel and are propagating viral spread dia about infringement of to form a secret agency
officer, people
through their actions, albeit often unknowingly. our basic rights and free- seems an unobtainable
Pandemic fatigue has led to the population doms. I even had some pa- continue to travel goal. Furthermore, I am
craving some degree of normalcy and perhaps tients complain that this and are propagating pretty sure Bill Gates has
reducing their commitment to follow provin- was just another way that viral spread through enough money and access
cial guidelines. “they” were trying to con- their actions, albeit without monitoring or re-
Worried that this third viral wave has the trol us. These are often the stricting the population’s
potential to overwhelm our hospital resources, same individuals who are
often unknowingly. activities.
against vaccines and mask Society already limits
wearing. (I also suspect many of them have red many individual choices for the good of the
MAGA hats hidden in their closets.) majority. For example, I’m not allowed to drive
I have often wondered who “they” are. I have drunk as a skunk without my seatbelt on at my
Secure cloud-based clinical even asked some of my patients, but I never chosen speed down the wrong side of the high-
speech recognition seem to get a clear answer. As best as I can way with a baby smoking on my lap.
tell, “they” is some secret level of government The current temporary travel restrictions are
Dictate into your EMR from or a collection of sinister wealthy individuals no different and were created to buy time while
almost anywhere (Bill Gates is often mentioned) who want to the vaccination process continues.
track and control our movements. When I ask “They” are simply trying to save some
Install within minutes across to what end would “they” want to restrict us, lives. n
unlimited computers I do not get a definitive answer. I do, however, —David R. Richardson, MD
One synchronized user
profile
Stunningly accurate with
accents
Contact us today for a free trial!
604-264-9109 | 1-888-964-9109
speakeasysolutions.com EA
SY SOLU
T
21
K
IO
SPEA
Professional Speech
NS
Technology Specialists YEARS OF EXCELLENCE
2000 - 2021
196 BC Medical Journal vol. 63 no. 5 | june 2021
Editorials
Restrictions on private health
insurance
W
“ ithout a right of challenge through appearance remains vivid. The judge arrived accepted that harms and deaths were avoidable
an independent body such as the in an escorted and chauffeured Rolls-Royce if doctors did their job properly. Government
judiciary, our legislative and ex- limousine with a small Union Jack flag on the lawyers described desperate and suffering pa-
ecutive bodies would be free to make arbitrary front. He wore impressive crimson and black tients accessing private clinics as “parasitic.”
and discriminatory decisions respecting the robes. He and the barristers wore wigs and The world has seen changes since the lower
health care benefits provided to Canadians with went through scenic and impressive court for- court hearings concluded, with the COVID-19
little or no consequence. Such a result would malities and rituals. All of pandemic being the most
be contrary to the societal values upon which these experiences, togeth- impactful. Our already
Canadian society is built.” Chief Justice Chris- er with our intervention We remain optimistic underperforming health
topher Hinkson of the BC Supreme Court in the 2005 Chaoulli trial, system now faces even
made this statement in November 2005. gave me some insight into
that the higher greater pressures.
This month, Justice John Steeves’ 2020 BC our legal case. courts will take some We will argue before
Supreme Court decision supporting govern- Significant differenc- guidance from the the higher courts that
ment restrictions on private health insurance es between Chaoulli and Chaoulli precedent. Canadian jurisdictions,
and physicians’ dual practice will face a judi- our case included the which ban patient choice
cial review by the BC Court of Appeal. This multiple patient plain- and exclude a safety valve,
appeal will rely almost exclusively on the evi- tiffs and the fact that we had authenticated, violate human rights. Even government experts
dence at trial, focusing on errors in law by the government-accepted, maximum wait times at trial gave evidence that Canada’s monopo-
trial judge. Justice Steeves had, coincidentally, for thousands of procedures. Courts no longer listic system is unique, and that all countries
received government-funded surgery at the had the burden of interpreting or defining what permit private sector participation.
private False Creek Surgical Centre. was acceptable. Governments had done that for Chaoulli also lost at the lower-court level in
Our legal challenge began in January 2009. them, and the trial judge acknowledged that, Quebec. We remain optimistic that the higher
We had expected that government would want despite downplaying their relevance. courts will take some guidance from the Cha-
a quick decision on whether its laws violated This data will, we hope and believe, prove to oulli precedent. In discussing the Chaoulli case,
the Canadian Charter of Rights. However, be vitally important and pivotal in later hear- Canada’s most renowned constitutional scholar,
the trial did not start until late 2016 and con- ings. For example, in 2017–2018, only 16% to the late professor Peter Hogg, QC, opined that
sumed 194 court days going into a fourth year. 38% of patients needing treatment for serious no provincial government would risk arguing
The 880-page written decision was unusually cancers of the bladder, ovary, prostate, lung, that their citizens deserved less freedom under
lengthy. and colon were treated within the maximum the law than those living in Quebec.
Like for many doctors, my courtroom expe- acceptable benchmark. Unfortunately, for the BC has proven him wrong.
rience has mostly been as an expert in patient tens of thousands of BC patients waiting, suf- Hogg also wrote: “No one was watching the
injury trials, but I had some previous informal fering, and sometimes dying on wait lists, the Chaoulli case as it bubbled on up, but people will
legal education. In the early 1960s I enjoyed a government’s own self-incriminating data were be watching the second case very, very closely. I
long-running and successful television show, largely ignored by the lower court. think in practical terms the ruling is extremely
Boyd QC, and a decade later, Rumpole of the Government lawyers implied that private important even if not literally binding for the
Bailey. More recently I watched Suits. Perhaps care was for the “wealthy and healthy,” despite rest of the country.”
more impactful was my even earlier “hands-on” the fact that not one patient witness was either. I have no doubt he will be proven right on
experience as a 5-year-old Crown witness (then The BC government did not call a single BC that. n
one of the youngest in legal history) in a Liver- patient witness or a single BC physician as an —Brian Day, MB
pool criminal trial. I gave evidence identifying expert. They focused on demonizing doctors for
a thief I had witnessed stealing a watch (from not accurately “triaging” patients and foreseeing
my own wrist). He was convicted and sentenced and forestalling any complications that wait-
to jail time. My recollection of that courtroom ing patients might possibly suffer. The judge
BC Medical Journal vol. 63 no. 5 | June 2021 197
for the PMA and gender equity could be a value
Letters to the editor We welcome
original letters of less than 300 words; we may edit them for clarity
that is baked into the process. Imagine what we
might achieve if this were the case!
I am excited that you have opened up this
and length. Letters may be emailed to journal@doctorsofbc.ca, submitted conversation in a meaningful way for Doctors
online at bcmj.org/submit-letter, or sent through the post and must include of BC and all of us in the province. I look for-
your mailing address, telephone number, and email address. Please disclose ward to reading more articles on what we are
any competing interests. doing and how well we are making progress to
reduce the gender pay gap. Thanks for taking
this brave step, since we know you are likely to
experience significant backlash as a result of
Compliments to the artist proceed to the OR, recognizing that it might
rarely end as an exploratory event. It’s now quite speaking out for gender equity.
The April issue’s cover image is credited to Jerry
kosher to listen to breath and heart sounds —Brenda Hardie, MD
Wong (Peaceful Warrior Arts). I want to pay a
through clothing—it’s happened to me, by a North Vancouver
compliment as this is truly one of the best and
most inspired covers I can recall. It truly illus- fine young physician. The world moves on, but
practising the fine points of physical diagnosis I appreciate Dr Sin’s call to action in her April
trates the story on ectopic pregnancy. I hope it
need not be a dying art. editorial [BCMJ 2021;63:101]: “Ultimately, the
is entered into some contest, as it’s a real winner!
—Neil Finnie, MD question we should each be asking ourselves is
—Paul Thiessen, MD, FRCPC
Victoria not whether a gender pay gap exists in medicine,
Vancouver
but what can I do to help close it?” And I urge
Re: The gender pay gap in our professional representative body (Doctors
Value of family physicians medicine of BC) and our main payer (BC Ministry of
Yesterday we were in need of a professional gas Health) to (1) engage experts to do a review of
Thank you, Dr Sin, for your April editorial
fitter to make a house call to fix a problem with processes and structures that are maintaining
on this important topic [BCMJ 2021;63:101].
a gas line in our home. It was a simple problem the gender pay gap, despite intentions to have
Studies show that women also have increased
for him, requiring about 10 minutes. His fee it change, and (2) start to publicly report what
rates of burnout compared with male colleagues.
was $156 plus tax for a basic house call. I con- this examination finds.
The pandemic has had an extra toll on women,
trast that with a basic house call that I make —Rita K. McCracken, MD, PhD, CCFP (COE), FCFP
making all of this much worse.
as a physician. The last time I looked, the fee Vancouver
You point out that there are some clear rec-
was about $110. I am thankful that none of my
ommendations that have been made to work
five children have chosen family medicine as a
to close this gap. We know this is a complex Re: On the nature of being a
career. They are all in technical trades or engi-
neering. It is interesting that I am to conclude
issue that will take many nuanced chang- professional
es, but a few broad strokes can happen now. Bravo, Dr Chow! I’m retired from practice now
that the services of a gas fitter are about 50%
Encouraging men to take parental leave is a after 50 years as a GP/FP and found your ar-
more valuable to society than the services of a
wonderfully achievable place to start, and is ticle in the April issue to be a breath of fresh air
family physician based on the fees paid to these
evidence-informed. Maybe we will see Doctors [BCMJ 2021;63:105]. The profession is facing
two respective professions.
of BC promote this more widely. Doctors of decreasing numbers of physicians. Physician
—Robert H. Brown, MD, CCFP
BC could also be targeting and measuring its burnout has become a byword. Physicians are
North Saanich
success in having women in leadership roles, losing the esteem from their patients, while
and being transparent about what percentage other health care professionals are enjoying
Re: Lost art of physical of stipends goes to men versus women might increasing popularity from their patients and
examination be an enlightening project. The kind of encour- clients. To be a physician was once to also be
I really appreciated Dr Walton’s germane reflec- agement needed for women to be in the places a trusted member of a patient’s and their fam-
tion on the role the physical examination seems where decisions are made is often structural. ily members’ special circle, trusted as a car-
to play in patient assessment these days [BCMJ This is not phoning, emailing, and telling them ing friend, but alas, the pressures of practice,
2021;63:102]. I’m one of those Neanderthal they would be great and should apply—not that bureaucracy, paperwork, and rules of conduct
retired family docs who practised before CT kind of encouragement. We are talking about have disenfranchised us from the art of med-
scans, MRIs, and other magical technologies. changing how we recruit, support, and retain icine, often creating a seemingly adversarial
An acute appendix was first on a differen- women in leadership by making gender equity relationship with those we care for. Your phi-
tial diagnosis as the result of history and spe- a priority through tangible goals, metrics, and losophy of medical practice illustrates a means
cific physical examination. It was okay to then system improvements. This is negotiation time to bring back the very real joy of being that
198 BC Medical Journal vol. 63 no. 5 | june 2021
letters
caring professional friend to those we care for. Authors reply Thought must also be given to how using
Thank you for the wise encouragement. Regarding use of the Adult Guardianship Act a support and assistance plan can modify the
—Brian S. Pound, MBBS, LRCP, MRCS, LMCC (AGA) for individuals with chronic substance identified risks of using substances, recognizing
Victoria use, it should be clarified that the Act allows that we cannot typically force individuals to ab-
involuntary admission in hospital to investigate stain from substances alone. Exceptions to this
Re: Managing vulnerable patients whether a person meets full criteria for Section do occur, rarely, for individuals with significant
I was interested to read the April 2021 article, 59. Section 59 allows ongoing hospitalization vulnerabilities; for example, a neurocognitive
“Management of vulnerable adult patients seek- until a support and assistance plan can be put disorder rendering them at risk of regular and
ing to leave hospital: Understanding and using in place to try to mitigate the risks of, in your significant substance abuse causing self-neglect.
relevant legislation,” having had just such a co- example, self-neglect. The first criterion of the However, these cases typically exist after less
nundrum during my shift the previous evening. AGA is that the adult is unable to seek sup- intrusive measures have failed and are likely to
Unfortunately, the article did not specifically ad- port and assistance when needed.1 Such assess- involve a court-ordered support and assistance
dress a certain common situation. Any insights ments are conducted by a designated responder, plan that restricts an individual’s access to sub-
from the authors would be much appreciated. typically a social worker, once an individual is stances due to residing in a care facility.
no longer intoxicated. Assessments for AGA Regarding the issue of “alcohol-induced
Incapacity due to addiction eligibility will often incorporate information incapacity,” it is important to answer the ques-
By my reading of the article, my patient (whose or assessments from other disciplines, such as tion, capacity for what kind of decision? It is
parents were strongly advocating be involun- occupational therapy, psychiatry, or geriatric certainly reasonable to question an individual’s
tarily admitted due to severe and progressive medicine to assess for factors that increase vul- capacity to make decisions about how they live
self-neglect as a result of alcoholism) fulfills nerability while not intoxicated, such as neu- their life when they are living at significant risk.
the criteria to allow treatment under the Adult rocognitive disorders. For many individuals For example, does the patient have capacity to
Guardianship Act (AGA) (1. self-neglect, 2. without baseline cognitive impairment, the pa- make decisions about being homeless, or using
risks, already experienced—e.g., loss of li- tient will demonstrate an ability to seek support substances? However, housing or substance
cence to drunk driving, assault charges etc., and assistance when not under the influence of use are not medical treatments and, therefore,
and 3. incapacity due to chronic unremitting substances, rendering them ineligible for Sec- don’t fall under the Health Care (Consent) and
intoxication). tion 59. However, if a patient shows that they Care Facility (Admission) Act. Therefore, say-
It is not regular practice to force treatment are unable to seek support and assistance even ing that an individual is incapable of making
due to addictions. This patient was kept under once they are no longer intoxicated, for example decisions regarding substance use or housing
the Health Care (Consent) and Care Facility because of a neurocognitive disorder secondary does not permit us to take any action in the
(Admission) Act until sober enough to ambulate to alcohol use, they may meet the criteria for way of appointing a substitute decision maker
safely and have a discussion regarding his situ- Section 59 if the other criteria are also satisfied, as we would for medical treatment. Further-
ation, at which point he could voluntarily con- as outlined in Figure 1 of our article.2 more, even if someone fails to see the negative
tinue treatment or leave against medical advice. foreseeable consequences of their substance use,
Continued on page 201
Is this sober window (reportedly the only such
window in a very long time) enough to allow
the patient to voluntarily proceed back into his
state of chronic alcohol-induced incapacity (not
withstanding that the illness of addiction renders
the patient incapable of avoiding further intoxica-
tion)? If it is not, should we be using the AGA
routinely in cases of addicted vulnerable adults?
Also, the fictional case of Ms Safe was a
useful illustration. I imagine the statement
that she’d “be fine” was explored in more detail.
What if she’d meant: (1) I’ll be fine because I
wish to die from this illness, or (2) I understand
the risks you’re telling me but I’ll be fine with
the natural medicines I’m using, or my faith
that God will heal me?
—Roger Seldon, MBChB, MD
Campbell River
BC Medical Journal vol. 63 no. 5 | June 2021 199
president’s comment
Keeping you
informed during
negotiations
A
s I write this at the end of April, the steps in preparing for and conducting the Negotiations Update, which will include as
our province is facing a surge of PMA negotiations. much information as we are able to disclose
COVID-19 cases. My neighborhood We have reached out to members in nu- and that will be updated regularly.
has been designated a high-transmission com- merous ways to determine your key priorities. Phases two and three of negotiations will
munity, and I have been encouraging, cajoling, These have included our negotiations survey, come into play if phase one is not successful.
and even pleading with all my neighbors to get meetings with the sections and other physician We would move into mediation and potential-
vaccinated. Perhaps shouting, “Get your shot!” groups, Zoom webinars, ly into conciliation, which
out my car window to pedestrians was a bit and a Representative As- ends with the release of a
much, but perhaps not. While I cannot claim sembly workshop. We will be more report from a neutral con-
any prescient ability, what I do know is that Among a number of proactive about ciliator. This is where we
doctors—wherever you are and whatever you priorities important to take the public foundation
communicating with we have built and increase
do—will have given your very best and fought you, which will be brought
hard for your patients. I, and every person in to the table, are two spe- members during the it, along with a number of
this province, thank you for this. cific ones that were shared negotiations process. other possible measures.
And now turning to something different: by a large majority of We have not had to do
negotiations. The 2019–2022 Physician Mas- members: addressing the this in recent times, but it
ter Agreement between Doctors of BC and continually increasing cost of running a prac- will come as no surprise to you that we expect a
the government will end on 31 March 2022. tice and the funding and provision of virtual challenging negotiation given the general state
Formal negotiations for our next agreement services on a permanent basis. These, among of society as it emerges from the pandemic.
begin in June. others, will be considered by the Board as its Bottom line, we want our communications
In the past, members have said they want to sets the mandate for the PMA negotiations. to you to demonstrate that you are being heard,
be better informed as we go through the pro- While we are in negotiations, public opinion that we understand your concerns, and that the
cess, which we will do to the best of our ability. is important because it will affect government negotiations team is doing its best to take your
Doctors of BC and the government have agreed priorities. We will continue to promote the requests into account. n
not to speak publicly about our bargaining posi- value doctors bring to the health care system, —Matthew C. Chow, MD
tions, the status of negotiations, and how talks their patients, and communities, and the effects Doctors of BC President
are going. This is not unusual—bargaining that of a shortage of doctors in several critical areas.
takes place in the public domain often signals During this pandemic year, we are able to talk
a serious problem. Still, we know you want to about how doctors showed leadership provin-
understand what is going on and how it will cially and in their communities, how quickly
affect you. doctors were able pivot to virtual care, and the
To this end, we will be more proactive about invaluable contribution of doctors to main-
communicating with members during the ne- taining capacity within the health care system.
gotiations process, within the limits of bargain- Our negotiations communications to mem-
ing rules. This will be a multiphased approach. bers will mostly be via the In Circulation elec-
We are currently in phase one, our lead-up tronic newsletter. For those who have not yet
to and moving through formal negotiations. signed up for it, I encourage you to do so at
Our goal during this stage, which could last www.doctorsofbc.ca/account/subscriptions (log
up to a year, is to keep members informed of in required). There is now a special section titled
200 BC Medical Journal vol. 63 no. 5 | june 2021
letters
Continued from page 199
which suggests incapacity, existing legislation
does not address forcing individuals to abstain News We welcome news items of less than 300 words; we may
from substances alone if they are incapable of edit them for clarity and length. News items should be emailed to journal@
making a decision to use them. Instead, it is doctorsofbc.ca and must include your mailing address, telephone number, and
best to focus on whether an individual meets email address. All writers should disclose any competing interests.
criteria for the AGA, or in some cases, the
Mental Health Act.
Regarding the case of Ms Safe, she had
communicated that she thought her health I arrived in Vancouver in 1947 as an
would remain unchanged or stable without IV 18-year-old immigrant, full of hope that I
antibiotics. Therefore, Ms Safe failed to ap- might be able to enter medical school here. I
preciate the foreseeable negative consequences learned with considerable anxiety that there
and risk of death if she refused treatment, was no medical school in BC, and that the
rendering her incapable of making a deci- likelihood of one opening soon was not very
sion to decline medical treatment. In reply good. Only 4 years later, I was in UBC Medi-
to another of your examples, such as if the cine’s second graduating class of 60 students,
patient said she wished to die from her illness, when the school was still located in former
that suggests she understands the foreseeable army barracks. Skeptics were abundant from
consequences of declining treatment, which is before the school opened and throughout its
one of several important criteria of capacity. early years; it was the dedicated deans, scien-
In our experience, that kind of response could tists, and healing practitioners who brought
signal a potential desire for hastened death, the dreams to reality.
which would trigger a psychiatric consult to This very handsome, easy-to-read book
rule out an underlying mood disorder. For the includes wonderful pictures of many of the
other examples, capable patients may have doctors, healers, scientists, and administra-
spiritual beliefs or preferences for nonconven- tors who made the school what it is today.
tional treatments. The test of capacity would The book is divided into seven parts. It starts
be whether the patient understands the nature with Dr John Sebastian Helmke’s ideas for
and anticipated effects of the proposed investi-
Book review: Dreamers,
a health service, for a then fledgling popula-
gation or treatment and available alternatives, Skeptics, and Healers: The tion, in the 1870s. And it ends with a proud
including the consequences of refusing.3,4 story of BC’s medical school celebration of the research and innovation that
—Jennifer Laidlaw, MD, FRCPC By Wendy Cairns; John Cairns, MD; Da- has taken place over the past 70 years, with
—Leanne Lange, MPA vid Ostrow, MD; Gavin Stuart, MD. Van- ideas for the future.
—Erin Henthorne, MSW, RSW couver: Page Two Books, 2021. ISBN In between are accounts of how the school
978-1-989603-89-5. Hardcover, 224 pages. took off after years of arguments and disap-
References The mastermind behind this history of pointments, the unavoidable growing pains,
1. Province of British Columbia. Adult guardianship UBC Medical School was UBC graduate and how it came into a respected early ma-
act. Victoria, BC; 2020. Accessed 25 August 2020. Wendy Elizabeth Cairns. After her premature turity, with some unexpected turnarounds, to
www.bclaws.ca/civix/document/id/complete/
statreg/96006_01.
death in 2018, her husband and former dean become a world famous medical school (the
2. Laidlaw J, Lange, L, Henthorne, E. Management of of the medical school, Dr John Cairns, along Faculty of Medicine is now home to more
vulnerable adult patients seeking to leave hospital: with Dr David Ostrow and Dr Gavin Stuart, than 4500 undergraduate, graduate, and post-
Understanding and using relevant legislation. BCMJ took up the pen to expand on and complete graduate students), with students learning the
2021;63:106-111.
3. Canadian Medical Protective Association. Is
the process of turning Wendy’s rich research art and science of medicine in almost every
this patient capable of consenting? 2021. Ac- materials into this book. The title, Dreamers, district of BC.
cessed 11 May 2021. www.cmpa-acpm.ca/en/ Skeptics, and Healers, accurately reflects the I had the feeling of reliving my student
advice -publications/browse -ar ticles/2011/ history of a medical school that admitted days as I read the sections on how Dr Kerr
is-this-patient-capable-of-consenting.
4. Canadian Medical Protective Association. Aid to
its first class in 1950 after years of contro- and Dr Walters conducted our oral exams at
capacity evaluation. 1996. Accessed 11 May 2021. versy and is now counted among the largest the bedside, how Dr Friedman, the head and
www.cmpa-acpm.ca/static-assets/pdf/education- and most respected medical schools in North professor of anatomy drew his diagrams on
and-events/resident-symposium/aid_to_capacity_ America. the blackboard with two hands at the same
evaluation-e.pdf.
BC Medical Journal vol. 63 no. 5 | June 2021 201
news
time, or how Dr John William Boyd, head and up with a plan for increasing the number of insurers, should you want additional features
professor of pathology, entertained us with his medical students and a plan for a campus hos- beyond what the group plan offers, such as pre-
witty lectures. pital or lose out on an unclaimed federal fund mium refund upon cancellation.
Each dean’s vision and legacy for the school that was about to be closed. Student numbers Critical illness insurance provides protection
over 70 years is sensitively explained. Some have were increased. against expenses that can come with a serious
come to life; some have not. For example, Dr The book will rekindle memories for some illness, and it can give you peace of mind that,
McCreary’s vision for an “if they learn togeth- and bring an understanding to nonmedical if you are diagnosed with one of the covered
er, they will work together” teaching program readers of the extreme complexity of gathering conditions, you will not derail your retirement
for all health professionals, for the purpose of and maintaining the enthusiasm of dedicated savings plan or be faced with increasing debt
strengthening integrated patient care by health practitioners, scientists, students, and other to assist with recovering. Proof of good health
sciences teams, is still not a reality. health-related professionals with the goal of is required at time of application to determine
Each section also introduces the leading understanding nature and serving mankind. eligibility. Doctors of BC advisors are avail-
figures in the various basic science and clinical —George Szasz, CM, MD able to discuss coverage options that best suit
faculties. The pictures of Dr Copp of physi- your needs.
ology, Dr Williams of dermatology, Dr Bry- What is critical illness —Hali Stus
ans of obstetrics and gynecology, Dr Slade of Insurance Advisor, Members’ Products
family practice, and many others will evoke
insurance? and Services
warm memories in former students. And, of As one of the licensed, noncommissioned
insurance advisors with Doctors of BC, I
course, there is the politics. I was at the tense Grant to offset costs of
locked-door meeting described in the book with meet with physicians every day to talk about
member-exclusive insurance offerings. Critical recruiting into team-based
Dr Pat McGeer, a graduate of the school, ac-
complished neuroscientist, UBC faculty mem- illness insurance is now part of every discus- care practices
ber, and BC’s Minister of Education at the time. sion, though it is less understood than life or A new team-based care grant provides $15 000
He issued an ultimatum to the university: come disability insurance. to eligible family practices that have onboarded
Critical illness insurance was introduced interprofessional team (IPT) members. The
to the insurance industry on 6 October 1983. grant will help to address the costs of recruit-
The founder, South African cardiac surgeon, Dr ing and onboarding into a practice, and it is just
Marius Barnard, identified a gap in the insur- one of the resources provided by the GPSC to
ance industry through the care of his patients. help break down barriers and provide supports
British Columbia
Since then, critical illness insurance has been for practices to implement team-based care.
Medical Journal
@BCMedicalJournal
accepted into insurance markets around the
world. These policies provide the insured with How does it work?
British Columbia Medical Journal a tax-free, one-time predetermined lump-sum The grant provides a lump sum payment of
@BCMedicalJournal payment in the event you are diagnosed with $15 000 for each FTE of net new eligible IPT
Systemic racism and medicine: A commentary
one of the 25 illnesses covered under the policy. positions filled by the family practice applying
You may wonder how this is different from for the grant. An eligible IPT position may be
A reflection on historical mistakes that we must
recognize and learn from to catalyze positive change.
disability insurance. While disability insurance filled by a staff member employed by the fam-
is designed to replace your income, critical ill- ily practice or another organization, such as a
Read the Premise: bcmj.org/premise/systemic-racism
-and-medicine-commentary
ness insurance is designed to help with costs so health authority. Eligible family practices may
you can focus on your health. These costs may apply for the grant for net new eligible IPT
include medical treatment not covered by MSP positions filled on or after 1 April 2019. An end
or your extended health benefits policy, in-home date has not yet been established for this grant.
care, modifications to your home, equipment to
assist with mobility, or replacement of income What are the requirements?
from a spouse who is caring for you. If you are A minimum of 0.5 FTE of IPT position is
fortunate to have a speedy recovery, you can use required to apply for this grant. To claim this
the money to pay down debt or top up savings. grant, a group of family doctors must submit
Doctors of BC offers a group term plan an online application form together after an
that is available to members, their spouses, and IPT position has been filled. Doctors and clinic
dependent children. In addition, our insurance owners may agree on how the funding is dis-
Follow us on Facebook for regular updates advisors can offer policies from major Canadian tributed among the parties.
202 BC Medical Journal vol. 63 no. 5 | june 2021news
What does it cover?
These are some examples of what family doctors
can do with the grant:
• Cover the cost of setting up and upgrading
EMR software and licensing and office
hardware to enable interprofessional care.
• Compensate physicians or clinic staff for
time spent:
• Reviewing and implementing changes
to office capacity to accommodate new
IPT members.
• Recruiting, interviewing, hiring, and
onboarding new IPT members.
• Reviewing medicolegal requirements
relevant for particular IPT members.
Are you eligible?
To be eligible, family doctors of the group prac-
tice applying for the grant must:
• Work within a group practice consisting of
two or more physicians that has added an
eligible IPT member to the group practice.
The physicians working together in a group
practice may or may not be co-located and
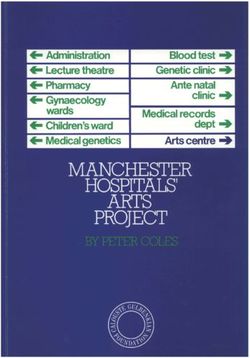
may have an arrangement to jointly fund Preventing symptom escalation among mild
an IPT position. COVID-19 patients
• Meet the definition of a community longi-
With several treatments available to care for the most urgent and severe cases of COVID-19,
tudinal family physician as per the GPSC
researchers are now investigating whether a common anti-inflammatory drug, ciclesonide,
preamble.
could help speed recovery in mild cases and put a stop to disease progression and potential
• Have completed phase two of the GPSC
hospitalization. When inhaled, the medication is directed to the nose and airways, the
phases of panel management.
areas of the body most affected by the COVID-19 virus. While the long-term effects of
• Commit to participating in quality im-
the virus are not fully understood, studies have found that any level of disease severity can
provement activities related to team-based
result in persistent physical and psychological symptoms. Ciclesonide has been shown to
care such as services offered through the
prevent viral activity against SARS-CoV-2 in some lab-based studies, and researchers
GPSC Practice Support Program, in-
hypothesize that giving it to patients early in the course of the disease could prevent the
cluding team-based care coaches. Quality
virus from replicating further and causing an increased inflammatory response.
improvement activities should be aligned
Ciclesonide was approved by the US Food and Drug Administration in January 2008
with the National Interprofessional Com-
for use in humans to treat asthma, rhinitis, and other nasal and airway conditions. The
petencies Framework.
CONTAIN study team selected ciclesonide as a possible treatment option because of its
• Agree to work collaboratively with the
low rate of side effects and drug interactions, as well as evidence linking this particular
Ministry of Health, the primary care net-
steroid with antiviral effects.
work (if applicable), and other partners to-
Dr Sara Belga, a clinical assistant professor in the Division of Infectious Diseases at
ward implementing the attributes of the
the University of British Columbia, is the principal investigator in the province of the
patient medical home and primary care
CONTAIN study, headed by Dr Nicole Ezer from the McGill University Centre for
network.
Health Outcomes Research. The study is recruiting individuals living in Quebec, Ontario,
For more information, visit https://gpscbc
or British Columbia. Adults 18 years and older can qualify to participate if they apply via
.ca/news/news/grant-announced-gpsc-offset
the CONTAIN study’s online portal within 5 days of being diagnosed with COVID-19.
-costs-of-recruiting-team-based-care-practices.
Eligible participants must also be recovering at home with a mild fever, shortness of breath,
and/or symptomatic cough. Visit www.contain-covid19.com for more information about
the study and how to participate.
BC Medical Journal vol. 63 no. 5 | June 2021 203BCMD2B
Clicks, tweets, and likes
Social media use by medical journals.
Faizan Bhatia, MD, Arman Mojtabavi, BSc, Azim Ahmed, BSc, Vishal Varshney, MD, FRCPC,
Alana M. Flexman, MD, FRCPC
ABSTRACT: Medical literature is expanding at an level of engagement with Twitter (100%), YouTube Methods
astonishing rate and physicians are increasingly (94.3%), Facebook (64.5%), and Instagram (62.5%). This analysis did not require ethics approval as
using social media professionally. Currently, we lack General (versus specialty) medical journals had all information was publicly available. The rank-
a comprehensive understanding about the use of higher H-indices and a larger numbers of followers ing of medical journals was obtained through
social media by medical journals. We included the on Twitter and Facebook. Higher-impact journals SCImago Journal and Country Rank database
top 100 medical journals by H-index, and analyzed were more likely to have social media accounts, (www.scimagojr.com). We selected the most
88 journals after excluding nonmedical journals. although this finding was not observed when con- recent ranking (2019) of the top 100 journals
We described the use of social media platforms trolling for journal type. The use of social media to by H-index. We excluded journals that were not
and followers stratified by H-index and journal facilitate education and knowledge dissemina- primarily focused on clinical medicine.
type (general versus specialty). We found a high tion is increasingly common and requires further We classified journals as having either a
research to determine the effectiveness. specialty or general medical focus by consensus
and noted the most recent H-index and im-
Dr Bhatia was a fourth-year medical student
Background pact factors available. We collected information
in the Vancouver Fraser Medical Program
Social media activity has been associated with on social media engagement across four social
at the University of British Columbia when
increased visibility of published articles, in- media platforms: Twitter, Facebook, Instagram,
he submitted this article for publication
cluding downloads and citations.1,2 As a result and YouTube. To optimize fast and accurate
consideration. He graduated from UBC
of the perceived benefits to and engagement data collection, we developed a program to
Medicine in May 2021. He is also a co-
with readers, medical journals are increasingly web-scrape data using Selenium Webdriver
founder of the UBC medical student podcast
using social media such as Twitter, Facebook, 3.141.0 on Python. All data from Instagram
MEDamorphosis (https://medamorphosis-
Instagram, and YouTube to share content. Many and Facebook were gathered on 16 February
podcast.simplecast.com). Mr Mojtabavi is a
physicians are also engaging with journals in 2020, while all Twitter and YouTube data were
recent graduate with an integrated science
this context and increasingly using social me- gathered on 2 March 2020. For each account,
degree in physiology, psychology, and
dia as an avenue for CME.3,4 Despite an in- when available, we noted followers, likes, and
pharmacology from the University of British
crease in activity over the past decade, little is number of posts.
Columbia and is a co-founder and director of
known about the frequency of social media Data were described using percentage and
the not-for-profit Campus Nutrition (https://
use by medical journals, including engagement median (interquartile range [IQR]). Normal
campusnutrition.ca). Mr Ahmed is a recent
with specific social media platforms, number of distribution of continuous variables was de-
graduate with an integrated science degree
followers, and the relationship between these termined using the Shapiro-Wilk test for nor-
in pathophysiology and kinesiology from the
activities and objective measures of journal im- mality. Specialty and general medical journals
University of British Columbia. Dr Varshney
pact such as the H-index. The journal H-index were compared using a Wilcoxon rank sum and
(@VarshneyMD) is a staff anesthesiologist
is defined as the number of articles (H) that Fisher’s exact test for continuous and categorical
and pain medicine physician at St. Paul’s
have received at least H citations and, there- data, respectively. Multivariable linear regression
Hospital and Providence Health Care, and a
fore, combines an assessment of both quantity was used to explore the relationship between
clinical instructor at the University of British
(number of papers) and quality (impact). H-index and the social media activity. P values
Columbia. Dr Flexman (@alanaflex) is a staff
Our primary study objective was to describe less than .05 were considered significant. Statis-
anesthesiologist and research director at St.
the use of various social media platforms by tical analysis was completed in R version 3.6.3
Paul’s Hospital and Providence Health Care, a
high-impact medical journals. Our second- and STATA 12.1 (StataCorp, Texas, USA).
clinical associate professor at the University
ary objectives were to analyze the relationship
of British Columbia, and an associate editor
between social media engagement and journal Results
at the Canadian Journal of Anesthesia.
type (specialty versus general), the impact factor, We identified the top 100 journals by H-index
and the H-index. and excluded 12 journals that were found to not
This article has been peer reviewed.
204 BC Medical Journal vol. 63 no. 5 | june 20210.2
0.0
Twitter Instagram Facebook
BCMD2B
YouTube
Social media platforms
be primarily medical after further review, leav-
ing 88 journals for the analysis. Missing data Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
were minimal and included only the YouTube 1.0 1.0
channel subscribers and views from three jour- 0.8 0.8
nals. We classified 84% (n = 74) of journals as
Frequency
Frequency
0.6 0.6
specialty and 16% (n = 14) as general. Charac-
teristics of included medical journals are sum- 0.4 0.4
marized in Table 1. Included journals (n = 88) 0.2 0.2
had a median H-index of 278 (IQR 245, 332) 0.0 0.0
and a median journal impact factor of 9.6 (IQR Twitter Instagram Facebook YouTube Twitter Instagram Facebook YouTube
6.1, 19.1). All journals had associated Twitter Social media platforms Social media platforms
accounts, while 94.3%, 64.8%, and 62.5%, of
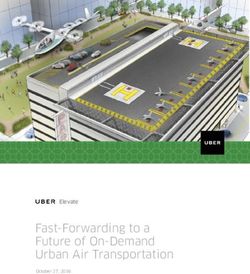
Figure 1. Frequency of social media platforms used Figure 2: Frequency of social media platforms used
journals had associated YouTube, Facebook,
by medical journals, stratified by H-index quartiles. by medical journals, stratified by impact factor quartiles.
and Instagram accounts, respectively. Follow- Q1 Q2 Q3 Q4
ers were the highest on Facebook, followed 1.0
by Twitter, Instagram, and YouTube. General Table0.81: Characteristics of included medical journals.
Frequency
medical journals had higher H-indices and
0.6
impact factors than specialty journals. Both Overall Specialty General
0.4
P value
types of journals used social media platforms (N = 88) (N = 74) (N = 14)
at similar frequency, although general medical 0.2
H-index 278 (245, 332) 270 (238, 326) 353 (289, 497) 0.0016
journals had more Twitter and Facebook fol- 0.0
Impact factor 9.6 (6.1, 19.1)YouTube 9.0 (6.1, 16.6) 22.5 (7.8, 51.3) 0.0277
lowers, and specialty journals had more Insta- Twitter Instagram Facebook
gram followers. Figure 1 and Figure 2 display Twitter (N, %) Social media platforms
88 (100) 74 (100) 14 (100) —
a general increase in the frequency of available Twitter followers 10 776 (3529, 29 689) 9006 (3212, 25 898) 82 956 (12 486, 331 681) 0.0054
social media accounts for medical journals from
Total tweets 3900 (2023, 7819) 3650 (1744, 7198) 12 134 (3531, 20 624) 0.0188
the lowest to highest H-index and impact fac-
tor quartile. From left to right, the bars under YouTube (N, %) 83 (94.3) 69 (93.2) 14 (100) 0.411
each category in Figure 1 signify quartile 1 to
YouTube subscribers 3705 (549, 12 000) 2950 (527, 11 600) 6845 (1960, 20 500) 0.1506
4: Q1 (< 244.5), Q2 (244.5 < < 278), Q3 (278
< < 332), Q4 (> 332), while those in Figure 2 YouTube videos 265 (77, 527) 265 (74, 527) 316 (88, 516) 0.8593
signify quartile 1 to 4: Q1 (< 6.08), Q2 (6.08 Facebook (N, %) 57 (64.8) 46 (62.2) 11 (78.6) 0.193
< < 9.5765), Q3 (9.5765 < < 19.1305), Q4 (>
Facebook followers 27 858 (8359, 99 880) 24 260 (4480, 74 045) 99 880 (46 489, 498 408) 0.0223
19.1305). Presence of an Instagram account
predicted H-index (coefficient 56.8, 95% CI 9.5 Facebook likes 26 853 (8012, 98 452) 23 500 (4402, 71 431) 98 452 (45 753, 492 594) 0.0223
to 104.1, P = 0.019) but not Facebook (coef- Instagram (N, %) 55 (62.5) 44 (59.5) 11 (78.6) 0.146
ficient 39.9, 95% CI -8.89 to 88.6, P = 0.108)
or YouTube (coefficient 60.1, 95% CI -41.2 to Instagram followers 5893 (1695, 87 979) 8483 (2478, 87 980) 2021 (162, 13 796) 0.0626
161.5, P = 0.241). When controlling for journal Instagram posts 276 (110, 771) 343 (158, 753) 114 (18, 925) 0.1779
type, the presence of social media accounts did All values are median (interquartile range) unless otherwise indicated.
not predict H-index [Table 2]. Since all journals
had associated Twitter accounts, the presence
of this account was not included in the model.
Table 2. Linear regression model to predict journal H-index.
Discussion
Coefficient 95% CI P value
Our analysis provides a contemporary snap-
shot and formal analysis of social media use Facebook 20.9 -24.0 to 65.7 0.358
by high-impact medical journals in 2020. We Instagram 36.6 -7.8 to 81.0 0.105
found that all journals included in our study
YouTube 33.3 -57.7 to 124.2 0.469
used some form of social media, with univer-
sal use of Twitter and frequent use of You- General (vs specialty) 127.6 69.8 to 185.4 < 0.001
Tube. Facebook and Instagram were used by R2 = 0.2613 p < 0.001
BC Medical Journal vol. 63 no. 5 | June 2021 205BCMD2B
a majority of journals but less frequently than social media platforms may drive traffic toward media coverage of scientific articles immediately after
other platforms. General medical journals had CME initiatives,14 and that social media cov- publication predicts subsequent citations - #SoME_Im-
pact Score: Observational analysis. J Med Internet Res
higher H-indices, impact factors, followers, and erage predicts citations of articles,2,15 although 2020;22:e12288-e12288.
higher engagement with social media compared greater social media attention may simply reflect 3. Wray CM, Auerbach AD, Arora VM. The adoption of an
to specialty journals. Of the four platforms an- higher-quality articles that are more likely to be online journal club to improve research dissemination
alyzed, journals had the greatest number of cited. Two randomized trials have found that and social media engagement among hospitalists. J
Hosp Med 2018;13:764-769.
interactions on Facebook (such as followers tweeting articles increased Altmetric scores 4. Ghanem O, Logghe HJ, Tran BV, et al. Closed Facebook™
and likes). Our data offer a unique perspec- and citations over time compared to those that groups and CME credit: A new format for continuing
tive that quantifies the use of social media by were not shared on Twitter.16,17 In contrast, an- medical education. Surg Endosc 2019;33:587-591.
high-impact medical journals, and describes a other randomized study did not find that social 5. El Bialy S, Jalali A. Go where the students are: A com-
parison of the use of social networking sites between
high level of engagement, particularly by general media exposure increased article citations or
medical students and medical educators. JMIR Med
medical journals. downloads.18 A recent systematic review found Educ 2015;1:e7.
The use of social media in medical publish- “suggestive yet inconclusive” evidence that the 6. Guraya SY. The usage of social networking sites by med-
ing to disseminate research and information use of social media increases article citations, ical students for educational purposes: A meta-analysis
and systematic review. N Am J Med Sci 2016;8:268-278.
has evolved relatively rapidly over the last de- with notable limitations and inconsistent find-
7. Lopez M, Chan TM, Thoma B, et al. The social media
cade. Social media itself has been introduced ings in the literature.1 editor at medical journals: Responsibilities, goals, bar-
relatively recently (Facebook was founded in Our analysis has several limitations. Al- riers, and facilitators. Acad Med 2019;94:701-707.
2004, YouTube in 2005, Twitter in 2006, and though we described the use of social media and 8. Siau K, Lui R, Mahmood S. The role of a social media
editor: What to expect and tips for success. United Eu-
Instagram in 2010). The adoption of social me- the relationship with journal impact (H-index),
ropean Gastroenterol J 2020;8:1253-1257.
dia is uneven, and its use varies among different we cannot establish a causative effect of social 9. Oska S, Lerma E, Topf J. A picture is worth a thousand
generations of medical professionals.5 Uptake media engagement on the journal’s performance views: A triple crossover trial of visual abstracts to ex-
is high among medical students; as many as or research. Furthermore, our results represent amine their impact on research dissemination. J Med
90% of medical students are active on social a snapshot in time that will continue to evolve, Internet Res 2020;22:e22327.
10. Thamman R, Gulati M, Narang A, et al. Twitter-based
networking sites.6 Many journals now formal- and further research to establish trends over learning for continuing medical education? Eur Heart
ly appoint a social media editor, a role which time would be valuable. Finally, we included J 2020;41:4376-4379.
encompasses a range of responsibilities from only the top 100 medical journals by H-index; 11. Topf JM, Sparks MA, Phelan PJ, et al. The evolution of
disseminating new publications via social me- the use of social media by lower-impact jour- the journal club: From Osler to Twitter. Am J Kidney
Dis 2017;69:827-836.
dia, summarizing articles, and managing social nals may vary. 12. Tunnecliff J, Weiner J, Gaida JE, et al. Translating evi-
media accounts.7,8 Sharing visual abstracts (vi- Our study findings clarify the current state dence to practice in the health professions: A random-
sual summaries of an article’s content) on social of social media use by high-impact medical ized trial of Twitter vs Facebook. J Am Med Inform Assoc
media is increasing and may improve an article’s journals and indicate these journals are highly 2017;24:403-408.
13. Chan WS, Leung AY. Facebook as a novel tool for
visibility and engagement compared to sharing engaged with these platforms. General medi-
continuous professional education on dementia: Pi-
citations only.9 Twitter is increasingly embraced cal journals have a greater impact and reach on lot randomized controlled trial. J Med Internet Res
as a CME tool, encompassing activities such social media compared to specialty journals, as 2020;22:e16772.
as online journal clubs and virtual networking. measured by followers and subscribers. The use 14. Flynn S, Hebert P, Korenstein D, et al. Leveraging social
media to promote evidence-based continuing medi-
These formats offer several advantages such as of social media to facilitate medical education
cal education. PLoS One 2017;12:e0168962.
lower cost, accessibility, and innovative methods and knowledge dissemination is increasingly 15. Chau M, Ramedani S, King T, Aziz F. Presence of social
of engagement.3,10,11 An open label randomized common and future research should address media mentions for vascular surgery publications is
trial found that CME practice tips provided questions about whether social media can in- associated with an increased number of literature ci-
tations. J Vasc Surg 2021;731096-1103.
by Twitter and Facebook can improve clinical crease article citation, improve CME, and ef-
16. Luc JGY, Archer MA, Arora RC, et al. Does tweeting
knowledge and promote behavior change,12 and ficiently disseminate knowledge. n improve citations? One-year results from the TSS-
another study found Facebook more effective MN prospective randomized trial. Ann Thorac Surg
than email at delivering medical education.13 Competing interests 2021;111:296-300.
Our study results suggest that the majority of Dr Flexman is an associate editor of the Canadian 17. Ladeiras-Lopes R, Clarke S, Vidal-Perez R, et al. Twitter
promotion predicts citation rates of cardiovascular
medical journals perceive these benefits and Journal of Anesthesia and the Journal of Neurosurgi- articles: A preliminary analysis from the ESC Journals
have now embraced these platforms. cal Anesthesiology. Randomized Study. Eur Heart J 2020;41:3222-3225.
Social media may offer several benefits to 18. Tonia T, Van Oyen H, Berger A, et al. If I tweet will
journals in promoting knowledge dissemina- References you cite? The effect of social media exposure of ar-
ticles on downloads and citations. Int J Public Health
tion and article engagement, although the evi- 1. Bardus M, El Rassi R, Chahrour M, et al. The use of so-
2016;61:513-520.
cial media to increase the impact of health research:
dence supporting an effect on citation is mixed.
Systematic review. J Med Internet Res 2020;22:e15607.
There is some evidence to suggest that use of 2. Sathianathen NJ, Lane III R, Murphy DG, et al. Social
206 BC Medical Journal vol. 63 no. 5 | june 2021You can also read