Effective Clinical Care for Patients With Comorbidities - Melinda Campopiano von Klimo, MD Senior Medical Adviser - RCORP ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Effective Clinical Care for
Patients With
Comorbidities
Melinda Campopiano von Klimo, MD
Senior Medical Adviser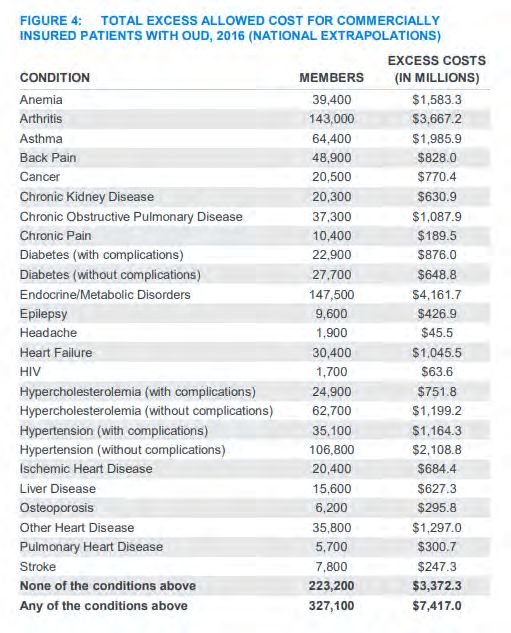
Submitting Questions and Comments
• Submit questions by using the Q&A feature. To open your Q&A window, click
the Q&A icon on the bottom center of your Zoom window.
• If you experience any technical issues during the webinar, please message
us through the chat feature or email RCORP-TA@jbsinternational.com.
2
Learning Objectives
• Be familiar with the evidence supporting the use of
integrated behavioral health care to improve patient
outcomes and reduce disparities.
• Understand the principles of integrated behavioral health
and be up to date on recent outcomes and implementation
research.
• Describe steps to implement integrated behavioral health
care.
3
The Current
Context for
Integration of
Behavioral
Health
4
COVID-19 and Mental Health
• CDC Household Pulse Survey
o Asks about anxiety and depression symptoms in the last 7 days
o Uses 2-item Patient Health Questionnaire (PHQ-2) and Generalized
Anxiety Disorder Scale (GAD-2)
• During the pandemic
o The proportion of Americans reporting symptoms of anxiety or
depression quadrupled.
o Women, young people, racial and ethnic minorities, and people with
disabilities bear a greater burden.
Mental Health - Household Pulse Survey - COVID-19 (cdc.gov) 5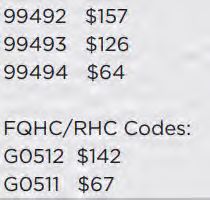
COVID-19 and Mental Health
• Symptoms of depression or anxiety, April 2021
• National 32.1%
• Men 27.9% Women 36.3%
• Age 19-29 51.7% All other ages 25.6%
• Disability 64.3% No Disability 27.4%
6COVID-19 and Mental Health
• Symptoms of anxiety or depression, April 2021
• Non-Hispanic other races or multiple races 41.7%
• Hispanic/Latino 38.6%
• Non-Hispanic Black 35%
• Non-Hispanic White 30.3%
• Non-Hispanic Asian 25.5%
7COVID-19 and Mental Health by State
• April 2021
• Symptoms of
anxiety or
depression
• Wyoming
22%
• West Virginia
42.1%
Mental Health - Household Pulse Survey - COVID-19 (cdc.gov) 8Opioid Use
Disorder and
Comorbidity
• Study of a
population with
commercial
insurance
• 60% of people
with OUD had at
least one
chronic medical
condition.
Costs and Comorbidities of
Opioid Use Disorder
(azureedge.net) 9Comorbid Conditions Common in OUD • HIV and hepatitis C virus (HCV) infection are common in patients with opioid use disorder (OUD). • Successful treatments for HIV and HCV can be provided to patients with OUD, regardless of ongoing substance use. • Complications of injection drug use, such as HIV, HCV, skin and soft tissue infections, and infective endocarditis, could be prevented with harm reduction practices (e.g., sterile syringe services and supervised injection facilities). • Rare, life-threatening bacterial infections may present with signs and symptoms that mimic intoxication, such as malaise or stupor, and should be thoroughly assessed in patients with fever or positive blood cultures. • Chronic opioid exposure can lead to hypogonadism, opioid-induced hyperalgesia, sleep-disordered breathing, and increased risk of cardiovascular disease and neurocognitive impairment. • Medications for OUD—buprenorphine, methadone, and naltrexone—are safe and effective, and awareness of adverse opioid effects can improve clinical practice. Caring for Patients With Opioid Use Disorder: What Clinicians Should Know About Comorbid Medical Conditions | Psychiatric Research and Clinical Practice (psychiatryonline.org) 10
Mental Health and Medical
Comorbidity: Cancer
• One third of people with cancer meet diagnostic criteria for a
psychiatric disorder.
• Prevalence is higher among people with advanced cancer.
• Comorbid mental disorders reduce quality of life and interfere
with treatment adherence.
• Depression may affect rate of cancer progression.
• People with cancer who have pre-existing depression have
higher all-cause mortality.
An integrative collaborative care model for people with mental illness and physical comorbidities |
International Journal of Mental Health Systems | Full Text (biomedcentral.com) 11Mental Health and Medical Comorbidity:
Cardiopulmonary Disease
• People who have suffered a heart attack are 3 times more
likely to be depressed compared to the general population.
• 20 to 45% of people with heart disease experience
depression.
• People with COPD are at increased risk of depressed mood
and anxiety compared to the general population.
An integrative collaborative care model for people with mental illness and physical comorbidities |
International Journal of Mental Health Systems | Full Text (biomedcentral.com) 12Mental Health and Medical
Comorbidity: Diabetes
• Depression is associated with a 60% increase in diabetes.
• Diabetes is associated with a 15% increase in depression.
• People with diabetes who report severe symptoms of
depression can be less compliant with treatment and are at
higher risk of coronary heart disease.
An integrative collaborative care model for people with mental illness and physical comorbidities |
International Journal of Mental Health Systems | Full Text (biomedcentral.com) 13Mental Health and Medical
Comorbidity: Arthritis
• People with depression have a 34% higher prevalence of
arthritis than people without depression.
An integrative collaborative care model for people with mental illness and physical comorbidities |
International Journal of Mental Health Systems | Full Text (biomedcentral.com) 14Integrated
Behavioral
Health Care
15Principles of Integrated Care
• Patient-centered team care
• Population-based care
• Measurement-based treatment to target
• Evidence-based care
• Accountable care
AIMS Center | Advancing Integrated Mental Health Solutions in Integrated Care (uw.edu)
16The
Collaborative
Care Model
Vs.
Integrated
Behavioral
Health Care
Watch the 7-minute patient video here:
Daniel's Story: An introduction to Collaborative Care | University of Washington AIMS Center (uw.edu)
17Principles of Integrated Care—
Patient-Centered Care Team
• Primary care and
behavioral health
providers
• collaborate
effectively
• using shared care
plans that
• incorporate patient
goals.
18Principles of Integrated Care—
How Is It Patient-Centered?
• Care incorporates patient goals.
• Patient receives care for both physical and mental health at
a familiar location that is comfortable to patients.
• Reduces burden of duplicate assessments.
• Increases patient engagement:
o better health care experience
o improved patient outcomes
19Principles of Integrated Care—
Population-Based Care
• Population: a defined group of patients cared for by
team
• Tracked in a registry to ensure no one falls
through the cracks.
• Practices reach out to patients who are not
improving.
• Mental health specialists provide caseload-focused
consultation, not just ad-hoc advice.
20Using a Patient Registry
• Track clinical outcomes and progress
o both the individual patient level and overall caseload level for the
target population
• Deliver prompt treatment-to-target
o summarizing patient’s improvement and challenges
o easily understandable and actionable way
• Facilitate efficient psychiatric consultation and case review
o prioritize patients who need to be evaluated for changes in
treatment or are new to the caseload
21Principles of Integrated Care—
Measurement-Based Treatment to Target
• Each patient’s treatment plan clearly articulates
personal goals and clinical outcomes.
• Goals and outcomes are routinely measured by
evidence-based tools.
• Treatments are actively changed if patients are not
improving as expected until the clinical goals are
achieved. (Sometimes called Stepped Care.)
22Treating to Target
• Collaborative care requires a
change in the treatment plan
every 10-12 weeks if the Example:
patient has not had at least a
50% improvement in symptoms If the treatment plan started
using a validated measure. with medication therapy as
the primary treatment, the
• This prevents the clinical inertia adjustment might be a
that often occurs in usual care change in dosage or the
and is likely one of the key
factors behind the better addition of evidence-based
treatment outcomes that can be psychotherapy.
achieved with collaborative
care.
23Tools for Treating to Target
Mental Health Well-Being and Function
• Patient Health Questionnaire-2. • Health Assessment Questionnaire-
Two items (low mood and loss of Disability Index (original)
interest) (ahrq.gov) (ahrq.gov)
• Patient Health Questionnaire • RAND 36 Item Short Form Health
(PHQ-9) (ahrq.gov) Survey SF-36 (ahrq.gov)
• Generalized Anxiety Disorder • Multidimensional Health
scale, GAD-2; 2 items (ahrq.gov) Assessment Questionnaire
• Generalized Anxiety Disorder (MDHAQ) (ahrq.gov)
scale, GAD-7; 7 items (ahrq.gov) • WHO Quality of Life Brief
• Geriatric Depression Scale-15 Instrument
(short version) (ahrq.gov)
24Principles of Integrated Care—
Evidence-Based Care
Evidence for the model Evidence-based treatments
• Collaborative care itself • Patients are offered
has a treatments with credible
substantial evidence research evidence to support
their efficacy in treating the
base for its target condition.
effectiveness.
• These include a variety of
• One of the few evidence-based
integrated care models psychotherapies proven to
that does. work in primary care.
25Behavioral Health Interventions
Effective in Primary Care
• Include a patient engagement component
• Be time efficient, running no more than 20-30 minutes a visit
• Follow a structured but patient-centered approach
• Minimize required clinical training and duration of treatment
• Be relevant and applicable to diverse patient populations
• Have a substantial research evidence base
26Behavioral Health Interventions
Effective in Primary Care
• Problem Solving Treatment-Primary Care (PST-PC)
Brief therapy that uses six to ten 30-minute sessions to help patients solve
the "here and now" problems contributing to their depression.
• Behavioral Activation (BA)
Psychotherapy that identifies work, social, health, or family activities
patients have stopped engaging in because of their mood.
• Cognitive Behavioral Therapy (CBT)
Short-term, goal-oriented therapy to interrupt patterns of thinking that
prevent patients from feeling better.
• Interpersonal Counseling (IPC)
Outgrowth of interpersonal therapy that focuses on current functioning,
recent life changes, sources of stress, and difficulties in interpersonal
relationships.
27Principles of Integrated Care–
Accountable Care
• Providers are accountable.
• Providers are reimbursed for
oquality of care and
oclinical outcomes,
onot just the volume of care.
28Recommendations for Use of Billing
Codes
• Allow paraprofessionals with formal education (BA level or
higher) or specialized training to serve as care managers.
• Keep options for diagnosis open and not limited to specific
conditions.
• Waive cost sharing (co-pays) when possible.
• Prior authorization should not be required.
• Allow specialists (i.e., cardiologists) to bill the codes if they
have established a Collaborative Care program.
APA-Best-Practice-for-Reimbursing-CoCM-in-Medicaid.pdf 29Billing Codes and Reimbursement 8-fold increase in use of these codes in 2017-2018, but use among eligible beneficiaries remains low. Provision of Collaborative Care Model and General Behavioral Health Integration Services in Medicare | 30 Psychiatric Services (psychiatryonline.org)
Evidence Base
for Integrated
Care
31Evidence of Effectiveness of
Integrated Care—Medical Illness
• Collaborative Care is effective for people with depression and chronic medical illnesses.
(Panagoti, 2016)
• Treatment with Collaborative Care is associated with significantly greater improvements
in depression, and diabetes and cardiovascular disease measures, along with better
quality of life and satisfaction with care. (Kanton, 2010)
• Collaborative Care was associated with significantly better depression outcomes, with
over 60% of people in the Collaborative Care arm showing improvement, compared to
17% in usual care. Patients in Collaborative Care also reported less fatigue, pain,
anxiety, and better quality of life. (Sharpe, 2014)
• Evidence-based programs for depression treatment and weight-loss treatment delivered
in primary care for adult patients with depression and obesity produces significant
reduction in Body Mass Index (BMI) and depression symptoms in those receiving
Collaborative Care, compared to no change in either BMI or depression symptoms over
12 months for those receiving usual care. (Ma, 2019)
• Treatment with Collaborative Care doubled the proportion of patients with depression
response and remission at 6 months in patients with HIV. (Pyne, 2011)
32Evidence of Effectiveness for Integrated
Care—Racial and Ethnic Minority
• Collaborative Care should be explored as an intervention for
treating depression for racial/ethnic minority patients in primary
care. (Hu, 2020)
• Effectiveness of depression treatment doubled at 12 months for
older minority patients (i.e., Black, Hispanic, “other”). (Arean,
2005)
• Racial minority patients benefited more than White patients when
both received Collaborative Care. (Cooper, 2013)
• Treatment outcomes were similar in all groups, though the Native
American/Alaska Native group had slightly higher proportion of
individuals with depression remission and significantly higher
proportion of individuals with depression response but had
slightly lower severity of baseline depression. (Bowen, 2020)
33Evidence of Effectiveness of
Integrated Care—Rural
• Eight rural clinics implemented Collaborative Care,
demonstrating that approximately 15% of the total clinic
populations were treated with Collaborative Care and that
patients receiving Collaborative Care experienced clinically
significant improvements in depression and reduction in
suicidal ideation. (Powers, 2020)
• Patients treated in the off-site Collaborative Care arm were
significantly (2-2.5 times) more likely to have depression
response or remission at 6, 12, and 18 months, compared to
the on-site arm. (Fortney, 2013)
34Evidence of effectiveness for
Integrated Care—Telemedicine
• Collaborative Care is effective when adapted to primary care
clinics without on-site psychiatrists using telemedicine.
(Fortney, 2007)
• Remotely delivered Collaborative Care provided greater
reduction in symptoms of PTSD at 6 and 12 months after
injury when delivered remotely (Fortney, 2015)
35Evidence of effectiveness for
Integrated Care—Mental Health
• Significant improvement in short-term depression and anxiety outcomes in adults
(Archer, 2012)
• Significantly more effective than usual care and improved depression outcomes at
6 months to 5 years (Gilbody, 2006)
• Doubled effectiveness of depression treatment in older adults (Unützer, 2002)
• Lower symptom severity and decreased risk of major depressive disorder in older
adults at 12 months (Gilbody, 2017)
• Doubled effectiveness of treatment for depression among adolescents.
(Richardson, 2014)
• Better outcomes for patients with anxiety in primary care (Roy-Byrne, 2010)
• Collaborative Care post-hospital discharge improved mental health outcomes,
including PTSD symptom severity and rates of alcohol use disorder. (Zatzick,
2004)
36References
Archer J, Bower P, Gilbody S, et al. Collaborative care for depression and anxiety problems. Cochrane Database of Systematic Reviews 2012, Issue 10.
Art. No.: CD006525. DOI: 10.1002/14651858.CD006525.pub2
Gilbody S, Bower P, Fletcher J, Richards D, Sutton AJ. Collaborative care for depression: a cumulative meta-analysis and review of longer-term outcomes.
Arch Intern Med. 2006;166(21):2314-21.
Unützer J, Katon W, Callahan CM, Williams JW, Jr., Hunkeler E, Harpole L, et al. Collaborative-care management of late-life depression in the primary care
setting. JAMA. 2002;288(22):2836-45.
Roy-Byrne P, Craske MG, Sullivan G, Rose RD, Edlund MJ, Lang AJ, et al. Delivery of Evidence-Based Treatment for Multiple Anxiety Disorders in Primary
Care: A Randomized Controlled Trial. JAMA. 2010;303(19):1921-8.
Zatzick DF, Roy-Byrne P, Russo J, et al. A randomized effectiveness trial of stepped collaborative care for acutely injured trauma survivors. Arch Gen
Psychiatry. 2004;61:498-506.
Gilbody S, Lewis H, Adamson J, et al. Effect of collaborative care vs usual care on depressive symptoms in older adults with subthreshold depression: The
CASPER Randomized clinical trial. JAMA. 2017;317:728737
Richardson LP, Ludman E, McCauley E, et al. Collaborative care for adolescents with depression in primary care: a randomized clinical trial. JAMA.
2014;312:809-816.
Fortney JC, Pyne JM, Edlund MJ, et al. A randomized trial of telemedicine-based collaborative care for depression. J Gen Intern Med. 2007;22:1086-1093.
Fortney JC, Pyne JM, Kimbrell TA, et al. Telemedicine-based collaborative care for posttraumatic stress disorder: a randomized controlled trial. JAMA
Psychiatry. 2015;72:58-67.
Hu J, Wu T, Damodaran S, Tabb KM, Bauer A, Huang H. The effectiveness of collaborative care on depression outcomes for racial/ethnic minority
populations in primary care: a systematic review. Psychosomatics. 2020, online first.
Arean P, Ayalon L, Hunkeler E. Improving depression care for older, minority patients in primary care. Med Care. 2005;43:381-390.
Davis T, Deen T, Bryant-Bedell K, Tate V, Fortney J. Does minority racial-ethnic status moderate outcomes of collaborative care for depression? Psychiatr
Serv. 2011;62:1282-1288.
37References, continued
• Cooper LA, Dinoso BK, Ford DE, et al. Comparative effectiveness of standard versus patient-centered collaborative care
interventions for depression among African Americans in primary care settings: the BRIDGE study. Health Serv Res. 2013;48:150-
174.
• Bowen D, Powers DM, Russo J, et al. Implementing collaborative care to reduce depression for rural native American/Alaska
native people. BMC Health Services Research. 2020;20:34 doi.org/10.1186/s12913-019-4875-6
• Panagioti M, Bower P, Kontopantelis E, et al. Association between chronic physical conditions and the effectiveness of
collaborative care for depression: an individual participant data meta-analysis. JAMA Psychiatry. 2016;73:978-989.
• Katon W, Lin EHB, Von Korff M, et al. Collaborative care for patients with depression and chronic illnesses. N Engl J Med.
2010;27:2611-2620.
• Sharpe M, Walker J, Hansen CH, et al. Integrated collaborative care for comorbid major depression in patients with cancer
(SMaRT Oncology-2): a multicentre randomised controlled effectiveness trial. Lancet. 2014;384:1099-1108.
• Ma, J, Goldman Rosas L, Lv N, et al. Effect of integrated behavioral weight loss treatment and problemsolving therapy on body
mass index and depressive symptoms among patients with obesity and depression: the RAINBOW randomized clinical trial.
JAMA. 2019;321:869-879.
• Pyne JM, Fortney JC, Curran GM, et al. Effectiveness of collaborative care for depression in human immunodeficiency virus (HIV)
clinics. Arch Intern Med. 2011;171:23-31.
• Powers DM, Bowen DJ, Arao RF, et al. Rural clinics implementing collaborative care for low-income patients can achieve
comparable or better depression outcomes. Fam Syst Health. 2020;38:242-254.
• Fortney JC, Pyne JM, Mouden SB, et al. Practice-based versus telemedicine-based collaborative care for depression in rural
Federally Qualified Health Centers: a pragmatic randomized comparative effectiveness trial. Am J Psychiatry. 2013;170:414-425.
38New Directions
and Current
Challenges
39Post-Concussive Symptoms in
Adolescents
• Cognitive behavioral therapy delivered remotely
• Adolescents followed for 1 year
• Randomized to 2 groups
o Usual care vs. Collaborative Care Model
• Both groups improved:
o Collaborative Care group had significantly better Health Behavior
Inventory Scores at 3 months.
o Collaborative Care group reported fewer symptoms and better
quality of life over the year.
Effect of Collaborative Care on Persistent Postconcussive Symptoms in Adolescents: A
Randomized Clinical Trial | Adolescent Medicine | JAMA Network Open | JAMA Network
40Variation in Effectiveness in
Depression Outcomes
• Average treatment response was lower compared to
randomized-controlled trials.
• Patient variables
o Severity of symptoms
• Practice variables
o Years of experience in collaborative care
o Level of implementation support for collaborative care
Variation In The Effectiveness Of Collaborative
Care For Depression: Does It Matter Where You
Get Your Care? | Health Affairs 41Implementation Lessons Learned in
Small Primary Care Practices
• Greater success associated with:
o On-site behavioral health integration service
o Champions for behavioral health integration
o Early and sustained training
o Involvement of both providers and administrators
o Use of collaborative agreements with external behavioral health
providers
o Successful reimbursement for behavioral health integration
• Challenges:
o Health information technologies across sites
o Financing and policy factors
Implementation of Behavioral Health Integration in Small Primary Care Settings:
Lessons Learned and Future Directions | SpringerLink 42Rural Collaborative Care Models Support
Training and Workforce Development
• Initial training was required to implement program.
• Consulting tele-psychiatrist continued to provide just-in-time
information, coaching, and support.
• Staff accumulated experience and knowledge of screening,
assessment, and treatment as they used the model with patients
and applied the skills to other patients.
• Staff described enhanced patient interactions and improved
competency.
• Perceived benefit in fidelity to care model, team resilience
despite turn-over, and enhanced capacity to use quality
improvement.
Telepsychiatric Consultation as a Training and Workforce Development Strategy for
Rural Primary Care | Annals of Family Medicine (annfammed.org) 43Getting started
• AIMS Center | Advancing Integrated Mental Health
Solutions in Integrated Care (uw.edu)
• Learn About the Collaborative Care Model (psychiatry.org)
• Welcome to the AHRQ Academy | The Academy
Integrating Behavioral Health and Primary Care
• Center of Excellence for Integrated Health Solutions
(thenationalcouncil.org)
• IBHP | Accelerating the integration of behavioral and
primary care throughout California. (ibhpartners.org)
• Behavioral Health Integration Compendium (ama-assn.org)
44Submitting Questions and Comments
Submit questions by using the Q&A feature.
To open your Q&A window, click on the
Q&A icon on the bottom center of your
Zoom window.
45Thank you
The purpose of RCORP is to support treatment for and prevention of
substance use disorder, including opioid use disorder, in rural counties at the
highest risk for substance use disorder.
mcampopiano@jbsinternational.comYou can also read