Effect of Calcification Based on Computer-Aided System on CT- Fractional Flow Reserve in Diagnosis of Coronary Artery Lesion
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hindawi
Computational and Mathematical Methods in Medicine
Volume 2022, Article ID 7020209, 10 pages
https://doi.org/10.1155/2022/7020209
Research Article
Effect of Calcification Based on Computer-Aided System on CT-
Fractional Flow Reserve in Diagnosis of Coronary Artery Lesion
Dongliang Fu ,1 Xiang Xiao,1 Tong Gao ,2 Lina Feng ,1 Chunliang Wang ,3
Peng Yang ,1 and Xianlun Li 1
1
Department of Cardiology, Integrated Traditional Chinese and Western Medicine, China-Japan Friendship Hospital, No. 2 East
Yinghua Road, Chaoyang District, Beijing 100029, China
2
Graduate School, Peking Union Medical College, Beijing 100730, China
3
Beijing Escope Tech Co., Ltd., Beijing, China
Correspondence should be addressed to Xianlun Li; 1811210693@bjmu.edu.cn
Received 19 September 2021; Revised 10 December 2021; Accepted 21 December 2021; Published 17 January 2022
Academic Editor: Osamah Ibrahim Khalaf
Copyright © 2022 Dongliang Fu et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This study was to analyze the diagnostic value of coronary computed tomography angiography (CCTA) and fractional flow
reserve (FFR) based on computer-aided diagnosis (CAD) system for coronary lesions and the possible impact of calcification.
80 patients who underwent CCTA and FFR examination in hospital were selected as the subjects. The FFR value of 0.8 was
used as the dividing line and divided into the ischemic group (FFR ≤ 0:8) and nonischemic group (FFR > 0:8). The basic data
and imaging characteristics of patients were analyzed. The maximum diameter stenosis rate (MDS %), maximum area stenosis
rate (MAS %), and napkin ring sign (NRS) in the ischemic group were significantly lower than those in the nonischemic group
(P < 0:05). Remodeling index (RI) and eccentric index (EI) compared with the nonischemic group had no significant difference
(P > 0:05). The total plaque volume (TPV), total plaque burden (TPB), calcified plaque volume (CPV), lipid plaque volume
(LPV), and lipid plaque burden (LPB) in the ischemic group were significantly different from those in the non-ischemic group
(P < 0:05). MAS % had the largest area under curve (AUC) for the diagnosis of coronary myocardial ischemia (0.74), followed
by MDS % (0.69) and LPV (0.68). CT-FFR had high diagnostic sensitivity, specificity, accuracy, truncation value, and AUC
area data for patients in the ischemic group and nonischemic group. The diagnostic sensitivity, specificity, accuracy, cutoff
value, and AUC area data of CT-FFR were higher in the ischemic group (89.93%, 92.07%, 95.84%, 60.51%, 0.932) and
nonischemic group (93.75%, 90.88%, 96.24%, 58.22%, 0.944), but there were no significant differences between the two groups
(P > 0:05). In summary, CT-FFR based on CAD system has high accuracy in evaluating myocardial ischemia caused by
coronary artery stenosis, and within a certain range of calcification scores, calcification does not affect the diagnostic accuracy
of CT-FFR.
1. Introduction stenosis or obstruction of the vascular cavity, myocardial
ischemia, hypoxia, or necrosis [3]. It has been proposed that
Cardiovascular disease, also known as circulatory system the pathophysiological basis of acute coronary syndrome is
disease, is a series of diseases involving the circulatory sys- the rupture of “vulnerable” single criminal plaque, which
tem. It has become the primary noncommunicable disease promotes the formation of acute thrombosis in situ and
threatening global public health. The World Health Organi- leads to the occurrence of acute coronary events [4, 5]. In
zation (WHO) global noncommunicable status report pre- short, the fight against cardiovascular disease has become a
dicts that by 2030, the number of deaths from common challenge for all mankind regardless of region,
cardiovascular diseases will reach 22.2 million every year race, and country.
[1, 2]. Coronary heart disease is a heart disease caused by There are many imaging diagnosis methods for cardiovas-
atherosclerotic lesions in the coronary artery, resulting in cular diseases, mainly including X-ray, echocardiography,2 Computational and Mathematical Methods in Medicine
angiocardiography, MRI, and CT. X-ray chest film can display method to measure the hemodynamic abnormalities of ste-
the size, shape, position, and contour of cardiac large vessels notic coronary artery.
and observe the relationship between the heart and adjacent The use of CT-FFR in the diagnosis of coronary artery
organs, but its imaging parts overlap, it is difficult to distin- disease is the focus of current research. Therefore, 80
guish details, and it does not have three-dimensional imaging patients with coronary artery disease were studied. The basic
characteristics; so, it is impossible to directly provide hemody- data and imaging characteristics of the patients were ana-
namic data [6, 7]. Echocardiography can not only make ana- lyzed, and the diagnostic value of CT-FFR based on CAD
tomical diagnosis of cardiovascular diseases but also make system for coronary artery disease was comprehensively
functional diagnosis. It can observe the intracardiac move- evaluated.
ment, ventricular wall thickness, and the connection of cardiac
great vessels from any angle, but it is seriously affected by fac- 2. Materials and Methods
tors such as sound, visual field, resolution, and operator expe-
rience [8–10]. Although MRI has high temporal resolution 2.1. Research Objects. In this study, 80 patients with con-
and soft tissue resolution, it has poor effect on coronary artery firmed coronary artery disease by imaging examination,
imaging due to the thin diameter of coronary artery, tortuous aged 35-80 years, who were admitted to hospital for CCTA
shape, and more adipose tissue in adjacent parts [11, 12]. CT examination and FFR examination from May 2, 2019 to June
can measure the human body with highly sensitive instru- 5, 2021, were selected as the study subjects. 49 males and 31
ments according to the different X-ray absorption and trans- females were divided into 40 cases of the coronary ischemia
mittance of different human tissues and show the small group (FFR ≤ 0:8) and 40 cases of the noncoronary ischemia
lesions in any part of the body [13]. Coronary computed group (FFR > 0:8). This study has been approved by the
tomography angiography (CCTA) has become an important ethics committee of hospital, and the family members of
method for early diagnosis of coronary heart disease as a rapid the patients are informed of this study and sign informed
noninvasive imaging method developed in the past decade. consent.
The increasing number of CCTA examinations and related Inclusion criteria are as follows: (1) patients of voluntary
medical research and applications urgently requires automatic cooperation examination, (2) patients who signed informed
segmentation of coronary arteries in CCTA images. This can consent, and (3) patients’ image quality was good.
not only provide rich postprocessing tools for clinical diagno- Exclusion criteria are as follows: (1) patients had a fluc-
sis but also improve the efficiency of clinical diagnosis. It can tuation range of invasive FFR value, (2) patients had abnor-
also provide quantitative evaluation indicators for the diag- mal origin of coronary artery, (3) patients had a history of
nosis of coronary heart disease and improve the accuracy coronary stent implantation, and (4) patients received coro-
and automation of diagnosis. This study proposes an auto- nary artery bypass grafting.
matic coronary artery segmentation algorithm, which can
accurately segment the coronary artery lumen area according 2.2. CCTA Examination. The patients were examined by
to the structure and image characteristics of the vascular CCTA using the second-generation ostentatious dual-
lumen and surrounding tissues. However, it can only provide source CT instrument of Siemens, Germany. Patients were
the stenosis degree and wall information of coronary artery given breath-holding training before scanning to reduce
lumen and cannot accurately determine whether stenosis image respiratory motion artifacts and sublingual nitroglyc-
leads to distal hemodynamic abnormalities resulting in myo- erin 3 minutes before scanning to expand the coronary
cardial ischemia. artery. The ECG activity of patients was monitored through-
Although the image diagnosis method is more and more out the whole process. If the heart rate of patients exceeded
accepted by doctors, the traditional image diagnosis can only 70 times per minute, about 60 mg esmolol hydrochloride
be qualitative observation, without quantitative information, injection was intravenously injected. At a speed of 5.2 mL/
cannot realize the conversion from data to information, and s, 60 mL of nonionic contrast agent of iopamidol and
largely depends on the experience and ability of doctors, 50 mL of 0.9% sodium chloride injection were intravenously
which is greatly limited. Computer aided diagnosis (CAD) injected before elbow. The contrast agent tracer method was
system combines computer technology with image process- used to select the region of interest at the aortic root to
ing to analyze the patient’s image information, finally detect monitor the CT attenuation value. When the CT attenua-
the lesion, and help clinicians obtain more accurate evalua- tion value reached 100HU, it was waited for 5 seconds to
tion results [14, 15]. CAD system can avoid the influence start scanning. The scanning range was from 1 cm above
of doctors’ subjective feelings and improve different diagnos- aortic arch to 1 cm below cardiac diaphragm. Scanning
tic outcomes caused by doctors’ personal experience and parameters are as follows: detector collimation 1:5 × 125
knowledge differences, which plays an important role in pro- × 0:5 mm. The thickness is 0.65 mm. The tube current is
moting the radiological diagnosis of clinical medicine [16]. 350 mAs/turn. Rotation time is 0.3 seconds/cycle, and tube
At present, the measurement of fractional flow reserve voltage is120 kV.
(FFR) combined with performing invasive coronary angiog-
raphy is the gold standard for the diagnosis of hemodynamic 2.3. FFR Test. FFR is defined as the ratio of the maximum
abnormalities caused by coronary artery stenosis [17, 18]. blood flow that can be obtained in the myocardial region
CT-FFR is based on computational fluid dynamics and uses supplied by this vessel to the maximum blood flow that
CCTA data to calculate FFR value. It is a new noninvasive can be obtained theoretically under normal conditions inComputational and Mathematical Methods in Medicine 3
the same region in the presence of stenotic lesions in the cor- Input
onary arteries, that is, the ratio of the mean intracoronary
pressure at the distal end of the stenosis (Pd) to the mean
aortic pressure (Pa) at the coronary artery orifice under the Primary data Output results
maximum myocardial hyperemia. Coronary angiography
was performed by Judkins method through femoral artery
puncture. FFR was measured with a pressure/temperature
guide wire of 0.036 mm in diameter. Adenosine triphosphate Segmenting aorta Perform segmentation
was injected into the median elbow vein at a flow rate of
about 150 μg/kg to induce coronary circulation load. The
theoretical normal value of FFR is “1,” if FFR0.8 lesion does
not induce myocardial ischemia. Similarity of
Construct interception
tubular structure
surface
2.4. Automatic Coronary Artery Segmentation Algorithm.
The tubular structure similarity is applied to the vascular
enhancement of medical images. Firstly, the tubular struc-
ture similarity function is set as follows. Extract seed points Get threshold
Sði, j, h ; αÞ = 0 β1 > 0orβ2 > 0,
Single scale is improved to Analysis of vascular
EA 2 EB 2
Sði, j, h ; αÞ = 1 − exp − 2 1 − exp − 2 multi-scale morphology
2a 2b
W2 Figure 1: Process of coronary artery automatic segmentation
1 − exp − 2 algorithm.
2c
ð1Þ
2.5. CAD System of Coronary Artery. Coronary artery CAD
β1 , β2 , and β3 are the eigenvalues of Hessian matrix. EA system is a large unit of clinical medical image. In order to
improve the effectiveness and reliability of clinical aided
and EB are used for the characteristic differences between
diagnosis, this study designs a customizable and easy to
different forms such as disc-shaped p and spot-shaped
ffiffiffiffiffiffiffiffiffi
ffi struc-
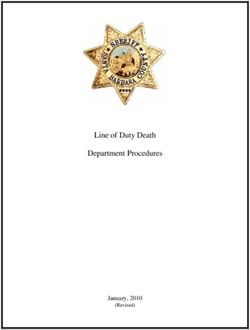
expand coronary artery CAD system (Figure 2). The system
tures, EA = jβ1 j/jβ2 j and EB = jβ3 j/ β1 β2 . W represents mainly includes data layer, model layer, and implementation
the brightness difference between the label and the sur-
qffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi layer. The data layer can realize the interaction and access of
rounding background, W = β1 2 + β2 2 + β3 2 . a is the pro- coronary CTA volume data, input the collected coronary
portion factor of influencing EA , b is the proportion factor data into the coronary CAD system for processing, and save
of influencing EB , and c is the proportion factor of influenc- the diagnosis results for clinical communication. The model
ing W, 0 < Sði, j, h ; αÞ < 1. layer contains the core technologies and algorithms of CAD,
In general, the radius of the coronary artery is between 2 which can extract valuable information from massive and
and 7 mm, and not all pixels can meet the current eigen- complex data. The implementation layer is a platform for
values under single-scale conditions; so, the similarity func- mutual communication between the system and doctors. It
tion needs to be calculated under multiscale conditions. can intuitively, quickly, and concisely display the data pro-
cessing results to users according to a certain workflow, such
as visual display of segmentation results, data query infor-
Sði, j, h ; αÞ = max fακ Sði, j, h ; αÞg: ð2Þ mation list, and operation log.
αmin ≤α≤αmax
In this study, the function of the whole system is divided
into multiple models for design, including command mod-
κ is the regularization coefficient. In practice, it is found ule, digital imaging, and communications in medicine
that the above algorithm still has the problems of low com- (DICOM) module, eXtensible Markup Language (XML)
putational efficiency and inaccurate seed point extraction in log module, report module, image module, script module,
single scale. Therefore, this study uses the position informa- data processing module, and algorithm module. The com-
tion of the ascending aorta to automatically locate the region mand module can uniformly process the input information
of interest, so as to reduce the range of seed point search area in the process of clinical diagnosis and coordinate the data
and reduce the computational complexity. In addition, the transmission between functional modules. DICOM module
three-dimensional geometric properties of coronary pixels can analyze and process different kinds of DICOM files to
and the brightness difference between coronary artery, bone ensure the correctness of the results and provide extended
tissue, and pulmonary vascular background are used to functions through the script system. The XML log module
restrict the extraction of coronary seed points and improve can parse and record the execution of each command, accu-
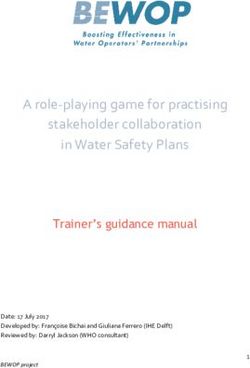
the accuracy of seed points. The final segmentation algo- rately locate the program exceptions, and output the param-
rithm flow is shown in Figure 1. eter information during execution. The report module can4 Computational and Mathematical Methods in Medicine
Focus Patient
Information Vascular
analysis information
transmission modeling
File query Implementation Data
Data layer Model layer
layer visualization
Data layer Coronary artery Vascular
segmentation Identification
information
algorithm result
extraction
Figure 2: CAD System for coronary artery.
automatically generate the corresponding graphic report tor analysis of variance was used for pairwise comparison.
according to the operation in the process of clinical diagno- The difference was statistically significant (P < 0:05).
sis. The image module can provide the function of drawing
various regions of interest. The script module can customize
and expand the function of coronary artery CAD using 3. Results
Python language. The data processing module can provide 3.1. Comparison of Basic Data of Patients. As shown in
the functions of saving, managing, and querying various Table 1, the age, height, weight, male ratio, hyperlipidemia,
data in the whole detection process. The algorithm module hypertension, diabetes, smoking history, total cholesterol,
is an embedded coronary artery CAD algorithm (Figure 3). HDL-C, LDL-C, triglycerides, and FPG of the ischemic
group and the nonischemic group were not statistically sig-
2.6. Clinical Data. Clinical information of patients was col- nificant (P > 0:05).
lected through the medical record system, including demo-
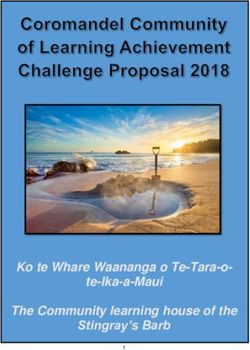
graphic characteristics (age, height, sex, weight), clinical 3.2. Imaging Data. Figure 4 shows the signs of normal coro-
history (lipidemia, hypertension, diabetes, smoking history), nary artery. The tube wall is smooth, and there is no stenosis
and biochemical examination results (total cholesterol (TC), in the lumen. Figure 5 shows the image of coronary artery
high-density lipoprotein cholesterol (HDL-C), low density calcification without stenosis. There is limited severe calcifi-
lipoprotein cholesterol (LDL-C), triglyceride (TG), and fast- cation near the heart, and the pipe wall is not smooth, but
ing plasma glucose (FPG)). there is no obvious stenosis at the location of calcification.
Figure 6 shows diffuse calcification with stenosis in the prox-
2.7. Image Features. Maximum diameter stenosis rate (MDS imal segment of the left coronary artery, with severe stenosis
%) and maximum area stenosis rate (MAS %) are measured in the corresponding segment.
and calculated, MDS% = ðBlood vessel diameter‐Diameter
of lumen at narrowest position/Blood vessel diameterÞ × 100 3.3. Comparison of CCTA Indexes between the Two Groups.
%, and MAS% = ðCross sectional area of blood vessel‐Cross‐ The MDS %, MAS %, and NRS of patients in the ischemic
sectional area of blood vessel at narrowest point/Cross group were significantly lower than those in the nonischemic
sectional area of blood vesselÞ × 100% . The total plaque vol- group (P < 0:05) (Figure 7). There was no significant differ-
ume (TPV), total plaque burden (TPB), calcified plaque vol- ence in RI and EI between the ischemic group and nonis-
ume (CPV), calcified plaque burden (CPB), noncalcified chemic group (P > 0:05).
plaque volume (NCPV), noncalcified plaque burden There was significant difference in TPV, TPB, CPV,
(NCPB), lipid plaque volume (LPV), lipid plaque burden LPV, and LPB between the ischemic group and the nonis-
(LPB), fiber plaque volume (FPV), and fiber plaque burden chemic group (P < 0:05) (Figure 8). There was no significant
(FPB) were measured. Napkin-ring sign (NRS), remodeling difference in CPB, NCPV, NCPB, FPV, and FPB between the
index (RI), and eccentricity index (EI) were calculated. ischemic group and nonischemic group (P > 0:05).
2.8. Statistical Methods. The data of this study were analyzed 3.4. Diagnostic Performance of Quantitative Indexes for
by SPSS19.0 statistical software. The measurement data were Coronary Myocardial Ischemia. From Figures 9 and 10, the
expressed by mean ± standard deviation (x ± s), and the diagnostic AUC area of MAS % is the largest (0.74), followed
counting data were expressed by percentage (%). Single fac- by MDS % (0.69), and LPV (0.68).Computational and Mathematical Methods in Medicine 5
The network transmits
various instructions
The documents are
DICOM
Data processed to ensure the
module
management Data module accuracy of the results
and query
Command
module
Coronary Function expansion
Algorithm Coronary
artery Script module based on python
model CAD system
segmentation language
Image module
Parsing and
recording Log module
commands
Reporting Generate graphic
module report
Draw various
regions of interest
Figure 3: Function demonstration of coronary artery CAD system module.
Table 1: Comparison of basic data of patients. 4. Discussion
Basic information Ischemic group Nonischemic group P value
In recent years, cardiovascular disease has developed into
Age (years old) 54:08 ± 10:11 50:89 ± 7:92 0.632
one of the diseases that seriously threaten human health,
Male (%) 66.38 63.92 0.583 and its early diagnosis and intervention are particularly
Height (cm) 161:41 ± 23:58 169:05 ± 21:44 0.591 important [19]. As a noninvasive imaging technology com-
Weight (kg) 63:94 ± 9:25 68:36 ± 8:11 0.792 monly used in clinic, CCTA has been proved to have high
accuracy in diagnosing coronary artery diameter stenosis
Hyperlipemia (%) 27.21 25.66 0.498
of cardiovascular diseases. With the development of CT
Hypertension (%) 62.07 69.44 0.511 imaging technology, the spatial resolution, temporal resolu-
Diabetes (%) 25.76 29.51 0.722 tion, and density resolution of CCTA have been greatly
Smoker (%) 26.09 30.75 0.537 improved, and CCTA has complete evaluation ability for
LDLC (mmol/L) 2:35 ± 0:74 2:48 ± 0:59 0.589 lesions with lumen diameter of more than 1.5 mm [20]. In
HDLC (mmol/L) 1:24 ± 0:35 1:09 ± 0:21 0.865 this study, 80 patients who underwent CCTA examination
and FFR examination in the hospital were selected as the
TC (mmol/L) 4:25 ± 0:84 4:11 ± 1:05 0.846 research objects. With FFR value of 0.8 as the dividing line,
FPG (mmol/L) 5:83 ± 1:38 6:13 ± 1:41 0.745 they were divided into the ischemic group (FFR ≤ 0:8) and
TG (mmol/L) 1:63 ± 0:36 1:44 ± 0:39 0.724 nonischemic group (FFR > 0:8). The basic data showed that
there were no significant differences in age, height, weight,
male ratio, hyperlipidemia, hypertension, diabetes, smoking
history, total cholesterol, HDL-C, LDL-C, triglycerides, and
3.5. Diagnostic Performance of CT-FFR in Two Groups of FPG between the ischemic group and nonischemic group
Patients. From Table 2, the diagnostic sensitivity, specificity, (P > 0:05), which provided reliability for subsequent
accuracy, cut-off value, and AUC area of CT-FFR for research results. Comparing the degree of lumen stenosis
patients in the ischemic group and nonischemic group are and the characteristic indexes of vulnerable plaque, it is
high, but the comparison between them is not statistically found that the MDS %, MAS %, and NRS in the ischemic
significant (P > 0:05). group are significantly lower than those in the nonischemic6 Computational and Mathematical Methods in Medicine
(a) (b)
Figure 4: Normal coronary artery signs ((a) is diastolic; (b) is systolic).
(a) (b)
(c)
Figure 5: Calcification of coronary arteries without stenosis ((a) is CCTA image; (b) is the reconstruction of surface; (c) is corresponding
angiography).
group (P < 0:05), while there is no significant difference in of lumen stenosis between ischemic and nonischemic patients.
RI and EI compared with the nonischemic group (P > 0:05), In addition, it was also found that there were significant differ-
which is similar to the research results of Zhang et al. (2020) ences in TPV, TPB, CPV, LPV, and LPB between the ischemic
[21], indicating that there are great differences in the degree group and the nonischemic group (P < 0:05), indicating thatComputational and Mathematical Methods in Medicine 7
(a) (b)
(c)
Figure 6: Calcification of coronary arteries with stenosis ((a) is CCTA image; (b) is the reconstruction of surface; (c) is corresponding
angiography).
90 ⁎ ⁎ ⁎
80 7
70
60 6
50 5
%
40
30 4
20 3
10
0 2
Ischemic group Non ischemic group
MDS% 52.66 65.41 1
MAS% 60.95 71.19 0
NRS (%) RI EI
MDS%
MAS% Ischemic group
Non ischemic group
(a) (b)
Figure 7: Comparison of the degree of lumen stenosis and characteristic indexes of vulnerable plaque between the two groups ((a) is MDS %
and MAS %; (b) is NRS, RI, and EI). Note: ∗ indicates that the difference is statistically significant compared with the ischemia group
(P < 0:05).8 Computational and Mathematical Methods in Medicine
⁎
Non ischemic group ⁎ Non ischemic group ⁎
Ischemic group Ischemic group
0 50 100 150 200 250 300 350 0 2 4 6 8 10 12 14
Ischemic group Non ischemic group Ischemic group Non ischemic group
TPB 51.37 60.82 CPB (%) 1.25 1.53
TPV 198.67 275.55 CPV (mm3) 4.12 9.35
TPB CPB (%)
TPV CPV (mm3)
(a) (b)
⁎
Non ischemic group Non ischemic group ⁎
Ischemic group Ischemic group
0 50 100 150 200 250 300 0 10 20 30 40 50 60 70 80
Ischemic group Non ischemic group Ischemic group Non ischemic group
NCPB (%) 47.46 52.59 LPB (%) 8.55 13.15
NCPV (mm^3) 203.36 231.17 LPV (mm^3) 33.74 56.94
NCPB (%) LPB (%)
NCPV (mm^3) LPV (mm^3)
(c) (d)
Non ischemic group
Ischemic group
0 50 100 150 200 250
Ischemic group Non ischemic group
FPB (%) 35.51 36.92
FPV (mm^3) 139.17 177.74
FPB (%)
FPV (mm^3)
(e)
Figure 8: Quantitative indexes of plaque volume and burden in two groups ((a) is TPV and TPB; (b) is CPV and CPB; (c) is NCPV and
NCPB; (d) is LPV and LPB; (e) is FPV and FPB). Note: ∗ indicates that the difference is statistically significant compared with the
ischemia group (P < 0:05).
70 0.75
100
60
80 0.7
50
60 40
0.65
%
30
40
20 0.6
20
10
0 0 0.55
MDS% MAS% LPV LPB MDS% MAS% LPV LPB
Sensitivity Truncated value
Specificity AUC area
Accuracy rate
(a) (b)
Figure 9: Diagnostic performance of quantitative indexes (MDS %, MAS %, LPV, and LPB) in coronary myocardial ischemia. Note: (a)
refers to sensitivity, specificity, and accuracy. (b) is the cut-off value and AUC area.Computational and Mathematical Methods in Medicine 9
100 120 0.64
0.62
100
80 0.6
80
0.58
60
60 0.56
%
40 0.54
40
0.52
20 20
0.5
0 0 0.48
TPB CPV CPB TPV TPB CPV CPB TPV
Sensitivity Truncated value
Specificity AUC area
Accuracy rate
(a) (b)
Figure 10: Diagnostic performance of quantitative indexes (TPB, CPV, CPB, TPV) in coronary myocardial ischemia. Note: (a) refers to
sensitivity, specificity, and accuracy. (b) is the cut-off value and AUC area.
Table 2: Diagnostic performance of CT-FFR in two groups of were high, but the comparison between them was not sta-
patients.
tistically significant (P > 0:05). This shows that CT-FFR
Index Ischemic group Nonischemic group P value based on computer-aided diagnosis system has high accu-
racy in evaluating myocardial ischemia caused by coronary
Sensitivity (%) 89.93 93.75 0.673
artery stenosis, and calcification does not affect the diag-
Specificity (%) 92.07 90.88 0.735 nostic accuracy of CT-FFR within a certain calcification
Accuracy rate (%) 95.84 96.24 0.626 score range.
Truncated value 60.51 58.22 0.857
AUC area 0.932 0.944 0.776
5. Conclusion
In this study, 80 patients who underwent CCTA examina-
there were differences in the characteristics of vulnerable pla- tion and FFR examination in the hospital were selected as
ques between the ischemic and nonischemic patients. In con- the research objects. Taking the FFR value of 0.8 as the
clusion, the characteristics of coronary artery disease dividing line, they were divided into the ischemic group
(coronary lumen area stenosis or vulnerable plaque compo- (FFR ≤ 0:8) and nonischemic group (FFR > 0:8). The basic
nent index, etc.) may have better diagnostic value for coronary data and imaging characteristics of the patients were
disease-specific myocardial ischemia. analyzed. The results showed that CT-FFR based on
The diagnostic performance of quantitative indexes for computer-aided diagnosis system had high accuracy in eval-
coronary myocardial ischemia was analyzed. The results uating myocardial ischemia caused by coronary artery steno-
showed that the diagnostic AUC area of MAS % was the sis, and calcification did not affect the diagnostic accuracy of
largest (0.74), followed by MDS % (0.69) and LPV (0.68), CT-FFR within a certain calcification score range. However,
which was consistent with the research results of Ghanem this study is a small sample, single center, and retrospective
et al. (2019) [22], indicating that MAS % was better than data, especially CT-FFR-related research, which is lack of
MDS % in the diagnosis of coronary lesion specific myocar- large-scale, multicenter, and prospective clinical data to ver-
dial ischemia. This may be because MAS % can provide ify. In the future, such studies will be carried out to verify the
more lumen information. On the one hand, because com- robustness of its diagnostic efficacy based on larger sample
plex lesions such as diffuse lesions and bifurcation lesions size. Therefore, this study provides a data reference for the
are common, MDS % can only provide diameter stenosis clinical accurate diagnosis of cardiovascular diseases.
information at the narrowest lumen, while MAS % can pro-
vide stenosis area of lumen cross section at the narrowest
lumen to reflect lumen stenosis more truly. On the other Data Availability
hand, in the presence of eccentric plaque, MDS % often
overestimates the true degree of stenosis of the lumen due The data used to support the findings of this study are
to the evaluation of the diameter stenosis at the most severe available from the corresponding author upon request.
stenosis [23, 24]. By analyzing the diagnostic performance of
CT-FFR in the two groups, it was found that the diagnostic Conflicts of Interest
sensitivity, specificity, accuracy, cut-off value, and AUC area
of CT-FFR in the ischemic group and nonischemic group The authors declare no conflicts of interest.10 Computational and Mathematical Methods in Medicine
Acknowledgments [15] Z. Lv, D. Chen, R. Lou, and Q. Wang, “Intelligent edge com-
puting based on machine learning for smart city,” Future Gen-
This work was supported by Capital Health Development eration Computer Systems, vol. 115, pp. 90–99, 2021.
Research Project (2018-2-4064). [16] H. Emami, R. A. P. Takx, T. Mayrhofer et al., “Nonobstructive
coronary artery disease by coronary CT angiography improves
References risk stratification and allocation of statin therapy,” JACC: Car-
diovascular Imaging, vol. 10, no. 9, pp. 1031–1038, 2017.
[1] Z. Zhou, L. Xu, N. Zhang et al., “CT coronary angiography [17] R. F. Li, C. L. Hou, H. Zhou et al., “Comparison on radiation
findings in non-atherosclerotic coronary artery diseases,” Clin- effective dose and image quality of right coronary artery on
ical Radiology, vol. 73, no. 2, pp. 205–213, 2018. prospective ECG-gated method between 320 row CT and
[2] M. J. Blaha, M. B. Mortensen, S. Kianoush, R. Tota-Maharaj, 2nd generation (128-slice) dual source CT,” Journal of Applied
and M. Cainzos-Achirica, “Coronary artery calcium scoring: Clinical Medical Physics, vol. 21, no. 8, pp. 256–262, 2020.
is it time for a change in methodology?,” JACC: Cardiovascular
[18] M. J. Bom, R. S. Driessen, A. Kurata et al., “Diagnostic value of
Imaging, vol. 10, no. 8, pp. 923–937, 2017.
comprehensive on-site and off-site coronary CT angiography
[3] H. W. Goo, “Quantitative evaluation of coronary artery visibil- for identifying hemodynamically obstructive coronary artery
ity on CT angiography in Kawasaki disease: young vs. old chil- disease,” Journal of Cardiovascular Computed Tomography,
dren,” The International Journal of Cardiovascular Imaging, vol. 15, no. 1, pp. 37–45, 2021.
vol. 37, no. 3, pp. 1085–1092, 2021.
[19] H. Lee, S. Martin, J. R. Burt et al., “Machine learning and cor-
[4] E. K. Kerut, M. E. Hall, M. C. Turner, and M. R. McMullan, onary artery calcium scoring,” Current Cardiology Reports,
“Coronary risk assessment using traditional risk factors with vol. 22, no. 9, p. 90, 2020.
CT coronary artery calcium scoring in clinical practice,” Echo-
cardiography, vol. 35, no. 8, pp. 1216–1222, 2018. [20] S. L. Sellers, T. A. Fonte, R. Grover et al., “Hypertrophic car-
diomyopathy (HCM): new insights into coronary artery
[5] P. Heermann, W. Heindel, and C. Schülke, “Coronary artery
remodelling and ischemia from FFRCT,” Journal of Cardiovas-
anomalies: diagnosis and classification based on cardiac CT
cular Computed Tomography, vol. 12, no. 6, pp. 467–471, 2018.
and MRI (CMR) - from ALCAPA to anomalies of termina-
tion,” Rofo., vol. 189, no. 1, pp. 29–38, 2017. [21] N. Zhang, G. Yang, W. Zhang et al., “Fully automatic frame-
[6] J. M. Wolterink, R. W. van Hamersvelt, M. A. Viergever, work for comprehensive coronary artery calcium scores analy-
T. Leiner, and I. Išgum, “Coronary artery centerline extraction sis on non-contrast cardiac-gated CT scan: Total and vessel-
in cardiac CT angiography using a CNN- based orientation specific quantifications,” European Journal of Radiology,
classifier,” Medical Image Analysis, vol. 51, pp. 46–60, 2019. vol. 134, article 109420, 2021.
[7] K. M. Johnson, H. E. Johnson, Y. Zhao, D. A. Dowe, and L. H. [22] A. M. Ghanem, A. H. Hamimi, A. M. Gharib, and K. Z. Abd-
Staib, “Scoring of coronary artery disease characteristics on Elmoniem, “Automatic assessment of 3D coronary artery dis-
coronary CT angiograms by using machine learning,” Radiol- tensibility from time-resolved coronary CT angiography,” in
ogy, vol. 292, no. 2, pp. 354–362, 2019. 2019 41st Annual International Conference of the IEEE Engi-
neering in Medicine and Biology Society (EMBC), pp. 836–
[8] F. G. Meinel, “Coronary artery plaque burden in smokers and
840, Berlin, Germany, 2019.
never-smokers: quantification with cardiac CT,” Academic
Radiology, vol. 26, no. 12, pp. 1589-1590, 2019. [23] S. Mushtaq, E. Conte, G. Pontone et al., “Interpretability of
[9] L. Fan and K. Fan, “Lung cancer screening CT-based coronary coronary CT angiography performed with a novel whole-
artery calcification in predicting cardiovascular events,” Medi- heart coverage high-definition CT scanner in 300 consecutive
cine (Baltimore), vol. 97, no. 20, article e10461, 2018. patients with coronary artery bypass grafts,” Journal of Cardio-
vascular Computed Tomography, vol. 14, no. 2, pp. 137–143,
[10] A. G. Gheorghe, C. Jacobsen, R. Thomsen et al., “Coronary
2020.
artery CT calcium score assessed by direct calcium quantifica-
tion using atomic absorption spectroscopy and compared to [24] Q. Li, Y. Tong, Y. Yin, P. Cheng, and G. Gong, “Definition of
macroscopic and histological assessments,” International Jour- the margin of major coronary artery bifurcations during radio-
nal of Legal Medicine, vol. 133, no. 5, pp. 1485–1496, 2019. therapy with electrocardiograph-gated 4D-CT,” Physica Med-
[11] E. K. Kerut and J. T. Balart, “"Diagnosis" of a hiatal hernia from ica, vol. 49, pp. 90–94, 2018.
a CT coronary artery calcium scan,” Echocardiography, vol. 34,
no. 10, pp. 1515–1518, 2017.
[12] J. M. Lee, K. H. Choi, B. K. Koo et al., “Prognostic implications
of plaque characteristics and stenosis severity in patients with
coronary artery disease,” Journal of the American College of
Cardiology, vol. 73, no. 19, pp. 2413–2424, 2019.
[13] E. Rinaldi, S. Sadeghi, S. Rajpal et al., “Utility of CT angiogra-
phy for the prediction of coronary artery compression in
patients undergoing transcatheter pulmonary valve replace-
ment,” World Journal for Pediatric and Congenital Heart Sur-
gery, vol. 11, no. 3, pp. 295–303, 2020.
[14] F. Nous, R. P. J. Budde, T. A. Fairbairn et al., “Temporal
changes in FFRCT-guided management of coronary artery dis-
ease - lessons from the ADVANCE registry,” Journal of Car-
diovascular Computed Tomography, vol. 15, no. 1, pp. 48–55,
2021.You can also read