DISABILITY AND LABOUR MARKET INTEGRATION - ANALYTICAL PAPER
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ANALYTICAL PAPER
DISABILITY AND LABOUR
MARKET INTEGRATION
Employment, MAY 2016
Social Affairs
and InclusionEurope Direct is a service to help you find answers
to your questions about the European Union.
Freephone number (*):
00 800 6 7 8 9 10 11
(*) The information given is free, as are most calls
(though some operators, phone boxes or hotels may charge you).
More information on the European Union is available on the internet (http://europa.eu).
Luxembourg: Publications Office of the European Union, 2016
ISBN 978-92-79-63218-1
doi:10.2767/26386
© European Union, 2016
Reproduction is authorised provided the source is acknowledged.
Cover picture: © European Union
The European Network of Public Employment Services was created following a Decision of the European Parliament and Council in June
2014 (DECISION No 573/2014/EU). Its objective is to reinforce PES capacity, effectiveness and efficiency. This activity has been developed
within the work programme of the European PES Network. For further information: http://ec.europa.eu/social/PESNetwork.
This activity has received financial support from the European Union Programme for Employment and Social Innovation "EaSI" (2014-2020).
For further information please consult: http://ec.europa.eu/social/easi
LEGAL NOTICE
This document has been prepared for the European Commission however it reflects the views only of the authors, and the Commission
cannot be held responsible for any use which may be made of the information contained therein.ANALYTICAL PAPER
DISABILITY AND LABOUR
MARKET INTEGRATION
Written by Ágota Scharle and Márton Csillag, Budapest Institute
MAY 20165
CONTENTS
1. BACKGROUND AND INTRODUCTION TO THE PAPER 6
2. CURRENT LABOUR MARKET SITUATION OF PEOPLE WITH DISABILITIES 7
3. POLICY FRAMEWORK FOR THE LABOUR MARKET INTEGRATION OF PEOPLE
WITH DISABILITIES 8
3.1 Types of policies supporting labour market integration 8
3.2 Recent policy developments 8
3.3 Role of public employment services 10
4. MEASURES AND SERVICES TO SUPPORT THE LABOUR MARKET INTEGRATION
OF JOBSEEKERS WITH DISABILITIES 12
4.1 Preventive measures 12
4.1.1 Mandatory rehabilitation during sick leave – Denmark 12
4.1.2 Experience rating in the Netherlands 13
4.1.3 Early intervention by the employer: the Dutch Gatekeeper protocol 13
4.2 Assessment of disability 14
4.2.1 Involvement of health specialists in Austria 14
4.2.2 Estonian reform of evaluating eligibility for disability benefit 15
4.3 Financial incentives to encourage job search and re‑employment 15
4.3.1 Financial incentives in Norway 15
4.3.2 Financial incentives in the Netherlands 16
4.4 Rehabilitation measures to improve employability 16
4.4.1 Personalised services provided in-house by the PES: examples from the UK 17
4.4.2 In-house rehabilitation services provided by the Hungarian PES 17
4.4.3 Subcontracted services for specific sub‑groups: a Dutch example 18
4.4.4 Specialised programmes for particular subgroups: a Danish example 18
4.4.5 Individual Placement and Support (IPS) 18
4.4.6 Social enterprise for placing jobseekers with disabilities in Austria 20
4.4.7 Sheltered employment in Spain 20
4.5 Engaging employers 21
4.5.1 Quota system in Austria and Spain 21
4.5.2 Wage subsidy in Sweden 21
4.5.3 Workplace adjustment scheme in the UK 21
4.5.4 Job creation by reallocating tasks in the workplace: a Dutch experiment 22
4.5.5 Anti-discrimination campaign in the UK 22
4.5.6 Appealing to CSR commitments: the two ticks symbol of the UK 23
5. SUMMARY OF EFFECTIVE APPROACHES AND GAPS IN THE EXISTING EVIDENCE.
RECOMMENDATIONS FOR FURTHER EVALUATIONS 23
REFERENCES 25
ANNEX 296
1. BACKGROUND AND
INTRODUCTION TO THE PAPER1
In Europe today, a large share of the population Against this background, this paper aims to review
suffers from a disability and consequently many recent policy initiatives supporting the labour mar-
people continue to be excluded from the labour ket integration of people with a disability, focus-
market; this exclusion can mean that people are ing on measures implemented by public employ-
either held back from accessing a job or they ex- ment services (PES). It builds on a previous paper
perience difficulties in finding and retaining a job. produced under the European Commission’s PES
Moreover, the number of people who suffer from to PES Dialogue programme that explored the
a disability that constrains their ability to work, ex- causes of and possible solutions to the rising inci-
ceeds the number of jobseekers in most EU Mem- dence of disability (EC 2013).
ber States (Eurostat 2011).2 Although there
is some evidence that the prevalence of health The next section summarises the main trends
problems improved (or at least stagnated) in most regarding the labour market situation of people
EU Member States until 2008, this trend turned with disabilities across the EU. Thereafter, Section
during the global financial crisis,3 and in several 3 briefly outlines the broader policy framework
Member States, the recent rise was especially and Section 4 describes policy measures that have
marked among youth (OECD 2015).4 been proven effective in increasing the employ-
ment rate of jobseekers with disabilities. Most
Disability exists on a continuum, ranging from of the measures presented come from Austria,
minor to severe and multiple disabilities. In par- Denmark, Hungary, the Netherlands and the UK,
ticular, Eurostat data shows that severe disabili- where significant policy reforms have taken place
ties affect only a small share of the working age in the past decade. We selected examples that
population. About 72 % of people with disabili- represent the main types of integration measures,
ties do not have a severe limitation in daily ac- which have also been evaluated by a counterfac-
tivities due to a health problem and about 75 % tual method. Section 4 concludes with a summary
do not need assistance in their daily activities.5 of the findings and some key recommendations
In this this paper the focus will be on the large for PES in supporting the labour market integration
majority of the population with disabilities who of people with disabilities.
are capable of working in the open labour market
and can potentially benefit from PES services. 6
1 Excellent research assistance by Adrienn Győry, Tamás
Molnár and Anna Orosz is gratefully acknowledged.
2 The exceptions include Greece, Spain, Ireland and Latvia,
according to the Eurostat survey of 2011 (comparing
the [hlth_dlm040] and [une_nb_a] indicators of Eurostat
online).
3 Based on the time series of the EU European Union
Statistics on Income and Living Conditions (SILC) indicator, 5 Eurostat online indicators [hlth_silc_06] and [hlth_
“People having a long-standing illness or health problem, dpeh130], age 15/16-64, self-reported disability, based
by sex, age and labour status” [hlth_silc_04]. on the SILC survey of 2012.
4 In some countries (e.g. Bulgaria, Germany, Greece, Spain, 6 It should be noted that national regulations vary
and Sweden), the rising incidence of health problems considerably: in some MS disability benefit recipients are
among youth is a relatively recent phenomenon, while obliged to cooperate with the PES (or another authority)
in other countries, a rising trend has been observed since in others there is no such obligation. In some countries all
2005 (e.g. increased for example Austria, France, Malta, in need can access PES services and ALMP, while in others
or Portugal) (Data from EU SILC, hlth_silc_04). this is tied to benefit receipt.7
2. CURRENT LABOUR
MARKET SITUATION OF
PEOPLE WITH DISABILITIES
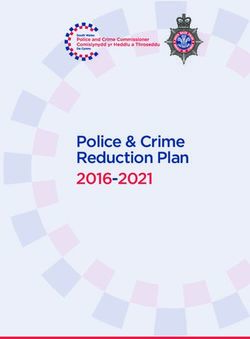
The employment rate of people with disabilities changes in labour supply and labour demand ap-
is significantly lower than those without. As Fig- pear more influential than demographic factors.8
ure 1 below shows, the employment gap of this For example, the sudden rise of disability benefit
group 7 ranges between 0.46 and 0.91 in the prime expenditure in the 1970s and 1990s was itself
age population. People with disabilities face more a response to changes in the labour market and
difficulty in finding employment and are there- welfare systems. The underlying cause was a de-
fore more likely to become long-term unemployed cline and structural shift in labour demand towards
or inactive (Eurostat 2015). While most of them skilled workers and a subsequent rise in long-term
are able to work, they often need additional sup- unemployment. More recently, as governments
port and the coordinated provision of employment, have curbed spending on unemployment benefits,
health and welfare services to be able to return disability benefits have become a benefit of last
to the labour market. resort for the long-term unemployed or inactive
population (EC 2013).
Figure 1: Employment gap of people with disabilities in the population aged 20-54 in 2011
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Ireland
Bulgaria
Slovakia
Romania
Netherlands
Croatia
Poland
Czech Republic
Denmark
Belgium
Lithuania
Greece
United Kingdom
Cyprus
Malta
Estonia
Germany
EU28
Portugal
Iceland
Slovenia
Spain
Turkey
Italy
Sweden
France
Latvia
Finland
Austria
Switzerland
Luxembourg
Hungary
Source: LFS 2011 ad hoc survey. Ratio of the employment rate of people with and without disabilities. The ratio equals 1 if people
with disabilities have the same employment rate as those without. Note that the countries covered in this paper are marked
in light blue.
The differences in health status only have a small The employment gap between people with dis-
role in explaining cross-country variation in the abilities and those without is determined by demo-
level or time trend in the incidence of disability graphic and economic factors, as well as national
claims. The impact of the business cycle also ap- welfare policies, but with no definitive empirical
pears to be small, although there is some evidence evidence on their relative strength. An OECD study
that disability benefit claims increase during reces-
sions (OECD 2010). In most countries, structural
8 As opposed to transitory effects of the business cycle,
structural changes may affect the equilibrium level
7 This is the ratio of the employment rate of people with of supply or demand, e.g. permanently reduce demand
disabilities to the employment rate of people without. for low-skilled workers.8
shows that the impact of the business cycle on the is likely to reflect medical practices, perceptions
employment gap is small compared to the effect and institutional features, as well as health condi-
of disability itself (OECD 2010).9 This suggests tions (EC 2013; Jones 2016).10 A further difficulty
that the above-mentioned structural shifts in la- in explaining the gap is that demand for workers
bour demand and the employment-friendly design with disabilities is determined by the perceived
of disability policies are likely to have a stronger productivity of such employees and possibly also
impact (OECD 2010). by discrimination (Jones 2006; Ward and Gram-
menos 2007; Baldwin and Choe 2014). While some
This lack of clarity on the causes is partly due to the of the employment gap can be clearly attributed
lack of reliable and comparable data on people with to the lower educational attainment of the popula-
a disability. Across Europe, the share of people with tion with disabilities (Eurostat 2015, Jones 2016),
disabilities varies between 5 % and 24 % of the the remaining gap is difficult to account for as the
working age population; this relatively wide range underlying causes cannot be directly measured.
3. POLICY FRAMEWORK FOR THE
LABOUR MARKET INTEGRATION
OF PEOPLE WITH DISABILITIES
This chapter briefly reviews the broader policy level and conditions of disability benefits, changes
framework and its recent changes, which determine in public education with an aim to improve access
the direction of developments for PES services and and quality, through to training programmes and
measures provided for jobseekers with disabilities. the integration of services. Active labour market
policies (ALMPs) offered to jobseekers with disa-
bilities may include mainstream programmes with
3.1 Types of policies supporting or without additional support to overcome their
labour market integration disability and programmes tailored to their specific
needs, such as vocational rehabilitation, supported
Policies promoting the labour market integration employment, targeted wage subsidies or sheltered
of people with disabilities may focus on the de- employment. Well-designed disability policies can
mand or the supply side. The former include anti- significantly increase the labour market integra-
discrimination legislation, awareness-raising cam- tion of people with disabilities and PES – as the
paigns, employment quotas, wage subsidies and main provider of labour market services and the
services for employers. Supply-side interventions prime contractor of ALMPs – have an important
may range from healthcare reforms, improvement role to play in implementing them.
of prevention and rehabilitation, regulation of the
9 A 1 %-point rise in the output gap (deviation from the 3.2 Recent policy developments
potential output of the economy) lowers the employment
rate of men with a disability by 1.1 %, while having As summarised by EC (2013), effective disability
a disability lowers the likelihood of employment by 19 %
(OECD 2010: 32). The impact on women is roughly twice
policy needs to tackle all the stages of entering
as large as for men. See also Meager and Higgins (2011). and exiting the labour market, and at all of these
10 The social perception of what constitutes a disability stages, measures need to ensure early and well tar-
varies across time and cultures and may also geted access to high-quality rehabilitation services,
be influenced by labour market status (Kreider and Pepper while targeting cash transfers on those in genuine
2007). The eligibility conditions of disability benefits also
need (rather than reducing levels of payments
vary considerably across time and between countries and
this may also influence self-perceived disability (Banks to those in need). In most Member States, the ex-
et al. 2004). isting policy framework is a considerable distance9
from achieving this ideal. However, there is a dis- served between 1990 and 2007 were larger in both
tinct tendency in most Member States to improve the integration and the compensation dimension.
the effectiveness of disability policies (Scharle, Though somewhat slower, policy developments
Váradi, and Samu 2015; OECD 2010). To visual- pointed in the same direction in both the Liberal
ise this tendency, OECD experts constructed two (Anglo-Saxon countries, except Ireland) and the Cor-
composite indicators measuring, on the one hand, poratist (Continental Europe and Ireland) regimes.12
the dominance of policies that encourage labour
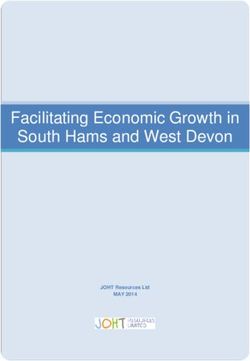
market integration, and on the other hand, the gen- Figure 2 illustrates that, despite the common trend,
erosity and targeting of cash benefits.11 By plotting there is considerable variation in the magnitude and
the value of the two indicators for each year, one pattern of change across countries. This variation
can produce a figure in which movement towards to some extent reflects the broader institutional
the upper left corner signals ‘progress’ in the sense context, or the so-called welfare regime type.13
that the changes lead to more employment-friendly Countries within the Social-Democratic regime (ex-
policies, as recommended by the OECD. Figure 2 emplified by Denmark and the Netherlands in Fig-
below shows the evolution of these two indicators ure 2) appear to have made most progress in both
in selected EU Member States between 1990 and dimensions: in terms of integration measures, Dan-
2014: in all countries there is a clear shift towards ish policies advanced from 29 to 37 points, while
strengthening integration measures (moving up- Dutch policies from 15 to 35 points. The generos-
wards) and tightening access to disability benefits ity of compensation measures was also tightened
(moving towards the left). considerably (from 39 to 24 in the Netherlands and
36 to 28 in Denmark) in both countries. Corporatist
regimes tended to advance in compensation rather
Figure 2: Main trends in disability policies in than in integration policies (as exemplified by Hun-
selected countries, 1990-2014 gary and Spain, and less so by Austria). Lastly, the
UK (which belongs to the Liberal type) focused more
45
on integration than on compensation in the period
between 1990 and 2008, given that their compen-
40
2014 sation policies were already rather parsimonious
2008
2014
2008
in 1990. This clear trend breaks in 2008, when
35
UK policies turn to the further tightening of com-
Integration score
2014 2014
2008 pensation measures, which is probably explained
30
2008 1990
DK by fiscal austerity triggered by the global crisis.
2014
25
2008 2014
2008
11 The Integration score is a composite indicator of legal
1990
20
AT 1990 provisions to enhance labour market integration and
1990 ES access to rehabilitation services; while the Compensation
HU
1990
15
1990 score is a composite indicator of rules of access to and
UK level of cash transfers. Both indicators are calculated
NL
as a sum of ten sub-indicators, which are measured
10
on a scale of 0 to 5 (for a detailed explanation see OECD,
10 15 20 25 30 35 40 45
2010: 85). For the integration score, 50 points indicate
Compensation score
highly developed and accessible rehabilitation services,
Source: Using the indicator system developed by OECD while for the compensation score, 50 points indicate very
(2010). For 1990-2007: OECD (2010), for 2008-2014: generous provisions that are likely to reduce incentives
Boeheim and Leoni (2015) for Austria, Denmark, the to work.
Netherlands, and Spain, own calculations for Hungary 12 This typology is based on clustering OECD countries
and the UK. against detailed indicators describing their disability
policies as observed in 2007. Thus, this typology may
not apply to the overall welfare system of any given
country and may also change over time. However, the
The OECD study of 2010 noted the striking similar- sorting of the countries mostly corresponds to the classic
ity of the trends in disability policies across welfare typology of Conservative-Corporatist, Liberal, and Social-
regime types, challenging earlier findings about the Democratic regimes formed by Esping-Andersen (1990)
reform-resistance of Continental regimes (OECD, on the basis of the main source of welfare provisions
(insurance, the market and the state, respectively).
2010; see Figure 6 below). On average, Social Dem-
13 The first typology of welfare regimes proposed by
ocratic regimes (including the Nordic states, Ger- Esping-Andersen (1990) distinguished the Conservative-
many and the Netherlands in their typology) moved Corporatist, the Liberal, and the Social-Democratic type,
faster than the others, i.e. the policy changes ob- based on the main producer of welfare.10
Though all countries have made some progress tend to increase during recessions (OECD, 2010)
towards achieving employment-friendly policies, and, as recent statistics on benefit expenditures
they differ considerably in the choice of particular suggest, the global financial crisis has indeed
measures in the period observed between 1990 put considerable pressure on social protection
and 2013 (Scharle et al 2015).14 There are a few budgets. Spending on disability cash benefits
measures that have been applied by almost all increased in several Member States after 2008
countries, regardless of the institutional context. (see Table A2 in the Appendix). Figure 2 suggests
These include the tightening of sickness absence that the crisis did not favour policy efforts in pro-
monitoring, limiting the permanence of benefit moting labour market integration either.
payments, introducing or tightening employer ob-
ligations (e.g. towards sick employees or the hir-
ing of workers with disabilities) and the expansion 3.3 Role of public employment
of personalised rehabilitation services. The timing services
of vocational rehabilitation was also brought for-
ward in most countries. Disability policies involve several policy areas
and institutions, starting from legislation on sick
The use of some measures seems regime-specific leave, disability benefits and pensions, through
(Scharle et al 2015). The combination of compul- to preventive healthcare to quota systems and
sory rehabilitation with significant investments vocational rehabilitation. Few European countries
in personalised reintegration services is mainly have a comprehensive system of prevention and
observed in Social Democratic countries, which rehabilitation measures: most Member States
have a long tradition of publicly supplied welfare provide legal protection against discrimination,
services and activation. Liberal regimes tended many have introduced quotas to encourage the
to rely on the further tightening of benefit access hiring of jobseekers with disabilities and several
combined with labour supply incentives for benefit Member States have tightened access to disabil-
recipients, with much less reliance on incentives ity pensions (EC 2013). But, with few exceptions,
for employers, which is consistent with a tradi- rehabilitation services have remained underde-
tion of market-friendly interventions and low (or veloped, underfunded or underused.16 Preventive
non-existent) minimum wages. By contrast, the measures during sick-leave and incentives to re-
popularity of wage subsidies in Corporatist re- duce the number of days spent on sick leave pose
gimes may reflect the need to win the support a challenge, even in those countries where acti-
of employers in a system where social partners vation measures are otherwise well developed.
have a strong influence on government policy and This highlights the need for strengthening the
where high minimum wages and labour taxation capacities of the PES, which have a leading role
increases the risk of hiring potentially low-produc- in managing or providing rehabilitation services
tivity workers with disabilities. and engaging employers in this area (Table 1).17
The observed policy shift also reflects the need
for combining incentives of labour supply and
demand. Shifting resources from cash transfers
to services can generate strong incentives for la-
bour supply, while also freeing up resources for
14 Scharle et al (2015) examines the patterns of policy
the development of rehabilitation measures. 15 change in 21 countries, including the EU-15 (except
The potential effects on employment are larger France, Italy and Greece), the Visegrad 4, Slovenia, Norway,
if the supply side measures are combined with Switzerland, as well as Australia and New Zealand.
incentives for employers, for example, in the form 15 The limitations of partial reforms is illustrated by the
of quotas, wage subsidies, or awareness-raising experience of Norway, where benefits levels are generous
and the employment gap between those with and without
about discriminatory hiring practices. disabilities has remained large, despite highly developed
rehabilitation services (Scharle and Váradi 2013).
It should also be noted that the global financial 16 While EU Member States spend between 0.1 and 17 %
crisis may have halted or slowed down policy de- of their GDP on active labour market policies and PES
velopments in some countries – in other words, services, funding for rehabilitation measures ranges
between 0.00 (Latvia) and 0.58 % (Denmark) (Eurostat
there were no or few reforms between 2008 online). Table A1 in the Appendix shows that per capita
and 2014 that made disability policies more spending on rehabilitation measures is very low, except
employment friendly. Disability benefit claims in the Scandinavian countries, France, and Germany.11
Table 1: Overview of the main types of ALMP targeting jobseekers with disabilities
SHELTERED VOCATIONAL SUPPORTED
WAGE SUBSIDIES
EMPLOYMENT REHABILITATION18 EMPLOYMENT19
Typical Public or non-profit PES or tax authority PES or non- PES or NGOs
provider companies governmental
organisations (NGOs)
Main Placement Subsidy to employer Ability testing, case Individualised
elements in a sheltered management, vocational
workshop, subsidy training, placement, rehabilitation and job
to employer and/or work adjustment preparation (trials),
employee, on the job measures job coaching and
training follow-up support
Target Severe disability Less severe disability Less severe disability All levels of disability
group
Typical Stable but segregated Employment in the Employment in the Permanent
outcome employment, open labour market open labour market employment in the
transition to open with subsidy with or without open labour market
labour market is rare subsidy
Source: EC (2013). See also Greve (2009) on sheltered employment.
Most Member States provide access to their regu- Most countries with an extensive rehabilitation
lar PES services and measures to jobseekers with system use one of two arrangements: Firstly,
disabilities. Where specialised rehabilitation ser- a dedicated unit within the PES provides services
vices are available, in most cases, these are also directly to jobseekers with disabilities (e.g. Den-
administered or signposted by the PES.20 Delegat- mark, France, Italy, Malta, or Sweden); and sec-
ing rehabilitation services to the PES may foster ondly, specialised counsellors refer such jobseek-
social integration (as it facilitates the meeting ers to external service providers, mainly NGOs
of jobseekers with and without disabilities), pro- with a specialisation in the specific disability (e.g.
mote activation and labour market integration Finland, Germany, Ireland, the Netherlands or the
(since that is the main function of the PES) and UK). In Finland, the PES have specialist counsellors,
is also likely to be more efficient as it avoids while in Germany and the Netherlands generalist
duplication in developing and providing services counsellors receive additional training to prepare
and maintaining vacancy databases. them for this task. In countries where rehabilita-
tion measures are less developed and counsellors
are not specialised, some PES offer at least diver-
sity awareness courses for counsellors.
17 In some countries, benefit claims are evaluated by a team
of experts including doctors and rehabilitation experts 19 For a more detailed description, see, for example, the best
who can assess the claimants’ potential for vocational practice guidelines issued by the UK Government (2011)
rehabilitation. In some cases, these experts are delegated or the toolkit of the European Commission and EUSE
by the PES (as in the Netherlands and the UK) or can (2010).
consult the PES (as in Hungary). 20 A few countries (e.g. Austria, Bulgaria, Romania) operate
18 For a more detailed description, see, for example, a separate system. In Hungary, a separate network
the list on the website of the Vocational Rehabilitation of rehabilitation centres was set up in 2011 and
Association UK. reintegrated into the PES in 2016.12
4. MEASURES AND SERVICES
TO SUPPORT THE LABOUR MARKET
INTEGRATION OF JOBSEEKERS
WITH DISABILITIES
This section presents the main types of policy eral terms, lower replacement rates, earlier and
intervention that are widely used in Europe, fo- more frequent visits to the rehabilitation counsel-
cusing particularly on those that have proved lor and more independent medical assessment
to be effective in supporting the labour market procedures prevent the prolongation of sick
integration of jobseekers with disabilities. These leave (beyond the time required for the recovery
include preventive measures, reliable assess- of health) and help maintain motivation for work
ment procedures and careful targeting, financial (Bound and Burkhauser 1999). Setting behav-
incentives, personalised rehabilitation services ioural conditions in order to prevent a move into
to improve employability, and engaging employ- unemployment during sick leave may also be ef-
ers. In selecting the measures we relied mainly fective, but is rarely used in Europe. One excep-
on counterfactual quantitative evaluations, but, tion is the so called Gatekeeper protocol in the
given the limited empirical evidence, in some Netherlands, which is detailed below (4.1.3).
cases we also used qualitative evaluations and
compilations of good practices. 4.1.1 Mandatory rehabilitation
during sick leave – Denmark
4.1 Preventive measures Denmark implemented a policy experiment
to measure the impact of intensive rehabilitation
In a broad sense, effective prevention requires support and activation during sick leave in 2009
measures in healthcare and work safety regu- (Rehwald, Rosholm, and Rouland 2015). At the
lation that reduce the incidence of illness and time of the experiment, sick leave was available
accidents, as well as an inclusive school system for a maximum of 52 weeks and the worker was
that ensures that children with disabilities have required to meet a municipal case manager (PES
an equal chance to get a high quality educa- counsellor) after the 8th week, and every fourth
tion. In this sub-section however, the focus is on week thereafter, to verify their health condition
a more narrowly defined range of institutional and discuss possible rehabilitation efforts. The
arrangements and measures centred on work- policy experiment was implemented by job cen-
ing-age adults who have lost some of their work tres in 16 municipalities, where every second new
capacity. In this case, prevention involves main- claimant was assigned to receiving intensified
taining or developing work capacity and the mo- support. The support lasted 18 weeks and con-
tivation to work or seek employment. Reviews sisted of weekly meetings with a caseworker and
of the existing policy practices suggest that early mandatory rehabilitation activities, which would
intervention is important in all stages of the re- take one of three forms (and could be applied
habilitation process – for people on sick leave, in combination as well). These included (a) voca-
as well as for disability benefit recipients (OECD tional counselling, skills development, on-the-job
2010, OECD 2015). Prolonged absence from training or internships; (b) paramedical care and
work tends to reduce motivation, employability, counselling; and (c) return to work with a grad-
and in some cases, the underlying health condi- ual increase of working hours. The combination
tion itself, all of which highlights the importance of the measures was determined by job centre
of early intervention. staff on the basis of the client’s needs. Workers
in the control group did not have access to para-
Most preventive measures focus on the indi- medical care and only met their caseworker every
vidual and relate to accessing benefits. In gen- four weeks.13
The outcomes were measured one, two and effect was observed only for workers with mild
three years after the first meeting with the cli- or medium disabilities.
ent. Results indicated that the intensified gradual
return-to-work option significantly improved out- 4.1.3 Early intervention by the employer:
comes in terms of return to regular employment, the Dutch Gatekeeper protocol
self-sufficiency, and unemployment, while the
intensified use of traditional activation meas- The Gatekeeper protocol was introduced in the
ures and paramedical care reduced subsequent Netherlands in 2002. The protocol obliges em-
performance. This means that those assigned ployers and employees on sick leave to develop
to the gradual return-to-work option worked 4.2 a return-to-work plan within eight weeks of ab-
weeks more in the first year after the start of the sence and continue efforts until the worker can
experiment, and 3.6-3.7 weeks more in the sub- resume work (Koning and Lindeboom 2015).
sequent two years (relative to the control group). The protocol also applies to disability insurance
Importantly, the positive effect of the gradual- claims: benefit claims can be awarded only after
return option was not present for workers with a mandatory waiting period of one year, during
a mental condition. which the employer pays sick leave benefit and
implements the return-to-work plan in coopera-
4.1.2 Experience rating in the Netherlands tion with the employee. The return-to-work plan
typically includes activities to re-organise work
Some countries employ incentives for employers to account for the work capacity of the sick per-
to prevent transitions into inactivity. For exam- son, as well as rehabilitation for long-term sick
ple, the Netherlands introduced experience-rated employees.
insurance, whereby firms with a worse record
of preventing or tackling disability pay higher in- If the worker has not fully returned to work at the
surance fees (J. de Koning 2004; de Groot, Nynke end of the waiting period, the worker then files
and Koning, Pierre 2016). A similar arrangement a disability benefit claim along with a return-
was introduced in Finland in 2007, but has had to-work report, which contains the original plan
no significant positive effect so far (Kyyrä and and an explanation of why it has not been ac-
Tuomala 2013; OECD 2008). complished. The social security administration
monitors the plan, and if they find that it is in-
In the Netherlands, experience rating in the dis- adequate or poorly implemented, the employer
ability insurance system was introduced in 1998, may be obliged to continue the payment of sick
which implied that employer contributions to the leave benefits for some months. This implies that
Disability Insurance Fund were linked to their the responsibility for early reintegration efforts
past experience of employees receiving disabil- is shifted from the social security administration
ity benefit. 21 Initially, employers were obliged to the employer.
to cover the costs of the first five years of dis-
ability benefits, which was extended to ten years The introduction of the protocol resulted in an
in 2006.22 immediate drop in the incidence of disability
insurance awards (from 1.4 % of the insured
A recent impact evaluation of the Dutch experi- population in 2001 to 0.8 % in 2004), which was
ence-rating regime (de Groot, Nynke and Koning, probably mainly due to screening effects. In a re-
Pierre 2016) used a modification in 2003, when lated study, Jong, Lindeboom, and Klaauw (2011)
small firms were temporarily exempted from the show that stricter screening causes both self-
experience-rated contributions. The estimates
compare inflows into disability benefit among
employees in small firms (not affected by the
21 The sickness benefit programme was privatised in 1996,
regime) and in other firms (subjected to the re- making employers fully responsible for covering these
gime), a few years before and after the modi- costs. Employers could reinsure this risk with private
fication. As other substantial reforms occurred insurers or bear this risk themselves (P. Koning and
in 2005, only short-term effects could be esti- Lindeboom 2015).
mated. The results show that entry into disability 22 The payment is calculated as a ratio of average disability
costs of (former) employees and the total wage costs
increased by 7 % while exits from disability de- of insured employees over five years, and both are taken
creased by 14 % for small firms no longer sub- with a two year lag. On average, the payment amounts
ject to experience-rated contributions. The second to about 1.5 % of the total wage cost.14
selection23 and increased effort to resume work as a potential target group of vocational reha-
during sick leave. These effects seem to have bilitation programmes (EC 2013). These clients
been further strengthened when the waiting pe- are in need of diverse support (physical/mental
riod was increased to two years in 2004 (Koning health support, employment support, information
and Lindeboom 2015). about the benefit claim process, etc.) and the as-
sessment of their work-readiness is often more
While these results confirm that making employ- difficult than it is generally the case with un-
ers financially responsible for their workers’ sick- employed clients. The lack of a well-coordinated
ness through the Gatekeeper protocol (as well and effective cooperation of the different actors
as experience-rated contributions) was an effec- involved in the assessment of the clients’ health
tive tool for prevention, it should also be noted status and the lack of timely action can be det-
that it may have some unintended negative side rimental to the clients’ rehabilitation. In recent
effects. Though rigorous evaluations are not yet years, Austria has seen a number of reforms that
available, there is some evidence of a recent can provide us with valuable information on im-
trend that vulnerable groups with bad health con- proved assessment methods and cooperation
ditions are directed towards flexible jobs, which practices.
are not subject to the same legislation. The Dutch
government is currently considering amendments 4.2.1 Involvement of health specialists in Austria
to both the Gatekeeper protocol and the expe-
rience-rating regime that would ensure strong The Fit2Work programme, launched Austria-wide
incentives at lower financial risks for employers in 2013, offers intensive case management and
(Koning and Lindeboom 2015). return-to-work support to clients with at least
40 days of sick leave. The aim of the initiative
is to reach people on sick leave before they reach
4.2 Assessment of disability the 40-day threshold and prevent job loss and
transit to long-term unemployment. Clients are
Effective rehabilitation services and permanent in part reached through contact with employers
disability benefits are costly, but these costs can (Fit2Work also provides consultancy to compa-
be mitigated by a transparent and reliable as- nies), but a large share of them enter Fit2Work
sessment procedure that ensures that in-kind and through referral by general practitioners or the
financial support is targeted to those in genuine PES. The programme is implemented by coun-
need. Reliable assessment requires the involve- sellors specialised in psychology, medicine and
ment of health and employment professionals social work and is funded and steered jointly
and a focus on remaining abilities beside the loss by the health insurance fund, the PES, the Min-
of particular functions. As jobseekers with dis- istry of Social Affairs and by the social partners
abilities often live with a permanent health con- (OECD 2015b; OECD 2015a). The majority (42 %)
dition, the cooperation between PES and health of the Fit2Work clients were found to suffer from
specialist is useful throughout the rehabilitation mental health issues. Fit2Work refers clients
process. to external psychiatrists or physiologists when
they are in need of a specific treatment.
Effective cooperation between the various actors
in benefit and service provision (such as pension The results of a recent impact evaluation
and health insurance funds, healthcare institu- by Statistik Austria (2015) suggest that on av-
tions, training providers and the PES) is key to the erage, participants of the programme spent
successful reintegration of people with chronic 15 days more in employment, 90 days after the
health problems, especially when considering end of the case management than their peers
that people with disabilities are often not treated in the control group and these positive results
hold for 180 and 360 days too. These results,
however, need to be interpreted with caution
23 The underlying idea is that people consider their chances because of the shortcomings in the evaluation
of meeting the benefit criteria and if screening is stricter, method (i.e. selection bias not addressed ade-
those with a less severe illness or disability will perceive quately; unclear matching procedure), but they
this chance to be lower and hence will not file a claim.
nevertheless indicate significant potential ben-
Thus, if it does not intimidate those who would in fact
be eligible for the benefit, stricter screening can improve efits of well-established disability assessment
the targeting efficiency of a scheme. procedures.15
Another relevant case from Austria is the ance Fund, which prepares the work ability as-
so called Health Road (Gesundheitsstraße), which sessment, which specifies the remaining abilities,
was initially implemented as a pilot in 2009 work capacity and options for suitable work.
and introduced nationwide in 2010. The objec-
tive of the project was to bring in line the as- The transition to the new system will be gradual.
sessment practices of the PES and the disabil- From 1 July 2016, the PES will start to assess
ity benefit agency and to eliminate duplications first-time claims, and from 1 January 2017, they
and uncertainties embedded in the procedures. will apply the new rules to working age bene-
In the new system, the assessment of clients ficiaries whose disability benefit entitlement
with more complex health problems takes place is about to expire.
within the framework of the Health Road, which
is structurally embedded in the disability insur-
ance agency, whose assessment is binding on the 4.3 Financial incentives
PES as well. This initial assessment is in all cases to encourage job search
financed by the PES. The reform replaced an old and re‑employment
system in which clients were sent back and forth
between the PES and the insurance agency, and Standard models of labour economics show that
where they had to get an official assessment the receipt of cash transfers tends to reduce
of their health condition from a number of differ- the motivation for work (Bound and Burkhauser
ent doctors. Evaluations of the reform concluded (1999)) and this applies to disability benefits
that it has accelerated the assessment process as well. Financial incentives that increase the
and in general led to greater transparency and relative gains of taking up a job, either by in-
efficiency. To one’s best knowledge, there are creasing in-work incomes or reducing out-of-work
unfortunately no impact evaluations measuring incomes, can therefore be effective in motivating
the labour market effects of this reform (OECD job search and re-employment. However, such in-
2015b; OECD 2015a). centives need to be designed carefully, so that
the main purpose of benefit payments (i.e. pro-
4.2.2 Estonian reform of evaluating eligibility viding an adequate income during unemployment
for disability benefit and allowing sufficient time for finding a suit-
able job) is not compromised. Incentives may fo-
As part of a broader policy reform 24 to reduce cus on the level and duration of different forms
the inflow into disability pensions and activate of sickness, disability and unemployment benefits
people with a disability, Estonia introduced new (as in the Norwegian reform of 2002) or on the
rules for evaluating applicants' work capacity and rules of benefit receipt while working (as in the
eligibility rules for the monthly financial social Norwegian reform of 2005).
security benefit (Masso 2015). As the new rules
only came into force in January 2016, there is no 4.3.1 Financial incentives in Norway
evaluation available about their effects yet.
Norway reformed their Temporary Disability Insur-
The new system shifts the focus from evaluating ance (TDI) system in January 2002. In the new
incapacity to work towards assessing the claim- system, the benefits are calculated on the basis
ant’s remaining work capacity. First, the claimant labour income observed in the last year (or last
needs to attend a doctor for three months before three years), rather than the entire employment
filing an application with the Estonian Unemploy- history of the individual prior to disablement.
ment Insurance Fund (which was recently merged At the same time, the minimum level of benefits
with the PES) to have her work ability assessed. was increased and the maximum child allowance
They fill in a self-assessment test of their abili- payment was cut. For certain groups this resulted
ties in a variety of activities, such as mobility, in an increase of their TDI benefits, while for oth-
personal care and learning. Next, a medical ex-
pert compares the test results with health re-
cords and provides an assessment of work ability. 24 These entailed among others, several measures
If there is a discrepancy or missing information, to increase the supply and quality of active labour
market services and rehabilitation services for the
the expert may invite the claimant to a personal people with an occupational disability. An overview of the
appointment. Lastly, the expert sends their as- reform as well as the details of the evaluation method
sessment to the Estonian Unemployment Insur- is available in English at the website of the line ministry.16
ers it decreased them. Fevang, Hardoy, and Røed uses more than 50 % of their remaining work ca-
(2013) found that a 10 % cut in the benefit level pacity. The subsidy is paid to the employee and
increases the likelihood of moving into regular em- its amount is such that the beneficiaries do not
ployment by about 3 % and into unemployment experience a drop in their incomes.26 The change
by 4.1 %, while it also increases the chance of exit implied strong incentives for employment dur-
to permanent disability by 3.4 %. This result un- ing the second phase, especially for those with
derlines the need for combining financial incen- a shorter employment history.
tives with transparent and reliable assessment
processes, which may prevent benefit substitution. In their evaluation of the Dutch reform, Koning
and van Sonsbeek (2016) found a significant
In the 2005 reform, the Norwegian government impact on the likelihood of staying or entering
introduced the option for Disability Insurance (DI) employment, which was larger for those aged
recipients returning to work to keep a portion below 45, having shorter (previous) employment
of their benefit. The amount of the partial ben- histories, and also for those with higher work dis-
efit is reduced by approximately 6 euros for every abilities and with mental disorders.
10 euros in earnings. Only recipients who had
been awarded DI before January 1, 2004 were
eligible to the programme. 4.4 Rehabilitation measures
to improve employability
An evaluation study by Kostol and Mogstad (2014)
found that three years after its implementation, As we show in this sub-section, the existing
this return-to-work incentive increased the labour empirical evidence suggests that personal-
force participation of DI recipients by 8 percentage ised services such as supported employment,
points in the 18-49 age group. According to their rather than large-scale uniform programmes
findings, besides increasing the overall earnings (training or sheltered workshops) are more ef-
of DI recipients, the programme also decreased fective in promoting a transition into the open
the costs covered by the central budget through labour market. A likely reason for this is the
a significant reduction of DI benefits and an in- large variation in the needs of people with dis-
crease in the taxes payed by DI recipients. abilities, as they require different forms of re-
training and counselling in adapting their daily
Importantly, the programme had no significant routine to changed abilities depending on the
effect among DI recipients aged 50-61 (those form and extent of their disabilities. This of-
who are approaching the retirement age). In the ten requires specialists who are not available
age group 18-49, the effects are substantially in PES. Outsourcing these services is most ef-
stronger for men, highly educated individuals and ficient in the case of hard-to-place clients, and
people living in areas with a low unemployment partially outcome-based financing can be espe-
rate. These results suggest that careful targeting cially effective(EC 2012). In the latter case, it is
can increase the efficiency of financial incentives. crucial that perverse incentives for creaming and
parking clients are constrained by financing tools
4.3.2 Financial incentives in the Netherlands and monitoring.
In the Netherlands, a negative financial incentive
was built into the new partial disability benefit
for those with substantial remaining work ca-
pacity (of 20-65 %), introduced in 2006.25 The
new benefit had two phases: in the first one, the
claimant may receive 70 % (same as before)
of their previous earnings for a maximum of 38
25 As inscribed in the Work and Income (Employment
months (the duration depends on prior employ- Capacity) Act of 2006. Note that those with a remaining
ment history), rather than 60 months, as it was work capacity of less than 20 % are considered ‘fully
in the earlier system. In the second phase, they disabled’, while those with remaining work capacity
receive a flat-rate benefit (which is set at 70 % of over 65 % are not entitled to disability benefits. Also,
the previous partial disability benefit was paid to workers
of the statutory minimum wage multiplied by the with a degree of disability of over 15 %.
percentage of incapacity) and are entitled to an 26 The subsidy effectively ‘tops-up’ the person’s income,
earnings subsidy if re-employed in a job that such that it reaches 70 % of previous earnings.17
4.4.1 Personalised services provided in-house gramme. 60 % of the participants were offered
by the PES: examples from the UK a work placement at charities or local communi-
ties, involving simple (e.g.: cleaning, shelf-stack-
The Pathways to Work programme in the UK was ing, etc.) and some more complex activities (e.g.:
introduced as a pilot experiment in different re- customer service). Those not in a job placement
gions in the UK in 2003. The Programme specifi- were focusing on looking and applying for jobs
cally targeted incapacity (disability) benefit recip- while receiving ongoing job search support from
ients, eight weeks after making a new or repeat their CAP provider.
benefit claim. The treatment group participated
on a voluntary basis in a series of Work Focused McAuley (2013) finds that in the long run (91
Interviews (WFI), while the control participants weeks) OCM has undoubtedly led to more posi-
had to attend only one WFI. WFIs comprised a se- tive employment and off-benefit outcomes than
ries of meetings between the programme partici- CAP. OCM participants spent 27 days less on any
pants and personal advisers. Personal advisers type of benefit and 13 days more in employ-
supported participants in focusing on their ability ment than the control group. Compared to the
to work, helped them develop a personal action control group receiving standard PES support,
plan, discussed work opportunities and counselled CAP participation has also produced better re-
them on various further issues (such as debt sults: they spent fewer days on benefit and more
management or financial assistance). In addi- in employment, however, the difference was not
tion to the WFIs, there were a number of further significant. For non-disabled participants without
provisions available to programme participants, disabilities and especially those above age 25,
such as mentoring, financial support upon finding the CAP programme had better results, implying
a job or in-work support. that work experience measures might not be ef-
fective enough for clients with more complex
Bewley et al. (2007) estimated that 18 months needs. Despite favourable employment and ben-
after the initial benefit inquiry, the control group’s efit (Jobseekers Allowance) outcomes, the share
probability of being employed was about 29.7 % of those receiving disability benefits or income
compared to 37.1 % in the treatment group. Im- support has also grown, partially offsetting the
portantly, the effect was driven by participants positive benefit effects.
no longer receiving incapacity benefit, i.e. those
with probably less severe disabilities. 4.4.2 In-house rehabilitation services provided
by the Hungarian PES
The UK introduced the so called Trailblazer pro-
gramme for the very long-term unemployed The Hungarian PES offered specific and person-
as a Randomised Control Trial in 2013 imple- alised services for jobseekers with disabilities
mented by the PES charities and local commu- between 2009 and 2013. The service offer was
nities. The intervention consisted of a 13 week available to all new claimants of the temporary
pre-treatment period during which participants rehabilitation allowance, which was introduced
were provided with information on another in- in 2008. The new allowance replaced permanent
tervention lasting for 26 weeks, starting at the disability pensions and provided support for up to
end of the pre-treatment period (the pre-treat- three years, with an obligation to cooperate with
ment period was used to test the deterrence job centres. The PES offered a personalised com-
effects of the measure.) During the treatment bination of subsidies and services: wage subsi-
period participants were randomly assigned to i) dies to employers and vocational rehabilitation,
Ongoing Case Management (OCM), ii) Commu- including covering the costs of training and vo-
nity Action Programme (CAP) and iii) to regu- cational education, psychological counselling and
lar PES support programs (control group). 34 % coaching. The scheme also reimbursed commut-
of the target group were made up of clients with ing and other related costs of working.
disabilities. OCM participants received intensi-
fied PES Jobcentre Plus services, had continu- Adamecz et al. (2016) estimated the impact
ous contact with their personal advisers (weekly of the services on uneducated participants (i.e.
meetings) and received flexible and personal- those who completed eight years of primary
ised services from the same adviser throughout education or less) by comparing employment
the entire programme period. CAP was a full- outcomes for participants and a comparable
time work experience or job-search support pro- control group. On average, about 70-93 % of the18
participants were reemployed during or shortly 4.4.4 Specialised programmes for particular
after completing the programme. Participants subgroups: a Danish example
of the programme were 26-30 percentage
points more likely to be re-employed than their Some types of disability require specialised
comparable peers who did not participate in the methods that are typically developed by innova-
programme. The programme also reduced the tive NGOs. An example for that is the Special-
probability of re-entering unemployment again, isterne Programme, which started as a Danish
by about 4-17 percentage points. The positive initiative and has grown to a global network. The
effect of the programmes is also significant programme targets clients aged 16-25 with au-
on the long-term unemployed and considerable tistic disorders and offers long-term mentoring
for those who did not receive wage subsidies. support, life skills and education services in or-
der to achieve labour market integration. The aim
There is likely to be an upward bias in these of the programme is to turn clients’ disability into
results, coming from the unobserved (self- a capability through employing them in sectors
selection) of the participants (which implies that where their skills and abilities (e.g. detail-orien-
they had already had an advantage before the tation, precision) are highly relevant to perform-
start of the programme) and the lack of data ing work-related tasks. Besides helping clients
on undeclared work. It seems likely that those in gaining work-specific skills, the company itself
not participating in any programme (and thus employs people with autistic disorders as busi-
not benefitting from a wage subsidy) are more ness consultants, competing as a relevant player
likely to be re-employed in the shadow economy, on the open market with other IT firms. The pro-
which imposes a downward bias in the observed gramme has not yet been evaluated, thus the
employment outcomes of the control group. size of its impact cannot be ascertained.
4.4.3 Subcontracted services for specific 4.4.5 Individual Placement and Support (IPS)
sub‑groups: a Dutch example
IPS is a specific method for providing individu-
An alternative to in-house provision by the PES alised support for labour market integration
is to subcontract specialised services to dedi- that was initially developed for jobseekers with
cated NGOs. One example for that is the Dutch a mental condition. The key principles of IPS
Vangrail programme financed by the PES. The include a focus on employment in the regular
programme helps young school dropouts (aged labour market, rapid placement with a mini-
16 and above) with mental disabilities smooth mum of assessment, training on the job instead
their integration into the labour market. It offers of prevocational training and the integration
tailor-made services to the youth, including voca- of vocational services with mental health care.
tional training, job-experience and skills training
and long-term employment support. The founda- In Europe, the effectiveness of IPS was tested
tion running the programme cooperates closely in an international project called EQOLISE (En-
with regional remedial education centres provid- hancing the Quality of Life and Independence
ing health care services, as well as health profes- of Persons Disabled by Severe Mental Illness
sionals and parents related to the clients. Based through Supported Employment). In the EQOLISE
on De Vos (2012), about one in three programme trial, 312 individuals with severe mental illness 27
participants achieved labour market integration were randomly assigned to receive either IPS
between 2005 and 2010. or standard vocational services starting in 2003.
The sample was drawn from six European cit-
ies: Groningen (Netherlands), London (UK), Rimini
(Italy), Sofia (Bulgaria), Ulm-Günzburg (Germany)
and Zurich (Switzerland). People who entered the
trial had been ill and experiencing major difficul-
ties accomplishing normal roles for at least two
years and had not been employed for at least one
year. They were followed for 18 months.
27 Schizophrenia and schizophrenia-like disorders, bipolar
disorder or depression with psychotic features, using
IDC‑10 criteria.You can also read