Diagnosis and Management of Infantile Hemangioma
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CLINICAL REPORT Guidance for the Clinician in Rendering Pediatric Care
Diagnosis and Management of Infantile
Hemangioma
David H. Darrow, MD, DDS, Arin K. Greene, MD, Anthony J. Mancini, MD, Amy J. Nopper, MD,
the SECTION ON DERMATOLOGY, SECTION ON OTOLARYNGOLOGY–HEAD AND NECK SURGERY, and SECTION ON PLASTIC SURGERY
abstract Infantile hemangiomas (IHs) are the most common tumors of childhood. Unlike
other tumors, they have the unique ability to involute after proliferation, often
leading primary care providers to assume they will resolve without
intervention or consequence. Unfortunately, a subset of IHs rapidly develop
complications, resulting in pain, functional impairment, or permanent
disfigurement. As a result, the primary clinician has the task of determining
which lesions require early consultation with a specialist. Although several
recent reviews have been published, this clinical report is the first based on
input from individuals representing the many specialties involved in the
treatment of IH. Its purpose is to update the pediatric community regarding
recent discoveries in IH pathogenesis, treatment, and clinical associations and
This document is copyrighted and is property of the American to provide a basis for clinical decision-making in the management of IH.
Academy of Pediatrics and its Board of Directors. All authors have filed
conflict of interest statements with the American Academy of
Pediatrics. Any conflicts have been resolved through a process
approved by the Board of Directors. The American Academy of
Pediatrics has neither solicited nor accepted any commercial
involvement in the development of the content of this publication. NOMENCLATURE
Clinical reports from the American Academy of Pediatrics benefit from The nomenclature and classification of vascular tumors and
expertise and resources of liaisons and internal (American Academy malformations have evolved from clinical descriptions (“strawberry
of Pediatrics) and external reviewers. However, clinical reports from
the American Academy of Pediatrics may not reflect the views of the birthmark,” “salmon patch,” “cavernous hemangioma,” and “port wine
liaisons or the organizations or government agencies that they stain”) to terminology based on their cellular features, natural history, and
represent.
clinical behavior. Originally described by Mulliken and Glowacki in 1982,
The guidance in this report does not indicate an exclusive course of
treatment or serve as a standard of medical care. Variations, taking
the most current and widely accepted classification of vascular anomalies
into account individual circumstances, may be appropriate. is that adopted by the International Society for the Study of Vascular
All clinical reports from the American Academy of Pediatrics Anomalies (Table 1).1 This system includes infantile hemangioma (IH)
automatically expire 5 years after publication unless reaffirmed, among the vascular neoplasms, which are lesions characterized by
revised, or retired at or before that time.
abnormal proliferation of endothelial cells and aberrant blood vessel
www.pediatrics.org/cgi/doi/10.1542/peds.2015-2485 architecture. In contrast, vascular malformations are structural anomalies
DOI: 10.1542/peds.2015-2485 and inborn errors of vascular morphogenesis.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Although IH is the most common neoplasm, this group also includes such
Copyright © 2015 by the American Academy of Pediatrics tumors as congenital hemangiomas, pyogenic granulomas, tufted
angiomas (TAs), and several types of hemangioendothelioma. Congenital
FINANCIAL DISCLOSURE: The authors have indicated they do not have
a financial relationship relevant to this article to disclose. hemangiomas are biologically and behaviorally distinct from IH. As
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they
reflected in the name, congenital hemangiomas are present and fully
have no potential conflicts of interest to disclose. formed at birth; they do not exhibit the postnatal proliferative phase
Downloaded from www.aappublications.org/news by guest on October 23, 2021
FROM THE AMERICAN ACADEMY OF PEDIATRICS PEDIATRICS Volume 136, number 4, October 2015
characteristic of IH. The 2 variants are It is a reactive proliferating vascular and may grow slowly over the course
the noninvoluting congenital lesion that is classified as a vascular of months to years, grow rapidly,
hemangioma (NICH), which remains neoplasm (Table 1). This common spontaneously regress, or remain
stable without growth or acquired vascular lesion of the skin dormant for years.14–16 Unlike KHE
involution,2,3 and the rapidly and mucous membranes primarily and TA, IHs are not associated with
involuting congenital hemangioma affects infants and children and is thrombocytopenia or coagulopathy.
(RICH), which undergoes a rapid frequently misdiagnosed as IH. Vascular malformations are
involution phase beginning in the first Approximately 12% occur in infancy, congenital lesions, but some may
year of life (Fig 1).4 RICHs, in some and 42% present during the first 5 become clinically apparent only later
cases, have been associated with years of life.10 Pyogenic granulomas in life, presumably because of slowly
thrombocytopenia but with milder are most commonly located on the progressive ectasia resulting from
and more transient coagulopathy head and neck, rapidly enlarge to intraluminal flow. They exhibit
than that seen in Kasabach-Merritt a median size of 6.5 mm, frequently a normal rate of endothelial cell
phenomenon (KMP; see discussion develop a pedunculated base, and, turnover throughout their natural
that follows); rarely, they can be with erosion, are prone to bleeding history but expand as the patient
associated with congestive heart that is difficult to control (Fig 2).10 grows. Vascular malformations do not
failure.5,6 Some RICHs show Pyogenic granulomas are seen with involute, and their growth may be
incomplete involution, and it is higher frequency within the skin influenced by trauma, infection, and
possible that RICH and NICH lie at containing capillary malformations. hormonal changes. Classification is
opposite ends of the same clinical Two other distinct benign vascular based on the predominant vessel
spectrum.7,8 Both subtypes of neoplasms, kaposiform type: capillary or venulocapillary,
congenital hemangioma were initially hemangioendothelioma (KHE) and venous, lymphatic, arterial, or
believed to be variants of IH that TA, have been confused with IH. KHE mixed.17 As with vascular neoplasms,
exhibited prenatal growth until North presents primarily in infancy but with the nomenclature of vascular
et al9 showed that, unlike IH, neither a far wider age range than IH, which malformations has led to great
lesion expresses glucose transporter is usually apparent in the first month confusion. Capillary or
protein isoform 1 (GLUT1). of life. KHE is considered a locally venulocapillary malformations have
Pyogenic granuloma, also known as aggressive neoplasm that typically had numerous alternative
lobular capillary hemangioma, is appears as a deep, soft tissue mass. designations, the most common being
neither pyogenic nor granulomatous. This lesion has been associated with “port wine stain” and “nevus
KMP,11 a potentially life-threatening flammeus.” Venous malformations
consumptive coagulopathy have often been mistaken for IH,
TABLE 1 Classification of Cutaneous characterized by severe platelet
Vascular Anomalies, 2014 trapping. Before KHE was described
Vascular malformations in the early 1990s, KMP was
Venous malformations erroneously thought to occur in
Lymphatic malformations
association with IH.
Capillary malformations
Arteriovenous malformations and fistulae Histopathologically, KHE shows
Mixed (combined) malformations infiltrating sheets of slender, GLUT1-
Vascular tumors negative endothelial cells lining
Benign slitlike capillaries.12 TAs are benign
Infantile hemangioma (IH)
vascular tumors that occur in infants,
Congenital hemangioma (rapidly involuting
[RICH]; non-involuting [NICH]) children, or young adults and are
Lobulated capillary hemangiomas (LCH) usually located on the neck or the
(pyogenic granuloma)* upper part of the thorax.13 Their
Tufted angioma (TA) clinical appearance is variable and
Others
includes erythematous to violaceous
Locally aggressive
Kaposiform hemangioendothelioma (KHE) patches, plaques, and nodules.
Kaposi sarcoma Histopathologically, TA shows well-
Others defined tufts of capillaries in the
Malignant dermis that lack cellular atypia or
Angiosarcoma
GLUT1 positivity and, like KHE, is
Others FIGURE 1
associated with increased lymphatic
Adapted from the International Society for the Study of RICH is fully formed at birth (A) and then
Vascular Anomalies, 2014, ref 1 (issva.org/classification). vessels and a predisposition to KMP. involutes, mostly during the first year of life. B,
*Reactive proliferating vascular lesion Both tumors behave unpredictably The same lesion seen at 8 months of age.
Downloaded from www.aappublications.org/news by guest on October 23, 2021
PEDIATRICS Volume 136, number 4, October 2015 e1061
termed “cavernous hemangiomas” years, especially predating the among female infants; however,
and “venous hemangiomas” in the distinction between IH and the although older data suggest female-
literature (Fig 3A). Lymphatic congenital hemangiomas. to-male ratios ranging from 3:1 to 5:1,
malformations, which are subdivided “Hemangioma” has also been more recent studies suggest a range
into microcystic and macrocystic inappropriately used to describe, in of 1.4:1 to 3:1.23,24 The gender
varieties on the basis of predominant general terms, varieties of other discrepancy appears to be increased
lacuna size, may also be mistaken for noninfantile hemangiomas and among children with PHACE
IH when there is bleeding into vascular malformations. syndrome (Posterior fossa defects,
vesicles at the surface of the skin or Hemangiomas, cerebrovascular
mucosa (Fig 3B). These lesions have Arterial anomalies, Cardiovascular
traditionally been referred to as anomalies including coarctation of
“cystic hygromas” or Highlights of This Section the aorta, and Eye anomalies), in
“lymphangiomas,” designations that which studies have found a 9:1
• Infantile hemangioma (IH) is
inaccurately presume proliferative female-to-male ratio.25 There is not
the currently accepted termi-
potential, thereby perpetuating the a definitive explanation for this
nology for the lesions that are
diagnostic confusion. gender difference.
the focus of this clinical report.
The use of various names for IH has Most studies report a significantly
• Congenital hemangiomas are
resulted in immense diagnostic higher incidence in white
biologically and behaviorally
confusion. For instance, the terms infants.23,24,26 On the basis of the
distinct from IH.
“capillary hemangioma” and success of IH treatment using
“capillary angioma” have been used to • Pyogenic granuloma is a re-
b-blocker therapy, it has been
refer to an IH that is located primarily active proliferating vascular
proposed that black infants may
in the dermis and is bright red in lesion that is classified as
exhibit some form of “endogenous
color. In contrast, the designations a vascular neoplasm and
that may occasionally be beta blockade,” and there are
“cavernous” or “venous” have molecular biological data to support
inappropriately been used to define misdiagnosed as IH.
this notion.27
an IH that, because of its depth below • Lesions diagnosed as “cav-
the dermis, may impart a blue tinge to ernous hemangiomas” are The incidence of IH is increased
the skin surface. In addition, deep usually, in fact, deep IHs or among preterm infants, affecting 22%
venous and lymphatic malformations venous malformations. to 30% of infants weighing less than
as well as arteriovenous • Kasabach-Merritt phenome- 1 kg.24,28 Multivariate analysis has
malformations have been incorrectly non or KMP (a consumptive revealed that low birth weight (LBW)
diagnosed as deep IH. Finally, by coagulopathy) is not associ- is the major contributor to this risk;
virtue of its sheer prevalence, the ated with IH but rather with there is a 25% increase in risk of
term “hemangioma,” without the 2 other vascular neoplasms, developing an IH with every 500-g
adjectival descriptor “infantile” or kaposiform hemangioendo- reduction in birth weight.29 Prenatal
with the descriptor “juvenile,” has thelioma (KHE) and tufted factors have also been investigated
been used in reference to IH for many angioma (TA). for their role in IH. Studies differ
regarding an increased risk resulting
from maternal chorionic villus
sampling24,30 or amniocentesis,30,31
EPIDEMIOLOGY and any increased risk attributable to
chorionic villus sampling appears to
Studies of the incidence of IH,
be limited to procedures performed
including a prospective study and
transcervically.31 Other possible
a review incorporating 1
retrospective study and 2 cross- prenatal factors include older
sectional cohorts, suggest that 4% to maternal age, multiple gestation
5% of infants are affected.18,19 Other pregnancy, placenta previa, and
studies suggest that IH is observed in preeclampsia.24 Placental anomalies,
1% to 3% of newborn infants20,21 such as retroplacental hematoma,
FIGURE 2 and 2.6% to 9.9% of older infarction, and dilated vascular
Pyogenic granulomas have some clinical and communications, have also been
children,22,23 but methodologic
histologic features similar to IHs, but they are
generally smaller, pedunculated, and more shortcomings may have influenced associated with IH development.32 It
likely to bleed. these findings. IHs are more common is theorized that the common thread
Downloaded from www.aappublications.org/news by guest on October 23, 2021
e1062 FROM THE AMERICAN ACADEMY OF PEDIATRICS
in these associations is placental
hypoxia.32,33
Although often suggested as a risk
factor, a family history of IH is
reported in only 12% of cases24;
however, familial clustering has been
reported.34,35 Associations are also
reported with maternal use of fertility
drugs,36 use of erythropoetin,37 level
of maternal education,36 breech
presentation,23 and being the first
born.23
FIGURE 3
A, The venous blood contained within a venous malformation imparts a bluish hue that may lead to
Highlights of This Section misdiagnosis as a deep IH. B, Bleeding into surface vesicles of a lymphatic malformation may lead to
misdiagnosis as an IH.
• The incidence of in the gen-
eral population is approxi-
mately 5%. vasculogenesis, or the de novo This concept developed from
• Risk factors for IH include formation of new blood vessels.39,40 research showing that molecular
being white, being female, This theory is supported by studies markers characteristic of placental
and having a low birth showing increased numbers of tissue, including GLUT1, Lewis Y
weight. circulating EPCs in blood samples antigen, merosin, Fc-g receptor-IIb,
• Associations are also from children with IH.41 Additional indoleamine 2,3-deoxygenase, and
reported with older mater- evidence comes from studies in which type III iodothyronine deiodinase,
nal age, multiple gestation multipotential stem cells derived were also present in IHs.3,9 Clinical
pregnancy, placenta previa, from IH specimens (HemSCs) have evidence for this theory is suggested
preeclampsia, use of fertility shown the ability to recapitulate by those studies showing an
drugs or erythropoietin, human IH in immunodeficient mice.42 increased incidence of IH in
breech presentation, and These HemSCs and cord blood EPCs association with chorionic villus
being the first born. behave similarly to each other in sampling, placenta previa, and
several in vitro assays, suggesting preeclampsia.24,30,31
that circulating EPCs could be the A unifying theory suggests that IH
origin of IH endothelial cells.42 The results from aberrant proliferation
concept that IHs originate from and differentiation of a hemogenic
PATHOGENESIS AND HISTOPATHOLOGY circulating multipotent progenitor endothelium with a neural crest
cells could explain some of the phenotype and a capacity for
Pathogenesis features they share with placental endothelial, hematopoetic,
The pathogenesis of IH, despite blood vessels, because dysregulated mesenchymal, and neuronal
intensive study, has not been circulating EPCs have also been differentiation. It is hypothesized that
completely elucidated. Lines of implicated in many of the associated placental chorionic villus
evidence support a cellular origin maternal and fetal comorbid mesenchymal core cells embolize to
from either intrinsic endothelial conditions (preeclampsia, retinopathy the developing fetus and that the
progenitor cells (EPCs) or angioblasts of prematurity, etc). HemSCs have timing of this embolization in relation
of placental origin, but intrinsic and also been shown to have an to the migration of neural crest cells
extrinsic factors are also thought to adipogenic potential,43 which may along their somitic routes determines
contribute to their development.38 explain the presence of adipocytes the morphology of the IH (segmental
Intrinsic factors include the influence noted during involution. The stimulus versus localized [focal]; see section
of angiogenic and vasculogenic for division of EPCs is unknown but entitled “Clinical Appearance”).44
factors within the IH. External factors may be a somatic mutation or The cytokine niche within the IH,
include tissue hypoxia and abnormal signals from local tissues. including vascular endothelial growth
developmental field disturbances. The theory of placental origin factors (VEGFs), insulin-like growth
The EPC theory holds that IHs suggests that fetal progenitor cells factors, the tumor necrosis
develop from clonal expansion of arise from the disruption of the factor–related apoptosis-inducing
circulating EPCs, resulting in placenta during gestation or birth. ligand-osteoprotegerin (TRAIL-OPG)
Downloaded from www.aappublications.org/news by guest on October 23, 2021
PEDIATRICS Volume 136, number 4, October 2015 e1063
pathway, and the renin-angiotensin is an important sensor of hypoxia.9 Histopathology
system, subsequently regulates GLUT1 has been shown to be Grossly proliferative and early
growth of the IH and its response to upregulated in hypoxic zones of involutive IHs are well-circumscribed,
pharmacologic therapies.44 Other mesenchymal tumors and in unencapsulated masses with red-to-
authors have also embraced the umbilical cord–derived human tan cut surfaces. Later involutive
“niche” concept, suggesting that mesenchymal stem cells under lesions are fibrofatty in consistency
circulating EPCs find their way to hypoxic conditions.49,50 Hypoxia-
and less defined. The histologic
certain locations that provide induced factors produced by
features of IH change dramatically as
conditions favorable for growth into endothelial cells appear to play an
they proceed through their natural
important role in trafficking of
placentalike tissues.44 In tissues such course of neonatal presentation, rapid
progenitor cells to ischemic tissue.
as the skin and liver, progenitor cells growth, and subsequent involution,
These factors have been shown to be
may encounter the cellular signals requiring interpretation within the
upregulated in the blood (VEGF-A,
and local tissue factors required to proper clinical context.52–54 There is
MMP-9) and in IH tissue (stromal
stimulate their development. no sharp dividing line between
cell–derived factor 1a, MMP-9, VEGF-A,
proliferation and involution, and
On the basis of the rapid proliferation and hypoxia-inducible factor 1a)
features of involution typically coexist
of endothelial cells, earlier from children with proliferating IH.41
with features of proliferation during
investigations of IH origin focused on In addition, it has been shown that
much of the process. Early proliferative
angiogenesis, the sprouting of the use of erythropoietin in preterm
phase IHs are composed of well-
endothelial cells from existing blood infants increases the risk of
defined, unencapsulated masses of
vessels. Such studies have shown an developing an IH.37 Thus, tissue
capillaries lined by plump endothelial
increased concentration of angiogenic ischemia resulting in
cells rimmed by plump pericytes
factors in IH, such as basic fibroblast neovascularization from circulating
growth factor (bFGF), VEGF-A, EPCs has been proposed as the embedded within a multilaminated
insulin-like growth factor, and matrix stimulus leading to the development basement membrane without
metalloprotease (MMP) 9 within the of IH.41 Clinically, an area of pallor or associated smooth muscle cells (Fig 4).
lesion during proliferation.45 Also decreased blood flow in the skin has Lesions at this stage may at least
in this phase, investigators been noted to precede the focally resemble other rapidly growing
have identified indoleamine development of IH, further vascular proliferations such as early
2,3-deoxygenase, a protein thought to supporting this hypothesis.51 pyogenic granulomas. The proliferating
slow the involution of IH by inhibiting capillaries are arranged in lobules,
cytotoxic T-lymphocyte response.46 separated by delicate fibrous septae or
During involution, endothelial cell by normal intervening tissue. These
apoptosis is accompanied by lesional capillaries, depending on tissue
downregulation of angiogenic factors, location, intermingle nondestructively
Highlights of This Section with superficial skeletal muscle fibers,
whereas inhibitors of angiogenesis
such as interferon-b and markers of • may develop either from in- peripheral nerves, salivary glands, and
cell maturation such as intercellular trinsic endothelial progenitor adipocytes. Endothelial cells and
adhesion molecule 1 are cells (EPCs) or from angio- pericytes show variably enlarged
upregulated.47 It has also been shown blasts of placental origin. nuclei and abundant clear cytoplasm.
that involuting IHs exhibit decreased • IH growth is affected by in- Normally configured mitotic figures are
production of nitric oxide, trinsic influences, such as relatively numerous (Fig 1B); and
a potentiator of the VEGF pathway, as angiogenic and vasculogenic widespread expression of cell
measured by reduced levels of factors within the IH, and by proliferation markers, such as Ki-67,
endothelial nitric oxide synthase.48 external factors such as tis- confirm that both pericytes and
sue hypoxia and de- endothelial cells are actively dividing.
It has been hypothesized that hypoxia
triggers a vascular response in velopmental field Because proliferative phase IHs are
disturbances. high-flow lesions, although typically
infants. As discussed above, LBW is
• A unifying theory proposes without significant arteriovenous
a significant risk factor for IH, and in
that circulating EPCs migrate shunting, they often contain enlarged
utero hypoxia is a common cause of
to locations in which con- draining veins with thick, asymmetric
LBW. Not surprisingly, there is
mounting evidence of the role of ditions are favorable for walls.
hypoxia in the development of IH. growth into placentalike Involuting IHs present different
GLUT1, a facilitative glucose tissues. diagnostic challenges. Mitotic figures
transporter used as a marker for IH, wane, and apoptotic bodies and masts
Downloaded from www.aappublications.org/news by guest on October 23, 2021
e1064 FROM THE AMERICAN ACADEMY OF PEDIATRICS
cellular linings. Epidermal atrophy
Highlights of This Section
and underlying fibrous scar tissue
may be present if the lesion ulcerated • Proliferating IHs are well
in the proliferative phase. Large circumscribed and lack
arteries and veins modeled during the a capsule.
high-flow proliferative phase do not • Involuting IHs are fibrofatty
completely regress when the capillary and less defined.
bed drops out and thus are often
• GLUT1 is a commonly used
present in involuting IH. This
immunochemical marker for
phenomenon, paired with loss of
IH.
FIGURE 4 endothelial mitotic activity, may lead
Proliferative phase IH. Well-circumscribed lobules to mistaken histologic diagnosis as
of closely packed capillaries composed of a vascular malformation.
plump endothelial cells and pericytes are sep- CLINICAL PRESENTATION,
arated by normal-appearing dermal stromal
Misdiagnosis can usually be avoided
by considering overall histologic COMPLICATIONS, AND ASSOCIATIONS
elements (hematoxylin and eosin stain; original
magnification 3100; photo courtesy of Paula appearance and clinical history. Phases of Growth
North, MD.) Ultimately, as discussed below, the
issue can be resolved by GLUT1 IHs exhibit a characteristic life cycle.
immunoreaction, because involuting Clinical observations have suggested
infantile IHs, but not malformations, that there are at least 2 dynamic
cells increase in number during early
will show GLUT1 immunopositivity in evolutionary phases, namely,
involution.48,55 Lesional capillaries
residual lesion-type capillaries.9,56 proliferation and involution.
begin to disappear. There is no
Proliferation occurs during early
evidence of thrombosis, and Histologic examination, accompanied infancy; gradual spontaneous
inflammation is not prominent. As by routine immunohistochemical involution or regression starts by
involution proceeds, lesional capillary studies, shows that proliferative 1 year of age.58–65 An intermediate
basement membranes become thick phase infantile IHs are complex period between proliferation and
and hyalinized and contain specks of cellular mixtures with large involution during mid-to-late infancy,
apoptotic debris (Fig 5). Eventually complements of endothelial cells, often referred to as the “plateau”
all that remains in an end-stage lesion pericytes, mast cells, and interstitial phase, more likely represents
is loose fibrous or fibrofatty stroma, dendritic cells. Electron microscopy a period of temporary balance
containing a few residual “ghost” reveals plump endothelial cells lining between individual cells that are
vessels composed of residual, small lumina and resting on proliferating and those undergoing
thickened rinds of basement a multilaminated basement involution and apoptosis.59–66 The
membrane material containing membrane that envelops a cuff of process of involution takes several
apoptotic debris and without intact pericytes. The endothelial cells of IH years and varies in duration.
have been reported to immunoreact
positively for “normal” endothelial Proliferative Phase (Up to 12 Months of
markers of the blood vasculature, Age)
such as CD31, CD34, factor
VIII–related antigen (von Willebrand Premonitory findings in the skin
factor), and others.57 Currently, the during early infancy may include
most useful and widely used localized blanching or localized
immunohistochemical marker for the macular telangiectatic erythema.
diagnosis of IH is GLUT1.9,57 GLUT1 is As endothelial cell proliferation
strongly expressed by endothelial continues, the IH enlarges, becomes
cells of IHs at all stages of their more elevated, and develops
evolution and is not expressed by a rubbery consistency. During this
other benign vascular anomalies and period, IHs often show surrounding
FIGURE 5 reactive proliferations. GLUT1 pallor and dilatation of surrounding
Involutive phase IH. Lesional capillaries are set veins. During rapid growth periods,
within loose fibro-adipose tissue and are less immunohistochemistry is frequently
used to distinguish IHs from other ulceration may arise, leading to pain
densely packed than in the proliferative phase.
Note the thickened and hyalinized basement vascular neoplasms and provides and eventual scarring.
membranes studded with apoptotic debris,
convincing evidence that IHs are IHs typically have their clinical onset
reflective of the involutive process. Residual
lining endothelial cells are mitotically inactive. indeed as biologically distinctive as before 4 weeks of age.66,67 They
(Photo courtesy of Paula North, MD) they are clinically distinctive. proliferate for variable periods of
Downloaded from www.aappublications.org/news by guest on October 23, 2021
PEDIATRICS Volume 136, number 4, October 2015 e1065
time, depending in part on their
morphology and configuration.
However, most IH growth appears to
occur between 1 and 2 months of
age.68 A large prospective study has
indicated that 80% of IH size is
generally reached by 3 months, and
most growth is completed by around
5 months of age.66 Deep IHs appear
somewhat later and grow somewhat
longer than their superficial
counterparts.66
Involution Phase
For most infants with IH, involution FIGURE 6
begins between 6 and 12 months of Cutaneous IHs may be classified on the basis of their depth. A, Superficial IHs are visible only at the
skin surface and may be focal (as shown) or segmental. B, Deep IHs have no surface involvement. C,
age. Although the process continues
Mixed, or compound, IHs have both superficial and deep components.
over years, the majority of tumor
regression occurs before age 4.48,69,70
As IHs involute, most lesions flatten
soft tissue depth.61,62,72 Superficial superficial and deep IHs. These
and shrink from the center outward.
IHs (Fig 6A) are those in which the observations indicate that deep IHs
For those with a superficial component,
surface of the tumor appears red and require a longer period of
this is accompanied by “central
there is little to no discernible monitoring than those with
clearing” or graying of the surface.
subcutaneous component; superficial morphology.
Although IHs generally undergo historically, these IHs have been A specific subtype of superficial IH
spontaneous regression, observations described as being of the has been variably referred to as an
of “maximal involution” do not “strawberry” type. Deep IHs (Fig 6B) abortive, nonproliferative, arrested-
necessarily imply complete are those in which the tumor resides growth, minimal-growth, nascent,
resolution. Indeed, approximately deep to the skin surface, and their reticular, or telangiectatic IH.73–76
50% to 70% of IHs resolve, leaving subcutaneous location results in This type of IH presents as a macular,
behind residual skin changes, a bluish surface hue or no evident telangiectatic patch that may be
including telangiectasia, fibrofatty surface changes; historically, these accompanied by blanching of the
tissue, redundant skin, anetoderma, have been referred to as “cavernous,” involved skin (Fig 7). Unlike most IHs,
dyspigmentation, or scar.71 an imprecise term that is no longer abortive IHs lack an obvious
commonly used. Combined, mixed, or significant proliferative phase.
compound IHs (Fig 6C) are those in Approximately two-thirds of these
Highlights of This Section which both superficial and deep lesions are situated on the lower
components coexist. extremities. Many are accompanied
• IHs usually make their initial
appearance before 4 weeks Superficial IHs tend to appear earlier by localized, small papular regions of
of age and complete most of and begin to involute sooner than vascular tissue growth, often around
their growth by 5 months of their deep counterparts, which, the periphery.77 Abortive IHs share
age. by contrast, tend to arise later with more typical IHs characteristic
and grow for longer periods surface markers (eg, GLUT1),
• Involution of IHs begins as
of time before involuting (on confirming that they are true IHs;
the child approaches 12
average, approximately 1 month however, their growth phase may be
months of age. In most cases,
more).62,64,66 Investigations into arrested. Many of these telangiectatic
the majority of involution is
these differences confirm that these IHs also involute more rapidly,
completed by age 4.
timelines represent characteristic sometimes before 1 year of age.78
growth patterns for these IHs rather Nevertheless, complications such as
than arising out of observational ulceration may occur. These IHs may
bias.66 As might be expected, those also be segmental and occasionally
Clinical Appearance IHs with a mixed morphology have have syndromic associations (see
During the proliferative phase, IHs a growth pattern that is intermediate section entitled “IH Syndromes and
can be classified on the basis of their between those associated with Associations”).79
Downloaded from www.aappublications.org/news by guest on October 23, 2021
e1066 FROM THE AMERICAN ACADEMY OF PEDIATRICS
definitively focal or segmental are Multifocal cutaneous IHs are
considered indeterminate. Multifocal frequently isolated to the skin but
lesions are focal lesions occurring at may also serve as markers for
more than 1 anatomic site. One large underlying hepatic involvement
study found that most IHs (67.5%) are (Fig 9).88–91 Previous retrospective
localized, whereas the remainder were reports26,81 suggested that the
segmental (13%), indeterminate presence of a large or segmental
(16.5%), or multifocal (3.6%).83 (.5 cm) cutaneous IH might prove
The presence of a large, facial a useful marker for hepatic IHs.
FIGURE 7 segmental IH is a hallmark sign of However, results from a large
Abortive IHs are macular, telangiectatic patches prospective study suggest that it is
that have failed to fully proliferate. PHACE syndrome,25 whereas large
segmental IHs of the anogenital and the number of cutaneous IHs rather
lumbosacral areas may be associated than their size that is the more
IHs may also be classified on the basis with genitourinary system and predictive factor.92 When 5 or more
of their anatomic configuration as spinal cord anomalies as part of IHs are present on cutaneous
either localized (focal), segmental, other syndromes84–86 (see section examination, ultrasonography may
indeterminate, or multifocal.26,80,81 entitled “IH Syndromes and be helpful in assessing potential
Localized (focal) IHs are discrete Associations”). More recently, it has hepatic involvement.84,93
lesions that seem to arise from been recognized that extracutaneous Hepatomegaly and congestive heart
a single focal point, whereas manifestations may also arise in failure also suggest the presence of
segmental lesions cover a territory association with segmental IHs liver IH.
that is presumed to be determined by involving other anatomic sites, as
embryonic neuroectodermal part of the so-called PHACE-without-
placodes.82 Segmental IHs tend to face phenomenon.87 These patients Highlights of This Section
involve a larger surface area of skin. may have segmental IHs of the upper • IHs are characterized as su-
Segmental IHs of the face have been chest, shoulder, or arm in the perficial, deep, or mixed and
observed to conform to unique absence of facial IH involvement and as focal, multifocal, or
developmental units, which have in conjunction with structural heart segmental.
been mapped into 4 distinct patterns: disease, aortic or other major vessel • Superficial IHs appear ear-
frontotemporal, maxillary, anomalies, central nervous system lier and begin involution
mandibular, and frontonasal and sternal defects, or eye sooner than their deeper
(Fig 8).82 Lesions that are not anomalies. counterparts.
• Segmental IHs are more
commonly involved in
PHACE (see text for defini-
tion) and other IH syn-
dromes and associations.
• The presence of more than 5
focal IHs suggests a higher
risk of hepatic involvement.
FIGURE 8
(A) Patterns of segmental IH of the face extracted from image analysisdefined. Seg1 (fronto- FIGURE 9
temporal), Seg2 (maxillary), Seg3 (mandibular), and Seg4 (frontonasal). (B) An ulcerated segmental Multifocal cutaneous IHs in a child with IH of
IH in the maxillary distribution. the liver.
Downloaded from www.aappublications.org/news by guest on October 23, 2021
PEDIATRICS Volume 136, number 4, October 2015 e1067
Complications to develop complications and 8 times usually results in scarring, with the
Although most IHs do not require more likely to receive treatment.84 risk of permanent disfigurement. As
urgent treatment, a minority may Segmental lesions tend to have longer a result, prompt initiation of therapy
develop function-threatening or life- proliferative phases, some with is essential in the management of
threatening complications, significantly prolonged duration of ulcerating IHs.
necessitating therapeutic growth as long as 10 to 44 months, The specific mechanisms resulting in
intervention. One study determined and may therefore require IH ulceration are poorly understood.
that approximately 24% of patients significantly longer treatment It has been hypothesized that
with IH who were referred to a group durations.94 ulceration may develop secondary to
of tertiary care dermatology practices The size of the IH was also an increased tissue hypoxia, which leads
experienced some complication important predictor of the need for to the development of dermal fibrosis
related to their IH.84 It is therefore treatment in the aforementioned and then progresses to surface
prudent for pediatric providers to cohort study, although this analysis breakdown.98 In such cases, early
remain vigilant of possible did not appear to control for white discoloration of an IH, possibly
complications and of risk factors that anatomic subtype.84 The mean size of representing superficial dermal
may herald future complications. complicated IHs was 37.3 cm2, fibrosis, may be a premonitory sign of
Ulceration accounts for the majority compared with 19.1 cm2 for impending ulceration.99 Other
of IH complications; others include uncomplicated IHs. In addition, IHs proposed mechanisms include
bleeding, visual impairment, that received treatment of any type outgrowing of the blood supply or
had a mean size of 30.4 cm2, which rapid expansion exceeding the elastic
auditory impairment, congestive
was 11.1 cm2 larger than those that capabilities of the skin.99,100
heart failure, and airway
did not receive treatment. However,
obstruction.84 Gastrointestinal Several studies have shown that
the mean size of segmental IHs is certain subsets of patients with IHs
bleeding has been reported as
approximately 10 times that of are at higher risk of ulceration. As
a complication of segmental
localized IHs,66 suggesting that discussed previously, superficial and
intestinal hemangiomatosis, in which
morphology may indeed be a more segmental IHs have been found to
the IH is typically situated in the
important indicator of potential be at higher risk of
distribution of the mesenteric
complications. ulcerating.96–98,101 In addition,
arterial system.94
Anatomic location was also specific locations at higher risk of
The single best predictor of
a predictor of complications due to ulceration include the head, neck,
complications and the need for
IH.84 Facial IHs were complicated 1.7 perioral, and perineal/perianal
therapeutic intervention for IH is
times more frequently than nonfacial regions and intertriginous sites
morphologic subtype.84 Focal IHs
IHs; they were also 3.3 times more (Fig 10).96–98,102 The neck and
have the potential to cause
likely than their nonfacial anogenital regions sustain
complications primarily by virtue of
counterparts to receive some form of maceration and friction, which may
their location on or near vital
therapy, likely because of concerns contribute to the development of
structures, such as the eye
for cosmesis. Periocular IHs and ulceration. Ulceration has also been
(amblyopia, astigmatism), nose
those in the “beard” distribution are noted to occur more frequently in
(anatomic distortion and
also more likely to require infants younger than 4 months,
cartilaginous destruction), ears
intervention, as described below. In a period of time during which the IH
(anatomic distortion and
1 study, perineal IHs were the most
cartilaginous destruction), lips
likely to ulcerate.95
(anatomic distortion and ulceration),
airway (obstruction), or anogenital
region (ulceration). On the face, focal Ulceration
lesions are 3 times more common Ulceration, or breakdown of the IH
than segmental IHs.81 Segmental IHs skin surface, occurs with an
are more frequently complicated by estimated incidence of 5% to 21%.96
ulceration.84 A prospective cohort Ulceration was the most common
study in 1058 patients undertaken to complication in a large prospective
identify clinical characteristics cohort of children with IHs,
predicting complications and need for occurring in 16% of the study
treatment found, after controlling for population.97 Ulceration can lead to
FIGURE 10
size, that segmental IHs were 11 significant pain, bleeding, and Ulcerated segmental IH of the perineal/perianal
times more likely than localized IHs secondary infection. Ulceration also region.
Downloaded from www.aappublications.org/news by guest on October 23, 2021
e1068 FROM THE AMERICAN ACADEMY OF PEDIATRICS
is actively proliferating.96–98 See the IHs had feeding and oral sensory develop noisy breathing or a hoarse
section entitled “Management of problems that resulted in failure to cry.106
Ulcerated IH” for a discussion in thrive.105 The cutaneous findings associated
greater detail. with underlying airway involvement,
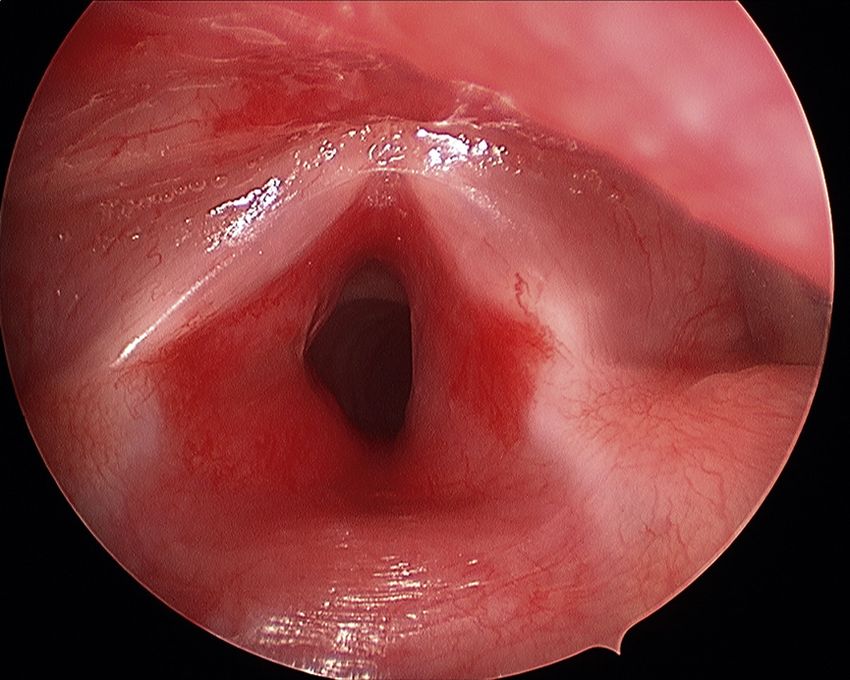
Airway Involvement and Obstruction when present, help to identify those
Airway IHs can occur in the presence patients at greatest risk of airway
Bleeding
or absence of skin findings. IHs. Cutaneous IHs in a “beard”
Although concern for potential Symptomatic obstructive airway IHs, distribution, defined as involving the
bleeding in IH is common among including supra- and subglottic IHs, preauricular regions, chin, anterior
caregivers and providers, it occurs usually present with progressive neck, or lower lip (Fig 11), have been
rarely and almost exclusively in biphasic inspiratory and expiratory associated with airway
ulcerated lesions. The majority of stridor during the first 6 to 12 weeks involvement.106,107 Infants with IHs
bleeding that occurs in nonulcerated of age as the lesion is proliferating.105 within this distribution bilaterally
IHs is minor and easily controllable Affected infants may also rapidly appear to be at an even higher risk of
with pressure. The most common
such scenario is an IH that has
sustained minor surface trauma (ie,
from friction or a fingernail), bled
minimally, stopped bleeding
spontaneously or with minimal
sustained pressure, and subsequently
presents with surface hemorrhagic
crusting.
In a large prospective study of
ulcerated IHs, bleeding occurred in
41% of lesions but was clinically
significant in only 2% of these
cases.96,98 Significant bleeding
requiring blood transfusion or other
intervention is infrequently
reported.98 Rare instances of life-
threatening bleeding have been
observed, including 1 report of
ulceration of a segmental neck IH into
arterial vessels, the bleeding from
which necessitated transfusions,
systemic and topical treatment of the
IH, embolization, and surgical
excision.102
Feeding Impairment
Feeding impairment can occur in
infants with IHs involving either the
perioral region or the airway. Infants
with ulcerated lip IHs may be unable
to latch onto a nipple secondary to
severe pain, which can lead to
impaired feeding.103 Obstructive
airway IHs may complicate
breathing and swallowing, also
leading to impaired feeding.104 In FIGURE 11
A, The presence of multiple IHs in the “beard” distribution is associated with a higher likelihood of
a small case series in infants with
airway involvement (reproduced with permission from J Pediatr. 1997;131(4):643–646 ©Elsevier).106
complicated facial IHs, several with B and C, Patient with airway involvement requiring tracheotomy is shown with “beard” involvement
ulcerated perioral lesions or airway at the lip and chin (B) as well as the parotid area and neck (C).
Downloaded from www.aappublications.org/news by guest on October 23, 2021
PEDIATRICS Volume 136, number 4, October 2015 e1069having associated airway compromise usually improves with anomalies. The best-known such
involvement; in a recent series in treatment of both the heart failure association is PHACE (Online
17 infants with airway IHs, bilateral and the IH. Mendelian Inheritance in Man
involvement of the lower facial Diffuse lesions of the liver may also 606519).114 The disorder is also
segment was present in 13 be associated with severe referred to as PHACES to include
(76%).106,108 Early referral to consumptive hypothyroidism caused potential ventral midline defects,
otolaryngology of infants with severe by excess production of type 3 specifically Sternal cleft and/ or
stridor and a cutaneous IH in the iodothyronine deiodinase. Liver IHs Supraumbilical raphe. Originally
“beard” distribution is advisable, are discussed in greater detail in the described as a “syndrome,” PHACE is
because airway involvement can be subsection entitled “Liver” of “IHs more appropriately termed an
life-threatening if diagnosis and With Special Anatomic Concerns.” association, although there are recent
treatment are delayed. In less data suggesting that chromosomal
symptomatic children, a high region 7q33 may provide a genetic
kilovoltage radiograph of the airway susceptibility to exhibit the PHACE
Highlights of This Section
may be useful in identifying phenotype.115
subglottic IH. Airway IHs are • Segmental IHs are far more
The spectrum of anomalies in PHACE
discussed in greater detail in the likely than focal IHs to result
syndrome and the ipsilateral
subsection under “IHs With Special in a complication, usually
relationship between such anomalies
Anatomic Concerns” entitled ulceration.
and cutaneous IH strongly suggest
“Airway.” • Focal IHs cause complica- a “developmental field defect,”
tions primarily by virtue of whereby an insult at a critical time in
Visual Impairment and Other Ocular their location on or near vi-
Complications embryogenesis gives rise to similar
tal structures.
developmental outcomes.116 The
IHs occurring within the orbit have the • Facial IHs cause complica- precise timing of such an insult in
potential to cause mechanical ptosis, tions more frequently than PHACE syndrome is speculative, but
strabismus, anisometropia, or nonfacial IHs and are several both the anatomic IH patterns and
astigmatism, which can quickly lead to times more likely to receive several of the associated structural
the development of amblyopia.108 some form of therapy. abnormalities point to changes early
Studies have identified specific
• Minor bleeding from an during the first trimester, probably
characteristics of periocular IHs, which
ulcerated IH is common, but within the first 3 to 12 weeks of
place the child at higher risk of
rarely of clinical significance; gestation before or during early
amblyopia. These include periocular
bleeding from a non- vasculogenesis.117 PHACE syndrome
IHs that are larger than 1 cm in
ulcerated IH is rare. is now understood to be
diameter, nasal location of the IH,
associated ptosis, eyelid margin • Patients with an extensive predominantly a congenital
change, or displacement of the IH in the “beard” distribu- vasculopathy. In fact, many of its
tion are more likely to have features can be explained as
globe.109–111 Orbital IHs are discussed
involvement of the airway. downstream events of arteriopathy
in greater detail in the subsection
• High-risk periocular IHs are with resultant ischemia, and it has
entitled “Eye and Orbit” under “IHs
With Special Anatomic Concerns.” those that are that are larger been hypothesized that vascular
than 1 cm in diameter, lo- dysplasia may be a key or even
Congestive Heart Failure and cated near the nose, associ- primary event in the pathogenesis of
Hypothyroidism ated with ptosis or eyelid PHACE syndrome.118
Although rare, high-output congestive margin change, or displacing Consensus criteria were recently
heart failure can occur in infants with the globe. developed for the diagnosis of PHACE
large IHs as a result of arteriovenous • Diffuse IH of the liver may syndrome (Tables 2 and 3).25 Clinical
shunting of a large blood volume be associated with severe examination of the skin and eyes as
through the lesion. This complication consumptive well as detailed imaging of the head,
has been reported in infants with hypothyroidism. neck, and chest are required to make
large cutaneous IHs and RICHs and in the diagnosis. More than 90% of
those with diffuse or multifocal infants with PHACE syndrome exhibit
hepatic IHs.91,92,112,113 Symptomatic more than 1 extracutaneous anomaly,
infants may present with difficulty IH Syndromes and Associations although very few manifest the
feeding, poor growth, heart murmur, A small subset of children with IH will complete spectrum.119 In contrast to
or hepatomegaly. The cardiac exhibit associated congenital nonsyndromic IH, PHACE syndrome
Downloaded from www.aappublications.org/news by guest on October 23, 2021
e1070 FROM THE AMERICAN ACADEMY OF PEDIATRICSTABLE 2 Consensus Algorithm for the Diagnosis of PHACE Syndrome is more common in full-term
PHACE Syndrome Possible PHACE Syndrome singleton infants of normal birth
Facial hemangioma Facial hemangioma Hemangioma of the No hemangioma plus
weight, although females are still
.5 cm in diameter .5 cm in diameter neck or upper 2 major criteria more commonly affected.120
plus 1 major criterion plus 1 minor torso plus 1 major
The hallmark of PHACE syndrome is
or 2 minor criteria criterion criterion or 2
minor criteria a large, segmental, often superficial
Adapted from ref 25.
IH, characteristically located on the
face, scalp, and/or neck (Fig 12).
PHACE syndrome–associated IHs
most commonly affect facial segments
1 and/or 3, which also confers a
particularly high risk of associated
central nervous system
TABLE 3 Consensus Diagnostic Criteria for PHACE Syndrome involvement.84,119
Organ System Major Criteria Minor Criteria
PHACE syndrome is not exceedingly
Cerebrovascular Anomaly of major cerebral arteries Persistent embryonic artery other rare, and probably even more
Dysplasiaa of the large than trigeminal artery
common than Sturge-Weber
cerebral arteriesb Proatlantal intersegmental
Arterial stenosis or occlusion artery (types 1 and 2) syndrome. 121 The segmental IH
with or without moyamoya Primitive hypoglossal artery associated with PHACE is
collaterals Primitive otic artery sometimes confused with the port
Absence or moderate-severe wine stain associated with Sturge-
hypoplasia of the large
Weber syndrome, especially in the
cerebral arteries
Aberrant origin or course of newborn period before significant
the large cerebral arteriesb IH proliferation or in cases of
Persistent trigeminal artery “minimal growth” IH in which there
Saccular aneurysms of any is an absence of significant
cerebral arteries
proliferation. The risk of PHACE
Structural brain Posterior fossa anomaly Enhancing extraaxial lesion with syndrome in an infant presenting
Dandy-Walker complex or features consistent with with a large, segmental IH ($22 cm2)
unilateral/bilateral cerebellar intracranial hemangioma
of the head or neck is approximately
hypoplasia/dysplasia Midline anomalyc
Neuronal migration disorderd one-third.120
Cardiovascular Aortic arch anomaly Ventricular septal defect Cerebrovascular anomalies, present
Coarctation of aorta Right aortic arch (double aortic arch) in more than 90% of patients, are the
Dysplasiaa most common extracutaneous feature
Aneurysm of PHACE syndrome, followed by
Aberrant origin of the subclavian
cardiac anomalies (67%) and
artery with or without a
vascular ring structural brain anomalies (52%).84
The most common arterial
Ocular Posterior segment abnormality Anterior segment abnormality abnormality in PHACE syndrome is
Persistent hyperplastic Microphthalmia
primary vitreous Sclerocornea
dysgenesis of the anterior circulation,
Persistent fetal vasculature Coloboma particularly within the internal
Retinal vascular anomalies Cataracts carotid artery.119 The neuroanatomic
Morning glory disc anomaly and cerebrovascular anomalies
Optic nerve hypoplasia observed in PHACE may lead to
Coloboma
Peripapillary staphyloma
a number of neurologic sequelae,
including motor and speech delays,
Ventral or midline Sternal defect Hypopituitarism seizures, migraine-like headaches,
Sternal cleft Ectopic thyroid
and rarely, arterial ischemic
Supraumbilical raphe
Sternal defects stroke.121 Hearing loss (conductive or
Adapted from ref 25. sensorineural) has also been reported
a Includes kinking, looping, tortuosity, and/or dolichoectasia. in PHACE syndrome, particularly
b Internal carotid artery, middle cerebral artery, anterior cerebral artery, posterior cerebral artery, or vertebrobasilar
when the IH involves the ear and
system
c Callosal agenesis or dysgenesis, septum pellucidum agenesis, pituitary malformation, or pituitary ectopia. periauricular scalp, which can be
d Polymicrogyria, cortical dysplasia, or gray matter heterotopia. related to the presence of ipsilateral
Downloaded from www.aappublications.org/news by guest on October 23, 2021
PEDIATRICS Volume 136, number 4, October 2015 e1071to be segmental and often “minimal
growth” in morphology.85 Such IHs
were often extensive (eg, involving the
entire leg) and showed additional
potential for ulceration and, rarely,
underdevelopment of the affected limb.
Like PHACE syndrome, the cutaneous
IHs and underlying anomalies showed
regional correlation. Myelopathies,
particularly spinal dysraphism, were
the most common extracutaneous
anomaly. Interestingly, arterial
anomalies were noted in a minority of
patients who were specifically studied
FIGURE 12
A, Frontotemporal segmental IH typical of PHACE syndrome. B, Sternal clefting characteristic of for such anomalies, although the true
PHACE syndrome (scar is congenital, not surgical). incidence and long-term risks are
unknown. Imaging is region-specific;
intracranial IH involving auditory risk infants, progressive
MRI is useful in delineating the extent
structures. It has been suggested that cerebrovascular changes may be
of lumbosacral involvement and
children with PHACE syndrome and identified early, and neurosurgical
potential myelopathy, whereas
periauricular IH be evaluated with revascularization procedures can be
additional imaging with MRA may be
both MRI and audiometric testing.122 performed to potentially reduce arterial warranted for infants with extensive
Cardiovascular anomalies are the ischemic stroke–related morbidity and lower limb involvement to assess for
second most common extracutaneous mortality.125 The presence of severe arterial anomalies.
manifestation of PHACE syndrome. The cerebrovascular and/or cardiovascular
aortic coarctation observed differs from arterial anomalies in patients with
classic coarctation in that it occurs in PHACE syndrome may preclude the use
Highlights of This Section
a more proximal location, often of propranolol for treatment of IH in
this population, or require dose • PHACE syndrome includes
involves the arteries feeding the upper
modification. (see section entitled features of Posterior fossa
extremities, and affects longer
“Medical Therapy for IH”). defects, Hemangiomas, cere-
segments, which may preclude
brovascular Arterial anoma-
detection based on a blood pressure LUMBAR syndrome (Lower body IH lies, Cardiovascular
gradient between the upper and lower and other cutaneous defects, Urogenital anomalies including co-
extremities. The aortic anomalies in anomalies and ulceration, Myelopathy, arctation of the aorta, and
PHACE syndrome are often noted to be Bony deformities, Anorectal Eye anomalies.
particularly unusual and severe, often malformations and arterial anomalies,
requiring surgical repair; thus, detailed • The hallmark of PHACE
and Renal anomalies) may be best
imaging of the arch is essential.123 syndrome is a large, seg-
considered the “lower half of the body”
mental IH, characteristically
Even in asymptomatic infants, MRI or variant of PHACE syndrome.85 located on the face, scalp,
magnetic resonance angiography LUMBAR has also been previously and/or neck.
(MRA) of the head and neck is described under the competing
indicated, especially given the known acronyms SACRAL87 (Spinal • The most common extra-
potential for progressive vasculopathy dysraphism, Anogenital anomalies, cutaneous features of PHACE
and resultant ischemic events in a small Cutaneous anomalies, Renal and syndrome are cerebrovascu-
subset of severely affected patients.124 urologic anomalies, associated with lar anomalies, followed by
Arterial ischemic stroke, a rare but Angioma of Lumbosacral localization) cardiac anomalies and
devastating complication, appears to be and PELVIS86 (Perineal hemangioma, structural brain anomalies.
more likely in patients with PHACE External genitalia malformations, • LUMBAR syndrome may be
who exhibit significant narrowing or Lipomyelomeningocele, Vesicorenal best considered the “lower
nonvisualization of large cerebral abnormalities, Imperforate anus, Skin half of the body” variant of
arteries, especially when more than 1 tag). The IHs are usually segmental PHACE syndrome and may
vessel is involved and/or if there are lumbosacral or anogenital lesions. In an be associated with urogeni-
associated cardiovascular morbidities analysis of 24 new patients and tal, anal, skeletal, and spinal
such as coarctation of the aorta.125 a review of 29 published cases, IHs in cord anomalies.
Through serial neuroimaging of high- association with LUMBAR were noted
Downloaded from www.aappublications.org/news by guest on October 23, 2021
e1072 FROM THE AMERICAN ACADEMY OF PEDIATRICSYou can also read

















































