CONFERENCE PROGRAMME AUSTRALASIAN SOCIETY FOR THE STUDY OF BRAIN IMPAIRMENT NEW ZEALAND REHABILITATION ASSOCIATION - and Shed 6, Queens Wharf ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
AUSTRALASIAN SOCIETY FOR THE STUDY OF BRAIN
IMPAIRMENT
and
NEW ZEALAND REHABILITATION ASSOCIATION
CONFERENCE PROGRAMME
Shed 6, Queens Wharf, Jervois Quay
Wellington, New Zealand
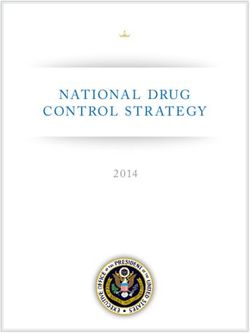
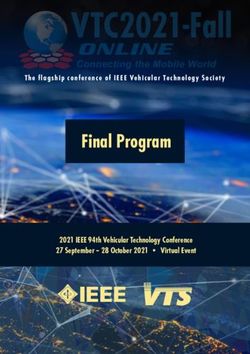
2nd – 4th May 2019Plan of Shed 6
Room 4
Room 1
Room 2 Room 3 Posters
Prep Room
Posters Reg Desk
Room 1 Room 3
Workshops 1 and 3 Concurrent Sessions 3, 6, 8, 11, 14, 17
Talk by Dr Shankar Sankaran NZRA AGM
Plenary 1, 2, 3, 6
Concurrent Sessions 1, 4, 9, 12, 15 Room 4
Awards and Conference Close
Morning tea
Room 2 Lunch
Afternoon Tea
Workshops 2 and 4 Datablitz Posters
Concurrent Sessions 2, 5, 7, 10, 13, 16
ASSBI Executive Meeting Prep Room
ASSBI AGM Speakers preparation room, access via Room 4
Student Workshop
Arcade Exhibitors in Arcade
Posters Accident Compensation Corporation (ACC)
Registration Desk Australasian Society for the Study of Brain
Toilets Impairment (ASSBI)
Exhibitors – in Room 4
Drake Medox ABI Rehabilitation NZ
Centre for Person Centred Research Medilink Australia
Rehabilitation Teaching and Research Unit Laura Fergusson New ZealandConnecting and Collaborating in Rehabilitation
THURSDAY 2nd May
8.00-9.00 Registration at Registration Desk
9.00 – 4.00 Workshops
9.00-12.00 Workshop 1 9.00-12.00 Workshop 2
Venue: Room 1 Venue: Room 2
Chair: Nicola Kayes Chair: William Levack
Prof Fiona Jones Prof Fary Khan and Dr Bhasker Amatya
Integrating self-management support in a brain Neurorehabilitation Research - All you need to know
injury service: lessons learnt and secrets of success to start
Fiona is brought to you by Drake Medox This workshop is brought to you by Laura Fergusson
New Zealand
10.30-10.45 Morning Tea
12.00-1.00 Lunch for delegates attending TWO workshops
12.30-1.00 Registration at Registration Desk
1.00-4.00 Workshop 3 1.00-4.00 Workshop 4
Venue: Room 1 Venue: Room 2
Chair: Jonathan Armstrong Chair: Andrew Clarkson
Prof Jonathan Evans Dr Matire Harwood
Rehabilitation of memory and executive functions Rehabilitation research and service development:
after brain injury meeting the rights of Indigenous people
2.30-2.45 Afternoon Tea
4.00 Workshops CLOSE
4.15 – 6.00 ASSBI Executive Meeting- Room 2
6.30: Mihi whakatau/welcome from mana whenua (the people of Te Whanganui-a-Tara/Wellington)
7.00: Dr Shankar Sankaran, Consultant Geriatrician: ACC Falls prevention & recognition of concussion
7.30-9.30 Welcome Reception in the Arcade and Room 4FRIDAY 3rd May
7.00 – 8.30 Put Posters up
8.30 –10.45 PLENARY 1
Venue: Room 1
Chair: William Levack
8.30 – 8.45 Welcome – William Levack
8.45 – 9.45 International Keynote Speaker: Fiona Jones
‘Feeling less alone’: co-producing self-management support following traumatic brain injury
9.45 – 10.30 Panel Discussion: Run by William Upscaling rehabilitation: policy, practice, and politics
Speakers: Dr Kathie Irwin – Head of Maori and Cultural Capability, ACC; Anne Hawker – Principal
Disability Adviser, Ministry of Social Development and Prof Katherine McPherson – Chief
Executive, Health Research Council of New Zealand
Fiona is brought to you by Drake Medox and Kathie is brought to you by ACC
10.30 – 11.00 Morning Tea
11.00 – 12.30 CONCURRENT SESSIONS 1 – 3
Session 1: 90 minutes Session 2: 90 minutes Session 3: 90 minutes
Venue: Room 1 Venue: Room 2 Venue: Room 3
Chair: Rachelle Martin Chair: Suzie Mudge Chair: Felicity Bright
Focus on family Emotions and cognition Understanding experiences of
recovery
11.00 Penny Analytis 11.00 Skye McDonald 11.00 Lee Cubis
The Experience of Attending a What causes impaired empathy Use of social identity mapping to
Camp for Families with a Child after traumatic brain injury? understand the impact of brain
with Acquired Brain Injury: Trialing an emotional Stroop task tumour on social groups and
Perspectives of Young People with 11.15 Barbra Zupan identity: A qualitative study
Acquired Brain Injury and Siblings What is the relationship between 11.15 Tenelle Hodson
11.15 Margaret Pozzebon empathic responses and emotion A journey of ambiguity – The
The spousal experience of Primary recognition following brain injury? healthcare experiences of people
Progressive Aphasia 11.30 Michelle Kelly with mild stroke
11.30 Libby Callaway Changes in social and emotional 11.30 Kate O’Reilly
Family and Traumatic Brain Injury: functioning in the early stages of Tarnished Dreams - Australian
An Investigation using the Family dementia women’s experience of traumatic
Outcome Measure 11.45 Rachael Rietdijk brain injury
11.45 Nic Ward Self-reported quality of life 11.45 Kate D’Cruz
Meeting Unmet Needs: Education outcomes after in-person and Humanising healthcare:
and Support for Adult Family telehealth social communication understanding the potential of
Members of Individuals with Brain skills training for people with narrative storytelling
Injury traumatic brain injury 12.00 Margaret Mealings. The
12.00 Emily Trimmer 12.00 Anneli Cassel student journey: Living and
Carers’ Way Ahead: A resource for Protocol, process, and progress on learning following traumatic brain
families caring for someone with a feasibility RCT targeting social injury
brain injury cognitive impairments after 12.15 Ronelle Hewetson
12.15 Narelle Higson acquired brain injury Exploring social network
Taking Action to Support Sexual 12.15 Jennie Ponsford maintenance and quality of life in
Expression Using a Team Cognitive Reserve and age predict people with social cognition
Approach: The Recognition Model cognitive recovery following TBI impairment post right hemisphere
stroke
12.30 – 1.45 Lunch
12.30 – 1.45 Room 2: ASSBI AGM & Room 3: NZRA AGM1.45 – 3.15 CONCURRENT SESSIONS 4 – 6
Session 4: 90 mins Session 5: 90 mins Session 6: 90 mins
Venue: Room 1 Venue: Room 2 Venue: Room 3
Chair: Jonathan Armstrong Chair: Debbie Snell Chair: Janet Wagland
Knowledge translation in Culture & equity Service delivery in rehabilitation
rehabilitation
1.45 Dana Wong 1.45 Ngawairongoa Herewini 1.45 Suzanne Barker-Collo
Evaluating the impact of the Maori cultural support: A unique Stroke and Traumatic Brain Injury
BRAINSPaN clinician and role within brain rehabilitation in New Zealand: Contrasting
researcher network on 2.00 Beth Armstrong incidence, and mood functioning
multidisciplinary collaboration and Aboriginal Australian experiences across two epidemiological studies
knowledge translation in the brain of brain injury and ways forward in 2.00 Lynne Turner-Stokes
impairment field culturally secure rehabilitation Estimated life-time savings in the
2.00 Elisa Lavelle Wijohn 2.15 Natalie Ciccone cost of on-going care following
Community–Academic Partnership Yarning together: Developing a specialist rehabilitation for severe
as an effective methodology for culturally secure rehabilitation traumatic brain injury (TBI) in the
research which can benefit approach for Aboriginal UK
participants, contribute to Australians after brain injury 2.15 Areti Kennedy
knowledge and impact policy 2.30 Frances Simmonds Preliminary Evidence from Action:
2.15 William Levack Does New Zealand’s geographical First year outcomes of the
Almost 1 in 10 Cochrane reviews and cultural challenges impact Acquired Brain Injury Transitional
are on rehabilitation patient access to inpatient Rehabilitation Service Pilot Project
interventions: findings from a rehabilitation services – a study 2.30 Kate Gould
Cochrane Rehabilitation review using five years of AROC data Hoarding and ABI: An overview
‘tagging’ project and Case Study
2:30 Laura De Lacy Datablitz 2.45 Jacinta Douglas
Using knowledge translation to 2.45 Saravana Kumar Enabling Hospitals to be more
develop a sensory modulation Meeting the needs of people who Inclusive and Responsive to People
pathway within acquired brain have sustained very serious with Cognitive Disabilities
injury rehabilitation lifelong injuries in South Australia: 3.00 Nicola Kayes
2.45 Christine Cummins A multi-method research project Measuring connection and
Creating opportunities for (DB1) collaboration in rehabilitation:
knowledge brokers to capitalise on 2.50 Emma Finch developing a measure of
the relational aspects of Exploring the unmet needs of therapeutic relationship
knowledge translation minor stroke survivors (DB2)
3.00 Jean Hay-Smith 2.55 Rebecca Andrews
From systematic review of Supporting persons with ABI and
rehabilitation exercise to clinical communication impairment to
practice: a knowledge translation access the legal system: A case
‘call to action’ study review (DB3)
3.00 Katie Hodge
Long-term follow-up of moderate-
to-severe traumatic brain injury in
the Canterbury region (DB4)
3.05 Danielle Sansonetti
Early intervention for social skills
impairment following acquired
brain injury: Promoting self-
awareness to optimise community
integration (DB5)
3.10 Elizabeth Beadle
Gaps in occupational participation
following severe TBI: associations
with cognition, mood, and
psychosocial function (DB6)3.15 – 3.45 Poster Session 1 and Afternoon Tea
3.45 – 5.00 PLENARY 2
Venue: Room 1
Chair: Jacinta Douglas
3.45 – 4.15 National Keynote Speaker: Prof Fary Khan
Fatigue Management in Neurorehabilitation
4.15 – 4.30 Dr Alison Drewry (brought to you by ACC)
Reducing the incidence and impact of brain injury in New Zealand
4.30 – 4.40 Information on the 2020 Conference in Perth
4.40 – 4.50 ASSBI Fellowship presentation
4.50 – 5.20 ASSBI Presidential Address: Prof Robyn Tate
Measuring outcomes and monitoring progress in the era of evidence-based clinical practice
5.30 – 6.30 Brain Impairment Editorial Board Meeting – Room 2
5.30 – 7.00 Student Networking Drinks – Mac’s Brewbar, 4 Taranaki St
7.15 Conference Dinner - Cable Room, Harbourside Function Venue, 4 Taranaki StPoster
# Name Title
Young People’s Experience of the Sibling Relationship When One Sibling
1 Analytis, Penny Has an Acquired Brain Injury
Concussion Essentials: Piloting a clinical trial to reduce persisting
2 Anderson, Vicki symptoms following child concussion
Support for Community Integration after Brain Injury within New
3 Armstrong, Jonathan Zealand Health Policy
Combined rehabilitation and glycosominoglycan treatment improves
4 Barwick, Deanna forelimb function following motor cortex stroke in mice
Standardising the Management of Behaviours of Concern in the Acute
5 Block, Heather Phase of Traumatic Brain Injury
A Systematic Review of the Evidence Relating the Management of
6 Block, Heather Behaviours of Concern in Acute Traumatic Brain Injury
The complexities of enacting person-centred practice in stroke
7 Bright, Felicity rehabilitation
Review and selection of outcome measurement within a complex model
8 Brosnan, Nicky of neurodisability provision
9 Brunner, Melissa What’s it like to use Twitter after a Traumatic Brain Injury?
A New Innovation: The Benefits of the Aphasia New Zealand
(AphasiaNZ) Charitable Trust’s Community Aphasia Advisor (CAA)
10 Castle, Emma Service
Intervening to improve quality of life several years after traumatic brain
11 Caukill, Kathryn injury
More than meets the eyes: Cerebellar white matter changes and
12 Chen, Yu contributions to cognitive dysfunction in frontotemporal dementia
An economic evaluation of constraint-induced movement therapy
13 Christie, Lauren implementation: The ACTIveARM Project
Environmental enrichment following prefrontal cortex stroke: good or
14 Clarkson, Andrew bad?
Evaluating a falls reduction intervention in older persons’ inpatient
15 Dickie, Benn rehabilitation: does it work in a new context?
Clinical Perspectives on Training and Delivering a Positive Behaviour
Support Intervention for People with Acquired Brain Injury: A
16 Gould, Kate Qualitative Study
Post-traumatic Parkinsonism following severe traumatic brain injury: A
17 Gozdzikowska, Kristin case report
Physical outcomes for people admitted to an adult Brain Injury
18 Hassett, Leanne Rehabilitation Unit: a cohort study
“I just let it ring now”: Maintaining friends after a right hemisphere
19 Hewetson, Ronelle stroke
20 Kumfor, Fiona Prevalence and neurocognitive basis of delusions in dementia
Development of an English-language version of a Japanese iPad
application to enhance person-centred goal setting in rehabilitation –
21 Levack, William with implications for indigenous communities
22 Lister, Helena The future of bariatric Care in TBI: Can we cope with the load?SATURDAY 4th May
7.00 – 9.00 Put Posters up
7.30-8.30 Breakfast “How to”: Sessions 7 – 8
Session 7: 60 mins Session 8: 60 mins
Venue: Room 2 Venue: Room 3
Chair: Jenny Fleming Chair: Libby Callaway
Lynne Turner-Stokes Libby Callaway
How to set structured goals for management of Identifying and mitigating risks when providing
patients on Prolonged Disorders of Consciousness therapy services to people with Acquired Brain Injury
(PDOC) in the National Disability Insurance Scheme
9.00 – 10.30 PLENARY 3
Venue: Room 1
Chair: Nicola Kayes
9.00 – 10.00 International Keynote Speaker: Jonathan Evans
Music, mindfulness and positive psychotherapy after brain injury
10.00-10.30 National Keynote Speaker: Matire Harwood
Mana Tū: Indigenous people ‘taking charge’ of living with long term conditions
10.30 – 11.00 Poster Session 2 and Morning Tea
11.00 – 12.30 CONCURRENT SESSIONS 9 – 11
Session 9: 90 mins Session 10: 90 mins Session 11: 90 mins
Venue: Room 1 Venue: Room 2 Venue: Room 3
Chair: Jean Hay-Smith Chair: Dana Wong Chair: Leanne Togher
Paediatric rehabilitation Technology in rehabilitation Communication
11.00 Sarah Badger 11.00 Leanne Hassett 11.00 Kellie Stagg
Short term outcomes of children Patient reported outcomes of Communication impairment and
with abusive head trauma two- usability and enjoyment of using the working alliance in stroke
years post-injury: A retrospective digital devices in rehabilitation as rehabilitation
review part of the AMOUNT (Activity and 11.15 Joanne Steel
11.15 MObility UsiNg Technology) Social communication assessment
randomised controlled trial for clinical practice: A review of
11.30 Therese Mulligan 11.15 Tamara Ownsworth innovative standardised tools and
‘You only get one brain’: An Perspectives on the use of discourse assessment methods
exploratory retrospective study on telerehabilitation for delivering 11.30 Elise Elbourn
life after adolescent traumatic community-based support to Recommendations to support
brain injury individuals with an acquired brain cognitive-communication recovery
11.45 Owen Lloyd injury during subacute and early
Impaired Self-Awareness after 11.30 Renerus Stolwyk community rehabilitation
Paediatric Traumatic Brain Injury: Utilising telehealth to deliver following severe Traumatic Brain
Liability or Protective Factor? neuropsychological rehabilitation Injury (TBI)
12.00 Jesse Shapiro services to rural patients with 11.45 Anna Copley
No diffusion imaging correlate of stroke: development and Remediation of cognitive-
paediatric post-concussion evaluation of a novel pilot communication disorders following
syndrome: a TBSS study program acquired brain injury using
12.15 Rachelle Martin 11.45 Vanessa Rausa telerehabilitation: A pilot study
Using a single-case experimental Delivering concussion evidence to
design to evaluate the the community: A digital solution Datablitz
effectiveness of therapeutic horse 12.00 Robyn Gibson
riding for children and young Datablitz What do SLTs think about aphasia
people experiencing disability 12.00 Melissa Brunner therapy? (DB13)
What Role does Social Media have 12.05 Salma Charania
in Rehabilitation after a Traumatic The Lived Experience of
Brain Injury? (DB7) Communication Changes Caused12.05 Duncan Babbage by MND in People with MND and
Person Centred Approaches to their Family and Friends: A Scoping
Future Technology for Review (DB14)
Rehabilitation (DB8) 12.10 Elise Elbourn
12.10 Lucy Arthur Objective clinical methods for
The Application of Wearable evaluating the severity of
Technology to Guide Therapy and discourse disorders and predicting
to Refine Interpretation of Non- psychosocial outcomes following
verbal Communication in a Non- severe Traumatic Brain Injury (TBI)
speaking client Illustrated by a (DB15)
case study: James (DB9) 12.15 Brooke-Mai Whelan
12.15 Vanessa Rausa Telerehabilitation and acquired
Development of a Concussion brain injury (ABI): An online high-
Digital Health Tool: HeadCheck intensity behavioural speech
(DB10) intervention using real-time
12.20 Di Winkler videoconferencing and store and
Integrated apartments for people forward functionality (DB16)
with disability: Individual 12.20 Nikki-Anne Wilson
experience and outcomes (DB11) Social Simulation: A Cognitive
12.25 Elizabeth Beadle Mechanism Associated with
The integration of telehealth in to Impaired Social Knowledge in the
a community based Behavioural-Variant of
interdisciplinary brain injury Frontotemporal Dementia (DB17)
service (DB12) 12.25 Crystal Kelly
Managing adults with cognitive-
communication disorders following
traumatic brain injury in
community settings across
Australia and New Zealand (DB18)
12.30 – 1.45 Lunch
12.45-1.40
Venue: Room 2
An informal lunchtime workshop for students entitled Utilising Positive Behaviour Support (PBS) to help
people improve quality of life and self-regulate behaviour after acquired brain injury (ABI).
Chair: Student Co-ordinator
Speaker: Dr Kate Gould (Clinical Neuropsychologist & Research Fellow)
Guest Speakers:
1.45 – 2.45 CONCURRENT SESSIONS 12 – 14
How to Session 12: 60mins How to Session 13: 60mins How to Session 14: 60mins
Venue: Room 1 Venue: Room 2 Venue: Room 3
Chair: Lucy Knox Chair: Debbie Snell Chair: Felicity Bright
1.45 Cathy Bucolo 1.45 Elizabeth Pritchard, Caroline 1.45 Johnny Bourke, Joanne
Participant Led Videos: supporting Fisher and Toni Withiel Nunnerley and Hamish Ramsden
people with cognitive- Answering to the call for action How to build capacity for
communication changes following from practitioners in response to meaningful consumer engagement
acquired brain injury to ‘voice’ family violence: A ‘how to’ in rehabilitation research
their goals, express their needs workshop.
and desires in their own words and
lead the creation of a training
video for their support workers.
2.45 – 3.15 AFTERNOON TEA3.15 – 4.15 CONCURRENT SESSIONS 15 – 17
Session 15: 60 mins Session 16: 60 mins Session 17: 60 mins
Venue: Room 1 Venue: Room 2 Venue: Room 3
Chair: Jacinta Douglas Chair: Skye McDonald Chair: Jennie Ponsford
Collaborative approaches Intervention implementation Diverse perspectives
3.15 Di Winkler 3.15 Lauren Christie 3.15 Cynthia Honan
Co-design, pilot and evaluation of Implementation of constraint- Cognitive fatigue in chronic fatigue
participant led videos to train induced movement therapy in syndrome: Comparisons with
support workers public health: The ACTIveARM individuals with multiple sclerosis
3.30 Eleanor Jackson Project and healthy individuals
Peer support following traumatic 3.30 Jai Carmichael 3.30 Felicity Bright
brain injury: Efficacy and impact of Readiness of Community ABI Recalibrating hope in the year
client-led group programmes Therapists to Learn and Implement after stroke: A call to move beyond
3.45 Lucy Knox Positive Behaviour Support: A ‘realistic’ hope
“If there’s an official term called Mixed-Methods Study
supported decision making, I have 3.45 Matt Thomas Datablitz
no clue”: Experiences of CIRCuiTS cognitive remediation 3.45 Chelsea Nicol
community-based rehabilitation trial in Orange, NSW The impact of primary brain
professionals in supporting tumour on subjective cognitive
decision-making participation for Datablitz functioning and associations with
adults after ABI 4.00 Travis Wearne psychological distress (DB22)
4.00 Liz Williams Regulating emotion following 3.50
“I really try to plug into the traumatic brain injury: Results (DB23)
person”: Strategies used by from a repeated biofeedback 3.55 Lisa Rapport
clinicians to build and nurture the treatment study (DB19) Selection Bias Associated with
therapeutic alliance in community 4.05 Elly Williams Eyetracking Research in Traumatic
brain injury rehabilitation Community rehabilitation: Brain Injury (DB24)
Increasing independence 4.00 Kerrin Watter
regardless of time since acquired Early intervention for cognitive-
brain injury (DB20) communication reading
4.10 Deborah Snell comprehension deficits after ABI:
‘Listening in’ for uncertainty during initial results (DB25)
recovery from mild traumatic brain 4.05 Freyr Patterson
injury: a mixed methods study Interactions during occupational
(DB21) therapy brain injury rehabilitation
groups: a descriptive video
analysis (DB26)
4.15 – 5.00 AWARDS AND CONFERENCE CLOSE
Venue: Room 1
Chair Robyn Tate
4.15 – 4.30 Thanks to Convenor, Committees and Sponsors
4.30 – 5.30 ASSBI Early Career Clinical Innovation Award
ASSBI Douglas Tate Award
ASSBI Student Awards
Kevin Walsh Award
Luria Award
Travel Award
NZRA Student Awards
Mindlink Brightwater
Award for Interdisciplinary PresentationPoster
# Name Title
A longitudinal investigation of dysarthria recovery over two years
1 Lu, Sheree following severe traumatic brain injury
Theoretical model development explaining how peer support
improves health outcomes for people with spinal cord impairment: a
2 Martin, Rachelle realist approach
Positive participation, therapeutic landscapes and personal agency
as active ingredients in rehabilitation interventions: therapeutic
3 Martin, Rachelle horse riding as an example
Improving functional independence and quality of life for clients with
an acquired brain injury undergoing community rehabilitation using
4 Martini, Angelita assistive devices for toileting
Early Action Appraised: Stakeholders’ perspectives on early pilot ABI
5 Nielsen, Mandy transitional rehabilitation in Queensland, Australia
Developing a Video Resource for Pressure Injury Prevention
6 Nunnerley, Joanne Education in Spinal Cord Injury
7 Ricciardi, Manjula Spasticity Management: Challenge and Experience
Application of generalisation principles in rehabilitation following
8 Sansonetti, Danielle brain injury
9 Shendyapina, Maria Stroke education as a part of rehabilitation process
Using CIRCuiTS cognitive remediation therapy to improve the
10 Thomas, Matt functioning of adults with schizophrenia
The Impact of Sleep and Fatigue on Social Cognition in Multiple
11 Turner, Jason Sclerosis
VanSolkema, Attention and communication following TBI: Making the connection
12 Maegan through a meta-narrative systematic review
VanSolkema, Hypoxic brain injury post-intensive rehabilitation: Are clients and
13 Maegan families ready for discharge?
A series of single-case experiments evaluating a novel massage
14 Verhagen, Heidie therapy for chronic lower back pain
Interdisciplinary goal planning in early rehabilitation: Exploring
15 Watter, Kerrin three different techniques
16 White, Brid Veterans Rehabilitation Strategy
17 Wiingaard, Signe Adjusting to changes in sense of self after traumatic brain injury
18 Williams, Katherine Dysphagia following moderate-to-severe traumatic brain injury
Establishing a framework to better understand and manage client
and families’ perception and expectation of recovery after an
Acquired Brain Injury within a community based residential
19 Yap, Adelene rehabilitation setting
20 Young, Tony TBI at ABI: Trends over the past three years
21 Young, Tony Visual care plans to enhance communication and efficiency
22 Young, Tony Enhancing early engagement for transitions to community
Zhavoronkova, Dual-tasking training improves cognitive functions in patients with
23 Ludmila mild traumatic brain injury
24 Zupan, Barbra Sex Differences in Emotional Self-Awareness and Emotional ClarityTHURSDAY ABSTRACTS conducting quantitative and/or qualitative
research, and acknowledging and incorporating
Workshop 1 values and preferences in clinical decision
making. The workshop will feature:
‘Integrating self-management support in a brain • Lectures from the experts: general issues in
injury service: lessons learnt and secrets of planning, executing, and evaluating research
success’ projects
Jones, Fiona1 • Interactive sessions, with free discussion
1
St George's University of London, London, UK including challenges and gaps in research in
rehabilitation settings
This workshop will explore what is meant by • Group activities and discussion in which
‘supported self-management’ in the context of participants will critically appraise papers,
integrating self-management support into a brain and develop case-based studies.
injury service. Using findings from recent projects Participants will receive critical appraisal tools
working across major trauma centres in London, and guidelines, examples of different types of
community and voluntary services attendees will studies (e.g. systematic reviews, RCTs,
critically reflect on the unifying components of observational studies), and useful links to
supported self-management and how they can background and additional readings. By the end
utilise key principles and best evidence in of this workshop the participants will have
everyday practice. learned how to:
• Formulate clear research questions
During the course of the workshop attendees will • Understand literature searching strategies
work together to explore ways to promote and be familiar with different resources
problem solving, facilitate self-discovery, goal (both primary and secondary database
setting, use of resources and create knowledge searches)
together about the best ways to support self- • Understand different study designs
management which is authentic and person (qualitative, quantitative)
centred. The workshop will also include • How to write an academic manuscript
examples of evaluating impact and sustaining a • Undertake critical appraisal of research
culture of self-management support within brain The workshop will be facilitated by Prof Fary
injury rehabilitation teams. Attendees will work Khan and Dr Bhasker Amatya, who have
together to create a shared understanding of the extensive experience in research in rehabilitation
secrets to success that can be implemented into settings (combined publication of over 400 peer-
their practice the next day. reviewed articles) and are practising/teaching
evidence-based practice and conducting research
Workshop 2 at sites across Australia and Asia.
Neurorehabilitation Research - All you need to Workshop 3
know to start
Khan, Fary1 and Amatya, Bhasker1 Rehabilitation of memory and executive
1
Department of Medicine (Royal Melbourne functions after brain injury
Hospital), The University of Melbourne, Evans, Jonathan1
Department of Rehabilitation Medicine and 1
University of Glasgow, UK
Australian Rehabilitation Research Centre, Royal
Melbourne Hospital, Parkville, VIC. Australia In this workshop Jon will update participants on
Workshop structure the evidence base for the rehabilitation of
This intensive and interactive workshop is memory and executive functions after brain
designed for healthcare professionals who wish injury. A particular focus will be on prospective
to develop their knowledge and skills in memory and goal management, which rely on
conducting research and in evidence-based the integration of memory, attention and
practice. Further, it will help participants to executive functions. Current developments in the
advance their skills in searching and critically use of reminding technology will be discussed
appraising the literature, designing and including ApplTree, a reminding app designedwith, and for, people with brain injury; fall, then taking action to get them the help &
interactive voice-based guidance, and the use of support they need. If an older person has
augmented reality. indicated they have had a slip, trip or fallen in the
At the end of this workshop participants will last year then they are potentially at risk of
• Be up-to-date on the current evidence having a (another) fall and will benefit from the
relating to the rehabilitation of memory and Live Strong for Longer programme.
executive deficits after brain injury. Further; falls are the leading cause of brain injury
• Understand how digital health technology in NZ; accounting 38% of all brain
may be used to assist memory and executive injury. Concussion is caused by a blow to the
functions in everyday life after brain injury head or body that could result in any shaking of
• Be aware of ongoing developments in the brain and a person does not have to be
technology that may assist memory and knocked out to be concussed. Early recognition
executive functioning in the future. and management is essential to minimise the
severity of the injury and decrease the risk of
Workshop 4 having prolonged symptoms. Keeping Older
people Independent & well living the life they
Rehabilitation research and service want to live – ultimate outcome.
development: meeting the rights of Indigenous
people’ FRIDAY ABSTRACTS
Harwood, Matire1
1
University of Auckland, New Zealand Plenary 1
Three outcomes for the workshop: ‘Feeling less alone’: co-producing self-
a. An understanding of the UN Declaration on management support following traumatic brain
the Rights of Indigenous peoples and its injury
application to rehabilitation services and Jones, Fiona1
research 1
St George's University of London, London, UK
b. Pathways to inequities
c. How to address the ‘Responsiveness to People with Acquired Brain Injury (ABI) can
Indigenous peoples’ question/s in business experience long-term cognitive, psychological,
case or funding applications emotional and social effects, frequently resulting
in ‘hidden disability’. Likewise, families navigate a
ACC Falls prevention & recognition of complex, changing situation that may include
concussion mood disturbances associated with their
Dr Shankar Sankaran relative’s injury and shifts in family relationships.
Consultant Geriatrician Self-management programmes have traditionally
been used for people with long-term chronic
NZ has a growing ageing population. With age the conditions and have shown impact on clinical,
risk of having a fall increases, those over 65 have psychological and social outcomes. There are
a 1 in 3 chance of having a fall and for those over challenges in providing self-management support
80 it’s 1 in 2, falls can be prevented. ACC, the for people with ABI and their families, which
Ministry of Health, Health Quality & Safety traditionally focus on behaviour change methods
Commission, DHBs, GPs, health professionals, and require cognitive abilities. The range of
home carers and community groups, all deliver complex issues experienced by people with ABI
services to older people. Working together we'll added to the perceptions of healthcare staff
better coordinate our efforts and create a system particularly in the acute settings, means that self-
that is easy to use and helps to reduce the management approaches which start early after
incidence and severity of falls and fractures. This injury are relatively rare.
approach has been the catalyst for the creation
of the Live Stronger for Longer movement the This keynote lecture will explore co-production
unifying brand that aims to unite the falls and methodology and a staged approach to co-
fracture system in NZ. Falls can be prevented by designing a new self-management approach.
identifying when an older person is at risk of a Using participatory methods we harnessed theknowledge, experiences, and power of a group of with ABI and their families from the perspective
14 people with ABI and their families and of young people with ABI and siblings.
developed a shared approach to self- Method: Semi-structured interviews were
management support across an acute conducted with seven young people with ABI and
neuroscience pathway. 110 staff in a major 11 siblings.
London trauma centre learned how to integrate Results: Using thematic analysis, four themes
self-management support strategies and patients were identified: Accepting ABI; Camp friendships;
with ABI and their families used new self- Personal mentoring; Escape from daily life.
management books. The co-designed books Participants experienced camp as an
embodied a person-centred approach to self- environment where ABI was understood and
management with stories, ideas and reflections accepted, and they felt relieved of the pressure
on life after ABI, and space for recording, hopes, to explain their family’s situation. This
targets, successes and strategies. The books had acceptance provided the background to camp
a ‘natural fit’ with patients and families and friendships and to having fun. By interacting with
provided staff with a shared mechanism to others in similar situations, participants felt they
implement self-management strategies within understood ABI better, and for some, this shaped
their everyday work. their values and future career choices. Whilst
There were clear benefits to taking part in a camp was viewed as an escape from daily life, for
process of authentic co-design and these will be some participants, negative experiences such as
discussed through the reflections of people with family conflict crept into the camp experience.
ABI, their families, healthcare staff and the project Conclusions: Condition-specific camps may
team. Finally, there will be a summary of lessons provide young people with ABI and siblings with
learnt and advice for those who seek to engage opportunities to better understand ABI and its
and involve people with ABI and their families in impact on the individual and the family. Camps
research and enhancing service provision. may also provide opportunities to have fun and
to make friends, providing a buffer against
Panel Discussion challenges faced by families with a child with ABI.
As such, camps may provide an important allied
Concurrent Session 1 health support service.
Correspondence: Penelope Analytis;
The Experience of Attending a Camp for Families penelope.analytis@monash.edu
with a Child with Acquired Brain Injury:
Perspectives of Young People with Acquired The spousal experience of Primary Progressive
Brain Injury and Siblings Aphasia
Analytis, Penelope1,2; Warren, Narelle3 and Pozzebon, Margaret1,2; Douglas, Jacinta1,3 and
Ponsford, Jennie1,2 Ames, David4
1
Monash-Epworth Rehabilitation Research
1
School of Allied Health, La Trobe University,
Centre, Monash University, Melbourne, Australia Melbourne, Australia
2
Monash Institute of Cognitive and Clinical
2
Speech Pathology Department, Royal Melbourne
Neurosciences, School of Psychological Sciences, Hospital, Melbourne, Australia
Monash University, Melbourne, Australia
3
Summer Foundation, Melbourne, Australia
3
School of Social Sciences, Faculty of Arts,
4
Academic Unit for Psychiatry of Old Age,
Monash University, Melbourne, Australia University of Melbourne, Melbourne, Australia
Background and Objectives: Paediatric acquired
brain injury (ABI) is associated with long-term Background and aims: Primary Progressive
negative sequelae, and families must continually Aphasia (PPA) is a neurocognitive-degenerative
adapt to meet the changing needs of the child disorder, characterised by early and ongoing
with ABI and family members. Interventions decline of language-communication-cognitive
which provide enriching educational abilities. Despite the pivotal role that spouses
opportunities, such as condition-specific camps, play in supporting their partner diagnosed with
may support families following ABI. This study PPA, little is known about how they deal with and
explored the experience of a camp for children face the challenges associated with this
progressive condition. The aim of this qualitativeresearch project was to gain an understanding of members and the relative with brain injury. This
the personal experiences of spouses living with study aimed to produce a profile (positive and
this condition. negative) of families supporting relatives with
Method: Thirteen spouses whose partners were traumatic brain injury (TBI) who experience high
diagnosed with PPA participated in 1:1 semi support needs.
structured, in-depth interviews to explore their Methods: A cross-sectional survey-based pilot
lived experiences of this illness. Using a study was undertaken with thirty-eight dyads.
constructivist grounded theory approach, Dyads consisted of a family member and relative
analysis moved through a process of data-driven with TBI and high daily support needs (median
open and focused coding, for the identification of Care and Needs Scale (CANS) score of 7,
emergent categories, themes and subthemes indicating near 24-hour per day care
that captured the lived experiences of spouses requirements). The survey examined
supporting partners with PPA. demographic and clinical characteristics of the
Results: A constructivist grounded theory relative with TBI and the family member; and the
analysis of the interview data revealed an CANS; Health of the Nation Outcome Scale–
overarching theme of ‘facing the challenges of Acquired Brain Injury; and Role Checklist for the
PPA’ that captured the overall experiences of person with TBI. Non-parametric bivariate
spouses. Four interdependent and overlapping analyses were conducted.
themes that sat within this overarching theme Results: Independence of the FOM-40 domains
included: acknowledging disconnect in the was confirmed. Place of residence (supported
spousal relationship, living the decline, re- accommodation/family home) was an important
adjusting sense of self, and getting on with living. predictor variable. Supported accommodation
Each of these core themes revealed how spouses was strongly associated with lower levels of
dealt with the ongoing and evolving challenges of burden reported in families. Family home was
PPA, particularly concerning changing relational strongly associated with better adjustment of the
dynamics with their partner and adjusting their relative with TBI. Family resilience was positively
own self-conceptualisation. associated with sustainability of support and
Conclusions: The findings highlight the comorbidity in the relative with TBI.
importance of addressing the relational Conclusions: Family outcomes were associated
consequences of PPA for spouses, specifically to with a variety of demographic and clinical
manage their changing emotional-relational characteristics of the relative with TBI including
connectivity within self, their partner and social residence, behaviour and mental health
world. symptoms. The results provide meaningful
Correspondence: Margaret Pozzebon; evidence for service providers given the
margaret.pozzebon@mh.org.au increasing investment in housing and support
options for people with disabilities, and the
Family and Traumatic Brain Injury: An ongoing reliance on families to provide informal
Investigation using the Family Outcome support after TBI.
Measure Correspondence: Christine Migliorini;
Migliorini, Christine1; Callaway, Libby1,2; Moore, christine.migliorini@monash.edu
Sophie1; and Simpson, Grahame K3,4
1
Department of Occupational Therapy, Monash Meeting Unmet Needs: Education and Support
University, Frankston, VIC, Australia for Adult Family Members of Individuals with
2
Neuroskills Pty Ltd, Sandringham, VIC, Australia Brain Injury
3
Brain Injury Rehabilitation Research Group, Ward, Nic1; Naidu, Nalita1; Palmer, Siobhan1 and
Ingham Institute of Applied Medical Research, Gozdzikowska, Kristin1
Sydney, NSW, Australia 1
Laura Fergusson Trust, Christchurch, New
4
Liverpool Brain Injury Rehabilitation Unit, Zealand
Sydney, NSW, Australia
Background and Objectives: Traumatic brain
Background and Objectives: The Family Outcome injury (TBI) has adverse, long-term impacts on
Measure (FOM-40) captures multidimensional not only survivors, but on family members as
data about wellbeing and capacity of family well. Family members often have criticalsupporting roles in the recovery process; individual with a brain injury and are often the
research has identified relationships between cause of increased stress and poor quality of life
family member well-being and survivor outcome. in both the person with brain injury and their
However, there is a gap in translating this families and social networks. Often access to
research to clinical practice due to limited intervention and support is limited for many
provision for funded interventions for family families, especially those living in rural areas. The
members. However, there has been a recent shift aim of this programme was to develop an easily
in policy with Accident Compensation accessible online resource for families to help
Corporation (ACC) TBI Strategy and Action Plan them understand and support their family
(2017 – 2021) stating clearly a goal “to improve member with challenging behaviours.
services that extend to whānau, taking a more Method: Eight family members of a person with
holistic approach.” brain injury completed the pilot trial of the
Method: Group programmes to educate and Carers’ Way Ahead programme. The programme
support adult family members were was developed by six clinicians and targets the
implemented over an 18-month period. This most common types of challenging behaviours
presentation will review the rationale, identified by family members in 7 modules.
intervention content, implementation process, Participants of the trial completed a number of
and pre-/post-outcome measures of these measures before and after completing the
services to date. programme and were also asked to provide
Results: Wilcoxon signed-rank test revealed a feedback on the feasibility and acceptability of
significant median decrease in self-ratings of the programme.
perceived stress following group intervention, as Results: Overall, feedback from families suggests
compared to pre-treatment self-ratings (z = - the programme “Carers’ Way Ahead” is both
2.070, p = 0.038). All participants reported they feasible and acceptable. All family members
would recommend the programme. Qualitative identified the need for support, especially those
data highlighted self-reported themes of in rural areas. Responses from families indicated
increased ability to cope, increased that an online programme is both easily
understanding of the individual with TBI, as well accessible and convenient to those with time
as benefits of peer-support. constraints.
Conclusions: Professionally-led family/whānau Conclusions: This project aims to address a
support and education appears integral for significant gap in resources for families trying to
individual and family systems’ optimal recovery manage challenging behaviour post brain injury.
and outcome after moderate to severe TBI. Correspondence: Emily Trimmer;
Understanding the importance of whānau emily.trimmer@gmail.com
contributions to recovery is also fundamental to
understanding Māori health and whānau ora, or Taking Action to Support Sexual Expression
supporting Māori families in collectively Using a Team Approach: The Recognition Model
achieving optimal wellbeing. Higson, Narelle1
Correspondence: Kristin Gozdzikowska; 1
Outside the Square OT Solutions, Perth, Western
Kristin@lftcant.co.nz Australia
Carers’ Way Ahead: A resource for families Although it is generally agreed among health care
caring for someone with brain injury professionals that engaging in activities related to
Trimmer, Emily1; McDonald, Skye1; Newby, Jill1; sexual expression may be an important part of
Grant, Samantha2; Gertler, Paul2 and Simpson, health and wellness for people of all ages,
Graham3 abilities and cultural backgrounds, there often
1
School of Psychology, University of New South remains a theory/practice when it comes to
Wales, Sydney, NSW, Australia addressing the area in rehabilitation and
2
Private practice community settings. Research suggests that
3
Ingham Institute of Applied Medical Research many healthcare workers do not feel adequately
equipped to address sexual concerns in a
Background: Challenging behaviours can have a competent, safe and supported manner.
major impact on family members caring for anThis presentation will outline the steps of The expression or a neutral face. Measures of
Recognition Model, a useful framework for team- empathy and emotion recognition were taken.
based practice published in 2010 by UK Results: People with TBI were slower than
occupational therapist Lorna Couldrick, which controls overall. They did, however, demonstrate
may be used to assist both individual a similar magnitude Stroop effect on incongruent
practitioners and health teams in a variety of trials. Stroop performance was not related to
work settings to positively support sexual emotion perception accuracy of self-reported
expression. The presentation will identify empathy.
potential challenges health conditions and Conclusion. This study found that rapid
disability may present to engaging in sexual conceptual processing of emotional faces was
expression, outline potential barriers to including preserved in people with TBI, despite
sexual expression in practice in a safe, respectful substantially slowed processing speed. There was
and inclusive way and identify practical strategies no evidence that this conceptual processing of
which may be used to assist in increasing emotional faces plays a role in the ability to
confidence, comfort and competence when recognise or to resonate with the emotions of
addressing this area. Resources and avenues of others after a TBI or in healthy controls.
support to foster further learning will also be Correspondence: Skye McDonald;
identified. s.mmcdonald@unsw.edu.au
Correspondence: Narelle Higson;
narelle@otsots.com.au What is the relationship between empathic
responses and emotion recognition following
Concurrent Session 2 brain injury?
Zupan, Barbra1 and Neumann, Dawn2
What causes impaired empathy after traumatic 1
Central Queensland University, Rockhampton,
brain injury: Trialling an Emotional Stroop Task Australia
McDonald, Skye1; Osborne-Crowley, Katie1; 2
Indiana University School of Medicine,
Wilson, Emily1; De Blasio, Frances; Wearne, Travis Department of Physical Medicine and
and Rushby, Jacqueline1 Rehabilitation, Indianapolis, United States
1
School of Psychology, UNSW, Sydney, Australia
Background and Objectives: Recognising
Background and Objectives: Emotional empathy emotions and empathising with others’ feelings
allows the observer to share, or ‘resonate’ with, contribute to positive psychosocial outcomes but
the emotional state of others. People with the relationship between them is not well
traumatic brain injury (TBI) often have a reduced understood. This study aimed to compare the
ability to resonate with the emotions of others association between emotion recognition and
but there is little research into the mechanisms empathic responses to film clips in people with
for this. The perception-action model (PAM) of and without TBI.
empathy proposes a mechanism whereby, when Method: 60 adults with moderate to severe TBI
an observer pays attention to another’s and 60 age and sex-matched healthy controls
emotional state, all relevant conceptual (HC) participated. Participants viewed affective
representations relating to the observed film clips, reported the character’s expressed
emotional experience are rapidly and emotions, and their own emotional responses to
automatically activated providing access to the the clips. Responses were considered empathic if
meaning in the stimuli. This study aimed to participants reported feeling the same emotion
determine whether people with TBI are also they had identified the character in the clip to be
rapidly accessing parallel emotional information, feeling.
making them susceptible to incongruity in an Results: Participants with TBI were significantly
Emotional Stroop task. less accurate than HCs at emotion recognition,
Method: 26 people with TBI and 30 matched t=.2.74, p=.007 and less likely to experience an
control participants were presented with 105 empathic response, χ2=14.33, pand empathically responded to the characters’ correlated with stress, and negatively correlated emotions more frequently, (78% versus 65% for with quality of the relationship (p
with a significant effect of time for the TH group attendance. Three cases will be illustrated to
only (p=.001). There were no significant convey the breadth of treatment responses: 1)
interactions, or time or group effects for other reliable and clinical improvements; 2) no change
QOLIBRI scales. post-treatment with delayed improvement; and
Conclusions: TBIconneCT participants reported 3) non-response.
improved QOL in social relationships. TH Conclusions: Challenges arising from the research
participants reported improved QOL in cognition, process will be discussed, including difficulties
whereas IP participants did not. with potential participant identification and
Correspondence: Rachael Rietdijk; maintaining group allocation. The case
rman7827@uni.sydney.edu.au illustrations will be reflected upon to consider
possible mediating factors to treatment
Protocol, process, and progress on a feasibility response.
RCT targeting social cognitive impairments after Correspondence: Anneli Cassel;
acquired brain injury anneli.cassel@unsw.edu.au
Cassel, Anneli1,2; McDonald, Skye1,2 and Kelly,
Michelle2,3 Cognitive Reserve and Age Predict Cognitive
1
School of Psychology, University of New South Recovery Following TBI
Wales, Sydney, Australia Ponsford, Jennie1,2; Fraser, Elinor1,2; Biernacki,
2
Moving Ahead Centre of Research Excellence in Kathryn2,3; McKenzie, Dean2 and Downing,
Brain Recovery, University of New South Wales, Marina1,2
Sydney, Australia 1
School of Psychological Sciences, Monash
3
School of Psychology, University of Newcastle, Institute of Cognitive and Clinical Neuroscience,
Newcastle, Australia Monash University, Clayton, Victoria, Australia
2
Monash Epworth rehabilitation research Centre,
Background and Objectives: Social cognitive Epworth Healthcare, Richmond, Victoria,
impairments are common after acquired brain Australia
injury (ABI) and detrimentally impact on social 3
Centre for Molecular and Behavioral
relationships. Despite this, few have treated Neuroscience, Rutgers University, Newark, USA
social cognitive deficits in this population. This
study aims to establish the feasibility of a novel Background and Objectives: Cognitive
social cognition group treatment (‘SIFT IT’) for impairments are common and disabling after TBI.
people with ABI. Little is known of factors associated with
Method: The SIFT IT study is a multi-site RCT. cognitive recovery. This longitudinal study
Recruitment commenced mid-2017 at three NSW examined the association of age, IQ and PTA
brain injury rehabilitation services and the duration with cognitive recovery 2-5 years
community. Eligible participants are randomly following TBI.
allocated into SIFT IT or Waitlist Control (WLC). Methods: 107 individuals with mild to severe TBI,
SIFT IT runs in small groups for 14 weekly 90- Mage 44.38 years, Meduc 14.04 years, MPTA = 21.66
minute sessions, delivered by a Clinical days and MIQ 109 were assessed early post-injury
Psychologist. The program covers: emotional self- and reassessed an average 44.65 months post-
awareness, emotion perception, perspective injury. A matched healthy control group (n=63)
taking, and choosing social responses. Feasibility, with Mage 46.92 years, Meduc 13.34 years, and MIQ
qualitative, and quantitative outcomes are 107.21 completed measures once. Measures
monitored. Measures are administered at three included the NART (premorbid IQ), Digit Symbol
time-points: T1 (eligibility); T2 (post-SIFT IT); and Coding (DSCT) (processing speed), RAVLT
T3 (post-waitlist SIFT IT/3-month follow-up). (memory) and Trail Making Test Part B (TMT-B)
Results: The study is ongoing with 23 participants (executive function). Regression analyses
eligible thus far: 12 randomly allocated to SIFT IT examined predictors of cognitive performance.
and 11 to WLC. Half of the recruitment waves are Results: Participants with TBI performed
complete, with four programs finished. By T3, significantly worse than controls on all measures
retention has been 91% with excellent group (all pin the TBI group at follow-up. Premorbid IQ was networks. “Continuation and stability” was
associated with gains on all measures, after characterised by long lasting and supportive
accounting for initial performance (β = 0.35, p < social networks which helped to maintain self-
.001), RAVLT (β = 0.22, p < .05), and TMT-B (β = – identity. “Maintenance and expansion” depicted
0.43, p < .001). Age was associated with gains on the experience of both retaining pre-existing
DSCT (β = –0.35, p < .001) and TMT-B (β = 0.28, p networks and forming new ones, and learning to
< .05). PTA duration was not significantly assimilate old and new identities. “Loss and
associated with cognitive recovery on any disconnection” reflected the loss of social groups
measure. without forming new connections and an ongoing
Conclusions: Findings support the contention struggle to rebuild one’s self-identity. “Loss and
that cognitive reserve and to a lesser extent age rebuilding” was characterised by disruption of
determine degree of long-term cognitive social groups, with new connections forming over
recovery following TBI. time to support a reconstituted self-identity.
Correspondence: Jennie Ponsford; Conclusions: Social networks can be substantially
jennie.ponsford@monash.edu altered following a brain tumour diagnosis.
Individuals who are able to maintain, expand or
Concurrent Session 3 rebuild their social networks typically experience
greater continuity or positive shifts in their self-
Use of social identity mapping to understand identity. The implications for psychosocial
the impact of brain tumour on social groups and interventions will be discussed.
identity: A qualitative study Correspondence: Lee Cubis;
Cubis, Lee1,2; Ownsworth, Tamara1,2; Pinkham, lee.cubis@griffithuni.edu.au
Mark3,4; Foote, Matthew3,4 and Chambers,
Suzanne1,2,5 A journey of ambiguity – The healthcare
1
School of Applied Psychology, Griffith University, experiences of people with mild stroke
Mount Gravatt, Australia Hodson, Tenelle1; Gustafsson, Louise2 and
2
Menzies Health Institute Queensland, Griffith Cornwell, Petrea2
University, Gold Coast, Australia 1
School of Health & Rehabilitation Sciences,
3
School of Medicine, University of Queensland, University of Queensland, Brisbane, Australia
Brisbane, Australia 2
School of Allied Health Sciences, Griffith
4
Department of Radiation Oncology, Princess University, Brisbane, Australia
Alexandra Hospital, Woolloongabba, Australia
5
Cancer Council Queensland, Fortitude Valley, Background and Objectives: Whilst it has
Australia recently been acknowledged that people with
mild stroke experience ongoing issues following
Background and objectives: Confidence in hospital discharge, mild stroke-specific services
support has been found to buffer the adverse are lacking internationally. Consequently, the
effects of brain tumour on psychological well- ability to understand how this population
being. This study aimed to explore individuals’ experiences health services is restricted, halting
experience of changes in social networks and the advancement in the area. It is imperative that the
impacts on self-identity after brain tumour. views of this population are sought in regards to
Method: A purposive sample of 20 adults with health services to address their needs and reduce
primary brain tumour (35% benign; 15% low the impact of ongoing issues. For this reason, this
grade; 50% high grade) participated in two semi- study aimed to answer the question: “How do
structured interviews over three months. A visual people with mild stroke perceive their experience
social map was used during the interviews to of stroke-related services?”
characterise members of their social network and Method: Qualitative investigation using an
their function, importance and meaning. Guided interpretative phenomenological analysis. Five
by phenomenology, interview transcripts and participants were interviewed at 1-, 3-, and 6-
social maps were analysed to identify major months post discharge. Visual Analogue Scale
themes. scores that measured satisfaction with health
Results: Four themes depicted patterns of loss, services were used for triangulation.
stability, growth and expansion of socialYou can also read