2019 of Medicine Review - Find out about the new ARCH Calgary program at PLC.
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

2019 Review
2018-19
ANNUAL REPORT
Department
of Medicine
Find out
about the
new ARCH
Calgary
program
at PLC.
5
PAGE
2019 Review DIVISION
DEPARTMENT OF MEDICINE PROFILES
UNIVERSITY OF CALGARY AND
ALBERTA HEALTH SERVICES Message from
Department Head
44K
2018-19 REPORT PAGE
56
Dermatology
PAGE
62
Endocrinology & Metabolism
PAGE
64
“We have worked hard to provide 44,069 outpatient clinical Gastroenterology &
Hepatology
referrals received by Central
reports and information that highlight Access & Triage (CAT).
PAGE
66
the Department's important clinical, PAGE General Internal Medicine
60 PAGE
educational, academic, and administrative 68
activities and accomplishments in the PHYSICIAN PROFILES Geriatric Medicine
Meet two members of the Department PAGE
2018-19 Fiscal Year.” of Medicine, Dr. Jane Lemaire and 70
Dr. Richard Leigh Dr. Habib Kurwa, and see how each, Hematology & Hematological
Professor and Head, Department of Medicine in their own ways, are working to Malignancies
PAGE
improve health care for all Albertans.
72
56
PAGE
PAGE
36 Infectious Diseases
PAGE
74
$30M
RE-THINKING HOW WE QUALITY IMPROVEMENT Nephrology
PROVIDE CARE INITIATIVES PAGE
Learn about several collaborative, In 2018-19, many of our Divisions 76
multidisciplinary programs that collaborated with Primary Care Respiratory Medicine
$29,991,365.87 in total provide care outside of a traditional and Strategic Clinical Networks on PAGE
annual research revenue, health care or hospital setting, QI initiatives. The changes made 78
tailor care to meet patients’ specific because of these initiatives have Rheumatology
including $6.88 Million in
needs, and meet patients ‘where allowed the Department to provide PAGE
CIHR revenue and $16 Million they’re at’. better, and more timely care for 80
in clinical research revenue. PAGE
all Albertans. Our Community
4 PAGE
82
PAGE PAGE
58 46
DEPARTMENT
497
INNOVATIONS IN
CLINICAL RESEARCH OPERATIONS
From ‘bench to bedside’: Find out Department Organization
geographic
PAGE
The Department of Foothills Medical Centre
Medicine is located in the (FMC) and UCalgary
about some of our recent innova-
tions in clinical research and how
The Department of Medicine 86
consists of 431 primary
scope Alberta Health Services
– Calgary Zone and at
Foothills Campus, Peter
Lougheed Centre (PLC)
Department of Medicine members
are working to improve the health members and 66 cross-
Department Demographics
PAGE
87
the Cumming School of and Sunridge Landing, PARENT ORGANIZATIONS and lives of Albertans. appointed members.
Medicine, University of Rockyview General Hospital The Department of Medicine exists as Awards
PAGE PAGE
Calgary. The Department (RGH), South Health a Department within both Alberta Health
Services (AHS) and the University
24 88 PAGE
89
serves a catchment of Campus (SHC), Richmond
2.4 million residents Road Diagnostic and of Calgary (UCalgary). To reflect this Patient Data
of Southern Alberta, Treatment Centre (RRDTC), unique dual-organizational structure, “Physician wellness is when you’re not PAGE
both AHS’ and the UCalgary’s logos 92
Southeastern British
Columbia and Southwestern
Sheldon M. Chumir Health
Centre, and the Associate and colour palettes are featured in
just surviving in your work, but you’re
Publications
Saskatchewan. Department Clinic, Gulf Canada Square. balance throughout this Report. thriving in your work, so that you can be PAGE
Members are located at 93
7 medical sites across at your very best and deliver excellent Revenue
Calgary, including the
patient care. Because that’s really what PAGE
94
our work is as physicians.” Physician List
PAGE
Dr. Jane Lemaire
Vice Chair, Physician Wellness & Vitality
95
PAGE
40
educating
the next
generation
Our Mandate is to identify
and mentor trainees who
have potential to become
academic leaders in
medicine and related fields:
powerful One of the core tenets of
the Department of Medicine
and Oncology, as well
as with the six Calgary
identify them, mentor and
support them, provide them
partnerships is that collaborative,
multidisciplinary teams
and Area Primary Care
Networks (PCNs). Our
with the opportunities to be
competitive for academic
are essential for providing members are also exten-
faculty positions, and ulti-
outstanding medical care sively involved within
mately recruit them as the
to all Albertans. We have Alberta Health Services’
medical leaders of tomorrow.
close working relationships sixteen provincial Strategic
with other Departments, Clinical Networks (SCNs).
including Community
Health, Cardiac Sciences,
6 THINGS YOU impactful Department Members as well as within W21C,
conduct world-class a research and innova-
research translational and health tion initiative based in the
SHOULD KNOW
outcomes research University of Calgary and
within all seven Research Calgary Zone of Alberta
Institutes at the University Health Services.
ABOUT THE of Calgary’s Cumming
School of Medicine
DEPARTMENT
OF MEDICINE innovation In collaboration and
partnership with PCNs
Other innovative programs
we have developed include
to improve and SCNs, the Department
has established numerous
the Geriatrics Fracture
Liaison Service, COPD
patient care Clinical Care Pathways and
Specialist Link services,
Initiative, Lung Cancer
Screening Program, Home
which have reduced wait Dialysis Program, Diabetes
lists for specialist services in Pregnancy Clinic, Health
and allowed more patients Analytics Working Group
to receive quality care in (HAWG), and the Calgary
the medical home. Zone Medical Services
Clinical Safety Committee
improving Our members are
committed to improving
both lead innovative clinical
and research programs to
(MSCSC).
public Public Health for the benefit
of all Albertans. Dr. John
improve patient care for
vulnerable populations,
health Conly, who is the current
Medical Director for W21C
including refugees and
patients with substance
and former Head of the use disorders. Dr. Cheryl
Department of Medicine, Barnabe, Vice Chair of
conducts groundbreaking Indigenous Health in the
research on antimicrobial Department of Medicine,
resistance and stewardship. is helping to drive work to
Dr. William Ghali is the improve health outcomes
Institute Director for
the O’Brien Institute for
for Indigenous patients.
our We are one of the
largest Departments in
appointments in the
Department of Medicine
Public Health. Drs. Gabriel
Fabreau and Prabh Lail membership the Cumming School of
Medicine and Calgary
or Division of Cardiology
(Cardiac Sciences),
Zone, and have grown to and 66 members with
just under 500 members cross-appointments to the
in 2018-19, including 431 Department of Medicine.
members with primary
2 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 3RE-THINKING HOW WE PROVIDE CARE
roviding health care to
Dr. Parabhdeep (Prabh) Lail THE PATIENT NEARLY DIES. He or she
General Internal Medicine Specialist,
is admitted to hospital with complica-
Medical Director, Addiction Recovery
and Community Health (ARCH) Calgary tions from liver disease. They have
thousands of Calgarians is a
gastrointestinal bleeding with massive
varices—veins that are enlarged and
ADDICTION swollen. The patient is resuscitated,
huge and complex undertaking. RECOVERY AND
the varices are banded and appropriate
medication is administered.
COMMUNITY When the clinician digs deeper
The Department of Medicine, AHS, and HEALTH (ARCH)
to explore the cause of the liver
disease, they may find the patient
has longstanding alcohol use disorder.
CONTRIBUTORS
Dr. Parabdheep
(Prabh) Lail UCalgary are constantly working together AT PLC
Delivering front-line acute care
In that case, the doctor will likely tell
the patient to stop drinking or face
certain death. But Dr. Prabh Lail
to find ways to improve how to provide
Dr. Karmon Helmle
Dr. Julie McKeen says the patient needs more than a
is demanding work, and it’s
Dr. Michelle Grinman directive, they need counselling and
Olive Wiley
an extra challenge to provide information on treatment options in
(patient)
Winnie Smith
(patient) better care. support for the many patients
who suffer from addictions.
Now, a special team at the
order to stop drinking.
That’s where the new Addiction
Recovery and Community Health
DIVISION INVOLVEMENT
Peter Lougheed Center is (ARCH) consultation service comes in.
Endocrinology &
Metabolism
In some cases, change starts when one individual person And you’ll read about a program that serves to bridge “Often the reason for admission or
helping give wraparound care
General Internal
who is paying close attention notices a gap in care for their acute care hospitals with people in the community who need a hospital visit is a consequence of or
Medicine to patients with addictions. directly because of a substance use
patients. In this chapter you will read about how a resident in lower acuity care, by bringing hospital-quality care home.
the Department started asking questions that led, eventually, We are dedicated to providing health care that supports disorder. There has been very little being
to scores of people from the Department, AHS and UCalgary the entire person—not just a single illness or condition. offered in acute care for these patients,
working together to close that gap and dramatically improve To ensure we do this we work collaboratively; bringing so there certainly was a gap,” says
care for people with diabetes who are admitted to hospital. different disciplines and partners together to develop new Lail, the medical director of the ARCH
Sometimes we start to re-think the way we’ve always programs that provide better care in the hospital and program at Calgary’s Peter Lougheed
done things when we see colleagues outside our jurisdiction beyond into the community. Centre, a specialist in substance
making changes and improving care by finding new ways to use disorders and a former Canada
tackle old problems. In this chapter we also bring you a story Addiction Medicine Research Fellow.
about a new team that’s emulating a program that began
in Edmonton to provide wraparound care to people with
addictions who are admitted to the Peter Lougheed Centre.
4 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 5“In terms of
emergency
room visits,
one-third of
patients—if
not more—
have some sort
of substance
use disorder.”
Dr. Prabh Lail
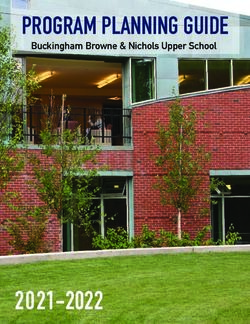
ARCH has operated at the Royal harm reduction and creating efficien- workers, especially in cases where a PREVIOUS PAGE
Peer Support Worker
Alexandra Hospital in Edmonton since cies in the system by improving health patient’s immediate needs are housing
Catherine MacAllister
2014 as part of the Inner City Health outcomes and health care access. and food. Many patients don’t even
takes Kari High, a
and Wellness Program. It launched in “Addiction is a disease that doesn’t dis- have photo identification. patient in the ARCH
Calgary in November 2018 and has a criminate,” says Lail. “Anyone from any Lail says many of her colleagues are Calgary program,
team of 12 physicians on rotation, two socio-economic background can have eager to learn more about ARCH while outside for a coffee
and conversation in the
social workers, two addictions coun- a substance use disorder and they can others may be critical of the service
sunshine – part of the
sellors, two peer support workers, an end up being very vulnerable.” ARCH and its patients. “We try to have open
“full wrap-around care”
outreach worker, a nurse practitioner, patients may also be socially vulnera- and honest conversations, no matter that ARCH provides.
a registered nurse, a clinical nurse ble; many are homeless. how difficult they are, with the goal of
PAGE 6
educator, an administrative assistant, ARCH provides what Lail calls educating and working towards a culture
Top left:
and a pharmacist. “full wrap-around care.” It starts with change that needs to happen in acute Dr. Prabh Lail, the
Demand for the ARCH’s services ensuring basic patient needs are met: care.” Lail and her team are working on Medical Director for the
has been steady. “We have seen close food, clothing and shelter. The next breaking down the considerable stigma ARCH Calgary program,
speaks with Catherine
to 1,000 patients at our site alone. It step is inquiring about housing status surrounding addictions, one patient and
MacAllister. The ARCH
motivates me to think that we certainly and testing for sexually transmitted one conversation at a time.
Team meets for rounds
need to expand this to other sites as infections, diabetes and dyslipidemia ARCH has become a vital resource every day to review
well,” she says. “When we think of the (abnormal levels of lipids in the blood), in Alberta, particularly in light of the patients currently in
visits to emergency rooms, on average screening for colon cancer and pap rising fentanyl crisis—front-line staff are the program.
one-third of patients—maybe more— smears for women. seeing cases of opioid use disorder and Bottom left:
also have addiction issues.” Intake forms are completed along related issues more frequently than ever All patients in the
ARCH sees people with addictions with full assessments of substances, before. Lail is hoping to dedicate time to ARCH Program receive
Naloxone Kits. These
from every walk of life; focusing on primarily alcohol, tobacco, opioids, training more clinicians in addictions so
kits are available free
cannabis, stimulants and benzodiazap- ARCH is able to expand across Calgary
of charge to anyone at
ines—depressant drugs that include and help more patients once they leave risk of opioid overdose.
sleeping pills and tranquilizers. This the hospital; preventing readmissions Family and friends can
assessment helps the ARCH team know and medical complications. also get a kit.
what they’re dealing with in terms of “The philosophy of our program
intoxication and withdrawal symptoms. is to meet patients where they’re at,”
Nurses initiate many of the consul- says Lail. “We don’t set the goal for
tations because they’re on the front the patient. We work with patients to
line and recognize when patients with set their goals and we support them
substance use issues would benefit in achieving those goals.”
from ARCH services. Addictions coun-
sellors become involved as do social
6 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 7“Addiction “There was very
is a disease little being
that doesn’t offered in acute
discriminate.” care for these
PROVIDING SUPPORT PREVIOUS PAGE
Top right:
Bottom right:
Drs. Prabh Lail and Kate
PAGE 8 AND 9
Brad Johnson and
Dr. Prabh Lail
patients so
there certainly
Brad Morrison is one Instead, everyone who In the Emergency Colizza review the list Dr. Prabh Lail visit with
of the ARCH support comes through the ARCH Department, Dr. Kate of consult requests for James Galant, another
program receives wrap- Colizza, ARCH Assistant patients with substance patient who is bene-
workers who meets
with and helps people
who have addictions
around care. And the peer
support workers play a
pivotal role in that care;
Medical Director, speaks
with Brad Morrison,
the program’s other
use issues who would
benefit from ARCH
services. Many of these
fitting from the ARCH
Calgary program.
was a gap.”
Peer Support Worker, consult requests are
Dr. Prabh Lail
when they’re admitted acting as a trusted bridge while Kai Johnson, RN initiated by nurses in the
to the Peter Lougheed between the person with prepares a Naloxone Kit. Emergency Department.
Centre in Calgary. addictions and the health
care professionals and
Brad Morrison has a deep provide “a warm handover.”
understanding of the ten or
so people he meets every “He felt,
day in his role as ARCH peer
support worker at the PLC. for the first
Morrison struggled with his time, that
own addiction issues for
decades and spent years somebody
trying to get clean and sober.
He started working with finally got
ARCH when it launched in it, and that
November, 2018 and so
far, the program has helped he wasn’t
more than 1,500 people.
One of them really stands going to be
out in his memory—a 60 stigmatized
year old man with alcoholism
who had been admitted to and sent
the emergency department
about 80 times in the year away without
prior. “He couldn’t stop any help
drinking,” says Morrison.
“He would do his best. He’d or under-
come to emerg, they would
rehydrate him, hold him for standing.”
four to six hours and then Brad Morrison
discharge him.” The man
would be sent on his way “Typically with the way
with advice to go to detox these patients have been
and quit drinking. treated, they don’t really trust
When inevitably, the man the staff in any health care
came back to the hospital, setting,” he says. “I reassure
Morrison sat with him and the patient that we are there
shared a bit about his own for them. Then I go to the
story before telling him how staff and let them know what
ARCH was going to help the patient’s going through,
him. “He held his blanket to what their fears are and why
his face and started crying. they’re here.”
He felt, for the first time, Morrison sees a bit of
that somebody finally got himself in every patient he
it, and that he wasn’t going meets. And he’s thrilled
to be stigmatized and sent he can help them.
away without any help or “You know, some Sundays
understanding.” I can’t wait to get here
Monday morning because
I love my job that much.”
8 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 9INITIAL “Residents
WHAT IS BBIT?
OBSERVATION BASAL INSULIN
Dr. Karmon Helmle, The questions asked about knew how Basal insulin is intermediate
or long acting and mimics the
to best treat
clinical assistant professor, the clinicians’ comfort level background insulin typically
Department of Medicine, with managing patients’ produced by the pancreas in
was in her first year of diabetes and whether they people without diabetes.
residency in Calgary when
she noticed the care given
to patients with diabetes on
felt they needed more
training or information.
The results of the
diabetes in BOLUS INSULIN
Bolus insulin is short or
the medical teaching unit
didn’t always line up with
survey—“We are very com-
fortable treating diabetes. hospital, but rapid acting and it balances
the carbohydrates consumed
in reality,
the guidelines that suggest We’re very comfortable with at meals.
doctors use BBIT. different insulins in different
So, for her first year complex scenarios. We INSULIN CORRECTION
resident’s research project,
she surveyed her colleagues
about diabetes management.
know that we should be
treating people with BBIT
strategies and not using the
actual treatment Insulin correction is another
short-acting insulin that
makes small corrections and
She asked clinicians to fill
out a questionnaire about
sliding scale”—did not line
up with what Dr. Helmle was didn’t match brings blood glucose back to
target, if needed.
with what
how they order insulin for observing in the hospital.
their patients and manage a TITRATE
variety of complex scenarios. Ensure blood glucose is
we knew we monitored four times daily
and insulin doses are
adjusted regularly to meet
should Diabetes Canada targets.
Dr. Helmle
Dr. Karmon Helmle
Clinical Assistant Professor,
ONE OF FIVE adults admitted to
the hospital in Alberta has diabetes.
decided to dive be doing.”
Department of Medicine
Physician Champion, Provincial Diabetes These patients are usually admitted in further Dr. Karmon Helmle
Inpatient Management Initiative, for a different medical reason but their
Diabetes Obesity Nutrition Strategic
diabetes creates complex issues and
Clinical Network
can dramatically slow their recovery.
Dr. Julie McKeen
Clinical Assistant Professor, People with diabetes are often
Department of Medicine experts in managing their chronic
5%
Physician Lead, Provincial Diabetes Inpatient
condition day-to-day, but that becomes
Management Initiative, Diabetes Obesity
Nutrition Strategic Clinical Network difficult when they’re in the hospital and
they have little control over their diet,
physical activity and other factors.
USING Basal bolus insulin therapy (BBIT)
DIGGING
KNOWLEDGE
is a proactive way to give insulin that
mimics the body’s natural production
DEEPER
TRANSLATION of the hormone. Research shows that
BBIT is a better way to treat people with For her second year difficult to actually order
TO IMPROVE diabetes while they’re in the hospital
than using sliding scale insulin (SSI),
residency research project,
Dr. Helmle looked at old
the sequence of insulin in
Calgary’s hospital’s software
INPATIENT where a patient is administered insulin DIABETES AFFECTS
electronic health records system, Sunrise Clinical AN ESTIMATED 1 IN 20
depending on their blood sugar levels. to see whether the records Manager (SCM). They CANADIANS.
DIABETES SSI is not individualized to the patient,
can result in large blood glucose fluctu-
aligned with the results
from her first-year survey.
needed an order set—a
group of pre-packaged
MANAGEMENT ations over the day which can increase
morbidity, mortality and length of stay.
The records supported her
observation that clinicians
instructions that allow clini-
cians to order BBIT for their
In 2007, a medical resident in The BBIT program was developed to were not, in fact, using BBIT patients in just a few clicks.
Calgary started asking questions make it easier for clinicians to follow the to treat their patients with Dr. Helmle worked with a few
necessary steps of ordering insulin for diabetes in hospital. colleagues in IT to develop
about how people with diabetes
their patients with paper order sets, or When Dr. Helmle started an order set and they saw
receive care in the hospital. Those in Calgary hospitals within the Sunrise asking her colleagues an uptake in clinicians in
initial questions have informed Clinical Manager (SCM) software. why they didn’t use BBIT, Calgary using BBIT.
a province-wide initiative that’s they told her it was really
standardizing and improving care
for patients with diabetes.
10 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 11$13b “It became a
PAGE 10 AND 11
Dr. Karmon Helmle
and Dr. Julie McKeen
question of
review analytical data
for the BBIT.ca and
KTToolkit.ca websites.
CANADA’S HEALTH CARE
how to take PAGE 13
The Improved Glycemic
Management core team
best evidence
BUDGET CONTRIBUTES meets at the Richmond
$13 BILLION A YEAR
Road Diagnostic and
FOR 2 MILLION PEOPLE
WITH DIABETES. Treatment Centre
and translate it
(RRDTC) to review the
status of the Provincial
In-Patient Diabetes
Management Initiative.
into practice—
the knowledge
translation
piece.”
Dr. Helmle had Dr. Julie McKeen
identified a care
gap for people
with diabetes in
hospital The DON SCN
core committee
identified diabetes
management
in hospitals as
a priority for
Alberta
ASKING
PATIENTS
Meanwhile, the Diabetes,
Obesity and Nutrition
Strategic Clinical Network
(DON SCN) did a patient
survey evaluating patient
DON SCN received
feedback from 672 patients
who have diabetes and
were admitted to an Alberta
hospital in 2014. Those
An Improved Glycemic
Management core team was
assembled. And it quickly
identified that about a third
of patients with diabetes had
20% 4th
ABOUT 20% OF ADULTS
ADMITTED TO ALBERTA
DIABETES IS THE
FOURTH MOST COMMON
HOSPITALS HAVE CO-MORBIDITY IN
perceptions of diabetes patients with diabetes blood sugar levels that were DIABETES. PATIENT CHARTS.
care in hospital. DON were less satisfied with well above the recommended
SCN, one of 16 SCNs in their care in hospital than guidelines. Further, the team
Alberta, is a network of people without the disease. found patients with diabetes
health care providers, The patients with diabetes stayed in hospital about 40
patients, researchers and identified three areas of less per cent longer compared to
policy makers with expertise satisfaction: blood sugar those without. The team also
in specific areas. SCNs control, nutrition and finally verified, provincially, that the
identify care gaps and find their relationships with their use of BBIT was low and cli-
innovative ways to deliver care providers and the rela- nicians were using outdated
care and provide better tionship between hospital SSI to treat their patients,
outcomes for Albertans. care providers. confirming a widespread,
complex problem.
12 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 13MAPPING EARLY
A STRATEGY ADOPTER
Moving from
Implementing BBIT order
sets and basic diabetes
importance of hypoglycemia
and its management, but best practices
SITES
education was only one equally important, the to common Beginning in early 2016, led the change, mindful of The DON SCN group
piece of a complex puzzle to recognition and treatment ten early adopter sites the barriers at that specific facilitated baseline and
practice started implementing the site and armed with specific audit data for 18 months.
improve the care of patients of hyperglycemia.
450%
with diabetes in hospital. Together, the transforma- knowledge translation plan tools to overcome them. The group gave the sites
The team developed a tive project was called the toward changing clinical While initial education was targeted feedback, provided
comprehensive strategy that Provincial In-Patient Diabetes practice from SSI to BBIT. important, tools to promote information and knowledge
included nine other support- Management Initiative. The After a few months, the sites and sustain change involved translation tools to share
ing initiatives, identified their overall goal was to improve gave feedback around what much more than just ongoing with frontline staff and
internal AHS sponsors and glycemic management in was working well to address education. Champions helped re-evaluate barriers
their barriers, and what worked to influence their
set out timelines. hospital, better aligning with Revising to address any practice
These other collaborative guidelines, available literature new barriers had emerged. peers and share successes drift, quickly and early.
initiatives included everything and how patients are taught
order The early adopter sites while on the lookout for There was consistent
from developing appropriate to manage their diabetes sets when IMPLEMENTING implemented in a staggered emerging barriers. With and sustained increase
PROGRAMS FOCUSED
nutritional support, ways outside of hospital. needed ON TREATING fashion, with each site con- support from their admin- in ordering of BBIT which
to manage patient-specific Team members identified HYPERGLYCEMIA SAW tributing to the knowledge istrators, audit data was led to improved glycemic
A 450% RETURN ON
dispensing of insulin as well a number of outcomes and INVESTMENT. and tools available to the collected and shared to control, decreased episodes
as policies and guidelines pulled together to reach them. next site. support and sustain the of hyperglycemia and no
for highlighting not only the At each of the early change from SSI to BBIT. increase in hypoglycemia.
Identifying adopter sites, physician, The early adopter sites
nursing, pharmacy and collaborated and solved
initiatives
40%
administrative champions problems together.
Research begins DEVELOPING KNOWLEDGE
into how other
sites implemented ORDER SETS TRANSLATION
BBIT When it came to developing Identifying best practice is The Improved Glycemic
the order sets—the specific one thing. Having people Management team worked
DON SCN IMPROVED GLYCEMIC
instructions about ordering adopt them is another matter with knowledge trans- MANAGEMENT TEAM
IN ALBERTA, PATIENTS BBIT for a patient—the team altogether. Even when there’s lation experts and the Dr. Julie McKeen
WITH DIABETES STAY IN
looked at all the order sets ample evidence and whole- Alberta SPOR Support Physician Lead
HOSPITAL 40% LONGER
THAN THOSE WITHOUT. Dr. Karmon Helmle
available in the published hearted support for changing Unit (SUPPORT = Support Physician Champion
and unpublished literature a clinical practice, the for People and Patient- Leta Philp
across Canada as well as process of establishing and Oriented Research and Clinical Practice Lead
IDENTIFYING hospitals and jurisdictions
across the country that had
sustaining the new patterns
of care can be challenging.
Trials) to develop a three
stage knowledge transla-
Glenda Moore
Past Project Lead
TEN EARLY
ADOPTER SITES
Rhonda Roedler
BARRIERS already implemented order
sets for BBIT.
That’s where the science
of knowledge translation
tion plan to promote the
change to BBIT. It identified
Provincial Pharmacy
Lead
−− Chinook Regional
Hospital
Edwin Rogers
The core team undertook The core team found Leveraging insights from comes in. It closes the gap and addressed barriers AHS, Analytics −− Canmore General
a national environmental that while each site had its those that had already imple- between ‘what we know’ and offered a deliberate Naomi Popeski Hospital
scan, collecting information own unique culture, many mented BBIT order sets, a and ‘what we do’—so called approach to help teams Assistant Scientific
Director, DON SCN −− Oilfields General Hospital
from dozens of acute care barriers and facilitators were unified provincial BBIT order ‘knowledge to action gaps’ adopt BBIT into their
Gabreille Zimmerman −− Calgary Urban Hospitalist
sites across Canada that shared amongst sites. The set was developed. AHS or K2A. These gaps can be daily routines. Program Coordinator,
had implemented order sets Alberta team concluded Human Factors supported a responsible for variations Knowledge Translation Program at Foothills
and Implementation Medical Centre, Peter
for BBIT. The Alberta team that to overcome these usability assessment and the in practice and big discrep- Science, AB SPOR
focused on the barriers the many shared barriers, an order set was revised where ancies in patient outcomes, Support Lougheed Centre,
hospitals had encountered organized, evidence-informed needed. The SCM BBIT quality and safety of care, Rockyview General
DON SCN LEADERSHIP
and what helped implemen- approach was required. Order Set was updated to efficiency and cost. Petra O'Connell
Hospital, and South
tation of BBIT order sets align with the provincial order Senior Provincial Health Campus
Director
at each site. set. Once implemented, −− University of Alberta
Dr. Peter Sargious
feedback was sought from Senior Medical Director Hospital
early adopter sites, and −− Grey Nuns Community
further revisions were made. Hospital
The order set is now on its −− Queen Elizabeth II
sixth iteration. Hospital
14 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 15PERFORMA
NCE SCORE
CARD
Basal B
olus Ins
ulin The
rapy Pro
The BBIT gram
initiative g
ets top m
arks for im
“This is a road inpatient d
PAGE 16
iabetes m proving
Dr. Karmon Helmle
anageme
reviews data on the Basal Bolu nt by supp
s Insulin T orting
map now.
BBIT website with
herapy ord
Core Team members ering prac
Gabrielle Zimmerman, GOAL tices.
Edwin Rogers, and
We’ve created a
RESULT
Leta Philp. Improve B
BIT orderi
in hospita ng
l Overall, B
BIT orderi
ng
process of how
2.5x from
baseline
Improve ra
tes of
to implement hyperglyc
emia 15% fewe
moderate
r days wit
or worse
h
this complex
hyperglyc
emia
Adoption
and contin
use of BB ued
practice change.
IT 97% of sit
es “satisfi
or “very s ed”
atisfied” w
implemen it h
tation. 95
BBIT site imple- sites repo % of
rt BBIT us
“frequentl e d
y” or “alw
after imple ays”
mentation
mentation
BBIT orde
ring adop
at all AHS ted
sites Of 106 ho
spital site
guidelines have in Alberta s
, 71 have
implemen
ted the BB
protocol, IT
been created
with an ad
9 sites in d itional
progress
and are shared
on our BBIT
website.”
Dr. Julie McKeen
5.3% 9.6% BBIT
IMPLEMENTED
ACROSS
THIS BBIT APPROACH
REDUCED THE FREQUENCY
OF HYPERGLYCEMIC
THE BBIT APPROACH
SAW A 9.6% REDUCTION
IN LENGTH OF STAY AT
ALBERTA
PATIENT-DAYS BY 5.3% THE CALGARY ZONE There are 106 acute care has been developed to barriers to BBIT imple-
WITHOUT INCREASING HOSPITALIST GROUP’S
THE FREQUENCY OF FOUR SITES. sites in Alberta. And most help other sites provincially, mentation, and links to the
HYPOGLYCEMIA. of them are either in the nationally, and internationally evidence-informed tools
process of implementing move to BBIT and improve targeted to each. All
BBIT order sets or have their patient care. Anyone tools have been made
already done so. Well can access the “BBIT Site publicly available.
beyond Alberta’s borders, Implementation Guidelines” As well as improving care
other acute care sites at BBIT.ca and tailor them to for patients with diabetes in
are contacting the people work in their own specific site. Alberta hospitals, the whole
who were involved in the A second website, process of implementing a
project to gain insights www.KTToolkit.ca, guides change in practice to BBIT
to lend to their own BBIT users through the process may serve as a road map for
implementation. of identifying cultural, other complex interventions
A website, www.BBIT.ca, awareness and capability, in the province.
containing all of the education communication, system,
and implementation guidelines resource, and patient-related
16 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 17Dr. Michelle Grinman FOR 89 OF HER 90 YEARS, Olive Willey in CCH or stay as an inpatient at the PAGE 18
Medical Lead, Complex Care Hub Top Left:
had never spent a night in hospital. hospital. Those who choose CCH are
Division of General Internal Medicine Dr. Michelle Grinman
Even after her visit to the emergency sent home where they receive daily meets with the Complex
department at Rockyview General care and monitoring from a team that
COMPLEX CARE
Care Hub team at RGH.
Hospital (RGH) last spring, she spent is overseen by a General Internist/
Bottom Left:
just one day in a hospital bed thanks Hospitalist, Clinical Assistant and
HUB BRINGS THE to the new Complex Care Hub Nurse Navigators. The team collabo-
Dr. Michelle Grinman
and Kirsten Proceviat,
(CCH) program. rates with the Mobile Integrated Health
HOSPITAL HOME
Manager of Transition
This innovative program is a Service, also known as the Community Services for Rockyview
General Hospital (RGH)
“virtual inpatient unit that allows Paramedics in the Calgary Zone who
Patients enjoy the benefits of eligible patients to receive the same serve as the eyes and ears of the
and South Health
Campus (SHC).
home with hospital-quality care. kind of care and treatment they would physicians in patients’ homes. Rigorous
Centre:
in hospital, but within the comfort of safety protocols ensure patients have
Barb Leteta, Nurse
their own home.” Says Dr. Michelle a direct line to their care team should Navigator, and
Grinman, a General Internal Medicine questions or concerns arise while Dr. Azadeh
specialist at RGH and originator of they’re at home. Tests and lab work can Motehayerarani,
CCH in the Calgary Zone. be ordered with the same priority as Clinical Assistant
– members of the
It serves as a bridge between inpatients. The CCH Nurse Navigators
Complex Care Hub
acute care sites and the community, report to Transition Services and are (CCH) team – review
she adds. Patients who come into the able to access home care services, a CCH patient’s chart.
emergency department or who are which enables them to leverage
PAGE 19
admitted to inpatient wards at RGH or existing pathways for comprehensive Drs. Grinman and
South Health Campus (SHC) requiring geriatric assessments provided by the Motehayerarani see
lower acuity care that would otherwise Geriatric Consult team, physiotherapy, Benjamin Predella at
require hospitalization are admitted occupational therapy and social work. the Rockyview General
Hospital, a patient who
to the CCH program. These patients Dr. Grinman and her team have
is also participating in
receive daily, sometimes twice daily, also fostered relationships with Primary the Complex Care
visits to manage their acute issues Care in order to enhance transitions of Hub program.
as they would under a conventional care from CCH to the health home.
hospital admission. But unlike tradi- The Calgary West Primary Care
tional inpatients, CCH patients aren’t Network (PCN) has hired two nurses to
transferred to a unit in the hospital to liaise with the CCH Nurse Navigators in
recover – instead they sleep at home. order to expedite transition of patients
Patients who meet the program’s back to the PCN and to support them in
criteria are given a choice – participate implementing their complex care plan.
18 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 19PAGE 20 AND 21
Complex Care Hub
patients, like Benjamin
Predella, can also be
monitored and seen by
the team at either RGH
or SHC when they come
to either site for medical
tests or procedures.
The East Family Care Centre has also “You’re in your own bed, you can
partnered with CCH to re-roster patients go have coffee with friends – you’re not
that require home visits or intensive stuck in a hospital bed the whole time,”
primary care services upon discharge say Willey. “When the doctor gave me
from the program. This comprehensive the option to stay in hospital or go home,
team approach not only benefits patients it was an easy decision to make.”
by allowing them to recover within the Daughter Dianne Arnott says she
comfort of their home, it also improves felt confident about her mom’s choice:
the healthcare system through more “There were no concerns for mom’s
efficient use of resources. care whatsoever. It was a logical
“We know that hospital-at-home choice, really. She wasn’t sick enough
services have been shown to reduce to stay in hospital, but she’s still getting
visits to emergency departments and the care she needs when she needs
provide flexibility during crises or surge it, whether it’s from her community
situations,” says Dr. Grinman. “Older paramedic or the doctor at Rockyview.
adults treated within this model are also The attention has been very fast and
less likely to have functional decline thorough. We’re very impressed.”
and need long-term care or assisted Winnie Smith, another patient in the
living one year later. program, also shared why she made
“Multiple systematic reviews and the decision to receive hospital-level
meta-analyses of Hospital at Home care at home through the Complex
programs around the world have shown Care Hub. “Privacy. Like having
reduced morbidity and mortality when somebody else next to you moaning
hospital-level care is delivered for the and crooning and everything you know.
right population of patients,” she says. I [would] rather be at home where I
“When a senior comes to the have peace and quiet,” says Winnie.
hospital and receives meals in bed
and isn’t walking around, they’re
more likely to deteriorate quicker than
patients being treated at home who
remain active and independent.”
For Willey and her family, the CCH
means quality of life isn’t sacrificed for
quality of care.
20 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 21PERFORMANCE SC
“Privacy. Like ORECARD
having somebody Complex Car
e Hub Progra
else next to you Data collected by
m
Complex Care H
moaning and 17-month period
ub staff over a
(Feb 2018 – July
crooning and the considerable
2019) confirms
success of the pr
everything you ogram to date:
PROGRAM MEASUR
know. I [would] ES
RESULTS
QUALITY OF
PRELIMINARY
“After going PAGES 22 AND 23 rather be at home CARE
96%
Percentage of pa
PROGRAM ANALYSIS The Complex Care tients (n=66) wh
o
Preliminary economic through this Hub allowed Olive
Willey (page 22, top)
where I have reported that th
from the Comple
e care they rece
ived
x Care Hub staff
analyses of the beginning
program, and Winnie Smith
(page 22, bottom; page
peace and quiet.” was good or ex
cellent
of the program suggest REGAINING
Winnie Smith, CCH patient
that providing care for CCH I realized 23) the opportunity to FUNCTION
81%
AND INDEPE
remain at home while NDENCE
patients may cost less than Percentage of pa
for inpatients matched by how much receiving hospital-level
care from a compre- reported that Co
tients (n=68) wh
mplex Care Hub
o
age, gender and diagnosis.
Responses from both
I never knew hensive team including
physicians, nurses, and
helped them rega
independence qu
in their function
ha
an
d
d
ite a bit or comple
patients and staff to date about my community paramedics
like Lou Labrash. PATIENT INVO
LVEMEN
tely
have been very positive. T
patients and
84%
Percentage of pa
Data collected by CCH tients (n=69) wh
reported always o
or usually being
staff over a 17-month period
show the program is a hit
that my care involved as muc
h as they wanted
to be in decision
with patients: was never and treatment
s about their care
−− On average, patients
rated their overall expe- complete. DAYS OF AC
UTE CARE PR
OV IDED
1,593.3
From Feb 2018
rience of the care they
received on the Complex
I feel this received care th
– July 2019, 141
rough the Comple
patients
x Care
Care Hub 9.5 out of 10 program is Hub, resulting in
days of acute ca
an estimated 1,59
3.3
Days
re provided
−− 96% of patients
reported that the care
wonderful
they received from the and gives
Complex Care Hub staff
was good or excellent us an oppor-
−− 84% of patients reported
always or usually being
tunity to
involved as much as help people
they wanted to be in
decisions about their in what they
care and treatment
actually
−− 81% of patients reported
that the Complex Care need.”
Hub helped them regain Anonymous Complex
their function and inde- Care Hub physician
pendence quite a bit
or completely
An anonymous CCH
physician remarked, “After
going through this program,
I realized how much I never
knew about my patients
and that my care was never
complete. I feel this program
is wonderful and gives us an
opportunity to help people in
what they actually need.”
While these are early
positive signals, the team
is embarking on a rigorous
evaluation of the program
as it is maturing.
22 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 23INNOVATIONS IN CLINICAL RESEARCH
edical research and innova-
Dr. Andrew Daly AN EXCITING NEW cancer treatment,
Division Head and Zone Clinical Section Chief
chimeric antigen receptor (CAR)
for Hematology & Hematological Malignancies
Former Director of the Alberta Blood and Bone T-cell therapy, is opening up a world
tion are fundamental to the
Marrow Transplant Program of potential for treating certain forms
Clinical Associate Professor,
of cancer and providing hope for
Cumming School of Medicine
people where, in many cases, there
Department of Medicine, CHIMERIC ANTIGEN
was little before. Essentially, CAR
T-cell therapy strengthens the body’s
immune system and pushes it harder
RECEPTOR T-CELL
UCalgary, and AHS. Researchers acquire (CAR T-CELL)
to fight cancer cells.
The type of genetic immunother-
apy re-engineers a patient’s own cells
CONTRIBUTORS
Dr. Andrew Daly
Dr. Kara Nerenberg
evidence and improve—or discover— THERAPY
from their immune system, giving them
instructions to attack cancer cells, and
injects them back into the body. The
treatments that help people here in Alberta
Liz Deneer Clinical trials are underway in process creates what is essentially
Sandra Burk
(patient) Calgary to use immunotherapy, a living drug—one that’s individually
a sort of “living drug,” to target customized for each patient.
and around the world.
DIVISIONS INVOLVED
Hematology & certain blood cancers. The first CAR T-cells were
Hematological developed in the 1980s but it has
Malignancies
taken tremendous time and effort to
General Internal
Medicine make them work says Dr. Andrew
Every year, UCalgary and AHS support thousands of new These mothers are at a higher risk for heart attack and Daly, Division Head and Zone Clinical
and ongoing studies that use UCalgary and AHS facilities, even premature death. In this chapter you will read about Section Chief for Hematology and
patient data and systems. In fact, Alberta has a higher an innovative research, new clinics and telephone health Hematological Malignancies in the
clinical trial enrolment rate than the national average. coaching program that is helping reduce women’s long-term Department of Medicine, former
In this chapter you will read about new clinical trials that risk factors of having high blood pressure during pregnancy. director of the Alberta Blood and
are testing an innovative and exciting immunotherapy to treat As members of the Department pursue their research Bone Marrow Transplant Program
some types of cancer. Chimeric Antigen Receptor T-Cell and perform clinical trials, the Department, UCalgary and and Clinical Associate Professor with
therapy is a type of “living drug” that is able to strengthen the AHS work with them, helping these world-class researchers the Cumming School of Medicine and
patient’s own immune system, pushing it to work harder and translate their discoveries from ‘bench to bedside’ and improve Arnie Charbonneau Cancer Institute
target certain blood cancers. the health and lives of people who live in Alberta and around at the University of Calgary.
Women who have high blood pressure when they’re the world.
pregnant often think their issues go away after their baby is
born. But researchers have determined that they’re likely to
continue to have problems long after they’ve had their babies.
24 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 25“We’ve been
leaders in stem
PREVIOUS PAGE
Dr. Andrew Daly
discusses CAR T-cells
Clinical trials have been happening
in various locations for the past few
Daly is a recognized leader in
stem cell therapy and transplantation.
cell transplants
for years, and
years. Now, Daly and his team have He made headlines in May 2019 after
with a patient on the
Hematology Unit at the started clinical trials that will help performing a stem cell transplant for
Foothills Medical Centre. advance CAR T-cell therapy and provide Revée Agyepong. She was the first
Dr. Daly and his team
have started clinical trials
that will help advance
renewed hope and improve the lives of
Albertans. “There are two established
indications for CAR T-cells right now,”
adult in Alberta whose sickle cell
anemia was cured with this treatment,
freeing her from the debilitating disease
so this is a
CAR T-cell therapy.
PAGE 26:
Jillian de Groot, a
he says. “One is relapsed, or refractory,
acute lymphoblastic leukemia, or ALL.
that caused excruciating pain and was
slowing killing her major organs. This
new opportu-
nity to look at
That’s the childhood type of leukemia, success was the latest to reinforce
Registered Nurse on
Unit 57 at the Foothills and then the indication in adults is Alberta’s leadership in stem cell
Hospital, begins to relapsed or refractory aggressive research and cancer treatment. Now,
prepare a patient for an
infusion of CAR T-cells,
a process similar to a
non-Hodgkin lymphoma.”
Daly and his colleagues at
Alberta Children’s Hospital have
Daly is applying the expertise to CAR
T-cell research, making advancements
that will open the doors to more “firsts”
a different type
blood transfusion.
PAGE 27:
After the CAR T-cells
begun clinical trials treating children
who have ALL and he hopes to treat
in Alberta health care.
of transplant
product.”
adults with non-Hodgkin lymphoma on PUSHING THE BOUNDARIES
are created and multi-
plied in Alberta Public similar trials. “My estimate is thirty or OF MEDICAL SCIENCE
Laboratory’s Cellular forty patients per year would have a In addition to trials in leukemia and
Therapy Lab, they disease that is eligible for CAR T-cells. lymphoma, Daly is collaborating on Dr. Andrew Daly
are cryopreserved in
Not every patient is going to be well a clinical trial in a different blood
liquid nitrogen.
enough to get them,” he says. cancer, multiple myeloma. “In multiple
Daly specializes in the transplan- myeloma, the CAR T-cell actually
tation of hematopoietic stem cells targets something different compared
– bone marrow cells that have the to what’s being targeted in the other
remarkable ability to develop into white two diseases that are treated.” His
blood cells, red blood cells or platelets. colleague Dr. Nizar Bahlis, Clinical
“We have an improved understand- Associate Professor with the
ing of how to engineer cells plus an Cumming School of Medicine and
improved understanding of how the member of the Division of Hematology
immune system works,” he says. & Hematological Malignancies, is
“Those are two very powerful tools principal investigator of the multiple
that are coming together and leading myeloma project.
to better treatments for patients.”
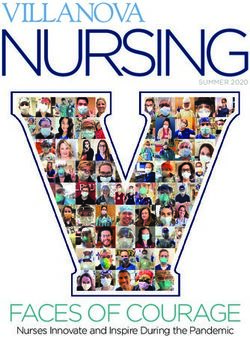
26 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 27CAR T-CELL THERAPY:
HOW IT WORKS
Chimeric antigen
3 receptor (CAR) T-cell
therapy is a new,
individualized cancer
treatment that boosts
the patient’s own
immune system to fight
cancer cells. Here’s
2
how it works:
STEP 1
Collect the patient’s T-cells
from their immune system.
STEP 2
Load the chimeric antigen
receptor (CAR) onto the
surface of the T-cells
creating CAR T-cells with
“Making CAR “Because we 1 4 instructions to look for
certain cancer cells.
T-cells work have a really STEP 3
Multiply the CAR T-cells
in the lab.
clinically took Daly and his team are also looking
to take part in another study that
“Some people may look at the prospect
of a two week hospitalization, being
good name PAGE 28
Once the patient’s
T-cells have been
STEP 4
a lot of work. in cancer
involves manufacturing CAR T-cells away from home, possibly ending up Give the patient chemother-
collected, the chimeric
“in house”. Due to the complexity of with really serious toxicity and say, apy to reduce the number of
antigen receptor (CAR)
the CAR T-cell manufacturing process, ‘You know, that’s not for me.’” is loaded onto the cancer cells in their body.
They’ve been most of these products are manufac-
tured by the pharmaceutical industry,
which adds to the cost of treating
That’s because roughly one-third
of those who receive CAR T-cells
require hospitalization in intensive
clinical trials surface of the T-cells,
creating the CAR
T-cells, on this machine
Put millions of CAR
T-cells into the patient’s
doing clinical in general, in the Alberta Public blood stream.
patients. Daly’s team has joined forces care for a week or more. Because of Laboratory’s Cellular
with researchers at the University of this consideration, Daly estimates their Therapy Lab at the The CAR T-cells will
trials with CAR people are
Alberta and the University of Ottawa capacity will be 26 to 30 patients per Foothills Medical Centre. continue to multiply in
in order to develop the expertise year to begin with. “We’re planning to the blood stream.
PAGE 29
necessary to manufacture CAR T-cells Daly is excited to think of a day keep people in hospital for about two Dr. Andrew Daly on
T-cells for the in Alberta Public Laboratory’s Cellular
Therapy Lab, located in Calgary. The
Calgary team was approached to take
when CAR T-cell therapy may even be
applied to cancers in which the immune
system doesn’t play such a central role,
weeks, and in order to be respectful of
the other areas of the hospital, and the
other resources in the hospital, we’re
starting to Hematology Unit 57
at the Foothills
Medical Centre.
STEP 5
The CAR T-cells look
for and set out to destroy
last five or part because of the existing equipment
and expertise made possible by the
such as cancer of the colon or kidney.
He points out that while these are
going to start off by treating one patient
every two weeks,” he says. “So we will
look at us 5
cancer cells that have a
specific antigen.
six years.” now as a place
strength of the research partnership of challenging to treat with immunother- try not to have more than one patient After receiving CAR T-cell
Alberta Health Services, Alberta Public apy, “people are trying to develop CAR getting CAR T-cells in the hospital at therapy, patients stay in
Laboratories, Cumming School of T-cells that actually function in those any one time.” the hospital and are
Dr. Andrew Daly Medicine and the University of Calgary.
Alberta’s international reputation as a
leader in cancer clinical trials makes this
environments, and when that happens
this field will explode.”
Over the years, Daly and other
researchers have made tremendous
progress exploring the intricacy and
to do CAR monitored and treated for
any side effects.
province a logical place for this sort of
cutting edge research. “We have a fairly
THE CHALLENGES
While the potential for living drug
complexity of the human body to
understand how CAR T-cell therapies
T-cell studies CAR T-cells may stay active
in the body and prevent the
as well.”
small population and we’re really spread therapy is very exciting, CAR T-cells can work and they are continuing to cancer from returning.
out,” he says. “But what we’ve done have an unfortunate element in push the boundaries and learn new
is we’ve really gotten out there, sold common with other cancer treatments: knowledge that will save lives.
ourselves, developed the infrastructure, it can make patients extremely ill. Dr. Andrew Daly
developed the standard operating pro- Daly says some patients may even
cedures, and because we have a really turn away the treatment. “Not every
good name in cancer clinical trials in patient is going to want to receive them
general, people are starting to look at us because of the toxicity and because of
now as a place to do CAR T-cell studies.” the unpredictable journey,” he says.
28 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 29“Women in
Canada are
Dr. Kara Nerenberg
Associate Professor,
Division of General Internal Medicine
UP TO ONE IN 10 Canadian women
will experience a high blood pressure
She received funding through Heart
and Stroke and CIHR as one of the
starting to indicate how many women have their
cholesterol and diabetes blood tests
PAGE 30
Dr. Kara Nerenberg,
who received funding
have heart
Cumming School of Medicine disorder in pregnancy (HDP), making recipients of the Women’s Heart and and the results.
from the Heart and
them two to five times more likely to Brain Health Chairs awards, a program This information will provide vital Stroke Foundation
have a heart attack or stroke before the designed to generate new knowledge insight into the best ways to reach
PROGRAM TO
and CIHR as one of
IMPROVE THE
age of 40 and die before they reach 60.
Even more troubling is that roughly half
of Canadian physicians are not aware
that improves awareness, prevention
and understanding of how biology and
socio-cultural factors affect women’s
attacks and women after they’ve had their babies. It
begins with improving clinic attendance.
Nerenberg’s research indicates 25
the recipients of the
Mid-Career Women’s
Heart and Brain Health
HEART AND of this risk, so they aren’t able to inform
their patients.
heart and brain health. The funding also
allowed Nerenberg to bring together 17
stroke even in per cent of new moms don’t show up
for their first post-partum visit and that
Chair awards, leads the
IMPROVE program.
PAGE 31
BRAIN HEALTH their 30s and
Dr. Kara Nerenberg is determined to other post-partum clinics from across grows to 50 per cent for later follow-up
Calgary mom Sandra
give young women the tools they need the country and form a national network visits. “There’s quite a big gap for these Burke was referred to
OF POST-PARTUM to take charge of their health through that’s developing best practices for women in terms of follow-up because the IMPROVE clinic in
CANADIAN WOMEN
the new clinic IMPROVE (Identifying
Methods for Postpartum Reduction
Of Vascular Events). She focuses on
managing women’s cardiovascular
health after pregnancy.
“Specialized follow-up clinics for
they’re dying it falls between the fields of obstetrics,
primary care and internal medicine,”
says Nerenberg. “To bridge that gap
June, 2018.
Research, new clinics and
a telephone health coaching
finding the best ways to prevent heart
attacks and strokes in young women
women after pregnancy across Canada
have started working together to share
in their 50s. we’ve done a couple things here in
Calgary such as starting a clinic called
We can’t wait
who were diagnosed with high blood clinic information so we can find out if PreVASC, a post-partum cardiovascu-
program for new moms are
pressure in pregnancy—roughly seven specialty clinics work better than usual lar risk reduction clinic, as well as our
helping to reduce women’s per cent of all pregnancies in Alberta. care clinics at finding and treating the IMPROVE post-partum clinic.”
long-term risk factors of
having high blood pressure
For example, preeclampsia, a condition
which includes high blood pressure, dis-
appears shortly after a woman delivers
heart and stroke risk factors,” says
Nerenberg. “These specialists will also
help us develop and test tools to help
until they’re 40 But these clinics can’t help if
women aren’t showing up for their
appointments. New moms can face
to 50 to start
during pregnancy.
her baby. But new research shows that doctors take better care of their patients. a number of challenges to get to the
the blood vessel damage that occurred If these tools work, we can test these clinic—caring for a little child can
treatments.”
during pregnancy, causing stiffening can tools in different clinics across Alberta make it difficult to travel to a medical
lead to accelerated atherosclerosis— as another starting point.” appointment and they may not have
hardening of the arteries. Nerenberg is leading the very first the money to pay for child care or the
“Women in Canada are starting to study to examine where, when and Dr. Kara Nerenberg additional expenses associated with
have heart attacks and stroke even in why women visit their doctors after travelling such as fuel and parking.
their 30s and they’re dying in their 50s,” pregnancy. This involves accessing After conducting surveys of new
says Nerenberg. “So we can’t wait health databases that already collect moms, it made sense to create a
until they’re 40 to 50 to start treat- information on women in Alberta and program that would bring help to them.
ments. We have to start in their 30s.”
30 DEPARTMENT OF MEDICINE 2018-19 ANNUAL REPORT 31You can also read