Clinical case & open questions - Luana Calabrò Center for Immuno-Oncology, University Hospital of Siena, Italy - Carcinoma Squamoso
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Clinical case & open questions
Luana Calabrò
Center for Immuno-Oncology,
University Hospital of Siena, Italy
MAT-IT-2001175
Disclosure
• Advisor/consultant:
Bristol Myers Squibb, Merck Sharp & Dohme, Roche-Genentech
• Compensated educational activities:
Bristol Myers Squibb, Astrazeneca, Sanofi-Genzyme
Immunotherapeutic agents approved in solid tumors
Maio M, et al, Clin Cncer Res 2020

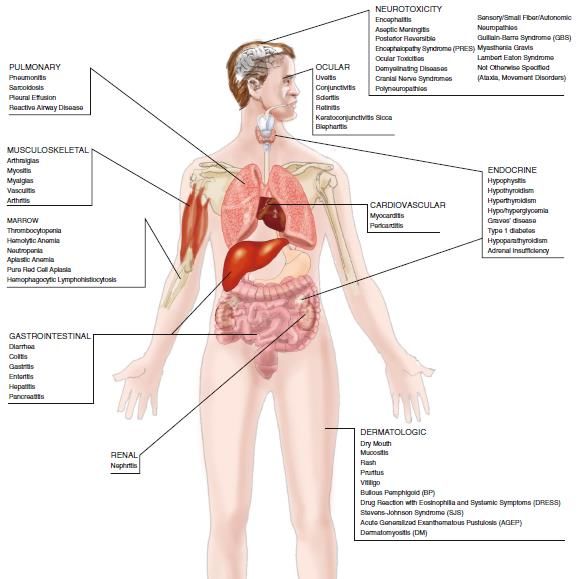
Immune-related Advers Events (irAEs) with immunotherapy
- Unique spectrum of side effects (timing and profile is
different then chemotherapy or target therapy)
- Quite broad spectrum of toxicity in terms of organ system
involvement and severity
- Highly unpredictable and often difficult to distinguish
between normal oncologic complications, progression of
disease, infection (may require biopsy).
- Require careful surveillance and early intervention to
mitigate adverse outcomes and often a multidisciplinary
management
Darnell Eli P, et al, Curr Oncol Rep 2020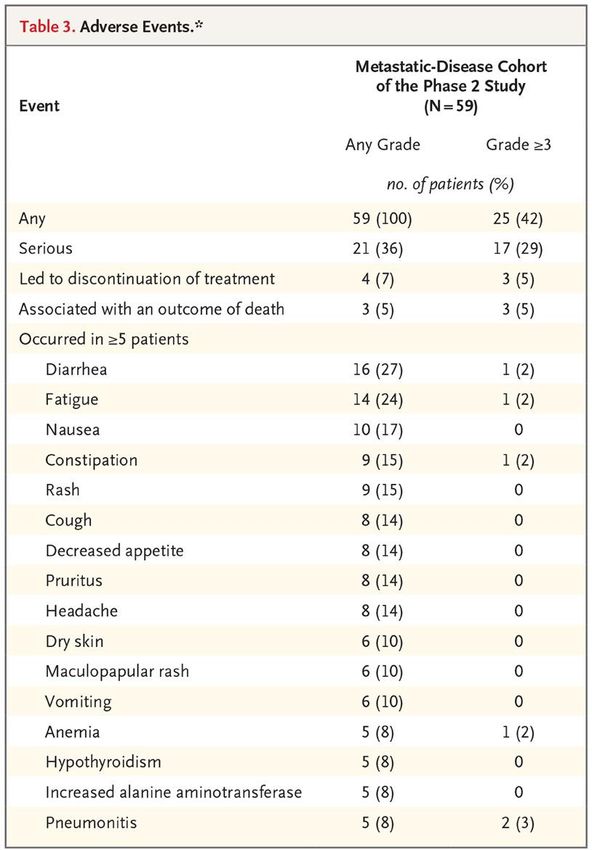
Most common irAEs Rare and emerging irAEs (< 3%)

Frequency and severity of irAEs with immune checkpoint inhibitors (ICI)
CSCC
Dougan M, et al, J Clin Invest 2020
Migden MR et al, NEJM 2018
Clinical case Male, 83 yrs old Comorbidities: hypertensive cardiopathy, degenerative aortic stenosis, hypercholesterolemia, hyperuricemia Brief oncological history Jul 2016 surgical excision of left nasal wing epithelioma Jun 2017 surgical excision of epithelioma of the scalp Jul 2019 surgical excision of epithelioma of the face Jan 2020 dermatological examination: several actinic keratoses of the face and scalp. Likely epitheliomatous evolution towards SCC of the frontal region, the vertex, the right subpalpebral region and preauricular region. Mar 20 facial lesion biopsy, E.I.: cutaneous squamous cell carcinoma →Tc scan/ultrasound: negatives for lymphonodes or distant metastases → Multidisciplinary evaluation: no indication for radical surgery or radiotherapy.
Clinical case
Baseline (May 2020)
Clinical case
Male, 83 yrs old
Comorbidities: hypertensive cardiopathy, degenerative aortic stenosis, hypercholesterolemia, hyperuricemia
May 2020 at our Center the patient is evaluated for treatment with anti-PD1 cemiplimab (no
controindications) and started anti-PD1 at a dose of 350mg iv, q 3wks (EAP)
w1 w4 w7 w10 w13 w16
Start 2nd dose 3rd dose 4th dose 5th dose 6th dose
treatment Aug 2020
May 2020
Time (weeks)Clinical case
May 2020 Aug 2020Clinical case
May 2020
Aug 2020Clinical case
Male, 83 yrs old
Comorbidities: hypertensive cardiopathy, degenerative aortic stenosis, hypercholesterolemia, hyperuricemia
May 2020 start treatment with anti-PD1 cemiplimab at a dose of 350mg iv, q 3wks (EAP)
PR irAE
w1 w4 w7 w10 w13 w16 w19
Start 2nd dose 3rd dose 4th dose 5th dose 6th dose
treatment Aug 2020
May 2020 Time (weeks)
09 Sep 2020 onset of diarrhoea (2-3 stools/die) →symptomatics
11 Sep 2020 visit at our Center: good clinical conditions, persisting diarrhoea (4 -5 stools/die).QUESTION #1
Quale comportamento seguire:
Risposta 1: Proseguire trattamento immunoterapico, con stretto monitoraggio clinico, se persiste la
tossictià gastroenterologica sospendere il trattamento immunoterapico
Risposta 2: Per la severità dell’evento avverso è opportuno sospendere definitivamente il trattamento
immunoterapico
Risposta 3: Sospendere temporaneamente il trattamento immunoterapico, avviare indagini per
correlare la tossicità all’agente immunoterapico, ed in tal caso iniziare terapia steroideaGastrointestinal irAEs
• Gastrointestinal toxicity may occur in any part of the alimentary canal, but small and large bowel are most
affected.
• Diarrhoea/colitis occur in 10%-25% with anti-CTLA-4, 1%-5% with anti-PD-1/PD-L1; ~20% with anti-CTLA-4 plus
anti-PD(L)-1.
• Time to onset around 5-10 weeks into treatment, but onset timing can vary broadly (also after treatment
discontinuation).
Management:
• Rule-out alternative etiologies (infection, metabolic, autoimmune). Instruct patients and caregivers to inform at first
signs. Useful GI consultation for irAE > Grade 2.
• Treatment based on grade of ir-AE:
- Grade 1 monitor, symptomatics
- Grade 2: hold ICI, oral/IV steroids
- Grade 3-4: hold ICI, IV steroids; other immunosoppressors for refractory irAE
Darnell Eli P, et al, Curr Oncol Rep 2020Clinical case
11 Sep 2020 diarrhoea G2 →coprocolture was negative; blood tests normal, no other etiologies
→hold cemiplimab and start oral steroid (prednisone 1mg/kg)
15 Sep Contact phone: good clinical conditions, no stools →we recommend to continue oral steroid
21 Sep 2020 visit at our Center: worsening of clinical conditions, astenia (G1). The patient reports relapse of
diarrhoea (4 stools/die) since yesterday (the patient has stopped steroid for 4 days), Blood test show
hypokalemia (G1).QUESTION #2
Quale comportamento seguire:
Risposta 1: Per la persistenza dell’evento avverso, il paziente può essere considerato refrattario agli steroidi,
pertanto è opportuno intraprendere terapia con altri immunosoppressori (infiliximab), e sospendere
definitivamente il trattamento immunoterapico
Risposta 2: Consultare un gastroenterologo ed eventualmente eseguire ulteriori indagini, riprendere terapia
steroidea per via parenterale
Risposta 3: Riprendere terapia con steroidiClinical case
21 Sep 2020 visit at our Center: worsening of clinical conditions, astenia (G1). The patient reports relapse of
diarrhoea (4 stools/die) since yesterday (the patient has stopped steroid for 4 days), Blood
test show hypokalemia (G1).
→ supportive therapy, tests exclude infections or other etiologies (GI consultation,
suggeted colonscopy that patient refuses) →restart steroid therapy (intramuscolar)
28 Sep 2020 good clinical conditions, resolution of toxicity → slow tapering of steroid therapyKEY TAKE AWAYS • To prevents irAEs: select patients and identify dysimmunity risk factor. • In case of AEs: rule out other etiologies, initiate prompt and appropriate treatment and eventually hold immunotherapy based on irAE grade (role of multidisciplinary team). A prompt identification and appropriate management can reverse many of irAEs, thus allowing to resume immunotherapy after irAEs resolution. • Slow tapering of steroid therapy is crucial to avoid IrAEs rebound. • Educate patients and caregivers on signs and symptoms of irAEs, stress the importance of early identification and reporting, and report every non conventional coumpounds they are taking. • In the next future, novel platform/methods of quantitative image analysis might hopefully provide information from macroscopic imaging features potentially predictive of clinical outcome in term of response or toxicity (predicting individual patient’s risk of developing irAEs or detecting toxicities before the clinical manifestation of irAEs).
Medical Oncology and Immunotherapy
Center for Immuno-Oncology
University Hospital of Siena - Italy
• Maresa Altomonte Michele Maio • Giovanni Amato
• Luana Calabrò • Sara Cannito
• Maria Grazia Daffinà • Sandra Coral
• Riccardo Danielli • Alessia Covre
• Anna Maria Di Giacomo • Ornella Cutaia
• Elisabetta Gambale • Carolina Fazio
• Santa Monterisi • Gianluca Giacobini
• Giulia Rossi • Elisa Ibba
• Monica Valente • Andrea Lazzeri
• Angela Iacovelli • Maria Lofiego
• Marilena Piccinelli • Fabbrizio Nardi
• Roberta Crispino • Claudio Rosati
• Vincenso Di NuzzoYou can also read

















































