Biomarcatori nel tumore del colon-retto: PASSATO, PRESENTE e FUTURO NOVITA' IN TEMA DI TUMORI DEL COLON - AIOM
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
NOVITA’ IN TEMA DI TUMORI DEL COLON
Biomarcatori nel tumore del colon-retto:
PASSATO, PRESENTE e FUTURO
MONICA NIGER
ISTITUTO NAZIONALE DEI TUMORI
MILANO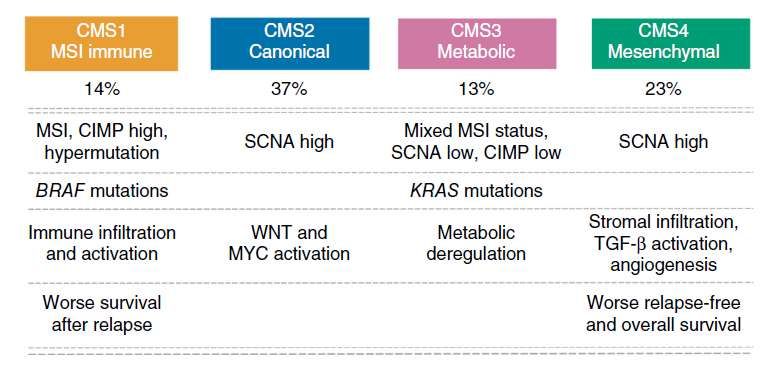
AGENDA
PAST AND PRESENT BIOMARKERS FOR mCRC
RAS
BRAF
FUTURE BIOMARKERS FOR mCRC
CMS
HER2
ALK/ROS/panTRK/ RET
MSI
MGMT
AGENDA
PAST AND PRESENT BIOMARKERS FOR mCRC
RAS
BRAF
FUTURE BIOMARKERS FOR mCRC
CMS
HER2
ALK/ROS/panTRK/ RET
MSI
MGMT
PAST (and PRESENT)
Extracted from Van Cutsem et al. Ann Oncol 2016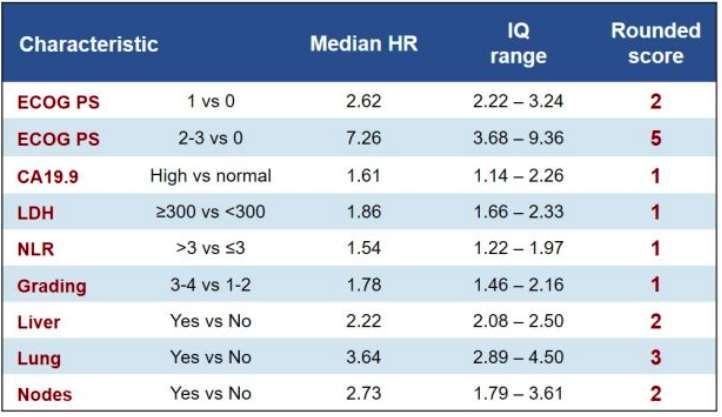
RAS in short
KRAS-mut (ex 1- 4) represent 35% of mCRC population and are predictive of
anti-EGFR resistance and NRAS-mut (ex 1-4)
NRAS-mut (ex 1- 4) represent 20% of mCRC population and are predictive of
anti-EGFR resistance
Sorich MJ et al 2014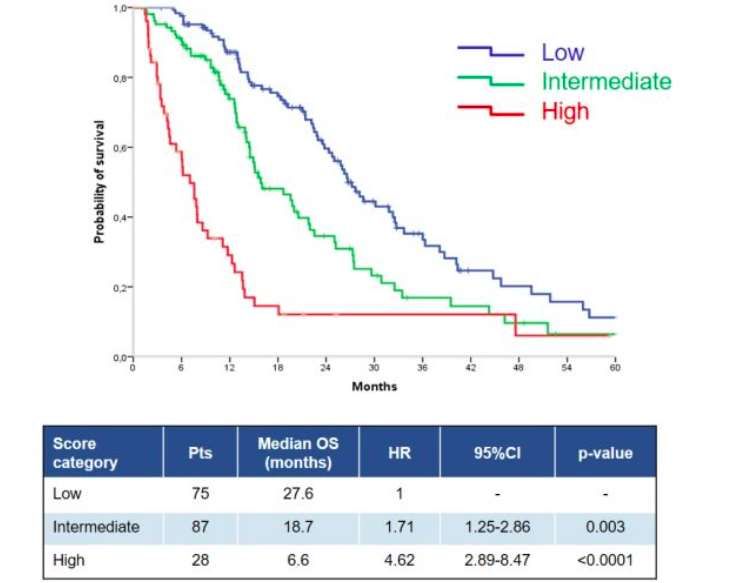
BRAF in short
BRAF-mut is a rare (8 - 10%) and aggressive molecular mCRC subtype.
Anti-EGFRs (w/o chemotherapy) and BRAFi (w/o MEKi) have limited activity
Preclinical and early phase 1/2 evidences suggested that anti-EGFRs plus BRAFi
targeted combinations have encouraging activity and a manageable safety profile.
Addionally, preclinical and early phase 1/2 evidences suggested that the addition
of irinotecan to cetuximab-vemurafenib is tolerable and may further increase
activity
Data from randomized clinical trials are still lacking
Not all BRAF are the same: non-V600E BRAF mutation (ex codon 594 and 596
mutant) have longer OS when compared to BRAF V600E
Pietrantonio et al, EJC 2015; Corcoran JCO 2015; Corcoran et al, ESMO 2016;
Yaeger CCR 2015; Hong et al, Cancer Discov ’16; Cremolini, Annal Onc 2015; Jones J.c. et al JCO 2017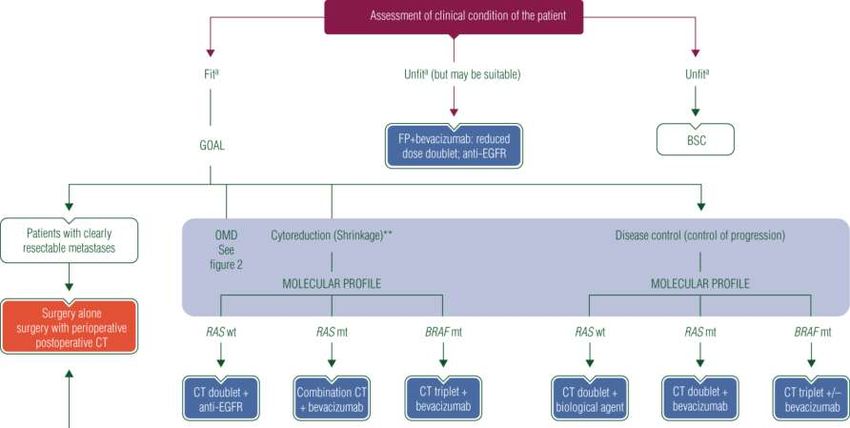
BRAF, BeCool
Multicenter retrospective study 395 BRAFm mCRC pts enrolled!
OS
OS
Loupakis et al. AIOM 2017
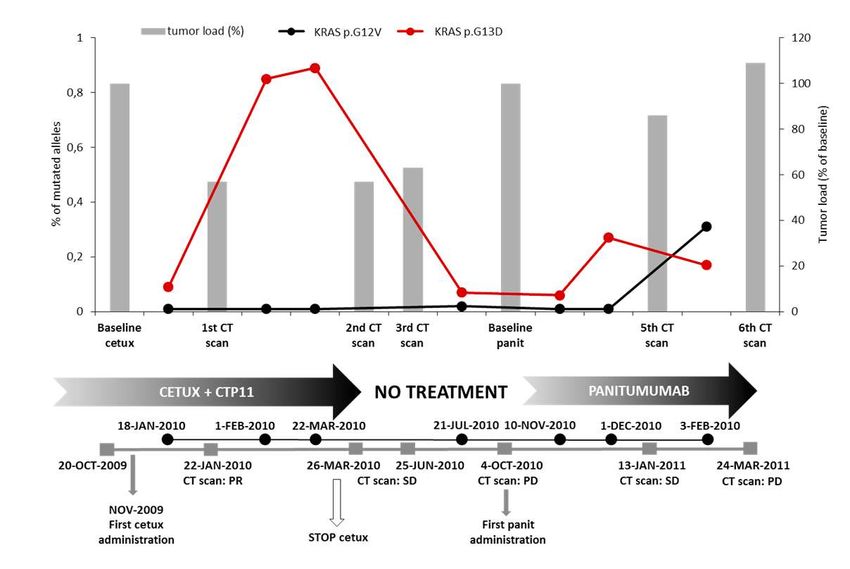
RECHALLENGE - rationale
Siravegna et al, Nature Medicine 2015
RECHALLENGE - Cricket
Cetuximab Rechallenge in Irinotecan-pretreated mCRC, KRAS, NRAS and BRAF
wild-type treated in 1st line with anti-EGFR Therapy.
PD PD
mCRC pts
FOLFIRI/ FOLFOX/XELOX/
Irinotecan
RAS and BRAF wt FOLFOXIRI FOLFOXIRI
+ Cetuximab
+ Cetuximab + Bevacizumab
Rossini et al. ASCO 2018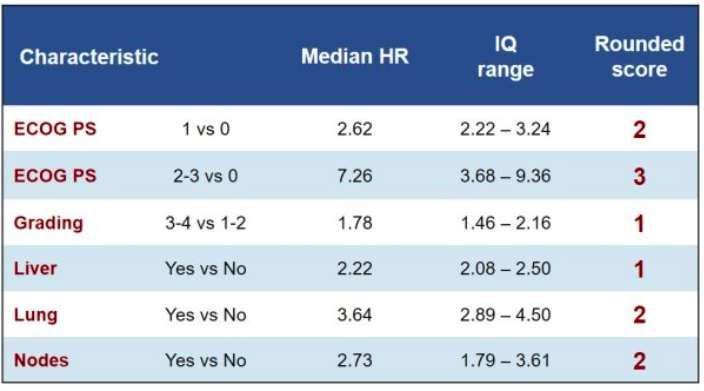
RECHALLENGE - CHRONOS
A Phase II Trial Of ReCHallenge With Panitumumab DRiven by RAS
ClONal-Mediated Dynamic Of ReSistance: The CHRONOS Trial
1st line including anti-EGFR 2nd line rechallenge
RATIONALE: expansion of extended-RAS RAS Baselineclones
Mutational Load
is the principal culprit of anti-
% mut RAS clones
EGFR acquired resistance, and these (BML) clones decay upon anti-EGFR treatment
RAS Intermediate
withdrawal, while tumor cells regainMutational sensitivity
Load (IML)to anti EGFR treatment.
RAS Rechallenge
Individuals who benefit from multiple challenges with anti-EGFR antibodies
Mutational Load
exhibit pulsatile levels of mutant time RAS. The CRC (RML)genome therefore adapts
Pre-Screen Molecular Screening Trial
dynamically to intermittent
1.Documented WT RAS exons 2, 3
anti-EGFR drug schedules
1. Imaging documented progression while
providing a molecular
1.Imaging documented progression at
explanation for the efficacy of
and 4 and BRAF V600E; on, re-challenge therapies
or within 6 months from first line based onchemotherapy
a 2nd line EGFR blockade
(regorafenib is
2.Complete or partial response to therapy including anti-EGFR mAb; allowed);
frontline chemotherapy including 2. A RAS-extended mutational load with > 2.A RAS-extended mutational load
anti-EGFR mAb 3% fractional abundance, measured on measured on plasma ctDNA at RML
plasma ctDNA at BML (maximum within (maximum within 1 week from 2nd
1 week of 1st line progression); line progression);
3. A planned 2nd line chemotherapy of any 3.A > 50% drop in RAS-extended
type with the exclusion of further anti mutational load between BML and
Tumor sensitivity to anti-EGFR EGFRs. RML;
sensitive resistant
EudraCT n. 2016-0902597-12PRESSING PANEL
Pz PRIMARIAMENTE RESISTENTI Pz RESPONSIVI
a anticorpi anti-EGFR
vs a anticorpi anti-EGFR
* Progrediti entro e non oltre 3 mesi di ** RP/SD confermata in almeno 2 TC durante anti-
trattamento contenente un anti-EGFR moAb EGFR in monoterapia o irinotecano+cetuximab in pz
chiaramente irinotecano-refrattari
• Amplificazione e mutazioni di HER-2,
• Amplificazione di MET,
• Fusioni di TRK/ROS/ALK/RET,
• Mutazioni attivanti dell’asse PIK3CA/PTEN/Akt e MAPKs
Cremolini et al, Annals Oncol 2017RESISTANT GROUP SENSITIVE GROUP
PRESSING PANEL
Progression Free Survival Overall SurvivalAGENDA
PAST AND PRESENT BIOMARKERS FOR mCRC
RAS
BRAF
FUTURE BIOMARKERS FOR mCRC
CMS
HER2
ALK/ROS/panTRK/ RET
MSI
MGMTCONSENSUS MOLECULAR SUBTYPES
Guinney J et al, Nature Med 2015CMS step 2
Mooi et al, ESMO ‘17
Smeby et al, Ann Oncol 2018HER 2: A HAPPY ENDING
27 HER-2 +, KRAS wt mCRC pts
progressed after fluoropyrimidine, Trastuzumab +
PD
oxaliplatin, irinotecan and Lapatinib
an anti-EGFR moAb
Phase II, primary endpoint: ORR (Recist 1.1)
Change in target lesion from baseline (%)
HER2 +
3%
SD
Objective Response space ( > 30% shrinkage)
Sartore Bianchi et al, Lancet Oncology ‘16ENTRECTINIB
Entrectinib is a pan-TRK, ROS1
and ALK inhibitor.
Combined analysis of two
Phase-1 Trials (ALKA-372-001
and STARTRK-1).
ALK/ROS1/NTRK
0.2%- 2.4%
Drilon et al, Cancer Discov 2017; Sartore-Bianchi et al, JNCI 2015; Amatu et al, BJC 2015FUSIONS in mCRC
Female
Older Age
Right colon
Lymph nodes mets
RAS&BRAF wt
MSI-high
Pietrantonio et al, JNCI 2017RET: PROGNOSTIC IMPACT
RET+
IHC FISH
< 1%
Pietrantonio et al, Ann Oncol 2018MSI AND IMMUNOTHERAPY
MMRD predicts response to immunotherapy...
MSI
15%
Le et al, N Eng J Med 2015; Le DT et al Science 2017MSI AND IMMUNOTHERAPY
…while there is low benefit for MSS CRC
Author Drug Population ORR
Topialan et al Nivolumab Refractory CRC 0% (n=19)
Le et al Pembrolizumab MSS CRC 0% (n=18)
Nivolumab +
Overman et al MSS CRC 5% (n=20)
Ipilimumab
Chung et al Tremelimumab Refractory CRC 2% (n=49)
Topialan et al, N Eng J Med, 2012
Le et al, N Eng J Med 2015
Overman et al, J Clin Oncol 2016
Chung et al, J Clin Oncol, 2016MSI AND IMMUNOTHERAPY
Nivolumab OS in MSI-H
Overman et al, ASCO GI 2018
Median OS [95% CI], months NR [19.6, NE]
12-month OS rate [95% CI], % 72 [60.0, 80.9]
18-months OS rate [95% CI], 67 [54.9, 76.9]
Nivolumab and ipilimumab efficacy in MSI-H
Median OS [95% CI], months NR [18, NE]
Thierry Andre et al, ASCO GI 2018 9 -month OS rate [95% CI], % 87 [80.0, 92]
12-months OS rate [95% CI], 85 [77.0, 90.2]ARE WE SURE?
Germano et al, Nature 2017MGMT
methylation MGMT in mCRC
40%
n(MGM RR DCR PFS mo OS mo
Ref. Schedule
T-m) (MGMT-m) (MGMT-m) (MGMT-m) (MGMT-m)
Amatu et al DTIC 250 mg/m2 per
day, d 1-4 q21d
68 (26) 3% (8%) 12% (44%) 1.7 (NR) /
Clin Cancer R. 2013
Hochauser et al TMZ 150 mg/m2 per
day 7 d on/7 d off
372 (37) 3% (3%) 44% (44%) / /
Mol Can Ther 2013
Pietrantonio et al
Ann Oncol 2014
TMZ 150 mg/m2 per
day d 1-5, q28d 323 (32) 12% (12%) 31% (31%) 1.8 (1.8) 8.4 (8.4)
Pietrantonio et al TMZ 75 mg/m2 per
24% (24%) 30% (30%) 2.2 (2.2) /
day, d 1-21 q28d 214 (21)
Target Oncol. 2016
TMZ 200 mg/m2
Amatu et al days 1-5 q28 150 (29) 3.4% (3.4%) 48% (48) 2.6 (2.6) 6.2 (6.2)
Ann Oncol 2016
TMZ 150-200 mg/m2
Calegari et al d 1-5, q28d 225 (41) 10% (10%) 32% (32%) 1.9 (1.9) 5.1 (5.1)
Br J Cancer 2017
TMZ 150 mg/m2per
Morano et al day, d 1-5
25 (25) 24% (24%) 70% (70%) 4.4 (4.4) 13.8 (13.8)
Ann Oncol 2018 q28d+Irinotecan 100
mg/m2 d1, 15 q 28dMGMT
methylation MGMT in mCRC
40%
n(MGM RR DCR PFS mo OS mo
Ref. Schedule
T-m) (MGMT-m) (MGMT-m) (MGMT-m) (MGMT-m)
Amatu et al DTIC 250 mg/m2 per
day, d 1-4 q21d
68 (26) 3% (8%) 12% (44%) 1.7 (NR) /
Clin Cancer R. 2013
Hochauser et al TMZ 150 mg/m2 per
day 7 d on/7 d off
372 (37) 3% (3%) 44% (44%) / /
Mol Can Ther 2013
Pietrantonio et al
Ann Oncol 2014
TMZ 150 mg/m2 per
day d 1-5, q28d 323 (32) 12% (12%) 31% (31%) 1.8 (1.8) 8.4 (8.4)
Pietrantonio et al TMZ 75 mg/m2 per
24% (24%) 30% (30%) 2.2 (2.2) /
day, d 1-21 q28d 214 (21)
Target Oncol. 2016
TMZ 200 mg/m2
Amatu et al days 1-5 q28 150 (29) 3.4% (3.4%) 48% (48) 2.6 (2.6) 6.2 (6.2)
Ann Oncol 2016
TMZ 150-200 mg/m2
Calegari et al d 1-5, q28d 225 (41) 10% (10%) 32% (32%) 1.9 (1.9) 5.1 (5.1)
Br J Cancer 2017
TMZ 150 mg/m2per
Morano et al day, d 1-5
25 (25) 24% (24%) 70% (70%) 4.4 (4.4) 13.8 (13.8)
Ann Oncol 2018 q28d+Irinotecan 100
mg/m2 d1, 15 q 28dTHE TEMIRI STUDY
mPFS 4.4 mos mOS 13.8 mos
N/Events 25/22 m
N/Events 25/15
Morano et al. Ann Oncol 2018THE RELEVANCE OF A BIOMARKER
• ALL MGMT-positive IHC patients were non-responders
• MGMT-negative/low IHC tumors had a longer mPFS
Morano et al. Ann Oncol 2018LOOKING FOR MORE
TRASLATIONAL/CLINICAL PRACTICE
RAS
BRAF
SINGLE MOLECULAR
MSI MGMT
HER2 ALTERATIONS
multiple molecular alterations
ALK/ROS1/NTRK/RET
HYPERMUTATED MULTIPLE MOLECULAR
CIMP-H ALTERATIONS
pathways of genomic instability
CONSENSUS
RESEARCH
MOLECULAR GENE EXPRESSION
SUBTYPES ANALYSES
Courtesy of F. MoranoRET: PROGNOSTIC IMPACT
Pietrantonio et al, Ann Oncol 2018You can also read