Assessment of Implementation of Janani Suraksha Yojna (JSY) - Sonitpur district, Assam
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Assessment of Implementation of
Janani Suraksha Yojna (JSY)
Sonitpur district, Assam
Human Rights Law Network
576 Masjid Road, Jangpura Bhogal
New Delhi-110014
1
Contents
l. Introduction: .............................................................................................................................................. 3
1.1. Background: ....................................................................................................................................... 4
1.2. Important Feature of JSY: ................................................................................................................. 5
a) Tracking Each Pregnancy: ................................................................................................................. 5
b) Eligibility for Financial Assistance: .................................................................................................... 5
c) Scale of Financial Assistance: ............................................................................................................ 5
(d) Disbursement of financial assistance to beneficiary for institutional delivery: .............................. 6
2. Methodology of the Study: ....................................................................................................................... 7
3. Sontipur District Profile: ............................................................................................................................ 7
4. Indicators: ................................................................................................................................................. 8
4.1. Awareness of JSY schemes: ................................................................................................................ 8
4.2. Registration of pregnant women under JSY: ..................................................................................... 9
4.3. Institutional Deliveries: .................................................................................................................... 12
4.4. Antenatal and Post Natal Care: ........................................................................................................ 13
4.5. Referral Transport facilitates: .......................................................................................................... 16
4.6. Receipt of Financial Assistance under JSY: ....................................................................................... 17
5. Issue of concerns:................................................................................................................................ 19
5.1. Lack of referral transport services: .................................................................................................. 19
5.2. Poor antenatal care and post natal care: ......................................................................................... 19
5.3. Non Receipt of JSY cash assistance .................................................................................................. 22
6. Findings: ................................................................................................................................................. 24
2
l. Introduction:
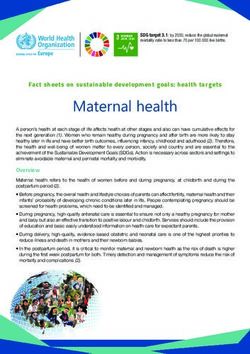
Maternal death is one of the biggest issues of concern in India. As reported in Indian
Express dated May 7, 2014 ‘India recorded highest number of maternal deaths in the
world with 17 per cent or nearly 50,000 of the 2.89 lakh women who died as a result
of complications due to pregnancy or childbearing in 2013. ’ The World Health
Organization (WHO) defines maternal death as, “the death of a woman while
pregnant or within 42 days of termination of pregnancy, irrespective of the duration
and the site of the pregnancy, from any cause related to or aggravated by the
pregnancy or its management but not from accidental or incidental causes.” Further
WHO reported that India’s MMR, has reduced from 560 in 1990 to 178 in 2010-
2012, the country is unlikely to meet its MDG target of 103.1 Many experts agree
that the drop in maternal mortality cannot be attributed to any government
intervention, but in fact is linked to a reduction in deliveries. Simply, if fewer women
become pregnant, fewer women will die.
To combat the increasing maternal mortality rate (MMR), and to provide basic
primary health care delivery system in rural areas, Government of India (GOI)
introduced National Rural Health Mission (NRHM) in 2005 which is now National
Health Mission (NHM). The main objective is to provide effective, equitable and
affordable quality health care services to the rural population.
Assam recorded highest maternal death in India, 328 (Sample Registration Survey
2010-2012) as compared to 178 for rest of India. As reported in Assam State
Programme Implementation Plan (PIP) for the year 2014-2015, the total MMR
recorded was 347 (AHS 2011-2012) whereas the state target was 210. Again the
1
lbid
3
state target for the year 2015-2016 is 328 (2010-2012 SRS) and the total MMR
recorded was 194.2 This clearly shows the state failure to achieve the target of
reducing MMR.
Two factors are responsible for Assam’s high rate of maternal death: Social factors
(child marriage) and Institutional factors (lack of awareness, non implementation of
government maternal benefit schemes, and lack of road connectivity to the nearest
health centers, poor antenatal care). In this background, social activists from the
Human Rights Law Network (HRLN) conducted a fact-finding in Sonitpur district,
Assam with the objective of finding out gaps in health services availability and in
accessing health services in the district. This report uncovers failures to implement
JSY in Sonitpur district.
1.1. Background:
With the objective of reducing maternal and neo-natal mortality, NHM introduced
Janani Suraksha Yojana (JSY). JSY is cash assistance, safe motherhood intervention
under the overall umbrella of (NHM). “It has been initiated by modifying the
existing National Maternity Benefit Scheme (NMBS). While NMBS is linked to the
provision of better diet for pregnant women from BPL families, JSY, integrates the
financial/cash assistance with antenatal care during the pregnancy period,
institutional care during delivery and immediate post-partum period in a health
centre by establishing a system of coordinated care by ASHA, the field level
workers. It is a fully centrally sponsored scheme.”3
2
Assam State PIP, 2014-2015, Chapter 1, page no 1
3
Operational Guidelines for Implementation of JSY, NHM
4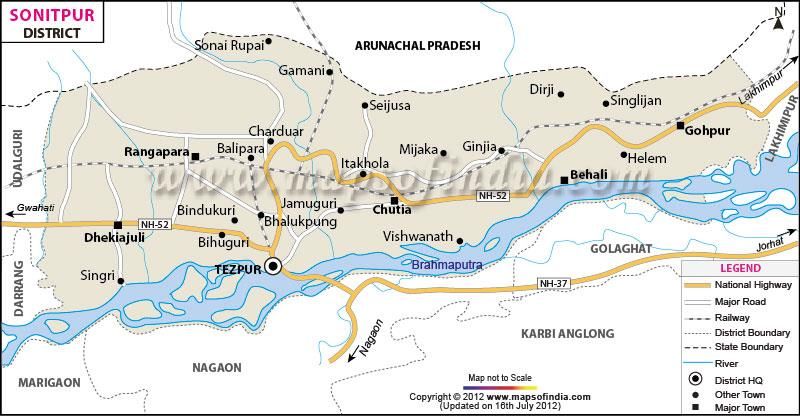
1.2. Important Feature of JSY: 4
a) Tracking Each Pregnancy:
Mothers who are registered under the scheme should have a JSY card along with a
Maternal and Child Health (MCH) card. ASHA / AWW/ any other identified link
worker under the overall supervision of the ANM and the MO PHC should prepare
a micro-birth plan effectively helps in monitoring Antenatal Check-up, and the post
delivery care.
b) Eligibility for Financial Assistance:
All pregnant women delivering in Government health centers like Sub-centre, PHC,
CHC/ FRU/ General wards of Sub Divisional, District and State Hospitals and Govt.
medical colleges will get covered under JSY benefits. Apart from the government
health centers, deliveries taking place in Municipal Hospitals and In case of
Accredited Private Institutions, only those families who have genuine BPL cards (as
per last approved BPL census) or SC/ST certificate(issued by concerned Tehsildar)
will be eligible for the benefits.
c) Scale of Financial Assistance:
JSY BENEFIT FOR INSTITUTIONAL DELIVERIES
(in Rupees)
Rural Urban
4
5Categor Assistanc Assistance Total Assistanc Assistance Total
y of e to to ASHA e Mother to ASHA
States mother
LPS* 1400 600 2000 1000 400 1400
HPS** 700 600 1300 600 400 1000
* Low Performing States (LPS) include Assam, Bihar, Chhattisgarh, Jammu &
Kashmir, Jharkhand, Madhya Pradesh, Odisha, Rajasthan, Uttar Pradesh, and
Uttaranchal.
** High Performing States (HPS) include all states that are not LPS.
(d) Disbursement of financial assistance to beneficiary for institutional delivery:
1. The financial assistance provided to mother under JSY meets the cost of
delivery and should be disbursed effectively at the institution itself.
2. All the pregnant women need to open a separate bank account to manage JSY
funds in any nationalized bank under the concerned Rogi Kalyan Samiti.
3. At the time of institutional delivery, payment ofRs.1400/- and above made to
the beneficiary will be done through cheque and not in cash. The cheque
would be jointly signed by the Medical Officer and a paramedic staff like Staff
Nurse or Health Worker (female), preferably the senior most in the hospital.
The signatories for the different categories of health institutions are outlined
below.
62. Methodology of the Study:
Lawyers and Social Activist from HRLN conducted fact-finding in Oct, 2014. The
fact-finding team surveyed six Tea Estate Hospitals, one village, and two PHCs in
the Blocks of Rangapara, and Biswanath Chariali. There was a second follow-up
fact-finding conducted in May, 2015 in the Blocks of Rangapara, Balipara, and
Biswanath Chariali. Both reports illustrated the Respondents’ utter failure to
implement the JSY scheme and highlighted the grim health situation of the state’s
female and adolescent population. This fact finding report is based on both primary
and secondary source of information. Interviews were used as the primary method
to collect information in the fact finding visit. Apart from the primary data, we also
analysed reports, literature as secondary sources of information.
3. Sontipur District Profile:
7Sonitpur is an administrative district of Assam with its district headquater in
Tezpur. In 1835 Sonitpur attained district status as Darrang district. Later it was
bifurcated in 1983 and Sonitpur was formed. Agriculture is the main source of
livelihood. Almost 80% of the population depends on agriculture for their
livelihood. 5 Apart from agrarian economy, tea gardens are another main source of
livelihood. There are total 73 tea gardens in the district.
4. Indicators:
As mentioned above JSY was adopted under NHM with the objective to reduce
MMR and to provide health service to rural population. With these objectives it the
scheme was adopted with guarantees for the implementation. In this report we will
highlight the implementation of JSY in Sonitpur district considering the following
guarantees/indicators:
1. Awareness of JSY scheme
2. Registration of pregnant women under JSY
3. Institutional Deliveries
4. Ambulance/transport facilities
5. Antenatal and Post natal care
6. Receipt of Financial Assistance under JSY
4.1. Awareness of JSY schemes:
At every facility visited and by interviewing pregnant women, the fact-finding team
found that women were unaware of the JSY scheme, women who heard vaguely of
5
Assam Info available at http://www.assaminfo.com/districts/24/sonitpur.htm
8something similar and women did not think they would be eligible for such a scheme
due to conditionalities. Many women believed that they needed a bank account in
order to receive cash incentives, and others believed that they had too many children
to be eligible. Furthermore, women were not sure who to ask or where to find
information concerning the scheme. Without the cash incentive, the cost of an
institutional birth is out of reach for most families. Families pay for medicines,
fluids, and for operations in cases of caesarean births. This is problematic as JSY
cash incentives are given in an effort to overcome barriers to service use – such as
awareness and cost. On both counts the JSY scheme has not been serving its purpose
in Sonitpur District.
It is one of the responsibilities of ASHA to make the people aware of JSY schemes.
But when asked about guarantees under JSY schemes the interviewed women
reported that they only know that it is a cash assistance scheme and they will receive
the payment only when they opt for institutional delivery. Moreover, one of the
provision to promote JSY scheme under Reproductive and Child Health (RCH)
along with programme like Pulse Polio Programme, Monthly Village Health day,
etc by distributing pamphlets regarding JSY guidelines, at PHCs/CHCs/District
Hospital and private hospital, organizing meetings/workshops at village level.
Interviewed pregnant women and ASHA worker reported that though there are
guidelines of JSY at PHCs/CHCs/hospitals but they are in English and it is difficult
for them to read.
4.2. Registration of pregnant women under JSY:
One of the feature of the scheme is to register women are registered under JSY for
their antenatal care. It is the duty of ASHA/ANM/AWW to identify and register of
9beneficiary at least 20-24 weeks before expected date of delivery. After their
registration each beneficiary will get JSY. “ASHA and other line worker under the
supervision of ANM and MO of PHC should mandatorily prepare micro-birth plan.”6
Under micro-birth plan
ASHA work needs to fill JSY along with Maternal and Child Health (MCH)
card for the registered beneficiary.
Informing date of three ANC and TT
Identify health center for all referral
Identify place of delivery
Informed expected date of delivery
Submission of the completed JSY card in the health center for verification
by the authorized/MO
Taking necessary steps towards arranging transport or making available cash
to the beneficiary to come to the health center for delivery
Ensure availability of funds to ANM/ASHA/health worker
Payment of cash benefit/incentive to the mother and ASHA
Payment of last installment to ASHA and settlement of advance paid.
Thus identification and registration of beneficiaries under JSY is the first step
towards making health care available and accessible for the rural population. The
following table shows number of JSY registration for the year 2013-2014 and 2014-
2015.
6
Operational Guidelines for Implementation of JSY, NHM
10Table 1: Total number of women registered under JSY
Total number of Number of Women
% JSY registration to
pregnant women registered under
Total ANC Registration
Indicators Registered for ANC JSY
2013-14 2014-15 2013-14 2014-15 2013-14 2014-15
1 Balipara 4,031 3,820 4,031 3,818 100 99.9
2 Behali 2,343 2,196 2,343 2,205 100 100.4
3 Bihaguri 4,227 4,346 2,904 2,310 68.7 53.2
Biswanath
4
Chariali 3,608 3,542 3,608 3,542 100 100
5
Dhekiajuli 6,266 5,939 4,932 4,646 78.7 78.2
6 Gohpur 4,551 4,257 4,530 4,257 99.5 100
North
7
Jamuguri 3,257 3,479 2,812 3,387 86.3 97.4
8 Rangapara 1,691 1,707 1,686 1,705 99.7 99.9
Sonitpur
9
Urban 643 463 102 59 15.9 12.7
10 Total 30,617 29,749 26,948 25,929 88 87.2
Source: NHM, Health Management Information System (HMIS)
By considering all pregnant women are registered under the ANC, the above table
shows that the total number of pregnant women registered for ANC decrease in 6
PHC (Balipara, Behali, Bihaguri, Biswanath Charali, Dhekiajuli and Sonitpur urban)
out of 9. Also, JSY registration decrease in 6 PHCs out of 9. Thus from the above
table it is clear that two year trends shows the decrease ANC and JSY registration.
From the fact-finding the team found out that institutional reason (lack of medicine,
11non-availability of doctors, and lack of infrastructure, lack of awareness) are the
main factors responsible for decrease in registration.
4.3. Institutional Deliveries:
One of the objectives of the scheme is to promote institutional deliveries. As
mentioned above cash assistance of Rs 1400/- is given for institutional deliveries
and Rs. 500 for home deliveries. According to the DLHS-3 there are 1,116 villages
in Assam. Shockingly, 158 villages do not have a single JSY beneficiary. The
following table highlights the number of institutional and home deliveries in
Sonitpur.
Table 2: Total number of institutional and home deliveries for the year 2013-15
% Institutional
Total reported % Home deliveries to
deliveries to Total
deliveries Total Reported Deliveries
Reported Deliveries
Indicators
2013-14 2014-15 2013-14 2014-15 2013-14 2014-15
1 Balipara 2,022 1,863 65.3 63.5 34.7 36.5
2 Behali 2,421 2,228 89.8 91.9 10.2 8.1
3 Bihaguri 2,912 2,210 88.6 76.5 11.4 23.5
Biswanath
4 Chariali 3,130 3,467 86.6 87.8 13.4 12.2
5 Dhekiajuli 4,121 3,913 77 78.1 23 21.9
6 Gohpur 3,486 3,530 91.6 92.2 8.4 7.8
North
7 Jamuguri 1,678 1,656 65.6 63.1 34.4 36.9
8 Rangapara 1,104 1,192 74.8 69.9 25.2 30.1
Sonitpur
9 Urban 5,514 5,434 100 100 0 0
1210 Total 26,388 25,493 85.6 84.7 14.4 15.3
Source: NHM, Health Management Information System (HMIS)
Thus, from the above table it is clear that the total number of reported deliveries
decreases in 7 PHCs (Balipara, Behali, bihaguri, Dhekiajuli, North Lakhimpur,
Rangapara, Sonitpur Urban) out of 9. Out of the total reported deliveries, there is an
increase in home deliveries in 4 PHCs (Balipara, Bihaguri, North Jamuguri,
Rangapar) as compared to institutional deliveries. Further, in 4 PHCs (Balipara,
Bihaguri, North Jammuguri and Rangapara) institutional deliveries decreased. The
main factors which lead to decrease in the total rate of institutional deliveries are the
institutional failure (like lack of medicines, doctors, ambulance services, etc). We
also witness decreasing trend in the number of reported deliveries, one of the reasons
which are contributing to it is that many a state fails to register birth of a baby.
4.4. Antenatal and Post Natal Care:
Regarding minimum maternal health services, subcentres/PHCs should provide
pregnancy registration in the first trimester; at least four antenatal checkups (ANCs);
minimum laboratory services; identification and prompt referral of high-risk
pregnancies; iron folic acid (IFA) tablets and other services to combat anameia;
vaccinations (including TT); malaria prophylaxis in malaria epidemic zones,
counseling and referral for Reproductive Tract and Sexually Transmitted Infections
(RTI/STIs); provision of a range of contraceptives; and information about
government incentive schemes, such as NMBS, JSY, and JSSK. Minimum child
health services should include essential newborn care; immunizations; Vitamin A
13prophylaxis; and prevention and treatment of malnutrition, anameia, infections,
diarrhoea, and other common childhood health problems.7
The team found that many facilities lacked essential and lifesaving drugs per
government standards under NRHM. Basic medicines like paracetamol, common
antibiotics and essential drugs used post delivery and life-saving vaccines were
found unavailable or, according to staff, frequently out of stock at a sizeable number
of primary health centers (PHC), Community health centers (CHC), and TE
hospitals. Further, in an interview with ASHA/ANM, we found out that there is no
blood bank in PHCs. Although there are blood banks and operational, but for every
request for blood someone must donate blood. Otherwise the cost is 500 Rs. per liter.
In Sonipurt there are only two blood storage unit in Bishwanat Charali and Gohpur
each.
According to DLHS 3, percentage of women who received three ANC care was 51.0
in urban areas and 48.9 is rural area which shows a clear decrease when compared
to 50.9 (urban areas) and 49.0 (rural areas) in DLHS 2. Thus it is clear that out of
the total mothers only 48 % received ANC.
7
Id., pp. 8–14, 18, 26–31, 60 (Annexure 11); Government of India, NHRM 2005–2012 Framework,
Annexure II (“Service Guarantees for Health Care”).
14Women had Minimum of Three Ante-natal
Check-up by Residence
80.0
60.0 50.9 51.0 49.0 48.9
Percent
40.0
20.0
0.0
Total Rural
DLHS - 2 DLHS - 3
Source: DLHS 3
Post natal care:
Getting a Post partum / Post-natal check-up soon after the birth of baby or within 48
hours is crucial for the health of both the mother and the child. Accordingly, two
indicators, viz., percentage of mothers who received Post-natal check-up within 48
hours of delivery, percentage of mothers who received Post-natal check-up within
48 hours and 14 days of delivery have been calculated and presented. The follows
table shows the total percentage of women who received post natal care out of the
total reported deliveries in the district.
Table 4: Total number of women who received post natal care period for the year 2013-2015:
% Women discharged % Women getting
in less than 48 hours of Post Partum
delivery to Total Checkup between 48
Total reported Reported Deliveries at hours and 14 days to
Indicators deliveries public institutions Total Deliveries
152013- 2013-14 2014-15
2014 2014-2015 2013-2014 2014-2015
1 Balipara 2,022 1,863 57.3 56.9 68.5 67
2 Behali 2,421 2,228 41.7 28.6 71.1 96.6
3 Bihaguri 2,912 2,210 88.3 68.7 36.2 71.2
Biswanath
4 Chariali 3,130 3,467 85.8 31 78.9 71
5 Dhekiajuli 4,121 3,913 88.5 90.7 47.2 49.2
6 Gohpur 3,486 3,530 69.5 27.1 73.8 78
North
7 Jamuguri 1,678 1,656 19.9 21.6 84.6 96
8 Rangapara 1,104 1,192 98.5 98.7 82.5 92
Sonitpur
9 Urban 5,514 5,434 5.4 13.2 14 33.8
10 Total 26,388 25,493 56.5 41.3 54 65.3
Source: NHM, Health Management Information System (HMIS)
Thus from the above table it is clear that in 5 out of 10 PHCs the total number of
women failed to receive post natal care after delivery. One of the reasons for such
decrease is the state failed to provide institutional facilitates for the quality care.
4.5. Referral Transport facilitates:
Availability of transport facilitates is an important element for timely referral. In
Assam, though there are services of 108/102 but from our fact finding we found that
such referral transport are not available in the rural areas. Also, under this scheme,
it is the duty of ASHA to arrange transport services during emergency. In an
interview with the ASHA worker we found that most of the time there is no
ambulance services and hence families have to hire private cars or auto. This
increases the medical expenses incurred by the families. In Assam Referral transport
services in Assam mainly operate through the following services:
161. Emergency Response Services – Mrituynjoy 108
2. Inter Facility Medical Ambulances Services- 102-IFT( under process of
implementation)
3. Hospital Base existing Ambulances services.
In Sonitpur, there are 54 hospital based ambulance and 17 Mritunjoy services for
1.92 million population (as per 2011 census).
4.6. Receipt of Financial Assistance under JSY:
Under this scheme every mother is entitled to Rs 1400/- for institutional deliveries.
“All mothers irrespective of age, birth order or income group (BPL and APL) will
get cash assistance of Rs 1400/- in one go at the time of delivery. Also, BPL pregnant
women aged 19 years and above preferring to deliver at home by a Trained
Traditional Birth Attended or Skilled Attended is entitled to cash assistance of Rs
500 per delivery. Such cash delivery is available only for two live birth and the
disbursement would be done at the time of delivery or around four days before the
delivery.”8 To receive JSY benefits, women must present a BPL or SC/ST Card, a
JSY Card, and a referral slip from an ASHA worker, Accredited Nurse Midwife
(ANM), or Medical Officer (MO). If the BPL certification is not available through
a legally constituted process, the beneficiary could still access the benefit on
certification by the Gram Panchayat/pradhan provided the delivery takes place in a
government institution. The new mother should be able to retrieve her financial
entitlement at the hospital’s cash counter at the time of discharge or access her cash
from the ASHA, ANM, or other health worker within seven days of delivery.
8
Operational Guidelines of JSY, NHM
17JSY BENEFIT FOR INSTITUTIONAL DELIVERIES
(in Rupees)
Rural Urban
Category Assistance Assistanc Total Assistanc Assistance Total
of States to mother e to e Mother to ASHA
ASHA
LPS* 1400 600 2000 1000 400 1400
HPS** 700 600 1300 600 400 1000
* Low Performing States (LPS) include Assam, Bihar, Chhattisgarh, Jammu &
Kashmir, Jharkhand, Madhya Pradesh, Odisha, Rajasthan, Uttar Pradesh, and Uttaranchal.
** High Performing States (HPS) include all states that are not LPS.
JSY Guidelines states: “as the cash assistance to the mother is mainly to meet the
cost of delivery, it should be disbursed effectively at the institution itself.”
Consistently, the team learned that women were unable to take advantage of the JSY
scheme because they did not have bank accounts and/or could not deposit cheques.
Furthermore, all the centers stated that women would receive their JSY payment one
week after the delivery. However the Centre Government guidelines provide: “the
mother and the ASHA (wherever applicable) should get their entitled money at the
health center immediately on arrival and registration for delivery.”
JSY is centrally funded and each state prepares its budget for JSY on the basis of
fund requirements for the district and below level institutions.
In 2013-2014 total 26,948 (in lakh) mothers registered under JSY and out of the total
beneficiary 314 (in lakh) mothers received cash assistance of Rs 1400/- for
18institutional deliveries and 6.54(in lakh) population received cash assistance of RS
500/- for home delivery. For the year 2014-2015, the total number of JSY beneficiary
decreased to 25,929. However, out of the total JSY beneficiary only 369 mothers
received cash assistance of Rs 1400/- and 5.37 mothers received cash assistance of
Rs 500 for home deliveries.9
5. Issue of concerns:
The following are the major issue of concerns:
5.1. Lack of referral transport services:
During an interview with the ASHA/pregnant women, informed that many times
during emergency ambulance services are not available. So the families have to hire
private vehicles to reach to the health centers. This clearly indicates the JSY
guarantees of providing free referral transport services. As mentioned above in
Sonitpur, there are 54 hospital based ambulance and 17 Mritunjoy services for 1.92
million populations (as per 2011 census).
5.2. Poor antenatal care and post natal care:
Under the scheme every woman is entitled to the three ANC and treatment of
anemia, malaria, High BP, STI, HIV,etc. From our fact finding visit, we found that
that Anemia is one of the major factor contributed for maternal death in Assam. Due
to lack of blood bank or blood storage unit in the district it is difficult to treat anemia
patient because of the severe anemic patient, blood transfusion is required.
9
Assam State PIP (2013-2014) and (2014-2015)
19Case Studies:
Purnima
Purnima died on 6th December,
2014 in her eight month of
pregnancy. She was pregnant with
her first child after two years of
marriage. She belongs to Below
Poverty Line (BPL) family and
could afford to eat twice a day. The
ASHA worker told the fact finding
team that Purnima suffered from
malnourishment and anemia.
For her antenatal care she was registered at Sonajuli tea estate hospital under Janani
Suraksha Yojna (JSY). Janani Suraksha Yojana (JSY) is a safe motherhood
intervention under the National Rural Health Mission (NHM) implemented with the
objective to reduce maternal and neonatal mortality by promoting institutional
delivery among poor pregnant women. Purnima’s pregnancy check up reports
diagnosed some potential complications in her pregnancy. Her medical report
revealed that she was suffering from moderate amount of anemia with a
haemoglobin rate of 8.6 gm/dl (as recorded in May, 2014) According to National
Family Health Survey (NFHS) 3 a pregnant woman should have a hemoglobin rate
between 10-10.9 gm/dl.10 Further, NFHS classified three type of anemaia – anemia,
moderate and severe and she falls under moderate anemia category. Due to severe
10
National Family Heath Survey (NFHS3), 2005-2006 published by International Institute of
Population Science.
20anemia she was constantly sick and breathless during her pregnancy with swollen
legs.
The tea estate hospital referred her to the nearest facility with a blood bank,
Rangpara Primary Health Centre 35 km from her residence. According to National
Health Mission (NHM) guidelines, all villages should have a PHC within a 10 km
radius. When the fact finding visited the tea garden area, we advised Poornima and
ASHA worker to take her to the hospital for blood transfusion. Purnima received
just 5 units of blood during her pregnancy. Before the team visit no one counseled
her or reffered her for blood transfusion despite suffering from anemia.
Rajini Satwal:
Ranjini Satwal admitted at Kanaklata Civil Hospital, Tezpur on 17/04/2015 for her
delivery and a male child was born to her that day. Her hemoglobin was 6 on that
day and she was advised for 2 units of blood and charged Rs.3500/ per unit by one
nurse of the maternity ward. As the patient is from a poor family and her husband is
working as a day laborer and earns Rs.500/ per week, she could not afford to pay for
the same. She was discharged from the hospital on 20th April, 2015. At the time of
discharge the staff nurse had forcefully insisted the victim to sign one paper where
it was written that no amount of Rs.1400/ will be received by her for the institutional
delivery. The team was also informed that Ranjini had not received any postnatal
check up as well.
21Leelaboti Kor, age 24
Lelavathi gave birth
to her first child at
12:26 PM, hours
before the team
arrived. Her pre-natal
care consisted of a
Tetnus Toxic (TT)
injection and folic
acid and iron supplements during her pregnancy. She lives three miles from the PHC
and came in a 108 ambulance, which arrived 15 minutes after it was called brought
her to the facility. Her mother-in-law accompanied her. She had a natural birth with
an episiotomy, or cutting of the perineum. Lelavathi will be discharged in 48 hours.
She was in the post-natal wing, which had two dogs sitting in the entranceway. There
was one bathroom at the end of the room, but it had not been cleaned recently. She
brought her own sheets and was wearing the clothes she delivered in despite her
fresh sutures.
5.3. Non Receipt of JSY cash assistance:
As mentioned above under JSY women received cash assistance of Rs 1400/- for
institutional deliveries and Rs 500/- for home delivers. During our fact finding visit
we found that most mother do not receive their payment after the delivery.
22Case Study:
Jyoti, age 22-23
When the team spoke to Jyoti,
she was about to deliver her
second child. She has a five
year old daughter. She is a
temporary worker at the TE.
She stopped working at the end
of the season, which coincided
with her pregnancy. She has not
worked during her pregnancy,
and does not have immediate
plans to return to work after
giving birth. Her labor pains had just started when the team interviewed her. She
came to the TE hospital with her mother-in-law. She received monthly check ups at
the TE hospital, for which she came alone and she took vitamins that were given to
her. The ASHA registered her pregnancy. Her father-in-law works in the hospital at
the dispensary. Her first child was born at home, she would have had this child at
home as well, however, she experienced some pain and came in for a checkup. The
hospital staff told her to stay as she would be delivering in the next few days, and
the pain was continuing. She did not use any spacing/contraception methods between
pregnancies. She is unaware of such methods, and has not considered her family
planning options after this delivery. She is furthermore unaware of where to access
contraception; she said no one talks about it. She was not aware of the specifics of
JSY, though she had heard of something similar from a friend. She said she is unable
to collect such a payment because she does not have a bank account.
23Seenimai, age unknown
Seenimai gave birth to a baby girl on 7th July, 2013. She traveled one hour in a hired
vehicle, costing her Rs. 350, to reach the CHC. This was her third child. She
delivered her first two at home. During her pregnancy, she traveled to the CHC once
a month for checkups. She decided to have an institutional delivery for this birth
because the ASHA worker told her she could get money. When the team spoke to
her, she had not received her JSY money. She has never used spacing methods and
she has no plan to do so in the future, though she does not want any additional
children.
6. Findings:
From the fact finding we found out that
1. Though the government has drafted guidelines for implementation of JSY
guidelines but such guidelines and information are in English. Women only
know that JSY is a cash assistance programme for institutional deliveries.
2. At every facility visited the fact-finding team found women who were
unaware of the JSY scheme, women who had heard vaguely of something
similar and women did not think they would be eligible for such a scheme due
to conditionalities. Many women believed that they needed a bank account in
order to receive cash incentives, and others believed that they had too many
children to be eligible. Furthermore, women were not sure who to ask or
where to find information concerning the scheme. Without the cash incentive,
the cost of an institutional birth is out of reach for most families. In Assam,
the average cost of delivery is Rs 1574.4. Families pay for medicines, fluids,
and for operations in cases of caesarean births. This is problematic as JSY
24cash incentives are given in an effort to overcome barriers to service use –
such as awareness and cost. On both counts the JSY scheme has not been
serving its purpose in Sonitpur District.
3. There is no monitoring system to review the payment scheme inorder to
ensure that disbursement is timely and effective.
4. Government of Assam receives funding for JSY implementation to ensure
adequate manpower, infrastructure of beds, operation theatres and drugs at
each service unit level. This funding is not being utilized appropriately
evidenced by lack of on the ground implementation, including understaffed
hospitals, an inadequate number of beds and drugs, and the large number of
women who are unable to access their cash incentives. Almost 20% of PHCs
in Assam do not have a doctor. At the CHC level, only 49% of the required
specialist posts have been sanctioned, and 25% positioned. Less than a third
of the required number of staff nurses has been positioned. This problem
persists despite Centre Government installment grants of Rs. 20 lakh provided
to all district hospitals of the country to improve their basic services, which
includes adequate staffing. In government facilities there is a shortage of
doctors, which according to hospital staff is due to a underestimation of needs
or delay in installing posts. Doctors told the fact-finding team that low pay in
the government sector and inadequate infrastructure in rural areas deters many
doctors from taking hardship posts. The quality of the health workforce is
crucial in delivering good health outcomes. A shortage of doctors at every
level contributes to preventable maternal mortality by creating a delay in
receiving adequate treatment upon reaching a medical facility.
Under JSY scheme, each state will “establish a grievance redressal cell in each
district, under the District Project Management Unit, mainly to facilitate people’s
25genuine grievances on- eligibility for the scheme, quantum of cash assistance, and
delays in disbursement of cash assistance.” The officer’s name, postal address and
his telephone number should be displayed prominently at all health centers and
institutions. Women can submit their grievances regarding eligibility for the
scheme, amount of cash assistance, and delays in disbursement of cash assistance
(payments should be disbursed no later than 7 days after delivery). However, this
grievance redressal system is not openly present in the institutions visited. Only
one center had a “complaints box” which did not display the required information.
26You can also read