2021 Curriculum for Acute Care Common Stem Training - The ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

2021 Curriculum for Acute Care Common Stem Training 20201001 V1.4.3 Implementation August 2021 College logos

Contents
1. Introduction to the Acute Care Common Stem curriculum .............................................. 4
2. Purpose ..................................................................................................................................... 5
2.1. Purpose statement ................................................................................................................ 5
2.2. Rationale ................................................................................................................................ 8
2.3. High level curriculum outcomes: ACCS Learning Outcomes (ACCS LOs) ..................... 8
2.4. Development ......................................................................................................................... 9
2.5. Training Pathway ................................................................................................................... 9
2.6. Duration of training ............................................................................................................. 11
2.7. Less than Full Time Training ................................................................................................. 11
2.8. Generic Professional Capabilities and Good Medical Practice ................................... 11
3. Content of learning ............................................................................................................... 14
3.1. Clinical ACCS Learning Outcomes ................................................................................... 14
3.2. Generic ACCS Learning Outcomes .................................................................................. 24
3.3. Presentations and conditions............................................................................................. 26
4. Learning and teaching ......................................................................................................... 33
4.1. The training environment .................................................................................................... 33
4.2. Teaching and learning methods ....................................................................................... 34
5. Programme of assessment ................................................................................................... 38
The purpose of the programme of assessment .......................................................................... 38
Assurance ........................................................................................................................................ 38
5.1. Programme design .............................................................................................................. 38
5.2. The ACCS assessment blueprint ........................................................................................ 40
5.3. Entrustment decisions ......................................................................................................... 41
5.4. Assessment of ACCS practical procedures (Clinical ACCS LO 5) ................................ 45
5.5. Assessment methods ........................................................................................................... 48
5.6. Decisions on progress (ARCP) ............................................................................................ 49
5.7. Assessment blueprint ........................................................................................................... 50
6. Supervision and feedback ................................................................................................... 52
6.1. Supervision ............................................................................................................................ 52
6.2. Appraisal .............................................................................................................................. 53
7. Quality management ........................................................................................................... 55
8. Intended use of curriculum by trainers and trainees ........................................................ 56
8.1. Recording progress in the e-Portfolio ................................................................................ 56
9. Equality and diversity............................................................................................................. 57
Annex A – Parent specialty learning outcomes .............................................................................. 58
Anaesthetics ................................................................................................................................... 58
Emergency Medicine .................................................................................................................... 59
Internal Medicine ........................................................................................................................... 60
Page 2 of 60Change log
This document outlines the curriculum to be used by doctors completing Acute Care
Common Stem (ACCS) training in the UK. It is accompanied by the Assessment strategy for
ACCS.
This is Version 1.0. As the document is updated, version numbers will be changed, and
content changes noted in the table below.
Version number Date issued Summary of changes
Page 3 of 601. Introduction to the Acute Care Common Stem curriculum
This document identifies the purpose, content of learning, process of training, and the
programme of assessment for Acute Care Common Stem training.
Page 4 of 602. Purpose
2.1. Purpose statement
This purpose statement addresses the requirements of the GMC Excellence by design:
standards for postgraduate curricula to include a clear statement, addressing patient and
service needs, and the scope of practice and level expected of those completing training.
CS1.1 The curriculum has a stated and clear purpose based on scope of practice, service,
and patient and population needs.
The purpose of the Acute Care Common Stem (ACCS) curriculum is to equip the trainee
doctor with the skills and competences required to recognise and undertake initial
management of the acutely unwell patient. Trainees will be able to define the nature of the
specialist intervention required and will have training in four complementary specialties.
The curriculum provides trainees with the generic professional and specialty specific
capabilities required to manage patients presenting with a wide range of acute medical
symptoms and conditions, so they can:
• deliver appropriate and timely care to all patients who become acutely unwell in all
clinical settings within an acute care facility; and
• work as part of and communicate effectively with the multidisciplinary team
managing these situations.
The ACCS curriculum provides a framework for training in four areas closely involved with
managing the acutely unwell patient: Anaesthesia, Internal Medicine, Intensive Care
Medicine and Emergency Medicine. The knowledge and skills of these specialties are closely
related and interface in the care of every acutely ill patient. By working in these specialties,
the ACCS trainee will become familiar with common acute and life-threatening
presentations, their rapid initial assessment and treatment, how to determine what definitive
care is needed and where it is best provided.
The ACCS curriculum is recognised as an exemplar of broad-based, general training with
many common learning outcomes. The universally accepted service model for provision of
care in Acute NHS Trusts necessitates and promotes the requirement for such a programme
of learning. In addition, recent workforce analysis has identified numerous vacancies in
Internal, Emergency and Intensive Care Medicine and Anaesthesia across the UK: the
expansion of acute services and increasing demands of an ageing population will place
further demands over the coming decade on all ACCS specialties.
It is widely acknowledged that the broader range of competences obtained by trainees
completing the ACCS curriculum enhances patient care, particularly in the provision of
emergency out-of-hours work. In addition, the skills gained through ACCS are transferable to
training in Intensive Care Medicine.
This curriculum provides the first two years of training in Emergency Medicine and delivers an
alternative route into training in Anaesthesia, Intensive Care Medicine and Internal Medicine.
The ACCS curriculum includes mandatory training placements in all of the ACCS ‘partner
specialties’, that is, Anaesthesia, Emergency Medicine Intensive Care Medicine and Internal
Medicine. The ACCS curriculum provides a broad-based, attractive programme for doctors.
The programme will help doctors develop knowledge, skills and attitudes to allow them to:
• assess any acutely ill patient and begin appropriate resuscitation
Page 5 of 60• diagnose the most important underlying problem(s)
• initiate appropriate investigations and start appropriate immediate treatment
• provide safe basic anaesthetic care, including safe procedural sedation
• manage critically unwell patients in conjunction with critical care teams
• identify and liaise with other teams to ensure appropriate definitive care
• understand the importance of patient flow through the acute services and within
the wider health community.
Generic Professional Capabilities, clinical skills and knowledge will be developed and
evidenced through achievement of ‘ACCS Learning Outcomes’ (ACCS LOs) across eleven
domains. The ACCS LOs to be achieved by trainees in each training placement capture the
skills, knowledge and behaviours required to fulfil the General Medical Council’s (GMC)
Generic Professional Capabilities1 for all trainees, and are described at a high level in the
table below:
A trainee completing ACCS will be able to;
ACCS Learning Outcome Title GPCs
Care for physiologically stable adult patients presenting to acute
1 1,2,3,4,5,6,7
care across the full range of complexity
Make safe clinical decisions, appropriate to level of experience,
2 1,2,3,4,6,7
knowing when and how to seek effective support
Identify sick adult patients, be able to resuscitate and stabilise and
3 1,2,3,4,5,6,7,8,9
know when it is appropriate to stop
4 Care for acutely injured patients across the full range of complexity 1,2,3,4,6,7
5 Deliver key ACCS procedural skills 1,2,3,4,5,6,7,8,9
6 Deal with complex and challenging situations in the workplace 1,2,3,4,5,6,7,8
7 Provide safe basic anaesthetic care including sedation 1,2,3,5,6,7
8 Manage patients with organ dysfunction and failure 1,2,3,5,6,7
9 Support, supervise and educate 8
10 Participate in research and manage data appropriately 9
Participate in and promote activity to improve the quality and
11 6
safety of patient care
Training and assessment in the areas outlined in the ACCS LOs will take place throughout the
four specialty training placements. On completion of the two generic years of the ACCS
curriculum, a trainee will be equipped with the competence and confidence to manage
uncertainty, to deal with comorbidities and to recognise when specialty opinion or care is
1GMC GPC Framework, https://www.gmc-uk.org/education/standards-guidance-and-curricula/standards-and-
outcomes/generic-professional-capabilities-framework
Page 6 of 60required. The ACCS curriculum focuses on initial assessment and management of patients in a
variety of acute hospital settings. The content of the curriculum reflects the wide range of
clinical and professional skills required to meet the needs of clinical services.
In order to demonstrate completion of the ACCS training programme in its entirety, trainees
are first required to complete this ACCS curriculum prior to further training in each of the
parent specialties. At this point trainees will continue to train as detailed for the relevant level
of training (ie ‘Stage 1’ or ‘Intermediate’) as defined in the curriculum of the respective Royal
College.
In order to progress into further training at ‘Stage 2’ or ‘Higher’ level in each of the parent
specialties, trainees must demonstrate achievement of all of the learning outcomes as
detailed for the relevant level of training in their respective parent specialty’s curriculum (ie
‘Stage 1’ or ‘Intermediate’).
Therefore, in addition to the ACCS LOs, completion of the ACCS (Anaesthetics) training
programme requires achievement of the learning outcomes for completion of ‘Stage 1’ of
the Anaesthetics curriculum.
In addition to the ACCS LOs, completion of the ACCS (Emergency Medicine) training
programme requires achievement of the learning outcomes for completion of ‘Intermediate’
of the Emergency Medicine curriculum.
In addition to the ACCS LOs, completion of the ACCS (Internal Medicine) training
programme requires achievement of the learning outcomes for completion of ‘Stage 1’ of
the Internal Medicine curriculum. It is not expected that trainees who choose ACCS core
training will apply for non-acute (group 2) physician specialties. However, if they wish to, they
will be eligible to apply for a group 2 specialty if they complete three years of the ACCS-IM
programme (equivalent to IM year 1 and IMY year 2).
Trainees who choose ACCS core training will be eligible to apply for ICM recruitment after
three years of the ACCS programme, as long as they have the respective route’s exam by the
time of appointment.
CS1.2 The curriculum considers interdependencies across related specialties and disciplines.
It demonstrates that it has addressed the expectations of the service and healthcare system.
The ACCS curriculum will produce a trainee workforce that reflects current trends of
increasing patient attendances to both primary care and emergency departments. This
workforce will have the skills to begin to manage complex multimorbidity in an ageing
population, and to liaise with all acute hospital specialties.
During its development, the ACCS curriculum has been presented to and discussed with
stakeholders including colleges and faculties, trainees, trainers, heads of schools,
educational and employer organisations in each of the four nations, COPMeD, patients and
protected characteristics groups. Each College/Faculty has consulted on the ACCS
curriculum as part of its engagement strategy for the respective parent specialty.
CS1.3 The curriculum supports the flexibility and transferability of learning.
The ACCS curriculum provides trainees with competences that are designed to be
appropriate and transferable to all acute care training programmes. A mapping exercise has
been conducted across the ACCS two-year curriculum and the curricula of all four parent
specialties to ensure that this can be easily facilitated.
Page 7 of 60By making the Generic Professional Capabilities explicit within the curriculum design, this eases
transfer of capabilities between specialties. ACCS LOs can be evidenced by experiences in a
wide range of posts and environments, allowing flexibility to meet the needs of both the service
and individual trainees.
This purpose statement has been endorsed by the GMC’s Curriculum Oversight Group and
confirmed as meeting the needs of the health services of the countries of the UK.
2.2. Rationale
The Shape of Training Review2 and the GMC’s Excellence by design: standards for
postgraduate curricula3 provide an opportunity to reform postgraduate training to produce
a workforce fit for the needs of patients, producing a doctor who is more patient focused,
more general and has more flexibility in career structure. The GMCs introduction of updated
standards for curricula and assessment processes laid out in Excellence by design, requires all
medical curricula to be based on high-level outcomes and to incorporate the GPCs
framework4. The curriculum is constituted of eleven learning outcomes, eight clinical and
three generic to be achieved by all ACCS trainees as they progress before appointment to
and commencement of Higher Training in their core speciality.
The curriculum for ACCS incorporates and emphasises the importance of the GPCs, which
provide the educational articulation of Good Medical Practice5. Such common capabilities
will promote flexibility in postgraduate training in line with the recommendations set out in the
GMC’s report to the four UK governments6, ensuring a sustainable model for training in each
of the parent specialties agile enough to respond to evolving patient need and service
opportunities, as well as resulting in a more flexible, adaptable workforce.
The curriculum provides further detail and guidance as to how the ACCS learning outcomes
can be achieved and demonstrated in section 5.
2.3. High level curriculum outcomes: ACCS Learning Outcomes (ACCS
LOs)
The 11 ACCS Learning Outcomes describe the professional tasks or work within the scope of
the ACCS specialities. Each ACCS LO has a set of key capabilities associated with that
activity or task. Key capabilities are intended to help trainees and trainers recognise the
minimum level of knowledge, skills and attitudes which should be demonstrated for an
entrustment decision to be made.
2
https://www.shapeoftraining.co.uk/static/documents/content/Shape_of_training_FINAL_Report.pdf_53977887.pdf
3
https://www.gmc-uk.org/education/standards-guidance-and-curricula/standards-and-outcomes/excellence-by-
design
4
https://www.gmc-uk.org/education/standards-guidance-and-curricula/standards-and-outcomes/generic-
professional-capabilities-framework
5
https://www.gmc-uk.org/ethical-guidance/ethical-guidance-for-doctors/good-medical-practice
6
https://www.gmc-uk.org/-/media/documents/adapting-for-the-future-a-plan-to-improve-postgrad-med-training-
flexibility_pdf-69842348.pdf
Page 8 of 60The eight clinical ACCS LOs describe the clinical tasks or activities which are essential to the
care of acutely ill and injured adults presenting to acute care. The clinical ACCS LOs have
also been mapped to the GPC domains and subsections to reflect the professional generic
capabilities required to undertake the clinical tasks. Satisfactory sign off requires
demonstration that, for each of the clinical ACCS LOs, the trainee’s performance meets or
exceeds the minimum expected level of performance expected for completion of this stage
of training, as defined in the curriculum (see section 5.3 ACCS Entrustment Requirements
which outlines the levels expected for each clinical ACCS LO in both years of ACCS training).
The three generic ACCS LOs cover universal requirements of all specialties, as described in
GPC framework. Assessment of the generic ACCS LOs will be underpinned by the relevant
GPC descriptors. Satisfactory sign off will indicate that the ACCS trainee has achieved these
LOs before they can progress.
2.4. Development
Responsibility for the ACCS curriculum rests with the Intercollegiate Committee for ACCS
Training (ICACCST), which has representation from all four parent specialities. The ICACCST
established the ACCS Curriculum Review Group (ACCSCRG) with delegated responsibility for
setting the direction of the curriculum revisions and overseeing and approving the review
work. The group’s membership represents a wide range of stakeholders including the four
parent specialty representation, the Lead Dean for ACCS, trainees and lay/patient groups.
The curriculum for ACCS has been developed with the support and input of trainees,
consultants actively involved in delivering teaching and training across the UK, service
representatives and lay persons. This has been through the work of the ACCSCRG and its
subgroups and at regular stakeholder engagement events.
2.4.1.Ongoing curriculum review
The curriculum will be reviewed regularly with an implementation date for any changes
being not less than six months after their publication date. All changes to the curriculum are
prospectively approved by the GMC before publication. When published, the curriculum
document will be annotated with the same version number and will be available on the
ACCS website, with a summary of changes also published.
Occasionally the ICACCST may have to take decisions that may affect the immediate
interpretation or application of specific items in this curriculum document or supporting
guidance manuals. These will be published as an update circular to all ACCS programme
directors and Heads of Schools [or Deanery equivalent], as well as being cascaded to
trainee groups and published on the ACCS website.
2.5. Training Pathway
The ACCS training pathway is entered following completion of the foundation programme
and its purpose is to ensure doctors demonstrate the ability to learn in the workplace and
develop their clinical and professional skills in readiness for higher specialty training.
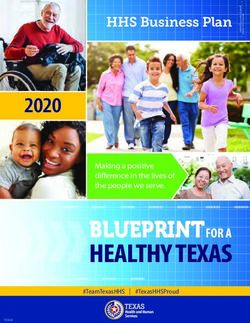
On successfully completing the ACCS generic two-year curriculum, ACCS trainees continue
to train in their chosen specialty (Anaesthetics, Emergency Medicine [EM], or Internal
Medicine [IM]) for a further period (see diagram below); until the completion of Stage 1
training in Anaesthetics, Stage 1 training in IM or Intermediate training in EM.
ACCS has a common aim, but each specialty has specific objectives for ACCS training:
Page 9 of 60Emergency Medicine
The first two years of ACCS training (EM, IM, Anaesthetics and ICM) are followed by a further
year gaining additional competences in adult EM (including musculoskeletal emergencies)
and Paediatric Emergency Medicine; thus fulfilling the requirements to progress to higher
training in EM.
Internal Medicine
ACCS is one of the training options available for delivering the core competences required for
a CCT in one of the acute medical specialties (group 1) managed by the Joint Royal Colleges
of Physicians Training Board (JRCPTB). The first two years of ACCS training (IM, EM, Anaesthetics
and ICM) are followed by a further two years in IM training. The trainee should take part in shifts
of acute medical take monthly to acquire evidence equivalent of 100 patients seen with
acute medicine problems by the end of ACCS. It is anticipated that this will be at least 4 shifts
of acute medical take per month during the six month period of training in medicine. The
trainee should also gain experience in managing patients with ambulatory medical conditions
in an area such as a Same Day Emergency Care (SDEC) unit. This four-year training programme
fulfils the requirements for progression to higher training in a group 1 specialty.
Anaesthetics
The training programme leading to a CCT in Anaesthesia can be entered directly via the Core
Anaesthetic Training (CAT) programme. However, those Anaesthetic trainees with an interest
in the ‘acute’ end of the Anaesthetic spectrum will find ACCS an ideal career starting point. It
provides trainees with more widely based experience than is available solely within the CAT
programme. The first two years of ACCS training (IM, EM, Anaesthetics and ICM) are followed
by a further two years spent gaining additional capabilities in Anaesthetics to complete Stage
1 of the Anaesthesia Training Programme and allow competitive entry into Stage 2.
It is widely acknowledged that the broader range of competences achieved by those on an
ACCS programme, compared to those pursuing CAT, enhances patient care particularly in
the provision of emergency out-of-hours work. This enables supervisors more discretion in the
deployment of trainees with wider-ranging skillsets. For example, the additional knowledge
and skills gained within the ACCS programme may enable trainees to work with lower
supervision levels where appropriate, in areas such as perioperative medicine, trauma
management and critical care. In addition, the skills gained as part of this four-year training
programme are transferable to training in ICM.
Page 10 of 602.6. Duration of training
The ACCS training programme covered by this curriculum will usually be completed in two
years of full time training. Duration of specialty training to CCT will vary by specialty. It may be
possible for those trainees who demonstrate exceptionally rapid development and
acquisition of capabilities, to complete training more rapidly than the current indicative time
of two years. However, it is recognised that clinical experience is a fundamental aspect of
development as a good clinician. There may be a small number of trainees who develop
more slowly and will require an extension of training in line the Reference Guide for
Postgraduate Specialty Training in the UK (The Gold Guide) 7.
2.7. Less than Full Time Training
Trainees are entitled to request less than full time training programmes. Less than full time
trainees should undertake a pro rata share of the out-of-hours duties (including on-call and
other out-of-hours commitments) required of their full-time colleagues in the same
programme and at the equivalent stage.
Less than full time trainees should assume that their clinical training will be of a duration pro-
rata with the time indicated/recommended, but this should be reviewed in accordance with
the Gold Guide.
2.8. Generic Professional Capabilities and Good Medical Practice
The GMC has developed the Generic Professional Capabilities (GPC) framework8 with the
Academy of Medical Royal Colleges (AoMRC) to describe the fundamental, career-long,
generic capabilities required of every doctor. The framework describes the requirement to
develop and maintain key professional values and behaviours, knowledge, and skills, using a
common language. GPCs also represent a system-wide, regulatory response to the most
7 A Reference Guide for Postgraduate Specialty Training in the UK
8 Generic professional capabilities framework
Page 11 of 60common contemporary concerns about patient safety and fitness to practise within the
medical profession. The framework will be relevant at all stages of medical education,
training and practice.
Good medical practice (GMP)9 is embedded at the heart of the GPC framework. In
describing the principles, duties and responsibilities of doctors the GPC framework articulates
GMP as a series of achievable educational outcomes to enable curriculum design and
assessment.
The GPC framework describes nine domains with associated descriptor outlining the
‘minimum common regulatory requirement’ of performance and professional behaviour for
those completing a CCT or its equivalent. These attributes are common, minimum and
generic standards expected of all medical practitioners achieving a CCT or its equivalent.
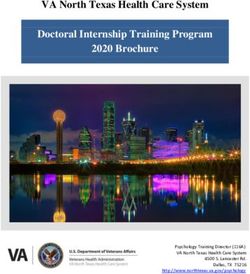
The 20 domains and subsections of the GPC framework are directly identifiable in the ACCS
curriculum. They are mapped to each of the clinical and generic ACCS LOs, which are, in
9 Good Medical Practice
Page 12 of 60turn, mapped to the assessment blueprints. This is to emphasise those core professional
capabilities that are essential to safe clinical practice and that they must be demonstrated
at every stage of training as part of the holistic development of responsible professionals.
This approach will allow early detection of issues most likely to be associated with fitness to
practise and to minimise the possibility that any deficit is identified during the final phases of
training.
Page 13 of 603. Content of learning
The practice of medicine in ACCS requires the generic and specialty specific knowledge,
skills, and attitudes to manage adult patients presenting acutely with a wide range of
presentations or conditions. It involves particular emphasis on diagnostic reasoning,
managing uncertainty, dealing with comorbidities, managing emergencies and recognising
when specialty opinion or care is required.
3.1. Clinical ACCS Learning Outcomes
The ACCS Learning Outcomes describe the professional tasks or work within the scope of
ACCS. The clinical ACCS Learning Outcomes are based on the concept of Entrustable
Professional Activities10 which are a method of using the professional judgement of
appropriately trained, expert assessors as a key aspect of the validity of assessment and a
defensible way of forming global judgements of professional performance.
Each clinical ACCS LO has Key Capabilities described. These are statements that are used to
frame entrustment decisions about the particular learning outcome. They are prefixed by ‘at
the end of ACCS’ to give clear guidance to trainees and faculty what is expected. Trainees
will have collated evidence against each of these, and the training faculty will make a
recommendation based on their answer to the question about whether these have been
met.
A set of descriptors are also associated with that activity or task. Descriptors are intended to
help trainees and trainers recognise the minimum level of knowledge, skills and attitudes
which should be demonstrated by ACCS trainees. They will provide evidence of how their
performance meets or exceeds the minimum expected level of performance for their year of
training. The knowledge skills and behaviour are listed for each, but these are not a
comprehensive list and there are many more examples that would provide equally valid
evidence of performance.
Many of the clinical ACCS LO descriptors refer to patient centred care and shared decision
making. This is to emphasise the importance of patients being at the centre of decisions
about their own treatment and care, by exploring care or treatment options and their risks
and benefits and discussing choices available.
Additionally, the clinical ACCS LOs repeatedly refer to the need to demonstrate professional
behaviour with regard to patients, carers, colleagues and others. Good doctors work in
partnership with patients and respect their rights to privacy and dignity. They treat each
patient as an individual. They do their best to make sure all patients receive good care and
treatment that will support them to live as well as possible, whatever their illness or disability.
Appropriate professional behaviour should reflect the principles of GMP and GPC (see
section 2.6).
By the end of training and in order to be recommended to the GMC for the award of CCT
and entry to the specialist register, the doctor must demonstrate that they are capable of
unsupervised practice in all generic and clinical Learning Outcomes. The ACCS training
programme, as the first stage of training for the constituent specialties, gives a sound
10 Nuts and bolts of entrustable professional activities
Page 14 of 60foundation for trainees to achieve this with expected performance levels for the clinical LOs
commensurate with this stage of training.
This section of the curriculum details the 11 generic and clinical ACCS LO with expected
levels of performance, mapping to relevant GPCs and the evidence that may be used to
make an entrustment decision.
Clinical ACCS LOs
1. Care for physiologically stable adult patients presenting to acute care across the
full range of complexity
Key ACCS At completion of ACCS a trainee:
Capabilities
• will be able to gather appropriate information, perform a relevant
clinical examination and be able to formulate and communicate a
management plan that prioritises patient’s choices and is in their best
interests, knowing when to seek help
• will be able to assess and formulate a management plan for patients
who present with complex medical and social needs
These capabilities will apply to patients attending with physical and
psychological ill health
Descriptors • Demonstrate professional behaviour with regard to patients, carers,
colleagues and others
• Deliver patient centred care including shared decision making
• Take a relevant patient history including patient symptoms, concerns,
priorities and preferences
• Perform accurate clinical examinations
• Show appropriate clinical reasoning by analysing physical and
psychological findings
• Formulate an appropriate differential diagnosis
• Formulate an appropriate diagnostic test and management plan,
taking into account patient preferences, and the urgency required
• Explain clinical reasoning behind diagnostic and clinical
management decisions to patients/carers/guardians and other
colleagues
• Appropriately select, manage and interpret investigations
• Recognise need to liaise with specialty services and refers where
appropriate
• Demonstrate awareness of the needs of vulnerable adults attending
the acute care sector
• Demonstrate professional behaviour with regard to patients, carers,
colleagues and others
GPCs Domain 1: Professional values and behaviours
Domain 2: Professional skills
• practical skills
• communication and interpersonal skills
• dealing with complexity and uncertainty
• clinical skills (history taking, diagnosis and medical management;
consent; humane interventions; prescribing medicines safely; using
medical devices safely; infection control and communicable disease)
Page 15 of 60Domain 3: Professional knowledge
• professional requirements
• national legislation
• the health service and healthcare systems in the four countries
Domain 4: Capabilities in health promotion and illness prevention
Domain 5: Capabilities in leadership and team-working
Domain 6: Capabilities in patient safety and quality improvement
• patient safety
• quality improvement
Mini-CEX
Evidence to
CbD
inform
ACAT
decision
Logbook
includes
E-learning module completion/self-directed learning
Entrustment decision
MSF
2. Make safe clinical decisions, appropriate to level of experience, knowing when
and how to seek effective support
Key ACCS At completion of ACCS a trainee:
capabilities
• will understand how to apply clinical guidelines
• will understand how to use diagnostic tests in ruling out key pathology,
and be able to describe a safe management plan, including
discharge where appropriate, knowing when help is required
• will be aware of the human factors at play in clinical decision making
and their impact on patient safety
Descriptors • Proficient in ECG and plain film interpretation, as relevant to acute
care
• Aware of the cognitive psychology of decision making
• Understand basic diagnostic test methodology
• Understand the fundamentals of decision rule design
• Aware of the strengths and limitations of using guidelines eg NICE
• Demonstrate capabilities in dealing with complexity and uncertainty
• Share decision making by informing patients, prioritising patient’s
wishes, and respecting their beliefs, concerns and expectations
GPCs Domain 1: Professional values and behaviours
Domain 2: Professional skills:
• communication and interpersonal skills
• dealing with complexity and uncertainty
• clinical skills (history taking, diagnosis and medical management;
consent; humane interventions; prescribing medicines safely; using
medical devices safely; infection control and communicable disease)
Domain 3: Professional knowledge
• professional requirements
Page 16 of 60• national legislation
• the health service and healthcare systems in the four countries
Domain 4: Capabilities in health promotion and illness prevention
Domain 5: Capabilities in leadership and teamworking
Domain 6: Capabilities in patient safety and quality improvement
• patient safety
Mini-CEX
Evidence to
CbD
inform
ACAT
decision
Logbook
includes
Entrustment decision
MSF
Feedback from patients
3. Identify sick adult patients, be able to resuscitate and stabilise and know when it is
appropriate to stop
Key ACCS At completion of ACCS a trainee:
capabilities
• will recognise and manage the initial phases of any acute life
threatening presentation including cardiac arrest and peri-arrest
situations
• will be able to provide definitive airway, respiratory and circulatory
support to critically ill patients
• will be able to establish the most appropriate level of care for critically
unwell patients - including end-of life decisions - and support their
needs as well as those of their loved ones
Descriptors • Identify an acutely ill patient by taking account of their medical
history, clinical examination, vital signs and available investigations
• Integrate clinical findings with timely and appropriate investigations to
form a differential diagnosis and an initial treatment plan
• Institute definitive airway management and initiate and maintain
advanced respiratory support
• Utilise intravenous fluids and inotropic drugs as clinically indicated,
using central venous access where required and monitored by
invasive monitoring techniques
• Manage life-threatening cardiac and respiratory conditions including
peri-arrest and arrest situations
• Formulate and initiate ongoing treatment plan for a critically ill acute
surgical or acute medical patient post resuscitation, including those
with sepsis and institute timely antimicrobial therapy with an aim for
ongoing stabilisation
• Communicate effectively and in a timely manner with fellow
members of the multidisciplinary team including those from other
specialties and completing accurate legible and contemporaneous
entries in the medical record
• Arrange escalation of care when required and provide a succinct
structured handover of the relevant patient details including
treatment to that point
Page 17 of 60• Recognise a patient who is in danger of deterioration or who requires
further treatment and provide explicit instructions regarding an
ongoing treatment plan and contact details should a further review
be required
• Decide when it is appropriate to end resuscitation, and be cogniscent
of the specific care needs of patients and their loved ones when this
decision has been made
• Respect patient autonomy and understand when and how they
should use advance directives and living wills
• Recognise the potential for organ donation in certain end of life
situations and be aware of associated best practice guidelines and
legislation
• Demonstrate effective consultation skills in challenging circumstances
• Demonstrate compassionate professional behaviour and clinical
judgement
GPCs Domain 1: Professional values and behaviours
Domain 2: Professional skills
• practical skills
• communication and interpersonal skills
• dealing with complexity and uncertainty
• clinical skills (history taking, diagnosis and medical management;
consent; humane interventions; prescribing medicines safely; using
medical devices safely; infection control and communicable disease)
Domain 3: Professional knowledge
• professional requirements
• national legislation
• the health service and healthcare systems in the four countries
Domain 4: Capabilities in health promotion and illness prevention
Domain 5: Capabilities in leadership and teamworking
Domain 6: Capabilities in patient safety and quality improvement
• patient safety
• quality improvement
Domain 7: Capabilities in safeguarding vulnerable groups
Mini-CEX
Evidence to
CbD
inform
ACAT
decision
DOPS
includes
Logbook
Entrustment decision
MSF
Feedback from patients
4. Care for acutely injured patients across the full range of complexity
Key ACCS At completion of ACCS, a trainee:
capabilities
• Will be an effective member of the multidisciplinary trauma team
Page 18 of 60• Will be able to assess, investigate and manage low energy injuries in
stable patients
Descriptors • Able to perform primary/secondary trauma survey
• Have examination skills required to identify/diagnose injury including
vascular and neurological consequences
• Appropriately use investigations including XR/CT/US/MRI to confirm
presence/consequences of injury
• Provide basic management of wounds, soft tissue injuries, fractures
and dislocations including local anaesthetic techniques
• Provide safe use of basic local anaesthetic techniques eg ring block,
fascia iliaca block
• Use a range of techniques for wound closure (simple dressing,
suturing, skin adhesive, steri-strips).
• Know the fundamentals of management of fractures and dislocations
(slings, splints, basic plastering, manipulation as appropriate)
• Able to remove foreign bodies from the eye and ear
• Provide opportunistic advice on accident prevention
• Understand the pathophysiology and management of injury
(including specific populations eg elderly, paediatric and pregnancy)
• Understand the social/economic consequences of injury upon
individuals
• Estimate a timeline of healing and give general and specific safety
net advice on concerning features of potential complications
• Understand the importance of considering safeguarding of vulnerable
patients
• Apply CT guidelines for suspected head and cervical spine injuries
• Provide initial care for patients with fractured neck of femur
• Understand the impact of injury on patients with markers of frailty
GPCs Domain 1: Professional values and behaviours
Domain 2: Professional skills
• practical skills
• communication and interpersonal skills
• dealing with complexity and uncertainty
• clinical skills (history taking, diagnosis and medical management;
consent; humane interventions; prescribing medicines safely; using
medical devices safely; infection control and communicable disease)
Domain 3: Professional knowledge
• professional requirements
• national legislation
• the health service and healthcare systems in the four countries
Domain 5: Capabilities in leadership and teamworking
Domain 6: Capabilities in patient safety and quality improvement
• Safety
Domain 7: Capabilities in safeguarding vulnerable groups
Mini-CEX
Evidence to
CbD
inform
ACAT
decision
DOPS
includes
Logbook
Entrustment decision
Page 19 of 60MSF
Feedback from patients
5. Deliver key ACCS procedural skills
Key ACCS At completion of ACCS a trainee:
capabilities
• Will have the clinical knowledge to identify when key practical
emergency skills are indicated
• Will have the knowledge and psychomotor skills to perform the skill
safely and in a timely fashion
Descriptors • Pleural aspiration of air
• Chest drain: Seldinger and open technique
• Establish invasive monitoring (CVP and Art line)
• Vascular access in emergency- IO, femoral vein
• Lumbar puncture
• Fracture/dislocation manipulation
• External pacing
• Point of care ultrasound- Vascular access and Fascia iliaca block
GPCs Domain 1: Professional values and behaviours
Domain 2: Professional skills
• practical skills
• communication and interpersonal skills
• dealing with complexity and uncertainty
DOPs
Evidence to
Logbook
inform
Entrustment decision
decision
MSF
includes
6. Deal with complex and challenging situations in the workplace
Key ACCS At completion of ACCS a trainee:
capabilities
• Will know how to reduce the risk of harm to themselves whilst working
in acute care
• Will understand the personal and professional attributes of an
effective acute care clinician
• Will be able to effectively manage their own clinical work load
• Will be able to deal with common challenging interactions in the
workplace
Descriptors • Know how to safely deal with violent or threatening situations
• Able to handle common but challenging situations:
o self-discharge against advice
Page 20 of 60o capacity assessment
o adult safeguarding issue
o Police/FME enquiries
• Aware of national legislation and legal responsibilities, including
safeguarding vulnerable groups
• Behave in accordance with ethical and legal requirements
• Demonstrate ability to offer an apology or explanation when
appropriate
• Demonstrate ability to lead the clinical team in ensuring that medical
legal factors are considered openly and consistently
• Interact effectively with hospital colleagues when handing over the
care of patients including in complex situations.
• Liaise effectively with healthcare professionals outside the hospital
about patient care.
GPCs Domain 1: Professional values and behaviours
Domain 2: Professional skills
• practical skills
• communication and interpersonal skills
• dealing with complexity and uncertainty
• clinical skills (history taking, diagnosis and medical management;
consent; humane interventions; prescribing medicines safely; using
medical devices safely; infection control and communicable disease)
Domain 5: Capabilities in leadership and team-working
Domain 6: Capabilities in patient safety and quality improvement
• patient safety
Domain 7: capabilities in safeguarding vulnerable groups
Mini-CEX
Evidence to
Logbook
inform
Entrustment decision
decision
MSF
includes
Feedback from patients
7. Provide safe basic anaesthetic care including sedation
Key ACCS At completion of ACCS a trainee will be able to:
capabilities
• Pre-operatively assess, optimise and prepare patients for anaesthesia
• Safely induce, maintain and support recovery from anaesthesia
including recognition and management of complications
• Provide urgent or emergency anaesthesia to ASA 1E and 2E patients
requiring uncomplicated surgery including stabilisation and transfer
• Provide safe procedural sedation for ASA 1E and 2E patients
Descriptors • Understand the risks, aetiology, treatment and control processes of
infection including the need for and ability to perform an aseptic
non-touch technique
Page 21 of 60• Pre-operatively assess patients’ suitability for anaesthesia, prescribe
suitable pre-medication, recognise when further investigation or
optimisation is required prior to commencing surgery and adequately
communicate this to the patient or their family
• Safely induce anaesthesia in ASA 1 and 2 patients, recognise and
deal with common and important complications associated with
induction
• Maintain anaesthesia for the relevant procedure, utilise appropriate
monitoring and effectively interpret the information it provides to
ensure the safety of the anaesthetised patient, as a member of the
multidisciplinary theatre team
• Safely care for a patient recovering from anaesthesia, recognise and
treat the common associated complications and manage
appropriate post-operative analgesia, anti-emesis and fluid therapies
• Provide urgent or emergency anaesthesia to ASA 1E and 2E patients
requiring uncomplicated surgery
• Plan and deliver safe sedation using appropriate agents for ASA 1/1E
and 2/2E patients requiring procedures
GPCs Domain 1: Professional values and behaviours
Domain 2: Professional skills
• practical skills
• communication and interpersonal skills
• dealing with complexity and uncertainty
• clinical skills (history taking, diagnosis and medical management;
consent; humane interventions; prescribing medicines safely; using
medical devices safely; infection control and communicable disease)
Domain 3: Professional knowledge
• professional requirements
• national legislation
• the health service and healthcare systems in the four countries
Domain 5: Capabilities in leadership and teamworking
Domain 6: Capabilities in patient safety and quality improvement
• patient safety
Domain 7: Capabilities in safeguarding vulnerable groups
Mini-CEX
Evidence to
CbD
inform
DOPS
decision
Logbook
includes
Entrustment decision
MSF
HALO in Sedation
IAC
8. Manage patients with organ dysfunction and failure
Key ACCS At completion of ACCS a trainee:
capabilities
Page 22 of 60• Will be able to provide safe and effective care for critically ill patients
across the spectrum of single or multiple organ failure
• Will be able to plan and communicate effectively with patients,
relatives and the wider multi-professional team when attending to the
clinical and holistic needs of patients
Descriptors • Recognise the limitations of intensive care and employ appropriate
admission criteria
• Recognise, assesses and initiate management for acutely ill adults
across the spectrum of single or multiple organ failure
• Recognise and manage the patient with sepsis and employ local
infection control policies
• Perform safely and effectively the clinical invasive procedures to
maintain cardiovascular, renal, and respiratory support.
• Undertake and evaluate laboratory and clinical imaging
investigations to manage patients during their intensive care stay
• Manage the ongoing medical/surgical needs and organ support of
patients during a critical illness, including the holistic care of patients
and relatives
• Plan and communicate the appropriate discharge of patients from
intensive care to health care professionals, patients and relatives
• Support the management of end of life care within the intensive care
environment with patients, relatives and the multi-professional team
• Understand the role of transplant services when appropriate and the
principles of brain-stem death testing
• Support clinical staff outside the ICU to enable the early detection of
the deteriorating patient
GPCs Domain 1: Professional values and behaviours
Domain 2: Professional skills:
• practical skills
• communication and interpersonal skills
• dealing with complexity and uncertainty
• clinical skills (history taking, diagnosis and medical management;
consent; humane interventions; prescribing medicines safely; using
medical devices safely; infection control and communicable disease)
Domain 3: Professional knowledge
• professional requirements
• national legislation
• the health service and healthcare systems in the four countries
• Capabilities in health promotion and illness prevention
• Capabilities in leadership and team-working
• Capabilities in patient safety and quality improvement
Domain 7: Capabilities in safeguarding vulnerable groups
Mini-CEX
Evidence to
CbD
inform
DOPS
decision
Logbook
includes
Entrustment decision
MSF
Page 23 of 603.2. Generic ACCS Learning Outcomes
The three generic ACCS LOs cover universal requirements of all specialties as described in
the GPC framework that are not exemplified by day to day activity in the workplace.
Assessment of the generic LOs will be underpinned by the descriptors from the relevant GPC
domains and evidenced against the performance and behaviour expected at that stage of
training. Satisfactory sign off will indicate that there are no concerns before the trainee can
progress to the next part of the assessment of clinical capabilities.
In order to ensure consistency and transferability, the generic ACCS LOs have been grouped
under GPC-aligned categories.
For each generic ACCS LOs is a set of descriptors of the observable skills and behaviours
which would demonstrate that a trainee has met the minimum level expected. The
descriptors are not a comprehensive list and there may be more examples that would
provide equally valid evidence of performance.
Generic ACCS LOs
9. Support, supervise and educate
Key ACCS At completion of ACCS a trainee:
capabilities
• Will be able to set learning objectives for and deliver a teaching
session
• Will be able to deliver effective feedback to a junior colleague or
allied health professional with an action plan
Descriptors • Delivers effective teaching and training to medical students, junior
doctors and other health care professionals
• Delivers effective feedback with action plan
• Able to supervise less experienced trainees in their clinical assessment
and management of patients
• Able to supervise less experienced trainees in carrying out appropriate
practical procedures
• Able to act as a clinical supervisor to doctors in earlier stages of
training
GPCs Domain 8: Capabilities in education and training
TO
Evidence to
Entrustment decision
inform
MSF
decision
ES report
includes
Relevant training course
End of placement reports
Page 24 of 6010. Participate in research and managing data appropriately
Key ACCS At completion of ACCS a trainee:
capabilities
• Will be able to search the medical literature effectively and know how
to critically appraise studies
Descriptors • Manages clinical information/data appropriately
• Understands principles of research and academic writing
• Demonstrates ability to carry out critical appraisal of the literature
• Understands the role of evidence in clinical practice and
demonstrates shared decision making with patients
• Demonstrates appropriate knowledge of research methods, including
qualitative and quantitative approaches in scientific enquiry
• Demonstrates appropriate knowledge of research principles and
concepts and the translation of research into practice
• Follows guidelines on ethical conduct in research and consent for
research
• Understands public health epidemiology and global health patterns
• Recognises potential of applied informatics, genomics, stratified risk
and personalised medicine and seeks advice for patient benefit when
appropriate
GPCs Domain 9: Capabilities in research and scholarship
e-Learning module completion/self-directed learning
Evidence to
Entrustment decision
inform
MSF
decision
MRCP(UK)
includes
ES annual report
GCP certificate (if involved in clinical research) or equivalent
Evidence of literature search and critical appraisal of research
Use of clinical guidelines
Quality improvement and audit
Evidence of research activity
End of placement reports
11. Participate in and promote activity to improve the quality and safety of patient
care
Key ACCS At completion of ACCS a trainee:
capabilities
• will be able to contribute effectively to a departmental quality
improvement project
Descriptors • Makes patient safety a priority in clinical practice
• Raises and escalates concerns where there is an issue with patient
safety or quality of care
• Demonstrates commitment to learning from patient safety
investigations and complaints
• Shares good practice appropriately
• Contributes to and delivers quality improvement
Page 25 of 60• Understands basic Human Factors principles and practice at
individual, team, organisational and system levels
• Understands the importance of non-technical skills and crisis resource
management
• Recognises and works within limit of personal competence
• Avoids organising unnecessary investigations or prescribing poorly
evidenced treatments
GPCs Domain 6: Capabilities in patient safety and quality improvement
• patient safety
• quality improvement
QIPAT
Evidence to
e-Learning module completion/self-directed learning
inform
MSF
decision
Entrustment decision
includes
ES annual report
End of placement reports
KEY
ACAT Acute Care Assessment Tool ALS Advanced Life Support
Direct Observation of Procedural
CbD Case-based Discussion DOPS
Skills
GCP Good Clinical Practice GPC General Professional Capabilities
Holistic Assessment of Learning
HALO IAC Initial Assessment of Competence
Outcome
Mini-
Mini-Clinical Evaluation Exercise MCR Multiple Consultant Report
CEX
Quality Improvement Project
MSF Multi-Source Feedback QIPAT
Assessment Tool
TO Teaching Observation
3.3. Presentations and conditions
The scope of ACCS is broad and cannot be encapsulated by a finite list of presentations and
conditions. Any attempt to list all relevant presentations, conditions and issues would be
extensive but inevitably incomplete.
The table below details key presentations and conditions in ACCS. Each of these should be
regarded as a clinical context in which trainees should be able to demonstrate the clinical
ACCS LOs and GPCs. Trainees will need to become familiar with the knowledge, skills and
attitudes around managing patients with these conditions and presentations. The patient
should always be at the centre of knowledge, learning and care.
Page 26 of 60You can also read