Watson Health 100 Top Hospitals Study 2019 - 26th edition | March 4, 2019 - IBM
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Watson Health 100 Top Hospitals Study 2019 26th edition | March 4, 2019
IBM Watson Health™ 75 Binney Street Cambridge, MA 02142 800-525-9083 ibm.com/watsonhealth Watson Health 100 Top Hospitals Study, 2019; 26th edition © 2019 IBM Watson Health. All rights reserved. IBM, the IBM logo, ibm.com, Watson Health, and 100 Top Hospitals are trademarks of International Business Machines Corp., registered in many jurisdictions worldwide. Other product and service names might be trademarks of IBM or other companies. Printed and bound in the United States of America. The information contained in this publication is intended to serve as a guide for general comparisons and evaluations, but not as the sole basis upon which any specific conduct is to be recommended or undertaken. The reader bears sole risk and responsibility for any analysis, interpretation, or conclusion based on the information contained in this publication, and IBM shall not be responsible for any errors, misstatements, inaccuracies, or omissions contained herein. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from IBM Watson Health. ISBN: 978-1-57372-474-6
Introduction
Contents
Welcome to the 26th edition of the
03 Introduction Watson Health 100 Top Hospitals® study
07 2018 100 Top Hospitals from IBM Watson Health™.
award winners
13 2018 Everest Award winners For over 25 years, the 100 Top Hospitals program
19 Findings has been producing annual, quantitative studies
35 Methodology designed to shine a light on the nation’s highest
51 Appendix A performing hospitals and health systems.
53 Appendix B
55 Appendix C: The 2019 study of US hospitals began with the
Methodology details same goal that has driven each study since the
beginning of the 100 Top Hospitals program:
To identify top performers and deliver insights
that may help all healthcare organizations
better focus their improvement initiatives on
achieving consistent, balanced, and sustainable
high performance.
Illuminating achievement for a
value-based world
Our research is based on clinical, operational, and
patient perception-of-care measures that form
a balanced scorecard. For over 25 years, the
hospitals achieving excellence on our scorecard
inherently set attainable benchmarks for others in
the industry to aspire to over time.
Providing these measures of successful
performance may be especially important today as
the healthcare landscape continues to evolve from
fee-for-service toward value-based care models.
3100 Top Hospitals winners
consistently set industry By finding ways to take balanced performance
benchmarks for measures to the next level, the winners of our 100 Top
like 30-day readmissions, Hospitals award are identifying opportunities to
mortality rates, patient deliver healthcare value to patients, communities,
experience, and profit and payers. The performance levels achieved
margins. by these hospitals may motivate their peers to
use data, analytics, and benchmarks to close
performance gaps.
Hospitals do not apply for our 100 Top Hospitals
selection process, and award winners do not pay
to market their honor.
Delivering a transparent assessment
To maintain the 100 Top Hospitals study’s integrity
and avoid bias, we use public data sources and
explain the methodologies we use to calculate
outcome metrics. This supports inclusion of
hospitals across the country and facilitates
consistency of definitions and data.
Our national balanced scorecard, based on Norton
and Kaplan’s concept1, is the foundation of our
research. It is comprised of key measures of
hospital performance: inpatient and extended care
quality, operational efficiency, financial health, and
customer experience. The composite score derived
from these measures reflects excellence in hospital
care, management, and leadership.
In addition, to support consideration of different
types of hospitals, the 100 Top Hospitals study
categorizes the nation’s hospitals into five groups:
major teaching, teaching, large community,
medium community, and small community
hospitals. This produces benchmarks that are
comparable and action-driving across each
organizational type. This is important because
each kind of hospital has its own set of challenges
and opportunities.
4 IBM Watson HealthYielding a measure of leadership excellence –– Provided faster emergency care
Since 1993, the 100 Top Hospitals program –– Kept expenses low, both in-hospital and
has also sought to shed light on the efficacy through the aftercare process
of innovative leaders. The methodology is
aimed at identifying leaders who can transform –– Scored higher on patient ratings of their overall
an organization by pinpointing improvement hospital experience
opportunities and adjusting goals for key
performance domains. We believe that higher Our study projections also indicate that if the
composite scores on the balanced scorecard benchmarks of performance established by our
typically indicate more effective leadership and a 2019 winners were achieved by all hospitals in the
consistent delivery of value. US, the following would be true:
–– More than 103,000 additional lives could be
The leadership of today’s hospitals, including saved in-hospital
the board, executive team, and medical staff
leadership, is responsible for ensuring all facets of –– Over 38,000 additional patients could be
a hospital are performing at similarly high levels complication-free
in both the short and long term. The 100 Top –– Over $8.2 billion in inpatient costs could
Hospitals study and analytics provide a view of that be saved
enterprise performance alignment.
––The typical patient could be released from
Comparing the performance of our the hospital a half a day sooner and would
2019 winners to nonwinners have 12 percent fewer expenses related to
the complete episode of care than the median
Using the measures presented in our national
patient in the US
balanced scorecard, this year’s 100 Top Hospitals
study revealed significant differences between –– Over 155,000 fewer discharged patients would
award winners and their nonwinning peers. be readmitted within 30 days
–– Patients would spend 17 minutes less in
Our study’s highest-performing hospitals:
hospital emergency rooms per visit
–– Had lower inpatient mortality, considering
patient severity This analysis is based on applying the difference
between study winners and nonwinners to
–– Had fewer patient complications
Medicare patient counts. If the same standards
–– Delivered care that resulted in fewer HAIs were applied to all inpatients, the impact would be
even greater.
–– Had lower 30-day mortality and 30-day
readmission rates
For more details about this study’s findings and the
–– Sent patients home sooner achievements of the 100 Top Hospitals, please see
the Findings section of this document.
5Welcoming your input In addition to the major studies, customized
The 100 Top Hospitals program works to ensure analyses are also available from the 100 Top
that the measures and methodologies used in our Hospitals program, including custom benchmark
studies are fair, consistent, and meaningful. We reports. Our reports are designed to help
continually test the validity of our performance healthcare executives understand how their
measures and data sources. In addition, as part of organizational performance compares to peers
our internal performance improvement process, we within health systems, states, and markets.
welcome comments about our study from health
system, hospital, and physician executives. To 100 Top Hospitals program reports offer a
submit comments, visit 100tophospitals.com. two-dimensional view of both performance
improvement over time, applying the most
current methodologies across all years of data
Showcasing the versatility of the to produce trends, as well as the most current
100 Top Hospitals program year performance.
The 100 Top Hospitals research is one of three
You can read more about these studies, order
major annual studies of the Watson Health
customized reports, and view lists of all winners by
100 Top Hospitals program. To increase
visiting 100tophospitals.com.
understanding of trends in specific areas of the
healthcare industry, the program includes:
–– 100 Top Hospitals and Everest Award studies About IBM Watson Health
Research that annually recognizes the 100 Each day, professionals throughout the health
top-rated hospitals in the nation based on ecosystem make powerful progress toward a
a proprietary, balanced scorecard of overall healthier future. At IBM Watson Health, we help
organizational performance, and identifies them remove obstacles, optimize efforts, and
those hospitals that also excel at long- reveal new insights to support the people they
term rates of improvement in addition to serve. Working across the landscape, from payers
performance and providers to governments and life sciences,
–– 50 Top Cardiovascular Hospitals study we bring together deep health expertise; proven
An annual study introduced in 1999 that innovation; and the power of artificial intelligence
identifies hospitals demonstrating the highest to enable our customers to uncover, connect, and
performance in hospital cardiovascular act as they work to solve health challenges for
services for four important patient groups: people everywhere.
heart attack, heart failure, coronary artery
bypass graft and percutaneous coronary For more information, visit ibm.com/watsonhealth.
intervention
–– 15 Top Health Systems study
An annual study introduced in 2009 that
provides an objective measure of health
system performance overall and offers insight
into the ability of a system’s member hospitals
to deliver consistent top performance across
the communities they serve, all based on our
national health system scorecard
6 IBM Watson HealthNote that the order of hospitals in the following
2019 tables does not reflect performance rating.
Hospitals are ordered alphabetically. For full details
100 Top Hospitals on these peer groups and the process we used to
select the winning benchmark hospitals*, see the
award winners Methodology section of this document.
The Watson Health 100 Top Hospitals® program
is pleased to present the 2019 Watson Health
100 Top Hospitals.
Major teaching hospitals*
Hospitals Location Medicare ID Total year(s) won
Advocate Illinois Masonic Medical Center Chicago, IL 140182 8
Ascension Providence Hospital Southfield, MI 230019 11
Banner - University Medical Center Phoenix Phoenix, AZ 030002 2
Cedars-Sinai Medical Center Los Angeles, CA 050625 3
Garden City Hospital Garden City, MI 230244 2
Mayo Clinic Hospital Jacksonville, FL 100151 2
Mount Sinai Medical Center Miami Beach, FL 100034 2
NorthShore University HealthSystem Evanston, IL 140010 20
Saint Francis Hospital and Medical Center Hartford, CT 070002 8
Spectrum Health Hospitals Grand Rapids, MI 230038 10
St. Joseph Mercy Hospital Ann Arbor, MI 230156 10
St. Luke's University Hospital - Bethlehem Bethlehem, PA 390049 7
The Miriam Hospital Providence, RI 410012 1
UCHealth University of Colorado Hospital Aurora, CO 060024 6
University of Utah Hospital Salt Lake City, UT 460009 2
* Everest Award winners are in bold type.
* To see a full list of our award winners through the years, visit https://www-01.ibm.com/common/ssi/cgi-bin/ssialias?htmlfid=40019540USEN&.
7Teaching hospitals* Hospitals Location Medicare ID Total year(s) won Abbott Northwestern Hospital Minneapolis, MN 240057 3 Aspirus Wausau Hospital Wausau, WI 520030 7 Brandon Regional Hospital Brandon, FL 100243 7 BSA Health System Amarillo, TX 450231 6 CHRISTUS St. Michael Health System Texarkana, TX 450801 3 Good Samaritan Hospital Cincinnati, OH 360134 6 Lakeland Medical Center St. Joseph, MI 230021 2 Mercy Hospital St. Louis St. Louis, MO 260020 7 Monmouth Medical Center Long Branch, NJ 310075 1 Morton Plant Hospital Clearwater, FL 100127 7 Mount Carmel St. Ann's Westerville, OH 360012 2 Park Nicollet Methodist Hospital St. Louis Park, MN 240053 5 Parkview Regional Medical Center Fort Wayne, IN 150021 4 PIH Health Hospital - Whittier Whittier, CA 050169 5 Riverside Medical Center Kankakee, IL 140186 10 Rose Medical Center Denver, CO 060032 12 Sentara Leigh Hospital Norfolk, VA 490046 5 Sky Ridge Medical Center Lone Tree, CO 060112 2 SSM Health St. Mary's Hospital - Madison Madison, WI 520083 6 St. Luke's Hospital Cedar Rapids, IA 160045 8 St. Mark's Hospital Salt Lake City, UT 460047 6 Sycamore Medical Center Miamisburg, OH 360239 10 UCHealth Poudre Valley Hospital Fort Collins, CO 060010 13 Utah Valley Hospital Provo, UT 460001 1 West Penn Hospital Pittsburgh, PA 390090 5 * Everest Award winners are in bold type. 8 IBM Watson Health
Large community hospitals*
Hospitals Location Medicare ID Total year(s) won
Advocate Sherman Hospital Elgin, IL 140030 2
Banner Del E. Webb Medical Center Sun City West, AZ 030093 1
Baylor Scott & White Medical Center - Grapevine Grapevine, TX 450563 1
Hoag Hospital Newport Beach Newport Beach, CA 050224 4
IU Health Bloomington Hospital Bloomington, IN 150051 1
Mease Countryside Hospital Safety Harbor, FL 100265 11
Memorial Hermann Memorial City Medical Center Houston, TX 450610 8
Mercy Health - Anderson Hospital Cincinnati, OH 360001 12
Mercy Health - St. Rita's Medical Center Lima, OH 360066 4
Mercy Hospital Coon Rapids, MN 240115 7
Mercy Hospital Oklahoma City Oklahoma City, OK 370013 4
Northwestern Medicine Central DuPage Hospital Winfield, IL 140242 10
Sarasota Memorial Hospital Sarasota, FL 100087 4
Scripps Memorial Hospital La Jolla La Jolla, CA 050324 4
St. Clair Hospital Pittsburgh, PA 390228 5
St. David's Medical Center Austin, TX 450431 10
St. Joseph's Hospital Tampa, FL 100075 3
Texas Health Harris Methodist Hospital Southwest Fort Worth Fort Worth, TX 450779 4
University of Maryland St. Joseph Medical Center Towson, MD 210063 1
WellStar West Georgia Medical Center LaGrange, GA 110016 3
* Everest Award winners are in bold type.
9Medium community hospitals* Hospitals Location Medicare ID Total year(s) won AdventHealth Wesley Chapel Wesley Chapel, FL 100319 2 Dupont Hospital Fort Wayne, IN 150150 5 East Cooper Medical Center Mt. Pleasant, SC 420089 1 East Liverpool City Hospital East Liverpool, OH 360096 2 Garden Grove Hospital Medical Center Garden Grove, CA 050230 5 IU Health North Hospital Carmel, IN 150161 2 IU Health West Hospital Avon, IN 150158 1 Logan Regional Hospital Logan, UT 460015 9 Memorial Hermann Katy Hospital Katy, TX 450847 3 Mercy Health - Clermont Hospital Batavia, OH 360236 10 Mercy Hospital Northwest Arkansas Rogers, AR 040010 1 Mercy Medical Center Cedar Rapids, IA 160079 7 Montclair Hospital Medical Center Montclair, CA 050758 4 Mountain View Hospital Payson, UT 460013 3 Northwestern Medicine Delnor Hospital Geneva, IL 140211 1 St. Luke's Anderson Campus Easton, PA 390326 1 St. Vincent's Medical Center Clay County Middleburg, FL 100321 1 UCHealth Medical Center of the Rockies Loveland, CO 060119 3 West Valley Medical Center Caldwell, ID 130014 6 Wooster Community Hospital Wooster, OH 360036 5 *Everest Award winners are in bold type. 10 IBM Watson Health
Small community hospitals*
Hospitals Location Medicare ID Total year(s) won
Alta View Hospital Sandy, UT 460044 6
Aurora Medical Center Two Rivers, WI 520034 3
Brigham City Community Hospital Brigham City, UT 460017 5
Buffalo Hospital Buffalo, MN 240076 5
Cedar City Hospital Cedar City, UT 460007 8
Hill Country Memorial Hospital Fredericksburg, TX 450604 8
Lakeview Hospital Bountiful, UT 460042 9
Lone Peak Hospital Draper, UT 460060 1
Marshfield Medical Center Rice Lake, WI 520011 4
Nanticoke Memorial Hospital Seaford, DE 080006 1
Parkview Noble Hospital Kendallville, IN 150146 2
Parkview Whitley Hospital Columbia City, IN 150101 1
Piedmont Mountainside Hospital Jasper, GA 110225 1
San Dimas Community Hospital San Dimas, CA 050588 3
Seton Medical Center Harker Heights Harker Heights, TX 670080 1
Southern Tennessee Regional Health System Lawrenceburg, TN 440175 2
Spectrum Health Zeeland Community Hospital Zeeland, MI 230003 5
St. John Owasso Hospital Owasso, OK 370227 3
St. Luke's Hospital - Quakertown Quakertown, PA 390035 2
Stillwater Medical Center Stillwater, OK 370049 2
*Everest Award winners are in bold type.
11This award recognizes the boards, executives, and
2019 Everest medical staff leaders who developed and executed
the strategies that drove the highest rates of
Award winners improvement, resulting in the highest performance
in the US at the end of five years.
The Watson Health 100 Top Hospitals® Everest
Award honors hospitals that have both the highest The Everest Award winners are a special group
current performance and the fastest long-term of the 100 Top Hospitals award winners that, in
improvement in the years of data analyzed. addition to achieving benchmark status for one
year, have simultaneously set national benchmarks
for the fastest long-term improvement on our
national balanced scorecard. In 2019, only 15
organizations achieved this level of performance.
The 2019 Everest Award winners
IBM Watson Health™ is pleased to present
the winners of the 2019 100 Top Hospitals
Everest Award.
2019 Everest Award winners
Hospitals Location Medicare ID Total year(s) won
Advocate Sherman Hospital Elgin, IL 140030 2
CHRISTUS St. Michael Health System Texarkana, TX 450801 1
East Liverpool City Hospital East Liverpool, OH 360096 2
Garden City Hospital Garden City, MI 230244 1
IU Health Bloomington Hospital Bloomington, IN 150051 1
Parkview Regional Medical Center Fort Wayne, IN 150021 1
Parkview Whitley Hospital Columbia City, IN 150101 1
Rose Medical Center Denver, CO 060032 1
Sentara Leigh Hospital Norfolk, VA 490046 2
St. Joseph Mercy Hospital Ann Arbor, MI 230156 3
St. Joseph's Hospital Tampa, FL 100075 2
St. Mark's Hospital Salt Lake City, UT 460047 1
Stillwater Medical Center Stillwater, OK 370049 1
UCHealth University of Colorado Hospital Aurora, CO 060024 1
Utah Valley Hospital Provo, UT 460001 1
13The value of the Everest Award measures to the –– What incentives do we need to implement
healthcare industry for management to achieve the desired
Leaders facing the challenges of a rapidly changing improvement more quickly?
healthcare environment may benefit from unbiased –– Will the investments we are considering help
intelligence that provides objective insights into us achieve improvement goals?
complex organizational performance. Those
insights may also help leaders balance short- and –– Can we quantify the long- and short-term
long-term goals to drive continuous gains in increases in value our hospital has provided to
performance and value. our community?
Transparency may present hospital boards and
CEOs with a public challenge to increase the value How we select the Everest Award winners
of core services to their communities. Providing Winners of the 100 Top Hospitals Everest
value is characteristically not a one-time event; it Award set national benchmarks for both fastest
is a continuous process of increasing worth over rate of improvement and highest current year
time. The goal of the 100 Top Hospitals program performance on the study’s balanced scorecard.
is to provide information that can help inform
the leadership decisions that guide hospitals to Everest Award winners are selected from among
achieve those objectives. the new 100 Top Hospitals award winners. The
national award and the Everest Award are based on
We believe the greatest value can be achieved a set of measures that reflect performance across
when leaders integrate knowledge of their the whole organization.
organization’s performance compared to
national benchmarks with information on rates Our methodology for selecting the Everest Award
of improvement compared to peers. In this way, winners can be summarized in three main steps:
leaders can determine the effectiveness of long-
1. Selecting the annual 100 Top Hospitals award
term strategies that led to current performance and
winners using our objective methodology*
understand where to act to course-correct.
based on publicly available data and a
balanced scorecard of performance measures
Our research is designed to help boards and CEOs
using the most current data available (2017 at
better answer questions such as:
the time of this study)
–– Did our long-term strategies result in a stronger
2. Using our five-year (2013 - 2017) trending
hospital across all performance areas?
methodology to select the 100 hospitals
–– Did our strategies drive improvement in some that have shown the fastest, most consistent
areas but inadvertently cause deteriorating improvement rates on the same balanced
performance in others? scorecard of performance measures
–– What strategies will help us increase the rate of 3. Identifying those hospitals that ranked in the
improvement in the right areas to come closer top 100 on both lists; these hospitals are the
to national performance levels? Everest Award winners
* For full details on how the 100 Top Hospitals winners are selected, see the Methodology section of this document.
14 IBM Watson HealthCombining these two methodologies yields a select For this year’s study, after excluding hospitals
group of Everest Award winners. The number with insufficient, missing, or invalid data, along
of winners will vary every year, based solely on with hospitals that would skew study results (for
performance in the two dimensions. example, specialty hospitals), we had a database
study group of 2,752 hospitals.
Comparison groups
Because bed size and teaching status have an
Top Everest Most improved effect on the types of patients a hospital treats
performance, Award performance, and the scope of services it provides, we assigned
current year winners five years each hospital in the study database to one of
five comparison groups according to its size and
teaching status (for definitions of each group, see
the Methodology section of this document):
–– Major teaching hospitals
––Teaching hospitals
Data sources
As with all 100 Top Hospitals studies, our –– Large community hospitals
methodology is designed to be objective, and –– Medium community hospitals
all data comes from public sources. We build a
database of short-term, acute care, nonfederal US –– Small community hospitals
hospitals that treat a broad spectrum of patients.
The primary data sources are the Medicare Provider To support evaluating hospitals fairly and
Analysis and Review (MEDPAR) patient claims data comparing them to like hospitals, we use these
set, the Centers for Medicare & Medicaid Services comparison groups for all scoring and ranking to
Hospital Compare hospital performance data set, uncover winners. For more information on how we
and the Hospital Cost Report Information System build the database, see the Methodology section.
Medicare Cost Report file. We use the most recent
five years of data available for trending and the
most current year for selection of winners*.
Residency program information, used in classifying
teaching hospitals, is from the Accreditation
Council for Graduate Medical Education (AMA-
accredited programs) and the American
Osteopathic Association.
* Hospital inpatient mortality and complications are based on two years of data combined for each study year data point. See the Performance Measures section of this
document for details.
15Performance measures present-on-admission (POA) data in our proprietary
Both the 100 Top Hospitals and the Everest Awards risk models. POA coding became available in the
are based on a set of measures that, taken together, 2009 MEDPAR data set.
are designed to assess balanced performance
across the organization, reflecting the leadership For the inpatient mortality and complications
effectiveness of board members, management, and (clinical measures with low frequency of
medical and nursing staff. These measures fall into occurrence), we combine two years of data for
five domains of performance: inpatient outcomes, each study year to stabilize results. This year, we
extended outcomes, operational efficiency, combined data sets as follows:
financial health, and patient experience. –– Study year 2017 = 2017 and 2016 MEDPAR
data sets
The 10 measures used to select the 2019
winners are: –– Study year 2016 = 2016 and 2015 MEDPAR
data sets
1. Risk-adjusted inpatient mortality index
–– Study year 2015 = 2015 and 2014 MEDPAR
2. Risk-adjusted complications index data sets
3. Mean healthcare-associated infection index –– Study year 2014 = 2014 and 2013 MEDPAR
4. Mean 30-day risk-adjusted mortality rate data sets
(includes acute myocardial infarction [AMI]), –– Study year 2013 = 2013 and 2012 MEDPAR
heart failure [HF], pneumonia, chronic data sets
obstructive pulmonary disease [COPD],
and stroke) For specific data periods used for each measure,
5. Mean 30-day risk-adjusted readmission rate see page 47 of the Methodology section.
(includes AMI, HF, pneumonia, THA/TKA,
COPD, and stroke)
6. Severity-adjusted average length of stay
7. Mean emergency department throughput
(in minutes)
8. Case mix- and wage-adjusted inpatient
expense per discharge
9. Adjusted operating profit margin
10. Hospital Consumer Assessment of
Healthcare Providers and Systems score
(overall hospital performance)
For full details, including calculation and scoring
methods, see the Methodology section. We use
16 IBM Watson HealthRanking and five-year trend summary
To select the 100 Top Hospitals award winners,
we rank hospitals on current year performance
on each of the study measures relative to other
hospitals in their comparison group. We then sum
each hospital’s performance-measure rankings and
re-rank them, overall, to arrive at a final rank for
the hospital. The hospitals with the best final ranks
in each comparison group are selected as the 100
Top Hospitals award winners. See the Methodology
section for details on the ranking methodology,
including measures, weighting, and selection of
100 Top Hospitals winners.
Separately, for every hospital in the study, we
calculate a t-statistic that measures five-year
performance improvement for each of the included
performance measures. This statistic measures the
direction and magnitude of change in performance,
and the statistical significance of that change. We
rank hospitals on the basis of their performance
improvement t-statistic on each of the study
measures relative to other hospitals in their
comparison group. We then sum each hospital’s
performance-measure rankings and re-rank them
overall, to arrive at a final rank for the hospital.
The hospitals with the best final rank in each
comparison group are selected as the performance
improvement benchmark hospitals. See the
Methodology section for details on trending,
including measure weighting.
As our final step, we find those hospitals that are
identified as benchmarks on both lists. These
hospitals are the Everest Award winners.
17–– Over 155,000 fewer discharged patients
Findings would be readmitted within 30 days
–– Patients would spend 17 minutes less in
The Watson Health 100 Top Hospitals® study hospital emergency rooms per visit
shines a light on the top-performing hospitals in
the country. According to publicly available data We based this analysis on the Medicare patients
and our transparent methodologies, these industry included in this study. If the same standards were
leaders appear to have successfully negotiated applied to all inpatients, the impact would be
the fine line between running highly effective even greater.
operations and being innovative and forward-
thinking in ways that grow their organizations over Note: All currency amounts listed in this 100 Top
the short and long term. Hospitals study are in US dollars.
Year after year, the public data we have gathered
for the 100 Top Hospitals studies has provided How the winning hospitals compared to
numerous examples of benchmark hospitals’ their peers
clinical, financial and operational excellence and In this section, we show how the 100 Top Hospitals
affirmed the validity and stability of this approach performed within their comparison groups
to performance measurement2–28. (major teaching, teaching, large community,
medium community, and small community
The study is more than a list of accomplishments; it hospitals), compared with nonwinning peers. For
is a method US hospital and health system leaders performance measure details and definitions of
can use to help guide their own performance each comparison group, see the Methodology
improvement initiatives. By highlighting what the section of this document.
highest-performing leaders around the country are
doing well, we create aspirational benchmarks for Note: In Tables 1 through 6, data for the 100 Top
the rest of the industry. Hospitals award winners is labeled “Benchmark,”
and data for all hospitals, excluding award winners,
Based on comparisons between the 100 Top is labeled “Peer group.” In columns labeled
Hospitals study winners and a peer group of similar “Benchmark compared with peer group,” we
hospitals that were not winners, we found that calculated the actual and percentage difference
if all hospitals performed at the level of this between the benchmark hospital scores and the
year’s winners: peer group scores.
–– Over 103,000 additional lives could be saved
in-hospital 100 Top Hospitals had better survival rates*
–– Over 38,000 additional patients could be –– Overall, the winners had 24% fewer deaths
complication-free than expected (0.76 index), considering patient
severity, while their nonwinning peers had 1%
–– Over $8.2 billion in inpatient costs could more deaths than would be expected (1.01
be saved index) (Table 1)
––The typical patient could be released from –– Small community hospitals had the most
the hospital a half day sooner and would dramatic difference between winners and
have 12% fewer expenses related to the nonwinners; the winning small hospital median
complete episode of care than the median mortality rate was 47% lower than nonwinning
patient in the US peers (Table 6)
* Risk-adjusted measures are normalized by comparison group, so results cannot be compared across comparison groups.
19–– Medium-sized community hospitals also had –– Overall, nationally, there were 35% fewer
a significantly lower median mortality index infections than expected at winning hospitals
values than nonwinning peer hospitals, with a (0.65 standardized infection ratio [SIR]
29.5% lower mortality index (Table 5) median), compared to 19% fewer infections
at peer nonwinning hospitals (0.81 SIR
100 Top Hospitals had fewer patient complications* median)*** (Table 1)
–– Overall, patients at the winning hospitals had –– On the HAI composite index, medium
23% fewer complications than expected (0.77 community hospitals showed the widest
index), considering patient severity, while difference between winning benchmark
their nonwinning peers had only 5% fewer hospital performance and nonwinners,
complications than expected (0.95 index)*** with the winning median HAI composite
(Table 1) index 30% lower than the median value of
nonwinners (0.51 and 0.73 median SIR values,
–– For complications, as with inpatient mortality,
respectively) (Table 5)
small community hospitals had the most
dramatic difference between winners and ––The winners among major teaching hospitals
nonwinners; the winning small hospital median had 19% fewer infections than expected (0.81
observed-to-expected ratio of complications SIR median), while their nonwinning major
was 41.5% lower than nonwinning peers’ index teaching peers had only 7% fewer infections
value (0.54 versus 0.92) (Table 6) than expected (0.93 SIR median) (Table 2)
100 Top Hospitals had fewer healthcare- 100 Top Hospitals had lower 30-day mortality
associated infections and readmission rates
Healthcare-associated infections (HAIs)**, Several patient groups are included in the 30-
captures information about the quality of inpatient day mortality and readmission extended care
care. Based on nation-wide data availability, we composite metrics. The mean 30-day mortality
built a composite measure of HAI performance rate includes heart attack (AMI), heart failure (HF),
at the hospital level, considering up to six HAIs, pneumonia, chronic obstructive pulmonary disease
depending on assigned comparison group. (The (COPD), and stroke patient groups. The mean 30-
HAI measure is not ranked for small community day readmission rate includes AMI, HF, pneumonia,
hospitals in the 2019 study.) The six reported HAIs total hip arthroplasty and/or total knee arthroplasty
are: methicillin-resistant staphylococcus aureus (THA/TKA), COPD, and stroke patient groups.
(MRSA-bloodstream), central line-associated blood
–– Mean 30-day mortality and readmission rates
stream infections, catheter-associated urinary tract
were lower at the winning hospitals than
infections, clostridium difficile (C.diff), surgical site
nonwinning hospitals, across all comparison
infections (SSIs) following colon surgery, and SSIs
groups (by 0.6 and 0.4 percentage points,
following an abdominal hysterectomy.
respectively) (Table 1)
* Risk-adjusted measures are normalized by comparison group, so results cannot be compared across comparison groups.
** As developed by the National Healthcare Safety Network and reported by the Centers for Medicare & Medicaid Services (CMS) in the public Hospital Compare data set.
*** Mortality, complications and HAI index values are calculated using a subset of hospitals from which the measures are developed, which is why there will be instances
where both peer and bench indexes are below 1.0 .
20 IBM Watson Health–– Major teaching hospital winners continued ––The most dramatic difference in emergency
to demonstrate the best 30-day mortality department (ED) service delivery times
performance among all hospital comparison between winning hospitals and their peers
groups, with a median rate at 11.7%) (Table 2) occurred in the major teaching category where
there was 69.3 minutes less time-to-service;
–– Small community hospital winners again had
winning teaching hospitals followed right
the best 30-day readmission performance
behind with 41.5 minutes less time-to-service
among all comparison groups (14.3%)
(Tables 2 and 3)
(Table 6)
–– However, major teaching hospitals had the
–– Major teaching hospital winners outperformed
longest throughput times of all comparison
nonwinners on 30-day readmissions by the
groups, at 246.5 minutes for winners and
greatest margin (0.7 percentage points)
315.8 minutes for nonwinners (Tables 2
(Table 2)
through 6)
Patients treated at 100 Top Hospitals returned –– Small community hospitals had the shortest
home sooner* throughput times of all comparison groups for
both winning and nonwinning hospitals (163
–– Overall, winning hospitals had a median
and 182.5 minutes, respectively) (Table 6)
severity-adjusted average length of stay (LOS)
that was a 0.5 day shorter than peers (Table 1)
100 Top Hospitals had lower inpatient expenses
–– Both the winning small- and medium-sized
––The findings show that overall, and in all
community hospitals had a large difference
comparison groups, the winning hospital
from the non-winners in average LOS, with
median for case mix- and wage-adjusted
a median average LOS of 0.7 days shorter
inpatient expense per discharge was lower
(Tables 5 and 6)
than the median for nonwinner peers this
–– Among major teaching hospitals, there was year (Tables 1 through 6)
also a large difference between winners and
–– Medium community hospital winners and
nonwinners on median average LOS, at 4.3
nonwinners had the lowest case mix- and
days versus 4.9 days (a 13.0% difference)
wage-adjusted inpatient expense per
(Table 2)
discharge than any other comparison
group with expenses at $5,894 and $6,742,
Patients spent less time in 100 Top Hospitals
respectively (Table 5)
emergency departments
––The largest difference in expenses between
–– Overall, winning hospitals had shorter median
and winning and non-winning hospitals was
wait times for emergency services** than their
found in the small hospital comparison group
peers, by 8% (Table 1)
with a difference of $1,340 (Table 6)
* Risk-adjusted measures are normalized by comparison group, so results cannot be compared across comparison groups.
** Includes median time from ED arrival to ED departure for admitted patients and median time from ED arrival to ED departure for non-admitted patients.
21100 Top Hospitals were more profitable
–– Overall, winning hospitals had a median
operating profit margin that was 11.9
percentage points higher than nonwinning
hospitals (15.6% versus 3.8%) (Table 1)
–– Profitability difference was the most dramatic
in the medium community hospital group,
where winners had operating profit margins
that were 17.1 percentage points higher than
nonwinners (Table 5)
–– Medium hospital winners also had the largest
median operating profit margin of any winning
group at 21.5% (Table 5)
–– In contrast, small community hospital winners
had the lowest median operating profit margin
of any winning group at 12.9% (Table 6)
Patients rated 100 Top Hospitals higher than
peer hospitals
–– Patients treated at the 100 Top Hospitals
reported a better overall hospital experience
than those treated in peer hospitals, with
a 3.0% higher median Hospital Consumer
Assessment of Healthcare Providers and
Systems (HCAHPS) overall rating score
(Table 1)
––The winning small community hospitals had
the highest median HCAHPS score of all
comparison groups, at 273 versus 265 for
nonwinners (maximum score is 300) (Table 6)
–– Large community hospital winners had the
biggest performance difference over peers
(4.0 % higher HCAHPS scores) among all
comparison groups (Table 4)
22 IBM Watson HealthTable 1. National performance comparisons (all hospitals in study)
Domain Performance measure Medians Benchmark compared with peer group
Benchmark
hospitals Peer hospitals Percent
(winners) (nonwinners) Difference difference Comments
Clinical Inpatient Mortality Index 1
0.76 1.01 -0.25 -24.9% Lower mortality
Outcomes
Complications Index 1
0.77 0.95 -0.18 -18.7% Fewer complications
HAI Index 2
0.65 0.81 -0.2 -19.3% Fewer infections
Extended 30-Day Mortality Rate3 12.0 12.7 -0.6 n/a6 Lower 30-day mortality
Outcomes
30-Day Readmission Rate3 14.5 14.9 -0.4 n/a6 Fewer 30-day readmissions
Operational Average Length of Stay 1
4.3 4.7 -0.5 -10.1% Shorter stays
Efficiency
ED Throughput Measure 4
196.8 214.0 -17.3 -8.1% Less time to service
Inpatient Expense per Discharge 5
$6,150 $6,980 -$830 -11.9% Lower inpatient cost
Financial
Operating Profit Margin5 15.6 3.8 11.9 n/a6 Higher profitability
Health
Patient Hospital Consumer Assessment of 271.0 263.0 8.0 3.0% Better patient experience
Experience Healthcare Providers and Systems
(HCAHPS) score4
1
Mortality, complications and average length of stay based on Present on Admission (POA)-enabled risk models applied to MedPAR 2016 and 2017 data (ALOS 2017 only).
2
Healthcare-Associated Infections (HAI) data from CMS Hospital Compare Jan 1, 2017 - Dec 31, 2017 data set (excluding Small Community Hospitals).
3
30-day rates from CMS Hospital Compare July 1, 2014-June 30, 2017 data set.
4
ED measure and HCAHPS data from CMS Hospital Compare Jan 1, 2017-Dec 31, 2017 data set.
5
Inpatient expense and operating profit margin data from CMS Hospital Cost Report Information System (HCRIS) data file, 2017.
6
We do not calculate percent difference for this measure because it is already a percent value.
23Table 2. Major teaching hospital performance comparisons
Domain Performance measure Medians Benchmark compared with peer group
Benchmark Peer hospitals Difference Percent How winning benchmark
hospitals (nonwinners) difference hospitals outperformed
(winners) nonwinning peer hospitals
Clinical Inpatient Mortality Index1 0.82 1.01 -0.19 -19.0% Lower mortality
Outcomes
Complications Index 1
0.95 1.03 -0.08 -8.0% Fewer complications
HAI Index 2
0.81 0.93 -0.1 -13.9% Fewer infections
Extended 30-Day Mortality Rate3 11.7 12.2 -0.6 n/a6 Lower 30-day mortality
Outcomes
30-Day Readmission Rate3 14.6 15.4 -0.7 n/a6 Fewer 30-day readmissions
Operational Average Length of Stay 1
4.3 4.9 -0.6 -13.0% Shorter stays
Efficiency
ED Throughput Measure 4
246.5 315.8 -69.3 -21.9% Less time to service
Inpatient Expense per Discharge 5
$6,761 $8,027 -$1,267 -15.8% Lower inpatient cost
Financial Operating Profit Margin 5
13.1 2.6 10.6 n/a 6
Higher profitability
Health
Patient HCAHPS Score4 270.0 263.0 7.0 2.7% Better patient experience
Experience
1
Mortality, complications and average length of stay based on Present on Admission (POA)-enabled risk models applied to MedPAR 2016 and 2017 data (ALOS 2017 only).
2
Healthcare-Associated Infections (HAI) data from CMS Hospital Compare Jan 1, 2017 - Dec 31, 2017 data set (excluding Small Community Hospitals).
3
30-day rates from CMS Hospital Compare July 1, 2014-June 30, 2017 data set.
4
ED measure and HCAHPS data from CMS Hospital Compare Jan 1, 2017-Dec 31, 2017 data set.
5
Inpatient expense and operating profit margin data from CMS Hospital Cost Report Information System (HCRIS) data file, 2017.
6
We do not calculate percent difference for this measure because it is already a percent value.
Table 3. Teaching hospital performance comparisons
Domain Performance measure Medians Benchmark compared with peer group
Benchmark Peer hospitals Difference Percent How winning benchmark
hospitals (nonwinners) difference hospitals outperformed
(winners) nonwinning peer hospitals
Clinical Inpatient Mortality Index1 0.82 1.00 -0.18 -18.2% Lower mortality
Outcomes
Complications Index 1
0.79 1.00 -0.20 -20.3% Fewer complications
HAI Index2 0.62 0.84 -0.2 -26.5% Fewer infections
Extended 30-Day Mortality Rate 3
12.1 12.7 -0.6 n/a 6
Lower 30-day mortality
Outcomes
30-Day Readmission Rate 3
14.5 15.0 -0.5 n/a 6
Fewer 30-day readmissions
Operational Average Length of Stay 1
4.4 4.9 -0.5 -11.2% Shorter stays
Efficiency
ED Throughput Measure 4
199.0 240.5 -41.5 -17.3% Less time to service
Inpatient Expense per Discharge5 $6,152 $6,797 -$645 -9.5% Lower inpatient cost
Financial Operating Profit Margin5 15.4 5.1 10.3 n/a6 Higher profitability
Health
Patient HCAHPS Score4 270.0 263.0 7.0 2.7% Better patient experience
Experience
1
Mortality, complications and average length of stay based on Present on Admission (POA)-enabled risk models applied to MedPAR 2016 and 2017 data (ALOS 2017 only).
2
Healthcare-Associated Infections (HAI) data from CMS Hospital Compare Jan 1, 2017 - Dec 31, 2017 data set (excluding Small Community Hospitals).
3
30-day rates from CMS Hospital Compare July 1, 2014-June 30, 2017 data set.
4
ED measure and HCAHPS data from CMS Hospital Compare Jan 1, 2017-Dec 31, 2017 data set.
5
Inpatient expense and operating profit margin data from CMS Hospital Cost Report Information System (HCRIS) data file, 2017.
6
We do not calculate percent difference for this measure because it is already a percent value.
24 IBM Watson HealthTable 4. Large community hospital performance comparisons
Domain Performance measure Medians Benchmark compared with peer group
Benchmark Peer hospitals Difference Percent How winning benchmark
hospitals (nonwinners) difference hospitals outperformed
(winners) nonwinning peer hospitals
Clinical Inpatient Mortality Index1 0.80 1.02 -0.22 -21.8% Lower mortality
Outcomes
Complications Index 1
0.86 1.00 -0.14 -14.0% Fewer complications
HAI Index 2
0.70 0.82 -0.1 -14.2% Fewer infections
Extended 30-Day Mortality Rate3 12.3 12.6 -0.3 n/a6 Lower 30-day mortality
Outcomes
30-Day Readmission Rate3 14.5 15.1 -0.6 n/a6 Fewer 30-day readmissions
Operational Average Length of Stay 1
4.6 5.0 -0.4 -8.3% Shorter stays
Efficiency
ED Throughput Measure 4
218.8 238.5 -19.8 -8.3% Less time to service
Inpatient Expense per Discharge 5
$6,231 $6,776 -$544 -8.0% Lower inpatient cost
Financial Operating Profit Margin 5
16.4 6.9 9.6 n/a 6
Higher profitability
Health
Patient HCAHPS Score4 272.5 262.0 10.5 4.0% Better patient experience
Experience
1
Mortality, complications and average length of stay based on Present on Admission (POA)-enabled risk models applied to MedPAR 2016 and 2017 data (ALOS 2017 only).
2
Healthcare-Associated Infections (HAI) data from CMS Hospital Compare Jan 1, 2017 - Dec 31, 2017 data set (excluding Small Community Hospitals).
3
30-day rates from CMS Hospital Compare July 1, 2014-June 30, 2017 data set.
4
ED measure and HCAHPS data from CMS Hospital Compare Jan 1, 2017-Dec 31, 2017 data set.
5
Inpatient expense and operating profit margin data from CMS Hospital Cost Report Information System (HCRIS) data file, 2017.
6
We do not calculate percent difference for this measure because it is already a percent value.
Table 5. Medium community hospital performance comparisons
Domain Performance measure Medians Benchmark compared with peer group
Benchmark Peer hospitals Difference Percent How winning benchmark
hospitals (nonwinners) difference hospitals outperformed
(winners) nonwinning peer hospitals
Clinical Inpatient Mortality Index1 0.68 0.97 -0.29 -29.5% Lower mortality
Outcomes
Complications Index 1
0.72 0.99 -0.26 -26.8% Fewer complications
HAI Index2 0.51 0.73 -0.2 -30.0% Fewer infections
Extended 30-Day Mortality Rate 3
12.1 12.7 -0.6 n/a 6
Lower 30-day mortality
Outcomes
30-Day Readmission Rate 3
14.8 15.0 -0.3 n/a 6
Fewer 30-day readmissions
Operational Average Length of Stay 1
4.2 4.9 -0.7 -13.9% Shorter stays
Efficiency
ED Throughput Measure 4
188.8 213.5 -24.8 -11.6% Less time to service
Inpatient Expense per Discharge5 $5,894 $6,742 -$848 -12.6% Lower inpatient cost
Financial Operating Profit Margin5 21.5 4.4 17.1 n/a6 Higher profitability
Health
Patient HCAHPS Score4 271.5 262.0 9.5 3.6% Better patient experience
Experience
1
Mortality, complications and average length of stay based on Present on Admission (POA)-enabled risk models applied to MedPAR 2016 and 2017 data (ALOS 2017 only).
2
Healthcare-Associated Infections (HAI) data from CMS Hospital Compare Jan 1, 2017 - Dec 31, 2017 data set (excluding Small Community Hospitals).
3
30-day rates from CMS Hospital Compare July 1, 2014-June 30, 2017 data set.
4
ED measure and HCAHPS data from CMS Hospital Compare Jan 1, 2017-Dec 31, 2017 data set.
5
Inpatient expense and operating profit margin data from CMS Hospital Cost Report Information System (HCRIS) data file, 2017.
6
We do not calculate percent difference for this measure because it is already a percent value.
25Table 6. Small community hospital comparisons
Domain Performance measure Medians Benchmark compared with peer group
Benchmark Peer hospitals Difference Percent How winning benchmark
hospitals (nonwinners) difference hospitals outperformed
(winners) nonwinning peer hospitals
Clinical Inpatient Mortality Index1 0.53 1.01 -0.47 -47.2% Lower mortality
Outcomes
Complications Index 1
0.54 0.92 -0.38 -41.5% Fewer complications
HAI Index 2
n/a n/a n/a n/a n/a
Extended 30-Day Mortality Rate3 12.1 12.7 -0.6 n/a6 Lower 30-day mortality
Outcomes
30-Day Readmission Rate3 14.3 14.7 -0.3 n/a6 Fewer 30-day readmissions
Operational Average Length of Stay 1
4.2 4.9 -0.7 -13.6% Shorter stays
Efficiency
ED Throughput Measure 4
163.0 182.5 -19.5 -10.7% Less time to service
Inpatient Expense per Discharge 5
$6,039 $7,379 -$1,340 -18.2% Lower inpatient cost
Financial Operating Profit Margin 5
12.9 1.8 11.0 n/a 6
Higher profitability
Health
Patient HCAHPS Score4 273.0 265.0 8.0 3.0% Better patient experience
Experience
1
Mortality, complications and average length of stay based on Present on Admission (POA)-enabled risk models applied to MedPAR 2016 and 2017 data (ALOS 2017 only).
2
Healthcare-Associated Infections (HAI) data from CMS Hospital Compare Jan 1, 2017 - Dec 31, 2017 data set (excluding Small Community Hospitals).
3
30-day rates from CMS Hospital Compare July 1, 2014-June 30, 2017 data set.
4
ED measure and HCAHPS data from CMS Hospital Compare Jan 1, 2017-Dec 31, 2017 data set.
5
Inpatient expense and operating profit margin data from CMS Hospital Cost Report Information System (HCRIS) data file, 2017.
6
We do not calculate percent difference for this measure because it is already a percent value.
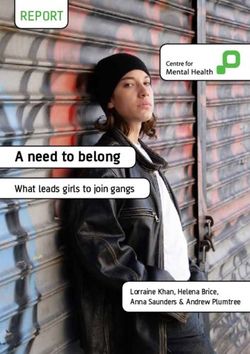
US map and states by region This analysis allows us to observe geographic
The US maps featured in Figures 1 and 2 patterns in performance. Among our observations:
provide a visual representation of the variability ––The Midwest continues to be the frontrunner
in performance across the country for the current in percentage of states in the top two
and previous studies (2019 and 2018). Additionally, performance quintiles versus other regions,
Table 7 shows each state’s rank quintile although with a slight decrease in this lead
performance, grouped by geographic region, for this year (83.3% of states in 2019 versus
the current and previous year studies. 91.7% in 2018)
To produce this data, we calculated the 100 Top ––The Northeast continues to show the poorest
Hospitals measures at the state level*, ranked each performance overall, by a large margin in both
measure, then weighted and summed the ranks to years, with 66.7% of its states in the bottom
produce an overall state performance score. States two quintiles in 2019 and 77.8% in 2018
were ranked from best to worst on the overall score, ––The South continues to show the same pattern
and the results are reported as rank quintiles. as last year with the majority of its states in
the bottom two quintiles (47.1% in 2019 and
52.9% in 2018)
* Each state measure is calculated from the acute care hospital data for that state (short-term, general acute care hospitals; critical access hospitals; and cardiac, orthopedic,
and women’s hospitals) with valid data for the included measures. Inpatient mortality, complications, and average LOS are aggregated from MEDPAR patient record data. HAIs,
30-day mortality rates, and 30-day readmission rates are aggregated from the numerator and denominator data for each hospital. Inpatient expense per discharge, operating
profit margin, and HCAHPS scores are hospital values weighted by the number of acute discharges at each hospital. Mean ED throughput is calculated by averaging the median
minutes of member hospitals to produce the unweighted mean minutes for each ED measure, then averaging the two ED measures to produce the state-level unweighted ED
throughput measure. For expense, profit, and HCAHPS, a mean weighted value is calculated for each state by summing the weighted hospital values and dividing by the sum of the
weights. To calculate the state overall score, individual measure ranks are weighted, using the same measure rank weights as in the 100 Top Hospitals study, then summed.
26 IBM Watson HealthFigure 1. State-level performance comparisons, 2019 study
WA
ME
MT
ND
MN VT
OR NH
MA
ID WI NY
SD RI
MI CT
WY
PA
IA NJ
NE
OH MD
NV IN DE
UT IL
WV
CO VA
DC (red)
KS MO
CA KY
NC
TN
AZ OK
SC
NM AR
MS AL GA
100 Top Hospitals performance
2019 study state-level rankings
TX LA
Quintile 1 - Best
FL
Quintile 2
HI
Quintile 3
AK
Quintile 4
Quintile 5 - Worst
State data note: The 2019 state findings were based on the 100 Top Hospitals measure methodologies, using 2016 and 2017 MEDPAR data
(combined) for inpatient mortality and complications; July 1, 2014- June 30, 2017, for 30-day rates, and 2017 data for all other measures.
27Figure 2. State-level performance comparisons, 2018 study
WA
ME
MT
ND
MN VT
OR NH
MA
ID WI NY
SD RI
MI CT
WY
PA
IA
NJ
NE
OH
NV IN DE
UT IL
WV MD
CO VA
DC (red)
KS MO
CA KY
NC
TN
AZ OK
SC
NM AR
MS AL GA
100 Top Hospitals performance
2019 study state-level rankings
TX LA
Quintile 1 - Best
FL
Quintile 2
HI
Quintile 3
AK
Quintile 4
Quintile 5 - Worst
State data note: The 2018 state findings were based on the 100 Top Hospitals measure methodologies, using 2015 and 2016 MEDPAR data
(combined) for inpatient mortality and complications; July 1, 2013- June 30, 2016, for 30-day rates, and 2016 data for all other measures.
28 IBM Watson HealthTable 7. 100 Top Hospitals two-year state-level performance comparisons
ME
Northeast Midwest South West
Current
VT study Previous study Current study Previous study Current study Previous study Current study Previous study
NH
NY Connecticut
MA Connecticut Illinois Illinois Alabama Alabama Alaska Alaska
RI
CT
Maine Maine Indiana Indiana Arkansas Arkansas Arizona Arizona
PA Massachusetts Massachusetts Iowa Iowa Delaware Delaware California California
NJ
New Hampshire
DE
New Hampshire Kansas Kansas District of District of Colorado Colorado
MD
Columbia Columbia
VA
DC (red)
New Jersey New Jersey Michigan Michigan Florida Florida Hawaii Hawaii
NC New York New York Minnesota Minnesota Georgia Georgia Idaho Idaho
Pennsylvania Pennsylvania Missouri Missouri Kentucky Kentucky Montana Montana
SC
Rhode Island Rhode Island Nebraska Nebraska Louisiana Louisiana Nevada Nevada
Vermont Vermont
100 Top Hospitals performance
North Dakota North Dakota Maryland Maryland New Mexico New Mexico
2018 study state-level rankings Ohio Ohio Mississippi Mississippi Oregon Oregon
Quintile 1 - Best South Dakota South Dakota North Carolina North Carolina Utah Utah
FL Wisconsin Wisconsin Oklahoma Oklahoma Washington Washington
Quintile 2
South Carolina South Carolina Wyoming Wyoming
Quintile 3
Tennessee Tennessee
Quintile 4 Texas Texas
Virginia Virginia
Quintile 5 - Worst
West Virginia West Virginia
29Performance improvement over time:
All hospitals
By studying the direction of performance change of
all hospitals in our study (winners and nonwinners),
we can see that US hospitals have not been able
to improve performance much across the entire
balanced scorecard of performance measures
(Table 8).
Notably, only one metric, 30-day readmissions,
had fewer than 75% of in-study hospitals in the
category of “no statistically significant change in
performance.”
Table 8. Direction of performance change for all hospitals in study, 2013 - 2017
Performance measure Significantly improving No statistically significant Significantly declining
performance change in performance performance
Count of Percentage of Count of Percentage of Count of Percentage of
hospitals1 hospitals2 hospitals1 hospitals2 hospitalsa1 hospitals2
Risk-adjusted inpatient mortality index 83 3.1% 2,374 88.1% 238 8.8%
Risk-adjusted complication index 198 7.3% 2,402 89.1% 95 3.5%
30-day mortality rate 33 1.2% 2,405 89.2% 257 9.5%
30-day readmission rate 1510 56.0% 1,165 43.2% 20 0.7%
Severity-adjusted average LOS 476 17.7% 2,050 76.1% 169 6.3%
ED throughput (minutes) 183 6.8% 2,050 76.1% 462 17.1%
Adjusted inpatient expense per discharge 71 2.6% 2,177 81.2% 434 16.2%
Operating profit margin 185 6.9% 2,336 87.0% 165 6.1%
HCAHPS score 286 10.6% 2,287 84.9% 121 4.5%
1. Count refers to the number of in-study hospitals whose performance fell into the highlighted category on the measure.
Note: Total number of hospitals included in the analysis will vary by measure due to exclusion of interquartile range outlier data points.
Inpatient expense and profit are affected. Some in-study hospitals had too few data points remaining to calculate trend.
2. Percent is of total in-study hospitals across all peer groups.
However, over the years we studied (2013 through
2017), many hospitals have been able to raise the
performance bar on many clinical and operational
measures (see green column in Table 8):
–– Over half (56%) of hospitals improved their 30-
day readmission rates, reiterating the attention
these measures continue to receive in payment
system incentives and penalties
–– Only 3.1% of hospitals improved their inpatient
mortality (88% had no change), while the great
majority of hospitals (nearly 90%) also had no
30 IBM Watson HealthYou can also read