16 Human Health - rioccadapt
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

16 Human Health Ana Rosa Moreno Sánchez (Mexico), Marilyn Aparicio Effen (Bolivia), Julio Díaz (Spain), Edgar González-Gaudiano (Mexico), José María Ordóñez Iriarte (Spain), and M. Cristina Tirado von der Pahlen (USA/Spain). This chapter should be cited as: Moreno A.R., M. Aparicio Effen, J. Díaz, E. González-Gaudiano, J.M. Ordóñez Iriar- te, and M.C. Tirado von der Pahlen, 2020: Human Health. In: Adaptation to Climate Change Risks in Ibero-American Countries — RIOCCADAPT Report [Moreno, J.M., C. Laguna-Defior, V. Barros, E. Calvo Buendía, J.A. Marengo, and U. Oswald Spring (eds.)], McGraw Hill, Madrid, Spain (pp. 615-658, ISBN: 9788448621667).

Chapter 16 - Human Health
CO N T E NTS
Executive summary.......................................................................................................................................................................................................................... 618
16.1. Introduction........................................................................................................................................................................................................................... 618
16.1.1. Conceptual framework...................................................................................................................................................................................... 618
16.1.2. Key sector/system figures.............................................................................................................................................................................. 619
16.1.3. Relationship of the sector with climate and climate change......................................................................................................... 620
16.1.4. Review of past reports ..................................................................................................................................................................................... 621
16.2. Risk components in relation to health................................................................................................................................................................... 622
16.2.1. Hazards..................................................................................................................................................................................................................... 622
16.2.2. Exposure................................................................................................................................................................................................................... 623
16.2.3. Vulnerability............................................................................................................................................................................................................ 624
16.3. Characterization of risks and their impacts........................................................................................................................................................ 626
16.3.1. Vector-borne diseases...................................................................................................................................................................................... 626
16.3.2. Extreme weather or climatic events.......................................................................................................................................................... 628
16.3.3. Air pollution............................................................................................................................................................................................................. 629
16.3.4. Water.......................................................................................................................................................................................................................... 630
16.3.5. Food ............................................................................................................................................................................................................................ 631
16.4. Adaptation measures....................................................................................................................................................................................................... 631
16.4.1. Adaptation options............................................................................................................................................................................................. 631
16.4.2. Planned adaptation actions............................................................................................................................................................................ 632
16.4.2.1. At the supranational scale............................................................................................................................................................. 632
16.4.2.2. At the national and subnational scale...................................................................................................................................... 633
16.4.2.3. At the local or municipal scale..................................................................................................................................................... 635
16.4.3. Autonomous adaptation actions.................................................................................................................................................................. 637
16.5. Barriers, opportunities and interactions............................................................................................................................................................... 637
16.6. Measures or indicators of adaptation effectiveness..................................................................................................................................... 638
16.7. Case studies.......................................................................................................................................................................................................................... 638
16.7.1. Vector-borne diseases – Adaptation challenges and options in Bolivia, with an emphasis on the Chaco region 638
16.7.1.1. Case summary..................................................................................................................................................................................... 638
16.7.1.2. Introduction to the case problem.............................................................................................................................................. 640
16.7.1.3. Case description................................................................................................................................................................................. 640
16.7.1.4. Limitations and interactions ....................................................................................................................................................... 642
16.7.1.5. Lessons learned.................................................................................................................................................................................. 643
16.7.2. Plan for Preventive Actions against the Health Effects of Excess Temperatures of the Ministry of Health
(Spain)........................................................................................................................................................................................................................ 643
16.7.2.1. Case Summary..................................................................................................................................................................................... 643
16.7.2.2. Introduction to the case problem.............................................................................................................................................. 643
16.7.2.3. Case description................................................................................................................................................................................. 644
16.7.2.4. Limitations and interactions........................................................................................................................................................ 644
16.7.2.5. Lessons learned.................................................................................................................................................................................. 644
16.7.3. Adaptation and resilience of communities vulnerable to flooding in Veracruz (Mexico)................................................ 644
16.7.3.1. Case summary..................................................................................................................................................................................... 644
616 RIOCCADAPT REPORT
Chapter 16 - Human Health
16.7.3.2. Introduction to the case problem.............................................................................................................................................. 644
16.7.3.3. Case description................................................................................................................................................................................. 645
16.7.3.4. Limitations and interactions........................................................................................................................................................ 645
16.7.3.5. Lessons learned.................................................................................................................................................................................. 645
16.7.4. Aeroallergen warning system in Spain through Red Palinocam................................................................................................... 646
16.7.4.1. Case Summary .................................................................................................................................................................................... 646
16.7.4.2. Introduction to the case problem.............................................................................................................................................. 646
16.7.4.3. Case description................................................................................................................................................................................. 646
16.7.4.4. Limitations and interactions........................................................................................................................................................ 647
16.7.4.5. Lessons learned.................................................................................................................................................................................. 647
16.7.5. Adaptation for food security and nutrition in the Dry Corridor in Central America (Guatemala, Honduras,
El Salvador)............................................................................................................................................................................................................. 647
16.7.5.1. Case summary..................................................................................................................................................................................... 647
16.7.5.2. Introduction to the case problem.............................................................................................................................................. 648
16.7.5.3. Case description ................................................................................................................................................................................ 648
16.7.5.4. Limitations and interactions........................................................................................................................................................ 649
16.7.5.5. Lessons learned.................................................................................................................................................................................. 649
16.8. Main knowledge gaps and priority lines of action........................................................................................................................................... 649
16.9. Conclusions............................................................................................................................................................................................................................ 650
Frequently Asked Questions...................................................................................................................................................................................................... 650
Acknowledgements.......................................................................................................................................................................................................................... 651
Bibliography......................................................................................................................................................................................................................................... 651
RIOCCADAPT REPORT 617
Chapter 16 - Human Health
Executive summary to its allergenic capacity. Risk communication could be the
tool to protect the health of vulnerable populations, such as
people with chronic respiratory problems and those suffering
In the context of the fight against climate change, human from allergies.
health should be considered a priority. There are still uncer-
tainties regarding the impacts of climate change on health. Early warning systems are an essential part of climate
Nevertheless, there is sufficient evidence to justify strength- change adaptation for populations exposed to extreme
ening the resilience of health systems to ensure that adap- hydrometeorological events. Consequently, to protect vul-
tation and mitigation actions effectively protect and promote nerable populations, efforts must be strengthened in terms
health. Consequently, health is best reflected as a priority of managing integrated information systems and communi-
area in climate change negotiations. cating risk to provide timely warnings and promote action;
the availability of trained and well-equipped personnel; and
Populations with fewer resources are the most vulnerable
posessing the necessary infrastructure to manage evacuees
to climate change. Approximately 197 million people in Latin
and provide medium- and long-term needs care to displaced
America were living in poverty in 2017. This condition—along
persons.
with poor infrastructure and health services—increases the
region’s vulnerability to climate change. An adequate health care response must be guaranteed at
both the remedial and preventive stages, which requires
The hazards and risks to health associated with climate
good planning and well-trained professionals from all fields.
change need to be determined and assessed by identify-
Although there is considerable information on the possible
ing vulnerable populations and their exposure to climate
impacts of climate change on vulnerable populations, there
change hazards. Based on this information, geographic infor-
is a lack of policy frameworks and evidence of its impacts
mation systems can be developed to identify, propose, and
at the regional level that would allow decision makers to
implement adaptation measures and co-benefits to reduce
promote the development of health services based on re-
the adverse effects of hazards on these populations.
gional medium- and long-term needs. Health services should
Temperature increases due to heat waves will increase the improve access to safe drinking water, sanitation, and pre-
risk of illness and death in vulnerable populations, such as vention programs such as vaccination, and strengthen sur-
the elderly and individuals with pre-existing diseases. Fur- veillance systems, including for climate-related diseases.
ther warming of urban areas can amplify the impacts of heat Effective planning and training for health professionals from
waves. Adaptation measures should aim to protect vulnerable various disciplines will enable them to provide high-quality,
individuals through early warning systems that inform the climate-adapted health services, ensuring that the popula-
population and raise awareness of protective measures for tion receives the necessary care to cope with the long-term
individuals and families, and of the health services that are challenges of climate change.
prepared to identify and assist people in need of emergency
services. Climate change adaptation is both necessary and urgent to
reduce climate change impacts on health. Health benefits
High temperatures can promote the transmission of vec- from adaptation include reducing the burden of climate-sen-
tor-borne diseases, particularly dengue fever and malaria. sitive diseases, decreasing the effects of climate change on
These diseases could expand their geographical reach and human health, and improving knowledge of the connection
their seasonality could be extended, increasing the number between climate, health, and regions within a country.
of people at risk. Adaptation measures include risk reporting
to prevent the presence of mosquitoes in households and to
protect against their bites. In addition, entomological surveil-
lance to detect vector dynamics should be ongoing. Pesticide 16.1. Introduction
spraying will be required in the event of epidemic outbreaks.
Rising temperatures will worsen the living conditions of 16.1.1. Conceptual framework
vulnerable populations such as farmers, fishers, and people
There is strong evidence that the planet’s climate is chang-
living in food insecurity. This will particularly affect children
ing, mainly due to human activities (IPCC, 2013). Tempera-
under the age of five and those living in poverty, severely
ture increases and sea level rise, changes in rainfall distribu-
threatening their health. Improved agricultural management
tion, and extreme events pose a range of hazards to health,
practices could be adopted to address this problem. Agri-
increasing the diversity of risk scenarios. These hazards vary
cultural biodiversity as a production strategy could support
from the direct effects of heat waves, floods, storms, and
adaptation to environmental pressures such as salinization,
droughts, to conditions associated with ecosystem damage
droughts, and floods, as could implementing programs and
that lead to the transmission of infectious diseases, adverse
policies to promote sustainable agriculture and fisheries.
changes in air pollution, food insecurity and malnutrition, and
Since ozone is temperature-dependent, increased tempera- impacts on socioeconomic sectors (Watts et al., 2018; Ebi et
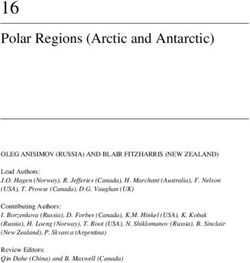
tures can raise the levels of this pollutant and affect the al., 2011). Figure 16.1 illustrates the connections between
health of urban populations, as can pollen production due climate change and human health, summarizing the various
618 RIOCCADAPT REPORTChapter 16 - Human Health
changes in climate due to GHG emissions that have resulted followed by Argentina and El Salvador. Millions of inhabi-
in health and security hazards. tants are therefore highly vulnerable to climate change, which
poses a major challenge for these countries. In terms of
Climate change will increase the difficulty of preventing and
the percentage of GDP allocated to health, in Uruguay this
responding to a wide range of health effects derived from
percentage is high, as it is in Spain and Portugal, followed by
population exposure to climate change hazards. While pop-
Brazil and Ecuador. Regarding this parameter, although the
ulations with fewer resources and greater vulnerability may
be the first to be affected, the fact that climate systems, poverty index for some of these countries is not available,
ecosystems, and global society are interconnected implies one could expect that they enjoy better health conditions and
that virtually no-one will be spared the consequences. have greater possibilities for investment in prevention and
medical care in the face of climate change impacts.
In terms of international health policy, the universal health
16.1.2. Key sector/system figures strategy constitutes the reference framework to improve the
well-being and health of all people, strengthen health sys-
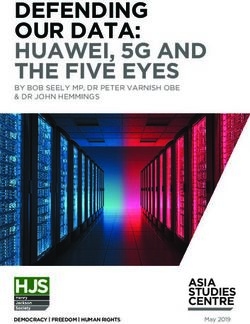
Table 16.1 presents several figures on current health ex- tems, and increase their resilience and ability to respond to
penditure and the national poverty threshold (UNDP, 2018).
challenges such as climate change (PAHO, 2017a).
This information enables visualizing the status of the sector
in terms of economic resources. A heterogeneous distribu- Healthcare benefits in the region are costly, which prevents
tion of poverty can be observed in these countries, with the many people with fewer economic resources from exercis-
highest values found in Honduras, Guatemala, and Mexico, ing their right to health. An estimated one-third of the pop-
GREENHOUSE GAS EMISSIONS
CLIMATE CHANGE
Temperature increase
Other atmospheric
pollutants
Altered rainfall patterns Extreme weather Sea level rise
Extreme events
Social
Reduced
determinants
productivity of
of health
fisheries and
aquaculture
Loss of bio-
Reduced Injuries,
diversity, eco-
agricultural Increase of air pollutants disease
system collapse
productivity and death
and pests
Gastrointestinal
diseases
Impacts on Cardiovascular Respiratory Vector-borne
Malnutrition
mental health diseases diseases diseases
Figure 16.1. Pathways of climate change incidence on human health. Source: compiled by the authors based on Watts et al., 2018, P. 2482.
RIOCCADAPT REPORT 619Chapter 16 - Human Health
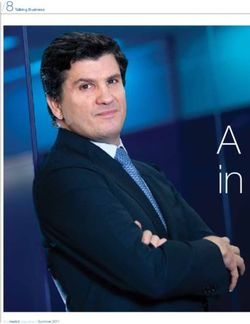
Table 16.1. Various indices and indicators of human development, logical events, the reliability and capacity to maintain these
RIOCC countries. Source: UNDP, 2018. types of services is particularly important from the health
perspective. With regard to water sources, practically all ur-
National poverty ban areas in the region receive this service. Overall, most of
Actual expenditure in
Country threshold, the Latin American region has sanitation services, with the
health, 2015 (% of GDP)
2006–2017 (%)
exception of the Andean Area. However, the figures for san-
Argentina 6.8 39.5 itation coverage are lower, both at the country and regional
Brazil 8.9 8.7 level and in urban areas. Compared to water, the Andean
Area, Central America, and rural areas of Brazil have the
Bolivia 6.4 28.0
poorest sanitation coverage, with unquestionably low figures.
Chile 8.1 * Limitations in both of these services result in conditions of
Colombia 6.2 28.0 vulnerability, with rural areas being noticeably less privileged.
Costa Rica 8.1 * Currently, only 3% of health resources are committed to pre-
Ecuador 8.5 21.5 vention, and only 0.5% of multilateral climate funding has
been specifically allocated to health projects (WHO, 2018a).
El Salvador 6.9 38.2
Spain 9.2 *
Guatemala 5.7 59.3 16.1.3. Relationship of the sector with
Honduras 7.6 60.9 climate and climate change
Mexico 5.9 43.6
According to the WHO (WHO, 2019b), the current situation
Nicaragua 7.8 24.9 and its upcoming challenges call for a transformation in
Panama 7.0 * environmental management as it relates to health. Current
Paraguay 7.8 28.9 approaches have provided a foundation but have been insuf-
ficient to sustainably and adequately reduce environmental
Peru 5.3 20.7
health risks and create favorable conditions for health and
Portugal 9.0 * security. Therefore, the answer is to build a new strategy for
Uruguay 9.2 * health, the environment, and climate change.
Venezuela 3.2 * Climate change undermines the social and environmental
determinants of health, including people’s access to clean
air, clean water, sufficient food, and safe shelter. This affects
health and increases its associated inequality, especially
ulation in the Americas still faces restrictions in accessing in the poorest and most vulnerable communities and least
health services. In addition, a number of obstacles, such
as relocation to rural or hard-to-reach areas and the lack of
well-equipped health centers, limits the provision of services
to people with fewer economic resources (Etienne, 2018). Table 16.2. Number of doctors, nurses, and dentists per
People living in rural or remote areas are also less likely to thousands of inhabitants in Latin American regions, Mexico, and
have access to sanitation, drinking water, and safe housing. Brazil. Note: Data for 2011, except where indicated with (*) 2014;
(**) 2016; (***) 2015. Sources: PAHO, 2014; World Bank, 2019;
Table 16.2 shows the number of doctors, nurses, and den-
Indexmundi, 2019; WHO, 2019a.
tists in Latin American regions and countries, in addition to
Brazil and Mexico, in 2011. The availability of medical per- Hospital
Medical staff/10,000 inhabitants
sonnel is variable. Mexico has a larger supply of doctors and Region/ beds/1,000
nurses than Brazil—especially nurses, whose role in public Country inhab. (2010–
Doctors Nurses Dentists 2013)
health is considered paramount in rural areas. At the regional
level, Central America and the Andean Area present similar Latin America 17.2 13.8 4.3 2
figures that stand out from those of the Southern Cone, with Mexico 21.2 25.1 1.0 1.5
a high number of doctors and dentists and a percentage of
nurses that surpasses that of Latin America. In terms of Central 12.6 9.7 3.5 0.9
America
hospital beds, the Southern Cone region is prominent, while
as a country, Brazil surpasses Mexico. Spain and Portugal Andean Area 13.4 8.8 4.8 1.4
have equal hospital bed coverage and a higher number of Brazil 15.1 7.1 5.5 2.3
doctors and nurses compared to Latin America.
Southern Cone 21.2 15.2 8.2 3.7
Table 16.3 outlines the percentage of services from improved Spain 40* 55.3** 4.5*** 3
water sources and sanitation facilities in Brazil, Mexico, and
Latin American regions in 2012. As regards hydrometeoro- Portugal* 40* 63.7** 5.6*** 3
620 RIOCCADAPT REPORTChapter 16 - Human Health
Table 16.3. Percentages of services from improved water sources and improved sanitation facilities in Latin American regions, Mexico, and
Brazil, 2012. Notes: (*) Population with access to basic drinking water supply systems, 2017; (**) National sanitation estimates, at least
basic, in 2015; (***) 2016. Source: PAHO, 2014; Statista, 2019; WHO and UNICEF, 2017; Portuguese Water Partnership, 2019.
Population using improved water sources Population using improved sanitation facilities
Region/Country
Region/ Country Urban areas Rural areas Region/ Country Urban areas Rural areas
Latin America 94 77 82 82 87 62
Mexico 95 96 91 85 87 79
Central America 92 98 84 76 83 67
Andean Area 89 94 73 75 82 57
Brazil 98 100 85 81 87 49
Southern Cone 98 99 90 96 98 82
Spain 100 100 100 100** 100** 100**
Portugal* 96*** ND ND 85*** ND ND
developed countries. In addition, the adverse effects of cli- into political will, resources, and programs to improve health
mate change are extremely broad, as they impact all human care and protection and aid climate-resilient development
organs and affect health institutions in terms of disease remains a challenge. For example, due to the close rela-
care and prevention, in addition to damaging public health tionship between air pollution and climate change, failure to
infrastructure. jointly address air pollution and climate change mitigation is
a missed opportunity to achieve multiple health, economic,
While all people are exposed to climate impacts, exposure and environmental benefits.
differs from place to place. Climate change happening place
more quickly in certain places than in others, and the risks Current governance mechanisms, including at the local level,
are not the same everywhere. The local context should there- have failed to effectively address the cross-cutting nature of
fore be considered in order to understand the challenges environmental problems that impact health, including climate
faced, the opportunities available, the inherent capacities of change. To the extent that policies continue to be imple-
these locations, and the actions to be taken to ensure the mented without identifying their possible impacts on health
resilience of the population and prevent adverse effects as and healthcare systems, their overall benefit will be limited
climate continues to change. (WHO, 2018a).
For more than two decades, scientists have been investi-
gating the implications of observed and projected climate
change, along with the magnitude and pattern of adverse
16.1.4. Review of past reports
health outcomes resulting from these changes. However, in The Fifth Assessment Report of the IPCC (Smith et al., 2014)
part due to financial constraints, in low-income countries the notes that, until the mid-century, climate change will continue
evidence base remains fragmented and particularly limited. to increase and even aggravate existing health problems.
The main health hazards from climate change include expo- Based on such assumptions, health issues arising from cli-
sure to extreme weather events that cause injury, mental mate change will imply higher risks of injury, disease, and
health problems, and death; heat waves, with their asso- death due to heat waves and wildfires; increased likelihood
ciated health problems and loss of life; poor water quality of malnutrition resulting from diminished food production in
and distribution, which is associated with gastrointestinal low-income regions and among people with fewer economic
diseases, algae growth, and leptospirosis; food insecurity resources; loss of working capacity and reduced labor pro-
leading to malnutrition, intoxication, and exposure to myco- ductivity in vulnerable populations; and increased risks from
toxins; alterations in vector ecology and distribution, with vector-borne diseases (VBDs) and food- and water-borne dis-
examples of vector-borne diseases (VBDs) such as dengue, eases. The expected beneficial impacts would be a moderate
chikungunya, zika, malaria, hantavirus, and encephalitis, decrease in morbidity, mortality, and, in some cases, VBDs
among others; and social factors that promote impacts on associated with low-temperature conditions, although at the
physical and mental health due to violent conflicts and forced global scale these impacts will be surpassed by the severity
migration (Haines and Ebi, 2019). and magnitude of the adverse effects (Smith et al., 2014).
This report emphasizes the need to strengthen public health
While promising progress has been made in integrating cli- programs, particularly the supply of potable water and san-
mate change and health, translating clear scientific evidence itation services, primary health care, child health services,
RIOCCADAPT REPORT 621Chapter 16 - Human Health
vector control and, most importantly, early warning systems This diversity of present and future climate effects exposes
(EWS) and disaster response systems, as well as the fight more people in more places to health hazards. A hazard is
against poverty (Smith et al., 2014). the possible occurrence of a physical event, a trend, or a
physical impact that may result in loss of life, injury, or
The special repor t on 1.5°C published by the IPCC
other health-related outcomes. The significance of a hazard
(Hoegh-Guldberg et al., 2018) has revealed, among other
will depend on its location, and identifying hazards requires
findings, that the impact of the scenarios studied will be
an awareness of all changes in the physical environment
lower if temperature is stabilized at 1.5°C, compared to
(UNEP, 2019).
the 2°C threshold. However, this does not guarantee an
absence of adverse effects, and the report reiterates that Populations can be exposed to a number of hazards, includ-
in order to achieve this goal it is essential that the actions ing changes in air or sea temperature and precipitation,
to stop warming increase and become more ambitious. The droughts, wildfires, storms, hurricanes, and sea level rise
document holds that, in the field of health, the main areas (UNEP, 2019). Some of these health hazards may be present
of risk are VBDs, food- and water-borne infections, extreme for longer periods or at unprecedented times of the year,
events, food insecurity, and air pollution. Health impacts and some people will be exposed to hazards that are new in
are expected to intensify, with socioeconomic factors influ- the place they live (Balbus et al., 2016), which can lead to
encing the magnitude and pattern of risks. In terms of food severe consequences when authorities and citizens alike are
security and health systems, adaptation may be more of a uncertain of how to act.
challenge at a temperature increase of 2°C than of 1.5°C.
Extreme weather events have tripled since the 1960s. They
The role of these systems remains essential to meet the
are estimated to cause more than 60,000 deaths per year,
challenges of rising temperatures. Empowering the health
par ticularly in developing countries. These increasingly
sector through intersectoral work is essential to coping with
intense events, coupled with sea level rise, can destroy
the impacts of climate change, as is supporting research
homes, medical services, urban services, and agricultural
into adaptation and mitigation with health co-benefits and
and livestock areas. Many people may be forced to migrate.
ensuring the availability of economic, technological, and hu- In addition, the increase in floods may create areas for vec-
man resources. A fundamental aspect is investing in various tor growth. Moreover, changes in temperature may prolong
areas in addition to health, such as education, public social transmission times and change their geographical distribu-
security systems, policies to fight poverty, and insurance tion (WHO, 2019a).
to manage risk, since significant synergies can be achieved
by these means (Ebi et al., 2018; Hoegh-Guldberg et al., Extreme events are responsible for deaths caused by car-
2018). diovascular and respiratory diseases, mental disorders,
communicable diseases, dermatological diseases, drown-
ing, physical injuries, and malnutrition. Floods and extreme
16.2. Risk components in relation precipitation also lead to serious health consequences. An
estimated 15% of all disaster-related deaths from extreme
to health events are due to floods (Raes, 2013). South America ac-
counted for 22% of the global occurrence of disasters be-
tween 2000 and 2015; of these, floods accounted for 50%
16.2.1. Hazards of the events, followed by storms (9%), landslides (8%), and
extreme temperatures (8%) (McBreen, 2016). Globally, 77%
Rising concentrations of greenhouse gases (GHGs) result of countries experienced an increase in the population’s daily
in changes in climate that manifest through increased tem- exposure to wildfires between 2001 and 2014 and 2015–
perature, changes in precipitation, increased frequency and 2018 (Watts et al., 2019). Nagy et al. (2018) have reported
intensity of some extreme weather events, and sea level that Bolivia, Brazil, Costa Rica, Honduras, Nicaragua, and
rise. These climate change impacts endanger health by af- Peru were the countries with the highest percentage of pop-
fecting food and water sources, the air we breathe, and the ulation affected by disasters and, to a lower extent, Mexico,
weather we endure, as well as our interactions with natural Paraguay, Uruguay, and Venezuela.
environments.
According to Nagy et al. (2018), in Latin America the impacts
The social determinants of health are the socioeconomic cir- of extreme meteorological events are mainly related to so-
cumstances in which people are born, grow up, live, work and cioeconomic and human development, geographical deter-
age, including the health system. Conversely, environmen- minants of health vulnerability to climate, and variables that
tal determinants are specific environmental health problems describe health disparities. Countries that experience the
arising from, inter alia, energy use, water resources, the pres- fewest direct impacts on human well-being are those with
ence or absence of basic sanitation, crops and agricultural the best human, socioeconomic, and vulnerability indices,
systems, labor conditions, the presence of hazardous waste, and the highest per capita expenditures on public health.
and air, water, and soil pollution (Galvão et al., 2010), as well Specifically, the countries with the highest public expendi-
as any environmental conditions that impact on health, such tures are Chile, Uruguay, Costa Rica, Panama, Argentina,
as climate change. Paraguay, Brazil, and Mexico.
622 RIOCCADAPT REPORTChapter 16 - Human Health
Some examples of the impact of extreme events during just placement events were organized by the authorities as part
one week in October 2019 include: 101,600 people affected of the risk management system (GRID, 2019). Digestive and
by floods and landslides in Guatemala, 400 houses at risk water-borne diseases are associated with heavy precipitation
of collapsing after heavy rains and floods in El Salvador, 530 and floods.
families affected by rain and floods in 14 municipalities in
There are other relevant variables that, when associated with
Nicaragua, and 9,000 families affected by wildfires in Bolivia
hazards, can strongly influence the impacts on a population.
(OCHA, 2019).
These variables include changes in poverty or socioeconomic
One-sixth of worldwide diseases and disabilities are due to status, and demographics such as age structure and ethnic
VBDs, with more than half of the world’s population at risk. composition (Oppenheimer et al., 2014).
More than one billion people are infected and more than one
If emissions are substantially reduced, projections indicate
million people die from malaria, dengue fever, schistosomia-
that by 2100 the world’s population could be simultaneously
sis, leishmaniasis, and Chagas disease every year. The per
exposed to the greatest magnitude of any of these hazards—
capita mortality rate is almost 300 times higher in develop-
or to all three, if emissions are not reduced, with some trop-
ing countries than in developed regions (Campbell-Lendrum
ical coastal areas being exposed to up to six simultaneous
et al., 2015).
hazards (Mora et al., 2018).
Regardless of how climate-displaced migrants are counted,
many factors contribute to health risks associated with mi-
gration. Wesselbaum and Aburn’s (2017) findings regarding 16.2.2. Exposure
migration indicate that climate change generates consider-
able adverse effects in migrants’ countries of origin, while it Both the frequency and the intensity of hazards may change
has been observed that the effect of temperature is stronger continuously. Health effects occur when individuals or pop-
than the combined effect of income and political freedom ulations who may be particularly vulnerable are exposed to
there. Moreover, the number of climate-related disasters in climate-related hazards. More intense storms are likely to
migrants’ home countries increases migration (Wesselbaum affect more people; likewise, an increase in their frequency
and Aburn, 2017). The resulting health impacts depend on may increase peoples’ exposure to their effects, while recur-
both pre-existing conditions (e.g. mental health and nutrition- ring events may have cumulative effects.
al status, desire to migrate, and existing health systems) and Exposure to hazards resulting from changes in climate can
interventions (e.g. access to health care, provision of food be acute, e.g. when populations experience a heat wave, or
and shelter, and changes in healthcare resources) (Watts et their effects can be observed in the medium term, such as
al., 2019). in drought conditions, where the impacts experienced will
Air quality can be affected by meteorological variables such depend on the duration and intensity of the hazard.
as wind and temperature. The World Health Organization The pathways of exposure to hazards will differ over time
(WHO, 2018b) has estimated that some seven million people and for different areas. Similarly, climate change-related
die annually from air pollution-related diseases, identified as exposure may affect different people and communities to
the main environmental health risk in the Americas (PAHO, various degrees. Exposure to multiple climate change-related
2018c). An estimated 93,000 deaths per year in low- and hazards may occur simultaneously, resulting in combined
middle-income countries and 44,000 in high-income coun- or cascading effects, which can also accumulate over time,
tries are attributable to pollution in the region (PAHO, 2018c). leading to long-term changes in resilience and health (Balbus
In Spain, pollution accounts for more than 10,000 deaths per et al., 2016)
year (Díaz, 2018), and in Portugal the number of deaths in
2015 was estimated at 15,000 (Marques, 2019). The heat island effect in cities is known to increase heat
stress from heat waves in their inhabitants (Zhao et al.,
Precipitation variability affects the availability of water, and 2018). These events cause excess mortality, increased in-
extreme events can also impact water quality, undermining cidence of heat exhaustion and heat stroke, exacerbation of
hygiene and increasing the likelihood of diarrheal infections circulatory, cardiovascular, respiratory, and renal diseases
that can lead to death, particularly in vulnerable populations in elderly populations, children (PAHO, 2017b), and persons
such as children under five years of age living in poverty and with pre-existing diseases (Linares et al., 2016) who live or
marginalization. In Guatemala, for example, cholera cases work in environments with no air conditioning. Due to hor-
increased almost tenfold after Hurricane Mitch in 1998. In monal changes, older women experience a direct impact
addition, of all deaths of children under five in 2015, diar- on their thermoregulatory capacity, leaving them especially
rhea accounted for 8% in Nicaragua, 7% in Guatemala, and vulnerable to the effects of high temperatures. This hazard
6% in Bolivia (PAHO, 2017b). Severe droughts can lead to is exacerbated in women who live alone (Díaz et al., 2018).
famine and migration. In 2018, some 67,000 new cases of
internal displacement associated with upstream flooding and Since 1990, hazards from extreme heat have increased
torrential rains were recorded in Colombia. In Mexico, 13,000 steadily in all regions, with 157 million more people exposed
new instances of internal displacement were reported as a to heat wave events in 2017 than in 2000 and 18 million
result of Hurricane Willa, which struck six states. These dis- additional exposure events compared to 2016. An estimated
RIOCCADAPT REPORT 623Chapter 16 - Human Health
153 billion working hours were lost due to exposure to high 16.2.3. Vulnerability
temperatures in 2017. In 2018, populations experienced 220
million heat wave exposure events worldwide, breaking the The extent and severity of climate change impacts on health
previous record of 209 million set in 2015. This increase depend on the interaction between exposure to alterations
in heat wave exposure poses a direct risk to the health of in the affected meteorological variables and the vulnerability
affected populations; moreover, there are additional indirect of the human and natural systems exposed to them, coun-
effects (e.g. food insecurity as a result of livestock exposure terbalanced by the responsiveness or adaptive capacity of
to heat waves). Due to rising temperatures and heat waves, these systems, which includes financial and technological
133.6 billion potential working hours were lost globally in resources and organizational and planning capacity (Ebi et
2018, 45 billion more than the 2000 baseline (Watts et al., 2011; Gutiérrez and Espinosa, 2010). For example, early
al., 2018). warning systems focused on vulnerable populations, such
Between 2010 and 2016, air pollutant concentrations wors- as the elderly, to alert them of heat waves, as well as pre-
ened in nearly 70% of cities worldwide, especially in low- and ventive health services prepared to assist them in case of
middle-income countries. Exposure to air pollution is estimat- emergency, are adaptation meaures that could reduce the
ed to have contributed to 130,000 deaths in the Americas in risk of aggravating health conditions or death.
2015 (Watts et al., 2018). As regards vulnerability in a given area, a series of relevant
According to the WHO (WHO, 2017), VBDs account for more factors may be its unique climate, including the intensity
than 17% of all infectious diseases and cause more than and frequency of weather phenomena, and its geograph-
700,000 deaths per year. More than 3.9 billion people in ical location, such as the coast, mountains, islands, etc.
over 128 countries are at risk of dengue fever, with an esti- Population-specific factors that affect vulnerability include
mated 96 million cases per year. Malaria causes more than demographic structure, the prevalence of pre-existing health
400,000 deaths each year worldwide, most of them among disorders, genetic factors, and acquired factors such as im-
children under five. An estimated 500,000 people are ex- munization. Another element is the coverage and effective-
posed to the severe dengue vector and require hospitalization ness of the public health system, as evidenced by the qual-
each year; a large percentage of whom are children (Camp- ity of monitoring and control programs and primary health
bell-Lendrum et al., 2015). care (Balbus and Malina, 2019). Relevant demographic and
socioeconomic factors are population density, resource dis-
Latin America, Spain, and Portugal are exposed to various tribution, and social capital, which play a decisive role in
hazards, incuding hydrometeorological events, VBDs, air vulnerability; these factors often interact with those of a
pollution, heat waves, and poor water availability and qual- biological nature.
ity. Each event has its own particularities, such as area of
impact, duration and timing of the event, intensity, and ex-
posure pathway.
Box 16.1. Poverty and climate change
Climate change will have devastating consequences for people liv- vulnerable to diseases, loss of crops, food price increases, and
ing in poverty, as the greatest burden will fall on them. Even in the death or disability caused by extreme events.
best-case scenario, hundreds of millions will face food insecurity,
Climate change threatens to undo the progress of the past 50 years
forced migration, disease, and death.
in terms of development and counteract efforts to reduce global
Health crises and ill health contribute to poverty through loss of health and poverty. It could even affect middle-class families and
income, health expenditures, and caregiving, so the impacts of cli- contribute to their impoverishment (Hallegatte et al., 2016).
mate change on health will act as an additional obstacle to poverty
reduction and increase inequality. Climate change will exacerbate existing poverty and inequality. Its
most severe impacts will be felt in low-income countries and regions
People living in poverty are likely to reside in areas more suscep- and in locations where people with incomes below the poverty line
tible to climate change and in less resilient housing. Their pos- live and work (UN Human Rights Council, 2019).
sessions may be affected by extreme events; they have fewer
resources, less government support, and weaker financial systems The World Bank estimates that without immediate action, climate
to cope with their losses, all of which may leave them too fragile to change could drive an additional 120 million people into poverty
recover from the impact. In addition, their livelihoods and assets by 2030, a figure that is likely underestimated and could increase
are more exposed (Hallegatte et al., 2016) and they are more in subsequent years (Hallegatte et al., 2016).
624 RIOCCADAPT REPORTChapter 16 - Human Health
Table 16.4. Variables that affect vulnerability, their specific associated conditions, and examples. Source: Ebi et al., 2011.
Variables that affect vulnerability Specific conditions Examples
Reference climate Projected magnitude and frequency of Being located in urban areas or flood zones
meteorological phenomena; geographical subject to various health and safety risk factors
circumstances
Effectiveness and coverage of the public Quality of monitoring and control programs Mortality and morbidity
health system and related institutions
Characteristics of the population Demographic structure; prevalence of pre-existing Vulnerable groups, such as women, children, the
medical conditions such as immunity and genetic elderly
factors
Demographic and socioeconomic factors Population density; social capital; resource Differences in ability to adapt or respond to
distribution exposure
Groups that are vulnerable to the impacts of climate change capacity to climate change. Rapid population growth increas-
consist of persons living in conditions of social inequality, es vulnerability and exposes more people to various risk fac-
children, older adults, women, people with disabilities, and tors, which will affect the population’s morbidity and mortality
people with pre-existing or chronic diseases who work out- rates (Soares da Silva et al., 2016).
doors (e.g. police officers, street vendors, construction work-
Many cities in developing countries lack adequate infrastruc-
ers) due to their exposure to heat waves (Beggs, 2010).
ture and urban planning, increasing their degree of exposure
In terms of age, infants are often the most affected by the and vulnerability to extreme events. For example, houses
potentially permanent effects of malnutrition due to hazards located on hills, in dry riverbeds, or near streams are vulner-
affecting food production and food security. Children are able to landslides.
among the most susceptible to diarrheal disease and expe-
In Latin America, the indigenous population—estimated at
rience the most severe effects of dengue fever. During ado-
42 million—is a highly vulnerable group (World Bank, 2017).
lescence and beyond, air pollution, driven mainly by fossil fu-
Much of their vulnerability is due to their dependence on
els and exacerbated by climate change, damages the heart,
land and natural resources, which are affected in various
lungs, and all other vital organs. Throughout life, families and
ways by climate change. Due to poverty and marginaliza-
livelihoods bear the risks of the increasing frequency and
tion, indigenous peoples often have very limited access to
severity of extreme weather conditions, with women being
mainstream health and prevention services and health pro-
among the most vulnerable in a variety of social and cultural
motion programs. For example, the Rarámuris, an indigenous
contexts. Another group identified as vulnerable comprises
people living in the northern Mexican highlands (sierras), ex-
workers, as rising temperatures and heat waves increasingly
perienced a drought that severely impacted the maize and
limit various populations’ ability to work. Other conditions
bean harvests, which are highly valuable crops in their food
that are difficult to quantify include migration, exacerbation
system (PAHO, 2017a).
of poverty, violent conflict, and mental illness, which can
affect people of all ages and regions regardless of where Gender is another condition for vulnerability. Women may
they live (Watts et al., 2019). be more vulnerable to psychosocial health impacts during
extreme events, as they are more likely to bear the burden of
Moreover, people’s vulnerability can be affected by the deg-
recovering from the event and continuing their lives to satisfy
radation of air quality, industrial pollutants, poor housing,
multiple demands both within and outside the home (Oswald
lack of air conditioning, and changes in the built environment
et al., 2014) and to lack access to health services during the
(PAHO, 2017b), while the occurrence of extreme events can
event (Kovats et al., 2003; Cannon, 2008).
exacerbate the vulnerability of a population (Sorensen et al.,
2017). Table 16.4 presents variables that affect vulnerabil- Indicators of climate change and its effects on human health;
ity, the specific conditions they are associated with, and a the adaptation measures planned to benefit the vulnerable;
few examples. With this information, it is possible to identify the monitoring and evaluation of the actions proposed, im-
elements that should be considered when designing adapta- plemented, and executed; and the resources invested can be
tion measures to protect people’s health. used to identify, analyze, and address vulnerability (Kovats
et al., 2003). This will enable adaptation measures to reduce
In recent decades, Latin America has experienced a signifi-
vulnerability in the medium and long terms, in addition to
cant growth in population and urbanization, and these trends
reducing the burden of disease.
are likely to continue. In Spain and Portugal, growth has been
quite low and, in some cases, slightly negative (National In- Ebi et al. (2011) have argued for the need to assess current
stitute of Statistics, 2017; IndexMundi, 2017). These trends and future vulnerability to health risks from climate change,
carry significant implications for vulnerability and adaptive as well as to evaluate policies that could focus on improving
RIOCCADAPT REPORT 625Chapter 16 - Human Health
resilience to health risks. This assessment could focus on of increasing temperature and changing climate threaten to
a region or locality, and its findings would provide valuable undermine recent global progress against some VBDs.
information to policymakers on the type and magnitude of
Vector-borne diseases are a major cause of death; they signifi-
the health risks associated with climate change, both now
cantly contribute to the global burden of disease and health
and in the future, and on the policies to avoid its existing
inequality, cause epidemics that disrupt health security, and
effects and prevent and reduce future ones. Likewise, it
place a strain on development and health services. About one-
would provide elements to define progress towards building
sixth of the illnesses and disabilities experienced worldwide are
climate-resilient communities and protecting the health of
caused by these diseases (Campbell-Lendrum et al., 2015).
the population.
The greatest risk of disease is usually faced by people with
fewer economic resources, due to their more limited environ-
16.3. Characterization of risks mental and social conditions (e.g. lower-quality housing near
vector breeding sites) and lack of access to preventive and
and their impacts remedial medical interventions and services (Ottesen et al.,
1997). Urbanization is another cause for concern, since in
developing countries it is uncontrolled and water and sewer-
Latin America and the Iberian Peninsula are vulnerable to
age services are not provided, thus creating conditions for
some of the most harmful aspects of climate change. Various
the proliferation of vectors (Hay et al., 2006).
hazards are responsible for changes in ecosystems, which in
turn give rise to various health risks. Figure 16.2 describes The WMO (2018) has noted that the emergence of the zika
the eight main risks to health, their climate determinant, virus epidemic, mainly transmitted in Latin America by the
magnitude, urgency, and affected regions. Central America Aedes aegypti mosquito and caused by drought and unusu-
stands out as the most vulnerable region. ally high temperatures, has developed at least since 2013
due to environmental changes caused by lack of humidity
and temperature increases. Changes in temperature, rain-
16.3.1. Vector-borne diseases fall, and humidity can have strong effects on leishmaniasis,
which in addition to drought, floods, and famine can lead
Diverse disease vectors exist, including mosquitoes, phlebot- to human migration to transmission areas. In the case of
omines, triatomine bugs, simulids, ticks, mites, snails, and dengue fever, geographical distribution can be significantly
lice. Mosquitoes are especially sensitive to changes in tem- affected by changes in temperature, rainfall, and humidity
perature and humidity (Smith et al., 2014). Current trends (Prüss-Ustün et al., 2016).
Box 16.2. Human rights and climate change
Climate change threatens the enjoyment of all internationally guar- 1. To mitigate climate change and to prevent its negative human
anteed human rights, including the rights to health, water, food, rights impacts
housing, self-determination, and life itself. Many people will be
living in poverty, but they will be far from the only victims (UN 2. To ensure that all persons have the necessary capacity to
Human Rights, 2019a). adapt to climate change
Any climate-related hazard can challenge the full and effective 3. To ensure accountability and effective remedy for human rights
enjoyment of various human rights worldwide, including the right harms caused by climate change
to life, to water and sanitation, to food, to health, to housing, to
4. To mobilize maximum available resources for sustainable,
self-determination, to culture, and to development (UN Human
human rights-based development
Rights, 2019a).
5. International cooperation
The adverse impacts of climate change are disproportionately suf-
fered by individuals and communities who are already at a disad- 6. To ensure equity in climate action
vantage due to geography, poverty, gender, age, disability, and
cultural or ethnic background. 7. To guarantee that everyone enjoys the benefits of science and
its applications
In order to promote policy coherence and help ensure that climate
change mitigation and adaptation efforts are adequate, sufficiently 8. To protect human rights from business harms
ambitious, non-discriminatory, and compliant with human rights
9. To guarantee equality and non-discrimination
obligations, the following considerations should be a part of all
climate actions (UN Human Rights, 2019b): 10. To ensure meaningful and informed participation
626 RIOCCADAPT REPORTYou can also read