Transparency in Drug Regulation: Mirage or Oasis? - By Joel Lexchin MD - ISBN 0-88627-385-4
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Transparency in Drug Regulation:
Mirage or Oasis?
By Joel Lexchin MD
ISBN 0-88627-385-4 October 2004
Transparency in Drug Regulation: Mirage or Oasis? 1Transparency in Drug Regulation:
Mirage or Oasis
By Joel Lexchin MD
ISBN 0-88627-385-4
October 2004
$10.00
About the author
Joel Lexchin is an Associate Professor at the York Universit School of Health Policy and Manage-
ment and a Doctor at the Emergency Department of the University Health Network in Toronto.
Acknowledgements
Barbara Mintzes contributed to the analysis of the contents of the Summary Basis of Decision docu-
ments and put together the table.
Larry Sasich provided valuable information about how the FDA system works.
Canadian Centre for Policy Alternatives
410-75 Albert Street, Ottawa, ON K1P 5E7
tel: 613-563-1341 fax: 613-233-1458
email: ccpa@policyalternatives.ca
http://www.policyalternatives.ca
2 Canadian Centre for Policy AlternativesContents
Executive Summary ..................................................................................................................................... 5
I. Introduction ............................................................................................................................................... 7
II. Causes for Concern ................................................................................................................................ 9
III. Is There a Rationale For Secrecy? ..................................................................................................... 11
IV. Previous Proposals to Increase Transparency in the Drug Approval Process ........................ 12
V. A Failed Model From Europe ............................................................................................................. 14
VI. Current Proposals for Reform ........................................................................................................... 15
VII: Is the Summary Basis of Decision Adequate ............................................................................... 19
VIII. Going Beyond Disclosure of Safety and Efficacy Information for Approved Drugs........... 21
VIII. Summary of Recommendations .................................................................................................... 23
References ................................................................................................................................................... 24
Appendix 1: Conditions for Endorsement of Summary Basis of Decision ................................... 26
Appendix 2 : Statement of the International Working Group on Transparency and Accountabil-
ity in Drug Regulation.......................................................................................................................... 27
Appendix 3: Abbreviations....................................................................................................................... 32
Transparency in Drug Regulation: Mirage or Oasis? 34 Canadian Centre for Policy Alternatives
Executive Summary
DRUG REGULATION IN CANADA is carried out in a very secretive manner because of
the unique relationship between the Therapeutic Products Directorate, the arm of Health
Canada in charge of approving new drugs, and the brand-name pharmaceutical industry.
Because of a lack of resources the TPD it is forced to cede some of its authority to the
industry. In addition, both the TPD and the pharmaceutical companies regard information
about safety and efficacy as a commodity to be guarded rather than as a resource to be shared.
This interpretation is reinforced by the Access to Information Act. As a result it is extremely
difficult to get any information about safety and efficacy of new drugs from the TPD.
Recently, there has been increasing concern ments do not apply when it comes to health and
about the lack of transparency due to industry safety data. There is no good evidence to show that
funding of the operations of the TPD. Reliance the interests of companies would be harmed by
on the industry for operating revenue has lead to a the disclosure of this type of information; specifi-
tilt in the TPD in favour of industry. Evidence from cally, confidentiality is not necessary to foster re-
the United States shows that industry funding may search and innovation.
result in lower approval standards. Without access Since 1995 there have been a number of at-
to the data that TPD reviewers are analyzing, the tempts to increase transparency in the drug ap-
suspicion continues that industry funding has proval process, most notably a report from Health
weakened review standards. Canada’s Science Advisory Board but all of these
Another reason to be concerned about the lack efforts have come to naught. In addition, the Eu-
of transparency is that when new drugs appear on ropean Public Assessment Reports which summa-
the market the volume of published literature that rize information about new drugs and which
is available to guide prescribing and use of these Health Canada is looking to as a model for im-
drugs is often extremely limited. The unpublished proved transparency have been unsuccessful be-
material that companies submit to the TPD could cause of a lack of standardization of these reports
potentially overcome this problem but this data is and an unwillingness to disclose sufficient clinical
unavailable. information.
Although there are valid reasons to protect There are currently three proposals at various
manufacturing secrets and the identities of patients stages of discussion and implementation in Canada
who have taken part in clinical trials these argu- for increasing transparency. The one that is the
Transparency in Drug Regulation: Mirage or Oasis? 5most advanced is the publication of a Summary pany has submitted along with the FDA review-
Basis of Decision for that would outline the scien- er’s analysis of this information. There is no justi-
tific and benefit/risk-based reasons for the deci- fication for Canada not matching the U.S. stand-
sion to approve a new drug. In order to assess the ard.
adequacy of the information in these SABs four Besides better access to information about
case studies are presented where access to infor- drugs that have been approved other measures are
mation given to regulators has lead to the discov- needed to increase transparency in the approval
ery of significant problems with medications. In system. Canada should also emulate the FDA’s sys-
none of these four cases would the amount of in- tem of public expert advisory committee hearings
formation in the SABs have been enough to un- for new drugs, albeit with stronger conflict-of-in-
cover the problems. terest rules than the FDA has. Safety and efficacy
In the United States after a drug has been ap- data also needs to be available for new drugs and
proved the Food and Drug Administration rou- new indications for old drugs in cases where the
tinely posts an approval package that contains a approvals were refused or where the company with-
detailed summary of the information that the com- drew the application.
Box 1 – Access to Information Act
Third Party Information
20. (1) Subject to this section, the head of a government insti-
tution shall refuse to disclose any record requested under this
Act that contains (a) trade secrets of a third party; (b) financial,
commercial, scientific or technical information that is confiden-
tial information supplied to a government institution by a third
party and is treated consistently in a confidential manner by
the third party; (c) information the disclosure of which could
reasonably be expected to result in material financial loss or
gain to, or could reasonably be expected to prejudice the com-
petitive position of, a third party; or (d) information the disclo-
sure of which could reasonably be expected to interfere with
contractual or other negotiations of a third party.
20. (6) The head of a government institution may disclose any
record requested under this Act, or any part thereof, that con-
tains information described in paragraph (1) (b), (c) or
(d) if that disclosure would be in the public interest as it relates
to public health, public safety or protection of the environment
and, if the public interest in disclosure clearly outweighs in
importance any financial loss or gain to, prejudice to the com-
petitive position of or interference with contractual or other
negotiations of a third party.
6 Canadian Centre for Policy AlternativesI. Introduction
THE PHARMACEUTICAL INDUSTRY and the Canadian government have long had a
close relationship based on a form of interaction known as clientele pluralism. This situation
occurs where the state has a high degree of concentration of power in one agency (the Therapeu-
tic Products Directorate (TPD) a branch of Health Canada), but a low degree of autonomy.
With respect to pharmaceuticals, in Canada, gov- sector actors, who, in turn, pursue objectives with
ernment regulation of drug safety, quality and ef- which officials are in broad agreement.
ficacy is almost solely the responsibility of the TPD. One way this relationship is manifested is the
But the state does not possess the wherewithal to agreement between the industry and the TPD that
undertake the elaborate clinical and pre-clinical all of the information that companies submit as
trials required to meet the objective of providing part of the regulatory approval process is deemed
safe and effective medications. Nor is the state will- confidential and will not be released without the
ing or able to mobilize the resources that would be express consent of the company involved. Health
necessary to undertake these tasks. Therefore, a Canada’s own Science Advisory Board agrees that
tacit political decision is made to relinquish some “in general, the Health Protection Branch [now
authority to the drug manufacturers, especially the Health Products and Food Branch] has . . .
with respect to information that forms the basis taken a very cautious position on what it releases
on which regulatory decisions are made. as public information.” This willingness to keep
On-the-other-hand, the association represent- information secret is reinforced in the Access to
ing nearly all of the multinational companies op- Information Act that states that “scientific or tech-
erating in Canada, Canada’s Researched-Based nical information that is confidential information
Pharmaceutical Companies (Rx&D), is highly mo- supplied to a government institution by a third
bilized to assume a role in the making and imple- party and is treated consistently in a confidential
menting of drug policy. It operates an elaborate manner by the third party.” (See Box 1) The Act
committee structure, has the ability to act on be- does provide a way to allow the release of informa-
half of its members and the capacity to bind mem- tion “if that disclosure would be in the public in-
ber firms to agreements. (There is an association terest as it relates to public health, public safety ”
of generic pharmaceutical manufacturers, the Ca- but that provision has never been used in this con-
nadian Generic Pharmaceutical Association, but text. In the late 1990s, an Ottawa researcher chal-
its members are responsible for less than 15% of lenged Health Canada in the Federal Court of
drug sales in Canada.) In clientele pluralism, the Canada seeking the release of information about a
state relinquishes some of its authority to private- class of drugs known as calcium channel blockers
Transparency in Drug Regulation: Mirage or Oasis? 7but the exemption was upheld (Ken Rubin, per- Imodium: the title page, the table of contents, the
sonal communication). title of a table and two pages with column head-
As a result obtaining even the barest form of ings with all of the data removed.
clinical information from the TPD about drugs is This approach to releasing the clinical infor-
exceedingly difficult. In the mid 1990s, I became mation that companies submit reflects a common
interested in the question of why Canada had li- understanding between officials in Health Canada
censed products for the treatment of acute pediatric and the pharmaceutical industry of medical infor-
diarrhea when the World Health Organization had mation as a commodity with commercial value that
concluded that these medications should not be must be protected. Such information can be
used. Accordingly, in November 1996 I made a “loaned” to the government for purposes of review
request through the Access to Information Act for but the companies do so with the expectation that
“all studies that the Health Protection Branch has the review will produce material gains through
that deal with the question of the efficacy of: marketing of their products. This market based
Donnagel, Donnagel-MB, Donnagel—PB, view stands in marked contrast to a view that data
Imodium, Kaopectate or Lomotil in a pediatric on health and safety is something that should be
population with acute infectious diarrhea.” I did shared directly with the people most affected –
receive some information as a result of this appli- those who prescribe and use the products. What
cation but after a wait of 21 months the final pack- we have instead is information filtered through,
age contained 5 pages from the dossier on and protected by, the officials in Health Canada.
8 Canadian Centre for Policy AlternativesII. Causes for Concern
i. Industry funding of the TPD pressure prompted the task force to recommend
that Canada consider relying more on foreign drug
In recent years with the introduction of cost re- reviews in its approval process. The recommenda-
covery there has been a growing concern that the tion was subsequently approved by senior man-
already tight relationship between the government agement in the TPP.
and the industry has been further strengthened Perhaps the most revealing statement about
leading to a pro-industry bias in drug approvals. this reorientation of the relationship between the
When the federal government was in the full government and the industry came from Dann
throws of deficit fighting back in the early 1990s, Michols, the Director General of the TPP. In an
it significantly cut the budget for the TPD (and internal bulletin distributed to TPP staff in Feb-
many other government agencies) and as a result, ruary 1997 he discussed the question of who is
the TPD turned to cost recovery to obtain the the TPP’s client. In the context of cost recovery
funds necessary to keep running. As a result by Mr. Michols advised staff that “the client is the
1999, industry was contributing about half the $70 direct recipient of your services. In many cases this
million used by the TPD. In return for these pay- is the person or company who pays for the serv-
ments, the industry is asking for action on the speed ice.” The one page document focused on service
with which new drugs are approved and in the to industry relegating the public to the secondary
2003 federal budget $190 million was committed status of “stakeholder” or “beneficiary”.
to improvements in the TPD, primarily to decrease Evidence that cost sharing and shorter approval
approval times. Other evidence of the increasing times might compromise safety and efficacy stand-
tilt towards industry comes from the lenient atti- ards when it comes to approving new drugs comes
tude towards direct-to-consumer advertising that from south of the border. There user fees paid to
should be illegal under the Food and Drugs Act the Food and Drug Administration (FDA) by the
In the mid 1990s, a working group from the brand-name pharmaceutical industry were tied to
Therapeutic Products Programme (TPP, predeces- quicker approvals by the FDA, with times drop-
sor to the TPD) looked at ways of efficiently man- ping for new molecular entities from 27 months
aging its limited resources and came up with a se- in 1993, when user fees were instituted, to 19
ries of recommendations for moving submissions months in 2001. The Washington based Public
through the system more rapidly. However, the Citizen Health Research Group surveyed FDA re-
working group admitted that “the pharmaceutical viewers in 1998 for their reaction to the changes
industry is looking for dramatic improvement in in the agency. Nineteen out of 53 medical officers
service” and “the implementation of the proposed identified a total of 27 new drugs in the past three
changes may not result in the level of improved years that they thought should not have been ap-
performance desired by our industry clients.” This proved but were; 17 said that standards were
Transparency in Drug Regulation: Mirage or Oasis? 9“lower” or “much lower” than they had been three formed choices about whether or not to use these
years previously. A subsequent survey by the Of- medications. For some drugs there are only single
fice of Inspector General confirmed some of these published randomized controlled trials (RCTs, the
findings. Although 64% of FDA respondents had gold standard in evidence). In other cases, drugs
confidence in the FDA’s decisions regarding the that are intended for long-term use have only been
safety of a drug, at the same time 40% who had studied for six months or less. Often there are only
been at FDA at least 5 years indicated that the re- comparisons against placebos not against other
view process had worsened during their tenure in drugs used for the same condition. Even in RCTs,
terms of allowing for in-depth, science-based re- safety data is frequently inadequately reported.
views. Ioannidis and Lau have examined the complete-
Without access to the data that TPD review- ness of safety reporting in RCTs in seven medical
ers are analyzing the suspicion continues that in- areas. Severity of clinical adverse effects and labo-
dustry funding has weakened review standards. ratory-determined toxicity was adequately defined
in only 39% and 29% of trial reports, respectively.
ii. Inadequate knowledge of drugs at Only 46% reported on the reasons for
discontinuations due to toxicity.
time of marketing Trial data that rests with the TPD may help
correct some of these deficiencies but at this time,
When new drugs come onto the Canadian market this information remains locked up in the TPD
the amount of published material is often grossly archives and will only be released with the agree-
inadequate to allow physicians to make rational ment of the company that submitted it.
prescribing decisions and consumers to make in-
10 Canadian Centre for Policy AlternativesIII. Is There a Rationale For Secrecy?
THERE ARE CLEARLY GOOD REASONS why agencies is never disclosed then this data will never
manufacturing information should be protected enter the normal peer review channels and is there-
by the TPD. This is proprietary knowledge and if fore not subject to scrutiny by independent scien-
it became public it could adversely affect the fi- tists. Without this type of feedback TPD review-
nancial status of a company by providing com- ers may be more prone to misjudge the accuracy
petitors with an unfair advantage. Personal data or usefulness of the data submitted; the scientific
that enters the files of regulatory agencies like the atmosphere in the agency may be stifled and the
TPD can include the identity of individual patients professional growth of its staff severely inhibited.
or health professionals as well as information on Deprived of any independent access to informa-
the illness from which the patient is suffering. In- tion, health professionals have to accept the TPD’s
formation that might lead to the identification of judgment about the safety and effectiveness of
individual patients or health professionals should products. In the case of well-established drugs this
also not be disclosed to any party (International is probably not much of a concern, but it may be
Working Group on Transparency and Accountabil- different with new drugs where experience is lim-
ity in Drug Regulation 1996). ited.
These arguments do not apply when it comes Finally, the public may be denied knowledge
to health and safety data. There is no good evi- of the full health effects of products so that they
dence to show that the interests of companies can decide for themselves whether or not to use
would be harmed by the disclosure of this type of them. Even if most consumers would never take
information; specifically, confidentiality is not nec- the time to read health and safety data, consumer
essary to foster research and innovation. On-the- oriented media in consultation with scientific ex-
other-hand, nondisclosure has serious disadvan- perts could use some of this information to in-
tages for the TPD, health professionals and the form the public of the risks and benefits of prod-
public. If information submitted to regulatory ucts.
Transparency in Drug Regulation: Mirage or Oasis? 11IV. Previous Proposals to Increase
Transparency in the Drug Approval Process
SINCE 1995, there have been a number of abor- Box 2 – Previous Transparency
tive efforts to increase transparency in the drug
approval. (See Box 2) Especially noteworthy was
Initiatives
the report of Health Canada’s own Science Advi-
December 1995
sory Board (SAB). The SAB was set up in 1997 by
• Dann Michols (Director General, Drugs Directorate):
Allan Rock, then Minister of Health, to advise the “A Canadian Summary Basis of Approval is also being
Minister on all matters of science as they affected considered as we streamline and standardize the re-
medications, food and medical devices. The SAB view practices. . . In addition, a project on the role of
formed an ad hoc Committee on the Drug Re- the Drugs Directorate in information dissemination
view Process because of a perceived lack of confi- to consumers and health practitioners is underway.”
dence in the regulatory process. Although the SAB • Nothing further heard for 2 years about either initia-
admitted that the review was not comprehensive, tive.
the Committee circulated questionnaires to
stakeholders and TPD employees, met with sen- April 1998
• Stakeholder Letter from TPD requesting input into
ior officials in the TPD as well as officials in the
proposal to make public names of drugs in approval
FDA, the Medicines Control Agency in the United
process.
Kingdom and the European Agency for the Evalu- • Nothing further heard about this proposal.
ation of Medicines.
The Committee’s 2000 report firmly stated June 1998
that “in our view and that of many stakeholders, • Dann Michols once again referred to development of
the current drug review process is unnecessarily Canadian Summary Basis of Approval: “additional time
opaque. Health Canada persists in maintaining a [to prepare such a document] is difficult to justify as
level of confidentiality that is inconsistent with the Programme strives to meet existing performance
public expectation and contributes to a public cyni- targets for all submission types.” He then went on to
cism about the integrity of the process.” In order talk about a strategy for information dissemination that
was initiated in 1997.
to remedy this situation the Committee recom-
• Nothing further heard about either Summary Basis of
mended “that HPB [Health Protection Branch,
Approval or strategy for information dissemination.
now Health Products and Food Branch] should
set new standards of access to information at all February 2000
stages of the drug review process, enhancing trans- • Health Canada, Science Advisory Board, “Report of
parency and public confidence. We perceived no the Committee on the Drug Review Process” Recom-
justification for current levels of delicacy regard- mendation 8.5: Enhance transparency in the drug re-
ing ‘commercial confidentiality’. We would note: view process.
(a) Canada can at least emulate the standards of • Nothing further done.
12 Canadian Centre for Policy Alternativesopenness of our nearest and largest trading part- this information should become part of the TPP’s
ner: [the FDA’s procedures will be discussed be- NDA [New Drug Application] review process, and
low] (b) New legislation should provide for public the applicant should be responsible for providing
hearings where appropriate; (c) If a product has copies of transcripts and videotapes”. Like previ-
gone through the FDA’s public hearing process, ous efforts this one too amounted to naught.
Transparency in Drug Regulation: Mirage or Oasis? 13V. A Failed Model From Europe A RECENT HEALTH CANADA DOCUMENT action of the drug was not fully presented. The on increasing transparency [see Section VI(iii) be- reporting of clinical trials was not always clear and low] favourably refers to the European Public As- none of the 9 EPARs mentioned references to pub- sessment Report (EPAR) which is a document pro- lished trials. Expert opinions along with the doubts duced by European Medicines Evaluation Agency and final positions of the experts were of variable (EMEA) after a drug has been approved. EPARs quality. The ISDB subsequently extended its analy- are supposed to reflect the assessment file submit- sis to cover all EPARs published in 1999 and 2000. ted by the manufacturer, its analysis by the EMEA’s The results were still very negative: the EPARs were scientific advisory body and the reasons underly- not harmonized, reliable or correctly updated. ing that body’s opinion. The International Society La revue Prescrire, a French drug bulletin con- of Drug Bulletins (ISDB) an international organi- siders that the EPARs have continued to deterio- zation of independent drug bulletins with 52 mem- rate in quality. They have “no documentary re- bers undertook an analysis of 9 EPARs issued be- sources independent of drug companies. In many tween September 1996 and August 1997. The most cases, analysis of EPARs suggests that these docu- striking finding was a lack of standard presenta- ments are totally or mainly written by the firms tion of information, for instance, the Scientific themselves, or edited by copying and pasting from Discussion section did not consistently include an the firms’s application. . . Irregular publication of introduction, it did not always have epidemiologi- their updates on the EMEA website means that cal data and in some EPARs the mechanism of their value is highly uneven”. 14 Canadian Centre for Policy Alternatives
VI. Current Proposals for Reform
i. Health Protection Legislative ii. Standing Committee on Health
Renewal
In June 2003, the House of Commons Standing
Committee on Health initiated hearings into a
Proposals to reform the system have recently ap-
wide range of issues affecting prescription drugs
peared from a number of quarters. As part of its
and over two months in the fall of that year had a
efforts to reorganize Canada’s health protection
series of open meetings across the country where
legislation, Health Canada put out a discussion
it heard briefs from a variety of individuals and
document in the summer of 2003. A number of
organizations. When it issued its report the fol-
measures are suggested to provide for more open-
lowing spring it called for increased transparency
ness but at the same time Health Canada seems to
and more accountability by Health Canada. To this
have accepted certain limitations in how far it is
end, it supported the development of mechanisms
willing to go and to have foreclosed other options.
to enable public disclosure of information about
For instance, the document points out that sec-
clinical trials without jeopardizing either the in-
tions of the North American Free Trade Agreement
tellectual property rights of drug companies or the
and the Trade-Related Aspects of Intellectual Prop-
privacy of individuals involved in the clinical
erty Rights Agreement “provide that the govern-
trialsand it recommended a “public database that
ment must protect the confidentiality of undis-
provides information on trials in progress, trials
closed test or other data provided by the applicant
abandoned and trials completed”.
to determine whether the use of such products is
safe and effective, where the origination of such
data involves considerable effort” although “this iii. TPD and the Summary Basis of
does not apply however in cases where the disclo- Decision
sure is necessary to protect the public or where
steps are taken to ensure that the data is protected In late winter 2004 Health Canada announced that
against unfair commercial use.” Health Canada it would publish a document entitled “Summary
proposed that only a summary of the safety and Basis of Decision” related to drug submissions and
effectiveness data submitted by the manufacturer medical device applications. The SBD would out-
would be made generally public. If consumers or line the scientific and benefit/risk-based reasons
health professionals want to see the full set of data for Health Canada’s decision to grant market au-
the proposal calls for a “reading room where peo- thorization for a product. The announcement was
ple could review all the data submitted by the followed up with a more detailed document whose
manufacturer but not transcribe or copy it, or oth- opening statement laid out the case for greater
erwise make that data available to interested mem- transparency: “Transparency is a fundamental good
bers of the public”. regulatory practice and a clear expectation of the
Transparency in Drug Regulation: Mirage or Oasis? 15Canadian public”. The “Scientific Discussion” sec- tocol the overall findings of the trial had to be sta-
tion of the EPAR was explicitly cited as the model tistically significant before exploratory analyses on
for the proposed SBD. subgroups would be conducted. This part of the
Out of the three proposals that have been put protocol was not followed and the authors made
forward, the use of SBDs is the most advanced conclusions about subgroups despite the lack of
and therefore merits a detailed analysis. The key significance in the primary study outcome. Finally,
part of the SBD document from the point of view and most importantly, at the 12-16 month time
of prescribers and consumers is the clinical infor- there was no difference in gastrointestinal adverse
mation that it contains. Is there enough informa- effects between the celecoxib and traditional
tion to allow for safe and rational use of new medi- NSAID groups.
cations. The best way to analyze the quality and Thus the published article presented a mislead-
quantity of information in the SBDs is to take ex- ing impression both of trial design and conclu-
amples of where access to unpublished data sub- sions. The trial was not 6 months in length; it was
mitted to drug regulators has uncovered impor- 12 to 16 months in length. It did not find evi-
tant clinical information about either the safety or dence of superior safety for celecoxib; the two com-
effectiveness of drugs on the market and then see parators (ibuprofen and naproxen) were found to
whether the same discoveries would have been be just as safe, including gastrointestinal safety.
possible using the SBDs. Health Canada has pub- Given the lack of evidence of superior effective-
lished two pilot SBDs that can be used in this re- ness for celecoxib, this difference is far from aca-
gard, one for rosuvastatin (Crestor) , a cholesterol demic.
lowering medication, and agalsidase beta Information necessary to uncover the prob-
(Fabrazyme) , an enzyme replacement for use in lem: These discrepancies between the published
Fabry’s Disease. study and what was submitted to the FDA were
discovered because the following information was
a. Celecoxib available on the FDA web site: study protocol, FDA
Celecoxib is a COX-2 inhibitor marketed for reviewer’s comments, detailed information on trial
analgesia and inflammation. Its purported benefit outcomes.
over older anti-inflammatory agents (NSAIDs), Health Canada SBDs: The study protocol and
such as ibuprofen and naproxen, is that it causes the reviewer’s comments are not included. Results
fewer serious gastrointestinal side effects. A study of the individual studies (efficacy results and side
published in JAMA (Journal of the American effects) are not presented. Therefore, based on the
Medical Association) in 2000 appeared to confirm SBDs it would also be difficult to determine if
this assertion and showed significantly less published studies combined the results of more
gastrointestinal toxicity with celecoxib compared than one clinical trial or if interim trial results are
to traditional NSAIDs after six months of treat- falsely presented as full trial results.
ment. However, material on the web site of the Conclusion: Most of the problems with the
FDA revealed a number of discrepancies between published study on celecoxib would not have been
the data as published in JAMA and as submitted found through using the SBD.
to the FDA. The published trial actually combined
the results of two trials one that continued for 12 b. Antidepressants
months and the second that ran for 16 months.
According to the FDA’s statistical reviewer the most 1. Efficacy of Antidepressants Compared to
appropriate period of analysis should have been Placebo
the entire study period not the 6 months as re- Kirsch and colleagues analyzed efficacy data
ported. Furthermore, according to the study pro- submitted to the FDA for approval of the six most
16 Canadian Centre for Policy Alternativeswidely prescribed antidepressants approved be- eventually published. The authors found three
tween 1987 and 1999 (fluoxetin, paroxetine, types of biases:
sertraline, venlafaxine, nefazodone and Multiple publication: 21 studies contributed
citalopram). They showed that 80% of the response to at least two publications each, and three studies
to medication was duplicated in placebo control contributed to five publications.
groups and the mean difference between drug and Selective publication: studies showing signifi-
placebo on the Hamilton Depression ScaleI was cant effects of drug were published as stand alone
of questionable clinical significance. Placebo con- publications more often than studies with non-
trolled trials of antidepressants are based on the significant results.
assumption that drug and placebo effects are ad- Selective reporting: many publications ignored
ditive, that is, the drug is deemed effective only if the results of intention to treat analyses and re-
the response to it is significantly greater than the ported the more favourable per protocol analyses
response to placebo, and the magnitude of the drug only.
effect is assumed to be the difference between the All of these biases resulted in a more favour-
response to drug and the placebo. The conclusion able opinion of the drug and could have signifi-
of this study was that if the effects are additive then cantly affected the results of systematic reviews and
the pharmacological effects of these antidepressants meta-analyses.
is negligible. If the effects are not additive, alter- Information necessary to uncover the prob-
native experimental designs are needed for the lem: These biases were discovered because the au-
evaluation of antidepressants. thors had enough information to be able to com-
Information necessary to uncover the prob- pare published studies with those submitted to the
lem: In order to be able to evaluate the efficacy of regulator, including details of methods and results
each of the antidepressants versus placebo it was of each individual study submitted to the manu-
necessary to have the data on the results of each facturer.
individual phase III (large clinical) trial submitted Health Canada SBDs: The information avail-
by manufacturers to obtain market approval. able in the SBDs includes study number, drug
Health Canada SBDs: This information is not doses, types of comparators and doses, number of
available. patients (it is unclear if this is number screened,
Conclusion: The conclusion that either these number enrolled or number analyzed) and dura-
six antidepressants are no more efficacious than tion of the trial. Results (efficacy and side effects)
placebo or that trial designs need to be modified are not presented individually.
would not have been possible to make based on Conclusion: The biases between the submit-
data in the SBDs. ted trials and the eventual publications would not
have been discovered using the SBDs.
2. Selective Serotonin Reuptake Inhibitors for
Major Depression c. Cardiovascular Risks of Hormone Re-
A 2003 study published in the BMJ (British placement Therapy (HRT)
Medical Journal) looked at 42 placebo controlled The publication of the results of the Women’s
studies of five SSRI antidepressants that were sub- Health Initiative (WHI) showed that use of
mitted to the Swedish drug regulatory authority estrogen and progestin in postmenopausal women
between 1989 and 1994 as a basis for marketing lead to increased cardiovascular risks. However, a
approval for treating major depression. These 42 combination of published and unpublished data
studies were compared with the ones that were submitted to regulatory authorities could have
Transparency in Drug Regulation: Mirage or Oasis? 17uncovered these risks earlier making the WHI cal (efficacy) trials would have revealed the effect unnecessary. In 1997 Hemminki and colleagues of hormone replacement therapy on cardiovascu- took data on cardiovascular and cancer events from lar risk much earlier, even than 1997 . . . [but] published randomized controlled trials on HRT many of the studies were unavailable”. and showed that odds ratio for cardiovascular and Information necessary to uncover the prob- thromboembolic (blood clots) events for women lem: In order to be able to add data from the un- taking HRT versus those not taking it was 1.97 published trials to the meta-analysis the authors (95% CI, 0.65, 4.21). In a second analysis, needed outcome and safety data on each individual Hemminki added results from unpublished trials unpublished trial. and although the overall results did not change Health Canada SBDs: This information is not significantly (odds ratio 1.97, 95% CI, 0.84, 4.63) available. the additional data hinted at publication bias as Conclusion: It would not have been possible the relative risk in the unpublished trials was about to find the negative risk-benefit ratio for combined 4.25 for cardiovascular events. McPherson and HRT in postmenopausal women based on data in Hemminki have concluded that “systematic syn- the SBDs. thesis of all data from well conducted small clini- 18 Canadian Centre for Policy Alternatives
VII: Is the Summary Basis of
Decision Adequate
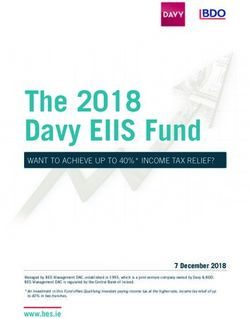
IN EACH OF THE FOUR EXAMPLES the Once a drug has been approved in the United
problems would not have been discovered using States the FDA posts on its web site a detailed sum-
Health Canada’s SBDs due to the lack of detailed mary of the information that the company has sub-
information of various types in these documents. mitted, including the clinical trial data. The Table
In each case, the necessary information includes a compares the extent to which clinical information
detailed report of the methods and results of each is reported in the two sample SBDs for rosuvastatin
clinical trial submitted by the manufacturer. Such (Crestor) and agalsidase beta (Fabrazyme) to the
reports should include study design (including information on the FDA website. It is clear that
numbers of centers and countries in which they compared to the U.S. what is available in Canada
were located), an identification number, inclusion is grossly inadequate. There is no justification for
and exclusion criteria for patients, analytical meth- Canada not matching the U.S. standard.
ods, numbers of patients screened, enrolled, fol- In order to be able to evaluate the thorough-
lowed, and withdrawn (including reasons for with- ness of the review process more than just the data
drawals) and details of study outcomes including that the companies submit is needed. It is also cru-
serious and total adverse events as well as efficacy cial to be able to see how the reviewers assessed
outcomes. that data, in-other-words, to have the reports from
A model for the minimum level of reporting the reviewers. This additional level of information
already exists in FDA approval packages. allows independent experts to understand what cri-
Comparison of Information Provided in Summary Basis of Decision (SBD) as compared to
U.S. FDA Approval Packages
Is the following information included? Sample SBD for Sample SBD for US FDA
rosuvastatin (Crestor) agalsidase beta approval
(Fabrazyme) package
List of individual Phase III trials [with ID Yes No ID’s, but there was only Yes
number] one phase III trial
Details on each study protocol, linked to No No Yes
study ID
Results (linked to study ID):
• Numbers of participants, baseline No [# of participants per No [# participants screened Yes
characteristics, withdrawals, follow-up study in total only; not per & randomized in total; not
treatment arm] per treatment arm]
• Primary and secondary efficacy outcomes No No Yes
(number and percent per treatment arm;
differences; tests of statistical significance)
• Fatal and non-fatal serious adverse events No No Yes
(number & type per treatment arm); total
adverse events, withdrawals due to
adverse events
Transparency in Drug Regulation: Mirage or Oasis? 19teria were used in making risk-benefit decisions to come but their exact form is deliberately being
andwhere there might be potential weaknesses in kept vague. Health Canada’s explanation for the
the analyses that were done by the regulators. This vagueness is that this is a new venture and each
type of information is also part of the FDA ap- step needs to be carefully evaluated.
proval package and comments from Canadian re- At the June consultation, this rational was not
viewers should be publicly available here. accepted by a number of organizations including
In June 2004, Health Canada held a the Alliance of Seniors to Protect Canada’s Social
multistakeholder meeting to discuss the progress Program, Canadian Treatment Action Council, Ca-
that had been made on the SBDs and proposed nadian Women’s Health Network and Women and
implementation steps. When officials were con- Health Protection. These groups drafted a state-
fronted with the limitations of the SBD they de- ment explicitly outlining additional commitments
fended the proposal by noting that this was only that Health Canada would have to make before
phase one of a proposed three phase model and they would endorse the process. Among the ele-
that even the current model for the SBDs was open ments that would have to be added to the pro-
to modification based, at least in part, on what posal were: the use of expert advisory groups to
was heard in the meeting. Subsequent phases would review new drug applications, providing informa-
examine the interpretation of the term “confiden- tion about drugs that were not approved, posting
tial information” and “may [emphasis added] see adverse drug reaction reports (with patient identi-
the inclusion of additional information” and “dis- fying information removed) on the Health Canada
closure of negative outcomes or withdrawals [re- web site, providing links to post-marketing infor-
fusals to approve new drugs or new indications for mation from other jurisdictions and ensuring that
older drugs, companies withdrawing submissions consumer and patient groups have adequate re-
before a decision has been made] would be explored sources to be able to continue to participate in any
[emphasis added]”. There are intimations of more further transparency initiatives (See Appendix 1).
20 Canadian Centre for Policy AlternativesVIII. Going Beyond Disclosure of Safety and
Efficacy Information for Approved Drugs
THE DISCLOSURE OF CLINICAL INFOR- The FDA committee system is not ideal. There
MATION is a key component to increasing trans- are reports that some of the experts who sit on
parency but there are further steps that must be these committees have conflicts of interest. The
taken to establish confidence in the drug regula- House of Representatives Government Reform
tory system and to ensure that drugs are prescribed Committee has investigated allegations that cer-
and used in an optimal manner. The Health tain physicians with multiple ties to heart drug
Canada discussion document on new health pro- manufacturers have been retained on the Cardio-
tection legislation asks if there should be an op- vascular and Renal Drugs Committee for extended
portunity for the public to present written com- periods in defiance of FDA regulations. An analy-
ments about new products prior to their approval sis by the newspaper USA Today found that more
and whether there should be public hearings “where than half of the experts who served on FDA advi-
considered appropriate by the Minister”. The Sci- sory committees from January 1, 1998, to June
ence Advisory Board’s Committee didn’t question 30, 2000 declared potential financial conflicts with
if public hearings should be held but rather felt the drug or policy being discussed or voted on.
they were “desirable” although the Committee did The federal agency is forbidden from using experts
go on to say that public hearings by themselves with financial conflicts unless a waiver is granted,
would not provide a sufficient level of transpar- usually on the grounds that the experts’ value out-
ency. The FDA provides an example of the use of weighs the seriousness of the conflict. The FDA
open hearings. About 30% of new drug applica- grants these waivers routinely. If Canada adopts a
tions made in the United States go to advisory system of public hearings with expert advisory
committee hearings. These hearings are both panels a strict system of screening for conflict-of-
videotaped and also broadcast on the internet. At interest will be necessary.
these hearings the company wishing to market the Finally, just having data on drugs that have
product defends its application; the advisory com- been approved is not enough. It is also important
mittee appointed by the FDA questions the appli- to know about new drugs and new indications for
cant, sometimes with the help of external experts; already marketed drugs that were either not ap-
and the general public has the opportunity to proved or had their applications withdrawn by the
present facts or arguments deemed relevant to the companies. New drugs not approved might be
application. Both the companies and the FDA chemically related to products already on the mar-
prepare material for the advisory committee mem- ket and reasons for their rejection might point to
bers that covers safety and efficacy of the new prod- unrecognized safety issues with the drugs that are
uct and all of that information is also made avail- available. Companies might resubmit applications
able on the FDA web site. These meetings provide for new drugs and in these cases it is necessary to
an opportunity for open public debate on the know why the drugs were initially turned down to
merits of new drugs before they are marketed.
Transparency in Drug Regulation: Mirage or Oasis? 21be able to see if the deficiencies have been cor- the companies have applied for use for the indica- rected. One such product on the Canadian mar- tion in question but been refused for either rea- ket is Diane-35 an oral contraceptive that is mar- sons of safety or effectiveness. Without knowing keted as a second-line agent for acne in women. about the failed application doctors will continue This drug was rejected by the TPD twice, in 1993 to prescribe and patients will continue to take a and 1996, before finally being approved Drugs are product that may either be harmful in that par- often used off-label, for uses that were never ap- ticular situation or ineffective. proved by the regulatory authority. It may be that 22 Canadian Centre for Policy Alternatives
VIII. Summary of Recommendations
1. A detailed summary of all clinical information an opportunity for members of the public to
that companies submit as part of the regula- make a statement to the committee.
tory approval process should be routinely
posted on the TPD web site along with the 3. There should be rigorous standards of conflict-
reports from TPD reviewers. of-interest for members of expert committees.
2. Applications for approvals should routinely be 4. Clinical information and reviewers’ reports
sent to expert advisory committees for exami- should be available for new drugs and new
nation. Hearings of these committees should indications for old drugs where their applica-
be public, interested members of the public tions were refused or where the company with-
should receive whatever information the com- drew the application.
mittee members are given and there should be
Transparency in Drug Regulation: Mirage or Oasis? 23References
(1998). Ken Rubin versus The Minister of Health. Case Health Canada (2004). Summary Basis of Decision
no. T-2408-98, Federal Court Trial Division. (SBD) Crestor - AstraZeneca Canada Inc. Ottawa.
Atkinson, M. M. and W. D. Coleman (1985). Corpo- Health Canada (2004). Summary Basis of Decision
ratism and industrial policy. Organized interests and (SBD) Fabrazyme - Genzyme Canada Inc. Ottawa.
the state. A. Cawson. London, Sage.
Health Canada (March 2004). HPFB to publish ‘Sum-
Atkinson, M. M. and W. D. Coleman (1989). The mary Basis of Decision’ documents. Ottawa.
state, business, and industrial change in Canada. To-
ronto, University of Toronto Press. Hemminki, E. and K. McPherson (1997). “Impact of
postmenopausal hormone therapy on heart disease and
Canada Department of Finance (2003). Building the cancer – pooled data from clinical trials.” BMJ 315:
Canada we want. Budget 2003: investing in Canada’s 149-153.
health care system. Ottawa, Public Works and Gov-
ernment Services Canada. Hemminki, E. and K. McPherson (2000). “Value of
drug-licensing documents in studying the effect of
Canada’s Research-Based Pharmaceutical Companies postmenopausal hormone therapy on cardiovascular
(September 2002). Improving health through innova- disease.” Lancet 355: 566-569.
tion: a new deal for Canadians. Ottawa.
House of Commons Standing Committee on Health
Cauchon, D. (2000). Number of drug experts avail- (2004). Opening the medicine cabinet: first report on
able is limited. Many waivers granted for those who health aspects of prescription drugs. Ottawa.
have conflicts of interest. USA Today: A1.
Hrachovec, J. B. and M. Mora (2001). “Reporting of
CBC News: Disclosure (January 14, 2003). Two-for- 6-month vs 12-month data in a clinical trial of
one. 2004. celecoxib.” JAMA 286: 2398.
Gardner, D. M., B. Mintzes, et al. (2003). “Direct-to- International Society of Drug Bulletins (June 1998).
consumer prescription drug advertising in Canada: ISBD assessment of nine European Public Assessment
permission by default?” CMAJ 169(5): 425-427. Reports published by the European Medicines Evalu-
ation Agency (EMEA). Paris.
Government of Canada (1985). Access to Information
Act. Ottawa. International Working Group on Transparency and
Accountability in Drug Regulation (1996). Statement.
Gribbin, A. (2001). House investigates panels involved Amsterdam, Health Action International.
with drug safety. Washington Times. Washington: A1.
Ioannidis, J. P. A. and J. Lau (2001). “Completeness
Health Canada (2003). Health protection legislative of safety reporting in randomized tirals: an evaluation
renewal: detailed legislative proposal. Ottawa. of 7 medical areas.” JAMA 285: 437-443.
Health Canada (2004). Issue analysis summary: sum- Kirsch, I., T. J. Moore, et al. (2002). “The emperor’s
mary basis of decision - draft 7. Ottawa. new drugs: an analysis of antidepressant medication
data submitted to the U.S. Food and Drug Adminis-
tration.” Prevention & Treatment 5 (Article 23).
24 Canadian Centre for Policy AlternativesKPMG Consulting LP (June 2000). Review of the Prescrire International (June 2002). Reorienting Eu-
Therapeutic Products Programme cost recovery initia- ropean medicines policy. Paris.
tive: volume 1.
Science Advisory Board Committee on the Drug Re-
Lexchin, J. (2002). “New drugs with novel therapeu- view Process (2000). Appendix C-1. Report: observa-
tic characteristics: have they been subject to randomized tions and consultations: Washington D.C., July 19-
controlled trials?” Canadian Family Physician 48: 21, 1999. Ottawa.
1487-1492.
Science Advisory Board Committee on the Drug Re-
Lurie, P. and S. M. Wolfe (1998). FDA medical offic- view Process (2000). Appendix F: notes on Canadian
ers report lower standards permit dangerous drug ap- law and the drug review process. Ottawa.
provals. Washington, Public Citizen.
Science Advisory Board Committee on the Drug Re-
McGarity, T. O. and S. A. Shapiro (1980). “The trade view Process (2000). Report to Health Canada. Ot-
secret status of health and safety testing information: tawa.
reforming agency disclosure policies.” Harvard Law
Review 93: 837-888. Silverstein, F. E., G. Faich, et al. (2000). “
Gastrointestinal toxicity with celecoxib vs nonsteroi-
McPherson, K. and E. Hemminki (2004). “Synthesis- dal anti-inflammatory drugs for osteoarthritis and rheu-
ing licensing data to assess drug safety.” BMJ 328: 518- matoid arthritis: the CLASS study: a randomized con-
520. trolled trial.” JAMA 284: 1247-1255.
Melander, H., J. Ahlqvist-Rastad, et al. (2003). “Evi- Working Group on Backlog Assessment (1994). Back-
dence b(i)ased medicine – selective reporting from stud- log assessment - final report. Ottawa, Drugs Directo-
ies sponsored by pharmaceutical industry: review of rate.
studies in new drug applications.” BMJ 326: 1171-
1173. Wright, J. M., T. L. Perry, et al. (2001). “Reporting of
6-month vs 12-month data in a clinical trial of
Michols, D. (1997). Drugs and Medical Devices Pro- celecoxib.” JAMA 286: 2398-2399.
gramme Quality Initiative Bulletin #2. Ottawa, Health
Protection Branch. Writing Group of the Women’s Health Initiative
(2002). “Risks and benefits of estrogen plus progestin
Office of Inspector General (March 2003). FDA’s re- in healthy postmenopausal women.” JAMA 288: 942-
view process for new drug applications: a management 945.
review. Washington, Department of Health and Hu-
man Services.
Transparency in Drug Regulation: Mirage or Oasis? 25Appendix 1
Conditions for Endorsement of Summary Basis of Decision
GROUPS AND INDIVIDUALS SIGNATORY 3. The history of the drug and approval process
to the letter recognize and appreciate the strides should also be posted on the web, including
made to date by the Health Products and Food rejections of market applications, and any of
Branch in creating an environment of consumer Health Canada’s decisions prior to a compa-
involvement and transparency. However, as it cur- ny’s withdrawal of an application;
rently stands, the model for a Summary Basis of
Decision put forward at this consultation does not 4. Product Monographs should be posted on the
meet these common goals. web, including patient product monographs,
We therefore recommend the following and all existing product monographs for cur-
amendments and additions to this process: rently approved drugs (previous versions plus
latest revised version with date);
1. Public hearings of expert advisory groups
which discuss regulatory decisions. Individu- 5. Adverse drug reaction reports should be posted
als and organizations should be able to make on the Health Canada website in a format that
submissions to these meetings, and the full is readily accessible and searchable by the pub-
materials disseminated to the committee and lic (reports submitted by the public, health
transcripts of hearings also publicly available professionals and manufacturers), as well as
(at the meeting and posted on the web). A linkages to international governmental
process for determining the model for such databases of adverse drug reaction reports;
hearings should be held with consumers or-
ganizations; 6. Links should be provided to post-market in-
formation from other jurisdictions and results
2. The full drug review should be posted on the of new clinical trials carried out in the post-
web when a new drug is approved, including approval period;
full reports of all chemical, pre-clinical and
clinical studies submitted to the regulatory 7. In order for consumer and patient groups to
agency, reviewers’ comments, and any condi- participate effectively in any advisory or con-
tions of approval (redaction by Health Canada sultation process, there is a need for adequate
only of information that could compromise resources to be provided for capacity-building,
individual privacy and commercial confiden- including training, internal consultation, and
tiality to a level currently in place at the US travel and accommodation.
FDA);
26 Canadian Centre for Policy AlternativesYou can also read