The Response of Healthy Men to Treadmill Exercise
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The Response
of Healthy Men to Treadmill Exercise
ROGER A. WOLTHUIS, PH.D., VICTOR F. FROELICHER, JR., LT COL, USAF, MC,
JOSEPH FISCHER, M.S., AND JOHN H. TRIEBWASSER, COL, USAF, MC, FS
SUMMARY Heart rates, blood pressures, and functional indicated measurements are individually described by the use of
responses to submaximal, maximal and postexertional treadmill test- percentiles. These data provide the practicing clinician with an ac-
ing are presented for a group of 704 healthy, asymptomatic air- curate and complete description of the response of healthy men to
crewmen referred to the USAF School of Aerospace Medicine. The treadmill exercise.
THE INTERPRETATION OF ELECTROCARDIO- to submaximal, maximal, and postexertional treadmill
GRAPHIC CHANGES in response to exercise testing is of testing. In addition to diagnostic use, these reference values
established value in the early detection, diagnosis, and sub- serve as a basis for monitoring individuals during treadmill
sequent management of coronary atherosclerotic heart dis- testing to assure patient safety. Finally, this study may
ease (CAD).'` The major emphasis placed on inter- provide the basis for subsequent studies which seek to es-
pretation of the exercise electrocardiogram (ECG) has, tablish discriminant values that separate healthy individuals
however, tended to de-emphasize the value and significance from those with specific health disorders.
of other commonly acquired exercise performance
measurements (i.e., heart rate, blood pressure, and func- Materials and Methods
tional capacity). These latter measurements are currently at-
tracting renewed attention as part of an effort to improve the The United States Air Force School of Aerospace
overall sensitivity and specificity of exercise testing. Recent Medicine (USAFSAM) provides a clinical consultation ser-
reports have suggested that maximal oxygen consumption,6 vice for the evaluation of referred, ambulatory aircrewmen
functional aerobic capacity estimated from maximal tread- with a broad spectrum of suspected or manifested medical
mill time,7 8 maximal and submaximal heart rate and blood disorders. These medical disorders, though mild and usually
pressure,9-" and the maximal heart rate-blood pressure asymptomatic, are potentially serious in view of modern air-
product,'2 may also be useful indices for identifying the crew responsibilities. All individuals in the present study
presence and/or severity of CAD in patients. were aircrewmen referred to this service.
The value of any measurement in providing useful diag- All referred aircrewmen are given a complete and com-
nostic information from treadmill testing depends upon: a) prehensive medical evaluation at the USAFSAM. This
the accuracy and completeness with which the measurement medical evaluation includes a history and physical examina-
has been made in healthy individuals (the reference values); tion by flight surgeons, internists, ophthalmologists, and
and b) the effectiveness with which certain limits of the ENT consultants, with further specialist work-ups where in-
measurement (discriminant values) separate healthy in- dicated. Extensive clinical laboratory studies are completed.
dividuals from those with known health disorders.'3 Additional procedures routinely accomplished include chest,
Previously published studies have reported reference values abdominal and sinus X-rays, resting ECG and VCG, max-
based on the response of healthy individuals to treadmill imal treadmill exercise testing, at least four hours of Holter
testing. Unfortunately, a majority of these studies were ECG monitoring, and spirometry.
based on a small sample size, and statistics based on them More then 2500 aircrewmen were seen at the USAFSAM
are less likely to provide a true estimate of population Consultation Service between 1973 and 1975; each of the in-
parameters than is a comparable study based on a larger dividual medical records and results of the USAFSAM
number. In the remaining few studies with a larger sample evaluation were reviewed for the purpose of identifying a
size, data for both submaximal and postexertional treadmill subgroup of healthy individuals. We excluded all individuals
responses are fragmentary and incomplete. Hence, the prac- with acute or chronic medical disorders or with any condi-
ticing clinician has not had a complete and readily available tion that might affect functional capacity. Additionally, men
set of reference values for use with his application of tread- with bundle branch block, significant Q waves, significant
mill exercise testing. ventricular arrhythmias, hypertension, on medication of any
The purpose of the present report is to establish a com- kind, or with any abnormality brought out by treadmill test-
plete set of reference values for the response of healthy men ing, were excluded. Men below age 25 or above age 54 were
excluded because their numbers were too small to provide
meaningful data. This left a subgroup of 704 healthy,
From the Internal Medicine Branch/NGI, USAF School of Aerospace asymptomatic aircrewmen; the treadmill test results from
Medicine, Brooks AFB, Texas.
The research reported in this paper was conducted by the personnel of the these 704 men serve as a basis for the present report.
Clinical Sciences Division, USAF School of Aerospace Medicine, Aerospace Maximal treadmill testing was conducted in the morning
Medical Division, AFSC, United States Air Force, Brooks AFB, Texas with each individual fasting and well rested. This was the
78235.
Dr. Froelicher's present address is Wilford Hall USAF Medical Center, subject's first treadmill test and initial experience with tread-
Lackland AFB, Texas. mill walking. Ambient temperature was typically main-
Address for reprints: Roger A. Wolthuis, Ph.D., Internal Medicine Branch,
NGI, USAF School of Aerospace Medicine, Brooks AFB, Texas 78235. tained in the range of 23 to 26°C. Multichannel ECG data
Received May 10, 1976; revision accepted August 16, 1976. were continuously collected using fluid column silver/silver
153154 CIRCULATION VOL 55, No 1, JANUARY 1977
chloride electrodes and associated ECG electronic equip- subsequently used to calculate the median (50th percentile)
ment as previously described.'4 Blood pressure was and the 10th and 90th percentile limits for each stated
measured at regular intervals in the left arm by auscultation; measurement at selected treadmill protocol times. We chose
Phase V (disappearance of sounds) was taken as the dia- this nonparametric approach in presenting our data because
stolic endpoint. Expired air was collected at full minute in- the use of percentiles 1) does not require an assumption of a
tervals as maximum treadmill effort was approached; air normal distribution of the population reported, and 2) this
collection was accomplished using a standard mouthpiece type of presentation is easily understood by most people.
and nose clip, Koegel's valves and turret,'5 and weather Our specific use of the 10th and 90th percentiles was an ar-
balloons. Gas volumes were measured with a Tissot bitrary choice and provides relatively conservative limits for
spirometer corrected for pressure and temperature. Expired the response of healthy men to treadmill exercise. Finally,
gas analysis for carbon dioxide and oxygen was performed linear regression equations were computed for maximum
with Beckman LB-l and E-2 instruments, respectively; these heart rate on age and maximum oxygen consumption on
instruments were calibrated daily with gases analyzed by the age.
micro Sch6lander technique. Results
The treadmill testing procedure included initial periods of
supine rest (2 min), quiet standing (3 min) and hyperven- For the 704 individuals that were studied, median (50th
tilation (0.75 min); then followed a treadmill walk at 3.3 percentile) age was 37 years, with 26 and 47 years as the 10th
mph with 1% grade increases each minute until a maximum and 90th percentiles. Median height was 178 cm, with the
effort had been performed.'6 Individuals were not allowed to 10th and 90th percentiles at 170 and 185 cm, respectively.
support their weight on treadmill handrails during the test. Median weight for the study population was 78 kg, with 67
All individuals were cooperative and gave what they and the and 89 kg being the 10th and 90th percentiles, respectively.
monitoring physician considered a maximal effort. Max- These heights and weights are remarkably similar to those
imum effort was followed by an 8-min supine recovery published for a non-service-related male population;'7 our
period. lower median age is characteristic of military populations in
All measurement data from each individual treadmill test general.
were entered into a computer data base. This data base was Supine rest (control period) and submaximal treadmill ex-
CONTROL SUB - MAXIMAL RESPONSE
F
r
-I
h
200F -190 -
174
L~~~158
HEART r 141 -3
RATE
lbpm) K102]
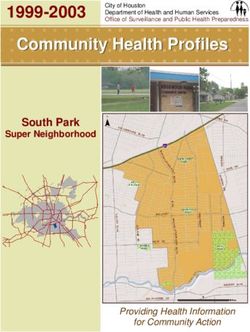
40 FIGURE 1. Control and submaximal treadmill
exercise measurement data are shown as median
220r - 208- (U) with 10th and 90th percentiles. Submaximal
data are presented for the 5, 10 and 15 percent
SYSTOLIC 7174 L-: grade within the Balke-Ware treadmill protocol;
BLOOD the relationship between these three grades and
PRESSURE other treadmill protocol stages is depicted at the
lmmHgl bottom of the figure.
z140 1 *2 The numbers of subjects with complete data for
110 each of the measurements are 698 for control;
IOOL
699, 700, and 503, respectively, for three sub-
maximal responses.
100 _
DIASTOLIC 90 X 90 90-90
BLOOD7
PRESSURE
(mmHg)
L 68
60~~~~~~~~~~~~~~~6
5 PERCENT rGRADE, 10 AT 3.3 MPH t5
L
mEI ,
,B | BRUCE |
ELLESTAD
|
[0 i~] McHENRYEXERCISE RESPONSE OF HEALTHY MEN/Wolthuis et al. 155
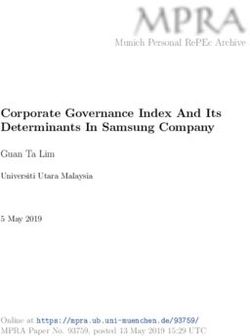
ercise test data are presented in figure 1. The control period Supine treadmill recovery data are shown in figure 3. As
heart rate and blood pressure data are in the expected range; expected, heart rate and blood pressure data show a fall at
the slight elevations in diastolic blood pressures are probably recovery minute two and a further fall at minute five from
due to anticipation of the treadmill test. Next, submaximal values attained during maximal exercise.
treadmill test data are given for 5, 10 and 15 min (or 5, 10, All blood pressures were measured by auscultation, and
and 15% grade) of the Balke-Ware treadmill protocol; time our presentation of these data should not obscure the lack of
and treadmill percent grade are numerically the same within accuracy inherent with this technique when applied to exer-
this protocol. As shown, heart rate and systolic blood pres- cising subjects.19- 20 On the other hand, auscultation is the
sure increased with time and workload, with the increase method typically used during clinical exercise testing and is
tapering off as maximum effort is approached. Diastolic felt to be of value.1' Within these limitations, the present
blood pressure stayed constant or fell slightly with increas- data are designed to provide a range of expected values for
ing effort. The relationship between the Balke-Ware sub- these conditions.
maximal workload levels and other well-known treadmill All patients were classified with respect to physical ac-
protocol stages is shown at the bottom of figure 1.18 tivity (i.e., active, moderately active, or sedentary) on the
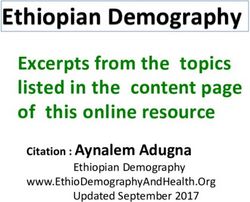
The response at maximal effort during treadmill testing is basis of a questionnaire.21 Linear regression equations were
shown in figure 2; these data are presented by age decades. computed by activity status for maximum heart rate on age
The observed drop in maximal heart rate, maximal oxygen and maximum oxygen consumption on age. The maximal
consumption, and maximal treadmill time with increasing heart rate/age relationship was not statistically different
age is consistent with changes noted in earlier studies. Max- between the three activity groups, and we have thus
imal systolic blood pressure and pressure-rate product presented a single regression equation based on the total
change little across the three age decades studied, while data (table 1). On the other hand, regression equations of
diastolic pressure increases slightly. maximal oxygen consumption on age differed in intercept
but not slope for the three activity groups; we have presented
MAXIMAL [last minutel RESPONSE separate intercepts and a common slope for this
220 _ relationship. In all cases, maximal heart rate and maximal
FIs^3 [200 194 oxygen consumption declined with age, a finding consistent
HEART F ] F with earlier reports. However, the low correlation
RATE
1bpm) 10L'162--
175J L17i0 coefficients and high variability about each of the regression
140L
RECOVERY RESPONSE
SYSTOLIC
BLOODO
r11 r24 26 160 r
138-1
I
HEART
RATE --116
(bpm) 1021 .'I
80 L -88J
DIASTOLIC 90
PRESSURE 540_
JmmHg)PRSURE60L L -60-I
;-;6
-El
:a
200 194-
SYSTOLIC
PRESSURE- 50 4 BLOOD
RATE
PRODUCT
40 - 4 39
L 1
PRESSURE m158n
3
92 (mmHg) -140-
(HR x SBPI 10320L
120 L L-120J
Ol 50 [48 ][4%74
(cc/kg - min) 34 2*9
90s 690
20 L 20t~~~~~ 31-
29
DIASTOLIC |
86
25 BLOOD |
BALKE MAX 21 -
20 19
PRESSURE
TIME (min)
13
(mmHg) 60 L
60 60
TIE(ioiL L1 [12 L
AGE GR:P: :25-34 235-4 45-54 I min.2 I| min.5 |
FIGURE 2. Maximal response treadmill exercise measurement FIGURE 3. Postexertional treadmill exercise measurement data
data are shown as median (-), with 10th and 90th percentiles, for are shown as median (-), with 10th and 90th percentiles, for
each of three age decades. minutes 2 and 5 of the recovery period.
The numbers of subjects with complete data for each of the The numbers of subjects with complete data for each of the
measurements shown are (from left to right) 287, 317, and 100. measurements shown are 692 and 698.156 CIRCULATION VOL 55, No 1, JANUARY 1977
TABLE 1. Linear Regression Equations for Maximal Oxygen ent study between physical activity groups, in part because
Consumption on Age, by Activity Status, and for Maximal of genetic and other biological differences, and also because
Heart Rate on Age of inadequacies in the available methods for classifying
(For active) VO = 50.6 - 0.17 X age (N = 99) physical fitness. Given these limitations and the desire to
(For mod active) VO2 = 45.8 - 0.17 X age (N = 258) keep our main data presentation simple and easy to use, the
(For sedentary) VO, = 43.2 - 0.17 X age (N = 34-5) reference values in figures 1, 2 and 3 are presented without
rpooled = -0.24 SEl"Epoolekd = 5.30
(For all) HR = 204 - 0.6 X age (N = 704) regard to physical activity.
rpooled= -0.40 SEEpoole(d = 10.12 Finally, learning to walk the treadmill more efficiently
Abbreviations: HR = heart rate; VO = oxygen consumption. leads to lowered heart rates at submaximal workloads and
an increase in maximal treadmill performance without im-
provement in cardiovascular status or physical fitness. This
lines, also demonstrated previously,'4 preclude the predic- learning can be done by allowing an individual to perform a
tive usefulness of these relationships. series of treadmill tests.24 Individuals used in the present
study were receiving their first treadmill test; repeat users
Discussion were excluded for the reasons given.
Comparison with Other Healthy Populations
Responses Outside the 10th and 90th Percentiles
The report by Bruce and colleagues, based on 1275
healthy individuals, is the only previous sizable study pre- The 10th and 90th percentiles were arbitrarily presented;
senting both control and submaximal treadmill response these are conservative reference values for the response of
data.'7 Mean heart rate and blood pressure values for the healthy men to treadmill exercise. Since 20% of our healthy
control period are essentially the same as our median con- population lay outside these limits, patients falling outside
trol period data shown in figure 1. Further, mean heart rate these limits may well be normal. However, our reference
and blood pressure values from the Bruce protocol stage 1 values help to exclude individuals having subclinical con-
are similar to the 5% grade values we have demonstrated.
ditions that compromise treadmill performance. Thus, men
Ellestad has graphically presented submaximal heart rate with responses lying outside these limits should be evaluated
and blood pressure data over a series of age decades.2" The since they may be at increased risk for having a health
average responses seem to agree with our median responses;
problem.
his 95% confidence values cannot be directly compared with Elevated heart rate values at submaximal exercise, max-
the percentile limits presented here. imal exercise, or recovery, could be due to vasoregulatory
The response of heart rate and oxygen consumption to asthenia2" or to any condition that decreases peripheral
maximal treadmill exercise are presented in figure 2 and resistance. Prolonged bed rest could also explain such heart
show agreement with other studies.6' 116, 2 The maximal
2,
rate elevations.26 A relatively low heart rate at any point
blood pressure and pressure-rate product values presented during submaximal work could be due to physical condition-
by Bruce and colleagues'7 are also in agreement with those ing and/or an enlarged heart with enhanced stroke volume,
shown in figure 2. Recovery heart rate data presented in or it could be due to drugs such as propanolol. Ellestad has
figure 3 are very similar to those published from this reported chronotropic incompetence, which he defines as a
laboratory on a smaller series." Visual inspection of the heart rate below the age-adjusted 95% confidence limits for
recovery data graphically presented by Ellestad across an 8
his treadmill protocol.22 His data demonstrate that
min recovery period22 again is quite similar to those chronotropic incompetence carries an increased risk for
presented in this report. CAD, even if there is a normal electrocardiographic
response to the treadmill test.9
Some Important Variables Affecting Treadmill Testing Systolic blood pressure has been seen to rise above the il-
lustrated limits in hypertensives." Such elevations have not
Age, physical fitness, and subject's treadmill experience been associated with any complications or ominous im-
are all known to have an effect on the treadmill measure- plications in our laboratory. An inadequate blood pressure
ments presented. With respect to age, there were some rise can be due to aortic valve disease or left ventricular im-
statistically significant age group differences within the pairment. The heart rate-blood pressure product at maximal
separate measurements during control, submaximal exer- exercise has been considered a measure of left ventricular
cise, and recovery periods. However, the differences were function.'2 An excessive elevation could cause a false
small and were not considered important for the purposes positive exercise test because of a physiological imbalance
for which these data are presented. With the exception of between myocardial blood supply and demand. We have not
maximal heart rate and oxygen consumption, differences in seen this occur in our laboratory. Low values could be due to
response to maximal exercise across the age decades were left ventricular dysfunction, outflow obstruction, poor
also small. Our presentation of the maximal measurement patient cooperation, or medication.
data by age decades was largely prompted by precedence Maximal oxygen consumption has been considered a
and the desire to permit comparison with other published valuable measurement since it noninvasively estimates max-
studies. imal cardiac output27 and is an index of work capacity and
With regard to physical fitness, individuals with a high maximal cardiovascular function.6 However, its practical
level of fitness are known to have lower heart rates at sub- diagnostic value is limited because of biological variability,
maximal workloads, higher maximal oxygen consumptions, the expense of measuring it accurately, and limitations in es-
and quicker drops in recovery heart rate than sedentary in- timating it from treadmill time'4' 20, 28 or by using some
dividuals. However, we observed much overlap in the pres- automated commercial devices. Possibly, determination ofEXERCISE RESPONSE OF HEALTHY MEN/Wolthuis et al. 157
an individual's maximal treadmill workload may be a more MC: Value of exercise testing for screening asymptomatic men for latent
accurate and/or adequate measure of maximal cardio- coronary artery disease. Prog Cardiovasc Dis 18: 265, 1976
6. Mitchell JH, Blomqvist G: Maximal oxygen uptake. N Engl J Med 284:
vascular function. 1018, 1971
Recovery heart rates return to near basal levels faster in 7. Bruce RA, Kusumi F, Hosmer D: Maximal oxygen intake and
individuals who are physically fit.2" The rate of change nomographic assessment of functional aerobic impairment in cardiovas-
cular disease. Am Heart J 85: 546, 1973
toward basal is also dependent upon the integrity of the car- 8. Bruce RA, Kusumi F, Niederberger M, Petersen JL: Cardiovascular
diovascular system and the health of an individual. mechanisms of functional aerobic impairment in patients with coronary
heart disease. Circulation 49: 696, 1974
9. Ellestad MH, Wan MKC: Predictive implications of stress testing.
Relevance of Regression Data Follow-up of 2700 subjects after maximum treadmill stress testing. Cir-
culation 51: 363, 1975
Regression analysis indicated that maximal heart rate 10. Bartel AG, Behar VS, Peter RH, Orgain ES, Kong Y: Graded exercise
declined with age as has been shown by many investigators.'8 stress tests in angiographically documented coronary artery disease. Cir-
culation 49: 348, 1974
Lester and colleagues reviewed the studies of maximal heart 11. Thomson PD, Kelemen MH: Hypotension accompanying the onset of ex-
rates and presented their results in a group of 190 male ertional angina. A sign of severe compromise of left ventricular blood
volunteers ranging in age from 15 to 75.23 They found a supply. Circulation 52: 28, 1975
12. Bruce RA, Fisher LD, Cooper MN, Gey GO: Separation of effects of
regression slope of -0.41 beats/min/year for both active cardiovascular disease and age on ventricular function with maximal ex-
and sedentary subjects, -but active subjects had a lower max- ercise. Am J Cardiol 34: 757, 1974
13. Sunderman FW Jr: Current concepts of "normal values," "reference
imal heart rate at any age. Other investigators have values," and "discrimination values" in clinical chemistry. Clin Chem 21:
suggested a decline in maximal heart rate of one 1873, 1975
beat/min/year.18 Our decline of -0.61 beats/min/year but 14. Froelicher VF, Thompson AJ, Yanowitz F, Lancaster MC: Treadmill ex-
ercise testing at the USAFSAM: Physiological responses in aircrewmen
without an effect of activity status numerically lies between and the detection of latent coronary artery disease. AGARDOGRAPH
these values. Maximal heart rate has clinical importance No. 210, 1975, NASA, Langley Field, Virginia 23365
since many clinicians use heart rate-targeted submaximal 15. Lenox J, Koegel E: Evaluation of a new low resistance breathing valve. J
AppI Physiol 37: 410, 1974
exercise tests. 16. Balke B, Ware RW: An experimental study of physical fitness of Air
The analysis of maximal oxygen consumption regressed Force personnel. US Armed Forces Med J 10: 675, 1959
17. Bruce RA, Gey GO Jr, Cooper MN, Fisher LD, Peterson DR: Seattle
on age showed a decline with age as found by other in- heart watch: Initial clinical, circulatory and electrocardiographic
vestigators.6' 14 Dehn and Bruce reviewed both cross-sec- responses to maximal exercise. Am J Cardiol 33: 459, 1974
tional and longitudinal studies of maximal oxygen con- 18. Fox SM III, Naughton JP, Haskell WL: Physical activity and the
prevention of coronary heart disease. Ann Clin Res 3: 404, 1971
sumption and presented their results in a group of 86 healthy 19. Henschel A, De La Vega F, Taylor HL. Simultaneous direct and indirect
men with various activity levels.30 Analysis of their cross sec- blood pressure measurements in man at rest and work. J Appl Physiol 6:
tional data yielded a regression equation (VO2 = 506, 1954
20. Nelson RR, Gobel FL, Jorgensen CR, Wang K, Wang Y, Taylor HL:
49.93 - 0.278 X age) comparable to the one obtained in our Hemodynamic predictors of myocardial oxygen consumption during
study. The poor correlation of maximal oxygen consump- static and dynamic exercise. Circulation 50: 1179, 1974
21. Froelicher VF Jr, Thompson AJ Jr, Noguera I, Davis G, Stewart A,
tion and age is likely due to the fact that multiple factors Triebwasser JH: Prediction of maximal oxygen consumption. Com-
besides age are involved; i.e., genetic make-up, current and parison of the Bruce and Balke treadmill protocols. Chest 68: 331, 1975
previous activity status, blood volume, hematocrit, cardio- 22. Ellestad MH: Stress testing: Principles and Practice. Philadelphia, FA
Davis, 1975
vascular integrity, and environmental conditions.6' 14 23. Lester M, Sheffield LT, Trammell P, Reeves TJ: The effect of age and
athletic training on the maximal heart rate during muscular exercise. Am
Heart J 76: 370, 1968
Acknowledgment 24. Froelicher VF Jr, Brammell H, Davis G, Noguera I, Stewart A, Lan-
caster MC: A comparison of the reproducibility and physiologic response
The authors express their appreciation to Mrs. Rosa Linda Rodriguez for to three maximal treadmill exercise protocols. Chest 65: 512, 1974
her support with the manuscript preparation. 25. Friesinger GC, Biern RO, Likar I, Mason RE: Exercise electrocardiog-
raphy and vasoregulatory abnormalities. Am J Cardiol 30: 733, 1972
26. Saltin B, Blomqvist G, Mitchell JH, Johnson RL, Wildenthal K, Chap-
man CB: Response to exercise after bed rest and after training: A
References longitudinal study of adaptive changes in oxygen transport and body
composition. Circulation 38 (suppl VII): VII-78, 1968
1. Simonson E: Electrocardiographic stress tolerance tests. Prog Cardio- 27. McDonough JR, Danielson RA, Wills RE, Vine DL: Maximal cardiac
vasc Dis 13: 269, 1970 output during exercise in patients with coronary artery disease. Am J
2. Blomqvist CG: Use of exercise testing for diagnostic and functional Cardiol 33: 23, 1974
evaluation of patients with arteriosclerotic heart disease. Circulation 44: 28. Froelicher VF Jr, Lancaster MC: The prediction of maximal oxygen con-
1120, 1971 sumption from a continuous exercise treadmill protocol. Am Heart J 87:
3. Rosing DR, Reichek N, Perloff JK: The exercise test as a diagnostic and 445, 1974
therapeutic aid. Am Heart J 87: 584, 1974 29. Shephard RJ: The prediction of maximum oxygen intake from post-
4. Froelicher VF Jr: The application of electrocardiographic screening and exercise pulse readings. Int Z Angew Physiol 24: 31, 1967
exercise testing to preventive cardiology. Prev Med 2: 592, 1973 30. Dehn MM, Bruce RA: Longitudinal variations in maximal oxygen intake
5. Froelicher VF, Thompson AJ, Longo MR Jr, Triebwasser JH, Lancaster with age and activity. J Appl Physiol 33: 805, 1972You can also read