Systematic overview of systematic reviews and clinical guidelines: assessment and prevention of behavioural risk factors associated with oral ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
SYSTEMATIC REVIEW
Systematic overview of systematic reviews and clinical
guidelines: assessment and prevention of behavioural
risk factors associated with oral cancer to inform
dental professionals in primary care dental practices
Sweta Mathur,*1 David I. Conway,2 Lorna M. D. Macpherson2 and Alastair J. Ross2
Key points
• There is clear evidence for the • There is no firm conclusion with regards • As there is evidence for effectiveness of
effectiveness of a ‘brief’, in-person, to optimal duration of brief interventions ‘brief’ interventions, very brief (or brief
motivational intervention for sustained (range 5–20 minutes) and there is limited advice of up to five minutes) should be
tobacco abstinence or reduced alcohol direct evidence from the dental practice trialled for tobacco and alcohol respectively
consumption, following risk factor setting (one high-quality systematic in a dental practice setting, after risk
assessment. review relating to tobacco prevention assessment tailored to patient motivational
and none relating to alcohol). Evidence status. Exploring delivery by the dental team
for combined behavioural interventions is supported, as effectiveness was generally
(tobacco + alcohol) is also lacking. independent of primary care provider.
Abstract
Aims/objectives Tobacco and alcohol are recognised as the major modifiable risk factors for oral cancer, the incidence of which is
rising globally and predicted to increase. This paper aimed to: 1) appraise and synthesise best practice evidence for assessing the major
behavioural risk factors for oral cancer and delivering behaviour change interventions (for example, advice, counselling, signposting/referral
to preventive services); and 2) assess appropriateness for implementation by dental professionals in primary care.
Methods A systematic overview was undertaken of systematic reviews and international clinical guidelines. This involved: systematically
searching and collating the international literature on assessing oral cancer risk and delivering preventive interventions within primary care;
quality appraising and assessing the risk of bias using validated tools; synthesising the evidence for best practice; and assessing application
of key findings to the dental setting.
Results and conclusions There is clear evidence for the effectiveness of a ‘brief’, in-person, motivational intervention for sustained tobacco
abstinence or reduced alcohol consumption, following risk factor assessment. Evidence for combined behavioural interventions is lacking. There
is no firm conclusion with regards to optimal duration of brief interventions (range 5–20 minutes). For tobacco users, longer (10–20 minutes) and
intensive (more than 20 minutes, with follow-up visits) interventions are more effective in increasing quit rates compared to no intervention; very
brief (less than five minutes) interventions in a single session show comparable effectiveness to the longer/more intensive interventions. For alcohol
users, 10–15-minute multi-contact interventions were most effective, compared to no intervention or very brief (less than five minutes) intervention
or intensive intervention; brief interventions of five-minute duration were equally effective. There is limited direct evidence from the dental practice
setting (one high-quality systematic review relating to tobacco prevention and none relating to alcohol). Thus, very brief, or brief advice of up to
five minutes, should be trialled for tobacco and alcohol respectively in a dental practice setting, after risk assessment tailored to patient motivational
status. Exploring delivery by the dental team is supported, as effectiveness was generally independent of primary care provider.
Introduction rapid increase in oropharyngeal cancer rates to increase further over the next decade,
The incidence of oral cancer continues to in the last decade.1,2 Globally, oral cancers so there is a pressing need to optimise oral
rise globally and in the UK, with a steady (including lip, oral cavity and pharynx) cancer prevention strategies.1,2
increase in oral cavity cancer rates and a have been estimated to be responsible for There is a significant increased risk for
529,500 incident cases and 292,300 deaths oral cancer among lower socioeconomic
1
Kaiser Permanente Centre for Health Research, Portland, in 2012, accounting for about 3.8% of all groups, men and older age groups,3 and
OR, USA; 2School of Medicine, Dentistry and Nursing, cancer cases and 3.6% of cancer deaths. In 1
there is recent recognition of the role of
University of Glasgow, UK.
*Correspondence to: Sweta Mathur Scotland, between 2001 and 2012, there was human papillomavirus in the aetiology of
Email address: mathursweta@outlook.com a dramatic increase in oropharyngeal cancer oropharyngeal cancers.4 However, tobacco
Accepted 19 Jan 2022 cases (85%), while incidence rates remained and alcohol use are recognised as the major
Online Publication 7 March 2022 relatively unchanged for oral cavity cancer modifiable risk factors for developing oral
https://doi.org/10.1038/s41432-022-0235-1
(10% increase). These rates are projected
2
cancers (oral cavity and oropharyngeal
© EBD 2022 1
© The Author(s), under exclusive licence to British Dental Association 2022SYSTEMATIC REVIEW
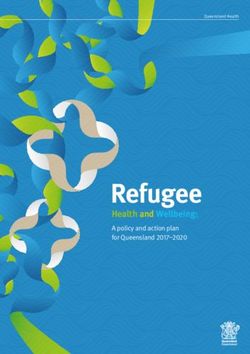
cancers).5,6 These modifiable behaviours are Fig. 1 PRISMA four-phase flow diagram for included systematic reviews
also associated with a wide range of diseases
affecting oral and general health and are Records identified through
thus denoted as ‘common risk factors’, database searching
Identification
increasing the public health benefit should (nSR = 1727)
they be tackled.7
There is therefore a clear need to implement
Records after duplicates removed
optimal preventive interventions in dental (nSR = 1271)
primary care.8 However, there are remaining
uncertainties about the best evidence for
particular strategies and approaches to
Titles screened Records excluded
assessing risk, giving advice, or referral to
(nSR = 1271) (n = 546)
specialist counselling or cessation services.8 A
Screening
particular evidence gap relates to the specific
form and content of such interventions (for
example, tailoring to need/assessing risk, Abstracts screened Records excluded
(nSR = 725) (n = 653)
duration, who delivers). 8,9,10,11
Most previous
studies have been carried out in medical or
community pharmacy settings,12,13 leading
to a number of items of clinical guidance.14,15 Full-text articles assessed Records excluded
Thus, the main aim of this paper was for eligibility (n = 44)
(nSR = 72)
Eligibility
to provide a comprehensive overview 21 Wrong setting
10 Wrong intervention
of systematic reviews (SRs) and clinical
8 Wrong population
guidelines (CGs) from across primary care 3 Review of reviews
to make recommendations for dental 1 Wrong outcomes
1 Wrong study design
practice in relation to assessing/targeting
the major behavioural risk factors (tobacco
smoking and alcohol drinking) associated
with oral cancer and delivering preventive Additional SRs identified through
hand searching (nSR = 3)
interventions. Specific objectives were: to
Included
assess best practice for assessing risks and
facilitating behaviour change; to assess
commonality and/or divergence between SR Studies included in narrative synthesis
(nSR = 31)
evidence and CG recommendations; and to
assess feasibility for the dental setting.
Methods literature search for SRs and CGs was carried cessation, harm reduction, brief
The study protocol, which details out in August 2015 and updated in August intervention, counselling)
the methodology for this systematic 2018, in the following electronic databases: • Primary care (for example: general
overview, was registered with PROSPERO Cochrane Library, Ovid Medline, Embase, dental practice, general medical practice,
(registration number CRD42015025289) Web of Science, PsychINFO, PubMed, TRIP pharmacy)
and implemented without any changes, has and Google Scholar. • Risk factors (for example: tobacco,
previously been published.16 The overview An internet search of the websites of alcohol).
was framed in accordance with the PICOS health boards and relevant (professional,
(population, intervention, comparator, medical, dental, public health, scientific) Inclusion and exclusion criteria
outcomes and setting) format and findings organisations/agencies was also carried SRs or meta-analyses (of randomised
were reported using the PRISMA statement out. The bibliographies or reference lists and non-randomised studies) and CGs
for reporting of SRs and meta-analyses.17 of identified documents were also hand- (published/e-learning) available worldwide
searched for additional references. Experts were included in this systematic overview.
Search strategy in the area were contacted to help locate Papers were included from all primary
Search terms were identified from scoping any unpublished and ongoing research care settings (dental/medical/pharmacy)
the initial literature and from MeSH subject as the overview proceeded to minimise if describing in-person or face-to-face
headings. The search was not limited to oral publication bias. The Ovid Medline search preventive interventions (including risk
cancer studies so as to include interventions strategy is provided in the protocol 16 and factor assessment, behavioural advice and/or
aimed at another clinical condition (for was adapted for other databases. Key terms signposting/referral) for tobacco and alcohol.
example, smoking cessation strategies were organised according to three subsets: No language restrictions were applied. Two
targeting periodontal disease). 18
The • Prevention (for example: advice, non-English papers were translated to
2 © EBD 2022
© The Author(s), under exclusive licence to British Dental Association 2022SYSTEMATIC REVIEW
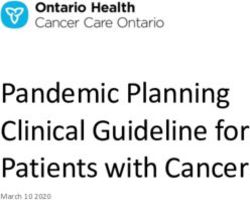
Fig. 2 Graphical representation of both AMSTAR and ROBIS scores common. To address this, a list of all authors
of all primary studies/trials referenced by all
12
Low Low included SRs was created, sorted and labelled
Low Low Low Low
10 to identify publications which appeared two
Low Low Low
or more times on the list.26 Where duplicates
Low
AMSTAR score (0-11)
8 were identified, overview results based on
High Low Low Unclear Low Low Unclear
Unclear High Low High Unclear individual trials have been synthesised here
6
High High High High from higher-quality/more recent SRs. This
High High avoided overstressing the evidence base by
4
High High
accumulating SR results which themselves
High
2 drew from the same evidential sources, thus
biasing findings. The 31 SRs reviewed a total
0 of 171 discrete original trials of face-to-face
1
2
3
4
5
6
7
8
9
10
SR 1
SR 2
13
14
15
16
SR 7
SR 8
19
SR 0
21
SR 2
23
SR 4
25
SR 6
27
SR 8
SR 9
SR 0
31
SR
SR
SR
SR
SR
SR
SR
SR
SR
1
1
1
1
2
2
2
2
2
2
3
preventive interventions in a primary care
SR
SR
SR
SR
SR
SR
SR
SR
SR
SR
SR
Systematic Review ID setting (that is, after removing duplicates).
*Blue vertical bars in the figure represent the AMSTAR scores (which ranges from 1-11) and The main characteristics and findings of
low/high/unclear written in boxes are ROBIS scores. the included 31 SRs are presented (see online
Supplementary Table S3); for example,
target risk factors, included preventive
English with the help of Google Translate along with guidance from the Centre for interventions, intervention provider, study
and private translation services. CGs were Reviews and Dissemination,23 and Petticrew quality, type of synthesis and outcomes.
limited to the last ten years (2006–2015). and Roberts,24 were adopted for conducting Study IDs (from online Supplementary Table
There were no date restrictions for SRs. a narrative synthesis for the overview. S1) are used to reference cohort SRs in the text
Narrative/literature reviews and SR protocols A final integrated/combined synthesis of this paper. The included SRs were relatively
were excluded. then compared and contrasted evidence heterogeneous in that they covered different
from the reviews and guidelines streams. primary care settings (dental/medical/
Data management and extraction The narrative synthesis assessed the best pharmacy), risk factors (tobacco/alcohol)
In accordance with Cochrane review group practice evidence by taking quality and and preventive interventions (motivational
guidance, all steps in data management recentness of evidence into account, giving interviewing/cognitive behavioural therapy).
(review of titles and abstracts, inclusion higher weighting to dental findings, and Preventive interventions also varied with
and exclusion decisions, data extraction, considering higher-quality and more recent respect to: duration of individual sessions;
quality appraisal, assessing risk of bias, medical/pharmacy findings applicable in a total number of sessions; follow-up visits;
collating themes for final synthesis) were dental practice setting – informed by the and provider training.
carried out independently by two members ADAPTE framework.25 The AMSTAR scores for all SRs are included
of the multidisciplinary review team (author (see online Supplementary Table S4); only
[SM] + one of three supervisors [AR/DC/ Results two SRs met all 11 criteria in AMSTAR (SR:
LM]) and discrepancies discussed. The data Systematic reviews 1, 16). This overview identified ten high-
extraction form was pilot tested on a small The search strategy retrieved 1,727 quality SRs (score range from 8–11), 18 mid-
set of papers (three SRs and three CGs) and potentially relevant records. Titles and quality SRs (score 4–7) and three low-quality
refined to ensure sensitivity and specificity. abstracts were screened independently by SRs (score 0–3). The ROBIS scores for all SRs
two reviewers (SM and AJR), and of these, are included (see online Supplementary
Quality appraisal 72 records were selected for full-text review. Table S5). Figure 2 shows AMSTAR and ROBIS
In order to assess the methodological Twenty-eight systematic reviews (SRs) scores. It can be seen that high AMSTAR
quality and risk of bias of included SRs, the were included after discussion and a few score SRs were correlated with low risk of
AMSTAR (A MeaSurement Tool to Assess discrepancies were discussed with the wider bias in ROBIS and vice versa, while risk of
systematic Reviews) and the ROBIS (Risk Of team (DC and LM). Three additional SRs bias was unclear in some SRs.
Bias In Systematic reviews) tools were used were included through hand searching of In this paper, the high-quality evidence/
respectively.19,20 The quality of the included the reference lists of the 28 included SRs. findings are presented from all low risk of
CGs was appraised using the AGREE II Thus, finally 31 SRs were included in this bias (low ROBIS) reviews, giving priority in
(Appraisal of Guidelines for REsearch & overview (Fig. 1). References to all included the narrative data synthesis to: firstly, high-
Evaluation II) instrument. 21
SRs are provided (see online Supplementary quality AMSTAR scores with low risk of bias
Table S1). A list of excluded studies (n = 44) in ROBIS (n = 10); and secondly, mid-quality
Data synthesis was presented with the reasons for exclusion AMSTAR scores but with low risk of bias in
The general frameworks for conducting (see online Supplementary Table S2). ROBIS (n = 5). Key findings from these high-
narrative (‘thematic’) synthesis developed As might be expected, there was trial quality SRs are shown in Tables 1 and 2. There
by the Economic and Social Research duplication or overlap in the included was only one high-quality SR in the dental
Council (ESRC) Methods Programme, 22 SRs; that is, reviews included some trials in practice setting relating to smoking cessation
© EBD 2022 3
© The Author(s), under exclusive licence to British Dental Association 2022SYSTEMATIC REVIEW
Table 1 Best practice (high-quality) evidence for smoking cessation and alcohol reduction interventions in the systematic
reviews (SRs) in the dental practice setting
Dental practice setting
Preventive interventions for smoking Strength of SRs Preventive interventions Strength of SRs
evidence supporting for alcohol evidence supporting
(based on evidence (based on evidence
effect size) effect size)
Ask/ Use patient’s charts, medical records or health Weak SR 12 None
assess questionnaires to determine tobacco use status
and at-risk groups
Record findings from oral examination and Strong SR 12
relate to patient’s tobacco use
Advise/ Brief (or very brief) behavioural advice > no Strong SR 12 None
arrange intervention
Personalised (tailored) feedback from the oral Strong SR 12
examination as to the oral effects of tobacco use
Intensive intervention > brief intervention Weak SR 12
Effectiveness of interventions delivered by trained None SR 12
professionals (effect sizes not reported)
Assist/ Brief advice plus quit-line referral > simple brief Weak SR 12 None
referral advice to quit (only one trial reported 3.3% quit rate)
Table 2 Best practice (high-quality) evidence for smoking cessation and alcohol reduction interventions in the systematic
and no reviews
reviews (SRs) at
in all
theon alcoholpractice
medical reduction. However, best practice recommendations
setting have been developed from synthesising
Medical practice setting
Preventive interventions for smoking Strength of SRs Preventive interventions for Strength of SRs
evidence supporting alcohol evidence supporting
(based on evidence (based on evidence
effect size) effect size)
Ask/ Assess and record patient’s smoking Strong SR: 1, 2, 6, Assess and record patient’s alcohol Strong SR: 7, 11,
assess status 7, 8, 10, consumption levels (moderate 17, 22, 25
16, 24, 27 or dependence), using validated
Details of smoking assessment; for None
screening tools to determine
example, duration, frequency, or type
treatment options
(cigarette, cigar, pipe)
Advise/ Theory-based or structured Strong SR: 1, 2, 7, Behavioural interventions (face-to- Strong SR: 7, 11,
arrange interventions > simple advice or 8, 16, 24, face tailored advice/counselling) > no 17, 22, 25
message to quit 27 intervention or usual care
Brief (or very brief) motivational Strong SR: 1, 2, 6, Brief (5–20 minutes) Strong SR: 11, 17,
interventions > no intervention 7, 8, 10, interventions > no intervention or 22
16, 24, 27 very brief or intensive intervention
Intensive interventions (more than 20 Moderate SR: 1, 6, Multiple sessions > single sessions Strong SR: 11, 17
minutes) > brief interventions (small 7, 8
but significant benefit)
Single sessions > multiple sessions Strong SR: 1, 7, 8 Intensive (more than 20 Weak SR 11
minutes) > brief intervention
Physician > nurses or counsellors Weak SR: 1 Very brief (less than five Weak SR 11
(reported in only two small trials) minutes) > brief intervention
Training received by providers > no None N/A Primary care providers (physician, Strong SR: 11
training (effects not reported) nurses, health educator) > research
personnel
Effectiveness of additional components: None Training received by providers > no None N/A
written materials or self-help aids (effect training (effects not reported)
sizes not reported)
Additional components to support None
written materials or self-help
manuals (effects not reported)
Assist Brief advice (3–5 minutes) plus referral Weak SR 8 Referral to specialised treatment None N/A
(referral) to cessation services > brief advice only services (outcomes for effectiveness
(effect sizes not reported) not reported)
4 © EBD 2022
© The Author(s), under exclusive licence to British Dental Association 2022SYSTEMATIC REVIEW
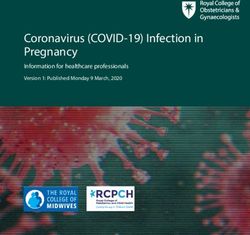
Fig. 3 PRISMA four-phase flow diagram for included clinical guidelines incorporated into clinical practice, however,
behavioural counselling (typically brief) in
Records identified through database conjunction with an oral examination was
searching (nGC = 2477) a consistent intervention component that
Identification
was also provided in some control groups’.
The nine high-quality medical practice
Records after duplicates Additional records identified reviews show that theory-based ‘brief’
removed through website searches
(nCG = 2381) (nCG = 12) interventions (motivational interviewing
in particular) delivered by primary care
professionals in a single session, following
an assessment of a patient’s smoking status,
Titles screened Records excluded are effective (compared to no intervention
(nCG = 2393) (n = 1906)
or simple advice) in increasing smoking
Screening
cessation rates. The lack of precise reporting
of intervention duration and number of
Abstracts screened Records excluded sessions (brief intervention described as 5–20
(nCG = 487) (n = 428) minutes) somewhat limited the inferences
regarding duration of sessions that can be
drawn. It was reported that although longer
Full-text articles assessed Records excluded interventions (10–20 minutes) were more
for eligibility (n = 32) effective in increasing quit rates, even very
(nCG = 59) 12 Wrong setting
Eligibility
brief interventions of as little as two minutes
8 Treatment or
management CG have also been shown to be effective (RR
6 Wrong intervention 1.66, 95% CI 1.42 to 1.94). There was a
2 Wrong study design small additional benefit of more intensive
2 Summary documents
(included full CG) interventions (more than 20 minutes, and
1 Practice/Professional more than one follow-up visit) compared
focussed to brief (or very brief) interventions (RR
1.37, 95% CI 1.20 to 1.56). Interventions
were reported to be effective if delivered by
Included
a primary care professional with minimal
Studies included in narrative synthesis training in theory-based approaches;
(n = 27; 2 CGs combined together as one document) however, effect sizes were not reported
(nCG = 26)
to compare interventions delivered by
professionals without training. Moreover,
the exact training characteristics to deliver
the best evidence from other primary care interventions delivered by trained dental the intervention require better reporting
(medical/pharmacy) settings, which could professionals incorporating an oral and clarification by future researchers.
be adapted/adopted for dental practice, examination component (compared to no Additional components (that is, written
along with synthesising the best-quality intervention or usual care) in increasing materials, self-help aids) were reported to
available guidance (discussed later). There tobacco abstinence rates for at least six support behavioural advice; however, again,
were 13 high-quality reviews (SR: 1, 2, 6, 7, months (OR = 1.71, 95% CI 1.44, 2.03; effect sizes were not reported to compare
8, 10, 11, 16, 17, 22, 24, 25, 27) of preventive n = 14 trials) among cigarette smokers and interventions ‘with’ versus ‘without’
interventions delivered in a primary care smokeless tobacco users. The effect was supporting materials. Furthermore, this
medical or community pharmacy setting. stronger in the adult smokers (OR = 2.38, overview shows a lack of trials reporting
Of these, eight SRs included trials/studies 95% CI 1.70, 3.35; n = 5 trials) compared effect sizes for referral pathway compared
with preventive interventions solely for to smokeless tobacco users (OR = 1.70, with behavioural advice for smoking
smoking (SR: 1, 2, 6, 8, 10, 16, 24, 27), four 95% CI 1.36, 2.11; n = 6 trials). Though cessation in primary care settings.
reviews included studies with preventive the review showed no additional benefit All high-quality SRs for reducing alcohol
interventions for alcohol only (SR: 11, 17, 22, of intensive intervention (gauged by consumption established that brief (10–
25), while one review (SR 7) included studies number of personal contact) over brief 15 minutes) multi-contact (two or more
delivering preventive interventions for both intervention, there was a lack of reporting follow-up visits over a year) motivational
smoking and alcohol separately; none of the of effect sizes comparing both. The dental interventions were most effective
studies included combined interventions review (SR 12) concluded that: ‘Differences (consumption decreased by 3.6 drinks per
targeting both smoking and alcohol. between the studies limit the ability to make week from baseline; 95% CI, 2.4 to 4.8
The dental review (SR 12) demonstrated conclusive recommendations regarding the drinks/week) (SR 11); interventions of up to
the effectiveness of brief (or very brief) intervention components that should be five minutes’ duration were also reported to
© EBD 2022 5
© The Author(s), under exclusive licence to British Dental Association 2022SYSTEMATIC REVIEW
Table 3 Best practice (high-quality) recommendations for smoking cessation and alcohol reduction interventions in the
clinical guidelines (CGs) in the dental practice setting
Dental practice setting
Preventive interventions for Strength of CGs supporting Preventive Strength of CGs supporting
smoking recommendation recommendation interventions for recommendation recommendation
(based on alcohol (based on
supported supported
evidence) evidence)
Ask/assess Ask and record Strong CG 11 Ask, assess and record Weak CG 11
patient’s smoking patient’s average
(or tobacco use) daily/weekly alcohol
status as part of consumption as part of
social history social history
Assess patient’s risk Strong CG 11 Use shorter versions of Weak CG 11
levels, and their validated screening tools
interest in stopping (AUDIT-PC, FAST)
smoking
Advise/ Offer brief or very Strong CG 11 Very brief advice – outline Weak CG 11
arrange brief opportunistic the possible harmful
interventions effects of excessive
alcohol consumption
Brief interventions Strong CG 11 (no details provided;
should be tailored eg duration, number of
to meet individual sessions, training)
needs
Advice supported Weak CG 11
with educational
materials or online
support
Assist/ Offer smokers (or Weak CG 11 Refer patients to general Weak CG 11
referral tobacco users) medical practitioner for
‘Smokeline’ further advice and help
numbers or
information on Provide online support Weak CG 11
local smoking (eg visit ‘Alcohol Focus
cessation services Scotland’ website)
be effective in equally higher-quality review specialist services would be more effective in this overview (SR: 1, 6, 8, 12, 16, 27). A list
(mean difference: -38 grams/week, 95% CI: for ensuring patients attended or were of excluded guidelines (n = 32) was presented
-54 to -23) (SR 17). Intensive interventions followed up. with the reasons for exclusion (see online
were also reported to be effective; however, Lastly, this overview showed a lack of Supplementary Table S2).
where compared, the reported effect rates combined interventions for smoking and Included CGs were from different countries/
were smaller for intensive compared to alcohol (only isolated interventions were regions across the world: Australia, Europe,
brief interventions (non-significant; SR reported). India, New Zealand, United Kingdom and
11). There was little evidence for the United States. Online Supplementary Table
effectiveness of very brief (less than five Clinical guidelines S6 presents the various recommendations
minutes) interventions in reducing alcohol The search strategy retrieved 2,477 made about the assessment of major risk
consumption (5–8% increased abstinence in potentially relevant records through factors and delivering behavioural preventive
very brief versus 7–12% in brief intervention) database searches and 12 additional records interventions for each of the included CGs
(SR 11). were identified through organisation or (n = 26), along with target risk factors, and
The effective brief advice was supported health board website searches. All included target users for these guidelines.
by written materials or self-help manuals; records were screened (title and abstract), The quality of all included CGs was
however, comparison of intervention and of these, 59 records were selected for assessed using the AGREE II instrument
‘with’ and ‘without’ supporting materials full-text review. Finally, 26 clinical guidelines (see online Supplementary Table S7); there
was lacking. We found an overall lack of (CGs) were included in this overview (Fig. 3), were 11 high-quality guidelines (score 6 or
studies reporting on local referral pathways references to which are provided in online 7), 15 mid-quality guidelines (score ranged
for reducing alcohol consumption and their Supplementary Table S1. The reference lists from 3 to 5) and no low-quality guidelines
effectiveness compared to brief interventions of the included CGs were hand searched for (score 1 or 2). As with the SR synthesis, high-
or usual care (referral to specialist services any relevant CGs (and SRs) to be included quality recommendations are synthesised
was indicated in cases of alcohol dependence in this overview. Some of the referenced SRs here, with preference given to recentness
only). Also, there was limited evidence on (which met our inclusion criteria) in the of publication and the level of evidence
whether signposting or formally referring to included guidelines were already included for particular recommendations within
6 © EBD 2022
© The Author(s), under exclusive licence to British Dental Association 2022SYSTEMATIC REVIEW
Table 4 Best practice (high-quality) recommendations for smoking cessation and alcohol reduction interventions in the
clinical guidelines (CGs) in the medical practice setting
Medical practice setting
Preventive interventions for Strength of CGs supporting Preventive Strength of CGs supporting
smoking recommendation recommendation interventions for recommendation recommendation
(based on alcohol (based on
supported supported
evidence) evidence)
Ask/assess Ask and record Strong CG: 1, 2, 5, 12, Ask, assess, and Strong CG: 1, 14, 21
every patient’s 14, 17, 18, 22, 23 record patient’s
smoking (or alcohol consumption
tobacco use) levels (moderate or
status, and update dependence), using
regularly (at every validated screening tools
visit or at least – to determine treatment
annually) options
Assess nicotine Weak CG: 12, 18, 23
dependence (by
asking amount
smoked)
Assess readiness to Strong CG: 1, 2, 5, 12,
change and their 14, 17, 18, 22, 23
interest in receiving
further help
Advise/ Offer brief or Strong CG: 1, 5, 12, 14, Offer behavioural Strong CG: 1, 2, 14, 21
arrange very brief tailored 17, 18, 22, 23 (face-to-face) structured
intervention to interventions to all
increase tobacco patients with excessive
abstinence rates alcohol consumption
Intensive Moderate CG: 1, 5, 12, 18, Brief (10–15 minutes) Strong CG: 1, 14, 21
interventions (over 23 multi-contact (two
multiple sessions) or more sessions)
more effective than interventions were
brief intervention recommended to be
(small additional most effective
effect)
Educational Weak CG: 1, 5, 12, 18, Very brief intervention Weak CG: 1, 14
materials to 23 (less than five minutes)
support advice or intensive interventions
(more than 20 minutes)
Intervention Strong CG: 1, 2, 5, 12, Additional components Weak CG: 1, 2, 14, 21
delivered by any 14, 17, 18, 22, 23 to support advice:
member of the written information
primary care team or self-help materials,
goal-setting
Training received Weak CG: 14, 17, 18, Intervention delivered Strong CG: 1, 2, 14, 21
by providers to 22, 23 by any member of the
deliver effective primary care team
intervention
Behavioural Strong CG: 1, 5, 12, 18, Training received by Weak CG: 1, 2, 14, 21
advice plus 23 primary care providers
pharmacotherapy (evidence not reported
effective to to support effectiveness)
increase abstinence
rates
Assist/ Make referral to Strong CG: 12, 18, 23 Make referral to specialist Weak CG: 1, 14, 21
referral quit-line services alcohol treatment
(proactive services (for alcohol
support), as part of dependence)
brief intervention
high-quality guidelines. Data duplication while presenting findings. The key Of the 11 high-quality guidelines, there
(that is, previous guidelines or SRs [used for recommendations from high-quality CGs was only one guideline (CG 11) which
developing guidelines]) was also considered are presented in Tables 3 and 4. provided recommendations for delivering
© EBD 2022 7
© The Author(s), under exclusive licence to British Dental Association 2022SYSTEMATIC REVIEW
behavioural preventive interventions more, thus making it difficult to determine a primary care practice. In addition, high-
delivered exclusively in a primary a precise specification of the intervention quality reviews and guidelines in the dental
care dental setting. This guideline was duration. It is further recommended, if the practice setting were lacking with regards to
developed by the Scottish Dental Clinical patient is willing to quit, to make referral evidence of effectiveness of interventions
Effectiveness Programme (SDCEP) and to quit-line services (proactive support) for for reducing alcohol consumption. All the
met all criteria in AGREE II. This guidance further help, which were reported to be high-quality advice for alcohol came from
presented clear and consistent advice to effective along with brief intervention and the primary care medical practice settings.
support dental professionals to deliver pharmacotherapy to increase abstinence Thus, there is a need for more studies to
preventive interventions for both smoking rates (RR 1.29; 95% CI: 1.20–1.38). Thus, the evaluate the effectiveness of behavioural
(or smokeless tobacco) and alcohol (Tables recommendations seem to be much stronger alcohol interventions in a primary care
3 and 4). Overall, it is recommended that from CGs regarding referral to cessation dental practice setting.
practitioners record a patient’s smoking services than came through from SRs in the Overall, the integrated findings from
(or tobacco use) status as part of social medical practice setting. In addition, it is this overview identified that risk factor
history, assess patients’ risk levels and offer recommended that primary care providers assessment is an important first step in
very brief opportunistic advice (for a few support advice with feedback, written any prevention intervention (that is,
minutes). It is further recommended to materials and follow-up support; however, questions must be asked to assess the risk
offer information on ‘quit-lines’ or local again, there is no direct evidence to support levels or dependence). Regarding tobacco
‘stop smoking’ services. However, not all its effectiveness. cessation intervention, it was found that
recommendations made are supported by For alcohol reduction interventions an appropriate intervention would be to
research evidence. For alcohol, practitioners in primary care medical practice, the offer an in-person brief, motivational,
should assess a patient’s alcohol recommendation is that practitioners tailored intervention, delivered by dental
consumption (using screening tools), and ask, assess and record an adult patient’s professionals, in a single session, following
follow this with very brief advice/discussion alcohol use in the clinical records. Use of an assessment of a patient’s tobacco use
to outline and discuss the possible harmful validated screening tools (for example, status (risk levels) and incorporating an
effects of excessive alcohol consumption, AUDIT, AUDIT-C, CAGE) is recommended oral examination component. Although
and then recommend that patients visit for assessing alcohol risk levels. Following longer (10–20 minutes) and intensive (more
their general medical practitioner for alcohol risk assessment, a brief (10–15 than 20 minutes, with follow-up visits)
further advice and help. However, there is minutes) multi-contact intervention (two or interventions have shown to be effective
no research evidence reported to support more sessions) delivered by a trained provider in increasing quit rates compared to
these recommendations. Thus, further is most effective. Very brief interventions shorter interventions, very brief (less than
guidance is required (supported with of less than five minutes are also five minutes) interventions also showed
evidence) regarding delivering effective recommended, but the evidence reported is comparable effectiveness to the longer brief
behavioural alcohol intervention in a weaker compared to the longer interventions or intensive interventions.
dental practice setting. to support this recommendation. Where For alcohol drinkers, after assessing
The remaining ten high-quality guidelines needed (for example, if a patient is the patient’s alcohol use or dependence
(CG: 1, 2, 5, 12, 14, 17, 18, 21, 22, 23) included dependent on alcohol), referral to specialist (using validated screening tools), a brief
interventions delivered in a primary care alcohol treatment services is recommended. motivational, tailored intervention,
medical or community pharmacy setting Advice should be supported with written delivered by dental professionals, could
(Tables 3 and 4). Five of these guidelines materials, self-help materials and/or goal be offered to motivate alcohol users to
(CG: 17, 18, 21, 22, 23) also included setting. However, research evidence for the reduce consumption in a dental practice
dental professionals as their target users. latter is lacking. setting. A brief 10–15-minute multi-contact
For smoking cessation, it is recommended Again, as with SRs, none of the CGs intervention was the best recommended
to ask, assess and record a patient’s tobacco recommended offering combined intervention in medical practice reviews
use status in the clinical records, and offer interventions for tobacco and alcohol. and guidelines for helping alcohol users to
an opportunistic ‘brief’ tailored intervention reduce consumption; brief interventions of
to all smokers (or tobacco users) by a Data synthesis five minutes’ duration were also reported
trained primary care provider (although Most of the high-quality SR evidence and CG to be equally effective. Thus, very brief
no evidence to support effectiveness of recommendations were in accordance with (less than five minutes) or brief advice (of
training), to increase abstinence rates; with each other; that is, guidelines were based up to five minutes) should be trialled for
some guidelines recommending very brief on the review evidence (Tables 1, 2, 3 and tobacco and alcohol, respectively, in a dental
intervention – but this had little evidence 4). However, there were some areas where practice setting (considering feasibility and
base. Intensive interventions (more than 20 evidence and guidance were lacking; for effectiveness as reported in reviews and
minutes) have a small additional effect on example, there were no validated screening guidelines), tailored to patient motivational
quit rates (in line with SR evidence; Tables tools reported for assessing a patient’s status. Exploring use of the dental team is
1 and 2). Again, the duration of effective tobacco use status in all high-quality reviews supported, as effectiveness was generally
interventions recommended ranged from and guidelines. This has implications for independent of primary care provider (that
as little as 3 minutes to 20 minutes or even the use of tobacco risk assessment tools in is, general practice physician or nurse).
8 © EBD 2022
© The Author(s), under exclusive licence to British Dental Association 2022SYSTEMATIC REVIEW
Discussion dental practice setting. Moreover, studies included SRs, and duplication of guidelines
This study was novel in synthesising evidence have reported various barriers to the and reviews within all included CGs, was
from both SRs and CGs for undertaking a risk successful implementation of these brief addressed; that is, none of the findings were
factor assessment and delivering preventive interventions in a dental practice – some of synthesised twice, thus strengthening the
interventions for major behavioural risk the barriers reported in previous feasibility robustness of the overview synthesis.
factors associated with oral cancer (tobacco studies being: lack of knowledge, skills, One of the main study limitations
and alcohol). The overview went beyond the confidence and time, and even doubts about concerned the limited number of SRs in
review and trial evidence, and contributed the effectiveness of counselling.27,28,29,30 The the dental practice setting, which resulted
to the knowledge by developing a robust lack of evidence supporting the effectiveness in restrictions and in extrapolating findings
framework for integrated or combined of brief alcohol reduction interventions in from other settings (medical/pharmacy) to
evidence synthesis (narrative ‘thematic’) primary care dental practices, in comparison the dental practice setting. The heterogeneity
across these information sources, addressing to other primary care medical practice among study populations, settings and
review/guideline quality, recentness and settings, has been reported in other existing outcomes was explored as an integral part
duplication. Reported findings were based literature. 10,31,32
of data synthesis, but as this work was not
on a much greater body of research in As discussed in the study protocol, meta-analytic, a narrative synthesis approach
the primary care medical practice setting multiple risk factors need to be considered was used to address the applicability of
compared to the limited research undertaken for oral cancer prevention, as tobacco and findings across professional groups and/
in the dental practice setting. Informed by alcohol in combination magnifies the or patient behaviours. Interpretation and
the ADAPTE framework,25 which provides a risk for oral cancer. However, combined recommendations were limited by lack of
systematic approach to adapting guidelines interventions were almost completely consensus in definitions of brief, very brief
developed in one setting for use in another lacking in this overview. Other existing and intensive interventions. Additionally,
setting, the high-quality evidence and reviews and guidelines have also reported a there was limited information provided
recommendations in the primary care similar lack of evidence focusing on the most on many occasions regarding details of
medical/pharmacy setting in this overview effective approach to deal with multiple interventions covered.
were adapted to develop recommendations behaviours (for example, if someone smokes Furthermore, there was very limited
relevant to the dental practice setting. and consumes alcohol above recommended evidence available in terms of effect sizes for
This overview describes transferable best limits). 33,34 The question thus remains: some interventions that both the SRs and
practice from medical practice settings should these behaviours be approached CGs were to some extent recommending.
for dental professionals who interact with in sequence or in combination, and how This included referral to specialist services
smokers (or tobacco users) in the clinical should this be decided? Hence, further and the use of patient educational materials
setting. The results from another overview investigation is needed to address this large such as posters and leaflets. Thus, this
study by Ramseier and Suvan,10 which aimed gap in knowledge about the effectiveness of heterogeneity (and limited information)
to improve periodontal health, supports multifactorial or combined interventions, constrained the ability to make conclusive
these findings and shows the effectiveness incorporating both smoking and alcohol recommendations regarding which
of tobacco use cessation interventions in advice in a primary care setting, including components of behavioural preventive
the primary care dental practice. The effect dental practice. interventions should be incorporated into
size reported in the study by Ramseier and primary care practices.
Suvan10 was similar to that reported in Strengths and limitations
this overview (OR 2.38; 95% CI 1.70–3.35) This extensive overview involved a Conclusion
with regards to increased odds of quitting systematic literature search (international In conclusion, this overview shows a lack
tobacco. However, it failed to report the literature, no language restriction and grey of direct evidence from the dental practice
type of intervention, optimal length and literature search for CGs). The systematic setting (one high-quality SR relating to
frequency of interventions for effective search was not limited to ‘oral cancer’ and tobacco prevention and none relating
tobacco cessation, and showed a need for ‘dental setting’; thus, the overview did not to alcohol). However, relatively strong
further research in this field.10 A similar lack rule out good guidelines and/or evidence evidence and recommendations from
of dental evidence was reported in reviews on how to assess risk and deliver prevention other primary care (medical/pharmacy)
and guidelines included in this overview for tobacco/alcohol, which may be aimed settings were identified and synthesised,
study; that is, insufficient number of studies at another clinical/medical condition which could potentially be adapted and
to determine the specific support measures (for example, lung cancer, periodontal adopted by dental professionals. Thus,
delivered by dental professionals to provide or cardiovascular disease).18,35,36 A robust very brief or brief advice of up to five
an increased effectiveness beyond brief quality appraisal was carried out to assess minutes should be trialled for tobacco and
advice.9,18 the methodological quality of included alcohol respectively in a dental practice
Dental professionals are in an ideal SRs (AMSTAR and ROBIS) and CGs (AGREE setting, after risk assessment tailored to
position to provide brief alcohol advice to II) independently by two reviewers, and patient motivational status. Exploring
their patients. Despite this opportunity, discrepancies discussed with the wider team. delivery by the dental team is supported,
there is a lack of studies developing and This helped to ensure the rigour of findings. as effectiveness was generally independent
evaluating alcohol brief interventions in a Moreover, the duplication of trials in all of primary care provider.
© EBD 2022 9
© The Author(s), under exclusive licence to British Dental Association 2022SYSTEMATIC REVIEW
Ethics declaration 6. International Agency for Research on Cancer. IARC Programme. 2006. Available at https://www.
monographs on the evaluation of carcinogenic risks to lancaster.ac.uk/media/lancaster-university/
The authors declare that they have no competing humans – Volume 96: Alcoholic drinking. Lyon: World content-assets/documents/fhm/dhr/chir/
interests. Health Organisation, 2007. NSsynthesisguidanceVersion1-April2006.pdf
7. Sheiham A, Watt R G. The common risk factor (accessed November 2021).
approach: a rational basis for promoting oral health. 23. CRD. Systematic reviews: CRD’s guidance for undertaking
Community Dent Oral Epidemiol 2000; 28: 399–406. reviews in health care. York: University of York NHS
Author contributions 8. Petersen P E. Oral cancer prevention and control–the Centre for Reviews and Dissemination, 2009.
SM wrote the first draft of the manuscript, with approach of the World Health Organisation. Oral 24. Petticrew M, Roberts H. Systematic reviews in the
Oncol 2009; 45: 454–460. social sciences: a practical guide. Oxford: Blackwell
feedback from other authors. SM, AJR, DIC 9. Carr A B, Ebbert J. Interventions for tobacco Publishing, 2008.
and LMDM participated in the study design, cessation in the dental setting. Cochrane Database 25. ADAPTE Collaboration. The ADAPTE process:
Syst Rev 2012; DOI: 10.1002/14651858.CD005084. resource toolkit for guideline adaptation (version
development, refinement of the methodological pub3. 2.0). 2009. Available at https://g-i-n.net/
10. Ramseier C A, Suvan J E. Behaviour change wp-content/uploads/2021/03/ADAPTE-Resource-
approach, quality appraisal and synthesis. All counselling for tobacco use cessation and promotion toolkit-March-2010.pdf (accessed November
authors contributed to revising the manuscript, of healthy lifestyles: a systematic review. J Clin 2021).
Periodontol 2015; 42 Suppl 16: S47–S58. 26. Dijkers M. Duplicate publications and systematic
and all authors read and approved the final 11. Grol R, Grimshaw J. From best evidence to best reviews: problems and proposals. 2018. Available
manuscript. practice: effective implementation of change in at https://ktdrr.org/products/update/v6n2/dijkers_
patients’ care. Lancet 2003; 362: 1225–1230. ktupdate_v6n2-508.pdf (accessed November
12. Kaner E F S, Dickinson H O, Beyer F R et al. 2021).
Effectiveness of brief alcohol interventions in primary 27. Macpherson L M D, McCann M F, Gibson J, Binnie
Funding information care populations. Cochrane Database Syst Rev 2009; V I, Stephen K W. The role of primary healthcare
The project has received funding from NHS DOI: 10.1002/14651858.CD004148.pub3. professionals in oral cancer prevention and
13. Lindson-Hawley N, Thompson Tom P, Begh detection. Br Dent J 2003; 195: 277–281.
Education for Scotland and the Glasgow Dental R. Motivational interviewing for smoking 28. Shepherd S, Young L, Clarkson J E, Bonetti D, Ogden
Educational Trust. cessation. Cochrane Database Syst Rev 2015; DOI: G R. General dental practitioner views on providing
10.1002/14651858.CD006936.pub3. alcohol related health advice: an exploratory study.
14. World Health Organisation. WHO framework Br Dent J 2010; 208: 5.
convention on tobacco control: report of the first 29. Amemori M, Michie S, Korhonen T, Murtomaa
Acknowledgements
sub-regional awareness raising workshop: Kathmandu, H, Kinnunen T H. Assessing implementation
The study is ethically approved by the University Nepal, 18–19 March 2004. Regional Office for South difficulties in tobacco use prevention and cessation
East Asia: World Health Organisation, 2004. counselling among dental providers. Implement Sci
of Glasgow College of Medical, Veterinary & 15. World Health Organisation. Public health problems 2011; 6: 50.
Life Sciences Ethics Committee. We gratefully caused by harmful use of alcohol: Report by the 30. Yusuf H, Tsakos G, Ntouva A et al. Differences by age
Secretariat. Geneva: World Health Organisation, and sex in general dental practitioners’ knowledge,
acknowledge the input and feedback provided 2005. attitudes and behaviours in delivering prevention.
16. Mathur S, Conway D I, Worlledge-Andrew H, Br Dent J 2015; 219: E7.
by John Gibson, Andrea Sherriff, Heather
Macpherson L M D, Ross A J. Assessment and 31. Dyer T A, Robinson P G. General health promotion
Worlledge-Andrew and Naeema Al-Balushi. prevention of behavioural and social risk factors in general dental practice – the involvement of the
associated with oral cancer: protocol for a systematic dental team. Part 1: a review of the evidence of
The views expressed are those of the authors and review of clinical guidelines and systematic reviews effectiveness of brief public health interventions.
not necessarily those of any of the funders or to inform Primary Care dental professionals. Syst Rev Br Dent J 2006; 200: 679–685.
2015; 4: 1. 32. McAuley A, Goodall C A, Ogden G R, Shepherd
organisations they represent. Systematic review 17. Moher D, Liberati A, Tetzlaff J, Altman D G. Preferred S, Cruikshank K. Delivering alcohol screening and
reporting items for systematic reviews and meta- alcohol brief interventions within general dental
registration: PROSPERO CRD42015025289.
analyses: the PRISMA statement. Ann Intern Med practice: rationale and overview of the evidence.
2009; 151: 264–269. Br Dent J 2011; 210: E15.
18. SDCEP. Prevention and treatment of periodontal 33. Goldstein M G, Whitlock E P, DePue J. Multiple
References diseases in primary care: Dental Clinical Guidance. behavioural risk factor interventions in primary care.
1. Shield K D, Ferlay J, Jemal A et al. The global Dundee: Scottish Dental Clinical Effectiveness Summary of research evidence. Am J Prev Med 2004;
incidence of lip, oral cavity, and pharyngeal cancers Programme, 2014. 27(2 Suppl): 61–79.
by subsite in 2012. CA Cancer J Clin 2017; 67: 51–64. 19. Shea B J, Grimshaw J M, Wells G A et al. 34. National Institute for Health and Care Excellence.
2. Conway D I, Purkayastha M, Chestnutt I G. The Development of AMSTAR: a measurement tool to Behaviour change: individual approaches. 2014.
changing epidemiology of oral cancer: definitions, assess the methodological quality of systematic Available at https://www.nice.org.uk/guidance/
trends, and risk factors. Br Dent J 2018; 225: 867. reviews. BMC Med Res Methodol 2007; 7: 10. ph49/resources/behaviour-change-individual-
3. Winn D, Lee Y C, Hashibe M, Boffetta P. 20. Whiting P, Savović J, Higgins J P et al. ROBIS: a new approaches-pdf-1996366337989 (accessed
The INHANCE consortium: toward a better tool to assess risk of bias in systematic reviews was November 2021).
understanding of the causes and mechanisms of developed. J Clin Epidemiol 2016; 69: 225–234. 35. Fiore M C, Jaen C R, Baker T B et al. Treating tobacco
head and neck cancer. Oral Dis 2015; 21: 685–693. 21. AGREE Next Steps Consortium. The AGREE II use and dependence: 2008 update. Rockville (MD):
4. Gillison M L, Chaturvedi A K, Anderson W F, Fakhry instrument (electronic version). 2009. Available US Department of Health and Human Services,
C. Epidemiology of human papillomavirus–positive at https://www.agreetrust.org/wp-content/ 2008.
head and neck squamous cell carcinoma. J Clin Oncol uploads/2013/10/AGREE-II-Users-Manual-and-23- 36. National Institute for Health and Care Excellence.
2015; 33: 3235. item-Instrument_2009_UPDATE_2013.pdf (accessed Alcohol-use disorders: preventing harmful drinking.
5. IARC. International Agency for Research on Cancer November 2021). 2014. Available at https://www.nice.org.uk/
working group on the evaluation of carcinogenic risks to 22. Popay J, Roberts H, Sowden A et al. Guidance on guidance/ph24/evidence/alcoholuse-disorders-
humans. Tobacco smoke and involuntary smoking v.83. the conduct of narrative synthesis in systematic preventing-harmful-drinking-evidence-update-
Lyon: World Health Organisation, 2004. reviews: A product from the ESRC Methods pdf-67327165 (accessed November 2021).
10 © EBD 2022
© The Author(s), under exclusive licence to British Dental Association 2022You can also read