Sunday Poster Presentations Session Category Parenteral Nutrition - American Society for ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Sunday Poster Presentations
Session Category
Parenteral Nutrition
S1 - The Association between a Four-Oil Lipid Emulsion and Parenteral Nutrition Associated Liver
Disease-Related Laboratory Values in Adult Patients Receiving Home Parenteral Nutrition.
Heather Stanner, RD, LDN, CNSC; Kristy Feeney, MS, RD, CNSC; Karen M. Sexton-Hamilton, MS, RD,
LDN, CNSC; Nicolette Burzawa, RD, LDN, CNSC; Kasia Ciaston, MS, RD, LDN, CNSC; Andrew
McArthur, MS, RD, CSSD, LDN, CNSC, FAND; Laura Trento, MS, RD, CNSC; Amy Tung, MS, RD,
CNSC; Andrea Marigold, RD, CNSC
Nutrition, Coram CVS Specialty Infusion, Denver, CO
Purpose: Home parenteral nutrition (HPN) is recommended for patients who are unable to meet their
nutrition needs through an oral or enteral route. HPN includes lipid injectable emulsions (ILE) as a
macronutrient component. Traditional ILE include those composed of soybean oil, a source of essential
fatty acids that prevents essential fatty acid deficiency (EFAD). The pro-inflammatory nature of soybean
oil is a potential factor in parenteral nutrition associated liver disease (PNALD) development. 1 An ILE
containing four types of oils (soybean oil, medium-chain triglycerides [coconut oil], olive and fish oil) is
now approved for use as a calorie and fatty acid source.2 Studies in HPN patients have shown mixed
results with regard to changes in liver function tests and fatty acid profiles while receiving a four-oil ILE.3-
5 The purpose of this study was to evaluate the association between a four-oil lipid emulsion and PNALD-
related laboratory values in adult HPN patients with baseline abnormal liver function tests.
Methods: Twelve branches of a large home infusion pharmacy in nine states were selected as study
sites. Eligible subjects included adult HPN patients with baseline abnormal alkaline phosphatase (ALP),
aspartate aminotransferase (AST), alanine aminotransferase (ALT) or total bilirubin (T bili) and receiving a
four-oil ILE (Smoflipid®). One of these values was required to be at least 1.5 times the high normal limit.
Seventy-seven adult patients were enrolled in the study. Sixty-two (80.5%) of these patients were
receiving a soybean oil-based ILE prior to starting a four-oil ILE. Data were retrospectively collected at the
following time points: Baseline, 1 Month, 2 Months, 3 Months, 6 Months and 12 Months. Laboratory
sampling coincided with the patients’ routine lab monitoring and included ALP, ALT, AST, T bili,
triglycerides (TG) and triene: tetraene ratio. Reports of physical manifestations of EFAD were also
collected. Primary outcome measures were changes between time points in ALP, ALT, AST, and T bili.
Secondary outcome measures included changes in TG and EFAD manifestation between time points.
Results: Baseline characteristics are listed in Table 1. Kruskal-Wallis tests and post hoc Mann-Whitney U
tests were used to detect changes in ALT, AST, ALP, T bili and TG levels between time points. Overall,
ALT, AST, ALP, T bili and TG decreased from Baseline to Month 12 time points with several statistically
significant decreases (see Table 2). A statistically significant decrease in ALT and AST was first detected
between Baseline and Month 1 time points, and a statistically significant decrease in ALP was first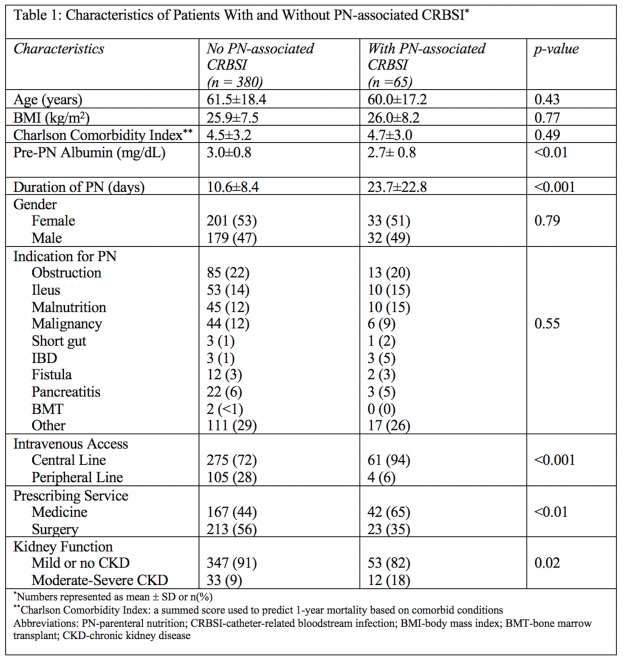
detected between Baseline and Month 2 time points. ALT, AST and ALP all showed statistically significant decreases between Baseline and Month 12 time points. There were two reports of physical manifestations of EFAD (dry, flaky skin) at the Baseline (n=1) and Month 1 time point (n=1) in the same patient. Of note, this patient had been receiving a soybean oil-based ILE prior to changing to a four-oil ILE. No triene:tetraene ratio results were reported for any subject at any time point. Conclusions: Use of a four-oil ILE is associated with a clinically and statistically significant decrease in ALT and AST in adult HPN patients with baseline abnormal liver function tests. Clinical significance is supported by the return from abnormal ALT and AST values at Baseline to a normal reference range at the Month 1 time point. There were also statistically significant decreases in ALP, but median Baseline values were within normal range. Overall, the use of a four-oil ILE may provide benefit over traditional ILE in adult HPN patients with PNALD-related laboratory values. Financial Support received from: N/A

S2 - Parenteral Nutrition is Associated with Increased Catheter-Related Blood Stream Infections in Patients Admitted to Medical Services Rachel Eklund, RD1,2; Olga Aroniadis, MD, MS1; Jennifer Katz, MD1 1Montefiore Medical Center, Bronx, NY; 2Albert Einstein College of Medicine, Bronx, NY Purpose: Parenteral nutrition (PN) is associated with an increased risk for bloodstream infections. The aim of this study was to identify risk factors associated with catheter-related bloodstream infections (CRBSI) in patients receiving PN through peripheral or central venous catheters in a 1491 bed tertiary hospital system. Methods: Our cohort included all adult inpatients hospitalized at Montefiore Medical Center between July 1, 2016 and December 31, 2017 who were started on PN during their admission. In-depth chart review was performed to obtain data on patient characteristics, including demographic factors and comorbidities,

indication for and duration of PN, and prescribing service (medicine vs. surgery). Cases of CRBSI were identified. Bivariate analyses and logistic regression were used to identify risk factors for PN-associated CRBSI. Results: 65 (14.6%) PN-associated CRBSIs (11.7 CRBSI per 1000 days of PN) were identified among 445 new PN prescriptions. There were no significant differences in age and Charlson comorbidity index between patients with and without PN-associated CRBSI (Table 1). Comparison of additional patient characteristics and risk factors between groups with and without PN-associated CRBSI are depicted in Table 1. After adjusting for age and gender, central venous access vs. peripheral access (OR 3.48; 95% CI 1.17-10.35), moderate-severe chronic kidney disease vs. mild or no kidney disease (OR 2.49; 95% CI 1.09-5.67), medical vs. surgical admitting service (OR 2.03; 95% CI 1.12-3.67) and longer duration of PN (OR 1.06; 95% CI 1.04-1.09) were statistically significantly associated with PN-associated CRBSI (Table 2). Conclusions: Similar to prior studies, we found that central venous catheters, chronic kidney disease, and longer PN duration are risk factors associated with bloodstream infections. In our cohort, we also identified a new association between medical admitting service and increased risk for PN-associated CRBSI. This could indicate important differences in PN management between medical and surgical services and requires further investigation. Financial Support received from: N/A


S3 - Home Initiated Parenteral Nutrition is a Safe and Cost-Effective Approach to Nutrition Support Jamie Haselhorst, RDN, LD2; Rebecca L. Brown, RDN, CNSC2; Casey Cooper, PharmD, CNSC1; Diana Ogden, RDN2; Shannon Slate, PharmD, CNSC1; Debbie Stevenson, MS, RDN2 1Pharmacy, Amerita Specialty Infusion Services, Amarillo, TX; 2Nutrition Support Services, Amerita Specialty Infusion Services, San Antonio, TX Purpose: Home initiation of parenteral nutrition (PN) has been a successful practice for over 20 years. Request for home start PN has increased to prevent initial hospitalization, prevent hospital readmissions, reduce costs and decrease the risk of hospital-acquired infection. However, some healthcare teams are not comfortable initiating PN in the home setting. The principal concern is related to patient safety and the risk of refeeding syndrome. Therefore, the primary purpose of this retrospective study is to evaluate the safety and efficacy of home start PN. With the increasing costs associated with the provision of healthcare today, a cost-analysis is also an important secondary factor to consider. Methods: The retrospective study design was approved by the Amerita clinical compliance team. Protected health information was not included, and informed consent was not required. A retrospective chart review was conducted on adult men and women > 18 years of age that started on home PN at the above home infusion pharmacy between 6/1/2017 and 6/30/2018. Individuals were excluded when therapy was less than 30 days. Data collected included the occurrence of hospitalizations, ER visits, central venous access device events (CVAD) and Adverse Drug Reactions (ADRs) over the first 30 days of therapy. Incidence of refeeding syndrome was determined for the home initiated PN patients, with refeeding defined as a decrease in electrolytes (potassium, phosphorus and magnesium) below normal limits following initiation of PN. Clinical judgment was exercised where individuals had increased fluid losses and low electrolytes that were not a result of refeeding. The number of days it took home start PN patients to reach caloric goal, defined as goal calories outlined in the initial nutrition assessment, was obtained. The sample groups were analyzed using a two-sample t-test (assuming equal variances) with one-tailed P values to demonstrate statistical significance. Results: 62 home start PN patients met selection criteria. 62 additional patients from the same geographical locations who started PN during the same timeframe in the hospital setting were randomly selected to constitute a matched control group. A statistically significant (P

PN patient was 9.7 days (Table 1).
Conclusions: Patients with home initiated PN had fewer hospital admissions after starting therapy than
hospital start PN. Home start PN vs. hospital initiated PN provides a cost savings of approximately $2000
per day (Fig 2). Additionally, starting PN in the home setting reduces exposure to hospital acquired
infections in nutritionally compromised patients. Refeeding risk remains a concern when initiating PN in
the home, but with close monitoring, significant adverse events can be prevented. Hospital start PN does
allow for closer monitoring of labs and average days to goal is half that of a home initiated PN. However,
home start PN is a safe alternative and should be considered given the cost savings, fewer readmissions,
and preventing hospital-acquired infections.
Financial Support received from: N/A
Table 1 - Outcome Incidence rates and additional data, Home Start PN vs. Hospital Start PN
# ER # CVAD
N # Hosp. # ADRs # Days to # RF % RF
visits events
= (30d) (30d) Goal Syndrome Syndrome
(30d) (30d)
Study Arm (Home
62 7 4 3 5 9.71 7 11.11%
Starts)
Comparator Arm
62 17 2 6 8 xxxxxxx xxxxxxx xxxxxxx
(Hospital Starts)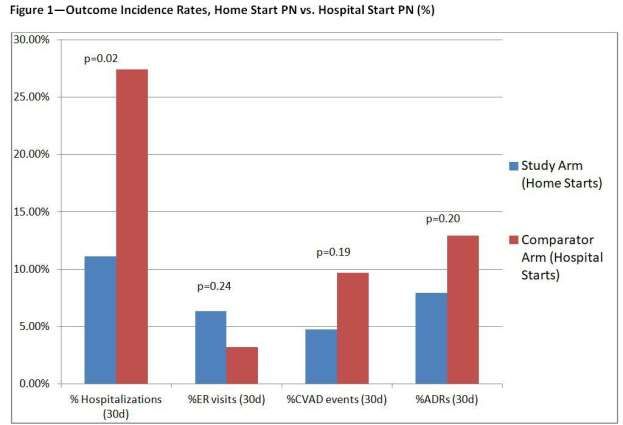
S4 - Effect of intravenous amino acid shortages on parenteral nutrition ordering practices in adult inpatients Diana W. Mulherin, PharmD, BCNSP; David P. Mulherin, PharmD, BCPS; Douglas L. Seidner, MD, AGAF, FACG, FASPEN, CNSC Vanderbilt University Medical Center, Nashville, TN Purpose: A nationwide shortage of intravenous amino acid (IV AA) products from 2017 - 2018 resulted in significant practice changes for parenteral nutrition (PN) formulations in the adult population of a large, academic medical center due to varying product availability. During this time, a multidisciplinary task force was formed to decide on prescribing strategies to help maintain product (Table 1). Several different IV AA products were used throughout this time period with different AA concentrations which resulted in a shift from our standard of practice. The purpose of this study is to describe the amino acid doses received from PN during the shortage and non-shortage time frames. Secondary outcomes include PN dextrose doses and volume in patients receiving PN during these times. Methods: Charts of patients who received PN during the shortage time frame (12/2017 – 3/2018) and a similar non-shortage time frame (12/2016-3/2017) were retrospectively reviewed for demographic information and PN formula information. Peripheral PN formulations were excluded. Protein doses were compared between shortage and non-shortage time frames. Dextrose and volume doses were also compared between groups. Student’s t-tests and Chi-square or Fisher’s exact tests were used to compare continuous and categorical variables, respectively. Results: Four hundred thirty-five patients received PN during the study time periods (pre-shortage n=233, shortage n=202). Baseline demographics were similar between pre-shortage and shortage groups with the exception of BMI (26.8 vs. 25, p=0.016), ICU status (44 vs. 71%, p

in maintenance of IV AA stock, it is unknown whether negative outcomes resulted in this clinically and
statistically significant reduction in prescribed protein. Continued focus should be placed on the clinical
implication of PN product shortages and prevention of these shortages.
Financial Support received from: N/A
Table 1. Protein shortage dosing for parenteral nutrition
Type of patient Longterm/HPN/unstressed Underweight BMI > 25 Critically ill
■ Protein dose 1.2
■ Protein dose - 1.5 g/kg/day for
1g/kg/day most ICU patients
■ ILE 2-3x/week, ■ Protein dose 2
consider daily fat g/kg/day for obese,
■ Protein dose
to meet kcal CRRT, open
1g/kg/day
requirements if abdomen, high
Approach to ■ Protein dose 1g/kg/day ■ ILE 2x/week
needed output fistula
initial ■ ILE 2-3x/week ■ Dextrose to
■ Increase kcal ■ Consider four-oil
macronutrient ■ Use dextrose to make up make up
every 4 days for ILE daily to meet
goals remaining kcal remaining kcal
weight gain EFA requirements
for total of 25
■ Ambulatory ■ Dextrose to
kcal/kg/day
patients with low make up remaining
to normal BMI - kcal
target 30-35 ■ Once stress level
kcal/kg/day is reduced, target
25-30 kcal/kg/day
■ Patients with partial GI function without significant tube feeding or oral intolerance
should have protein supplementation ordered to meet protein requirements outside of
the PN formula
■ Re-assess protein and energy needs weekly at minimum
Other
■ Document in initial consult note that protein goal is reduced because of amino acid
considerations
shortage
■ For patients with anticipated transition from PN to EN/PO, contact primary team
daily if PN is to be continued to ensure PN orders are not discontinued by primary
service and PN bags are not wasted
Table 2. PN prescription differences between study periods
Pre-shortage (n=233) Shortage (n=202) p-value
Cumulative grams of protein received per patient 832 ± 608 552.7 ± 608.1 0.004
Grams of protein per order 104 ± 23.6 76.7 ± 25.2Kristy Feeney, MS, RD, CNSC; Heather Stanner, RD, LDN, CNSC; Karen M. Sexton-Hamilton, MS, RD, LDN, CNSC; Jessi McCarroll, MBA, RD, CNSC; Katie Kelly, MS, RD, CNSC; RaLyn Lasley, MS, RD, CNSC, LD; Charmagne K. Emelue, MS, RD, LD, CNSC Nutrition, Coram CVS Specialty Infusion, Denver, CO Purpose: Home parenteral nutrition (HPN) is recommended for patients who are unable to meet their nutrition needs through an oral or enteral route. HPN includes lipid injectable emulsions (ILE) as a macronutrient component, traditionally composed of soybean oil. The pro-inflammatory nature of soybean oil is a potential factor in parenteral nutrition associated liver disease (PNALD) development, the most frequent complication of long-term PN.1,2 The incidence of liver disease may be up to 50% in infants receiving PN for two months, and up to 90% in premature infants receiving PN for more than three months.3 Because of the high risk of PNALD development in pediatric HPN patients, further study of an ILE containing four types of oils (soybean oil, medium-chain triglycerides [coconut oil], olive and fish oil) and its association with PNALD-related lab values is warranted.4 The purpose of this study was to evaluate the association between a four-oil lipid emulsion and PNALD-related laboratory values in pediatric patients with baseline abnormal liver function tests. Methods: Six branches of a large home infusion pharmacy in five states were selected as study sites. Eligible subjects included pediatric HPN patients with baseline abnormal alkaline phosphatase (ALP), aspartate aminotransferase (AST), alanine aminotransferase (ALT) or total bilirubin (T bili) and receiving a four-oil ILE (Smoflipid®). One of these values was required to be at least 1.5 times the high normal limit. Seventeen patients were enrolled in the study. Twelve (70.6%) of these patients were receiving a soybean oil-based ILE or a combination of fish oil- and soybean oil-based ILE prior to starting a four-oil ILE. Data were retrospectively collected at the following time points: Baseline, 1 Month, 2 Months, 3 Months, 6 Months and 12 Months. Laboratory sampling coincided with the patients’ routine lab monitoring and included ALP, ALT, AST, T bili, triglycerides (TG) and triene: tetraene ratio. Reports of physical manifestations of essential fatty acid deficiency (EFAD) were also collected. Primary outcome measures were changes between time points in ALP, ALT, AST, and T bili. Secondary outcome measures included changes in TG and EFAD manifestation between time points. Results: Baseline characteristics are listed in Table 1. Kruskal-Wallis tests and post hoc Mann-Whitney U tests were used to detect changes in ALT, AST, ALP, T bili and TG levels between time points. Overall, ALT, AST, ALP, T bili and TG decreased from Baseline to 12 Month time points with several statistically significant decreases (see Table 2). A statistically significant decrease in ALT, AST and T bili was first detected between Baseline and Month 3 time points. T bili returned to the normal range at the Month 3 time point, and ALT and AST returned to normal range by the Month 12 time point. AST, ALT and T bili all showed statistically significant decreases from Baseline to Month 12 time points. There were no reports of physical manifestations of EFAD and one triene: tetraene ratio checked at the Month 2 time point, which was within normal limits. Conclusions: Use of a four-oil ILE is associated with a clinically and statistically significant decrease in ALT, AST and T bili in pediatric HPN patients with baseline abnormal liver function tests. Clinical significance is supported by the return from >1.5 times the high normal limit values at Baseline to a normal reference range at the Month 3 time point for T bili and Month 12 time point for ALT and AST. Overall, the use of a four-oil ILE may provide benefit over traditional ILE in pediatric HPN patients with PNALD-related laboratory values. Financial Support received from: N/A
S6 - International Travel Made Possible For Home Nutrition Patients Jessica Wishon, MS, RD, CNSC; Michael Medwar, BA Coram CVS Specialty Infusion Services, Franklin, MA Purpose: Our objective is to show assisting patients to travel internationally while dependent on parenteral nutrition (PN) requires careful planning and consideration of key obstacles. A national home infusion company assists hundreds of Home Parenteral Nutrition (HPN) patients to travel each year; a small percentage travel out of the U.S. Three cases of HPN-dependent patients who successfully traveled internationally are presented. (Table 1) Methods: A is a 67-year-old female with short bowel syndrome (SBS). After starting teduglutide, weight
gain and increased energy levels led to her decision to return home to Germany for a month. Given the
trip duration, a shelf-stable/pre-mixed (SS/PM) formula that would meet her metabolic and fluid needs
was required.
B is a 73-year-old female with SBS. After a diagnosis of terminal cancer, it was her wish to return home to
Guatemala. An appropriate SS/PM formula was found, but it did not meet guidelines set by Medicare.
C is a 44-year-old female on PN for 3 years who desired to travel to Bahrain and Amsterdam for 13 days
to see family and for pleasure. Her clinical team recommended she use a SS/PM formula for the duration
of the trip. (Table 2)
Results: Patient A was started on a SS/PM formula 3 weeks before her trip to allow her clinical team to
monitor labs and educate on diet adjustments. She packed 4 days of PN in her carry-on with supplies and
pump. The remainder was packed in checked luggage. Patient was required to pay for extra bags despite
containing medical items. Patient reported no issues with TSA or customs and arrived safely in Germany.
Patient B’s doctor wrote a letter of medical necessity to allow an exception for the appropriate formula to
be covered by Medicare so that she could safely travel home. All PN was carried on the plane carried in a
carry-on to avoid lost luggage. The airline approved extra medical baggage with no additional fees.
Patient C’s team placed her on a shelf-stable formula for the trip. She arranged assistance through
special services with each airline. In Amsterdam before the trip home her IV pole was confiscated by
airport security. She reported the trip went “very well,” however, she was fatigued after arriving home and
became septic. Her line was changed 2 weeks after the trip.
Patients were advised to locate a medical center at their destinations for weekly central line dressing
changes if they did not have assistance from a trained caregiver. Emphasis was placed on the need to
prevent sepsis by staying diligent with proper line care.
Conclusions: Safe and successful international travel is possible. Patients should prepare and notify
their clinical team early for best outcomes.
Clinical teams can work with prescriber on using a SS/PM formula, which enables long trips.
Patients can successfully navigate TSA and customs with large amounts of medically necessary liquids.
Airline policies on medical baggage differ.
Unexpected issues can arise during planning and at any time during the trip. Patients should be closely
monitored after exhausting travel.
Financial Support received from: N/A
Table 1: Considerations
Travel Considerations Solution
Transporting compounded PN
Use carry-on rolling coolers that fit in overhead compartments.
on plane
Dressing changes Patient/caregiver independence or locate hospital abroad to perform.
Labs Hold if stable until return or coordinate care aboard
Security screening at U.S. Request assistance through TSA Cares/Passenger Support Specialist
airports Program. Provide TSA Disability Notification Card.
Carry medical inventory and letter from prescriber stating patient is
Customs/international airport
stable to travel, medical necessity of PN, and dates patient will be in
screening
visiting country.
Airline baggage fees/carry-on, Consult airline website; contact customer service manager.
weight limits Ask to pre-board if exceeding carry-on limits.
Wheelchair assistance/help
Request through airline when booking reservation
with bags neededRequest commercial airline authorization letter from pump
Infusing during flight
manufacturer.
Pump failure Have patient bring a back-up pump
Different electrical outlets in
Consult pump manufacturers for adapter recommendations
different countries
Considerations for Shelf-Stable Considerations When Transitioning to Shelf-Stable PN from a
PN Use Compounded Solution for International Travel
Beyond-use dating for trips Is there a shelf-stable product that will closely match required nutrition,
over 8 days electrolyte and volume needs?
Inadequate refrigeration at Do shelf-stable solutions result in formula that falls outside of insurance
destination coverage guidelines?
Is there time to trial formula before patient departs and make necessary
Convenience
ORS and dietary adjustments?
Table 2: Process for Safe Transition to Shelf Stable PN
Evaluate macronutrients & electrolytes of the SS/PM solution & identify one that is closest to the
compounded formula
Trial SS/PM 1-2 weeks in advance travel
Check BMP 24-48h after first dose to evaluate changes in serum electrolytes
As appropriate, provide patients with Oral Rehydration Solution recipes or samples to replace Na, Cl &
K
Reeducate on appropriate oral diet for condition to mitigate further malabsorption while traveling
Recheck BMP after ORS & diet change to assure serum stability before travel
S7 - Hypophosphatemia Resulting from Calcium Gluconate Shortage in Patients Receiving Home
Parenteral Nutrition: Case Series.
Vanessa Kumpf, PharmD, BCNSP1; Douglas L. Seidner, MD, AGAF, FACG, FASPEN, CNSC 2
1Center for Human Nutrition, Vanderbilt University Medical Center, Nashville, TN; 2Medicine, Vanderbilt
School of Medicine, Nashville, TN
Purpose: Patients receiving home parenteral nutrition (HPN) are particularly vulnerable to adverse
events related to product shortages because they are not as closely monitored as those receiving PN in
the hospital. The purpose of the report is to increase awareness of potential hypophosphatemia resulting
from inadequate calcium intake due to a calcium gluconate product shortage in patients receiving HPN.
Methods: In this report, calcium gluconate injection was unavailable and omitted from the HPN formula in
3 patients that resulted in a low serum phosphate concentration. The charts of these 3 patients were
retrospectively reviewed to describe the timing and extent of the complication and to describe the impact
of oral calcium to minimize the complication.
Results: Table 1 outlines the calcium and phosphate content in the HPN formula and Table 2 outlines
the associated serum calcium and phosphate concentrations of 3 patients at 4 separate data points: prior
to calcium gluconate removal, first lab result obtained after calcium removal, and the first 2 lab results
obtained following calcium replacement. Case 1: She is a 65-year old with short bowel syndrome (SBS)
who has been PN dependent for over 4 years and consumes a SBS diet. HPN frequency is daily and she
takes oral calcium carbonate 600 mg/ vitamin D three times daily. Hypophosphatemia develops one week
after removal of calcium from the HPN. Calcium gluconate is then added back at a lower dose (10 mEq).
Serum phosphorus normalizes when rechecked in 2 weeks. Case 2: She is a 43-year old with Crohn’s
disease on bowel rest who has been receiving HPN daily for 3 months. When calcium is removed from
the HPN, she is instructed to start calcium carbonate 500 mg/vitamin D orally twice daily.Hypophosphatemia is noted two weeks after removal of calcium gluconate, at which point the phosphate
dose is increased and calcium resumed at a lower dose (5 mEq) in the HPN. One-week later, the serum
phosphorus remains low but patient admits to stopping the oral calcium supplement since she was told
calcium was added back to the HPN. After resuming the oral calcium supplement, serum phosphorus
normalized when rechecked a week later. Case 3: He is a 54-year old who underwent biliopancreatic
diversion with duodenal switch 10 years ago and has required PN daily for about 6 months due to
malabsorption and failure to thrive. He was instructed to start calcium citrate 500 mg/vitamin D orally
twice daily when calcium gluconate was removed from the HPN. Hypophosphatemia was noted two
weeks after removal of calcium. Calcium gluconate was resumed at a lower dose (from 15 to 10 mEq) in
the HPN. After 2 weeks, serum phosphorus improved from 1.6 to 2.1 mg/dL but did not normalize until it
was rechecked at week 5. All patients had normal serum magnesium and vitamin D concentrations.
Serum albumin was normal in cases 1 and 2 and mildly depleted in case 3.
Conclusions: These 3 case reports demonstrate the development of hypophosphatemia in association
with the removal of calcium gluconate in patients receiving long-term HPN. Hypophosphatemia was noted
1 to 2 weeks after calcium removal and resolved when calcium gluconate was added back to the HPN.
Serum calcium remained in the normal range in case 1 and decreased slightly but returned to baseline in
cases 2 and 3. Oral calcium supplementation appeared effective in helping maintain normal phosphorus
concentrations while allowing for a reduced calcium gluconate dose in the HPN. Although parathyroid
hormone was not measured, we suspect that serum concentrations increased in response to decreased
calcium intake leading to release of calcium phosphate from bone and increased renal clearance of
phosphorus.
Financial Support received from: N/A
Table 1. Calcium and phosphate content in HPN.
Case 1 Case 2 Case 3
Ca dose Phos dose Ca dose Phos dose Ca dose Phos dose
(mEq/d) (mmol/d) (mEq/d) (mmol/d) (mEq/d) (mmol/d)
Prior to Ca removal 15 40 10 20 15 45
Ca removal 0 40 0 20 0 45
Ca replacement (1) 10 40 5 30 10 45
Ca replacement (2) 10 40 5 40 10 45
Ca, calcium; Phos, phoshate
Table 2. Serum calcium and phosphorus concentrations.
Case 1 Case 2 Case 3
Serum Ca Serum Phos Serum Ca Serum Phos Serum Ca Serum Phos
(mg/dL) (mg/dL) (mg/dL) (mg/dL) (mg/dL) (mg/dL)
Reference range 8.2-10.1 2.4-4.3 8.4-10.5 2.3-4.7 8.9-10.5 2.5-4.6
Prior to Ca removal 8.2 3.4 9.4 3.5 8.2 2.6
Ca removal 8.6 2.1 9.0 1.6 7.5 1.6
Ca replacement (1) 9.8 2.9 9.3 1.8 8.2 2.1
Ca replacement (2) 9.0 2.4 9.8 2.7 8.1 2.8
Ca, calcium; Phos, phosphorusENCORE
Presented: 10th International Pediatric Intestinal Failure and Rehabilitation Symposium
S8 - A Single Institution’s Experience with a Composite Lipid Emulsion: Patient Response and
Safety Concerns
Katie Huff, MD1,2; Francine D. Breckler, PharmD2; Wendy Cruse, RD2; Elaina Szeszycki, PharmD2;
Charles Vanderpool, MD1,2
1Indiana University School of Medicine, Indianapolis, IN; 2Riley Hospital for Children at IU Health,
Indianapolis, IN
Purpose: To describe our experience with initial institutional use of a composite lipid emulsion, including
frequency and predictors of patient response and safety concerns.
Methods: We performed a retrospective chart review of hospitalized children from September 2016 to
May 2018, identifying 36 patients who had received composite lipid emulsion (Smoflipid®). All patient
charts were reviewed for demographics, nutrition administration, growth parameters, laboratory data, and
adverse outcomes. We defined cholestasis as a direct bilirubin >2 mg/dL. Patient response was defined
as a resolution of cholestasis with direct bilirubin below 2 mg/dL or cholestasis improvement with a 20%
reduction of direct bilirubin but without resolution. Patient parameters were then compared between the
response groups using nonparametric statistical analysis.
Results: A total of thirty-two, or 89%, of patients had cholestasis at the start of composite lipid treatment
with a direct bilirubin greater than 2 mg/dL. The average starting dose of composite lipid was 2.1
gm/kg/day with an average maximum dose of 2.5 gm/kg/day. Of the 32 patients with cholestasis, 39%
had resolution of cholestasis, and 23% had improvement in direct bilirubin value (Figure 1). The overall
median length of composite lipid treatment was 53 days. When comparing patient parameters between
the response groups (Table 1), no parameters were found to be statistically significant between the
response groups. Safety concerns are listed in Table 2. Thirteen patients (54%) developed laboratory
evidence of essential fatty deficiency. Five patients (14%) suffered rapid infusion of the composite lipid
emulsion, leading to aminotransferase elevation, metabolic acidosis, and thrombocytopenia in some.
Eleven additional patients had adverse events leading to omission of lipid dose, incorrect dosage, or
issues with IV access.
Conclusions: Institutional introduction of the composite lipid emulsion included both patient benefit and
safety concerns within our initial cohort of patients. Treatment with the composite lipid emulsion was
associated with at least a 20% improvement in direct bilirubin in 62% of patients. However, only 39% of
patients had resolution of their cholestasis. While varying patient responses to treatment were noted, no
evaluated patient parameters were found to be significant between the three response groups, limiting
our ability to determine patient-specific factors that may predict cholestasis response. In response to
adverse events, our institution has developed a protocol for composite lipid emulsion use, including
mandatory nutrition support team consultation. We also developed additional education and safeguards in
an effort to reduce risk of lipid hyperinfusion. Further monitoring of patient outcomes into the future with
these policy changes in place is needed to better understand our influence on patient care.
Financial Support received from: N/A
Table 1: Patient Parameters and Response to Treatment
No Response Improvement Resolution P-
Patient Parameter
(n=12) (n=7) (n=12) value
Percentage Necrotizing Enterocolitis
33.3 (4) 0.0 (0) 41.7 (5) 0.168
(n)
Median Birth Weight (IQR)
1.0 (0.8, 2.1) 2.3 (0.6, 3.6) 2.0 (0.9, 2.6) 0.463
(kg)
Median Gestational Age (IQR) 30.5 (26.1, 35.1) 37.1 (25.9, 37.4) 34.4 (29.4, 36.4) 0.597Median Days Prior Soy Lipid (IQR) 32.5 (11, 64) 37.0 (24, 58) 50.0 (25, 74) 0.497
Median Enteral Volume Prior (IQR)
72.0 (18, 117.5) 24.0 (7, 76) 83.5 (21, 150) 0.322
(ml/kg/d)
Median Feeding Volume After (IQR)
85.0 (8, 133) 115.0 (112, 130) 58.0 (32, 121) 0.563
(ml/kg/d)
Median Peak Direct Bilirubin Prior
(IQR) 5.1 (3.8, 9.3) 5.6 (3.6, 16.1) 3.8 (3.1, 5.9) 0.226
(mg/dL)
Median Direct Bilirubin at Start
(IQR) 4.4 (3.4, 6.7) 5.0 (4.2, 7.1) 4.2 (3.4, 5.6) 0.525
(mg/dL)
Median Total Bilirubin at Start (IQR)
6.2 (4.6, 11.4) 9.3 (6.6, 11.5) 6.9 (4.9, 9.4) 0.413
(mg/dL)
Median ALT at Start (IQR)
50.0 (24, 77) 78.5 (63, 108) 73.5 (53, 140) 0.366
(U/L)
Median AST at Start (IQR)
57.0 (52, 77) 140.0 (75, 239) 101.5 (70.131) 0.087
(U/L)
Table 2: Safety Concerns Associated with Composite Lipid Emulsion Use
Safety Concern Total Patients (%)
Essential Fatty Acid Deficiency 13/24 (54%)
Rapid Infusion of Composite Lipid 5/36 (14%)
Missed/Held Dose 7/36 (19%)
Incorrect Order 2/36 (6%)
Incorrect Infusion Length 2/36 (6%)
S9 - Evaluation of Monitoring and Administration of Cyclic Parenteral Nutrition
Rachel Lavelle, PharmD1; Jessica Kaczor, PharmD, BCPS1; David C. Evans, MD, FACS2; Lisa
Mostafavifar, PharmD, BCPS, BCNSP11Pharmacy, The Ohio State University Wexner Medical Center, Columbus, OH; 2Department of Surgery, The Ohio State University, Columbus, OH Purpose: In patients with chronic gastrointestinal conditions that require long-term use of parenteral nutrition (PN), conversion from continuous, 24-hour PN to cyclic PN is necessary to avoid serious complications. Though generally well tolerated, cyclic PN can be associated with hyper- and hypoglycemia. To attenuate post-PN hypoglycemia, cyclic PN is commonly run at a 50 mL/hour “taper” for the last 2 hours of the infusion. At our institution, the nutrition policy suggests conversion to cyclic PN in patients who will eventually require outpatient PN administration. To assess for tolerability (defined as a blood glucose level
S10 - Improving transition of care using a parenteral nutrition discharge checklist. Linda D. Mlynarek, RPh, BCNSP; Jean Y. Doh, PharmD; Laura N. Hencken, PharmD, BCCCP; Nancy C. MacDonald, PharmD, BCPS, FASHP Pharmacy, Henry Ford Hospital, Detroit, MI Purpose: Purpose: The purpose of this study was to improve transition of care (TOC) for patients being discharged on parenteral nutrition (PN) by evaluating the impact of a standardized PN discharge checklist. The checklist incorporates Medicare requirements and ensures the necessary elements are coordinated early in the admission and met prior to discharge. Methods: Methods: This study was an IRB approved, retrospective quasi-experimental study of patients discharged on PN between January 1, 2014 and May 31, 2018. The primary endpoint was the completion
of a PN discharge bundle (identification of a responsible provider to monitor PN after discharge, meeting daily caloric requirement of 20-35 kcal/kg/day, cycling PN prior to discharge). Secondary endpoints included documentation of PN discharge checklist components, hospital length of stay, frequency of thirty-day hospital encounters, cause of hospital encounters, and time to readmission. Results: Results: After screening 753 patients, 50 encounters were included in the pre- and post-group each (n=100). There was a significant increase in completion of the TOC bundle in the post-group (54% vs 76%, p = 0.035), driven by improvement in identifying a responsible provider for outpatient PN management (54% vs 82%, p=0.005). Other PN discharge checklist components impacted included: case manager had the PN prescription for home infusion (50% vs 80%, p = 0.003), assessment for home glucometer (40% vs 90%, p
S11 - The use of parenteral nutrition in a tertiary hospital in Singapore- Are we doing it right? Zhen Xi Joel Lee, MBBS(S'pore), MRCP(UK), MMed(Internal Medicine); Yunn Cheng Ng, MBChB(UK), MRCP(UK); Leping Koay, MBBS(UK), MRCP(UK); Doris Hui Lan Ng, MBBCh BAO(UK), MRCP(UK), PhD(UK) Gastroenterology and Hepatology, Tan Tock Seng Hospital, Singapore, Singapore Purpose: Parenteral Nutrition (PN) is an important therapy for patients whose gut is not functioning. Inappropriate use, which can lead to infectious and metabolic complications, has been widely reviewed and reported. Our Nutrition Support Team (NST), in her advisory role, continued to audit the use of PN, with the aim of striving towards international standards of practice. Based on guidelines from the American Society of Parenteral and Enteral Nutrition (ASPEN) 2016 and European Society of Parenteral and Enteral Nutrition (ESPEN) 2017, this study reported on the appropriateness of the use of PN and its related complications. Methods: A retrospective cohort study of adult patients receiving PN from December 2014 to December 2016 in Tan Tock Seng Hospital was conducted. Data on patient demographics, Subjective Global Assessment (SGA) and PN indication, duration and related complications were reviewed. Based on ASPEN 2016 and ESPEN 2017 guidelines, inappropriate use of PN was defined as SGA A patients who had received PN for less than 7 days and all patients,regardless of SGA, who had received PN for less than 4 days. Overall composite percentage for inappropriate use was adjusted for overlap between these 2 definitions. Indications for PN use outside these 2 definitions were also examined. Results: A total of 399 (84% surgical) patients, (65% males, 35% females; median age 69 years, range 17-94) received PN over 24 months. 84.7% and 15.3% were managed by NST and Surgical Intensive Care Unit (SICU) respectively. Patients’ SGA status were A (34.2%), B (53.8%) and C (12%). Median PN duration was 8 days (range 1-71) and 90 (22.6%) patients received PN beyond 14 days. Common indications for PN were intestinal obstruction (25.8%) and post-operative ileus (23.1%). 11.4% were SGA A patients who received less than 7 days of PN and 6.3% received less than 4 days of PN regardless of SGA. Overall inappropriate PN use was 15.6%. 12.5% were SGA A patients who had more than 7 days of PN for pre-operative nutrition, routine post-operative nutrition and prolonged bowel rest. It was not possible to clearly determine if PN was indicated in this group due to poor documentation of clinical decisions. Complications of PN include hypertriglyceridemia (16.3%), liver enzyme derangement (14%), refeeding syndrome (8.9%), hyperglycaemia (8.5%) and feeding catheter infection (5.3%). Compared to SICU, patients under NST had lower incidences of feeding catheter infection (8.2% vs 5.6%) and refeeding syndrome (16.4% vs 9.2%). Conclusions: Our inappropriate PN use of 15.6% compares favourably with 15.9%-18.8% reported by local studies. However, this figure could be higher if we were able to determine if PN was truly indicated in 12.5% of cohort where the indications for PN were not strong. Under the NST, rates of feeding catheter infection and refeeding syndrome were lower. Intensive monitoring by NST also enabled early detection of hypertriglyceridemia, hyperglycaemia and liver enzyme derangement so that appropriate measures could be taken. Changing our NST’s advisory role to one which has a mandate to override inappropriate PN use may lead to improvement in the use of PN and its related complications. Financial Support received from: N/A S12 - Home parenteral nutrition in older versus younger patients: clinical characteristics and outcomes from Canadian home parenteral nutrition patient registry. Nicha Somlaw, MD1,2; Monica Ponta, MD3; Johane Allard, MD2,3 1Medicine, King Chulalongkorn Memorial Hospital and Chulalongkorn University, Bangkok, Thailand; 2Medicine, University of Toronto, Toronto, Canada; 3Gastroenterology, University Heath Network, Toronto, Canada
Purpose: With changes in demography, older patients receive home parenteral nutrition (HPN) more frequently but how the older fare compare to younger patients on HPN has not been well described. The main goal of the study was to compare the clinical characteristics and outcomes of older versus younger HPN patients. Methods: This retrospective study evaluated a cohort of patients that was prospectively enrolled in the Canadian HPN registry. Baseline and two year data entries were used for the analyses. Two groups of patients were compared: one aged 18-59 and another, aged 60 or over. Patient demography, indication for HPN, HPN regimen, nutrition assessment, vascular access, line sepsis, liver function tests, hospitalization and quality of life were evaluated. Results: Two hundred and thirty six patients were eligible for the study, 151 patients aged 18 to 59 (younger group: Y) and 85 patients aged 60 or over (older group: O). Body mass index (BMI) was similar at baseline (Y=20.8 kg/m 2 vs O=21.1 kg/m2, p= 0.475). Most common indication for HPN in Y group was surgical complication (Y=30% vs O=33%, p= 0.543) while the O group was cancer (Y=27% vs O=42%, p=0.017). Peripherally inserted central catheter (PICC) was the most common type of vascular access in both groups (Y=56% vs O=56%, p=0.901). Catheter infection rate per 1000 days was higher in Y group (Y=1.19 vs O=0.6, p=0.045). Daily energy provision from HPN regimen was similar in between groups; however, protein provision was higher in Y group (Y=1.41 g/kg/day vs O=1.33 g/kg/day, p=0.018). Over 2 years of HPN, alkaline phosphatase and bilirubin significantly increased in the O group (p=0.017 and 0.024 respectively). Quality of life improved in alive patients in Y group after 2 years of HPN, based on Karnofsky performance scale (KPS) from 70 to 90 (p< 0.001), while KPS changed from 70 to 85 (p=0.081) in O group. Conclusions: Older patients have cancer as the most frequent HPN indication, a lower rate of catheter infections but increases in liver enzymes and poorer quality of life that may reflect underlying disease rather than HPN, when compare to younger patients. Financial Support received from: N/A S13 - Relationship between Insulin Requirements, Energy Supply and Triglyceride Concentrations in Diabetic and Non-diabetic Patients Receiving Parenteral Nutrition Neha Lalani, MD1; Melissa Parkhurst, MD2; John M. Miles, MD1 1Medicine, University of Kansas, Kansas City, KS; 2Univ of Kansas Medical Center, Lenexa, KS Purpose: A comparison of studies of tight glucose control with intravenous insulin in patients receiving nutritional support suggests that there is a strong relationship between energy supply and insulin requirements. However, this relationship has not been examined using individual data from a single cohort of patients. Although the presence of diabetes and body mass index (BMI) ≥25 kg/m 2 has been shown to predict a need for insulin, previous studies did not consider subcutaneous insulin and did not exclude parenteral nutrition (PN) of short duration (
(30.2±0.5 v 27±0.3 kg/m2), and had higher glucose (165±2 v 133±1 mg/dl) and triglyceride (160±5 v 140±2 mg/dl) concentrations, despite lower relative energy supply (104±1% v 110±1% of estimated BER), all P
took 20 minutes to complete. Encounters prevented an adverse event in the home in 28 (42%) and prevented a medication error in the home in 13 (19%). Among the 98 families receiving care from the BCH HPN program, 34 (35%) responded to the PICS survey with overall satisfaction with access to care, communication with our team and team function. Only eight (25%) families reported knowledge of long-term goals (>6 months) of care in a clinic setting, and 12 (37%) reported that no single person followed up on long-term goals. Discussion: HPN requires a significant amount of care coordination, which is not reimbursable in the current fee-for-service insurance market. Assessment of resource allocation and family perception is needed to justify value with shift to Accountable Care Organizations. A notable finding is that a significant number of care coordination encounters prevented adverse events at home. Survey results identified an opportunity to improve goal making with families. In the next phase of a QI initiative, HPN providers and families recorded short- and long-term goals on a paper Action Grid during all ambulatory encounters. BCH HPN program plans to repeat PICS to measure changes in family perception over time. Conclusions: Conclusion: Significant and measurable healthcare resources must be allocated to HPN programs in order to provide this life-sustaining therapy. Future studies should quantify how resource allocation and parent perception are associated with patient outcomes. Financial Support received from: N/A S16 - Success,Safety and Savings of a Dedicated Nutrition Support Team Sandra Kless, PharmD BCNSP; Linda Hale, RN; Kendra Atherholt, BSN RN; Lori Holaly, BSN RN; Ann Christina, NP CNSC; Olaf Kroneman, MD CNSC Pharmacy, Beaumont Health - Royal, Madison Heights, MI Purpose: Dedicated Nutrition Support Teams have disappeared from hospitals over the last couple of decades. These Interdisciplinary teams have shown to be effective in utilizing the appropriate form of nutrition (Enteral Nutrition (EN) vs Parenteral Nutrition (PN)), based on evidence-base practice, thereby providing a cost savings to the institutions. The Nutrition Support Service (NSS) at Beaumont Health, Royal Oak is a multidisciplinary team that is comprised of a physician, nurse practitioner, pharmacist, and three nurses. It is our responsibility as clinicians to be cognizant of the cost, including risk and benefits of nutritional therapies and recommend appropriate options. Our goal is to demonstrate the decrease in inappropriate PN and Percutaneous Endoscopic Gastrostomy (PEG) placements as Electro-Magnetic Placement Device (EMPD) placements increased, providing a financial savings along with appropriate therapies. Methods: We reviewed the number of PN starts, PEG tube placements, naso-enteric feeding tube placements with the (EMPD) without x-ray, from January 2013 - December 2017. We obtained our institution's cost for: naso-enteric feeding tubes placed utilizing the EMPD, PEG tube placement and the average daily cost of PN. In addition, we obtained from literature the cost of blind placement of naso-enteric feeding tubes, average pneumothorax rate and associated cost along with the national average of inappropriate PN. From the data collected, we calculated cost savings. Results: Our institution's inappropriate PN rate decreased from 3.97% to 1% over the last five years, while the national average is reported to be approximately 15%. Our savings for PN over a five-year period was $387,611, with PN solution cost at $130.00 per day at our institution. The national average cost savings utilizing the EMPD over blind placement of naso-enteric feeding tube over a five-year period was $2,231,460 (blind placement cost $3,324,420 vs EMPD cost $1,092,960). Additional cost savings shown in avoidance of pneumothorax was $811,520. Over the last five years PEG tubes have decreased from 275 to 154.which demonstrated a net cost savings of approximately $300,000. Conclusions: The NSS core team at Beaumont Health - Royal Oak, has demonstrated a cost savings of $3,730,591 dollars over 5 years. A dedicated Nutrition Support Team is beneficial in providing the appropriate nutrition to patients as well as decreasing nutrition related hospital costs.
Financial Disclosure: Linda Hale and Kendra Atherholt have received payments for training healthcare providers to use EMPD Financial Support received from: N/A Figure 2. Cost savings of our institution inappropriate PN rate based on literature average
Cost Savings utlizing EMPD for naso-enteric tube placement vs Blind Placement vs PEG S17 - INTESTINAL FAILURE TYPE II IN ENTEROPERITONEAL TUBERCULOSIS Mario E. Ferreyra, MD PhD Consultant Surgeon4,2; Luisa Guerrero, RN MSc2,4; María Ocaña, Pharm D PhD (Hon)2,1; Roxana Soto, RD3; Rosario Holguin, RD3 1Pharmacy, Rebagliati Hospital, Lima, Peru; 2Nutritional Support, Nutrimedic, Bellavista, Peru; 3Nutrition, Rebagliati Hospital, Jesus Maria, Peru; 4Surgery, Rebagliati Hospital, Jesus Maria, Peru Purpose: Tuberculosis(TB) is a systemic disease and is on the rampage. Each year about 1.7 million people die of tuberculosis and 9 million new cases occur, worldwide. For every 25 to 30 cases of lung TB there is one case of enteroperitoneal TB. Humans are the natural reservoir of M. tuberculosis and about 500,000 people are infected with a multidrug-resistant strain of M. tuberculosis. Enteroperitoneal tuberculosis is a tragic life threatening condition associated with a completely "frozen" abdomen that clearly depicts an abdominal catastrophe. Mortality is up to 26%. Clinical presentation makes even the situation worse for it presents in some cases without concomitant lung disease so the first clinical impression is pelvic malignant disease with serum markers positive for cancer like Ca 125, so clinicians are mislead. Even laparoscopy may become very dangerous as bowel loops are stuck to the abdominal wall and perforation occurs, but at the same time no surgical approach is feasible. Three patients are presented in whom surgical treatment of complications was only feasible after sound nutritional support. Methods: Between 2009 and 2018 three female patients were diagnosed of enteroperitoneal TB without concomitant lung disease. Ages of diagnosis were 18, 22 and 27 years. The three patients were on TPN for periods of 2 to 6.5 months. Two patients developed enterocutaneous fistulas: one patient was on TPN for 2 months and Total Enteral Nutrition with peptides for 8.7 months and the other one was only on TPN,
for 6.5 months. The third patient had intestinal obstruction and was only on TPN, for 2 months. M. bovis was ruled out. Tuberculosis multidrug treatment was of between 6 to 24 months. Surgical procedures were: 1)Diagnostic laparotomy, colostomy and rectal and vaginal reconstruction, 2)right hemicolectomy and 3) 35-cm distal small bowel resection. Results: The three patients were discharged in good condition with complete systemic and gut rehabilitation after long periods of nutritional support and concomitant multidrug treatment. The concept of waiting 90 days on nutritional support before surgical treatment for a persistent gastrointestinal fistula without associated laparostomy, is challenged with enteroperitoneal tuberculosis, as it was necessary to wait for 6 to 26 months before surgical therapy, so that 90 days would not be feasible for this disease. Conclusions: The corner stone, we firmly believe, to cure severe cases of enteroperitoneal TB is transdisciplinary nutritional support as multidrug treatment is the conventional approach that will only be properly delivered once nutritional support is conceived as such, whatsoever. Financial Support received from: N/A S18 - Home Initiation of Parenteral Nutrition for the Bariatric Surgery Patient: A Multi-Team Approach Elaine Souza, MPH, RD, CSOWM 2; Angela Damron, RD2; Lisa M. Kinder, RD, CNSC1; Shirley Au, RD, CNSC1; Barbara Jachniewicz, CRNFA, MS, FNP-BC2 1Home Infusion Services , Briova Rx , Sacramento , CA; 2Bariatric Surgery Program , University of California Davis , Sacramento , CA Purpose: Bariatric patients may be at risk for post-operative complications, with parenteral nutrition (PN) support indicated during significant nutrition compromise. The purpose of this abstract is to showcase this bariatric team’s (BT) unique approach to PN support, which promotes avoidance of re-hospitalization via early post-op nutrition assessment, and when PN support is necessary, collaborates with a home infusion nutrition support team (HNST) for a safe and timely home PN initiation utilizing a customized PN order form (Image 1). Methods: The BT’s nutrition assessment, monitoring, and education includes multiple pre-op appointments with follow up beginning two weeks post-op. A customized post-op bariatric surgery form is utilized in clinic to capture patient’s daily trends and highlight areas that may be affecting oral intake, including social factors (Table 1). Post-op monitoring includes evaluation and education as well as instructions for patient to notify the BT immediately if symptoms occur that may interfere with oral intake. When the BT dietitian and NP nutrition assessments determine that PN support is indicated (Image 2), the BT notifies the HNST via a customized home initiation PN order form. The BT and HNST collaborated to create this form, which expedites and simplifies the PN initiation process. The PN formula macronutrient options promote achievement of appropriate bariatric surgery weight loss goals, incorporate safety measures for the prevention of refeeding syndrome, and provide an option to order additional fluids. Our case study demonstrates a real time line and activation of our unique approach of a home PN initiation (Table 2). During home PN support, comprehensive monitoring is performed by the BT and HNST, with the BT determining the PN macronutrient goals and readiness for weaning from PN. The HNST assesses labs, adjusts PN electrolytes, with the HNST dietitian providing nutrition assessment updates to the BT. Results: Case study: Patient presented on POD 15 after a laparoscopic Roux-en-Y gastric bypass reporting adequate oral intake. Days later patient developed nausea/vomiting, and inability to tolerate liquids. POD 23 patient received 3L IVFs in clinic. POD 29 revealed symptoms continued despite interventions. Social influences also affected oral intake and delayed patient in notifying BT of status. Due to persistent vomiting and inadequate oral intake, a PICC was placed on POD 37 for IVF and possible PN support. PN support started on POD 44, continuing for 4 months. Barriers to weaning PN included persistent nausea/vomiting, abdominal pain and early satiety. Once vomiting resolved, BT challenged patient to focus on oral intake while holding the PN, and providing IVF prn. PN support was discontinued once patient demonstrated 75% and 65% of fluid and protein needs orally, respectively.
Conclusions: This collaborative approach between the BT and HNST results in timely and appropriate
initiation of home PN support, avoiding unnecessary re-hospitalization, as evidenced in the case
described. Home PN support aids in maintaining adequate macronutrient, electrolyte, and fluid intake until
the bariatric surgery patient is able to achieve adequate oral intake. Use of the customized PN order form
and multi-team monitoring provides a consistent and safe approach to home initiation of PN support in
this unique patient population.
Financial Support received from: N/A
Table 1: Post-Op Bariatric Surgery Form - Factors to Consider
Nutrition Social
Fluids Hours of sleep in 24 hour period
Grams of protein Support at home
GI symptoms Caring for others/schedule demands
Supplements Depression/psych issues
Exercise Lack of prioritization
Dumping Stress level
Intake dose (too fast/too much) Financial
Table 2: Case Study
Weight
Factors to Consider Nutrition Support Algorithm
(lbs)
Date of
291
RYGBP
POD 15 277 Adequate PO intake No intervention
Fluids < 48oz, protein < 30gm (x 7 days)
POD 23 Poor PO intake
- IVF
N/V, poor PO intake, time spent caring Fluids < 48oz, PN recommended by RD,
POD 29 268
for others, finance issues PICC order placed for IVF (PN if needed)
POD 30 Fluids < 48oz - IVF
POD 35 Poor PO intake Fluids < 48oz
POD 37 Ongoing symptoms of N/V PICC placed - IVF
POD 41 Insurance changes Unable to initiate PN
Abdominal pain, poor PO intake, time
POD 43 260 IVF
spent caring for others
POD 44 PN initiated
Little improvement in nausea, less
POD 50 262 Fluids < 48oz
emesis
Nausea improved, poor PO intake d/t
POD 64 258 Fluids < 48oz
pain
Fluids < 48oz, recommend decrease PN
Pain resolved, early satiety with fluid
POD 76 261 regimen, encouraged patient to track PO
intake, increase in PO intake
intake
POD 77 PN adjustedAll previous symptoms returned, time
POD 92 253 spent caring for others, self stopped PN PN continued, encouraged daily infusion
x3 nights
POD 104 255 Abdominal pain, early satiety, vomiting Added 1L IVF 3x/week
Not consistent tracking, early satiety,
POD 125 252 Fluids < 48oz
time spent caring for others
Fluids 36-56oz, protein 50gm daily, plan
POD 139 249 Improved PO intake
to hold PN x2 weeks
Fluids 48oz, protein 50-60gm,
POD 153 244
recommend hold PN and additional IVF
POD 171 241 Improved PO intake Recommend d/c PICC
POD 192 237 Adequate PO intake No interventionImage 1: Customized PN Order Form
You can also read