Strengthening sepsis care at a tertiary care teaching hospital in New Delhi, India
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Open access Original research
BMJ Open Qual: first published as 10.1136/bmjoq-2020-001335 on 3 August 2021. Downloaded from http://bmjopenquality.bmj.com/ on October 7, 2021 by guest. Protected by copyright.
Strengthening sepsis care at a tertiary
care teaching hospital in New
Delhi, India
Charu Malhotra ,1 Akshay Kumar,1 Ankit Kumar Sahu,1
Akshaya Ramaswami ,1 Sanjeev Bhoi,1 Praveen Aggarwal,1 Rakesh Lodha,2
Arti Kapil,3 Sonali Vaid,4 Nitesh Joshi1
To cite: Malhotra C, Kumar A, ABSTRACT Surviving Sepsis Campaign (SSC) guidelines
Sahu AK, et al. Strengthening Introduction Failure of early identification of sepsis in the recommend the implementation of a 1-hour
sepsis care at a tertiary care
emergency department (ED) leads to significant delays in bundle for patients with sepsis to reduce
teaching hospital in New
antibiotic administration which adversely affects patient morbidity and mortality.3 The guidelines
Delhi, India. BMJ Open Quality
2021;10:e001335. doi:10.1136/ outcomes. recommend sending blood cultures prior to
bmjoq-2020-001335 Aim The primary objective of our Quality Improvement (QI)
antibiotics, administering antibiotic, starting
project was to reduce the door-to-antibiotic time (DTAT) by
►► Additional online
appropriate fluid resuscitation, measuring
30% from the preintervention in patients with suspected
supplemental material is sepsis. Secondary objectives were to increase the blood lactate and starting inotropes if necessary
published online only. To view, culture collection rate by 30% from preintervention, within the first hour of recognising sepsis and
please visit the journal online septic shock. Nevertheless, the translation of
investigate the predictors of improving DTAT and study
(http://dx.doi.org/10.1136/
the effect of these interventions on 24-hour in-hospital evidence-based guidelines to clinical practice
bmjoq-2020-001335).
mortality. remains a challenge. Quality improvement
Methods This QI project was conducted in the ED of (QI) initiatives in this field are much needed
Received 2 January 2021 a tertiary care teaching hospital of North India; the ED to bridge the ‘know- do gap’. These initia-
Accepted 16 May 2021 receives approximately 400 patients per day. Adult patients
tives conducted to improve patient safety
with suspected sepsis presenting to our ED were included
have successfully been implemented in high-
in the study, between January 2019 and December 2020.
The study was divided into three phases; preintervention income countries (HICs). However, limited
phase (100 patients), intervention phase (100 patients) data are available regarding their impact on
and postintervention phase (93 patients). DTAT and blood sepsis care in LMICs.4
cultures prior to antibiotic administration was recorded The emergency department (ED) of
for all patients. Blood culture yield and 24-hour in- our institution caters to 400 patients daily,
hospital mortality were also recorded using standard data with sepsis being the most common life-
templates. Change ideas planned by the Sepsis QI Team threatening emergency. Being a tertiary care
were implemented after conducting plan-do-study-act academic centre located in a highly dense
cycles.
population zone of North India, our depart-
Results The median DTAT reduced from 155 min in
preintervention phase to 78 min in postintervention phase. ment caters to a large proportion of critically
© Author(s) (or their ill patients. Sepsis care in our high-volume,
employer(s)) 2021. Re-use
Drawing of blood cultures prior to antibiotic administration
permitted under CC BY-NC. No improved by 67%. Application of novel screening tool resource strapped setting was often found
commercial re-use. See rights at triage was found to be an independent predictor of to be suboptimal by the staff. In an effort to
and permissions. Published by reduced DTAT. promote patient safety and care, a QI initia-
BMJ. Conclusion Our QI project identified the existing lacunae tive for sepsis patients was planned in ED. We
1
Department of Emergency in implementation of the sepsis bundle which were dealt intended to focus on implementing two most
Medicine, All India Institute of with in a stepwise manner. The sepsis screening tool and important aspects of the sepsis bundle that
Medical Sciences, New Delhi, on-site training improved care of patients with sepsis. A
India is, administering antibiotics within 1 hour
similar approach can be used to deal with complex quality
2
Department of Pediatrics, issues in other high-volume low-resource settings.
of presentation to the ED and draw blood
All India Institute of Medical cultures prior to antibiotic administration.
Sciences, New Delhi, India The primary objective of our QI project was
3
Department of Microbiology,
All India Institute of Medical INTRODUCTION to reduce the door-to-antibiotic time (DTAT)
Sciences, New Delhi, India Sepsis is a dysregulated host response to by 30% from preintervention. Secondary
4
Incluve Labs LLP, New Delhi, infection causing life-threatening organ objectives were to increase the blood culture
India dysfunction.1 In 2017, around 11 million collection rate by 30% from preintervention,
Correspondence to sepsis-
related deaths have been reported investigate the predictors of improving DTAT
Dr Akshay Kumar; worldwide with highest burden in low-income
Open access
BMJ Open Qual: first published as 10.1136/bmjoq-2020-001335 on 3 August 2021. Downloaded from http://bmjopenquality.bmj.com/ on October 7, 2021 by guest. Protected by copyright.
METHODS Preintervention phase was from January 2019 to April
This study was conducted in the ED of a tertiary care 2019. During this period, preintervention data such as
teaching hospital of North India. The staff work in 6-hour demographic and clinical details, DTAT, blood culture
shifts every day. In each shift, 20 residents are supported information and 24- hour in-
hospital mortality among
by a team of 30 nursing officers with one resident and one suspected sepsis patients were collected (data collection
nursing staff posted at triage. Around 100 new patients sheet in online supplemental material). Analysis of the
are screened for emergency conditions in every shift. preintervention data was conducted using fishbone anal-
Adult patients with suspected sepsis presenting to our ysis (online supplemental material) and process flow
ED were included in the study, from January 2019 to chart. Detailed process flow chart of suspected sepsis
December 2020. Paediatric patients (
Open access
BMJ Open Qual: first published as 10.1136/bmjoq-2020-001335 on 3 August 2021. Downloaded from http://bmjopenquality.bmj.com/ on October 7, 2021 by guest. Protected by copyright.
Table 1 Characteristics of study population
Characteristics Preintervention (n=100) Intervention (n=100) Postintervention (n=93) Overall (n=293)
Dates January 19–April 19 May 19–May 20 June 20–December 20 January 19–
December 20
Age in years 45 (30–63) 42.5 (23–56.3) 51 (35–61.5) 45 (29–60)
Males, n (%) 67 (67) 65 (65%) 55 (59) 187 (63.8)
Triage as red, n (%) 89 (89) 98 (98) 90 (97) 277 (94.5)
Source of sepsis, n (%)
Abdominal 18 (18) 31 (31) 11 (11.8) 60 (20.5)
Cellulitis 3 (3) 4 (4) 8 (8.6) 15 (5.1)
Central Nervous 11 (11) 1 (1) 8 (8.6) 20 (6.8)
System infections
Others 11 (11) 18 (18) 12 (12.9) 41 (14)
Respiratory tract 51 (51) 45 (45) 48 (51.6) 144 (49.1)
Urogenital tract 6 (6) 1 (1) 6 (6.5) 13 (4.4)
Number of comorbidities
None 26 (26) 50 (50) 30 (32.3) 106 (36.2)
One 59 (59) 45 (45) 45 (48.4) 149 (50.9)
Two 12 (12) 2 (2) 14 (15.1) 28 (9.6)
More than two 3 (3) 3 (3) 4 (4.3) 10 (3.4)
Presenting vitals
Heart rate, per min 112 (89–127) 121 (109–134) 100 (90–130) 113 (90–130)
Systolic Blood 110 (84–134) 90 (80–99) 112 (91–138) 100 (85–126)
Pressure, mm Hg
Oxygen saturation, % 92 (84–98) 97 (94–98) 96 (87–98) 96 (89–98)
Respiratory Rate, per 22 (20–26) 20 (20–23) 26 (22–28) 22 (20–26)
min
Glasgow Coma Score 15 (12–15) 15 (15–15) 15 (12–15) 15 (13–15)
(GCS)
Sepsis screening tool 0 (0) 61 (61) 48 (51.6) 109 (37.2)
applied, n (%)*
Blood cultures collected, 0 (0) 17 (17) 63 (67.7) 80 (27.3)
n (%)*
Door to antibiotic time* 155 (92–438) 118.5 (73.8–221.8) 78 (54–122.8) 115 (70–202)
Door to antibiotic time 8 (8) 13 (13) 34 (36.6) 55 (18.8)
less than 60 mins, n (%)*
24-hour mortality, n 23 (31.5) 7 (19.4) 4 (7.8) 34 (21.3)
(%)*†
*POpen access
BMJ Open Qual: first published as 10.1136/bmjoq-2020-001335 on 3 August 2021. Downloaded from http://bmjopenquality.bmj.com/ on October 7, 2021 by guest. Protected by copyright.
is non-specific and had more utility as a mortality predictor
in Intensive Care Unit (ICU) settings.6–8 Considering the
sensitivity of National Early Warning Score (NEWS) in
identifying Sepsis,9 NEWS was tried as a screening tool
in our ED from 6 May 2019 to 13 May 2019. The NEWS
score was found to be tedious as it required calculating
the score every time. During the busy hours in triage the
front-line staff often found it challenging to use this score
and hence it was abandoned.
PDSA 2: On-site teaching and awareness
We had learnt from our earlier experiences that class-
Figure 2 Photographs of quality improvement (QI) team, on- room teaching often failed due to poor attendance. This
site QI training and QI meeting. was largely due to shift duties of the emergency staff.10
On 15 October 2019, we did our first PDSA (onsite aware-
defined were implemented. Timewise implementation of ness and training to identify sepsis) wherein we started
change ideas is presented in figure 3. A data collection on-site training for nurses and residents working in
team was formed within the study team and included the triage. The training was planned in the early hours of the
nursing staff posted in triage. They were asked to note shift between 7:00 and 8:00 hour to allow ample time with
the patient’s arrival time (T1) to triage in an anonymous residents and nurses as the patient load was scarce. The
manner on a small data collection sheet and share the training was easy to perform, lasting only 10–15 min each
copy of the data sheet on a small closed WhatsApp group time and simple to replicate. We got a positive response
that was formed. The nursing staff in-charge of electronic from the front-line staff. A total of five training sessions
health records (EHR) posted inside the ED would then were conducted and all staff members working in triage
identify these patients during their rounds and add the were included. The sessions were led by residents and
antibiotic administration time from the case notes of nursing officers regularly working in triage. The data on
the patient as T2. The times were then noted on a data DTAT was recorded continuously on these days, but we
collection sheet present with this staff. The data in-charge did not expect to see any improvement in this regard, as
routinely collected information from the other team the team in the treatment area of the emergency was not
members and updated in the excel sheet. involved in training.
PDSA-1 National Early Warning Score for Sepsis Screening PDSA 3: Implementation of a ‘Sepsis Screening Tool’
Tool at triage In view of the specific challenge of lack of a sepsis
To achieve compliance with administration of antibiotics screening tool, we devised a novel tool specifically for
within 1-hour, recognising sepsis at triage was the major utility in our ED. The existing AIIMS Triage Protocol11
bottleneck identified. For this purpose, a screening tool was modified to include triage clinical features of infec-
for suspecting sepsis in a patient was needed. Of the preex- tion (tCFI),7 12 to form a novel ‘AIIMS Sepsis Screening
isting screening tools, quick Sequential Organ Failure Tool (SST)’ (details in online supplemental figure 2).
Assessment (qSOFA) score was rejected by consensus as it The AIIMS SST was developed using the Delphi method.
The SST was tried in a PDSA cycle conducted between
22 October 2019 and 29 October 2019 and was adopted
successfully by the triage staff. The triage staff and resi-
dents were asked to highlight ‘Suspected sepsis’ or ‘?
Sepsis’ on the patient record paper at the triage desk. The
doctors and nurses in triage were encouraged to apply the
novel SST during their respective morning shifts. DTAT
was continuously being recorded. The clinical process was
tested during five morning shifts and the front-line staff
found it straightforward to use and easy to integrate into
the current system of triage. Due to the large number of
doctors and nurses on rotating and changing shifts at any
point of the day, it was not possible to train all concerned
stakeholders at the same time. Thus, we decided to focus
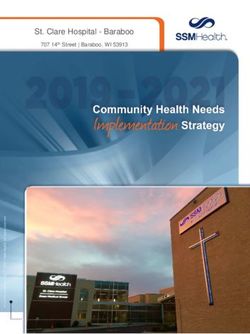
Figure 3 Run chart of the quality improvement project,
on different areas of the department one by one. With
depicting the weekwise door to antibiotic time (in minutes), the success of this change idea in the morning shift, we
stretching over all the three phases of the study. January-19, decided to test it on a larger scale. Starting 31 October
w1 denotes first week of the month January 2019 (similar 2019, this new clinical process was implemented in all
notion applies to all the data points in x-axis). shifts.
4 Malhotra C, et al. BMJ Open Quality 2021;10:e001335. doi:10.1136/bmjoq-2020-001335Open access
BMJ Open Qual: first published as 10.1136/bmjoq-2020-001335 on 3 August 2021. Downloaded from http://bmjopenquality.bmj.com/ on October 7, 2021 by guest. Protected by copyright.
PDSA-4: Regular teaching and awareness sessions Data collection and analysis
Residents and nursing staff posted in the triage area and Time of arrival to ED of suspected sepsis patients was noted
ED floor had regular on-site training sessions organised on the case sheet along with vitals and chief complaints
in October and November 2019. Short on-site training on presentation. Time of first antibiotic administration
sessions were organised for the staff and residents before was noted from the patient case notes after the patient
morning shift started. They were briefed regarding the was shifted to the treatment area. DTAT was calculated
importance and implementation of 1-hour sepsis bundle from the above-mentioned time stamps. Blood cultures
for patients presenting with suspected sepsis. drawn prior to antibiotic administration were recorded
In view of change in the ED staff due to the COVID-19 by the data collection team from the details mentioned
pandemic, the teaching programme was incorporated regarding the same in the patient case sheets. This infor-
in the weekly academic activities of the department in mation was collected and reviewed by the members of the
September and October 2020. QI team weekly. Interrupted time series charts were made
to see the effect of PDSAs. Probability based rules of run
PDSA 5: Sepsis checklist charts were applied on the interrupted time series chart
In February 2020, a sepsis checklist highlighting the to investigate the non-random variations.13 Quantitative
important aspects of the 1-hour sepsis bundle was intro- variables were tested for normality using Kolmogorov-
duced. This checklist was required to be attached to the Smirnov test. Normally distributed quantitative variables
case sheet of patients presenting with suspected sepsis. were expressed as mean and SD. Non-normally distrib-
Due to COVID-19 pandemic, the checklist was abandoned uted variables were expressed as median and IQR. Cate-
to decrease virus transmission by fomites. Following this, gorical variables were summarised as frequency (%). Data
the triage team was instructed to mention ‘prescription analysis was done in IBM SPSS Statistics for Windows, V.27
of appropriate antibiotics and blood cultures to be drawn (IBM). A pOpen access
BMJ Open Qual: first published as 10.1136/bmjoq-2020-001335 on 3 August 2021. Downloaded from http://bmjopenquality.bmj.com/ on October 7, 2021 by guest. Protected by copyright.
Figure 5 Adjusted OR of all the predictors of ‘Door to
antibiotic timeOpen access
BMJ Open Qual: first published as 10.1136/bmjoq-2020-001335 on 3 August 2021. Downloaded from http://bmjopenquality.bmj.com/ on October 7, 2021 by guest. Protected by copyright.
solution to the problem rather than a short-term inter- workers to embrace an unfamiliar system. Our experience
vention. This initiative is one among few to be set in shows that QI projects in resource-constrained settings
LMICs. Our study underscores the value of incorporating are better applicable for individual components of a care
simple measures viz. using a sepsis screening tool and bundle rather than all at once.
regular on-site teaching and training without incurring Short on-site teaching and training sessions were instru-
any additional cost. All change ideas were implemented mental in spreading awareness and motivating front-line
after conducting PDSA cycles which ensured their accept- staff. ED differs from other departments in having a shift
ance by the healthcare workers. Due consideration was work culture. A problem in the teaching programme was
given to avoid any cumbersome change ideas as found by to find a common time and place to gather staff. This
the team. issue was overcome by short and crisp on-site and on-duty
No major costs were incurred during conduct of this teaching sessions which were conducive to our settings.
project. No equipment was procured, no additional staff Significant delay was noted in improving blood culture
were recruited and no construction was undertaken in rates prior to antibiotic administration. The delay was
the existing hospital building. The focus, instead, was on partly attributable to the existing SOP for procuring blood
changing processes of care to make it easier for residents culture bottles for the ED. This problem was solved with
and staff to adhere to components of the 1-hour sepsis due cooperation from the Department of Microbiology,
bundle. thereby emphasising the role of interdepartmental coop-
Reduction in DTAT was found to be statistically signifi- eration to improve patient care. Increasing blood culture
cant. There was an increase in the rate of blood cultures rates prior to antibiotic administration should improve
drawn prior to antibiotic administration from 0% in the blood culture yield rates. This in the long run will assist
preintervention phase to 68% in the postintervention the development of department- specific antibiogram
phase. Increased compliance with sepsis bundle showed contributing to an antibiotic stewardship programme.
a direct correlation with clinical outcomes as was demon- This project has brought about better implementation
strated by reduction in mortality. The 24-hour mortality of sepsis bundle in a busy ED. Biannual on-site training
although statistically different between preintervention sessions have been initiated along with inclusion of sepsis
and postintervention groups is prone to bias because screening tool in a teaching manual for newly joined
significant cohort of patients were transferred to other residents of the department. The momentum attained
hospitals. by our project will be carried on by two new projects
Previous studies on QI initiatives in sepsis patients planned in the ED, one being validation of the novel
showed significant improvement in practice after imple- sepsis screening tool and the other being improving the
mentation of change ideas.12 14–19 Most of these studies blood culture positivity rate. To ensure that the improve-
were conducted in HICs, used laboratory parameters ments are sustained, periodic audits by the QI team will
to recognise sepsis and had the provision for electronic be conducted.
medical records. Our study differs in the critical aspect as There were certain limitations to our study. In our QI
being one of its kind to be conducted in a high-volume, initiative, only two components of the Surviving Sepsis
low-resource setting. As part of this QI effort, data were guidelines were taken into consideration. Our project
collated from different sites in the ED. included patients presenting with suspected sepsis at
Our sepsis QI team included all staff members involved triage, leaving out patients developing sepsis after arrival
in patient care viz. consultants, residents, nursing officers to ED. Collection of DTAT during our QI project was by
and hospital attendants. Each team member enlisted the forming a WhatsApp group with data being collected by
issues faced in patient care from their unique perspec- the QI team members, which appears to be tedious. For
tive and helped in establishing an efficient data collection future activities in the department, we have planned to
technique over a period of 2 years. collect this data from the ED EHR. We are planning to
Sepsis Screening Tool implementation was found to be select the patients with ‘? Sepsis’ diagnosis, retrieve the
associated with improved compliance with drawing blood T1 (time of admission to ED) and T2 (administration of
cultures and antibiotic administration within 1 hour. As a first dose of antibiotics as recorded by the nursing staff)
clinical outcome, direct correlation with mortality reduc- and calculate DTAT. Further initiatives would be required
tion was demonstrated. Conventional sepsis screening for other components, that is, time to start inotropes and
tools were found unsuitable for our settings. qSOFA was lactate clearance. The novel screening tool used in this
less sensitive causing over-triage and NEWS was cumber- project has not been validated earlier. As the implementa-
some to implement.6–9 AIIMS triage protocol was modi- tion of well validated qSOFA and NEWS scores were failed
fied to look for tCFI in patients triaged RED as per criteria in PDSAs, we developed the novel sepsis screening tool
of altered physiology. It was readily accepted by the resi- using Delphi method. The tool has to be prospectively
dents and staff posted in triage since this was a part of validated internally and externally in future studies.
our existing protocol. This showcased the fact that in a Yield rates would increase with the improvement in
high-volume setting with a constantly changing resident the technique of obtaining blood cultures, which was not
and staff population, efforts to modify the existing system included in our study. In view of COVID-19 pandemic,
prove more sustainable than convincing healthcare restructuring of triage and segregation of patients with
Malhotra C, et al. BMJ Open Quality 2021;10:e001335. doi:10.1136/bmjoq-2020-001335 7Open access
BMJ Open Qual: first published as 10.1136/bmjoq-2020-001335 on 3 August 2021. Downloaded from http://bmjopenquality.bmj.com/ on October 7, 2021 by guest. Protected by copyright.
respiratory infection may be a confounding factor for Open access This is an open access article distributed in accordance with the
reduced DTAT in postintervention phase. Although the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which
permits others to distribute, remix, adapt, build upon this work non-commercially,
improvement in blood culture rates and proportion of and license their derivative works on different terms, provided the original work is
patients receiving antibiotics within an hour has surely properly cited, appropriate credit is given, any changes made indicated, and the use
improved, the standard of sepsis care is still suboptimal. is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Important factors preventing an optimal outcome were ORCID iDs
found to be regular change of staff and a large cohort Charu Malhotra http://orcid.org/0000-0003-0824-5574
of untrained residents and staff employed in the ED. Akshaya Ramaswami http://orcid.org/0000-0002-1683-9658
Regular teaching initiatives by the department would
help sustain this improvement and achieve the highest
possible standards in patient care in the future. REFERENCES
1 Singer M, Deutschman CS, Seymour CW, et al. The third
International consensus definitions for sepsis and septic shock
(Sepsis-3). JAMA 2016;315:801–10.
CONCLUSION 2 Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and
Streamlining sepsis care is essential in all EDs as sepsis national sepsis incidence and mortality, 1990–2017: analysis for the
is a life-
threatening and time-sensitive condition. This global burden of disease study. The Lancet 2020;395:200–11.
3 Levy MM, Evans LE, Rhodes A. The surviving sepsis campaign
QI initiative helped in successful implementation of the bundle: 2018 update. Intensive Care Med 2018;44:925–8.
two main components of the SSC bundle. Fever, altered 4 Becker JU, Theodosis C, Jacob ST, et al. Surviving sepsis in low-
income and middle-income countries: new directions for care and
sensorium and application of sepsis screening tool were research. Lancet Infect Dis 2009;9:577–82.
independent predictors of reduced DTAT. The crude 5 POCQI-Learner-Manual.pdf. Available: https://www.newbornwhocc.
org/POCQI-Learner-Manual.pdf [Accessed 24 Mar 2021].
mortality rate significantly reduced in the postinterven- 6 Cutler NS. Diagnosing sepsis: qSOFA is not the tool we're looking
tion phase when compared with the preintervention for. Am J Med 2020;133:265–6.
group. New SOP to procure blood culture bottles helped 7 Filbin MR, Thorsen JE, Lynch J, et al. Challenges and opportunities
for emergency department sepsis screening at triage. Sci Rep
in improving the blood culture rates. On-site training 2018;8:11059.
sessions were key in spreading awareness and engaging 8 Kalil AC, Machado FR. Quick sequential organ failure assessment is
not good for ruling sepsis in or out. Chest 2019;156:197–9.
with front-line staff. 9 Usman OA, Usman AA, Ward MA. Comparison of SIRS, qSOFA,
Twitter Sonali Vaid @sonalivaid and news for the early identification of sepsis in the emergency
department. Am J Emerg Med 2019;37:1490–7.
10 Kumar A, Lakshminarayanan D, Joshi N, et al. Triaging the triage:
Acknowledgements We hereby acknowledge all the members of our quality reducing waiting time to triage in the emergency department
improvement team viz, Mr Dheeneshbabu Lakshminarayanan, Ms Charulatha at a tertiary care hospital in New Delhi, India. Emerg Med J
Sasidharan, Mr Mohammed Jesal, Mr Dyal, Mr Pramod Kumar, Mr Ratan Meena, 2019;36:558–63.
Mr Gulabchand, Ms Pooja, Ms Nisha, Dr Nitish, Dr Tarun Yadav, Mr Thasteen 11 Sahu AK, Bhoi S, Galwankar S, et al. All India Institute of medical
TS, Dr Soorya Sureshbabu, Dr Rajalekshmi, Dr Aaditya Katyal, Dr Roshan PK sciences triage protocol (ATP): ATP of a busy emergency department.
and Dr Archana Nair for their valuable support and contributions to our quality J Emerg Trauma Shock 2020;13:107–9.
12 Filbin MR, Thorsen JE, Zachary TM, et al. Antibiotic delays and
improvement project.
feasibility of a 1-Hour-From-Triage antibiotic requirement: analysis
Contributors Study planning: CM, AKu, SB, PA, RL and AKa. Study conduct: CM, of an emergency department sepsis quality improvement database.
AKu, SV and NJ. Data collection: CM. Data analysis: AKS and CM. Manuscript Ann Emerg Med 2020;75:93–9.
writing: CM and AR. Proofreading: CM, AKu, SB, PA, RL, AKa and AR. 13 Perla RJ, Provost LP, Murray SK. The run chart: a simple analytical
tool for learning from variation in healthcare processes. BMJ Qual
Funding Publication of this article is made Open Access with funding from the Saf 2011;20:46–51.
Nationwide Quality of Care Network. 14 Gatewood Medley O'Keefe, Wemple M, Greco S, et al. A quality
improvement project to improve early sepsis care in the emergency
Competing interests None declared. department. BMJ Qual Saf 2015;24:787–95.
Patient consent for publication Not required. 15 Scheer CS, Fuchs C, Kuhn S-O, et al. Quality improvement initiative
for severe sepsis and septic shock reduces 90-day mortality: a 7.5-
Ethics approval The Institute Ethics Committee for this Quality Improvement Project Year observational study. Crit Care Med 2017;45:241–52.
was obtained prior to the project on 28.12.2018. (IECPG-620/19.12.2018) 16 Lane RD, Funai T, Reeder R, et al. High reliability pediatric septic
shock quality improvement initiative and decreasing mortality.
Provenance and peer review Not commissioned; externally peer reviewed. Pediatrics 2016;138:e20154153.
Data availability statement Data are available on reasonable request. Data are 17 Nates LKC, Pereira AJ, Neto AC. A quality initiative to implement
available on reasonable request to the corresponding author. a managed sepsis protocol in a public hospital based on the
IHI quality improvement model: experience report. Quality in
Supplemental material This content has been supplied by the author(s). It has Primary Care 2017;25 https://primarycare.imedpub.com/abstract/
not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been a-quality-initiative-to-implement-a-managedrnsepsis-protocol-in-
peer-reviewed. Any opinions or recommendations discussed are solely those a-public-hospital-based-onrnthe-ihi-quality-improvement-model-
of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and experiencernreport-20929.html
18 Mariani B, Corbella M, Seminari E, et al. Evaluation of a model to
responsibility arising from any reliance placed on the content. Where the content
improve collection of blood cultures in patients with sepsis in the
includes any translated material, BMJ does not warrant the accuracy and reliability emergency room. Eur J Clin Microbiol Infect Dis 2018;37:241–6.
of the translations (including but not limited to local regulations, clinical guidelines, 19 Seoane L, Winterbottom F, Nash T, et al. Using quality improvement
terminology, drug names and drug dosages), and is not responsible for any error principles to improve the care of patients with severe sepsis and
and/or omissions arising from translation and adaptation or otherwise. septic shock. Ochsner J 2013;13:359–66.
8 Malhotra C, et al. BMJ Open Quality 2021;10:e001335. doi:10.1136/bmjoq-2020-001335You can also read