STERILIZATION POLICY & GUIDELINE - Department: Quality Improvement Department - Dubai HealthCare City Authority
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

STERILIZATION
POLICY & GUIDELINE
Department: Quality Improvement Department
Document Identifier: PP/HCO/012/01
POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
INTRODUCTION
With the advent of managed healthcare, increasing numbers of patients are now being cared for in ambulatory-care
and home settings. Many patients in these settings might have communicable diseases, immunocompromising
conditions, and/or invasive devices. Therefore, adequate disinfection in these settings is necessary to provide safe
patient care.
Major risk of all invasive procedures is the introduction of pathogens that can lead to infection. Failure to
properly disinfect or sterilize equipment carries not only risk associated with breach of host barriers but also risk for
person-to-person transmission (e.g., hepatitis B virus) and transmission of environmental pathogens (e.g.,
Pseudomonas Aeruginosa).
Disinfection and sterilization are essential for ensuring that medical and surgical instruments do not transmit
infectious pathogens to patients. Because sterilization of all patient-care items is not necessary, healthcare policies
must identify, primarily on the basis of the items' intended use, whether cleaning, disinfection, or sterilization is
indicated.
Sterilization refers to the complete eradication of all living organisms, including spores. Common sterilization
techniques include the application of wet heat, dry heat, chemicals, and radiation. The type of material, the
container, and quantity of items to be sterilized determines which method to use. Various types of equipment
are used for sterilization in the facilities, but the autoclave is the primary means of sterilizing supplies. The
autoclave is also used to sterilize infectious waste. Sterilization will occur when the conditions of steam,
pressure, temperature and time are met.
1. PURPOSE
1.1
The purpose of this guideline is to provide minimum standards and procedures guideline in
sterilization practices for healthcare operators in outpatient clinics and other clinical
support and medical facilities in Dubai Healthcare City (DHCC).
1.2
This guideline has been developed to assist healthcare operators implement best practices in
sterilization procedures and may be adopted by licensed healthcare operators in DHCC as part of
their internal policies, procedures and guideline.
1.3
The ultimate goal of these recommendations is to reduce rates of health-care associated
infections through appropriate use of both disinfection and sterilization.
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 1 / 30
POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
2. SCOPE OF APPLICATION
2.1 This guideline is applicable to all hospitals, outpatient clinics, surgical facilities, day care surgery units
or any other facility providing services related to reprocessing and sterilization.
2.2 This guideline should be used in conjunction with the autoclave manufacturer’s manual and other
relevant required organizational and DHCR regulatory policies and procedures e.g. Medical Equipment
Management Policy & Guideline, Infection Control Guidelines (Sharps management guideline,
Standard Precautions Guideline, Hand hygiene guideline)etc.
2.3 This guideline consist of an on-site sterilization and off site sterilization (outsourced) procedures and
serves as a basic guide for High-Level Disinfection of Endoscopes.
2.4 This guideline does not provide a comprehensive reference to practice or to the various types and
methods of sterilization available.
2.5 There are several types of sterilizers (steam autoclaves, Ethylene Oxide gas, plasma, etc.) used in the
decontamination and sterilization process in healthcare, however this guideline only focuses on the
procedures for steam sterilizers (also known as autoclaves).
3. POLICY STATEMENTS
3.1 HCO undertaking reprocessing of equipment, devices or items must adopt and maintain basic
infection prevention and control systems and programs for all staff members.
3.2 HCO must have written evidence based policies and procedures within the facility to address in detail
the whole disinfection and sterilization process, incident reporting and recall process, and preventive
maintenance plan of the equipment used.
3.3 All manufacturer’s instructions and user manuals should be adhered to and copies must be kept
within the work areas for ease of reference. Ensure that manufacturer instructions matches
international recommendations and does not contradict it.
3.4 HCO is responsible for consistent staff education, training, competencies and orientation of their
personnel.
3.5 Items purchased, loaned, physician owned, research equipment or items obtained by any other
method must meet consistent practices of sterilization.
3.6 The HCO takes responsibility for correct management when reprocessing clinically used items and
devices.
3.7 Should any of the functions in this policy be performed by another party, on behalf of the HCO, the
requirements of this policy shall continue to apply to all reprocessing activities. Other forms of
sterilization not addressed in this policy can be utilized when met with manufacturers requirements
for installation and instructions for use.
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 2 / 30
POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
3.8 The reuse of single-use medical devices is not permitted.
3.9 Use of Flash Sterilizers are not permitted.
4. GUIDELINE
4.1 Structure & Layout of Sterilization Unit:
4.1.1 All surfaces e.g. walls, floors, ceilings, shelves should be washable.
4.1.2 Rooms should be well ventilated and lit.
4.1.3 The environment should be free of dust, flies, damaged infrastructure or extreme heat/cold.
4.1.4 An uninterrupted supply of water and electricity is essential.
4.1.5 Physical separation between dirty and clean areas.
4.1.6 Access must be restricted to qualified personnel only.
4.2 Principles of Contamination:
4.2.1 A body penetrated by disease‑causing microorganisms is said to be “contaminated”.
4.2.2 Instruments used during an operation are also considered to be contaminated by the patient’s
microorganisms and pathogens. If these instruments are not meticulously cleaned and
sterilized before being used on another patient, pathogens can be passed from one patient to
another.
4.2.3 Cross‑infection is one of the major causes of nosocomial infection. It has a huge impact on
the patient as it can extend their stay in the facility leading to more nursing care, more
operations/procedures and more rehabilitation. It also increases health complications that
can ultimately result in death. Therefore it is essential for HCPs to understand the
mechanisms by which infection is transmitted and follow correct processes to provide good
quality health care to those who need it.
4.3 Aseptic Technique
4.3.1 Before an instrument can be used, several process steps must be followed to prevent/
minimize risk to the patient. Sterilization is only one step in the process required to make an
instrument sterile at the moment of use.
4.3.2 Each step in the process involves specific methods and techniques that prevent
contamination of instruments, materials and living tissue. This is called the aseptic technique
and is designed to prevent contamination of instruments, materials and living tissue.
4.3.3 The aseptic technique must also be followed in the sterilization unit. There are various
methods of organizing the entire instrument sterilization process i.e. collection,
pre‑disinfection, cleaning, disinfection, packaging, sterilizing, distributing and storage.
4.4 Methods of Reducing the Bioburden:
4.4.1 Cleaning
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 3 / 30
POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
The process of removing dirt and soils, but not killing microorganisms and spores.
4.4.2 Disinfection
The process of destroying all pathogenic microorganisms, but not bacterial spores.
4.4.3 Sterilization
The process of destroying all forms of microbial life on instrument surfaces, including bacterial
spores. Sterilization methods include steam, dry heat and chemical sterilization. Steam is the
preferred method for sterilizing critical medical and surgical instruments that are not damaged
by heat, steam, pressure, or moisture.
4.4.4 Low-Level Disinfection
This procedure kills most vegetative bacteria except M. tuberculosis, some fungi, and
inactivates some viruses. The EPA approves chemical germicides used in this procedure in the
US as "hospital disinfectants" or "sanitizers." Low-level disinfection is performed for
noncritical patient-care surfaces (e.g., bedrails, over-the-bed table) and equipment (e.g., blood
pressure cuff) that touch intact skin.
4.4.5 Intermediate-Level Disinfection
Some items that may come in contact with non-intact skin for a brief period of time (i.e.,
hydrotherapy tanks, bed side rails) are usually considered noncritical surfaces and are
disinfected with intermediate-level disinfectants (i.e., phenolic, iodophor, alcohol, chlorine). This
procedure kills vegetative microorganisms, including Mycobacterium tuberculosis, all fungi, and
inactivates most viruses. Chemical germicides used in this procedure often correspond to
Environmental Protection Agency (EPA) - approved "hospital disinfectants" that are also
"tuberculocidal." They are used commonly in laboratories for disinfection of laboratory benches
and as part of detergent germicides used for housekeeping purposes.
4.4.6 High- Level Disinfection
High-level disinfection traditionally is defined as complete elimination of all microorganisms in
or on an instrument, except for small numbers of bacterial spores. The FDA definition of high-
level disinfection is a sterilant used for a shorter contact time to achieve a 6-log10 kill of an
appropriate mycobacterium species. Cleaning followed by high-level disinfection should
eliminate enough pathogens to prevent transmission of infection.
4.4.6.1 Semi-critical devices require high-level disinfection using chemical disinfectants like
ortho-phthaldehyde (OPA), hydrogen peroxide, chlorine dioxide and peracetic acid
that are cleared by the Food and Drug Administration (FDA). This procedure kills
vegetative microorganisms and inactivates viruses, but not necessarily high numbers
of bacterial spores. Such disinfectants are capable of sterilization when the contact
time is relatively long (e.g., 6 to 10 hours).
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 4 / 30
POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.4.6.2 As high-level disinfectants, they are used for relatively short period of time (e.g., 10
to 30 minutes). These chemical germicides are potent sporicides and, in the United
States, are classified by the FDA as sterilant/disinfectants. They are formulated for
use on medical devices, but not on environmental surfaces such as laboratory
benches or floors.
* For Classes of Chemical Disinfectants & Activity Level please refer to Appendix 1.
4.5 Classification of Instruments (Spaulding Classification):
4.5.1 Critical Items/devices present high risk of infection to the patient if they are contaminated
with any microorganism and as they enter a normally sterile area of body (sterile tissue or the
vascular system) and therefore require sterilization. This category includes surgical
instruments, cardiac and urinary catheters, implants, and ultrasound probes used in sterile
body cavities. Most of the items in this category should be purchased as sterile or be sterilized
with steam if possible. Heat-sensitive objects can be treated with ethylene oxide (EtO),
hydrogen peroxide gas plasma; or if other methods are unsuitable, by liquid chemical sterilants.
4.5.2 Semi-critical Items/devices contact mucous membranes or non-intact (broken) skin.
Examples of such devices includes respiratory therapy and anesthesia equipment, esophageal
manometry probes, cystoscopes, anorectal manometry catheters, diaphragm fitting rings,
laryngoscope blades, rectal speculums, and some types of flexible endoscopes.
4.5.2.1 These medical devices should be free from all microorganisms; however, small numbers
of bacterial spores are permissible.
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 5 / 30
POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.5.2.2 These items minimally require high-level disinfection using chemical disinfectants
which should eliminate most viruses, bacteria (particularly mycobacteria), fungi, and in
some cases bacterial spores.
4.5.2.3 Typical biocides widely used as high-level disinfectants include ortho-phthaldehyde
(OPA), hydrogen peroxide, chlorine dioxide and peracetic acid and are cleared by the
Food and Drug Administration (FDA). When a disinfectant is selected for use with
certain patient-care items, the chemical compatibility after extended use with the
items to be disinfected also must be considered.
4.5.3 Non-critical Items/devices are also called as low risk devices, and are those that come in
contact with (non-broken) intact skin but not mucous membranes therefore, the sterility of
items coming in contact with intact skin is "not- critical." Non-critical items are divided into
non-critical patient care items and non-critical environmental surfaces. Examples of non-
critical patient-care items are bed rails, some food utensils, bedside tables, patient furniture,
floors bedpans, blood pressure cuffs, crutches, computers, stethoscopes, sinks, general work
surfaces etc.
4.5.3.1 In contrast to critical and some semi critical items, most non-critical reusable items
may be decontaminated where they are used and do not need to be transported to a
central processing area.
4.5.3.2 It is recommended that such surfaces/devices be treated either with disinfectant that
have a low or intermediate level of disinfection or even in some cases just by cleaning
alone (to physically remove soil and microorganism). Examples of biocides used in
low/intermediate level disinfectants are quaternary ammonium compounds, phenolics
and alcohol. Mops should be laundered daily. Single-use disposable towels
impregnated with a disinfectant also can be used for low-level disinfection when spot-
cleaning of non-critical surfaces is needed.
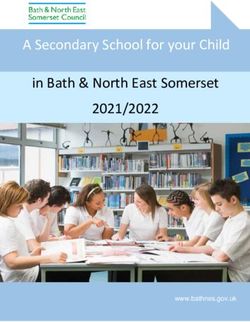
4.6 Zoning: The flow of instruments through the central sterile supplies department should follow the
following four zones.
3.Autoclaving 4. Storage &
1. Cleaning - 2. Packaging -
- Distribution
Dirty Zone Clean Zone Zone
Sterile Zone
4.6.1 Zone 1: Cleaning (or dirty) zone: This is the area in which reusable instruments are collected,
registered, cleaned and dried. These activities can all be carried out in the same room,
provided that all steps are carried out in one direction only and that nothing ever moves back
towards the dirty zone – dirty and clean items must never cross. The dirty zone should be laid
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 6 / 30
POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
out in a way that facilitates this flow. In some settings, a wall will separate the dirty zone from
the clean zone, although the two have to be connected via a doorway (or a wicket) to
facilitate the transfer of instruments. All items must be checked to ensure they have been
properly cleaned before they leave the dirty zone, and before being dried and packaged. Any
items that are not properly clean must be re cleaned before they are taken out of the dirty
zone. The dirty zone should be easily accessible from the operating, obstetric and surgical
emergency units to facilitate the reception of reusable instruments. It must also be located
next to the clean zone. Instruments and equipment should be pre‑disinfected and cleaned as
soon as possible after use to prevent the formation of a biofilm. Discard the used solution
away and prepare a fresh one for each load.
4.6.1.1 Manual cleaning steps:
Don personal protective apparel.
Assemble the required cleaning brushes and accessories.
Use a “dirty to clean” principle.
Flush the items in running water, temperature 15 °C to 30 °C, to remove gross
visible blood and body substance. Failure to remove protein prior to immersion of
instruments into detergent will result in coagulation of protein rendering soil
more difficult to remove.
Fill sink with warm water (approximately 45 °C) add appropriate detergent to the
concentration recommended by the manufacturer. All items returned should be
considered contaminated, used or not.
Dismantle or open all items prior to placement in the cleaning solution.
Hold the items low in the sink to limit the generation of aerosols during
scrubbing. Wash all surfaces of the item, including brushing lumens and valves,
using the correct size brush. Remove stubborn stains with an appropriate brush.
Rinse the item in warm to hot running water.
Remember: If it’s not clean, it’s not sterile
4.6.1.2 Ultrasonic Cleaning:
Ultrasonic cleaners work by subjecting stainless steel instruments to high
frequency, high energy sound waves, causing soil to be dislodged from
instruments and to drop to the bottom of the tank or be sufficiently loosened to
ensure removal during the rinsing process.
All visible soil should be removed prior to emersion in order to minimize bio-
burden in the tank.
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 7 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
An ultrasonic cleaner is recommended for the cleaning of delicate instruments
and hard to access channels, threads, joints and lumens. Manufacturer’s
instructions regarding steps of cleaning, type of water to be used, water quality,
temperature of added water and additives are to be followed to avoid damage to
equipment.
Ultrasonic cleaners are not to be used for plastics or similar materials or
cemented lenses or telescopes. These cleaners must have lids and are operated
on the single load principle.
4.6.2 Zone 2: Packaging (or clean) Zone:
This is the area for checking/inspecting instruments, reassembling instrument sets, high‑level
disinfection, packaging and storage of packages ready to be sterilized. The clean zone should
be separated from the dirty zone by a wall, with a door (or a wicket) connecting them to
facilitate the transfer of material. It should be located between the dirty zone and the sterile
zone. Steps include:
4.6.2.1 Inspecting Instruments:
Check and ensure that instruments are intact. Small deposits of blood may easily
develop into serious corrosion (rust) and this corrosion is aggravated by the moisture
and high temperatures of the sterilization process. Corrosion will result in serious
damage to the instruments and may even render them useless and dangerous for the
patient. This is why every instrument should be checked carefully before being
packed. If it is damaged or no longer functioning, alert the person in-charge so that
the instrument can be exchanged. Apply oil if necessary, but use only specific
silicone‑free instrument oil, which allows steam to penetrate during sterilization. The
instrument should be rinsed to remove excess oil and dried.
4.6.2.2 Before sterilization: packaging protects the clean instruments from the risk of
contamination.
4.6.2.3 Appropriate supplies used for packing should be available and adequate.
4.6.2.4 Develop a tracking system for each load and identification for patient file entry.
4.6.2.5 Checklist for instruments to be placed in each set should be available.
4.6.2.6 Drying area for cooling unloaded racks should be of adequate space. Condensate
within bundles and trays continues to dissipate for a minimum period of 45 minutes
following sterilizer unloading.
4.6.2.7 Mark items and sets with the sterilization date, batch number and method to track
procedural items used into patient records.
4.6.2.8 Packaging must allow the packages to be opened easily and aseptically.
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 8 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.6.2.9 Packaging must be permeable to steam, water repellent, resistant to tears and
impermeable to microorganisms.
4.6.2.10After sterilization: packaging must keep the instruments sterile until they are used.
4.6.3 Zone 3: Autoclaving (or sterile) zone:
This is the area in which the instruments ready to be sterilized by steam sterilization in an
autoclave are registered. It is important to ensure that there is enough space on all sides of
the autoclave for safe use and maintenance. A steam exit has to be provided in line with the
manufacturer’s specifications to prevent scalding. This access must be restricted to qualified
personnel only.
4.6.3.1 Steam Sterilization:
Of all the methods available for sterilization, moist heat in the form of saturated
steam under pressure is the most widely used and the most dependable. Steam
sterilization is nontoxic, inexpensive, rapidly microbicidal, sporicidal, and rapidly heats
and penetrates fabrics. The basic principle of steam sterilization, as accomplished in
an autoclave, is to expose each I item to direct steam contact at the required
temperature and pressure for the specified time. Thus, there are four parameters of
steam sterilization: steam, pressure, temperature, and time. The two common
steam-sterilizing temperatures are 121°C (250°F) and 132°C
(270°F). These temperatures (and other high temperatures) must be
maintained for a minimal time to kill microorganisms.
4.6.3.2 The Steam Sterilization Cycle:
1. Start – door seals, jacket warms chamber
2. Purge – steam enters chamber, while air is purged through the chamber drain
3. Conditioning – positive pressure and negative vacuum pulses continue to heat
load and purge air
4. Heat up – steam pressure builds to selected exposure temperature and pressure
5. Exposure – timing begins for selected exposure time and temperature
6. Exhaust – chamber drain opens and ejector water creates vacuum in chamber to
exhaust steam
7. Drying – ejector water controls vacuum in chamber for selected dry time
8. Air in – chamber returns to atmospheric pressure
9. Cycle complete – door can be opened
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 9 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.6.3.3 The following are basic instructions for autoclave use but do not replace the
manufacturer's operating instructions and hands-on training. Before using any
autoclave for the first time, read and thoroughly understand the owner's manual
because many makes and models have unique characteristics.
1. Follow the sterilization times, temperatures, and other operating parameters
(e.g., gas concentration, humidity) recommended by the manufacturers of the
instruments, the sterilizer, and the container or wrap used, and that are
consistent with guidelines published by government agencies and professional
organizations.
2. Use low-temperature sterilization technologies (e.g., EtO, hydrogen peroxide gas
plasma) for reprocessing critical patient-care equipment that is heat or moisture
sensitive.
4.6.4 Zone 4: Storage and distribution zone:
This is the area in which sterile packages are stored until distributed. It is important to have a
storage place in which instruments and sterile items are protected from the risk of
recontamination, i.e. dust, insects, damage to packages, humidity, light, and in which their
sterile status is maintained until they are used. It should be located next to the autoclaving
zone.
4.6.4.1 Distribution of items to external departments should be logged when released to the
department and signed by the receiving staff member. They should be transported in a
wire cart or trolley with a dust cover or shroud or a closed cart dedicated to the
distribution of sterile supply.
4.6.4.2 Non-Sterile consumables should not be stored on the sterile stock shelves or in sterile
stock areas.
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 10 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.6.4.3 Shelf life and rotation of stock should be a department policy and all staff should be
aware of methods used to ensure items rotate. Factors which influence shelf life are
event related and include packaging material, storage and handling conditions,
likelihood of product material deterioration and package design.
4.7 Safety
4.7.1 Because autoclaves use steam, heat and pressure, the risk of individual exposure and injury is
high. Personnel should wear proper personal protective equipment (PPE), i.e. heat‑resistant
gloves, eye protection and a gown, particularly when unloading the autoclave.
4.7.2 Do not assume that the temperature and pressure have fallen when opening the chamber.
Even if the pressure gauge shows “0”, open the chamber carefully; start by opening the door
just a crack to allow steam to dissipate (don’t fling the door open, as steam might billow out
and scald exposed skin).
4.7.3 After opening the door, leave the items inside for five minutes before handling. This will reduce
the risk of boil‑over and scalding.
4.7.4 Regularly inspect the autoclave to make sure it is working properly.
4.7.5 Have a trained technician follow a maintenance schedule.
4.8 Use of Indicators
4.8.1 Chemical Indicator (also referred to as a CI) is a monitoring system that responds to a change
in one or more pre-defined variables, based on a chemical or physical change resulting from
exposure to a process. There is no hierarchal significance in the classes of indicators (see pic in
section 7.1). The choice of indicators should be based on the parameters being measured, as
each class has its own unique characteristics and intended use. For example, Class IV is not
superior to Class I; they simply measure different variables.
4.8.2 Use both internal and external chemical indicators.
4.8.3 For every load, it must be possible to prove that the autoclave was working properly on that
date and that the sterilization cycle achieved the necessary standard. Record the physical
conditions (or parameters) in the sterilizer during the process.
- Checking the sterilization cycle
- Chemical indicators = TST STRIP
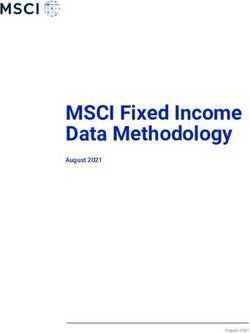
4.8.4 Internal indicators undergo a chemical change (from yellow to dark blue) when exposed
to Time – Steam – Temperature (TST). A TST strip must be put in the big surgical wire basket
to monitor time, steam and temperature inside the packages.
(example below)
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 11 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.8.4.1 Write the date of sterilization and the autoclave and cycle number on the TST strip.
4.8.4.2 After sterilization is completed and before any instruments are sent to the storage
room, confirm that the TST strip has changed color as shown in the above diagram; if
it has not, the complete load must be considered unsterile and sent for repackaging
and re‑sterilization.
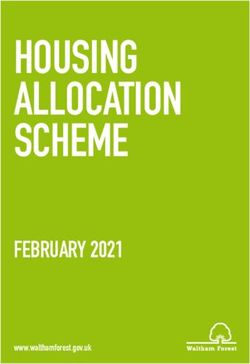
4.8.4 External indicator = Tape
These indicators are used only to identify packages that have been through a sterilization
process. Autoclave indicator tape consists of yellow indicator stripes and pressure‑sensitive
adhesive. When the steam sterilization is completed, the color of the indicator strips will turn f
from yellow to dark brown or black.
4.8.4.1 Autoclave steam indicator tape should be used in each autoclave load. It may be used
to secure packages and also to indicate that those packages have been exposed to the
proper levels of heat and moisture needed to achieve sterility. After proper exposure,
dark diagonal lines appear on the tape.
4.8.4.2 While this color change is not a guarantee of sterility and should be evaluated with
biological monitoring tests, it does indicate that all factors necessary for sterilization
were present during processing.
4.8.4.3 Check that the package is undamaged at the end of the cycle upon unloading, the
packages should not be damp or wet and the paper covering should be intact.
4.8.4.4 Inspect each package for tears/holes.
4.8.4.5 Torn packages are unsterile and must be sent for repackaging and re‑sterilization
(example below)
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 12 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.8.5 Biological Indicators:
4.8.5.1 Chemical indicators do not indicate that a device is sterile and should not replace
biological indicators.
4.8.5.2 The biological spore test is still the gold standard and the most accepted means for
monitoring sterilization. The biological indicator test consisting of bacterial spores
demonstrates the actual killing of an organism against a control test containing viable
bacteria.
4.8.5.3 These results must be recorded in the log book.
4.8.5.4 In the event of a failed biological spore test, you would need to recall the instruments
that were used on each client and determine the cycle, load and sterilizer affected.
4.8.5.5 Each facility should develop their own written evidence based protocol to recall all
improperly reprocessed devices and instruments.
4.8.5.6 All items being reprocessed should be recorded and tracked in the event of a failed
biological spore test.
4.9 Bowie‑Dick Test on Autoclaves with Vacuum Pump
4.9.1 Checking the airtight seal before sterilization = Bowie‑Dick test
4.9.2 The Bowie‑Dick Test is performed to assess air removal efficiency in steam sterilizers used in
pre‑vacuum sterilization cycles. It detects air leaks and inadequate air removal. It is mandatory
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 13 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
for pre‑vacuum sterilizers and has to be carried out on a daily basis in an empty autoclave,
before the first load.
4.9.3 A commercially available Bowie‑Dick Test sheet is placed in the center of the package. The test
package is placed horizontally in the front, bottom section of the sterilizer rack, near the door
and over the drain, in an otherwise empty chamber. The test is run at 134°C for 3.5 minutes.
4.9.4 The test is performed each day the vacuum‑type steam sterilizer is used, before the first load
is processed. Air that is not removed from the chamber will interfere with steam contact.
Sterilizer vacuum performance is acceptable if the sheet inside the test package shows a
uniform color change. Entrapped air will cause a spot to appear on the test sheet, because the
steam is unable to reach the chemical indicator.
4.9.5 If the sterilizer fails the Bowie‑Dick Test, do not use it until it has been inspected by the
sterilizer maintenance personnel and passes the Bowie‑Dick Test.
4.9.6 The Bowie‑Dick Test does not replace the TST strips. In an autoclave with a vacuum pump, the
Bowie‑Dick Test must be performed daily. TST strips must be used in every load as described
above and recorded in the log.
(example below)
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 14 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.10 Reading the graph for a vacuum‑pump autoclave:
4.10.1 Check if the time exposure is correct.
4.10.2 Check that the three vacuum peaks are visible.
4.10.3 Check that the “sterilization plateau” is parallel for temperature and pressure.
4.10.4 Once all these checks have been performed, the load can be “cleared”, meaning that it has been
correctly sterilized (following the right procedure).
(example below)
4.11 Chemical Storage
4.11.1 All items required for the CSSD should be in a limited supply close at hand for ease of use by
staff. Chemicals should be housed in a separate cool, locked cupboard with the MSDS at hand.
4.11.2 Cardboard/cartons should not be kept in this area as it holds moisture and can harbor insects
and bacteria.
4.11.3 All supplies should be elevated from the floor and away from the ceiling for adequate
ventilation.
4.11.4 Staff should be aware of the safety requirements for handling the chemicals.
4.11.5 There should be an area for receiving and unpacking supplies and removing outer packaging
for discard.
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 15 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.12 Tracking and Traceability of Medical Devices:
4.12.1 It is important to be able to trace products through the decontamination processes to which
they have been subjected and to the patient on whom they have been used.
4.12.2 The ability to track and trace medical devices and equipment enables corrective action to be
taken when necessary.
4.12.3 Records should be maintained for all the trays cleaned, identifying:
The cleaning and sterilization method used;
The name of the person undertaking the decontamination;
Details of the actual tray being processed;
Which patients have been treated with the tray.
4.12.4 This information is required so that instrument trays can be traced, if required, in the event of
a failure in the decontamination cycle or for infection control reasons.
4.12.5 The use of untracked supplementary instruments should be avoided where possible and
instruments grouped together into traceable trays.
4.12.6 Each sterilizing cycle must be recorded in a log. The log should contain the following data:
Date
Contents of the load
Cycle number
The TST
Name of the person performing the sterilization.
Each autoclave must have its own log.
4.13 Monitoring of Sterilizers & Quality Control Checks:
4.13.1 Use mechanical, chemical, and biologic monitors to ensure the effectiveness of the sterilization
process.
4.13.2 Monitor each load with mechanical (e.g., time, temperature, pressure) and chemical (internal
and external) indicators. Do not use processed items if the mechanical (e.g., time, temperature,
pressure) or chemical (internal and/or external) indicators suggest inadequate processing.
4.13.3 Use appropriate type or class of chemical indicators. See Table in Appendix 8.1 for Classes of
Chemical Indicators.
4.13.4 Use biologic indicators to monitor the effectiveness of sterilizers at least weekly with an FDA-
cleared commercial preparation of spores (e.g., Geobacillus Stearothermophilus for steam)
intended specifically for the type and cycle parameters of the sterilizer. After a single positive
biologic indicator used with a method other than steam sterilization, treat as non-sterile all
items that have been processed in that sterilizer, dating from the sterilization cycle having the
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 16 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
last negative biologic indicator to the next cycle showing satisfactory biologic indicator results.
These non-sterile items should be retrieved if possible and reprocessed.
4.13.5 After a positive biologic indicator with steam sterilization, objects other than implantable
objects do not need to be recalled because of a single positive spore test unless the sterilizer
or the sterilization procedure is defective as determined by maintenance personnel or
inappropriate cycle settings. If additional spore tests remain positive, consider the items non
sterile and recall and reprocess the items from the implicated load(s).
4.13.6 Use biologic indicators for every load containing implantable items and quarantine items,
whenever possible, until the biologic indicator is negative.
4.13.7 Compare the reprocessing instructions (e.g., for the appropriate use of endoscope connectors,
the capping/non-capping of specific lumens) provided by the instrument manufacturer and
the sterilizer manufacturer and resolve any conflicting recommendations by communicating
with both manufacturers.
4.13.8 Ensure reprocessing instructions are current and accurate and are correctly implemented.
4.13.9 Document all deviations from policy. All stakeholders should identify what corrective actions
will be implemented.
4.13.10 Ensure a system of process monitoring: air-removal testing for pre-vacuum steam sterilizers;
visual inspection of packaging materials; and traceability of load contents.
4.13.11 For each sterilization cycle, record the type of sterilizer and cycle used; the load identification
number; the load contents; the exposure parameters (e.g., time and temperature); the
operator’s name or initials; and the results of mechanical, chemical, and biological monitoring.
4.13.12 Retain all sterilization records (mechanical, chemical, and biological) for a minimum of 2 years.
4.13.13 Preventive maintenance on sterilizers should be performed by qualified personnel who are
guided by the manufacturer’s instruction.
4.13.14 Maintain a sterilizer maintenance contract with records of service.
4.13.15 Discontinue use immediately if an autoclave is not working properly. Post a sign on the
autoclave to notify others that the autoclave is not operational.
4.13.16 Bowie‑Dick Test must be performed daily.
4.14 Off-site/ Outsourced Sterilization:
The outsourcer should provide the following details to the HCO:
4.14.1 An opportunity to conduct an onsite visit at the outsourcer site to determine if they meet the
requirements of the sterilization service.
4.14.2 An opportunity to review tracking and qualification documents relating to washer disinfector,
ultrasonic cleaner, sealer machines, sterilizers of any type and all equipment used for testing
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 17 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
and achieving sterilization e.g. commissioning, calibration, validation, biological spore testing
and preventive maintenance.
4.14.3 A service agreement/contract which determines what items are agreed to be processed for
sterilization. It should detail how processes are to be managed, what methods of
decontamination cleaning, drying, packaging materials and sterilization will be used for each
type of item.
4.14.4 Sterilizer description, method of sterilizing, sterilizing agent, process challenging devices used,
cycle time and temperature parameters, for each method used. HCO should verify that these
are satisfactory for the items being sent.
4.14.5 Tracking methods to indicate records of sterilization load batches, records of batches for HCO
items, an identifying batch number for patient records and a detailed recall protocol should
there be a failure of a cycle or a failed test during performance compliance e.g. biological
testing.
4.14.6 Transportation methods for collection/delivery. Detailed outline of steps taken and items used
to ensure there is no cross contamination or breach of sterility and the frequency of collection.
4.14.7 A written description of the decontamination process used for transport boxes.
4.15 Endoscopy Management- High-Level Disinfection of Endoscopes
4.15.1 Endoscopes fall into 2 main categories: (Spaulding)
4.15.1.1Critical - when used in joint spaces, sterile cavities and for cutting tissue. Biopsy
forceps used for cutting tissue, brushes, alligator forceps and any instrument which
breaks the mucosal barrier must be subject to a complete sterilization process.
Endoscopes inserted into sterile body cavities are to be sterile at the time of use e.g.
operating telescopes used during surgery, cystoscopes and bronchoscopes.
4.15.1.2Semi-critical - hollow viscera, e.g. gastroscopy and colonoscopy procedures.
4.15.2 In general, endoscope disinfection or sterilization with a liquid chemical sterilant involves five
steps after leak testing:
4.15.2.1Clean: mechanically clean internal and external surfaces, including brushing internal
channels and flushing each internal channel with water and a detergent or enzymatic
cleaners (leak testing is recommended for endoscopes before immersion).
4.15.2.2Disinfect: immerse endoscope in high-level disinfectant (or chemical sterilant) and
perfuse (eliminates air pockets and ensures contact of the germicide with the internal
channels) disinfectant into all accessible channels, such as the suction/biopsy channel
and air/water channel and expose for a time recommended for specific products.
4.15.2.3Rinse: rinse the endoscope and all channels with sterile water, filtered water
(commonly used with automated endoscope reprocessor (AERs) or tap water (i.e.,
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 18 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
high-quality potable water that meets federal clean water standards at the point of
use).
4.15.2.4Dry: rinse the insertion tube and inner channels with alcohol, and dry with forced air
after disinfection and before storage.
4.15.2.5Store: store the endoscope in a way that prevents recontamination and promotes
drying (e.g., hung vertically).
4.15.3 Design facility where endoscopes are used and disinfected to provide a safe environment for
healthcare workers and patients.
4.15.4 Proper ventilation of the processing area is essential to remove potentially toxic chemical
vapors.
4.15.5 Use air-exchange equipment (e.g., the ventilation system, out-exhaust ducts) to minimize
exposure of all persons to potentially toxic vapors. Do not exceed the allowable limits of the
vapor concentration of the chemical sterilant or high-level disinfectant (e.g., those of ACGIH
and OSHA).
4.15.6 In addition to the endoscope reprocessing steps, a protocol should be developed that ensures
the user knows whether an endoscope has been appropriately cleaned and disinfected and is
ready for patient use.
4.15.7 Appropriate Cleaning equipment and accessories should be available.
4.15.8 Flexible endoscopes can be difficult to clean and high-level disinfect or sterilized because of
intricate device design (e.g., long narrow lumens, hinges) therefore meticulous cleaning must
precede any high-level disinfection or sterilization process.
4.15.9 Immediately after use, meticulously clean the endoscope with an enzymatic cleaner that is
compatible with the endoscope. Cleaning is necessary before both automated and manual
disinfection.
4.15.10 Disconnect and disassemble endoscopic components (e.g., suction valves) as completely as
possible and completely immerse all components in the enzymatic cleaner. Steam sterilize
these components if they are heat stable.
4.15.11 Flush and brush all accessible channels to remove all organic (e.g., blood, tissue) and other
residue. Clean the external surfaces and accessories of the devices by using a soft cloth or
sponge or brushes. Continue brushing until no debris appears on the brush.
4.15.12 Use cleaning brushes appropriate for the size of the endoscope channel or port (e.g., bristles
should contact surfaces). Cleaning items (e.g., brushes, cloth) should be disposable or, if they
are not disposable, they should be thoroughly cleaned and either high-level disinfected or
sterilized after each use.
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 19 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.15.13 Discard enzymatic cleaners (or detergents) after each use because they are not microbicidal
and, therefore, will not retard microbial growth.
4.15.14 Process endoscopes (e.g., arthroscopes, cystoscope, and laparoscopes) that pass through
normally sterile tissues using a sterilization procedure before each use; if this is not feasible,
provide at least high-level disinfection. High-level disinfection of arthroscopes, laparoscopes,
and cystoscopes should be followed by a sterile water rinse.
4.15.15 Phase out endoscopes that are critical items (e.g., arthroscopes, laparoscopes) but cannot be
steam sterilized. Replace these endoscopes with steam sterilizable instruments when feasible.
4.15.16 Mechanically clean reusable accessories inserted into endoscopes (e.g., biopsy forceps or other
cutting instruments) that break the mucosal barrier (e.g., ultrasonically clean biopsy forceps)
and then sterilize these items between each patient.
4.15.17 Use ultrasonic cleaning of reusable endoscopic accessories to remove soil and organic material
from hard-to-clean areas.
4.15.18 Process endoscopes and accessories that contact mucous membranes as semi-critical items,
and use at least high-level disinfection after use on each patient.
4.15.19 Use an FDA-cleared sterilant or high-level disinfectant for sterilization or high-level
disinfection. When using FDA-cleared high-level disinfectants, use manufacturers’
recommended exposure conditions. Certain products may require a shorter exposure time.
4.15.20 Select a disinfectant or chemical sterilant that is compatible with the device that is being
reprocessed. Avoid using reprocessing chemicals on an endoscope if the endoscope
manufacturer warns against using these chemicals because of functional damage.
4.15.21 Completely immerse the endoscope in the high-level disinfectant, and ensure all channels are
perfused.
4.15.22 After high-level disinfection, rinse endoscopes and flush channels with sterile water, filtered
water, or tap water to prevent adverse effects on patients associated with disinfectant
retained in the endoscope (e.g., disinfectant induced colitis). Follow this water rinse with a
rinse with 70%-90% ethyl or isopropyl alcohol.
4.15.23 After flushing all channels with alcohol, purge the channels using forced air to reduce the
likelihood of contamination of the endoscope by waterborne pathogens and to facilitate drying.
4.15.24 Hang endoscopes in a vertical position to facilitate drying.
4.15.25 Store endoscopes in a manner that will protect them from damage or contamination.
4.15.26 Sterilize or high-level disinfect both the water bottle used to provide intra procedural flush
solution and its connecting tube at least once daily. After sterilizing or high-level disinfecting
the water bottle, fill it with sterile water.
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 20 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.15.27 Maintain a log for each procedure and record the following: patient’s name and medical record
number (if available), procedure, date, endoscopist, system used to reprocess the endoscope (if
more than one system could be used in the reprocessing area), and serial number or other
identifier of the endoscope used.
4.15.28 Make PPE (e.g., gloves, gowns, eyewear, face mask or shields, respiratory protection devices)
available and use these items appropriately to protect staff from exposure to both chemicals
and microorganisms (e.g., HBV).
4.15.29 If using an automated endoscope reprocessor (AER), place the endoscope in the reprocessor
and attach all channel connectors according to the AER manufacturer’s instructions to ensure
exposure of all internal surfaces to the high-level disinfectant/chemical sterilant. Automated
endoscope reprocessors (AER) are preferred over manual reprocessing as they automate and
standardize several important reprocessing steps and offer several advantages.
4.15.30 Ensure the endoscope can be effectively reprocessed in the AER. Also, ensure any required
manual cleaning/disinfecting steps are performed (e.g., elevator wire channel of
duodenoscopes might not be effectively disinfected by most AERs).
4.15.31 Do not use the carrying case designed to transport clean and reprocessed endoscopes outside
of the healthcare environment to store an endoscope or to transport the instrument within
the healthcare environment.
4.15.32 If a cluster of endoscopy-related infections occurs, investigate potential routes of transmission
(e.g., person-to-person, common source) and reservoirs.
4.15.33 Report outbreaks of endoscope-related infections to persons responsible for institutional
infection control and risk management and take appropriate actions.
4.15.34 Compare the reprocessing instructions provided by both the endoscope’s and the AER’s
manufacturer’s instructions and resolve any conflicting recommendations.
4.15.35 To detect damaged endoscopes, test each flexible endoscope for leaks as part of each
reprocessing cycle. Remove from clinical use any instrument that fails the leak test, and repair
this instrument.
4.15.36 Always check with device manufacturers for information about germicide compatibility with
the device. If the germicide is FDA-cleared, then it is safe when used according to label
directions; however, scientific literature should be review for newly available data regarding
human safety or materials compatibility.
4.15.37 A vast selection of AER’s are available on the market and a variety of chemicals are
recommended by the Manufacturer for operating them. Manufacturer’s instructions for the
use of the selected AER is the foremost guide to follow, to ensure correct performance.
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 21 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.15.38 Manual cleaning of flexible endoscopes is a preliminary and accompanying process to the use
of an AER. Manual cleaning, leak testing of the endoscope and the use of an AER, ensures
correct cleaning, checking and disinfection of flexible endoscopes in between patient use.
4.15.39 Leak testing verifies the patent integrity of the endoscope sheath after each use.
4.15.40 Dry leak test: performed prior to wet immersion
4.15.41 Immersion leak test: performed when the endoscope is being immersed.
An endoscope failing a dry leak test should not undergo an immersion leak test. A well
ventilated adequately sized processing area with a delineated clean and soiled area with 2
sinks, adequate plumbing, storage cabinets and equipment to enable proper cleaning and
processing.
4.15.42 Rinsing endoscopes and flushing channels with sterile water, filtered water, or tap water will
prevent adverse effects associated with disinfectant retained in the endoscope (e.g.,
disinfectant-induced colitis). Items can be rinsed and flushed using sterile water after high-
level disinfection to prevent contamination with organisms in tap water, such as
nontuberculous mycobacteria, Legionella, or gram-negative bacilli such as Pseudomonas.
Alternatively, a tap water or filtered water (0.2μ filter) rinse should be followed by an alcohol
rinse and forced air drying.
4.15.43 Forced-air drying markedly reduces bacterial contamination of stored endoscopes, most likely
by removing the wet environment favorable for bacterial growth.
4.15.44 After rinsing, items should be dried and stored (e.g., packaged) in a manner that protects them
from recontamination.
4.15.45 Water quality used for cleaning is important and consideration to water testing and recording
should be given to ensure mineral content is not destructive to surfaces.
4.16 Staff Training, Education and Recordkeeping:
4.16.1 Inform each worker of the possible health effects of his or her exposure to infectious agents
(e.g., hepatitis B virus [HBV], hepatitis C virus, human immunodeficiency virus [HIV]), and/or
chemicals. The information should be consistent with Occupational Safety and Health
Administration (OSHA) requirements and identify the areas and tasks in which potential
exists for exposure.
4.16.2 Staff performing sterilization must be competent and well trained and the certificates of
trainings must be maintained in their staff files.
4.16.3 Staff must be aware of Standard Precautions and Infection Control principles.
4.16.4 Educate health-care workers in the selection and proper use of personal protective equipment
(PPE).
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 22 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
4.16.5 Provide comprehensive and intensive training for all staff assigned for sterilization to ensure
they understand the importance of reprocessing these instruments.
4.16.6 Achieve and maintain competency of the staff by:
4.16.6.1providing hands-on training according to the institutional policy for reprocessing
critical and semi critical devices;
4.16.6.2supervising all work until competency is documented for each reprocessing task;
4.16.6.3conducting competency testing at beginning of employment and regularly thereafter
(e.g., annually); and
4.16.6.4reviewing the written reprocessing instructions regularly to ensure they comply with
the scientific literature and the manufacturers’ instructions.
4.16.7 Provide personnel assigned to reprocess endoscopes with device-specific reprocessing
instructions to ensure proper cleaning and high-level disinfection or sterilization. Require
competency testing on a regular basis (e.g., beginning of employment, annually) of all
personnel who reprocess endoscopes.
4.16.8 Educate all personnel who use chemicals about the possible biologic, chemical, and
environmental hazards of performing procedures that require disinfectants.
4.16.9 Ergonomics training should be given to the staff so that ergonomics is considered in the
selection of trolleys and containers to ensure the risk of injury to staff during manual handling
is reduced. Ease of transfer and handling of containers, height and weight transfer of items to
bench tops to reduce bending and lifting are important.
4.16.10 Individual training records, their core competencies and any other training, should be
maintained and updated regularly. Designated personnel are responsible for maintaining these
records.
4.16.11 Autoclave user training shall be given by the trainer/sterilizer manufacturer and the training
must be documented.
4.16.12 HCO shall have policies in place providing a permanent record of flexible endoscope use and
reprocessing, and a system to track endoscopes and patients, including recording the
endoscope number in the patient record.
4.16.13 Handling of flexible endoscopes, their accessories and associated equipment must be done by
staff trained and qualified to do so. Due to the extent of the procedures involved, mastery of
dedicated protocols are recommended to understand the complexity of endoscope care.
4 COMMUNICATION (check all that apply)
☒ Announcement
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 23 / 30POLICY & GUIDELINE – Sterilization: Reprocessing of Reusable Items for
Sterilization
☐ Awareness
☐ Training
☒ Other specify: website upload
5 DEFINITIONS & ABBREVIATIONS
5.2 Aseptic: Free from disease‑causing contaminants
5.3 ACGIH: American Conference of Governmental Industrial Hygienists. ACGIH is a scientific
organization that studies occupational and environmental health issues.
5.4 Bioburden: -The number of viable microorganisms in or on an object entering a sterilization process.
-The population of viable organisms on materials, instruments, linen, etc., is referred to as the
“bioburden”, or initial contamination.
5.5 Biocides: Biocides are antimicrobial chemicals and are used to kill (in disinfectants/sterilants) or
inhibit (preserve as preservatives) microorganisms. Some may also be used as hydrolysis (soil
breakdown).
5.6 Biofilm: A thin, usually resistant layer of microorganisms (e.g. bacteria) that forms on and coats
various surfaces
5.7 Calibration: The process of calibrating a Sterilizer is to measure and ensure that all temperature
pressure and time parameters displayed or used within any sterilization cycle are within allowed
deviations as defined under Australian Standards.
5.8 Cleaning:
- Consists of removing organic and non‑organic substances through the physical‑chemical action of a
detergent combined with a brushing and rinsing action.
- is the removal of visible soil (e.g., organic and inorganic material) from objects and surfaces and
normally is accomplished manually or mechanically using water with detergents or enzymatic
products. Thorough cleaning is essential before high-level disinfection and sterilization because
inorganic and organic materials that remain on the surfaces of instruments interfere with the
effectiveness of these processes.
5.9 Contamination: The presence of a minor and unwanted constituent (contaminant) on a material or in
a physical body
5.10 Cross‑infections: are infections transmitted from one patient to another through contaminated
equipment, instruments and materials.
5.11 CSSD: Central Sterile Services Department
Identifier: DHCR/PP/HCO/012/01 Issue Date: 11/12/2018 Review Date: 11/12/2020 Page Nu: 24 / 30You can also read