SATELLITE SYMPOSIUM DISCLOSURE - MSVIRTUAL2020 INDUSTRY SUPPORTED
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

MSVirtual2020 Industry Supported
Satellite Symposium Disclosure
This activity is an independently supported
Satellite Symposium not included in the MSVirtual2020
accredited program. CME certification provided by
Penn State College of Medicine.
Please note by viewing the symposium, you agree to
share contact details with the symposium organizer.
PRESENTED AT Disclosure slide is property of MSVirtual2020. Permission required for reuse.
#MSVirtual2020
What’s New in Relapsing MS? Expert Perspectives on Pathogenesis, Targeting B Cells for Treatment, and Advances in Disease-State Monitoring

Disclosures Xavier Montalban, MD, PhD, FEAN, FAAN, has a financial interest/relationship or affiliation in the form of: Consultant and/or Advisor for Actelion Pharmaceuticals Ltd; Alexion Pharmaceuticals, Inc.; Biogen; Celgene Corporation; EMD Serono, Inc.; F. Hoffman-La Roche Ltd.; Genzyme Corporation; Immunic, Inc.; MedDay Pharmaceuticals; Merck & Co., Inc.; Mylan Inc.; NervGen Pharma Corp.; Sanofi; Teva Pharmaceutical Industries Ltd.; and TG Therapeutics. Grant/Research Support from Actelion Pharmaceuticals Ltd; Alexion Pharmaceuticals, Inc.; Biogen; Celgene Corporation; EMD Serono, Inc.; F. Hoffman-La Roche Ltd.; Genzyme Corporation; Immunic, Inc.; MedDay Pharmaceuticals; Merck & Co., Inc.; Mylan Inc.; NervGen Pharma Corp.; Sanofi; Teva Pharmaceutical Industries Ltd.; and TG Therapeutics. This CME activity is jointly provided by Penn State College of Medicine and PVI, PeerView Institute for Medical Education. This activity is supported by an educational grant from EMD Serono, Inc.

Disclosures Prof. Dr. med. Dr. h. c. mult. Ludwig Kappos has a financial interest/relationship or affiliation in the form of: Consultant and/or Advisor for Actelion Pharmaceuticals Ltd.; Allergan plc; Almirall, S.A; Baxalta; Bayer AG; Biogen; Celgene Corporation/Receptos; CSL Behring; Desitin Arzneimittel GmbH; EXECMED; Eisai Co., Ltd.; F. Hoffmann-La Roche Ltd.; Genzyme Corporation; JT International SA; Minoryx Therapeutics SL; Merck & Co., Inc.; Novartis AG; Pfizer AG; Sanofi; Santhera Pharmaceuticals; and Teva Pharmaceutical Industries Ltd. Grant/Research Support from Bayer AG; Biogen; The European Union; Novartis AG; Inno-Suisse; Roche Research Foundations; The Swiss MS Society; and The Swiss National Research Foundation. Other Financial or Material Support from steering committees for Actelion Pharmaceuticals Ltd.; Allergan plc; Almirall, S.A; Baxalta; Bayer AG; Biogen; Celgene Corporation/Receptos; CSL Behring; Desitin Arzneimittel GmbH; EXECMED; Eisai Co., Ltd.; F. Hoffmann-La Roche Ltd.; Genzyme Corporation; JT International SA; Minoryx Therapeutics SL; Merck & Co., Inc.; Novartis AG; Pfizer AG; Sanofi; Santhera Pharmaceuticals; and Teva Pharmaceutical Industries Ltd. License fees for Neurostatus-UHB products. This CME activity is jointly provided by Penn State College of Medicine and PVI, PeerView Institute for Medical Education. This activity is supported by an educational grant from EMD Serono, Inc.

Disclosures Amit Bar-Or, MD, FRCPC, has a financial interest/relationship or affiliation in the form of: Consultant and/or Advisor for Atara Biotherapeutics, Inc.; Biogen; Celgene Corporation/Receptos Inc.; F. Hoffmann-La Roche Ltd/Genentech, Inc.; Janssen Pharmaceuticals, Inc./Actelion Pharmaceuticals Ltd; Merck & Co., Inc./EMD Serono, Inc.; Novartis Pharmaceuticals Corporation; and sanofi-aventis U.S. LLC/Genzyme Corporation. Grant/Research Support from Biogen; EMD Serono, Inc.; F. Hoffmann-La Roche Ltd/Genentech, Inc.; and Novartis Pharmaceuticals Corporation. This CME activity is jointly provided by Penn State College of Medicine and PVI, PeerView Institute for Medical Education. This activity is supported by an educational grant from EMD Serono, Inc.

Visit us at
PeerView.com/MSLive2020
• Rewatch this afternoon’s web broadcast online (available within
the next 24 hours) or watch for the onDemand version in the
coming weeks
• Download the slides and Practice Aids Join the
conversation on
• Apply for CME credit Twitter @PeerView
Need more information?
Send an email to live@PeerView.com
MS Clinical Characteristics and
Patterns of Disease Progression
Xavier Montalban, MD, PhD, FEAN, FAAN
Chairman and Director
Neurology-Neuroimmunology Department & Neurorehabilitation
Multiple Sclerosis Centre of Catalonia (Cemcat)
Vall d’Hebron Barcelona Hospital Campus
Barcelona, Spain
MS Phenotype Descriptions for Disease Courses1
Relapsing Disease Progressive Disease
Progressive accumulation
Clinically Not activea of disability from onset
isolated Activea and with progressionc
syndrome Activea,b
(CIS) (Primary Progressive)
Active but without progression
Progressive Disease Not active but with progression
Relapsing- Not activea (Secondary Progressive) Not active and without
remitting progression (stable disease)
disease Progressive accumulation
(RRMS) Activea of disability after
relapsing course
a Activity determined by clinical relapses and/or MRI activity (contrast-enhancing lesions; new or unequivocally enlarging T2 lesions assessed at least annually); if
assessments are not available, activity is “indeterminate.” b CIS, if subsequently clinically active and fulfilling current multiple sclerosis (MS) diagnostic criteria, becomes
relapsing-remitting MS (RRMS). c Progression measured by clinical evaluation, assessed at least annually. If assessments are not available, activity and progression
are “indeterminate.”
1. Lublin FD et al. Neurology. 2014;83:278-286.
MS Clinical Courses1,2
RRMS SPMS PPMS
Disability
Disability
Disability
Time Time Time
Relapse RRMS
Active (relapse or new MRI activity)
Active without worsening Active (relapse or new MRI activity) with progression
with progression
Worsening Not active without progression (stable)
(incomplete recovery from relapse) Active (relapse or MRI activity)
without progression Not active with progression
Stable without activity
Not active with progression Active without progression
New MRI activity
Not active without progression (stable) New MRI activity
New MRI activity
1. Lublin FD et al. Neurology. 2014;83:278-286. 2. https://www.nationalmssociety.org/What-is-MS/Types-of-MS.
2020 Clarification: Recommended Terms and Time Frames1
Recommended
Term Definition
Time Frame for Evaluation
Active disease Clinical: relapses, acute or subacute episodes of new or Annually (but can be another time
increasing neurologic dysfunction, followed by full or partial frame, as long as it is specified)
recovery, in the absence of fever or infection
and/or
Imaging: gadolinium-enhancing lesions or new or Annually (but can be another time
unequivocally enlarging T2 lesions frame, as long as it is specified)
Progressing Accrual of disability, independent of any relapse activity, Annually by clinical assessment
disease or disease during the progressive phase of MS (PPMS or SPMS) (but can be another time frame,
progression as long as it is specified)
Worsening disease Any increase in impairment/disability irrespective of
whether it has resulted from residual deficits following a
Not required
relapse or (increasing) progressive disability during the
progressive phase of the illness
1. Lublin FD et al. Neurology. 2020;94:1088-1092.Research Needed to Better Understand
and Define Phenotypes (2013)1
• Longitudinal studies to better associate imaging with phenotypes and transitions
between subtypes over time
• Imaging studies of correlation between phenotypes and measures of tissue damage
• Clinical and imaging assessment of RIS to speed MS diagnosis
• Identification of optimal assessment time frames
• Cohort studies
– Importance of clinical and imaging activity in mid- and long-term outcomes
– Impact of degree of acute relapse recovery on outcomes and phenotype
descriptions
– Potential fluid-borne markers
• Exploration of electrophysiologic assessments and patient-reported outcomes relative
to clinical course
1. Lublin FD et al. Neurology. 2014;83:278-286.Imaging That!
Imaging Techniques
for MS Assessment
Prof. Dr. med. Dr. h. c. mult. Ludwig Kappos
Chair Neurology
Departments of Medicine, Biomedicine,
Clinical Research and Biomedical Engineering
University Hospital Basel
Basel, SwitzerlandMRI Provides More Information for MS Management1
MRI Roles in MS Assessment1 Deeper Information With MRI2
• Diagnostic component
Detectable/measurable
in real-world setting
• Staging and disease progression Relapses
Disability
Clinical assessments
– Baseline tissue damage and New or enlarged T2 lesions
Gd-enhancing lesions Conventional MRI
subsequent repair Black holes
– Lesion burden Cortical lesions
Brain volume
Advanced MRI
NAWM
– Assessment of prognosis/long- NAGM
Neurofilaments
term disability risk Cytokines CSF/serum
No metabolites biomarkers
• Monitoring of treatment response
Neurotrophic factors
1. Wattjes MP et al. Nat Rev Neurol. 2015;11:597-606. 2. Gasperini C et al. Neurology. 2019;92:180-192.2017 McDonald Diagnostic Criteria1
• DIS by MRI: ≥1 T2 hyperintense lesions in
≥2 of 4 areas (periventricular, cortical or
Data Needed juxtacortical, infratentorial, and spinal
Attacks Lesions cord)
for Diagnosis
≥2 ≥2 None • DIT by MRI: simultaneous GAD-
enhancing and nonenhancing lesions or
≥2 1 + historical None new lesion on follow-up
evidence of DIS
MRI updates versus 2010
≥2 1 DISa • Inclusion of symptomatic, as well as
1 ≥2 DITb asymptomatic, lesions in determining DIS
and DIT
1 1 DISa and DITb
• Inclusion of cortical, as well as
juxtacortical, lesions in determining DIS
• DIS with OB+ are also diagnostic
aDemonstrated by attack at implicating a different site or MRI. b Demonstrated by attack implicating a different site, MRI or OCB.
1. Thompson AJ et al. Lancet. 2018;17:162-173.Conventional MRI for Monitoring
Disease State and Treatment Effects1
• Conventional MRI
– T2-weighted sequences
– Contrast-enhanced T1-weighted sequences
• Active MRI lesions are detected more frequently than clinical relapses
– 5- to 10-fold more
– Especially in RRMS
• MRI lesions suggest insufficient biological effect of treatment
1. Gasperini C et al. Neurology. 2019;92:180-192.Recent MAGNIMS Position Paper:
Monitoring Treatment Response1
Clinical Axis Clinical Axis Clinical Axis
Neurodegeneration Neurodegeneration Neurodegeneration
Disability did
not worsen
Disability did
not worsen
Disability
worsen
did not
CSF/Serum
Axis
No MRI MRI No MRI No loss of MRI
NEDA-3 NEDA-4
activity Axis activity brain volume Axis MRI
No MRI NEDA-5 No loss of
activity brain volume Axis
No Relapse
No Relapse
Relapse
No
Inflammation Inflammation Inflammation
Recommendations and future directions
• Adopt NEDA for future clinical trials
• Consider expanding NEDA with other activity indicators
• For real-world applicability, consider MEDA (eg,Recent MAGNIMS Consensus Statement:
Recommendations for Atrophy Measures in Clinical Practice1
Defining and Predicting Monitoring
Clinical Implementation
MS Severity Therapeutic Effect
• Measurement of global brain • Whole brain atrophy over ≥12 • Appropriate management of
volume to gauge disease months as a clinical trial scanner-related factors to
burden endpoint ensure reliability
• Measurement of cervical cord • Gray matter volume loss as an • Appropriate management of
area loss outcome measure (expected) physiological and MS-related
factors
• Further research: relevance of • Re-baseline at 6 to 12 months • Use of software approved as a
gray matter volume changes, to limit pseudoatrophy impact medical device and evaluated in
including thalami, basal ganglia, MS—further validation of
and specific cortical areas existing software
• Further research: association
between treatment effects on
brain atrophy and disability;
spinal cord atrophy
1. Sastre-Garriga J et al. Nat Rev Neurol. 2020;16:171-182.Association of Deep Gray Matter and Thalamic Volume Loss
With Disability Progression in MS1
• Longitudinal study
– 6 years
– Participants: RRMS (n = 179), SMPS (n = 50)
• Thalamus and striatum volumes were associated with EDSS at baseline
• Only thalamic volume loss was associated with EDSS change at follow-up (anterior
nucleus, pulvinar, ventral anterior nuclei)
• MS phenotype and annual rates of volume loss (thalamus, bentral lateral nucleus)
predicted worsening disability
1. Magon S et al. J Neurol. 2020;267:1536-1546.Emerging MRI Approaches1
Normal-appearing WM: Leptomeningeal infiltrates
1H-MRS; TSC; (ELFS): high and ultra-high
DWI/NODDI; MT imaging field MRI (post-contrast 3D
(eg, qMT, ihMT); MWI T2-FLAIR)
WM lesion: peripheral rim Cortical lesions: expanded
(susceptibility weighted inclusion criteria (McDonald
imaging/iron deposits), criteria); networks
SELs; CVS approaches; fMRI
Normal-appearing GM:
registration techniques for
PBVCs; spatiotemporal
pattern/advanced MRI
sequences
1. Cortese R et al. Ther Adv Neurol Disord. 2019;12:1-15.Central Vein Sign (CVS): MS Diagnosis
• Criteria for use of CVS in MS diagnosis CVS in Patient With MS
have been proposed (eg, >40% of
lesions)1,2
• Proportion of lesions with CVS3
− RRMS: 50%
− CIS: 60%
− NMSOD: 0%
− SLE: 16%
− Migraine/cluster headache: 9%
• Potential for MS diagnosis in CIS, RIS, or
atypical neurological presentations, but
more trials are needed1,2
3D
1. Sorensen PS et al. Brain. 2020 July 24 [Epub ahead of print]. 2. Vattoth S et al. Curr Probl Diagn Radiol. 2020 June 29 [Epub ahead of print]. 3.
Sinnecker T et al. JAMA Neurol. 2020;76:1446-1456.Peripheral Rim (Susceptibility-Weighted Imaging and
Paramagnetic Rims): MS Progression
• Chronic active lesions detected
using susceptibility-based MRI1-4
• Non-gadolinium enhancing, with
paramagnetic rim1-3 Imaging of Lesion With Paramagnetic Rim4
− Indicate demyelination
(edge), remyelination failure,
and axonal degeneration
− Rims have iron-containing,
activated macrophages,
and microglia
− Correlate with disability
− More common in PMS
than RRMS
1. Sorensen PS et al. Brain. 2020 July 24 [Epub ahead of print]. 2. Absinta M et al. JAMA Neurol. 2019;76:1474-1483. 3. Matthews PM. Nat Rev
Neurol. 2019;15:582-593. 4. Bagnato F et al. J Neuroimaging. 2020;30:251-266.Leptomeningeal Enhancement (LME)
Ectopic lymphoid follicle-like structures (ELFs), identified through LME, are associated more with cortical
atrophy and disability, and have been considered to be more prevalent in progressive MS1
7T MRI Cerebral LME in RRMS2 ELFs in Progressive MS3
• Gadolinium-enhanced 3D MP2RAGE and • Autopsy tissue (UK MS Tissue Bank); 11 PPMS,
FLAIR (Fig: pre- and post-contrast) 22 SPMS, 2 Parkinson’s disease, 15 healthy
• LME identified in 20/30 individuals with RRMS control
• Associated with longer disease duration, • More ELFs in SPMS samples (Fig)
increased cortical and thalamic lesion number • B cells and lack of regulatory T cells identified in
and volume the ELFs P = .032
100 Score 1
80 Score 2
Percentage
Score 3
Higher score 60
indicates more 40
lymphocytes 20
0
SP PP SP PP -MS
Brain Spinal Cord
1. Cortese R et al. Ther Adv Neurol Disord. 2019;12:1-15. 2. Zurawski J et al. Mult Scler. 2020;26:177-187. 3. Bell L et al. Front Immunol. 2020;10:3090.Case-Based Discussion Assessment of MS Disease Status
Clinical Case 33-year-old male Born in Venezuela; living in Barcelona for the last 1.5 years Smoker Ex-alcoholic Major depressive syndrome with several suicide attempts Gastric bypass for morbid obesity He was admitted in our hospital for an important gait problem, and bradyphrenia
Clinical Case Continued
OB +
Ab. Anti AQ4 negative
Ab. Anti MOG negativeClinical Case Continued
10
RM cerebral 07/19
9 ↑ Volumen lesional, patrón tipo Baló
8
7
EDSS Score
PLEX
6
5
IVMP
4
3
2
1
06/2019 07/2019 08/2019 09/2019 10/2019 11/2019 12/2019 01/2020 02/2020 03/2020 04/2020Clinical Case Discussion • What MRI features could have informed the diagnosis and treatment? • How would identification of these features affect treatment?
Current Perspectives
on MS Pathogenesis
Amit Bar-Or, MD, FRCPC
Melissa and Paul Anderson Distinguished Professor
Director, Center for Neuroinflammation and Experimental Therapeutics
Chief, Multiple Sclerosis Division, Department of Neurology
Perelman Center for Advanced Medicine (PCAM)
University of Pennsylvania
President, International Society for Neuroimmunology
Philadelphia, PennsylvaniaOverview of Current Perspectives on MS Pathogenesis
Overview of Current Perspectives on MS Pathogenesis • Historical perspectives: T cells as main mediators of MS pathogenesis
Overview of Current Perspectives on MS Pathogenesis
• Historical perspectives: T cells as main mediators of MS pathogenesis
• Emerging concepts in MS immune pathogenesis (evolving landscape)
– Updated understanding of roles of pathogenic elements
Cell types: B cells, T cells, myeloid cells; microglia, astrocytes
Cell interactions: through cytokines, receptors
– Distinguish roles of these elements in relapsing and progressive MSOverview of Current Perspectives on MS Pathogenesis
• Historical perspectives: T cells as main mediators of MS pathogenesis
• Emerging concepts in MS immune pathogenesis (evolving landscape)
– Updated understanding of roles of pathogenic elements
Cell types: B cells, T cells, myeloid cells; microglia, astrocytes
Cell interactions: through cytokines, receptors
– Distinguish roles of these elements in relapsing and progressive MS
• Implications to patient care and future therapeuticsSimplified Model of MS Immunopathogenesis
Periphery
BBB
CNSSimplified Model of MS Immunopathogenesis
1. Activation
B cell
Th
Periphery
BBB
CNSSimplified Model of MS Immunopathogenesis
1. Activation
B cell
Th
2. Adhesion
Periphery
BBB
CNSSimplified Model of MS Immunopathogenesis
1. Activation
B cell
3. Attraction
Th
2. Adhesion
Periphery
BBB
CNSSimplified Model of MS Immunopathogenesis
1. Activation 4. Invasion
B cell
3. Attraction
Th
2. Adhesion
Periphery
BBB
CNSSimplified Model of MS Immunopathogenesis
1. Activation 4. Invasion
B cell
3. Attraction
Th
B cell
2. Adhesion
5. Reactivation
6. Neural/glial
responses
Periphery
BBB
CNST Cells as Main Mediators of MS Immune Pathogenesis
1. Activation 4. Invasion
B cell
3. Attraction
Th
B cell
2. Adhesion
5. Reactivation
6. Neural/glial
responses
Periphery
BBB
CNSCellular Interactions Drive MS Immune Pathogenesis
1. Activation 4. Invasion
B cell
3. Attraction
Th
B cell
2. Adhesion
5. Reactivation
6. Neural/glial
responses
Periphery
BBB
CNSCellular Interactions Drive MS Immune Pathogenesis
1. Activation 4. Invasion
B cell
3. Attraction
Th
B cell
Relapsing 2. Adhesion
5. Reactivation
biology
6. Neural/glial
responses
Periphery
BBB
CNSCellular Interactions Drive MS Immune Pathogenesis
1. Activation 4. Invasion
B cell
3. Attraction
Th
B cell
Relapsing 2. Adhesion
5. Reactivation
biology
6. Neural/glial
responses
Periphery
BBB
Progressive
CNS
biologyCellular Interactions Drive MS Immune Pathogenesis
1. Activation 4. Invasion
B cell
3. Attraction
Th
B cell
Relapsing 2. Adhesion
5. Reactivation
biology
6. Neural/glial Infiltrating
responses immune cells;
Periphery microglia, astrocytes
BBB
Progressive
CNS
biologyOverview of Current Perspectives on MS Pathogenesis
• Historical perspectives: T cells as main mediators of MS pathogenesis
• Emerging concepts in MS immune pathogenesis (evolving landscape)
– Updated understanding of roles of pathogenic elements
Cell types: B cells, T cells, myeloid cells; microglia, astrocytes
Cell interactions: through cytokines, receptors
– Distinguish roles of these elements in relapsing and progressive MS
• Implications to patient care and future therapeuticsCellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
Myeloid cells
‘M2’: IL-10 (M2a-c)
‘M1’: IL-12 / IL-23
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
Myeloid cells
‘M2’: IL-10 (M2a-c)
‘M1’: IL-12 / IL-23
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
? CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
B cells Myeloid cells
‘M2’: IL-10 (M2a-c)
‘M1’: IL-12 / IL-23
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
Traditional CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
View
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
B cells Myeloid cells
‘M2’: IL-10 (M2a-c)
‘M1’: IL-12 / IL-23
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
Traditional CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
View
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
B cells Myeloid cells
‘M2’: IL-10 (M2a-c)
‘M1’: IL-12 / IL-23
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
Traditional CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
View
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
B cells Myeloid cells
‘M2’: IL-10 (M2a-c)
‘M1’: IL-12 / IL-23
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
Traditional CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
View
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
B cells Myeloid cells
MS: Abnormal CNS ‘M2’: IL-10 (M2a-c)
antibody production ‘M1’: IL-12 / IL-23
and deposition, OCB
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
B cells, PB/PC Myeloid cells
Breg: IL-10 / IL-35 ‘M2’: IL-10 (M2a-c)
Beff: LT / TNFa ‘M1’: IL-12 / IL-23
IL-6 / GM-CSF
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
B cells, PB/PC Myeloid cells
Breg: IL-10 / IL-35 ‘M2’: IL-10 (M2a-c)
Beff: LT / TNFa ‘M1’: IL-12 / IL-23
IL-6 / GM-CSF
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
B cells, PB/PC Myeloid cells
Breg: IL-10 / IL-35 ‘M2’: IL-10 (M2a-c)
Beff: LT / TNFa ‘M1’: IL-12 / IL-23
IL-6 / GM-CSF
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
B cells, PB/PC Myeloid cells
Breg: IL-10 / IL-35 ‘M2’: IL-10 (M2a-c)
Beff: LT / TNFa ‘M1’: IL-12 / IL-23
IL-6 / GM-CSF
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
Anti-CD20
B cells, PB/PC Myeloid cells
Breg: IL-10 / IL-35 ‘M2’: IL-10 (M2a-c)
Beff: LT / TNFa ‘M1’: IL-12 / IL-23
IL-6 / GM-CSF
1. Li R et al. Nat Immunol. 2018;19:696-707.Cellular Immunology of Multiple Sclerosis:
Major Checkpoints Regulating Disease1
T cells
CD4+ Teff: ThIL-17; Th IL-17/IFNg; Th GM-CSF
CD8+ Teff: Conventional CD8; MAIT cells
Treg: nTreg; iTreg; CD8-suppressors
CNS-Directed
ANTIGEN-
SPECIFIC
RESPONSE
BTKi BTKi
B cells, PB/PC Myeloid cells
Breg: IL-10 / IL-35 ‘M2’: IL-10 (M2a-c)
Beff: LT / TNFa ‘M1’: IL-12 / IL-23
IL-6 / GM-CSF
1. Li R et al. Nat Immunol. 2018;19:696-707.Targeting B Cells as an Emerging
Approach for MS Treatment
Xavier Montalban, MD, PhD, FEAN, FAAN
Chairman and Director
Neurology-Neuroimmunology Department & Neurorehabilitation
Multiple Sclerosis Centre of Catalonia (Cemcat)
Vall d’Hebron Barcelona Hospital Campus
Barcelona, SpainGrowing Evidence Supports Multiple Roles
for B Cells in MS Pathophysiology1-7
Autoantibody T-Cell Activation Cytokine Formation of Ectopic
Production B cells are highly Production Follicle-Like
B-cell clones produce efficient at presenting B cells from patients Structures
antibodies in the CSF antigen to and with MS have abnormal Ectopic B-cell follicles are
and CNS activating T cells proinflammatory profiles found in the meninges of
patients with MS
1. Colombo M et al. J Immunol. 2000;164:2782-2789. 2. Qin Y et al. J Clin Invest. 1998;102:1045-1050. 3. Constant SL. J Immunol.
1999;162:5695-5703. 4. Crawford A et al. J Immunol. 2006;176(6):3498-3506. 5. Bar-Or A et al. Ann Neurol. 2010;67:452-461.
6. Lisak RP et al. J Neuroimmunol. 2012;246:85-95. 7. Uccelli A et al. Trends Immunol. 2005;26(5):254-259.Anti-CD20 Antibodies in Multiple Sclerosis1
Rituximab (RTX) Ocrelizumab (OCR) Ofatumumab (OFA) Ubilituximab (UTX)
Structure Chimeric IgG1 Humanized Recombinant Glycoengineered
(65% human) IgG1 (>90% fully human chimeric IgG1
human) IgG1
Regimen 1 g IV 300 mg IV 20 mg sc 450 mg IV
d 1 & d 15, d 1 & d 15, every 4 w d 1 & d 15,
followed followed by followed by
by 1 g 600 mg 450 mg IV
every 24 wk every 24 wk every 24 wk
Primary CDC ADCC CDC ADCC
mechanism
Mouse Mouse Mouse
of action
Human Human Human Human
Generation First Second Third Third
Glycoengineered
Immunogenicity +++ ++ + Fc ++
1. Ancau M et al. Expert Opin Biol Ther. 2019;19:829-843.Ocrelizumab: Phase 3 OPERA I and OPERA II
Pooled Study Design1,2
Open-Label Extension Screening
Double-Blind Treatment Open-Label Extension
Ocrelizumab Ocrelizumab
Screening
Dose 1: 300 mg × 2 Dose 5: 300 mg × 2
Dose 2 to 4: 600 mg × 1 Dose 6 to N: 600 mg × 1
Interferon β-1a Ocrelizumab
3x weekly Dose 5: 300 mg x 2
Dose 6 to N: 600 mg x 1
Dose 1 2 3 4 5 6 7 N
Visit
Week 0/2 12 24 36 48 60 72 84 96 0/2 12 22, 24 46, 48 70, 72 N-2, N
Safety Follow-Up B-Cell Monitoring
Duration at least 48 weeks from the date of the last infusion Duration as required
Visits every 12 weeks from the date of the last visit. Visits every 24 weeks
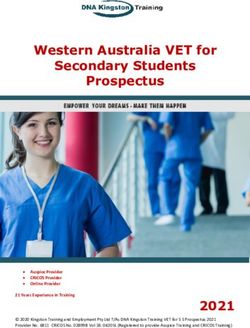
1. https://www.ncbi.nlm.nih.gov/books/NBK534377. 2. https://commons.wikimedia.org/wiki/File:Monthly_multiple_sclerosis_anim_bg.gif.OPERA I and OPERA II: Clinical Benefit of Ocrelizumab in
RRMS After 5 Years of Treatment1
ARR Over 5 Years: DBP and Years 1 to 3 of the OLE Proportion of Patients With CDP During the DBP and OLE Periods
25 IFN β-1a/OCR 600 mg (n = 829)
Proportion of Patients With CDP, %
Patients receiving IFN β-1a 44 mcg during the DBP
0.4 Patients receiving OCR 600 mg during the DBP and continuing OCR into OLE OCR 600mg/OCR 600 mg (n = 872)
Patients switching from IFN β-1a to OCR at OLE baseline
P = .001 20
Adjusted ARR
0.3 0.274
P = .001
15 DBP: HR = 0.60; P = .003
0.203
0.2
0.14
P = .8 10
0.125 P = .97 P = .7
0.098 0.103
0.081 0.081 Start of OLE: All patients treated with OCR
0.1 0.072 0.065 5
Δ = 4.31 Δ = 5.44 Δ = 4.21 Δ = 5.20
(1.27, 7.35) (1.97, 8.91) (0.35, 8.08) (1.05, 9.35)
P = .005 P = .002 P = .032 P = .014
0.0 0
713 765 623 702 594 665 570 639 Baseline 24 48 72 96 120 144 168 192 216 240
n= 829 827
Year 2 Year 3 Year 4 Year 5
Year 1 Year 2 Year 3 Year 4 Year 5 (OLE baseline) (OLE year 1) (OLE year 2) (OLE year 3)
(OLE year 1) (OLE year 2) (OLE year 3)
Time to onset of CDP, wk
• At the start of the OLE period, patients who completed the DBP either continued ocrelizumab
(OCR-OCR) or were switched from IFNβ-1a to ocrelizumab (IFN-OCR)
• Switching from IFNβ-1a to ocrelizumab was associated with a reduction in ARR; patients in both groups
maintained a reduction in ARR through 4 years of follow-up
• After 6 years of follow-up, the proportion of patients with CDP at 24 weeks remained lower in those who were
initiated to ocrelizumab earlier compared with patients who received IFNβ-1a and also showed that the
benefit of early initiated ocrelizumab was maintained compared with patients switching from IFNβ-1a
1. Hauser SL et al. Neurology. 2020 July 20 [Epub ahead of print].OPERA I and OPERA II: Total Number of T1 and T2 Lesions
in the DBP and OLE1
Patients receiving IFN β-1a 44 mcg during the DBP
T1 Gd-Enhancing Lesions
P = .001 Patients receiving OCR 600 mg during the DBP and continuing OCR into OLE
0.6
Patients switching from IFN β-1a to OCR at OLE baseline
Gd-Enhancing Lesions per
0.491
0.5 P = .001
P = .001
Total Number of T1 0.4 0.335 0.342
MRI Scana,b 0.3
0.2
0.1 0.029 0.007 0.005
0.011 0.017 0.004 0.017 0.004 0.006
0
n= 744 767 691 750 646 718 576 641 531 595 500 544
Week 24 Week 48 Week 96 Week 142 Week 190 Week 238
Year 1 Year 2 Year 3 Year ~4 Year ~5
(OLE year 1) (OLE year 2) (OLE year 3)
New or Enlarging T2 Lesions
P = .001
3 2.583
P = .001
Enlarging T2 Lesions per
Total Number of New or
2.5
2.06
2
MRI Scana,b
P = .001
1.5 1.154
0.931 P = .001
1
0.371
0.5 0.091 0.038 0.031
0.061 0.063 0.063 0.08
0
n= 747 772 694 754 650 720 580 646 536 599 505 550
Weeks 0- 24 Weeks 24-48 Weeks 48-96 Weeks 96-142 Week 142-190 Week 190-238
Year 1 Year 2 Year 3 Year ~4 Year ~5
(OLE year 1) (OLE year 2) (OLE year 3)
a DBP Week 24, DBP Year 1 and DBP Year 2 data include the ITT population; Year 3 (OLE Year 1), Year 4 (OLE Year 2), and Year 5 (OLE Year 3) data include
the OLE ITT population; clinical cut-off date: February 5, 2018. b Unadjusted rate.
1. Hauser SL et al. Neurology. 2020 July 20 [Epub ahead of print].Ofatumumab: Phase 3 ASCLEPIOS I and II Study Design1
• Double-blind, double-dummy, active comparator, controlled trial
Ofatumumab 20 mg SC once every
• Ages 18 to 55 y
4 wka plus placebo oral once daily
• Confirmed RRMS or SPMS ASCLEPIOS I (n = 465)
with activity ASCLEPIOS II (n = 481)
• EDSS score 0 to 5.5 Open label
• ≥2 relapses within 2 y before R extension
screening OR ≥1 relapse within study ≤5 y
Teriflunomide 14 mg oral once daily
1 y before screening OR
plus placebo SC once every 4 wk
T1 Gd+ lesion during year
ASCLEPIOS I (n = 462)
before randomization
ASCLEPIOS II (n = 474)
• Primary endpoint: ARR
• Secondary endpoints
− Clinical: 3-mo and 6-mo CDW, 6-mo CDI
− MRI and biomarker: Gd+ T1 lesions, new or enlarging T2 lesions, BVL, serum NfL levels
− Safety
aLoading dose: 3 weekly doses, 20 mg SC.
1. Hauser SL et al. N Engl J Med. 2020;383:546-557.ASCLEPIOS I and II:
Efficacy of Ofatumumab in RRMS1
• ASCLEPIOS I and II compared subcutaneous ofatumumab with oral teriflunomide
ARR Confirmed Disability Worsening at 3 and 6 Months
0.30 ASCLEPIOS I ASCLEPIOS II
Cumulative Event Rate, %
Kaplan-Meier Estimate of
Cumulative Event Rate, %
3-Month CDW
Adjusted ARRa
Kaplan-Meier Estimate of
20 6-Month CDW
0.25 50.5% 58.5% 24
22 18
0.25 Ofatumumab Ofatumumab
0.20 relative relative 20
Teriflunomide
16 Teriflunomide
0.22 18 15.0% 14
reduction; reduction; 16 12.0%
0.15 14 12
P < .001 P < .001 12 10.9% 10 8.1%
0.10 10 8
8
0.11 0.10 6 Risk reductionb 6
Risk reductionb
0.05 4 4
2 34.4%; P = .002 2 32.5%; P = .012
0.00 0 0
Teriflunomide Ofatumumab Teriflunomide Ofatumumab 0 3 6 9 12 15 18 21 24 27 30 33 0 3 6 9 12 15 18 21 24 27 30 33
(n = 452) (n = 454) (n = 469) (n = 469) No. at Risk Study Month No. at Risk Study Month
ARR ratio: 0.495 (95% CI, 0.374-0.654) ARR ratio: 0.415 (95% CI, 0.308-0.559) Ofatumumab 944 908 878 844 810 784 534 319 176 49 1 0 944 908 878 845 815 791 544 324 180 50 1 0
Teriflunomide 932 901 841 804 756 718 478 298 146 41 1 0 932 902 849 812 769 734 487 305 151 43 1 0
Gadolinium T1 Lesions HR = 0.656 (95% CI, 0.499-0.862) HR = 0.675 (95% CI, 0.498-0.916)
0.60 ASCLEPIOS I ASCLEPIOS II
• Ofatumumab led to significant reductions in relapse
Gd+ T1 Lesionsa
0.50
0.40 0.4523
97.5% 0.5141 93.8% • ARR average approximately one relapse every 10 years
relative relative
0.30 reduction; reduction; • Key secondary endpoints also showed benefit in patients
P < .001 P < .001
0.20 with RRMS
0.10
0.0115 0.0317 • MRI data indicated >95% reduction in focal gadolinium
0.00
Teriflunomide Ofatumumab
(n = 422) (n = 432)
Teriflunomide Ofatumumab
(n = 434) (n = 439)
lesions with ofatumumab and a similar reduction in rates
Rate ratio: 0.025 (95% CI, 0.013-0.049) Rate ratio: 0.062 (95% CI, 0.037-0.101) of new or enlarging T2 lesions
aNegative binomial regression model. b Cox regression model.
1. Hauser SL et al. N Engl J Med. 2020;383:546-557.Ublituximab: Phase 2 Multicenter Study Design1
Participants
• Had completed RDBPC
Infusion Schedule and Assessmentsa
52-wk study (TG-1101
RMS 201), which
assessed a range of UTX UTX UTX UTX UTX
UTX IV infusion speeds,
frequencies, and doses;
had received
≥3 UTX infusions
and completed all Baseline Week 12
OLE Week 48
assessments in TG- MRI
Week 4 EDSS Week 72 Week 96
1101 RMS 201; and MRI
B-cell Week 24 EDSS EDSS
were in good health with a
depletion MRI MRI MRI
stable disease
• 45 of 48 entered OLE
• Primary efficacy endpoint: responder rate (ie, median B cell depletion >95%)
• Mean age: 40 ± 10 y
a B cells and labs were assessed at weeks 0, 1, 2, 3, 4, 8,12,16, 20, 24, 28, 32, 36, 40, 44, 48, 60, 72, 84, 96; clinical assessment included EDSS and,
in addition to times noted on figure, was also assessed at 36, 60, and 80 weeks.
1. Fox E et al. Mult Scler. 2020 Apr 30 [Epub ahead of print].Ublituximab Phase 2 Study Results1
T2-Weighted Lesion Volume Change ARR at Baseline and Week 48 Proportion of Patients With
-7.3% -10.6%
no Evidence of Disease
16,000 15,410 (P = .006) 1.50 1.45 95% Reduction Activity at Week 48
Annualized Relapse Rate
(P = .002)
Mean T2 Lesion Vol (mm3)
15,000 -3.6% 1.25 No
(P = .019)
1.00 No Evidence No 24-wk
14,000 Relapses
0.75 of Clinical CDP
13,000 93% Disease 93%
0.50 87%
1,000 0.25 0.07
0 0.00 NEDA
Baseline Week 48 74%
Baseline Week 24 Week 48
No
No New/
No T1 Gd+ Evidence
Enlarging
Lesions of MRI
T2 Lesions
100% Disease
83%
83%
1. Fox E et al. Mult Scler. 2020 Apr 30 [Epub ahead of print].Ublituximab: Phase 3 ULTIMATE 1 and 2 Study Design1-3
• Phase 3, double-blind, active-control studies to assess safety and efficacy of ublituximab vs teriflunomide
in patients with RMS
• Ages 18 to 55 y Ublituximab 450 mg
• Diagnosis of RRMS or SPMS in 1-h infusion
with activity q 24 wk + oral placebo
• EDSS score 0 to 5.5 Recruitment completed
• ≥1 relapses within 1 y of R Ultimate 1: N = 549
screening OR ≥2 relapses within ULTIMATE 2: N = 545
2 y of screening OR 1 Gd+ Teriflunomide 14 mg oral
lesion during year before once daily + IV placebo
randomization q 24 wk
• Primary endpoint: ARR
• Secondary endpoints
− GD+ lesions, no.; NEDA, %; 3-mo CDW, %; patients with relapse, %; time to first confirmed relapse
1. Steinman L et al. European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS 2019). Poster P991.
2. https://clinicaltrials.gov/ct2/show/NCT03277261?term=NCT03277261&draw=2&rank=1.
3. https://clinicaltrials.gov/ct2/show/NCT03277248?term=NCT03277248&draw=2&rank=1.Rationale of BTK Inhibition in MS1-5
B Cells CNS Microglia
BCR activation Immune complex activation
Lyn Lyn
P BTK P BTK
Syk Plcγ Syk Plcγ
P P
DAG IP3 Ca2+ DAG IP3 Ca2+
• B-cell maturation
• Proliferation (NF-κB) • Microglial activation
• Autoantibody production • Pro-inflammatory cytokine secretion
• Cytokine secretion (eg, TNFα, IL-1β, IL-6)
1. Lang C et al. Eur J Med Chem. 2018;151:315-326. 2. Keaney J et al. J Neuroimmune Pharmacol. 2019;14:448-461. 3. Weber A et al. Front Immunol. 2017;8:1454.
4.Gabhann JN et al. PLoS One. 2014;8:e85834. 5. Hendricks RW et al. Nature Chem Biol. 2011;7:4-5. Figure adapted from Hendricks RW et al. Nature Chem Biol.
2011;7:4-5.Evobrutinib: Phase 2 Study Design1
Placebo (n = 54) Evobrutinib 25 mg qd
Evobrutinib 25 mg qd (n = 52)
Patients
Evobrutinib 75 mg qd (n = 53)
with RMS R Evobrutinib
(1:1:1:1:1) 75 mg qd
Evobrutinib 75 mg bid (n = 54)
Active control (dimethyl fumarate) (n = 54)
Safety
Screening follow Open label
4 weeks Blinded treatment 24 weeks Blinded extension 24 weeks up 4 extension
weeks
Visits (Week) -4 0 4 8 12 16 20 24 36 48 52
Endpoint MRI scan Blood test MRI Endpoints: Number of Gd+ T1 lesions (primary), number of T2
lesions; volume of Gd+ T1 lesions. Clinical Endpoints: ARR EDSS
1. Montalban X et al. NEJM. 2019;380:2406-2417.Results From a Phase 2 Study: Efficacy and Safety of
Evobrutinib in Relapsing Forms of MS1
Patients with relapsing MS were randomized to evobrutinib 25 mg once daily, 75 mg once daily,
75 mg twice daily, placebo, or open-label DMF
8
7 • A trend towards a reduction in ARR was seen
in patients on evobrutinib, with evidence of
6
4.78 (22.05) dose response (P = .03)
Mean (SD)
5 4.06 (8.02)
• Rates of TEAEs, including grade 3 and serious
3.85 (5.44)
4 TEAEs, were comparable with evobrutinib
3 25 and 75 mg once daily and placebo but higher
1.69 (4.69) with evobrutinib 75 mg twice daily (driven by
2 1.15 (3.70)
asymptomatic increases in liver transaminases)
1
• Evobrutinib 75 mg once daily and twice daily
0 significantly reduced T1 gadolinium-enhancing
Placebo Evobrutinib Evobrutinib Evobrutinib DMFa
25 mg QDa 75 mg QD 75 mg BID lesions per scan versus placebo
Lesion rate ratiob (95% CI)
1.45 0.30 0.44 – Evidence of a dose-response relationship was
(0.72-2.91) (0.14-0.63) (0.21-0.93)
P .2947 .0015 .0313
observed (trend test; P = .0001)
a Two patients (evobrutinib 25 mg, n = 1; dimethyl fumarate, n = 1) were considered T1 Gd+ outliers. b Based on a negative binomial model for total lesion count
(summed over available scans through week 24) that adjusts for baseline lesion activity. Scans collected within 3 weeks of high-dose corticosteroid use are considered
missing. Subjects missing all post-baseline scans have total lesion count imputed.
1. Montalban X et al. NEJM. 2019;380:2406-2417.Evobrutinib Phase 2 Study: ARR at Week 24 and Week 481
Placebo Evobrutinib 25 mg QD Evobrutinib 75 mg QD Evobrutinib 75 mg BID
Placebo/evobrutinib 25 mg QD (switch) Dimethyl fumarate
0.57
0.6 (0.30-0.97) 0.52
Unadjusted ARR (95% CI)
(0.33-0.78)
0.5
0.37 0.37
0.4 (0.17-0.70) (0.21-0.59)
0.25
0.3 0.20 (0.12-0.44)
0.13 (0.06-0.47) 0.14
0.2 0.11 (0.06-0.29)
(0.03-0.38) 0.08 (0.04-0.25)
0.1 (0.01-0.30)
0
Wk 0 - 24 Wk 0 - 48
1. Montalban X et al. NEJM. 2019;380:2406-2417.Evobrutinib:
Phase 3 Evolution RMS1 and RMS2 Study Design1,2
• Ages 18 to 55 y Evobrutinib plus
• RRMS or SPMS with activity placebo comparator
• ≥1 relapse within 2 y before screening
with 1 relapse within Open label
1 y before randomization OR ≥1 T1 Gd+
R extension
lesion within 6 mo before randomization
• EDSS score 0 to 5.5 Placebo evobrutinib plus
• EDSS score ≤2 if disease duration ≤10 y active comparatora
• Primary endpoint: ARR at week 96
• Secondary endpoints
− Time to first 12-wk and 24-wk CDP EVOLUTION RMS 1 scheduled completion: October 2026
− T1 Gd+ lesions; EVOLUTION RMS 2 scheduled completion: June 2023
− New or enlarging T2 lesions
− PROMIS MS scores at 96 wk
− AEs
Since the clinical trial was designed, the active comparator has been changed from interferon to teriflunomide.
1. https://clinicaltrials.gov/ct2/show/NCT04032158?term=NCT04032158&draw=2&rank=1.
2. https://clinicaltrials.gov/ct2/show/NCT04032171?term=NCT04032171&draw=2&rank=1.SAR442168: Phase 2 Study Design1
Primary Endpoint Primary Endpoint
SAR442168 (12 wk)
Placebo run-in
(4 weeks)
5 mg d (n = 15) • SAR442168 is an
15 mg d (n = 15)
N = 60 irreversible covalent, oral
Cohort 2
30 mg d (n = 15)
End of core study
60 mg d (n = 15)
small-molecule BTK
Primary Endpoint
S R inhibitor
SAR442168 (12 wk)
• Designed to access the
Cohort 1
Placebo run-in
5 mg d (n = 15)
15 mg d (n = 15)
(4 weeks)
N = 60
brain and spinal cord by
30 mg d (n = 15)
60 mg d (n = 15) crossing the blood–brain
LTSS
barrier
Wk 0 Wk 4 Wk 8 Wk 12 Wk 16
Images courtesy of https://commons.wikimedia.org/wiki/File:Monthly_multiple_sclerosis_anim_bg.gif.
1. https://clinicaltrials.gov/ct2/show/NCT03889639?term=NCT03889639&draw=2&rank=1.Efficacy of SAR442168 at Week 121
Primary Endpoint: Number of New Gd-Enhancing Lesions Secondary Endpoint: Number of New or Enlarging T2 Lesions
Relative change Relative change
vs placebo 56% 63% -13% -85% vs placebo -10% -37% -39% -89%
95% CI (-17%, 194%) (-42%, 356%) (-67%, 126%) (-97%, -28%) 95% CI (-57%, 86%) (-71%, 38%) (-76%, 57%) (-96%, -68%)
Number of Lesions, Mean (SD)
Number of Lesions, Mean (SD)
5 P = .0178 9 P = .0001
4
6
3
2
3
1 1.39
1.03 2.12 1.90 0.23
0.77 0.76 0.13 1.32 1.30
0 0
Placebo 5 mg 15 mg 30 mg 60 mg Placebo 5 mg 15 mg 30 mg 60 mg
SAR442168 SAR442168
Analysis Group Analysis Group
Number of Number of
59 31 31 33 31 59 31 31 33 31
patients patients
1. https://clinicaltrials.gov/ct2/show/NCT03889639?term=NCT03889639&draw=2&rank=1.SAR442168 Phase 3 Trial1 • Global, randomized, double-blind trial comparing SAR442168 to teriflunomide • N = 900 participants with relapsing forms of MS • Primary outcome: efficacy of daily SAR442168 compared to a daily dose of 14 mg teriflunomide measured by ARR • Secondary outcomes: efficacy of SAR442168 compared to teriflunomide on disability progression, MRI lesions, cognitive performance and quality of life 1. https://www.globenewswire.com/news-release/2020/06/23/2051690/0/en/Principia-Announces-First-Patient-Enrolled-in-Sanofi-s-Phase-3-Trial-of-SAR442168-in- Relapsing-Multiple-Sclerosis.html.
Case-Based Discussion The Clinical Potential of Targeting B Cells in MS
Clinical Case Revisited 33-year-old male Born in Venezuela; living in Barcelona for the last 1.5 years Smoker Ex-alcoholic Major depressive syndrome with several suicide attempts Gastric bypass for morbid obesity He was admitted in our hospital for an important gait problem, and bradyphrenia
Clinical Case Continued
10
RM cerebral 07/19
9 ↑ Volumen lesional, patrón tipo Baló
8
7
EDSS Score
PLEX
6
5
IVMP
4
3
2
1
06/2019 07/2019 08/2019 09/2019 10/2019 11/2019 12/2019 01/2020 02/2020 03/2020 04/2020Clinical Case Continued
10
9
8 OCR 300mg
IVMP MR 11/2019
7
EDSS Score
PLEX ↓ Burden
6 OCR 300mg 0 new / no active
5
IVMP
4
OCR
3 600mg
2
1
06/2019 07/2019 08/2019 09/2019 10/2019 11/2019 12/2019 01/2020 02/2020 03/2020 04/2020Clinical Case Discussion Possible Candidates for BTK Inhibitor therapy • Active naïve patients • Switching from first line for inefficacy/intolerance • Switching from second line for safety issues • After anti-CD 20 treatment in stable patients • Others
Key Takeaways for Your Clinical Practice
Remember to complete and submit your Post-Test and
Evaluation at PeerView.com/MSLive2020-Credit for CME credit.
Missed anything?
Visit us at: PeerView.com/MSLive2020
• Download slides and Practice Aids
• Watch for the onDemand version of this symposium
• Join the conversation on Twitter @PeerView
Thank you and good day.Abbreviations ADCC: antibody dependent cellular cytotoxicity CVS: central vein sign ARR: annualized relapse rate DAG: diacylglycerol BBB: blood-brain barrier DBP: double-blind phase BCR: B-cell receptor DIS: dissemination in space Beff: effector B cell DIT: dissemination in time BID: twice daily DMF: dimethyl fumarate Breg: regulatory B cell DWI: diffusion weighted imaging BTK: Bruton tyrosine kinase EDSS: expanded disability status scale BTKi: Bruton tyrosine kinase inhibitor ELFS: ectopic lymphoid follicles BVL: brain volume loss GAD: gadolinium CD: cluster of differentiation Gd: gadolinium CDC: complement-dependent cytotoxicity GM-CSF: granulocyte-macrophage colony-stimulating factor CDI: confirmed disability improvement IFN: interferon CDP: confirmed disability progression IFNγ: interferon gamma CDW: confirmed disability worsening ihMT: inhomogeneous magnetization transfer
Abbreviations
IL-10: interleukin 10 MT: magnetization transfer
IL-12: interleukin 12 MWI: myelin water imaging
IL-17: interleukin 17 NAGM: normal-appearing gray matter
IL-1β: interleukin 1 β NAWM: normal-appearing white matter
IL-23: interleukin 23 NEDA: no evidence of disease activity
IL-35: interleukin 35 NfL: neurofilament light chain
IL-6: interleukin 6 NF-κB: nuclear factor kappa-light-chain-enhancer of activated B
cells
IP3: inositol 1,4,5-trisphosphate
NMSOD: neuromyelitis optica spectrum disorder
iTreg: induced regulatory T cell
NODDI: neurite orientation dispersion and density imaging
IVMP: intravenous methylprednisolone
nTreg: natural regulatory T cell
LTSS: long-term safety study
OB: oligoclonal band
MAGNIMS: magnetic resonance imaging in multiple sclerosis
OCB: oligoclonal band
MAIT: mucosal-associated invariant T cell
OCR: ocrelizumab
MEDA: minimal evident disease activity
OLE: open-label extension
MRS: magnetic resonance spectroscopy
PB: plasma blastAbbreviations
PBVC: percentage brain volume change SPMS: secondary progressive multiple sclerosis
PC: plasma cell T2-FLAIR: T2-weighted-fluid-attenuated inversion recovery
Plcγ: phospholipase gamma TEAE: treatment-emergent adverse event
PLEX: plasma exchange Teff: effector T cell
PPMS: primary progressive multiple sclerosis Th: T-helper cell
PROMIS: Patient-Reported Outcomes Measurement Information TNFα: tumor necrosis factor alpha
System
Treg: regulatory T cell
QD: once daily TSC: tuberous sclerosis complex
qMT: quantitative magnetization transfer UTX: ublituximab
RDBPC: randomized, double-blind, and placebo-controlled WM: white matter
RIS: radiologically isolated syndrome
RMS: relapsing multiple sclerosis
SEL: slowly evolving lesion
SLE: systemic lupus erythematosusYou can also read