Safe Patient Handling and Mobility
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Supplement to
www.AmericanNurseToday.com
September 2014
Current
Topics in
Safe
Patient
Handling
and
Mobility
This supplement was funded by an
unrestricted educational grant from
Hill-Rom. Content of this supplement
was developed independently of
the sponsor and all articles have
undergone peer review according to
American Nurse Today standards.

Safe patient handling and
mobility: A call to action
Much more must be done to enhance safety for
patients and caregivers.
By Melissa A. Fitzpatrick, MSN, RN, FAAN
confluence of demographic While the intentions of manual transportation orderlies, and others
A and economic trends is
pushing us toward the per-
fect storm:
patient mobilization may be honor-
able, the effects are far from opti-
mal for all involved. There’s no such
in implementing the standards and
creating a culture of safety in their
organizations. However, only 11
• Today’s nursing workforce is thing as “safe lifting” when we use states have enacted SPHM laws
aging. The average age of the our bodies as the lifting mechanism. and these laws vary significantly.
American registered nurse is Old-school teachings about safe Much more work needs to be done
44.6. body mechanics have been proven to enhance safety for patients and
• The patients we serve are heav- invalid, and many of us must un- caregivers.
ier than ever. learn them. As nurses, we must This special report provides a
• Experts predict increases in pa- change our mindset and get in the helpful resource to caregivers as
tient acuity, age, and comor- habit of using safe patient handling they continue to practice SPHM—or
bidity. and mobility (SPHM) technology to to embark on their SPHM journey if
• Staffing issues continue to cause keep both our patients and our- they’re not already on it. National
concern. Some experts project selves safe from harm. experts share their perspectives and
the United States will be short How many times have you or a best practices to align people,
about 250,000 nurses over the colleague suffered an injury to processes, and technology to set
next 10 to 12 years. your back, shoulder, or both during the course for action. I’d like to
• Economic imperatives require us manual patient handling? How thank all of the authors who’ve con-
to move patients through the many colleagues have we lost to tributed to this special report for
healthcare delivery system more our profession because of a career- sharing their expertise and strate-
quickly to shorten stays and en- ending injury? How many millions gies, which we hope will be imple-
hance financial reimbursement. of dollars are spent on workers’ mented where you work. Please
compensation claims for employees take these best practices to heart
Any one of these trends is who’ve had patient handling and and engage your colleagues to do
cause for concern. All of them mobility injuries? Caregiver injuries the same. And please join all of us
occurring at once is cause for adversely affect staff morale, at Hill-Rom on our mission to ensure
alarm—and a call to action. staffing levels, and, ultimately, pa- SPHM. Much is at stake, and noth-
Imagine older nurses lifting heav- tient safety. Such injuries have ing is more important than your
ier, older, and sicker patients. Ob- made headlines in many communi- health and well-being—to enable
viously, all parties are at greater ties and are top of mind for health- you to continue doing what only
risk for injury. care leaders. Legislatures have tak- nurses can do. We’ve never need-
In too many cases, nurses contin- en on the issue, and in 2013 the ed nurses more than we do now.
ue to deliver care “the way we’ve American Nurses Association
Selected references
always done it.” For many, this (ANA) supported a federal bill to
American Nurses Association. Safe Patient Han-
means doing the heavy lifting need- eliminate manual patient handling, dling and Mobility: Interprofessional National
ed to mobilize patients manually in including lifting, transferring, and Standards. Silver Spring, MD: Author; 2013.
an attempt to avoid the many se- repositioning patients. That same Buerhaus PI, Auerbach DI, Staiger DO. The recent
quelae of immobility—decreased year, ANA published national inter- surge in nurse employment: causes and implica-
tions. Health Aff (Millwood). 2009;28(4):w657-68.
cardiovascular, pulmonary, integu- professional standards to guide
mentary, and psychological func- caregiving teams of nurses, physi- Melissa A. Fitzpatrick is vice-president and chief
tioning, to name a few. cal therapists, nursing assistants, clinical officer at Hill-Rom.
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 1
Current Topics in Safe Patient
Handling and Mobility
CONTENTS
1 Safe patient handling and mobility: A call to action
By Melissa A. Fitzpatrick
“The way we’ve always done it” is no longer an acceptable rationale for manual patient handling and
mobilization. We must change our mindset and embrace appropriate technology to keep ourselves and
our patients safe from harm.
4 Elements of a successful safe
patient handling and mobility
program
By John Celona
To build a successful program, identify
your facility’s specific needs, design the
program, obtain leaders’ and nurses’
commitment, and provide effective
education and training.
7 Transforming the culture:
The key to hardwiring early
mobility and safe patient
handling
By Kathleen M. Vollman and Rick Bassett
Accomplishing early patient mobility and safe handling requires a culture change, deliberate focus, staff
education, and full engagement.
11 Standards to protect
nurses from handling
and mobility injuries
By Amy Garcia
Learn about ANA’s
interprofessional national
standards on safe patient
handling and mobility,
developed by a panel of
interdisciplinary experts.
2 Current Topics in Safe Patient Handling and Mobility September 2014 www.AmericanNurseToday.com
Supplement to
www.AmericanNurseToday.com September 2014
13 Implementing a mobility assessment
tool for nurses
By Teresa Boynton, Lesly Kelly, and Amber Perez
The authors describe a nurse-driven tool you
can use at the bedside to evaluate your
patient’s mobility level and guide decisions
about patient lifts, slings, and other
technology.
17 The sliding patient: How to respond
to and prevent migration in bed
By Neal Wiggermann
Pulling patients up in bed carries a high risk
of caregiver injury. Find out how to prevent
patient migration and manage it safely when
it occurs.
20 Prepare to care for patients of size
By Dee Kumpar
Nearly a third of patient-handling injuries
involve bariatric patients. Handling and
mobilizing these patients safely requires skill
and specialized technology.
23 Developing a sling management system
By Jan DuBose
Disposable or launderable slings? In-house or outsourced laundering? These and other key decisions
require input from all departments involved.
26 Making the business case for a safe patient
handling and mobility program
By John Celona
The author explains three approaches to justifying a
safe patient handling and mobility program and presents
a decision-analysis case study.
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 3
Elements of a
successful safe patient
handling and mobility
program
Program success hinges on leaders’ and nurses’
commitment.
By John Celona, BS, JD
ince safe patient handling
S and mobility (SPHM) efforts
began more than a decade
ago, data show dramatic reduc-
tions in caregiver injuries after a
safe patient handling and mobility
(SPHM) program is implemented.
So why doesn’t every healthcare
facility have one?
The first reason is cost. An
SPHM program requires a sub-
stantial outlay. Second, SPHM
program results have been incon-
sistent. Tales abound of equipment
bought but not used because it’s
too much trouble to fetch it from
the closet, or because no one can
locate the necessary sling. Finally,
SPHM program value costs are
clear but benefits are hard to
quantify.
This article addresses these is-
sues by laying out the basic ele-
ments of a successful SPHM pro-
gram. These elements can be
divided into two broad cate-
gories—determining out what you
need and making it happen. (See
Simplifying the equation.)
Determining what you
need
Start by estimating how many pa-
tients on a given unit are totally
4 Current Topics in Safe Patient Handling and Mobility September 2014 www.AmericanNurseToday.com
Simplifying the equation
This diagram shows in broad strokes how a healthcare organization can develop and imple-
dependent on the nurse to lift or ment a safe patient handling and mobility program.
mobilize them. Then estimate how
many patients on the unit need
Determining what you need
partial assistance with mobility ac-
tivities, such as toileting or moving
from bed to chair.
For each patient category, esti-
mate the numbers and types of
mobilization each will need over
the course of an average stay.
Types of mobilization include
boosting, turning, moving from
bed to chair, assisting with ambu-
lation, and so on. For these cate-
gories and frequencies of mobi-
lization tasks, figure out how much
and what types of equipment are
needed to eliminate variation in
practice and standardize how to
safely accomplish the task.
In practice, most people devel-
op rules of thumb or use intuition
and experience rather than calcu-
lating the four types of information
described above. Also, vendors of
handling and mobility equipment
have experience in determining re- Compliance rate available, an organization can’t
quired equipment. When designing and implement- standardize a new mobilization
I’ve observed three different ap- ing an SPHM program, the compli- process, so the equipment gets
proaches to supplying the equip- ance rate is the key variable an used for relatively few mobiliza-
ment needed to mobilize patients: organization is driving. The com- tions. With higher investment lev-
• installing overhead lifts—ceiling pliance rate is defined as the num- els, using the equipment becomes
tracks to which lifting slings are ber of mobilizations for which part of caregivers’ routine, so the
attached SPHM equipment is actually used, compliance rate goes up.
• using portable lifts—floor- divided by the number of mobiliza-
mounted structures for mobiliz- tions for which it should be used. Making it happen
ing patients that can be moved The compliance rate is critical be- A successful SPHM program re-
around as needed cause it drives program benefits. quires leadership commitment,
• going the “equipment light” A rate of 0% means the equipment nursing commitment, and an edu-
route—using a low-tech system is never used and isn’t producing cation and training plan. Leader-
that combines slide sheets, limb benefits. A rate of 100% means ship commitment is needed to ap-
lifters, and slide boards to mo- caregivers are using the equipment prove SPHM equipment purchase,
bilize patients instead of using every time they should be, creat- design of training plans, and time
ceiling-mounted or portable ing the maximum possible value away from duty for training. Such
floor lifts. from the SPHM program. commitment is best obtained by
Any of these approaches will A small level of investment in creating a business case to de-
work to mobilize patients and SPHM equipment makes little dif- scribe the proposed SPHM pro-
reduce caregiver injuries if the ference in the compliance rate or gram and quantify its total costs
healthcare organization can get program results. Without the right and benefits, including return on
staff to use them. amount or type of equipment investment (ROI). (See “Making
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 5
the business case for a safe pa- Why feedback is important ing more efficient lifting methods
tient handling and mobility pro- Feedback is crucial for tracking and equipment might yield addi-
gram” in this report.) and monitoring the SPHM program tional program benefits from time
The entire nursing staff must be to determine how well it’s working. savings. Stanford University Med-
committed, especially the chief Successful programs use two types ical Center compared the average
nursing officer, who has to ap- of feedback. Compliance rate time for a chair-to-bed transfer
prove the time required for staff monitoring gives some reassurance using ceiling lifts vs. portable
training and education. Nursing that caregivers actually are using lifts. On average, a ceiling-lift
commitment should be easy to get SPHM technology when they transfer was completed before the
if the business case has identified should be. Such monitoring may portable-lift transfer even began.
the program’s potential for reduc- be done indirectly by requiring an- These data were used to justify
ing caregiver injuries, increasing nual staff certification to ensure ceiling lift installation in Stanford’s
staff availability for duty due to in- they know how to use the equip- new hospital.
jury reduction, and improving ment. Direct methods include ob- Monitoring SPHM program re-
nursing retention and satisfaction. serving the unit to see if caregivers sults and comparing them against
An education and training plan use appropriate SPHM methods. the potential results quantified in
addresses which SPHM technolo- Some newer types of equipment the business case are crucial for
gy is purchased, installed, and de- come with devices to measure how ensuring the program is working
ployed and when and where it’s many times they’re used. as designed and the organization
installed and deployed; who gets Program result monitoring, on is realizing the projected ROI.
trained, at what level of training, the other hand, depends on SPHM When results vary from the ranges
and when training takes place; program goals. These vary by identified in the business case, the
and how program data will be facility but may include reduced cause must be identified and re-
tracked and monitored to deter- caregiver injuries from patient medial action must be taken.
mine if it’s achieving the intended handling, decreases in pressure Understanding and implement-
results. In many cases, training ac- ulcers and patient falls, increased ing the essential elements of an
counts for half or more of total patient and staff satisfaction, and SPHM program will help you en-
SPHM program costs. improved staff retention. The busi- sure that your organization’s pro-
ness case and ROI for the SPHM gram is successful and can truly
Levels of expertise program should identify which achieve better outcomes for care-
Three levels of expertise in using program results create the most givers and patients. 8
SPHM equipment and methods exist: value. Methods for monitoring
• A facility champion can “train these results should be created if A valuable resource for establishing a
safe patient handling and mobility pro-
the trainers” and aid program they don’t already exist. gram is Implementation Guide to the Safe
design and revision (adjusting Most SPHM programs monitor Patient Handling and Mobility Interprofes-
the deployed equipment or workers’ compensation costs from sional National Standards, available at
www.nursesbooks.org/SPHM-Package.
training if needed). To be effec- caregiver injuries related to pa-
tive, this person needs both ex- tient handling. Usually, this neces- Selected references
tensive training and experience. sitates connecting incidence data Department of Veterans Affairs, Veterans Health
Administration. VHA Directive 2010-032. Safe
• A super user (such as a unit on the types and causes of injuries
Patient Handling Program and Facility Design.
peer leader at the Veterans (such as on the Occupational June 28, 2010. www.va.gov/vhapublications/
Health Administration) can train Safety and Health Administration’s ViewPublication.asp?pub_ID=2260. Accessed
other caregivers in the unit and Form 300) with costs associated July 3, 2014.
Hodgson MJ, Matz MW, Nelson A. Patient han-
answer questions. Reaching this with those injuries (found in the
dling in the Veterans Health Administration: fa-
level of expertise requires in- workers’ compensation system). cilitating change in the health care industry. J
depth training. Any equipment strategy (over- Occup Environ Med. 2013;55(10):1230-7.
• A general caregiver knows head lifts, portable lifts, “equip-
John Celona is a principal at Decision Analysis
how to use SPHM technology ment light” or a combination) can Associates, LLC, in San Carlos, California. He is
and methods but may not be drive a high compliance rate and the author of Decision Analysis for the Profes-
qualified to train others. favorable program results. But us- sional, 4th ed.
6 Current Topics in Safe Patient Handling and Mobility September 2014 www.AmericanNurseToday.com
Transforming the
culture: The key to
hardwiring early
mobility and safe
patient handling
Culture change requires deliberate focus, staff
education, and full engagement.
By Kathleen M. Vollman, MSN, RN, CCNS, FCCM, FAAN, and Rick Bassett, MSN, RN, APRN, ACNS-BC, CCRN
arly mobility in the intensive
E care unit (ICU) is critical to a
patient’s short- and long-term
recovery. Studies show early mo-
bility programs result in more venti-
lator-free days, fewer skin injuries,
shorter ICU and hospital stays, re-
duced delirium duration, and im-
proved physical functioning.
But accomplishing early mobili-
ty requires significant coordina-
tion, commitment, and physical ef-
fort by the multidisciplinary team.
How do we balance the benefits
of early mobilization against the
potential risk of staff or patient in-
jury during the mobilization activi-
ty? Part of the solution to ensuring
safe mobilization of critically ill bility practices without a protocol,
patients is to view mobilization and 52% hadn’t incorporated ear-
along a continuum based on pa- ly mobility into routine care prac-
tient readiness, progression based resources, patients’ physiologic in- tices. Barriers to implementation of
on goals, strategies to prevent stability, lack of emphasis on the mobility initiatives included com-
complications, and assessment of value and priority of mobilizing peting staffing priorities, insuffi-
activity tolerance. This view keeps patients, and the ICU culture relat- cient physical therapy staff, and
safety at the forefront. ed to mobility. A 2014 internation- concern about patient and care-
Within the ICU, barriers to ear- al survey of early mobilization giver injury. The study found that a
ly mobility may include clinicians’ practices in 833 ICUs found only standardized protocol may pro-
knowledge deficits and fears, in- 27% had formal early mobility mote successful implementation of
sufficient human and equipment protocols, 21% had adopted mo- an early mobility program.
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 7
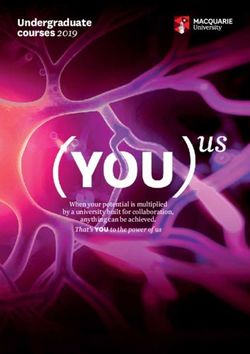
Learning progression for patient mobility
This diagram shows the four stages of staff learning regarding early patient mobility and
safe patient handling. Importance of a culture
change
Sustaining any clinical improve-
Right type of support, right time ment initiative requires an organi-
zational culture change. Baseline
To progress to the next level: Educate regarding
evidence and progressive mobility continuum,
assessment of the current culture as
use scenarios to build problem-solving skills well as early engagement of team
around contingencies and high-risk patients. members is the starting point. In
Leverage physical therapy in teaching nurses 2012, the authors led a VHA, Inc.
Conscious
specific skills. critical care improvement team col-
laborative of 13 ICUs from eight
STAGE 2: Conscious, STAGE 3: Conscious, organizations to implement safe
unskilled skilled and effective early patient mobility
“I care now, but I feel clueless.” “I know but need support and in the ICU. Efforts focused on
2 3
• Staff are receptive to
extra time to execute.” elements central to sustainable
progressive mobility concepts. • Staff are ready to put progressive change. First, team members
• Staff may be fearful of process mobility into daily practice. acquired key knowledge to under-
and risks. • Staff are motivated by sense of stand why ICU mobility is impor-
efficacy and success/failure tant. Next, strategies for organiza-
experiences.
tional, leadership, and clinical staff
engagement were discussed. To
promote the transition in practice
To progress to the next level: and the required culture change,
Overcome staff's emotional and To progress to the next level: ICU clinicians needed guidance.
Consciousness
intellectual barriers by using Coach and mentor staff during An organizational development
storytelling and evidence, execution. Encourage through tool was designed to help teams
engage in discussions and failure experiences (such as
patient not tolerating mobility),
create an effective culture change.
address positive/negative aspects
of immobility. Include sources and build sense of competence Although it was adapted specifical-
(evidence and experience) by recognizing successes. ly to integrate with early patient
outside the organization as well. mobility efforts in the ICU, this tool
can be applied to other settings.
(See Learning progression for pa-
STAGE 1: Subconscious, STAGE 4: Subconscious, tient mobility.)
unskilled skilled Three elements are crucial to
“I don’t know why I should care “I am skilled and can help others.” successfully implementing and sus-
1 4
about patient mobility.” taining an improvement initiative:
• Staff skillfully put progressive
• Staff are unclear on purpose mobility into daily practice. • Team members must understand
behind progressive mobility. • Further staff learning is and be able articulate what’s
Subconscious
• Old paradigms and enhanced by teaching and being proposed. To help them
assumptions around immobility mentoring others.
understand, they must receive
are present.
evidence-based literature and
To support process:
educate staff regarding other relevant information.
how to effectively • Team members must grasp why
mentor, coach.
Skilled the initiative is important to the
Unskilled Exapnd role: patient, themselves, and the or-
storyteller, champion, ganization. Clinicians typically
and mentor.
respond favorably to change
© 2010 Brandwene Associates
when they can connect it to
real impacts.
• The leader of the initiative must
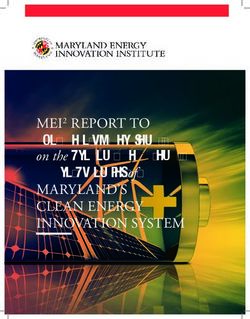
8 Current Topics in Safe Patient Handling and Mobility September 2014 www.AmericanNurseToday.comDecision tree for mobilizing hemodynamically
unstable patients
define the role of each team
This diagram helps clinicians determine whether and when an intensive care unit patient is
member and discipline. Under- ready to begin mobility activities.
standing team roles creates a
solid platform on which the cul-
ture change builds. Screen for mobility readiness
within 8 hours of admission to the Key
ICU and daily and initiate in-bed HR: heart rate
Four stages of learning mobility strategies as soon as
To learn a skill or concept, a per- ICU: intensive care unit
possible. MAP: mean arterial pressure
son progresses through four
SBP: systolic blood pressure
stages, according to a learning O2 sat: oxygen saturation
model attributed to Abraham Is the patient hemodynamically
Maslow. This model can be ap- unstable with manual turning?
plied to clinicians learning about • O2 Sat ≤ 90%
safe patient handling and mobility • New-onset cardiac arrhythmias No Begin in-bed mobility techniques
or ischemia
(SPHM). and progress to out-of-bed
• HR < 60 or >120
mobility as the patient tolerates.
• MAP < 55 or >140
Stage 1: Subconscious, • SBP < 90 or >180
unskilled • New or increasing vasopressor
In this stage, team members are infusion
unaware of how little they know
and don’t realize a change is nec- Yes
essary. Also, they may have fears
Is the patient still
and misconceptions about the No
hemodynamically unstable after Begin in-bed mobility techniques
change. For example, some criti- allowing a 5- to 10-minute and progress to out-of-bed
cal care clinicians believe reposi- adaptation after position change mobility as the patient tolerates.
tioning or mobilizing critically ill before determining tolerance?
patients threatens the security of
vital tubes and lines. But with the Yes
proper knowledge, training, and No Allow the patient a minimum of
Have activities been spaced 10 minutes of rest between
resources, staff can mobilize and
sufficiently to allow rest? activities and then try again to
reposition ICU patients safely with- determine tolerance.
out jeopardizing tubes and lines.
Yes
In one study, 1,449 activity events
(such as sitting up in bed, sitting Has the manual position turn or No Try the position turn or head-of-
in a chair, and ambulating) were head-of-bed elevation been bed maneuver slowly to allow
performed with mechanically venti- performed slowly? adaptation of cardiovascular
response to the inner-ear
lated patients; fewer than 1% ex- postiion change.
perienced adverse events. As part Yes
of the culture change, misconcep-
tions about SPHM need to be ad- Initiate continuous lateral
dressed through education and rotation therapy via a protocol to
train the patient to tolerate
coaching. Once the purpose of turning.
SPHM is defined clearly and mis- © 2012 Kathleen Vollman-Advancing Nursing LLC.
conceptions have been addressed,
team members are ready to move
on to stage 2.
team members understand why they may have fears about specif-
Stage 2: Conscious, SPHM is important but don’t ic processes or actions involved
unskilled know how to accomplish it. Al- in patient mobilization. For in-
In the conscious, unskilled stage, though open to new learning, stance, they may fear certain
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 9In bed and out-of-bed
activities
types of mobilization activities staff. During the transition from
can cause hemodynamic instabili- stage 3 to stage 4, the skills and
ty. Education and practical appli- Strategies to promote patient and knowledge required for the SPHM
cation experiences can help them caregiver safety during mobiliza- initiative must become “hard-
overcome this fear. Another way tion can be divided into two basic wired” or ingrained into care-
educators can break through such categories—those used when the givers’ subconscious. This requires
barriers is to use a decision tree patient is in bed and those used deliberate, focused energy on con-
that incorporates the latest scien- when the patient is out of bed. In- tinued engagement. However,
tific knowledge to help clinicians bed mobility encompasses reposi- staff energy, resource availability,
minimize the hemodynamic im- tioning activities, lateral-rotation and competing priorities may pose
pact or retrain patients to tolerate therapy, tilt-table exercises, and barriers to sustaining the change.
movement. (See Decision tree for bed-chair sitting. Modern critical- Throughout stage 3, positive
mobilizing hemodynamically un- care beds should be capable of ro- feedback, motivation, and sharing
stable patients.) tating the patient continuously, cre- of successes and challenges are
A critical resource used with ating a tilt table through the use of important for driving continual im-
the VHA team was a nurse-driven, a reverse Trendelenburg position provement and culture change.
evidence-based multidisciplinary and an adjustable footboard, pro- These goals can be accomplished
progressive mobility continuum gressing the body through the in various ways. Here are some
tool that addresses mobility phas- head elevation–foot down position examples:
es and corresponding interven- to a chair, and ultimately assisting • Networking with other organi-
tions. The team received education the patient with standing. These zations in various stages of the
on the tool and how to apply it in features reduce the risk of patient practice change can be ex-
and caregiver injury and make it tremely useful. It allows collabo-
In-bed mobility encompasses easier to perform mobility actions.
For in-bed repositioning from
rative identification and sharing
of challenges, struggles, effec-
repositioning side to side and moving up, using
a breathable glide sheet and spe-
tive strategies, and success sto-
ries. This process creates syner-
activities lateral-rotation cially designed foam wedges gistic energy among the team
helps reduce shear and friction for members, helping to motivate
therapy, tilt-table exercises, and the patient and help prevents in- them and accelerate the
juries to caregivers because they change.
bed-chair sitting. require a pulling rather than lifting • Within the VHA mobility collab-
motion. In one study, implementa- orative network, teams shared
practice. The tool provided a visu- tion of this turn-and-position system reward strategies. One team
al foundation to guide safe mobili- reduced hospital-acquired pres- gave out M&Ms® when “caught
ty practices, create consistency, sure ulcers by 28% and reduced in the act” of Moving and Mo-
promote team communication, and staff injuries by 58%. Lifts can be bilizing patients. Such moments
enhance processes. used for some in-bed mobility ac- present crucial coaching oppor-
Numerous studies show that ed- tivities and are effective during tunities. For example, after a
ucation, skill building, and proto- ambulation and the transition from mobility event, staff can huddle
cols may not be enough to create in-bed to out-of-bed activities. briefly to discuss the event and
sustainable change. Using strate- what, if any, improvements
gies to evaluate available nursing Stage 3: Conscious, skilled could be made to make the
resources and systems that can Stage 3 learning focuses on imple- process more effective.
produce change makes it easier menting the change, with attention
for clinicians to provide the right to fine-tuning the process. Coach- Stage 4: Subconscious,
care for the right patient at the ing, mentoring, and maintaining skilled
right time while balancing these engagement are critical. In previ- During this stage, the practice and
needs against caregivers’ needs ous stages, much effort was ex- culture changes are well on their
for safety. pended in educating and training (continued on page 25)
10 Current Topics in Safe Patient Handling and Mobility September 2014 www.AmericanNurseToday.comStandards to protect
nurses from handling and
mobility injuries
Learn about ANA standards that help
safeguard both nurses and patients.
By Amy Garcia, MSN, RN, CAE
he intense focus on safe pa-
T tient handling and mobility
(SPHM) in acute and long-
term care has yielded a valuable
benefit for nurses and other health-
care workers—a decrease in staff
lifting injuries for the first time in
30 years. Nonetheless, nurses still
suffer more musculoskeletal disor-
ders than employees in the manu-
facturing, construction, and ship-
building industries.
Many employers and nurses be-
lieve lifting injuries can be pre-
vented by using proper body me-
chanics and that lifting equipment most patients’ weight. experts to develop standards. Par-
is warranted only for obese A patchwork of regulations with- ticipants included representatives of
adults. But the evidence contra- out teeth contributes to a hazardous patients; nursing; surgery; therapy;
dicts this notion. The National In- environment for caregivers and biomedical engineering; risk man-
stitute of Occupational Safety and patients. Congress passed the er- agement; architecture; law; acute,
Health calculates maximum loads gonomic standard of the Occupa- long-term, home health, and hos-
for manual lifting, pushing, tional Safety & Health Administra- pice care; the military; Department
pulling, and carrying using a tion in 2000 but rescinded it in of Defense; certain government
range of variables. Typically, a 2001 before the regulations could agencies; vendors; and profession-
maximum load for a box with han- take effect. Only 10 states have al associations.
dles is 51 lb (23 kg)—lower when laws requiring comprehensive In 2013, ANA published Safe
the lifter has to reach, lift near the SPHM programs, typically targeting Patient Handling and Mobility: In-
floor, or assume a twisted or awk- acute and long-term care settings. terprofessional National Standards
ward position. Of course, patients Across the Care Continuum. Previ-
don’t come in simple shapes or ANA standards ous documents referred to safe pa-
have handles. They may sit or lie The American Nurses Association tient handling and movement. The
in awkward positions, move unex- (ANA) recognized the need for a workgroup changed the terminolo-
pectedly, or have wounds or de- standard of care that applies to all gy from movement to mobility to
vices that interfere with lifting. Al- healthcare disciplines and encom- distinguish patient-initiated mobility
though proper body mechanics passes the entire continuum of care. from movement accomplished by
and good lifting technique are im- In 2012, ANA convened an inter- others. Also, nurses use the word
portant, they don’t compensate for professional group of subject matter mobility differently than physical or
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 11occupational therapists. The termi- is an important step toward mini- sist on manual handling. It outlines
nology change is designed to mizing risk to patients and nurses. the importance of using SPHM tech-
align our practices with patients’ nology in a therapeutic manner,
needs and highlight new research Standard 3: Incorporate er- with the goal of promoting inde-
on the importance of early and gonomic design principles to pro- pendence. Nurses working in reha-
progressive mobility in the inten- vide a safe care environment. bilitation or assisted-living settings
sive care unit. The workgroup also This standard is based on the con- may believe using lifts or other tech-
chose the term technology to de- cept of prevention through design, nology limits the patient’s independ-
scribe all lifts, slings, slide sheets, which considers the physical lay- ence, but selecting SPHM techn-
computer programs, and other out, work-process flow, and use of ology to be used in a progressive
items used to promote patient mo- technology to reduce exposure to manner can provide support and a
bility. It decided that the term injury or illness. Healthcare facili- sense of safety as the patient gains
healthcare recipient is more inclu- ties should consider diverse per- or regains independent movement.
sive than patient for general use. spectives, including those of nurs- For example, a patient may need
es and therapists, when planning full-body lift technology immediately
A closer look at the for construction or remodeling. after surgery, but then progress to a
standards sit-to-stand lift for bedside toileting
The eight ANA standards are Standard 4: Select, install, and and then to technology that sup-
complemented by substandards, maintain SPHM technology. This ports ambulation.
examples, resources, and metrics standard provides guidance in se-
for evaluation. lecting, installing, and maintaining Standard 7: Include SPHM in
reasonable accommodation and
Standard 1: Establish a culture
SPHM technology. It emphasizes
post-injury return to work. This
of safety. This standard calls for
the importance of investing in ap-
propriate amounts and types of standard promotes an employee’s
the employer to establish a com- SPHM technology to meet the early return to work after an injury
mitment to a culture of safety. This needs of patients in the organiza- and use of differently abled work-
means prioritizing safety over tion’s specific environment. ers through a comprehensive
competing goals in a blame-free SPHM program.
environment where individuals can Standard 5: Establish a system
report errors or incidents without for education, training, and main- Standard 8: Establish a compre-
fear. The employer is compelled to taining competence. This stan- hensive evaluation system. The fi-
evaluate systemic issues that con- dard outlines employee (and vol- nal standard calls for a compre-
tribute to incidents or accidents. unteer) training and education hensive evaluation system for each
The standard also calls for safe needed to participate in the SPHM SPHM program component, with
staffing levels and improved com- program. Education should be remediation of deficiencies.
munication and collaboration. multidisciplinary and include docu- The appendix of Safe Patient
Every organization should have a mented demonstration of compe- Handling and Mobility provides
procedure for nurses to report tency before the employee uses an extensive list of resources for
safety concerns or refuse an as- SPHM technology. meeting each standard. To order
signment due to concern about pa- the ANA book and the accompa-
tients’ or their own safety. Standard 6: Integrate patient-cen- nying Implementation Guide to the
tered SPHM assessment, plan of Safe Patient Handling and Mobili-
Standard 2: Implement and sus- care, and use of SPHM technolo- ty Interprofessional National Stan-
tain an SPHM program. This stan- gy. This standard focuses on the pa- dards, visit www.nursesbooks.org/
dard outlines SPHM program com- tient’s needs by establishing assess- SPHM-Package. 8
ponents, including an assessment, ment guidelines and developing an Visit www.AmericanNurseToday.com/
written program, funding, and individual plan of care. It also ad- Archives.aspx for a list of selected references.
matching the program to the spe- dresses the need to establish an or- Amy Garcia is chief nursing officer for Cerner
cific setting. Evaluating the physi- ganizational policy on the rights of Clairvia, specializing in workforce issues and was
cal requirements of a task or role patients or family members who in- the technical writer for the SPHM standards.
12 Current Topics in Safe Patient Handling and Mobility September 2014 www.AmericanNurseToday.comImplementing a
mobility assessment
tool for nurses
A nurse-driven assessment tool reveals the patient’s
mobility level and guides SPHM technology choices.
By Teresa Boynton, MS, OTR, CSPHP; Lesly Kelly, PhD, RN; and Amber Perez, LPN, BBA, CSPHP
patient’s mobility status af-
A fects treatment, handling
and transfer decisions, and
potential outcomes (including
falls). Hospital patients spend most
of their time in bed—sometimes
coping with inadvertent negative
effects of immobility. Assessing a
patient’s mobility status is crucial,
especially for evaluating the risk
of falling. Yet no valid, easy-to-
administer bedside mobility as-
sessment tool exists for nurses
working in acute-care settings.
Various safe patient handling
and mobility (SPHM) technologies
allow safe transfer and mobiliza-
tion of patients while permitting
maximum patient participation
and weight-bearing (if indicated).
A mobility assessment helps identi-
fy the SPHM technology needed to
ensure safe activities while taking
the guesswork and uncertainty out
of deciding which SPHM technolo- need for SPHM technology. For and management have been un-
gy is right for which patient. both patient and staff safety, a pa- der the purview of physical thera-
Because mobility is so impor- tient’s mobility level must be linked pists (PTs) through consultations.
tant during hospitalization, mem- with use of SPHM technology. But the entire healthcare team
bers of a Banner Health multidisci- When used consistently, appropri- needs to address patient mobility.
plinary SPHM team determined ate technology reduces the risk of Nurses conduct continual surveil-
nurses should take a more active falls and other adverse patient out- lance of patients and their pro-
role in assessing and managing comes associated with immobility. gress, but typically they haven’t
patient mobility. We concluded it (See The link between patient im- performed consistent, validated
was crucial to develop and vali- mobility and staff injuries.) mobility assessments. Instead,
date a tool that nurses can use they’ve relied on therapy services
easily at the bedside to assess a Communication barriers to determine the patient’s mobility
patient’s mobility level and the Historically, mobility assessments level and management.
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 13The link between patient immobility and staff
injuries
Current mobility
Patient immobility poses the risk of injury to healthcare workers. Nurse workloads continue to
rise as patient acuity levels increase and hospital stays lengthen. This situation increases pa- assessment options
tients’ dependence on nurses for assistance with their mobility needs. Although tools to assess mobility
What’s more, nursing staff frequently rely on the patient or a family member to report the and guide SPHM technology selec-
patient’s ability to stand, transfer, and ambulate. But this information can be unreliable, espe- tion are used in hospitals, their val-
cially if the patient has cognitive impairment related to the diagnosis or medications or if he or ue for the bedside nurse may be
she has experienced unrecognized decreased mobility and deconditioning from the disease or
injury that necessitated hospitalization.
limited or inappropriate with many
To decrease the risk of caregiver injury, nurses should assess patient mobility and use safe patients in acute-care settings.
patient handling and mobility (SPHM) technology. SPHM algorithms from the Depart-
ment of Veterans Affairs have been
valuable as training and decision-
ed to perform SPHM. Especially if making tools in determining which
Nurses aren’t trained in PTs aren’t available, nurses must SPHM technology to consider for
rely on their own judgment to specific tasks. But these can be
skilled therapy move and mobilize patients safely. hard to use at the bedside. Also,
But they may be uncertain as to they assume the patient’s mobility
techniques and may be ill which equipment to use for which status is known and don’t provide
prepared to mobilize patients patients. While a total lift may be quick guidance in determining a
used with many patients, such a patient’s overall mobility level.
safely during routine daily lift doesn’t maximize the patient’s (See Limitations of common mobili-
mobility potential. ty assessment tools.)
activities.
In many cases, though, a PT’s Limitations of common mobility
assessment doesn’t translate to assessment tools
meaningful actionable items for
Several of the mobility assessment tools discussed below already are in use, but
nurses. What’s more, PTs don’t al- each has certain drawbacks.
ways adequately communicate a The Timed Get Up and Go Test starts by having
patient’s SPHM needs to other the patient stand up from an armchair, walk 3
healthcare team members. For ex- meters, turn, walk back to the chair, and sit down.
ample, confusion surrounds termi- But it gives no guidance on what to do if the pa-
tient can’t maintain seated balance, bear weight,
nology typically used by PTs, such
or stand and walk.
as numeric mobility levels (1+, 2+, The Quick 5 Bedside Guide tool, developed by
indicating a one-person or two- a registered nurse and physical therapist (PT),
person assist, respectively) as well was the basis for a research project on what be-
as ranges (minimum, moderate, or came known as the Quick 3. This tool takes the
patient through three functional tasks but doesn’t
maximum assist by one or more
fully address patient limitations. Nor does it rec-
healthcare workers). Also, PTs are ognize weight-bearing limitations or address the
consulted only for a limited num- issues or abilities of an ambulatory patient. Also,
ber of patients and at different it provides only limited recommendations for
points during the hospital stay. SPHM technology.
Nurses, for their part, aren’t The Egress test, also developed by a PT, is used
in hospital settings. It starts with the patient per-
trained in skilled therapy tech-
forming three repetitions of sit-to-stand, at the
niques and may be ill prepared to bedside, marching in place, and advance step and
mobilize patients safely during return with each foot. But it’s tailored to PTs and
routine daily activities. doesn’t address how the patient performs bed mobility or comes to a standing po-
In addition to communicating sition. Also, it gives only limited guidance for nurses on use of SPHM technology
and isn’t appropriate for certain patients (such as those unable to weight bear on
potential risk to other healthcare
one or both legs).
team members, mobility assess-
ment can identify technology need-
14 Current Topics in Safe Patient Handling and Mobility September 2014 www.AmericanNurseToday.comBanner Mobility Assessment Tool for nurses
Nurses have found that the Banner Mobility Assessment Tool (BMAT) is an effective resource for performing a bedside assessment of patient
mobility.
Fail = Choose most appropriate
Test Task Response equipment/device(s) Pass
Assessment Sit and shake: From a semi-reclined Sit: Patient is able to follow MOBILITY LEVEL 1 Passed Assessment
Level 1 position, ask patient to sit upright and commands, has some trunk strength; • Use total lift with sling and/or Level 1 = Proceed
Assessment of: rotate* to a seated position at side caregivers may be able to try weight- repositioning sheet and/or straps. with Assessment
• Trunk strength of bed; may use bedrail. bearing if patient is able to maintain • Use lateral transfer devices, such Level 2.
• Seated balance Note patient’s ability to maintain seated balance longer than 2 minutes as roll board, friction-reducing
bedside position. (without caregiver assistance). device (slide sheets/tube), or
Ask patient to reach out and grab your Shake: Patient has significant upper air-assisted device.
hand and shake, making sure patient body strength, awareness of body in Note: If patient has strict bed rest
reaches across his/her midline. space, and grasp strength. or bilateral non-weight-bearing
restrictions, do not proceed with the
assessment; patient is MOBILITY
LEVEL 1.
Assessment Stretch and point: With patient in Patient exhibits lower extremity MOBILITY LEVEL 2 Passed Assessment
Level 2 seated position at side of bed, have stability, strength and control. • Use total lift for patient unable to Level 2 = Proceed
Assessment of: patient place both feet on floor (or stool) May test only one leg and weight- bear on at least one leg. with Assessment
• Lower extremity with knees no higher than hips. proceed accordingly (e.g., • Use sit-to-stand lift for patient who Level 3.
strength Ask patient to stretch one leg and stroke patient, patient with can weight-bear on at least one leg.
• Stability straighten knee, then bend ankle/flex ankle in cast).
and point toes. If appropriate, repeat with
other leg.
Assessment Stand: Ask patient to elevate off bed or Patient exhibits upper and lower MOBILITY LEVEL 3 Passed Assessment
Level 3 chair (seated to standing) using assistive extremity stability and strength. • Use non-powered raising/stand aid; Level 3 AND no
Assessment of: device (cane, bedrail). May test with weight-bearing default to powered sit-to-stand lift assistive device
• Lower extremity Patient should be able to raise buttocks on only one leg and proceed if no stand aid is available. needed = Proceed
strength for off bed and hold for a count of five. May accordingly (e.g., stroke patient, • Use total lift with ambulation with Assessment
standing repeat once. patient with ankle in cast). accessories. Level 4.
Note: Consider your patient’s cognitive If any assistive device (cane, • Use assistive device (cane, walker, Consult with
ability, including orientation and CAM walker, crutches) is needed, crutches). physical therapist
assessment if applicable. patient is Mobility Level 3. Note: Patient passes Assessment Level when needed
3 but requires assistive device to and appropriate.
ambulate or cognitive assessment
indicates poor safety awareness;
patient is MOBILITY LEVEL 3.
Assessment Walk: Ask patient to march in place at Patient exhibits steady gait and good MOBILITY LEVEL 3 MOBILITY LEVEL 4
Level 3 bedside. Then ask patient to advance balance while marching and when If patient shows signs of unsteady gait MODIFIED
Assessment of: step and return each foot. stepping forward and backward. or fails Assessment Level 4, refer INDEPENDENCE
• Standing balance Patient should display stability while Patient can maneuver necessary turns back to MOBILITY LEVEL 3; Passed = No
• Gait performing tasks. for in-room mobility. patient is MOBILITY LEVEL 3. assistance needed
Assess for stability and safety awareness. Patient exhibits safety awareness. to ambulate; use your
best clinical judgment to
determine need for
supervision during
ambulation.
Always default to the safest lifting/transfer method (e.g., total lift) if there is any doubt about the patient’s ability to perform the task.
Banner Mobility nurse-driven bedside assessment achieve (such as mobility level
Assessment Tool of patient mobility. It walks the 1). Then it guides the nurse to the
At Banner Health, we developed patient through a four-step func- recommended SPHM technology
the Banner Mobility Assessment tional task list and identifies the needed to safely lift, transfer,
Tool (BMAT) to be used as a mobility level the patient can and mobilize the patient. (See
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 15Banner Mobility Assessment Tool appropriate interventions are im- or require greater focus. Although
for nurses.) plemented and the outcomes eval- we know nurses should be more in-
uated. Nurses need to be empow- volved in assessing mobility than
Implementing BMAT ered and able to recognize the they have been historically, we rec-
The BMAT was created in our hos- connection between these assess- ognize the value of involving and
pital’s electronic medical record ments and choice of interventions, communicating effectively with all
(EMR) in a way that guides the including SPHM technology. members of a good interdiscipli-
nurse through the assessment Here’s an example of BMAT in nary team to help reduce patient
steps. Patients are determined to action at Banner: A 35-year-old falls and staff injuries caused by
have a mobility level of 1, 2, 3, male was admitted to a surgical patient handling. 8
or 4 based on whether they pass floor late in the evening. He was
Selected references
or fail each assessment level. Edu- 6'2" tall and weighed 350 lb Dionne M. Practice Management: Stand and de-
cational tools and tip sheets are (158 kg). He didn’t want to use a liver. Physical Therapy Products. March 2005.
used to train nurses and support bedpan, but his nurse wasn’t com- www.ptproductsonline.com/2005/03/stand-
and-deliver/. Accessed June 30, 2014.
staff on what technology to consid- fortable getting him up to use the
er for patients at each level. bathroom because he hadn’t been Hook ML, Devine EC, Lang NM. Using a com-
puterized fall risk assessment process to tailor
evaluated by physical therapy, interventions in acute care. In: Henriksen K, Bat-
and a PT wasn’t available in the tles JB, Keyes MA, Grady ML, eds. Advances in
To stay current on the patient’s evening. A nurse passing by
who’d used the BMAT (which had-
Patient Safety: New Directions and Alternative
Approaches; vol 1. Assessment. AHRQ Publica-
tion No. 08-0034. Rockville, MD: Agency
mobility status nurses are n’t been formally rolled out Ban- for Healthcare Research and Quality; 2008.
www.ncbi.nlm.nih.gov/books/NBK43610. Ac-
ner-wide at that time) came in and
expected to complete the BMAT on cessed July 10, 2014.
assessed the patient; the assess-
Mathias S, Nayak US, Isaacs B. Balance in eld-
ment found him at mobility level 3.
admission, once per shift, and with erly patients: the “get-up and go” test. Arch
He was transferred to the toilet us- Phys Med Rehabil. 1986;67(6):387-9.
ing a nonpowered stand aid. Both
the patient status changes. Oliver D, Healey F. Falls risk prediction tools for
patient and nurse were relieved hospital inpatients: do they work? Nurs Times.
and happy. 2009;105(7):18-21.
Communication tools also are Oliver D, Healey F, Haines TP. Preventing falls
and fall-related injuries in hospitals. Clin Geriatr
used. For instance, a sign outside A step in the right Med. 2010;26(4):645-92.
the patient’s room indicates his or direction Nelson AL. Safe patient handling and move-
her mobility level, instantly telling As a quick bedside assessment ment: A guide for nurses and other health care
anyone passing by or entering if tool, the BMAT is a step in the right providers. New York, NY: Springer Publishing
the patient can ambulate inde- direction. It’s part of a broad pro- Company, Inc.; 2006. www.springerpub.com/
samples/9780826163639_chapter.pdf. Ac-
pendently or if SPHM technology gram of increased staff awareness, cessed June 30, 2014.
must be used. To stay current on education, and training around pa- Nelson A, Harwood KJ, Tracey CA, Dunn KL.
the patient’s mobility status (for in- tient assessments, preventing staff Myths and facts about safe patient handling in
stance, at handoffs, after proce- injuries and patient falls, and rehabilitation. Rehabil Nurs. 2008;33(1):10-7.
dures, with medication changes, achieving better patient outcomes. Wright B, Murphy J. “Quick-5 Bedside” Guide.
Franklin, MA: Liko, Inc.; 2005.
or after a potentially tiring therapy Initial evidence from a validation
session), nurses are expected to study completed at one Banner hos-
Teresa Boynton is an injury prevention and
complete the BMAT on admission, pital supports the BMAT as a valid workers’ compensation consultant, ergonomics
once per shift, and with the pa- instrument for assessing a patient’s specialist, and certified safe patient handling
tient status changes. The BMAT mobility status at the bedside. professional for Risk Management at Banner
also is linked to Banner’s fall as- As we work toward customizing Health, Western Region, based in Greeley, Col-
sessment risk in the EMR. actions and interventions to meet orado. Lesly Kelly is the RN clinical research
program director for Banner Good Samaritan
Throughout BMAT implementa- individual patient needs, we contin- Medical Center in Phoenix, Arizona. Amber
tion, we recognized that identify- ue to evaluate which additional as- Perez is a safe patient handling clinical con-
ing a patient’s mobility level and sessment components or fall inter- sultant for Handicare North America based in
fall risk score are pointless unless ventions or precautions are needed Phoenix, Arizona.
16 Current Topics in Safe Patient Handling and Mobility September 2014 www.AmericanNurseToday.comThe sliding patient:
How to respond to
and prevent migration
in bed
Migration can cause negative patient outcomes and
caregiver injuries resulting from repositioning.
By Neal Wiggermann, PhD
n hospital settings, where the A 1995 study at one hospital carries an extremely high risk of
I head of the bed (HOB) com-
monly is elevated, gravity caus-
es patients to slide, or migrate,
found nurses pulled patients up in
bed an average of 9.9 times per
shift. More recent evidence sug-
caregiver injury. Less research
has been done on the effects of
migration on patients. This article
toward the foot of the bed. Nurs- gests this activity may be even describes how migration can af-
es are well aware of this, as more common in some hospitals fect patient outcomes, outlines rel-
they’re regularly required to pull and units. evant scientific evidence, and dis-
patients back toward the HOB if Studies show that pulling pa- cusses strategies for managing
they can’t reposition themselves. tients who’ve migrated in bed patient migration.
www.AmericanNurseToday.com September 2014 Current Topics in Safe Patient Handling and Mobility 17Considerations when purchasing hospital
beds
n't been studied for hospital beds,
Before purchasing hospital beds, clinicians and hospital purchasing staff should evaluate rele-
vant manufacturer claims and test data to determine how well the product performs to reduce it’s reasonable to expect migration
patient migration. Keep the following points in mind. would result in discomfort, espe-
• Migration test results may vary based on methodology, so be suspicious of marketing cially in patients with low back
materials that don’t describe test methods. pain or disc herniation.
• Consider the relevance of test conditions to their clinical application.
• Be aware that a proper experimental design can improve test result accuracy. For exam- Responding to patient
ple, a laboratory motion-capture system produces less error than a tape measure, and a migration
large subject sample (10 or more) with subjects of varied heights and weights is more ac- To help prevent negative outcomes
curate than a small or homogenous sample. associated with patient migration,
• Make sure migration is reported with respect to the bed surface. Because the top sections be diligent in repositioning pa-
of some hospital bed frames can move back relative to the floor, measuring migration tients who’ve migrated downward.
relative to the floor rather than the bed surface can lead to the mistaken conclusion that But be aware that repositioning is
a patient has migrated several inches less than he or she actually has.
most likely to affect outcomes relat-
ed to torso angle (such as VAP, re-
duced lung capacity, and discom-
Negative effects of tion decreases. A pilot investiga- fort)—not friction and shear linked
migration tion of 10 healthy subjects lying to pressure-ulcer development.
A 2013 study found that patients with the HOB at 30 degrees Among patients unable to boost or
in traditional hospital-bed designs showed their torso angle was reposition themselves in bed,
migrated about 13 cm (5") when about 30 degrees when properly those on mechanical ventilators
the HOB was raised to 45 de- aligned with the hip indicator, and those with back pain may be
grees. Both bed movement and compared to about 12 degrees most in need of repositioning by
gravity cause patients to slide when they migrated 23 cm (9") the nurse.
down in bed over time if the HOB past the hip indicator. Repositioning patients manual-
is kept elevated. Such migration Positioning the HOB at or ly is associated with a high risk
presumably causes friction and above 30 degrees is intended of musculoskeletal injury, so al-
to reduce the risk of ventilator- ways use repositioning aids for
associated pneumonia (VAP) be- patients unable to reposition
cause torso elevation decreases themselves. Using lift equipment,
Once patients have migrated the risk of aspirating gastric con-
tents into the lungs. Once patients
such as a ceiling-mounted or mo-
bile lift, is the best way to reduce
farther down the mattress, have migrated farther down the healthcare worker strain, accord-
mattress, elevating the HOB may ing to the American Nurses Asso-
elevating the HOB may no no longer reduce aspiration risk ciation’s Safe Patient Handling
because their torsos are flatter. At and Mobility: Interprofessional
longer reduce aspiration risk. that point, if they’re not reposi- National Standards, which calls
tioned, they may be at increased for eliminating manual lifting in
risk for VAP. all healthcare settings.
shear forces between the mattress When patients migrate down in If lift equipment isn’t available,
and skin as the patient slides bed with the HOB up, they slide use a friction-reducing sheet and
against the bed surface. Although out away from the pivot of the place the bed in the Trendelenburg
friction and shear have been HOB section and the lumbar spine position (if the patient can tolerate
linked to pressure-ulcer formation, goes unsupported, causing kypho- it). If the patient is on an air sur-
no research has evaluated whether sis. Kyphosis reduces lung capaci- face, use the “max inflate” func-
friction and shear caused by mi- ty, so respiratory function may tion. Patients who can provide par-
gration directly contribute to pres- diminish in patients who’ve migrat- tial assistance should participate in
sure-ulcer risk. ed. Although the relationship be- mobilization by placing their feet
As patients migrate toward the tween kyphotic postures caused flat on the mattress and “bridging”
foot of the bed, the torso eleva- by migration and discomfort has- when being repositioned. The pa-
18 Current Topics in Safe Patient Handling and Mobility September 2014 www.AmericanNurseToday.comYou can also read