Prescription Opioids and Heroin Epidemic in Georgia
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Prescription Opioids SARA Executive Committee
Jim Langford – Chair, SARA; Executive Director,
and Heroin Epidemic Georgia Prevention Project
in Georgia Dr. Amanda Abraham – Assistant Professor, School of
Public and International Affairs, University of Georgia
- A White Paper Dr. Aaron Johnson – Associate Professor, Institute of
Public and Preventive Health, Augusta University
Dr. Merrill Norton – Clinical Associate Professor,
College of Pharmacy, University of Georgia
Dr. Glenda Wrenn – Associate Professor, Director
of Behavioral Health, Satcher Health Leadership
Institute, Director, Kennedy Center for Mental Health
Policy, Morehouse School of Medicine
2017
©2016 Georgia Prevention Project - All Rights Reserved.
TABLE OF
Prescription Opioids and Heroin Epidemic in Georgia CONTENTS
Contents
Prescription Opioids and Heroin Epidemic in Georgia
Executive Summary
Findings and Policy
Recommendations
I. Opioids overview III. Proposed legislative agenda
1. What opioids are for Georgia
2. How opioids affect the human body 1. Increase access to Naloxone
3. The U.S. opioid epidemic 2. Improve access to opioid use disorder
treatment, including medication assisted
4. Relationship between nonmedical use of treatment (MAT and recovery support
prescription opioids and heroin use services)
5. Impact of opioid use 3. Increase state funding for substance abuse
a. Overdose deaths in Georgia prevention education
b. How Georgia compares to other states 4. Increase funding and improve
and the nation mechanisms for addressing neonatal
abstinence syndrome (NAS)
6. Economic costs of opioid misuse and
abuse in Georgia and the United states 5. Strengthen the Prescription Drug
Monitoring Program (PDMP)
6. Increase oversight of pain clinics
II. Key Georgia issues
7. Create standards for physician education
1. Overdose reversal
8. Create a “blue ribbon” commission on
2. Medication assisted treatment & recovery substance use recovery supports and
support services recovery-oriented systems of care
3. Prevention education
4. Neonatal abstinence syndrome IV. Appendix
5. Controlling access to opioids V. Resources
a. Prescription Drug Monitoring Program
b. Pain clinics
c. Prescriber education
©2016 Georgia Prevention Project - All Rights Reserved. 2
EXECUTIVE
Prescription Opioids and Heroin Epidemic in Georgia SUMMARY
Introduction
Substance Abuse Research Alliance (SARA) is a program of the Georgia Prevention Project, and it
initiated this study in April of 2016 as the organization’s first collaborative project with a primary goal to
assist the Georgia State Senate Study Committee on Opioids and Heroin in its work.
With more than 60 participants, SARA includes researchers and practitioners with a wide spectrum of
experience in substance misuse work. SARA participants represent the following organizations:
• Applied Research Services, Inc. • Georgia State University – multiple
• Augusta University departments and programs
• Carter Center Mental Health Program • Lab Solutions, Inc.
• Centers for Disease Control and Prevention • Mercer School of Medicine
• Emory University – multiple departments • Morehouse School of Medicine – multiple
and programs departments and programs
• Georgia Council on Substance Abuse • Parkaire Consultants, Inc.
• Georgia Department of Behavioral Health • Partnership for Drug-Free Kids
and Developmental Disabilities (DBHDD) • Skyland Trail
• Georgia Department of Public Health (DPH) • The Council on Alcohol and Drugs
• Georgia Prevention Project • University of Georgia – multiple departments
• Georgia Southern University and programs
SARA believes that opioid and heroin
use in Georgia seriously threatens the What you need to know now
health, prosperity and general well-
being of Georgians throughout the The U.S.
state, across almost all sectors of life 200 percent prescription opioid overdose (OD) deaths
and work. increase since 2000
Like Georgia, several other states struggle 125 million Americans who reported misusing
prescription pain relievers in the past year
over how to ameliorate the suffering and
death rates associated with prescription 80 percent of heroin users reported using
opioids and heroin, how to prevent prescription opioids for non-medical
reasons before beginning to use heroin
citizens from misusing these substances,
and how to intervene effectively to treat
Georgia
opioid use disorder and promote long-
term recovery. 549 opioid drug ODs in 2015
29 counties where drug OD rates outpace U.S. average
SARA stands ready to assist the Georgia
Legislature and the State Senate Study 11 Georgia ranks among top 11 states with most
prescription opioid OD deaths
Committee in any way that we can.
©2016 Georgia Prevention Project - All Rights Reserved. 3
EXECUTIVE
Prescription Opioids and Heroin Epidemic in Georgia SUMMARY
Executive Summary
Georgia’s prescription opioid and heroin opioid receptors, most prominently the Mu (μ)
problem threatens the well-being of every receptors. Mu receptors account for most of
Georgian at every socio-economic level and in the effects of opioids and are primarily located
every geographic region of the state. in the brain, spinal cord, peripheral nervous
system, and intestinal tract.
This study by the Substance Abuse Research
Alliance (SARA) seeks to educate public By stimulating the Mu receptors, opioids
officials and the general public about the opioid reduce the perception of pain by slowing
epidemic that is devastating communities down and blocking pain signal transmission
across the country and here in Georgia. We to the brain while also triggering the release
answer key questions and also offer a proposed of dopamine, a neurotransmitter used in
legislative agenda to consider as Georgia the brain’s pleasure or reward system. When
legislators move to address this pervasive and activated, dopamine produces a pleasurable
growing challenge in our lives and communities. and often euphoric feeling.
What Are Opioids? How Do They Use of opioids for more than a short period
Affect The Human Body? of time leads to tolerance and physical and
psychological dependence. This means opioid
Opioids are a class of drugs that act on the users must take larger doses of opioids over
body’s opioid receptors including natural, time to achieve the same effect. Additionally,
semi-synthetic and synthetic opioids. Natural opioid users must not stop taking these drugs
opioids include drugs such as morphine, which abruptly, or they will experience withdrawal
are derived from the resin of the opium poppy, symptoms such as agitation, anxiety, muscle
semi-synthetic opioids such as hydrocodone and bone pain, insomnia, vomiting or diarrhea.
and oxycodone, and synthetic opioids such as Withdrawal symptoms occur when the amount
fentanyl and methadone. of opioids used decreases or stops.
Opioids are often used medically to relieve
moderate to severe pain, but can also be used
How Did We Get To A U.S.
for other conditions -- for example, to suppress Opioid Epidemic?
cough, to treat diarrhea and even to treat Opioid overdoses - including prescription opioids
opioid use disorder. Opioids are very effective and heroin - kill 78 people daily. This number has
for treating severe pain such as that associated quadrupled since 1999. In 2015 alone, opioids
with cancer, post-surgery, or accident-related were involved in over 28,470 deaths.
injuries. While opioids provide pain relief, they
Despite the staggering statistic, the number
also cause physical dependence, respiratory
of prescriptions written for opioid analgesics
depression, euphoria, reduced intestinal motility
continues to increase.
and other desired and undesired effects. Since
these pharmacologic effects focus on blocking Misuse of prescription opioids, and heroin use,
pain, opioids have high potential for misuse. are also on the rise. In 2015, approximately
12.5 million Americans reported misusing pain
Opioid drugs mimic the body’s natural
relievers in the previous year and approximately
response to pain by stimulating the body’s
914,000 Americans reported use of heroin.
©2016 Georgia Prevention Project - All Rights Reserved. 4
EXECUTIVE
Prescription Opioids and Heroin Epidemic in Georgia SUMMARY
And, the costs of this epidemic of prescription prescribing of prescription opioids (e.g., PDMPs)
opioid overdose and misuse are high, estimated may be a driver of increased deaths from heroin
at $78.5 billion in 2013 alone. overdose, there is little empirical evidence of a
causal link.
Who Is At Greatest Risk?
Instead, the evidence suggests that market
The highest rates of prescription opioid
forces such as increased availability, reduced
overdose deaths from 1999 to 2014 were
price and increased purity of heroin could be
among non-Hispanic whites and American
more important drivers of increased heroin use
Indian or Alaskan Natives, persons aged 25 to
and heroin overdose deaths.
54, and men. Rates of prescription overdose
deaths are on the rise for women (Centers for What Is The Impact Of Opioid Use
Disease Control, CDC, 2016). Risk factors for In Georgia?
prescription opioid misuse and overdose include
doctor shopping (i.e., receiving overlapping Similar to national trends, deaths related to
prescriptions from multiple providers and opioid overdose continue to rise in Georgia.
pharmacies), taking high daily doses of Recent data from the Georgia Department of
prescription pain relieves, having mental illness Public Health indicate that deaths related to
or a history of substance misuse, being low- drug overdose are now almost equal to deaths
income, and living in a rural area (CDC, 2016). due to motor vehicle crashes (Figure 1).
According to Centers for Disease Control and Opioids, primarily prescription pain relievers and
Prevention, people at highest risk for heroin heroin, are the main driver of drug overdose
addiction are those addicted to prescription deaths. Of the 1,307 drug overdose deaths in
opioid painkillers, cocaine, marijuana and 2015 in Georgia, 900 or 68 percent were due
alcohol; people 18 to 25 years of age living in to opioid overdoses including heroin (Figure 2).
large metropolitan areas, and people without Further, a statistically significant increase in the
insurance or enrolled in Medicaid. drug overdose death rate occurred from 2013
to 2014, and overdose deaths tripled between
What Is The Relationship Between 1999 and 2013 in Georgia.
Non-Medical Use Of Prescription Prescription opioid overdose deaths in Georgia
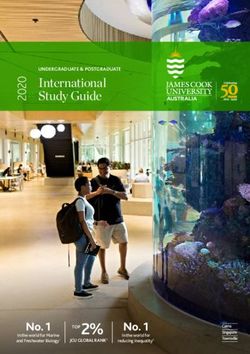
Opioids And Heroin Use? increased tenfold to 549 deaths, or a rate of 5.5
Several descriptive and observational studies per 100,000 age-adjusted deaths, between 1999
suggest a link between non-medical use of and 2014. Georgia: Among top 11 states with
prescription opioids and heroin, particularly the most prescription opioid overdose deaths
among people with frequent nonmedical use or (Figure 3).
people with prescription-opioid use disorder. Recent data indicate that 55 of Georgia’s 159
Two recent national studies found that about counties had higher drug overdose rates
80 percent of heroin users reported using than the U.S. average in 2014. This marks a
prescription opioids for non-medical reasons significant increase from 11 years ago, when just
before beginning use of heroin. However, 26 Georgia counties exceeded the U.S. average.
it is important to note that only a small Sixty percent of the 55 counties with drug
percentage (less than 5 percent) of people overdose rates higher than the national average
who use prescription opioids for non-medical in 2014 are located in rural areas with limited
reasons begin using heroin. This small access to substance use disorder treatment
percentage translates to several hundred and/or medication-assisted treatment. These
thousand new heroin users per year and numbers suggest that two-thirds of all counties
should not be minimized. in Georgia and 77 percent of rural counties
While some argue that implementation of have limited or no access to an evidence-based
policies to address misuse and inappropriate practice for opioid use disorder.
©2016 Georgia Prevention Project - All Rights Reserved. 5
EXECUTIVE
Prescription Opioids and Heroin Epidemic in Georgia SUMMARY
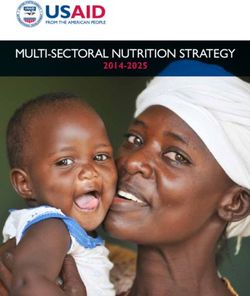
Figure 1:
Deaths Related to Drug Overdose and Motor Vehicle Crashes, Georgia, 2001-2015
1,673
1,670
1,568
1,509
1,492
1,482
1,456
1,387 Source:
1,345
1,307
1,274
1,253
1,248
1,223
1,223
1,219
Georgia
1,177
1,125
1,070
1,059
1,074
Department
1,006
956
of Public
859
767
Health,
697
682
647
611
Office of
559
Health
Indicators
for
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Planning,
Drug Overdose Deaths Motor Vehicle Crash Deaths Death files.
Figure 2:
Number of Drug Overdose Deaths Related to Opioids
including Heroin in Georgia, 2001-2015 1,274
1,307
1,074 1,070 1,059 1,125
1,006
956
859 900
767 795
647 697 682 Source:
611 600 622 633 606
559 554 Office of
467 Health
380 Indicators
265 277 294
243 246 242 for Planning
90 121 (OHIP),
3 2 3 1 6 20 16 3 25 31 48
1 5 Georgia
Department
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
of Public
All Drug Overdose Deaths Opioid Overdose Deaths, Including Heroin Heroin Overdose Deaths, Only Health.
While prescription opioid deaths declined last year, users began shifting from prescription opioids to
heroin. Hence, the spike in opioid deaths which include heroin.
Figure 3:
Number of Prescription Opioid Overdose Deaths in Georgia, 2001-2015
Source: Centers
588
549
for Disease
Control and
498 488
464 Prevention
448 441 (CDC), National
Center
362 for Health
348
308 Statistics.
270 Multiple Cause
221 of Death
171 186 1999-2014 on
152 CDC WONDER
Online
Database. Data
1
are from the
Multiple Cause
of Death Files,
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
1999-2015.
©2016 Georgia Prevention Project - All Rights Reserved. 6
EXECUTIVE
Prescription Opioids and Heroin Epidemic in Georgia SUMMARY
What Is The Cost Of Opioid Use And The Patient Protection and Affordable Care
Misuse In Georgia And The U.S.? Act (ACA) of 2010 provides greater access
to SUD treatment through major coverage
The economic burden of prescription opioid expansions, regulatory changes requiring
overdose, misuse and disorders in the U.S. is coverage of SUD treatments in existing
estimated at $78.5 billion in 2013 with over one insurance plans, and requirements for SUD
third of this amount coming from increased treatments to be offered on par with medical
health care and substance use treatment and surgical procedures. The ACA enables
costs ($28.9 billion). The health care costs states to address the opioid epidemic through
associated with opioid misuse in Georgia four primary mechanisms: insurance coverage
alone were estimated at $447 million in 2007 expansions, regulatory insurance reforms that
with estimated per-capita costs at $44. Given require inclusion of SUD treatments, enhanced
the increase in overdose deaths and misuse parity, and opportunities to integrate SUD
of opioids in Georgia over 11 years, some treatment and mainstream healthcare.
estimates indicate that health care costs
associated with opioid misuse in Georgia have On July 22, 2016, President Obama signed
increased by 80 percent since 2007. the Comprehensive Addiction and Recovery
Act (CARA). This is the most comprehensive
Hospitalizations related to opioid use and effort undertaken by Congress to address the
misuse in Georgia also have skyrocketed, opioid epidemic.
from about 302,000 in 2002 to about 520,000
in 2012. Similarly the cost of opioid related While it authorizes over $181 million each year
inpatient care more than doubled during the in new funding to fight the opioid epidemic over
same time period, rising to $15 billion in 2012. the next 10 years, monies must be distributed
annually through the regular appropriations
What Has Congress Done?
process. CARA establishes a comprehensive,
Three major pieces of federal legislation coordinated, and balanced strategy through
addressed substance use disorders (SUD) in the enhanced grant programs that would expand
past decade: prevention and education efforts, while also
• Mental Health Parity and Equity promoting treatment and recovery. The bill
Addictions Act of 2008 passed the U.S. Senate in March 2016, by a
• Patient Protection and Affordable vote of 94-1. The bill passed the U.S. House of
Care Act of 2010 Representatives in May 2016, by a vote of 400-5.
• Comprehensive Addiction and CARA Six Pillars of Coordinated Response:
Recovery Act of 2016. Solving the Opioid and Heroin Problem.
The Mental Health Parity and Equity
Addictions Act of 2008 requires private group
Comprehensive
health plans with 50 or more employees and
Addiction and Recovery Act
Medicaid managed care plans that cover SUD (CARA)
treatment do so in a manner that is no more
restrictive than coverage of other medical and
Overdose Reversal
Law Enforcement
surgical procedures. Parity requirements have
Criminal Justice
Prevention
not been extended to private plans in state
Treatment
Recovery
Reform
health insurance exchanges and Medicaid
expansion plans.
©2016 Georgia Prevention Project - All Rights Reserved. 7
EXECUTIVE
Prescription Opioids and Heroin Epidemic in Georgia SUMMARY
Key Provisions of CARA
• Expand prevention and educational efforts—particularly aimed at teens, parents and
other caretakers, and aging populations—to prevent the use of methamphetamines,
opioids and heroin, and to promote treatment and recovery
• Expand the availability of naloxone to law enforcement agencies and other first
responders to help in the reversal of overdoses to save lives
• Expand resources to promptly identify and treat incarcerated individuals suffering
from substance use disorders by collaborating with criminal justice stakeholders and
by providing evidence-based treatment
• Expand disposal sites for unwanted prescription medications to keep them out of
the hands of our children and adolescents
• Launch an evidence-based opioid and heroin treatment and intervention program to
expand best practices throughout the country
• Launch a medication assisted treatment (MAT) and intervention demonstration
program
• Strengthen prescription drug monitoring programs (PDMP) to help states monitor
and track prescription drug diversion and to help at-risk individuals access services
What should Georgia do?
After a careful review of recent recommendations from the National Safety Council and the National
Governors Association, SARA proposes a legislative agenda for Georgia as briefly outlined below.
SARA provides detailed recommendations in the body of this study.
In addition to the legislative agenda outline below, SARA recommends that the State conduct a
comprehensive needs assessment specifically related to the opioid crisis and develop both a strategic
plan and an implementation plan to guide the State’s response to this epidemic.
Phase I – Georgia’s most urgent needs
1. Increase access to naloxone.
More than 1,300 Georgians die each year from prescription opioid and heroin overdoses. Many
of these deaths could be avoided with the use of naloxone, an opioid antagonist medication
that reverses opioid overdose without significant negative side effects. First responders,
parents, and educators should have easy access to naloxone and should have training in how to
administer the drug.
2. Improve access to opioid use disorder treatment including medication-assisted
treatment (MAT) and recovery support services.
Anyone misusing prescription opioids or using heroin should have access to the full range of
opioid use disorder treatment services including medically managed detoxification/withdrawal
management, behavioral therapy, medications and recovery support services. These services
should include support for 1) families who have members in recovery and 2) community
organizations that focus on recovery.
(continued next page)
©2016 Georgia Prevention Project - All Rights Reserved. 8EXECUTIVE
Prescription Opioids and Heroin Epidemic in Georgia SUMMARY
3. Increase funding for substance misuse prevention programs.
The Georgia Legislature significantly reduced funding to DBHDD in 2010 for substance misuse
prevention programs and administration. While DBHDD distributes and manages Federal
substance misuse prevention funds, total State spending on substance misuse prevention
within DBHDD currently is only $232,000 per year. Prescription drug education programs should
target teens, young adults and parents.
4. Increase funding and improve mechanisms to address neonatal abstinence
syndrome (NAS).
Some hospitals in Georgia are overwhelmed with infants born with NAS. The problem is on
the rise, and these hospitals need significant assistance in treating and managing the care of
these infants.
Moreover, health care providers need better education and training on how to deal with NAS. Our
recommendations focus on three areas: 1) reducing incidence of NAS, 2) reducing NAS severity
and optimizing health outcomes, and 3) leveraging resources and reducing costs of NAS.
5. Strengthen the Prescription Drug Monitoring Program (PDMP).
While Georgia implemented important changes and enhancements to its PDMP during the 2016
legislative session, much work remains to be done. The PDMP helps track the writing and filling
of prescriptions of controlled substances, particularly opioid-based painkillers.
Phase II – Comprehensive and systematic approaches for Georgia
1. Increase oversight of pain clinics.
Georgia passed the Pain Management Clinic Act in 2013. Consistent with the National Safety
Council and the National Governor’s Association recommendations, Georgia should do two
things: 1) require pain clinics to register with and use Georgia’s PDMP, and 2) conduct an
evaluation of the legislation to determine if it is being enforced and what impact it has had on
opioid prescribing and overdose deaths.
2. Create standards for prescriber education.
The Georgia Composite Medical Board (CME) should mandate that a minimum of 5 hours
of the 40 hours of required biannual credit hours focus specifically on the Georgia PDMP,
pain management, and guidelines for prescribing opioid medications for chronic pain and/or
substance use disorders.
Longer term, Georgia should create a task force to address more detailed methods of educating
all levels of health professionals on pain management and incorporating technology that
integrates the PDMP more directly with patient electronic health records (EHR).
3. Create a recurring “blue-ribbon” commission on substance use and recovery.
The Georgia Legislature, in collaboration with the Governor’s Office, should create a recurring
commission that convenes every 5-7 years to establish strategy and statewide goals,
recommend appropriations, and review progress on reducing substance misuse and expanding
local systems of recovery supports and treatment services in Georgia.
©2016 Georgia Prevention Project - All Rights Reserved. 9EXECUTIVE
Prescription Opioids and Heroin Epidemic in Georgia SUMMARY
The Georgia Prevention Project
The Georgia Prevention Project - SARA’s host project ran more than 26,000 radio spots,
organization - is a statewide not-for-profit effort placed 23,000 television ads, and placed more
that focuses on reducing the use of dangerous than 588 billboards all over Georgia. This
substances among teens and young adults. saturation effort significantly changed teens’
We accomplish our work through awareness perceptions of risk about the drug and produced
campaigns, educational programming and results very similar to the Montana program.
strategic partnerships with national and Riding the momentum of the successful “Not
community based organizations. Even Once” Meth prevention campaign, the
The Georgia Prevention Project evolved from Georgia Prevention Project launched in 2014
the Georgia Meth Project founded in 2009. capitalizing on the Meth Project techniques and
Created by the Siebel Foundation, the national expanding its focus to include prescription drug
Meth Project effort won more than 45 national misuse and heroin use.
and international awards for its hard-hitting The Georgia Prevention Project partners with
educational campaigns that helped reduce community members, schools and prevention
first-time Meth use by more than 65 percent professionals to develop strategy, build coalitions
in its first two years in Montana. Subsequent and provide drug education resources to bring
launches in Idaho and Wyoming saw similar attention to the health and future of youth.
results and led to the addition of Hawaii,
Colorado and Georgia as part of the Meth Through its Teacher Substance Abuse
Project family. Training Program, GPP has worked to ensure
that large numbers of Georgia teens gain
In Georgia, the campaign led to significant in-depth knowledge of the risks associated
changes in teens’ perceptions of risk associated with the misuse of prescription drugs and
with Meth. During the media portion of the the misuse of dangerous substances such as
campaign of 2010-2012, the Georgia Meth methamphetamine and heroin.
For more information, or Jim Langford
to discuss this Executive Executive Director, Georgia Prevention Project; Chair, SARA
Summary, please contact us. 3715 Northside Parkway
Suite 1-320
Atlanta, GA 30327
404-831-1959
Email: info@georgiapreventionproject.org;
jlangford@georgiapreventionproject.org
Web sites: www.georgiamethproject.org;
www.georgiapreventionproject.org
©2016 Georgia Prevention Project - All Rights Reserved. 10Prescription Opioids and Heroin
Epidemic in Georgia
- Findings and Policy Recommendations
2017
©2016 Georgia Prevention Project - All Rights Reserved.FINDINGS & POLICY
Prescription Opioids and Heroin Epidemic in Georgia RECOMMENDATIONS
I. Opioid Overview
1. What opioids are
Opioids are a class of drugs that act on the a neurotransmitter used in the brain’s pleasure
body’s opioid receptors including natural, semi- or reward system. When activated, dopamine
synthetic and synthetic opioids. Natural opioids produces a pleasurable, often euphoric feeling,
include drugs such as which contributes to opioid misuse, as people
seek to repeat these sensations.
• morphine, derived from the resin of the
opium poppy Use of opioids for more than a short period
• semi-synthetic opioids such as of time leads to tolerance, physical and
hydrocodone and oxycodone psychological dependence. This means opioid
users must take larger doses of opioids over
• synthetic opioids such as fentanyl and time to achieve the same effect. Additionally,
methadone opioid users must not stop taking these drugs
Opioids are often used medically to relieve abruptly or they will experience withdrawal
moderate to severe pain, but can also be symptoms such as: agitation, anxiety, muscle
used for example, to suppress cough, treat and bone pain, insomnia, vomiting or diarrhea.
diarrhea, and even treat opioid use disorder. Withdrawal symptoms occur when the amount
Opioids are very effective for treating severe of opioids decrease or are stopped.
pain such as that associated with cancer, post- “Substance use disorders are a chronic medical
surgery or accident-related injuries. While illness characterized by clinically significant
opioids provide pain relief, they also cause impairments in health, social function and
physical dependence, respiratory depression, voluntary control over substance use (not a moral
euphoria, reduced intestinal motility and other failing or character flaw).” - Surgeon General’s
desired and undesired effects. Since these Report, Facing Addiction in America, 2016.
pharmacologic effects focus on blocking pain,
opioids have high potential for misuse. 3. The U.S. Opioid epidemic
2. How opioids affect the human body In 2015, overdose deaths associated with
prescription and illicit opioids increased to
Opioid drugs mimic the body’s natural 33,091, from 28,647 in 2014 (CDC), suggesting
response to pain by stimulating the body’s that 90 people die daily on average in the
opioid receptors, most prominently the Mu (μ) U.S. from opioid overdoses. Over the past
receptors. Mu receptors account for most of 15 years, overdose deaths related to opioids
the effects of opioids and are primarily located have reached epidemic proportions (Rudd et
in the brain, spinal cord, peripheral nervous al., 2015). The rate of opioid-related overdose
system, and intestinal tract. deaths has increased over 200% since 2000.
By stimulating the Mu receptors, opioids reduce Between 2011 and 2015, deaths related to
the perception of pain by slowing down and heroin more than tripled to 12,990 (National
blocking pain signal transmission to the brain, Center for Health Statistics).
while also triggering the release of dopamine,
©2016 Georgia Prevention Project - All Rights Reserved. 12FINDINGS & POLICY
Prescription Opioids and Heroin Epidemic in Georgia RECOMMENDATIONS
Despite these staggering increases in deaths Studies show a shift in the demographics of
related to opioid overdose, the number of heroin users in recent years. In the 1960s,
prescriptions written for opioid analgesics those initiating heroin use were predominantly
continues to increase (Volkow et al. 2014). young men from minority groups living in urban
The number of written prescriptions for opioid areas. Now those initiating heroin use tend
medications rose from 75.5 to 209.5 million over to be somewhat older (mean age of first use
the past decade (National Institutes of Health, is 22.9 years compared to 16.5 years), more
2014). According to a recent report, sales of concentrated in rural and suburban areas, and
opioid analgesics quadrupled from 1999 to 2010 white (Cicero et al., 2014).
(Frenk et al., 2015).
According to the CDC, people at highest
Misuse of prescription opioids and heroin risk for heroin addiction are those addicted
use is also on the rise. In 2015, approximately to prescription opioid painkillers, cocaine,
12.5 million Americans reported misusing marijuana and alcohol, people 18 to 25 years
pain relievers in the previous year and 2.0 of age living in large metropolitan areas,
million Americans had a pain reliever drug use and people without insurance or enrolled in
disorder (SAMHSA, 2016). In the same year, Medicaid (CDC, 2016 http://www.cdc.gov/
approximately 914,000 Americans reported vitalsigns/heroin/).
use of heroin and 519,000 Americans met
4. Relationship between nonmedical use of
diagnostic criteria for a heroin use disorder
prescription opioids and heroin use
(SAMHSA, 2016). The cost of prescription
opioid misuse is high, estimated at $78.5 billion Studies found that about 80% of heroin
in 2013 alone (Florence et al., 2016). Also see users reported using prescription opioids for
opioids deaths by type of opioid: heroin: 2014 nonmedical reasons before beginning use of
chart (Kaiser Family Foundation) in Appendix. heroin (Jones, 2013; Muhuri et al. 2013).
The highest rates of prescription opioid Overall, these studies suggest a link between
overdose deaths from 1999 to 2014 were nonmedical use of prescription opioids and
among non-Hispanic whites and American heroin, particularly among people with frequent
Indian or Alaskan Natives, persons aged 25 to nonmedical use, or people with prescription-
54, and men. The rates of prescription opioid opioid use disorder. However, it is important
overdose deaths are on the rise for women to note that only a small percentage (less than
(CDC, 2016). 5% of people who use prescription opioids for
nonmedical reasons) begin using heroin. This
small percentage translates to several hundred
Risk factors for prescription opioid
thousand new heroin users per year and should
misuse and overdose:
not be minimized (Compton et al., 2016).
• doctor shopping (i.e., receiving
overlapping prescriptions from multiple While some argue that implementation of
providers and pharmacies) policies to address misuse and inappropriate
prescribing of prescription opioids (e.g.,
• taking high daily doses of prescription
pain relievers PDMPs) could be a driver of increased deaths
from heroin overdose, there is little empirical
• having mental illness or a history of
evidence of a causal link. Instead, the evidence
substance abuse
suggests that market forces such as increased
• being low-income availability, reduced price and increased purity
• living in a rural area of heroin could be more important drivers
(CDC, 2016). of increased heroin use and heroin overdose
deaths (Compton et al., 2016).
See Appendix for opioids overdose deaths by Public health efforts to address either
Type of Opioid: Heroin, 2014. Kaiser Family prescription opioids or heroin use must consider
Foundation State Health Facts. interrelationships between prescription opioid
©2016 Georgia Prevention Project - All Rights Reserved. 13FINDINGS & POLICY
Prescription Opioids and Heroin Epidemic in Georgia RECOMMENDATIONS
and heroin use and focus on a comprehensive 100,000 persons in the U.S. occurred during the
approach that includes all levels of prevention same time period.
(i.e., primary, secondary, and tertiary), with
However, the rate of increase in opioid deaths
emphasis on harm reduction approaches as a
in Georgia was much higher than the rate of
principal tertiary prevention strategy (Kolodny et
increase of opioid deaths in the U.S. Sales of
al., 2015).
opioids also quadrupled in the U.S. between
5. Impact of opioid use 1999 and 2014.
a. Overdose deaths in Georgia Similar to national trends, deaths related to
opioid overdose continue to rise in Georgia.
Opioid overdose death rates including heroin in
Even more alarming, recent data from the
Georgia increased significantly - from 0.6 to 5.5
Georgia Department of Public Health indicate
per 100,000 persons between 1999 and 2014 -
that deaths related to drug overdose surpassed
while a comparable increase from 1.4 to 5.9 per
deaths due to motor vehicle crashes in 2014.
Figure 1:
Deaths Related to Drug Overdose and Motor Vehicle Crashes, Georgia, 2001-2015
1,673
1,670
1,568
1,509
1,492
1,482
1,456
1,387
Source:
1,345
1,307
1,274
1,253
1,248
1,223
1,223
1,219
Georgia
1,177
1,125
1,070
1,059
1,074
Department
1,006
956
of Public
859
767
Health,
697
682
647
611
Office of
559
Health
Indicators
for
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Planning,
Drug Overdose Deaths Motor Vehicle Crash Deaths Death files.
Opioids, primarily prescription pain relievers and Further, the state experienced a statistically
heroin, are the main driver of drug overdose significant 10.2% increase in the overdose death
deaths. Of the 1,307 overdose deaths in 2015 rate from 2013 to 2014 (CDC, 2016), and a tripling
in Georgia, 900, or 88% were due to opioids. of overdose deaths between 1999 and 2013.
Figure 2:
Number of Drug Overdose Deaths Related to Opioids
including Heroin in Georgia, 2001-2015 1,274
1,307
1,074 1,070 1,059 1,125
1,006
956
859 900
767 795
697 682 Source:
647 622 633
611 600 606 Office of
559 554
467 Health
380 Indicators
265 277 294
243 246 242 for Planning
90 121 (OHIP),
3 2 3 1 6 20 16 3 25 31 48
1 5 Georgia
Department
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
of Public
All Drug Overdose Deaths Opioid Overdose Deaths, Including Heroin Heroin Overdose Deaths, Only Health.
©2016 Georgia Prevention Project - All Rights Reserved. 14FINDINGS & POLICY
Prescription Opioids and Heroin Epidemic in Georgia RECOMMENDATIONS
Prescription opioid overdose deaths also significantly increased in Georgia, according to the CDC
WONDER Online Database (see Figure 6, retrieved from http://wonder.cdc.gov/mcd-icd10.html).
Figure 3:
Number of Prescription Opioid Overdose Deaths in Georgia, 2001-2015 Source: Centers
588 for Disease
549 Control and
498 488 Prevention
464 (CDC), National
448 441
Center
362 for Health
348
308
Statistics.
270 Multiple Cause
of Death
221
186 1999-2014 on
171
152 CDC WONDER
Online
Database. Data
are from the
Multiple Cause
of Death Files,
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 1999-2015.
While 50 prescription opioid overdose deaths It is important to note that 60% of the 55
occurred in 1999, resulting in a rate of 0.6 per counties with overdose rates that were higher
100,000 age-adjusted deaths, the most recent than the national average in 2014 are located in
available data show a tenfold increase to rural areas.
588 deaths, or a rate of 5.8 per 100,000 age-
6. Economic costs of opioid misuse in Georgia
adjusted deaths, in 2014.
and the United States
The economic burden of prescription opioid
This puts Georgia in the overdose, misuse and dependence in the U.S.
top 11 states nationwide with the was estimated at $78.5 billion in 2013 with over
most prescription opioid one third of this amount coming from increased
healthcare and substance use treatment costs
overdose deaths. ($28.9 billion) (Florence et al., 2016). The
healthcare costs associated with opioid misuse
b. How Georgia compares to other states and in Georgia alone were estimated at $447 million
the nation in 2007 and the estimated per-capita costs were
$44 in Georgia.
While Georgia has a lower rate of all drug
overdose deaths (11.9 per 100,000) compared to Given the increase in overdose deaths and
the U.S. average (14.7 per 100,000) (CDC, 2016), use of opioids in Georgia since 2007, some
55 of the 159 counties in the state had higher experts have estimated a rise in those costs of
rates than the U.S. average in 2014 (CDC/NCHS, at least as 80% since that time. Those same
National Vital Statistics System, mortality data experts agree that the state needs to monitor
(see http://www.cdc.gov/nchs/deaths.htm); and the escalation. Hospitalizations related to
Health Indicators Warehouse (see http://www. opioid use and dependence in Georgia also
healthindicators.gov/Indicators/Drug-poisoning- have skyrocketed from about 302,000 in 2002
deaths-per-100000_10016/Profile). to about 520,000 in 2012. Similarly, the cost of
opioid related inpatient care more than doubled
This marks a significant increase from 11 years
during the same time period, rising to $15 billion
ago, when just 26 counties in Georgia had
overdose death rates that were higher than the
in 2012. 3
U.S. average.
©2016 Georgia Prevention Project - All Rights Reserved. 15FINDINGS & POLICY
Prescription Opioids and Heroin Epidemic in Georgia RECOMMENDATIONS
II. Key Georgia
Issues
1. Overdose reversal
Naloxone, available since 1971, is an allowing pharmacists to dispense naloxone,
opioid antagonist used to reverse opioid and passing Good Samaritan legislation.
overdose through intravenous, intranasal The National Safety Council and Governors
(NARCAN® Nasal Spray), and intramuscular Association submitted recommendations in
formulations. Intramuscular delivery is available 2016 for increasing access to naloxone (NSC,
by syringe in various generic forms or by auto- 2016; NGA, 2016). See Appendix.
injector (EVZIO®).
Georgia’s Naloxone Legislation
Naloxone is highly effective and safe and quickly
House Bill 965, the Georgia 911 Medical
(within a few minutes) restores breathing. It
Amnesty Law, signed on April 24, 2014,
binds to opioid receptors, blocking the effects
expanded access to naloxone. The law
of opioids and endorphins. Side effects include
authorizes administration of naloxone by
withdrawal symptoms in most cases; while they
trained first responders (law enforcement,
are uncomfortable, they are not life threatening.
firefighters, EMS personnel) for overdose
It produces no effect in persons who do
reversal. Additionally, the law allows for
not have opioids present. Naloxone is not
medical professionals to write naloxone
designated as a controlled substance and does
prescriptions, in good faith, to those at risk of
not produce tolerance.
opioid-related overdose.
Because the nature and concentration of the
This law also allows for administration of
opioid causing the overdose is unknown,
naloxone by lay people to persons suspected of
treatment may require multiple doses of
experiencing an opioid overdose and provides
naloxone depending on the severity of
protection from arrest and prosecution for
respiratory depression. Fentanyl (50 to
people who call 911 seeking medical assistance
100 times more potent than morphine) or
for those experiencing alcohol or other drug-
Carfentanil (10,000 times more potent than
related overdose.
morphine) may unknowingly be present
in other substances (e.g., heroin, cocaine, Ultimately this means that neither the
marijuana, counterfeit benzodiazepines, etc.), caller nor victim can be arrested, charged,
significantly increasing overdose risk due to or prosecuted for small amounts of drugs,
high concentration of opioids in undetectable alcohol, or drug paraphernalia if the evidence
quantities (e.g., size of a grain of salt or smaller) was obtained as a result of seeking medical
and require more doses to reverse overdose. assistance. This is important because the timely
administration of naloxone has been proven to
States can increase access to naloxone through
reverse the effects of opioids such as heroin
a number of mechanisms including allowing
and opioids including hydrocodone, oxycodone,
naloxone to be prescribed with standing orders,
methadone and others drugs.
©2016 Georgia Prevention Project - All Rights Reserved. 16FINDINGS & POLICY
Prescription Opioids and Heroin Epidemic in Georgia RECOMMENDATIONS
Victims of opioid overdose who Georgia Overdose Prevention. GOP
receive naloxone in time are less likely to die or (georgiaoverdoseprevention.org) is
suffer long-term brain or tissue damage than a grassroots organization of parents,
those who do not. Removing barriers to health- healthcare professionals, harm reduction
seeking behavior is a crucial step in the fight advocates and friends of those who have
against opioid related deaths. lost loved ones to accidental drug overdose.
GOP formed to create and advocate for the
Naloxone Availability in Georgia
passage of the Georgia 911 Medical Amnesty
Pharmacies. Naloxone is available from some Law described above. The GOP provides
pharmacies in Georgia. Individuals can ask overdose reversal training and a simple
for naloxone without bringing in their own message based on the belief that when one is
prescription at pharmacies because of standing breathing, there is still hope: Don’t run, call 911.
orders that allow dispensing to individuals who
First Responders. The extent to which police
meet specified criteria. Georgia residents may
departments, fire departments, and emergency
obtain Narcan without a prescription from
medical services have naloxone available across
Georgia pharmacies.
the state is unknown. Not all police precincts
Adapt Pharma, a manufacturer of naloxone, have naloxone, and precincts differ in the
provides a naloxone prescription request form availability of naloxone to officers. Cost and the
with a National Drug Code (NDC) number to shelf life of naloxone are concerns.
facilitate filling the prescription by pharmacies.
Medical settings. Naloxone availability or
However, no centralized information exists on
distribution from various types of medical
which pharmacies in Georgia carry naloxone.
settings is unknown. Autoinjectors have
Individuals need to contact pharmacies directly
been distributed free of charge from EVZIO®
to find out whether the pharmacy carries it and
donations to opioid treatment provider clinics.
how to obtain it.
Schools. Because overdose may occur in
The Georgia Pharmacy Association participated
schools, naloxone availability in schools is
in Project DAN (Deaths Avoided by Naloxone) to
receiving increasing attention. The National
help make naloxone available to pharmacies and
School Nurses Association sees naloxone
first responders. Georgia Pharmacy Foundation
availability in schools as an element of a
partnered with Medical Association of Georgia
school’s emergency and response plan for safe
(MAG) Foundation’s Think About It campaign to
and effective reversal of opioid pain reliever
distribute naloxone to pharmacies in 13 northeast
overdose.
counties in 2015. This effort included working to
encourage pharmacies to carry naloxone. Adapt Pharma is offering NARCAN free to
schools around the country. The Clinton
Community organizations that legally can hand
Foundation’s Health Matters Initiative is a
out naloxone (syringe kits or Narcan) are those
partner in this effort. (http://www.drugfree.
with a standing order prescription on file from a
org/news-service/naloxone-offered-free-high-
medical director, and a pharmacy through which
schools-around-country/) Pennsylvania was
to order the prescription.
the first state to make naloxone available in all
Two organizations meet these criteria – the public schools through this program (http://
Georgia Overdose Prevention and the Davis fox43.com/2016/02/01/heroin-overdose-drug-
Direction Foundation. Naloxone kits are naloxone-to-be-provided-free-to-all-pa-public-
distributed through the Atlanta Harm Reduction schools/). States, such as Vermont, Delaware,
Coalition by the Georgia Prevention Project. Illinois, and New York have made naloxone
Availability is supported by grant funding from available in schools.
DBHDD and donations.
Home. Naloxone availability at home provides
for rapid overdose reversal. Overdose may
occur not only from heroin use and non-
prescription use of opioid medications, but
©2016 Georgia Prevention Project - All Rights Reserved. 17FINDINGS & POLICY
Prescription Opioids and Heroin Epidemic in Georgia RECOMMENDATIONS
also from prescription use. Errors in use, does not directly address reducing opioid
sharing of medications, and use according misuse. There is no evidence that availability
to prescription may result in overdose. Co- of life saving overdose reversal medication
prescribing of naloxone with opioid medication increases opioid overdose risk.
can reduce overdose. (Coffin et al., 2016;
2. Awareness, availability, and training on use.
https://www.drugabuse.gov/news-events/
Limited awareness about the potential for
news-releases/2016/06/co-prescribing-
overdose and the availability of overdose
naloxone-in-primary-care-settings-may-reduce-
reversal medication is a concern among
er-visits). H.R. 3680 - Co-Prescribing to Reduce
those who may encounter opioid overdose
Overdoses Act of 2016 was passed by the U.S.
but who have not been properly trained on
House of Representatives in May 2016 and
administration procedures.
is under review by the Senate. https://www.
congress.gov/bill/114th-congress/house- 3. Cost of medication and medication
bill/3680/text expiration.
Escalating Naloxone Cost 4. Limited data on reversals. The ability
to track overdose reversals is limited to
Naloxone costs have increased substantially
documentation by first responders and
over the past decade, particularly since 2014.
emergency rooms. Information from
Naloxone increased from $.92 per dose in 2005
multiple sources needs to be collected and
to $15 - $17 per dose by one manufacturer
validated in a single system.
in 2014 and up to $41 per dose in 2015 by
When naloxone is administered by
another. Narcan costs $63 per single dose, but
individuals without the involvement of
sells at about half that cost to government
first responders or medical services, no
agencies, community organizations and those
information on use is available. A system
without insurance.
for centralized data collection from entities
The cost of Evzio auto-injectors is substantially that distribute naloxone would provide more
higher, having jumped in price from $287.50 accurate information.
in July 2014 to $375 in November 2015, with
5. Linkage to services following reversal.
further increases in 2016 to $2,250 per single
Successful overdose reversals without linkage
dose. Since scrutiny of these prices increases,
to services to reduce or prevent future
manufacturers have responded with discounts
overdose of the same individual is a concern.
and rebates. ADAPT makes Narcan available
First responders report multiple reversals
free of charge to schools and has donated
on the same individual. Furthermore,
50,000 doses, and Kaleo has donated 150,000
subsequent overdoses may lead to
autoinjectors to first responders and nonprofits.
death because intervention with reversal
Most insurance covers naloxone including medication did not occur in time. Evidence-
Medicaid, and EVZIO promotes a zero based, effective systems are needed to link
co-pay option. individuals experiencing an overdose reversal
to services preferably via assertive case
Naloxone Concerns
management and warm hand-offs.
Although Georgia has made progress in this
At present, Georgia Department of Behavioral
area, additional efforts to increase access to
Health and Developmental Disabilities (DBHDD)
naloxone are needed. General concerns about
is developing business-card size materials to
naloxone fall into the five areas: outline below.
distribute. More effective measures for reducing
1. Possible perception as safety net for risk repeat overdose are needed, such as creating
opioid use. Some groups and individuals linkage directly between individuals who can
are concerned that availability of overdose provide direct, culturally congruent support and
reversal medication may be perceived ongoing recovery services. These efforts have
as a safety net by opioid users at risk of been put in place in other communities, and
overdose, and that naloxone availability need exploration for their use in Georgia.
©2016 Georgia Prevention Project - All Rights Reserved. 18FINDINGS & POLICY
Prescription Opioids and Heroin Epidemic in Georgia RECOMMENDATIONS
2. Medication assisted treatment & recovery
SARA Makes the Following support services
Recommendations Regarding
To meet the needs of patients with OUD, it is
Medications
important for patients to have access to the full
1. Increase awareness about overdose and range of SUD treatment services including:
overdose reversal medication.
• outpatient treatment
2. Increase access to naloxone and training
• intensive outpatient treatment
on use of the medication.
• residential treatment
3. Develop a plan to address
naloxone cost. • detoxification
4. Implement information technology • medications
systems to improve tracking of • recovery support services
naloxone use.
(ASAM, 2016).
5. Establish immediate linkages to recovery
services following overdose reversal to According to a National Safety Council report,
Georgia does not meet the indicator for
• reduce the potential for repeat “meets need for OUD treatment”, measured by
overdose, and sufficient buprenorphine treatment capacity.
• increase the likelihood of sustained Ongoing treatment and recovery support of
recovery individuals affected by opioid use disorders
6. Mandate Insurance Coverage for involves addressing physical dependence
Opioid Overdose-Reversal Medication: (including overdose risk) and the behavioral
Naloxone revives an individual from a and psychosocial skills required for managing
heroin or other opioid overdose and has recovery. Treatment decisions could depend
saved thousands of Georgians’ lives. upon a range of factors including substance
use history (e.g., duration, substances used,
It has no psychoactive effects and prior recovery efforts), co-occurring disorders,
concomitantly, no misuse potential. treatment availability, cost/payment options,
To expand access to this life-saving family support, and legal requirements.
medication, the new legislation requires Behavioral counseling, a key component of
insurance companies to cover the costs Georgia’s recovery-oriented systems of care for
of naloxone when prescribed to a person opioid addiction, generally follows the National
who is addicted to opioids and/or to Institute on Drug Abuse (NIDA)’s Principles
his/her family member/s on the same of drug addiction treatment: A research-
insurance plan. based guide (2012; 3rd edition: drugabuse.
gov/publications/principles-drug-addiction-
treatment/evidence-based-approaches-to-drug-
addiction-treatment/behavioral-therapies).
How Georgia’s public behavioral health
treatment system is managed currently
The Department of Behavioral Health and
Developmental Disabilities’ mission is to lead
an accountable and effective continuum of
care to support Georgians with behavioral
health challenges, and intellectual and
developmental disabilities in a dynamic
healthcare environment. State funds and federal
©2016 Georgia Prevention Project - All Rights Reserved. 19FINDINGS & POLICY
Prescription Opioids and Heroin Epidemic in Georgia RECOMMENDATIONS
block grants support a network of six regional opioid detoxification services and medication
offices that administer each region’s hospital extremely limited in Georgia.
and community resources. (Community
Medications to manage withdrawal
services are provided through contracts with
symptoms during detoxification from
private, for-profit, non-profit, and quasi-public
opioids include methadone, buprenorphine
agencies under contract with DBHDD through
alone or with naloxone (Suboxone®), milder
the regional offices. Services focus on addictive
opioids, and clonidine. The length of the
diseases, behavioral health, behavioral health
detoxification process varies by individual
prevention and other services.
factors and goals. It may include use of
Key Terms and Implications multiple medications concurrently or
sequentially. Individual differences may
Medication-assisted Treatment (MAT)
include level of tolerance, substances used,
Medication-assisted treatment (MAT) refers length of use, and medical complications.
to multi-faceted individualized substance use
In addition to becoming opioid free, goals
disorder treatment models that employ both
may include transition to methadone,
medications and other services and supports for
buprenorphine, or extended-release injectable
recovery maintenance.
naltrexone, each of which may affect length of
The Georgia Department of Behavioral Health time required. Transition to extended-release
and Developmental Disabilities (DBHDD) injectable naltrexone requires a 7-10 day opioid
recognizes that MAT provides specific free period to avoid precipitating withdrawal.
interventions for reducing and/or eliminating the
Gaps in medication may make an individual
use of illicit opioids and other drugs of misuse;
vulnerable to using substances in their
while developing the individual’s social support
recovery process. Establishing systems for the
network and necessary lifestyle changes;
most effective implementation of treatment
psychoeducational skills; pre-vocational skills
protocols can lessen these vulnerabilities and
leading to work activity (by reducing substance
provide greater supports for recovery.
use as a barrier to employment); social and
interpersonal skills; improved family functioning; Management of tapers or transitions
the understanding of addictive disease; and from the opioid agonists, methadone or
the continued commitment to a recovery and buprenorphine, to extended-release injectable
maintenance program. naltrexone could be affected by approved
usage of transitional medications.
Medically Managed Detoxification/Withdrawal
Management Reduction in use of methadone and
buprenorphine requires a long taper. The
Opioid withdrawal, whether from prescription
length of the taper can be reduced with use of
medication or heroin, often produces extreme
alternative medications, such as milder opioids,
and extended discomfort. Symptoms include:
which may not be approved for opioid tolerance
sweating, shaking, chills, body aches, yawning,
management. Longer tapers increase cost and
large pupils, headache, drug craving, nausea,
impact the viability of transitioning clients.
vomiting, abdominal cramping, diarrhea,
inability to sleep, confusion, agitation, Access to medically managed detoxification for
depression, anxiety, … and other behavioral opioids and other substances differs broadly
changes, and can last for days and weeks. across the country, from no availability to
Fear of withdrawal symptoms is a significant free walk-in 24/7, for anyone, regardless of
deterrent to discontinuing opioid use, and a insurance status.
frequent reason for relapse.
Outpatient and inpatient options might be
Because opioid withdrawal is not considered appropriate for opioid detoxification. Insurance
life threatening, detoxification is generally not coverage restrictions, as well as lack of available
covered by Medicaid and private insurance, beds or outpatient services, limit access to
making access to inpatient or outpatient detoxification for many individuals ready to
©2016 Georgia Prevention Project - All Rights Reserved. 20You can also read