DRUG WORLD 7 - GLOBAL OVERVIEW OF DRUG DEMAND AND SUPPLY - ReliefWeb
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
GLOBAL OVERVIEW OF
DRUG DEMAND AND SUPPLY
Latest trends, cross-cutting issues
2
WORLD
2017
DRUG
REPORTThis booklet constitutes the second part of the World Drug Report 2017. © United Nations, May 2017. All rights reserved worldwide. ISBN: 978-92-1-148293-5 eISBN: 978-92-1-060625-7 United Nations publication, Sales No. E.17.XI.8 This publication may be reproduced in whole or in part and in any form for educational or non-profit purposes without special permission from the copyright holder, provided acknowledgement of the source is made. The United Nations Office on Drugs and Crime (UNODC) would appreciate receiving a copy of any publication that uses this publication as a source. Suggested citation: United Nations Office on Drugs and Crime, World Drug Report 2017 (ISBN: 978-92-1-148291-1, eISBN: 978-92-1-060623-3, United Nations publication, Sales No. E.17.XI.6). No use of this publication may be made for resale or any other commercial purpose whatsoever without prior permission in writing from UNODC. Applications for such permission, with a statement of purpose and intent of the reproduction, should be addressed to the Research and Trend Analysis Branch of UNODC. DISCLAIMER The content of this publication does not necessarily reflect the views or policies of UNODC or contributory organizations, nor does it imply any endorsement. Comments on the report are welcome and can be sent to: Division for Policy Analysis and Public Affairs United Nations Office on Drugs and Crime PO Box 500 1400 Vienna Austria Tel: (+43) 1 26060 0 Fax: (+43) 1 26060 5827 E-mail: wdr@unodc.org Website: www.unodc.org/wdr2017
PREFACE
I am proud to say that this year we are marking 20 As the World Drug Report 2017 clearly shows, there
years of the World Drug Report. is much work to be done to confront the many
harms inflicted by drugs, to health, development,
Over the past two decades, the United Nations
peace and security, in all regions of the world.
Office on Drugs and Crime (UNODC) has been
at the forefront of global research into complex areas Globally, there are an estimated minimum of
of drug use and supply, supporting international 190,000 — in most cases avoidable — premature
cooperation and informing policy choices with the deaths from drugs, the majority attributable to the
latest estimates, information on trends and use of opioids.
analysis. The terrible impact of drug use on health can also
This year we are launching a new format, with the be seen in related cases of HIV, hepatitis and
report available as five separate booklets: the execu- tuberculosis.
tive summary, together with the report’s conclusions Much more needs to be done to ensure affordable
and policy implications; a global overview of drug access to effective scientific evidence-based preven-
use and supply; a market analysis of plant-based tion, treatment and care for the people who
drugs; a market analysis of synthetic drugs; and a desperately need them, including those in prison
thematic booklet on the links between drugs and settings. As just one example, this year’s report high-
organized crime, illicit financial flows, corruption lights the need to accelerate accessibility to the
and terrorism. We have done this in response to treatment of hepatitis C, a disease whose negative
readers’ needs and to improve user-friendliness, health impact on people who use drugs is far greater
while maintaining the rigorous standards expected than that of HIV/AIDS.
from the Office’s flagship publication.
Recent attention has focused on the threats posed
The 2017 report comes at a time when the interna- by methamphetamine and new psychoactive sub-
tional community has acted decisively to achieve stances (NPS). However, as the report shows, the
consensus on a way forward for joint action. manufacture of both cocaine and opioids is increas-
ing. These drugs remain serious concerns, and the
The outcome document unanimously adopted at opioid crisis shows little sign of stopping.
last year’s special session of the General Assembly
on the world drug problem contains more than 100 The World Drug Report 2017 further looks at the
concrete recommendations for implementing bal- links with other forms of organized crime, illicit
anced, comprehensive and integrated approaches to financial flows, corruption and terrorism. It draws
effectively addressing and countering the world drug on the best available evidence and, most of all, high-
problem. lights the fact that much more research needs to be
carried out in these areas.
Moreover, at its sixtieth session, in March 2017, the
Commission on Narcotic Drugs adopted resolution Corruption is the great enabler of organized crime,
60/1, reinforcing commitment to implementing the and opportunities for corruption exist at every stage
outcome document and charting a course to the of the drug supply chain. However, too little is
2019 target date of the 2009 Political Declaration known about how different types of corruption
and Plan of Action on the world drug problem, as interact with drug markets.
well as strengthening action towards the Plan of The outcome document of the special session of the
Action’s agreed goals and targets. General Assembly on the world drug problem and
3WORLD DRUG REPORT 2017
Security Council resolutions express concern about As the special session of the General Assembly and
terrorist groups profiting from drug trafficking, the recent session of the Commission on Narcotic
among other forms of transnational organized crime. Drugs have shown, the international community is
equipped to respond swiftly and decisively to global
It is well established that there are terrorists and
drug-related challenges.
non-State armed groups profiting from the drug
trade — by some estimates, up to 85 per cent of For example, in March, the Commission scheduled
opium poppy cultivation in Afghanistan is in terri- two precursors and an analogue to the scheduled
tory under influence of the Taliban. drug fentanyl. This important step will make it
harder for criminals to illicitly manufacture fentanyl
However, evidence on the organized crime-terrorism
and its analogues and, I hope, can help to stem the
nexus remains patchy at best. Moreover, these links
tragic increase in opioid overdoses in recent years.
are not static. Relations between organized crime
and terrorists groups are always evolving, much like However, there remains an enormous need for
drug markets themselves. capacity-building and technical assistance, and fund-
ing continues to fall far short of political
As we have seen with the NPS market, drug use,
commitment. Further resources are urgently needed
supply, trafficking routes and the substances them-
to help all Member States implement the recom-
selves continue to shift and diversify at alarming
mendations contained in the outcome document
speed.
of the special session of the General Assembly and
Drugs continue to represent a major source of rev- achieve related targets under the Sustainable Devel-
enue for organized crime networks, but business opment Goals.
models are changing, with criminals exploiting new
The many evolving drug challenges also highlight
technologies, such as the darknet, that are altering
the importance of prevention — science- and rights-
the nature of the illicit drug trade and the types of
based drug use prevention — but also prevention
players involved, with looser, horizontal networks
of crime, corruption, terrorism and violent extrem-
and smaller groups becoming more significant. New
ism, in line with commitments under the
ways of delivering drugs further point to the need
conventions and United Nations standards and
to involve other sectors such as postal services in the
norms.
fight against drug trafficking.
Finally, I ask all Governments to help us improve
Clearly, countries must be able to act and react to
the evidence base for these reports. Areas such as
an ever-changing and formidable array of threats
the links between drugs, terrorism and insurgency
and problems. UNODC is fully engaged in strength-
clearly touch upon sensitive intelligence, and there
ening responses, working closely with our United
are legitimate concerns about compromising sources,
Nations partners and in line with the international
collection and operations. But if we want to effec-
drug control conventions, human rights instruments
tively address drug challenges we need to strengthen
and the 2030 Agenda for Sustainable Development,
international cooperation and information-sharing
which are themselves complementary and mutually
to the extent possible, to close the gaps and ensure
reinforcing.
that joint action is targeted, effective and timely.
Yury Fedotov
Executive Director
United Nations Office on Drugs and Crime
4CONTENTS
BOOKLET 1 EXECUTIVE SUMMARY — CONCLUSIONS AND POLICY IMPLICATIONS
GLOBAL OVERVIEW OF DRUG DEMAND AND SUPPLY
BOOKLET 2 Latest trends, cross-cutting issues
PREFACE. . .......................................................................................................... 3
EXPLANATORY NOTES...................................................................................... 7
KEY FINDINGS................................................................................................... 9
INTRODUCTION.. ............................................................................................. 11
A. EXTENT OF DRUG USE������������������������������������������������������������������������������� 13
A quarter of a billion people use drugs globally�����������������������������������������������������������������������������������13
Problem drug use as reflected in the demand for drug treatment���������������������������������������������������������15
B. HEALTH IMPACT OF DRUG USE����������������������������������������������������������������� 19
Almost 12 million people worldwide injected drugs in 2015���������������������������������������������������������������19
HIV and hepatitis markedly impact on people who inject drugs���������������������������������������������������������19
Drug use and tuberculosis�������������������������������������������������������������������������������������������������������������������21
At least 190,000 mostly preventable drug-related deaths in 2015��������������������������������������������������������26
C. PHARMACEUTICAL OPIOIDS���������������������������������������������������������������������� 29
Access to pain medication: key issues and considerations��������������������������������������������������������������������30
Misuse of prescription opioids�������������������������������������������������������������������������������������������������������������31
Use of prescription opioids and heroin in the United States����������������������������������������������������������������32
Misuse of tramadol in Africa and Asia�������������������������������������������������������������������������������������������������38
D. EXTENT OF DRUG SUPPLY������������������������������������������������������������������������� 39
Cultivation and production�����������������������������������������������������������������������������������������������������������������39
After cannabis, cocaine accounts for the largest quantities seized���������������������������������������������������������40
Drug trafficking over the darknet continues to increase at a fast pace �������������������������������������������������42
ANNEX............................................................................................................ 47
Annual prevalence of drug use�������������������������������������������������������������������������������������������������������������47
Number and prevalence of people who inject drugs and those living with HIV����������������������������������49
Opium/Heroin������������������������������������������������������������������������������������������������������������������������������������50
Coca/Cocaine��������������������������������������������������������������������������������������������������������������������������������������58
Cannabis���������������������������������������������������������������������������������������������������������������������������������������������60
GLOSSARY.. ..................................................................................................... 65
REGIONAL GROUPINGS. . ................................................................................. 66
MARKET ANALYSIS OF PLANT-BASED DRUGS
BOOKLET 3 Opiates, cocaine, cannabis
MARKET ANALYSIS OF SYNTHETIC DRUGS
BOOKLET 4 Amphetamine-type stimulants, new psychoactive substances
THE DRUG PROBLEM AND ORGANIZED CRIME,
BOOKLET 5 ILLICIT FINANCIAL FLOWS, CORRUPTION AND TERRORISM
5Acknowledgements
The World Drug Report 2017 was prepared by the Research and Trend Analysis Branch, Division for
Policy Analysis and Public Affairs, United Nations Office on Drugs and Crime, under the supervision
of Jean-Luc Lemahieu, Director of the Division, and Angela Me, Chief of the Research and Trend
Analysis Branch.
General coordination and content overview Editing
Chloé Carpentier Jonathan Gibbons
Angela Me
Graphic design and production
Analysis and drafting Anja Korenblik
Philip Davis Suzanne Kunnen
Kamran Niaz Kristina Kuttnig
Thomas Pietschmann
Coordination
Data management and estimates production Francesca Massanello
Enrico Bisogno
Data Support
Jesus Maria Garcia Calleja (WHO)
Diana Camerini
Riku Lehtovuori
Raffaella Conconi
Andrea Oterova
Sarika Dewan
Umidjon Rakhmonberdiev
Ali Saadeddin Administrative support
Keith Sabin (UNAIDS) Anja Held
Antoine Vella Iulia Lazar
Review and comments
The World Drug Report 2017 benefited from the expertise and invaluable contributions of UNODC
colleagues in the Drug Prevention and Health Branch of the Division for Operations; the Corruption
and Economic Crime Branch, the Organized Crime and Illicit Trafficking Branch and the Terrorism
Prevention Branch of the Division for Treaty Affairs; and the Research and Trend Analysis Branch of
the Division for Policy Analysis and Public Affairs.
The Research and Trend Analysis Branch acknowledges the invaluable contributions and advice
provided by the World Drug Report Scientific Advisory Committee:
Jonathan Caulkins Charles Parry
Paul Griffiths Peter Reuter
Marya Hynes Francisco Thoumi
Vicknasingam B. Kasinather Alison Ritter
Letizia Paoli Brice De Ruyver
UNODC gratefully acknowledges the contribution of Masoud Dara and Annabel Baddeley of the
World Health Organization to the section on tuberculosis.
The research and preparation of the joint UNODC/UNAIDS/WHO/World Bank estimates of
the number of people who inject drugs were partly funded by the HIV/AIDS Section of the Drug
Prevention and Health Branch of the Division for Operations of UNODC.EXPLANATORY NOTES
The boundaries and names shown and the designa- All uses of the word “drug” in the World Drug Report
tions used on maps do not imply official endorsement refer to substances under the control of the inter-
or acceptance by the United Nations. A dotted line national drug control conventions.
represents approximately the line of control in
All analysis contained in the World Drug Report is
Jammu and Kashmir agreed upon by India and Paki-
based on the official data submitted by Member
stan. The final status of Jammu and Kashmir has
States to the United Nations Office on Drugs and
not yet been agreed upon by the parties. Disputed
Crime through the annual report questionnaire
boundaries (China/India) are represented by cross-
unless indicated otherwise.
hatch owing to the difficulty of showing sufficient
detail. The data on population used in the World Drug
Report are taken from: United Nations, Department
The designations employed and the presentation of
of Economic and Social Affairs, Population Divi-
the material in the World Drug Report do not imply
sion, World Population Prospects: The 2015
the expression of any opinion whatsoever on the
Revision.
part of the Secretariat of the United Nations con-
cerning the legal status of any country, territory, city References to dollars ($) are to United States dollars,
or area, or of its authorities or concerning the delimi- unless otherwise stated.
tation of its frontiers or boundaries. References to tons are to metric tons, unless other-
Countries and areas are referred to by the names wise stated. R stands for the correlation coefficient,
that were in official use at the time the relevant data used as measure of the strength of a statistical rela-
were collected. tionship between two or more variables, ranging
from 0 to 1 in case of a positive correlation or from
All references to Kosovo in the World Drug Report,
0 to -1 in case of a negative correlation.
if any, should be understood to be in compliance
with Security Council resolution 1244 (1999).
Since there is some scientific and legal ambiguity
about the distinctions between “drug use”, “drug
misuse” and “drug abuse”, the neutral terms “drug
use” and “drug consumption” are used in the World
Drug Report.
72
KEY FINDINGS
Harm caused by drug use remains more DALYs are lost as a result of hepatitis C than
considerable of HIV infection among people who use drugs. Most
of those DALYs are the result of premature death,
An estimated quarter of a billion people, or around
while the remainder are the result of years lived with
5 per cent of the global adult population, used drugs
disability.
at least once in 2015. Even more worrisome is the
fact that about 29.5 million of those drug users, or People who use drugs particularly
0.6 per cent of the global adult population, suffer vulnerable to tuberculosis
from drug use disorders.
Based on the limited data available from studies in
The magnitude of the harm caused by drug use is Europe, Asia and the Americas, the prevalence of
underlined by the estimated 28 million years of tuberculosis among PWID is estimated at approxi-
“healthy” life (disability-adjusted life years (DALYs)) mately 8 per cent, which compares with less than
lost worldwide in 2015 as a result of premature death 0.2 per cent in the general population.
and disability caused by drug use. Of those years
lost, 17 million were attributable solely to drug use People who use drugs may have a particular need
disorders across all drug types. DALYs attributable for interventions that prevent and treat tuberculosis.
to morbidity and mortality resulting from all causes They may be disproportionately affected by the risk
of drug use have increased overall in the past decade. factors for the disease. Infection with HIV is one of
Yet, with fewer than one in six persons with drug the main reasons for the high prevalence of tuber-
use disorders provided with treatment each year, the culosis among PWID and tuberculosis is one of the
availability of and access to science-based services leading causes of mortality among people who use
for the treatment of drug use disorders and related drugs and are living with HIV.
conditions remain limited. Treatment of tuberculosis is particularly complex
Opioids, the most harmful drug type for people who use drugs as they may be living with
multiple, co-existing infectious diseases and psychi-
Opioids, including heroin, remain the most harmful
atric and medical co-morbidities in addition to drug
drug type in health terms. A significant proportion
dependency. Furthermore, many barriers to the pre-
of the large number of premature deaths among
vention and treatment of tuberculosis are more
people who use drugs is attributable to opioids. In
difficult to surmount for people who use drugs than
addition, opioid use disorders account for the
for the general population.
heaviest burden of disease attributable to drug use
disorders: in 2015, almost 12 million DALYs, or 70 Prison a high-risk environment for the
per cent of the global burden of disease attributable spread of infectious diseases
to drug use disorders, were attributable to opioids.
Drug use, including the use of heroin and injecting
Hepatitis C causing greatest harm among
drug use, are commonplace in many prisons. One
people who use drugs
out of three prisoners has used an illicit substance
People who inject drugs (PWID) face some of the at some time while incarcerated, with 16 per cent
most severe health consequences associated with reporting current (past-month) use. Cannabis is by
drug use. Almost 12 million people worldwide inject far the most commonly used drug in prison, while
drugs, of whom one in eight (1.6 million) are living heroin ranks second. Approximately 10 per cent of
with HIV and more than half (6.1 million) are living prisoners report using heroin at some time while
with hepatitis C. incarcerated, one third of whom report current
(past-month) use within prison.
The number of deaths attributable to hepatitis C
among people who use drugs is greater than from Unsafe injecting practices help to spread HIV among
other causes of death related to drug use. Overall, PWID in prison populations and ultimately to the
9WORLD DRUG REPORT 2017
wider community. People who use drugs who are products while actually containing fentanyl and fen-
incarcerated are also placed at greater risk of tanyl analogues, as well as non-opioid substances
tuberculosis. such as derivatives of benzodiazepine and
Higher rate of increase in the burden of
methylphenidate.
disease from drug use disorders among Expansion of the cocaine market
women than among men Data on drug production, trafficking and use point
At least twice as many men than women suffer from to an overall expansion of the market for cocaine
drug use disorders. However, once women have ini- worldwide. Following a long-term decline, coca bush
tiated substance use, in particular, use of alcohol, cultivation increased by 30 per cent during the
cannabis, opioids and cocaine, they tend to increase period 2013-2015, mainly as a result of increased
their rate of consumption more rapidly than men. cultivation in Colombia. Total global manufacture
of pure cocaine hydrochloride reached 1,125 tons
In the past decade, the negative health impact of in 2015.
drug use has increased more rapidly among women
than among men. The rate of increase in the number The quantities of cocaine seized are also on the
of DALYs attributed to drug use disorders in 2015, increase, reaching a record level of 864 tons in 2015.
particularly opioid and cocaine use disorders, was Opium production on the increase
greater among women (25 per cent and 40 per cent, In 2016, global opium production (6,380 tons)
respectively) than among men (17 per cent and 26 increased by one third compared with the previous
per cent, respectively). year. Although there was also an increase in the size
Evidence shows that making pharmaceuti- of the area under opium poppy cultivation, the
cal opioids available to the population major increase in opium production was primarily
who need them most often does not lead the result of an improvement in opium poppy yields
to their misuse or addiction in Afghanistan compared with the previous year.
Despite the fact that pharmaceutical opioids for Global seizures relatively stable
pain management and treatment of opioids use dis- The largest quantities of drugs seized were of can-
orders are included in the list of essential medicines nabis, followed by coca/cocaine related substances
by WHO, there remain significant gaps and barriers and opioids.
in the access to and availability of pain medications
in most parts of the world. The sharpest increases in quantities seized over the
period 2010-2015 were reported for synthetic NPS,
Fear of addiction to pharmaceutical opioids which increased fourfold, and of ATS, which dou-
contributes to the complex dynamics influencing bled. Sharp increases, in particular during 2015,
access to and availability of controlled medicines. were also reported for cocaine, in line with reports
However, a structured review of the literature found of rising levels of cocaine manufacture.
that 3 per cent of chronic non-cancer pain patients
Trafficking through the darknet: relatively
regularly taking opioids developed opioid use
small but growing fast
disorders.
The darknet allows users to buy drugs with a crypto-
Opioid market in a constant state of currency, such as bitcoin, and have their purchases
change delivered to them in a concealed manner. Typical
The opioid market is becoming more diversified: buyers are recreational users of cannabis, “ecstasy”,
this is illustrated by the example of the United States, cocaine, hallucinogens and NPS. They are less likely
where the opioid market comprises a combination to order heroin or methamphetamine. Although the
of internationally controlled substances, particularly darknet accounts for only a small percentage of drug
heroin, and prescription medicines that are either sales, the market has been growing by around 50
diverted from the legal market or produced as coun- per cent per year in recent years.
terfeit medicines on a large scale. These counterfeit
medicines are made to look like pharmaceutical
10INTRODUCTION
Although presented as a stand-alone publication, who use drugs, both in the general population and
this booklet constitutes the second chapter of the in prisons, as well as challenges in the treatment of
World Drug Report 2017. It provides a global over- tuberculosis among those groups, is featured for the
view of the latest estimates of and trends in drug first time in the World Drug Report. An analysis of
use and drug supply, as well as of several cross-cut- the dynamics of and trends in the misuse of pre-
ting issues related to the world drug problem. Such scription opioids is also included, as is a brief
issues include the health impact of drug use, includ- discussion of the issues related to making opioid
ing trends among people with drug use disorders, painkillers available and accessible to the population
problem drug use as reflected in treatment demand in need of them. Finally, the booklet contains a
and estimates of the number of people who inject global overview of the latest estimates of and trends
drugs (PWID) and of those living with HIV and in cultivation, production and trafficking of illicit
hepatitis. drugs, including on the Internet, using the
darknet.
The present booklet also examines the global extent
of drug-related deaths, particularly of fatal overdoses,
with recent trends in some countries being presented
as illustrative. A review of tuberculosis among people
28 million healthy years of life lost as a result of drug use
17 million healthy years of life lost as a result of drug use disorders
28 million
disability “healthy” years of life lost
drug use
premature
death
years of
life lost
DALYs
attributed
birth to drug use expected
life years
years of “healthy” years of life lost as a
DALYs = life lost as a result + result of premature
of disability death
17 million DALYs attributed to drug use disorders
10 million years of life lost as a result of disability caused by drug use
18 million years of life lost as a result of premature death caused by drug use
11GLOBAL OVERVIEW OF DRUG DEMAND AND SUPPLY A. Extent of drug use
2
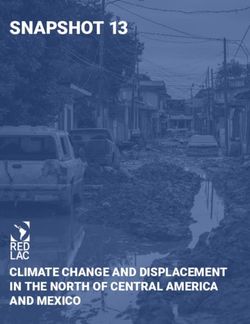
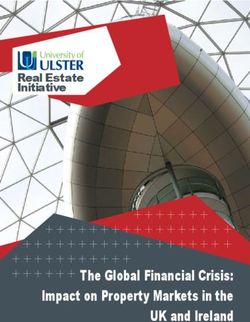
Fig. 1 Global trends in estimated number of
A. EXTENT OF DRUG USE
population age 15-64 (percentage) drug users, 2006-2015
Number of people who use drugs
8
A quarter of a billion people use 350
Annual prevalence among
drugs 7globally 300
6 255
It is estimated that a quarter of 5.2
a billion people,
5.2 5.2 or
5.2 5.3 250 240 243 246 247
226
4.9 4.9 4.8 5.0
about 5 5per cent of 4.6
the adult population aged 15-64 208 211 203 210
(millions)
200
4 drugs at least once in 2015 (range: 158
years, used
million 3to 351 million),1 meaning that the extent 150
of drug2 use among the world population has 100
remained stable
1 0.6
over the past five years. Globally, 50 28.0 27.3 27.1 27.127.327.4 27.4 28.7 29.5
over 11 per cent of people who use drugs, or around 26.0
0 0
29.5 million people (range: 15.3 million to 43.1
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
million), are estimated to suffer from drug use dis-
orders.This means that
Prevalence their drug
of people whouse
useisdrugs
harmfull to Number of people who use drugs
the point that they may
Prevalence experience
of people withdrug
drug dependence
use disorders Number of people with drug use disorders
and require treatment. Moreover, the Global Burden Source: UNODC, responses to annual report questionnaire.
of Disease Study 2015 estimated that around 17 Note: Estimates are for adults (aged 15-64) who used drugs in the
million "healthy" years of life lost (disability- past year.
adjusted life years or DALYs)2, 3 were attributable Fig. 2 Global trends in the estimated
to drug use disorders in that year. prevalence of drug use and prevalence
Opioids are the substances that cause the highest of people with drug use problems,
negative health impact, but cannabis remains the 2006-2015
population age 15-64 (percentage)
Number of people who use drugs
8 350
world’s most widely used drug, with an annual
Annual prevalence among
prevalence of 3.8 per cent of the adult population, 7 300
or an estimated 183 million people (range 128 6
5.2 5.2 5.2 5.2 5.3 250
million to 238 million), having used cannabis in 5 4.9 4.9 4.6 4.8 5.0 208 211
(millions)
the past year. Cannabis use has increased in parts of 200
4
North and South America, while its use is declining 3 150
or stabilizing in parts of Europe, albeit from or at 100
2
high levels. Amphetamines remain the second most
commonly used drug worldwide, with an estimated 1 0.6 50 28.0
26.0
35 million past-year users (range 13 million to 58 0 0
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2006
2007
million), and the use of amphetamines, particularly
methamphetamine, is perceived to be increasing in Prevalence of people who use drugs Number
many subregions, including North America, Oceania Prevalence of people with drug use disorders Number
and most parts of Asia.
Source: UNODC, responses to the annual report questionnaire.
Note: Estimated percentage of adults (aged 15-64) who used
1 These estimates are based on updates by some 25 countries drugs in the past year.
in which new data were available, and reflect the best data
currently available on the global extent of drug use.
2 As defined by the Word Health Organization (WHO), one The number of past-year users of opiates and per-
DALY is one lost year of “healthy” life. “Healthy” years of sons who misuse prescription opioids is estimated
life lost is the combination of life lost as a result of prema- at about 35.1 million people (range 28.3 million to
ture death and life lost as a result of disability (any short-
term or long-term health loss). 42.7 million), of whom some 17.7 million are esti-
3 Global Burden of Disease Study 2015 DALYs and HALE mated to have used opiates (heroin and opium).
Collaborators, “Global, regional, and national disability- The misuse of pharmaceutical opioids remains of
adjusted life years (DALYs) for 315 diseases and injuries and concern in many countries, particularly the United
healthy life expectancy (HALE), 1990-2015: a systematic
analysis for the Global Burden of Disease Study 2015”, States of America, where, coupled with an increase
The Lancet, vol. 388, No. 10053 (2016), pp. 1603-1658. in heroin and fentanyl use, it has resulted in a
13WORLD DRUG REPORT 2017
Drugs and infectious diseases that produce the highest negative health
impact of drug use
The Global Burden of Disease Study 2015 examined the con- from all causes of drug use increased in the period 2005-2015,
nection between the use of drugsa and the development of with DALYs increasing from 24 million to 28 million, whereas
poor health.b The most negative health consequences of drug the burden of disease attributed to drug use disorders alone
use are associated with untreated hepatitis C (which can lead increased from 14 million to 17 million DALYs over the same
to liver cirrhosis and cancer) and opioid use disorders. period. The largest increase in DALYs was attributed to opioid
use disorders, but large increases were also attributed to disor-
The burden of disease is greater for health consequences related
ders resulting from use of amphetamines and use of cocaine.
to hepatitis C than to HIV infection: considerably more deaths
(222,000 from hepatitis C; 60,000 from HIV) and DALYs (6.3
The fact that opioids, including heroin, account for most of the
million from hepatitis C; 3.0 million from HIV) are attributable
negative health consequences of drug use is also reflected in
to hepatitis C than to HIV. Most of those DALYs are the result
data provided by hospital emergency departments. In Europe,
of premature death, while the remainder are the result of years
opioids and heroin are most frequently associated with acute
lived with disability.
toxicity presentations, with heroin involved in almost one out
Opioids remain major drugs in terms of health consequences, of four cases. Cocaine and cannabis are also prominent (each
with nearly 12 million of the total 17 million DALYs attrib- accounting for 16 per cent of presentations), with new NPS,
uted to drug use disorders in 2015 being attributed to opioid mostly synthetic cathinones, and mephedrone in particular,
use disorders.c Opioids also account for the majority of drug- accounting for 11 per cent. Polydrug use presentations are also
related deaths in many subregions. The overall burden of disease common in Europe, being involved in 38 per cent of cases.d
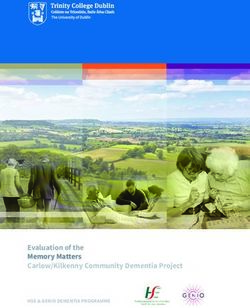
Number of deaths and “healthy” years of life lost (DALYs) attributable to drug use, 2015
Number of deaths (thousands) attributable “Healthy” years of life lost (DALYs) (millions)
to drug use, 2015 attributable to drug use, 2015
0 50 100 150 200 0.0 5.0 10.0 15.0
HIV/AIDS—tuberculosis -25.7 -27.1
HIV/AIDS resulting in other diseases -3.6 -5.6
Hepatitis C -12.0 -12.3
Percentage change from 2005
Percentage change from 2005
Liver cancer resulting from hepatitis C 39.0 27.5
Cirrhosis and other chronic liver diseases 19.0 12.1
resulting from hepatitis C
Opioid use disorders 29.6 22.3
Cocaine use disorders 49.7 37.0
Amphetamine use disorders 67.5 40.1
Cannabis use disorders 5.3
Other drug use disorders 23.0 21.8
Self-harm 2.6 0.1
Source: “Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic
risks or clusters of risks, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015”.
Notes: Error bars represent uncertainty intervals. Numbers given in charts are percentage changes from 2005.
a In the Global Burden of Disease Study, drug use as a risk factor c Global Burden of Disease Study 2015 DALYs and HALE Col-
is defined as the extent of the population who are dependent on laborators, “Global, regional, and national disability-adjusted
opioids, cannabis, cocaine or amphetamines and the population life years (DALYs) for 315 diseases and injuries and healthy life
who have ever injected drugs (i.e., extent of exposure to drug use expectancy (HALE), 1990-2015: a systematic analysis for the
as a risk factor). Global Burden of Disease Study 2015”, The Lancet, vol. 388, No.
b Global Burden of Disease Study 2015 Risk Factors Collaborators, 10053 (2016), pp. 1603-1658.
“Global, regional, and national comparative risk assessment of d European Monitoring Centre for Drugs and Drug Addiction,
79 behavioural, environmental and occupational, and metabolic Hospital Emergency Presentations and Acute Drug Toxicity in
risks or clusters of risks, 1990-2015: a systematic analysis for the Europe: Update from the Euro-DEN Plus Research Group and the
Global Burden of Disease Study 2015”, The Lancet, vol. 388 EMCDDA (Luxembourg, Publications Office of the European
(2016), pp. 1659-1724. Union, 2016).
14GLOBAL OVERVIEW OF DRUG DEMAND AND SUPPLY A. Extent of drug use
2
combined and interrelated epidemic and an increase Problem drug use as reflected in the
in morbidity and mortality related to opioids.4 demand for drug treatment
There are also indications of a recent increase in
heroin use in parts of Western and Central Europe, Information on people in treatment for disorders
suggesting that the long-term downward trend in related to the use of different drugs can be taken as
parts of that subregion may be coming to an end. a proxy to understand the nature and extent of prob-
lem drug use. However, this is only a latent indicator
With a high prevalence of cocaine use in North of trends in the use of drugs, owing to the time lag
America (1.8 per cent, Western and Central Europe between the period when people start using drugs,
(1.1 per cent) and Oceania (1.5 per cent, primarily when they develop drug use disorders and when
Australia and New Zealand), it is estimated that they seek treatment for drug use.
there are nearly 17 million past-year users of cocaine
worldwide. Although cocaine use is decreasing or For people with drug use disorders, the availability
stabilizing in parts of Europe, wastewater analysis and access to treatment services, particularly of
suggests an increase in consumption of the drug in science-based services, remains limited at the global
the past five years (see booklet 3, chapter B). There level, with one out of six people with drug-use
are also indications of an increase in parts of North disorders being provided with treatment each year.
America. Some 21.6 million people are estimated On average, among those treated, the proportion
to be past-year users of “ecstasy”, the use of which of people with cannabis and opioid use disorders
remains high in Oceania (primarily Australia and remains larger than the proportion of people with
New Zealand), Europe and North America. disorders related to the use of other substances. It
“Ecstasy” use had been declining in Western and is important to understand, however, that there is
Central Europe, but since 2013, data from many great variability in the definition and practice of
European countries, particularly in Western and what constitutes treatment of cannabis use disorders.
Central Europe, show an increase in its use. At present, such treatment consists of behavioural
or psychosocial interventions that may vary from a
Many drug users, both occasional and regular, tend
to be polydrug users. In order to enhance the overall Fig. 3 Proportion of people in treatment for
psychoactive experience of the drugs taken, they use different drugs, global averages
more than one substance concurrently or sequen-
tially to experience a cumulative or synergistic effect,WORLD DRUG REPORT 2017
Gender and drug use
Compared with drug use among men, overall drug use According to the Global Burden of Disease Study, men
remains low among women. At the global level, men suffer at least twice as much as women from drug use
are three times more likely than women to use can- disorders and therefore from the consequences of drug
nabis, cocaine or amphetamines. By contrast, women use, as expressed in DALYs. Between 2005 and 2015,
are more likely than men to misuse prescription drugs, DALYs attributed to drug use disorders increased by 24
particularly prescription opioids and tranquillizers.a, b This per cent,d which is attributed to an increase in expo-
mainly reflects differences in opportunities to use drugs sure to risk, i.e. an increase in the prevalence of drug
owing to the influence of social or cultural environments, use disorders, coupled with an increase in the popula-
rather than intrinsic gender vulnerability.c Women typi- tion. The relative increase in the prevalence of drug use
cally begin using substances later in life than men, but disorders (exposure to risk factors) was higher among
once they have initiated substance use, women tend to women than among men in this period.e Similarly, the
increase their rate of consumption of alcohol, cannabis, per cent increase in DALYs caused by drug use disor-
opioids and cocaine more rapidly than men and may ders, particularly opioid and cocaine use disorders, was
progress more quickly than men to the development of greater among women (25 per cent and 40 per cent,
drug use disorders. respectively) than among men (17 per cent and 26 per
cent, respectively).
"Healthy" years of life lost (DALYs) attributable to drug use disorders among men and
women, 2005 and 2015
14,000,000
12,000,000 Increase in DALYs as a result
of drug use disorders
10,000,000 Men: 19 per cent
DALYs
Women: 25 per cent
8,000,000
6,000,000
4,000,000
2,000,000
0
Drug Opioid Cocaine Amphetamine Cannabis Other drug
use use use use use use
disorders disorders disorders disorders disorders disorders
Women 2005 Women 2015 Men 2005 Men 2015
Source: Global Burden of Disease Data, Institute for Health Metrics and Evaluation.
a World Drug Report 2015 (United Nations publication, d Global Burden of Disease Study 2015 DALYs and HALE
Sales No. E.15.XI.6). Collaborators, “Global, regional, and national disability-
b Christine E. Grella, “From generic to gender-responsive adjusted life years (DALYs) for 315 diseases and injuries
and healthy life expectancy (HALE), 1990-2015: a sys-
treatment: changes in social policies, treatment services, tematic analysis for the Global Burden of Disease Study
and outcomes of women in substance abuse treatment”, 2015”, The Lancet, vol. 388, No. 10053 (2016), pp.
Journal of Psychoactive Drugs, vol. 40, SARC Suppl. No. 5 1603-1658.
(2008), pp. 327-343.
e Global Burden of Disease Study 2015 Risk Factors Col-
c Michelle L. Van Etten and James C. Anthony, “Male-
laborators, “Global, regional, and national comparative
female differences in transitions from first drug opportu- risk assessment of 79 behavioural, environmental and
nity to first use: searching for subgroup variation by age, occupational, and metabolic risks or clusters of risks,
race, region, and urban status”, Journal of Women Health 1990-2015: a systematic analysis for the Global Burden
and Gender Based Medicine, vol. 10, No. 8 (2001), pp. of Disease Study 2015”, The Lancet, vol. 388 (2016), pp.
797-804. 1659-1724.
16GLOBAL OVERVIEW OF DRUG DEMAND AND SUPPLY A. Extent of drug use
2
Fig. 4 Primary drug of concern among people in drug treatment, by region, 2015
80
People in treatment (percentage)
Hallucinogens
70 Tranquillizers and
sedatives
60
Amphetamines
50 Cocaine
40 Opioids
30 Cannabis
20
10
0
Africa North Latin Asia Eastern and Western Oceania
America America South-Eastern and Central
and the Europe Europe
Caribbean
Source: UNODC, responses to annual report questionnaire.
one-time online contact, or a brief intervention in treatment are still receiving treatment for opioid use
an outpatient setting, to a more comprehensive disorders. Cannabis is the main drug for which drug
treatment plan involving the treatment of other use treatment is sought in Africa, but many coun-
co-morbidities in an outpatient or inpatient setting.5, tries, most notably Mozambique, Nigeria, South
6, 7, 8 Africa and the United Republic of Tanzania, have
Opioids remain of major concern in South-West reported an increasing number of people entering
and Central Asia and in Eastern and South-Eastern treatment for opioid use disorders.
Europe. In South-Eastern Europe, nearly three out Information on the number of people in treatment
of every five people in drug treatment are in treat- for drug use disorders for the first time shows an
ment for opioid use disorders. Treatment for cocaine increasing trend in opioid use, including heroin, in
use remains prominent in North America, Latin North and South America, as well as in Eastern and
America and the Caribbean and, to a lesser extent, South-Eastern Europe, where nearly a third of
in Western and Central Europe, while ampheta- people in treatment for opioid use disorders were
mines remain a problem primarily in East and first-time entrants into treatment. Accounting for
South-East Asia and to some extent in North Amer- more than half of those treated, the proportion of
ica. The number of people in treatment for disorders people seeking treatment for cannabis use disorders
resulting from use of amphetamines has been for the first time remains high at the global level.
increasing in Asia, although half of people in
Although, overall, nearly one out of three people in
5 Wayne Hall, Maria Renström and Vladimir Poznyak, eds., treatment for the use of tranquillizers and sedatives
The Health and Social Effects of Nonmedical Cannabis Use is a woman, women account for only one out of five
(Geneva, WHO, 2016). people in treatment for drug use disorders. Younger
6 Jan Copeland, Amie Frewen and Kathryn Elkins, Manage- people are seeking treatment for disorders related
ment of Cannabis Use Disorder and Related Issues: A Clini- to the use of cannabis and amphetamines (with an
cian’s Guide (Sydney, National Cannabis Prevention and
average age of 24 and 25, respectively) more than
Information Centre, University of New South Wales, 2009).
7 Divya Ramesh and Margaret Haney, “Treatment of cannabis
for other substances, reflecting increasing use of can-
use disorders”, Textbook of Addiction Treatment: International nabis and amphetamines. Meanwhile, people in
Perspectives, vol. I, Nady El-Guebaly, Giuseppe Carrà and treatment for opioid- or cocaine-related disorders
Marc Galanter, eds. (Milan, Springer, 2015).
are typically in their 30s and, in many subregions,
8 Alan J. Budney and others, “Marijuana dependence and its
treatment”, Addiction Science and Clinical Practice, vol. 4, reflect an ageing cohort of users in treatment. It
No. 1 (2004), pp. 4-16. should be borne in mind, however, that between 40
17WORLD DRUG REPORT 2017
Fig. 5 Total number of people in treatment, by drug type and by region, 2015 or latest available
data
Latin America and the Carribean North America
35,000 600,000
11 countries 3 countries
30,000
500,000
25,000
400,000
20,000
15,000 300,000
10,000 200,000
5,000 100,000
0 0
Number of people in treatment
Western and Central Europe Eastern and South-Eastern Europe
300,000 90,000
25 countries 6 countries
250,000 80,000
70,000
200,000 60,000
150,000 50,000
40,000
100,000 30,000
50,000 20,000
0 10,000
0
Africa
25,000 Asia Africa
700,000 (18 countries) 25,000
20,000 29 countries 18 countries
600,000
15,000 20,000
500,000
400,000 15,000
10,000
300,000
5,000 10,000
200,000
0 100,000 5,000
0 0
Amphetamines
Cannabis
Opioids
Others
Cocaine
Cannabis
Opioids
Cocaine
Amphetamines
Tranquilizers
Cannabis
Opioids
Cocaine
Amphetamines
Tranquilizers
With prior treatment
First time in treatment
With prior treatment
Source: UNODC, responses to annual report questionnaire.
First time in treatment
Note: The figures are based on data for 2015 or the latest year since 2010. The number of people treated for different drugs in a region
is weighted by the total number of people treated in a country. Member States in Oceania (Australia and New Zealand) do not provide
information on the proportion of people in treatment for the first time, and therefore information for Oceania is not reflected in the
above figures.
per cent and 80 per cent of people reported in treat-
ment for drug use disorders are diagnosed with
polydrug use, reflecting the complexity of the drug
use phenomenon and the challenge of treating
people with drug use disorders effectively.
18GLOBAL OVERVIEW OF DRUG DEMAND AND SUPPLY B. Health impact of drug use
2
B. HEALTH IMPACT OF HIV and hepatitis markedly impact on
people who inject drugs
DRUG USE
PWID are a key population at increased risk of HIV
Almost 12 million people worldwide infection as a result of unsafe injecting practices
injected drugs in 2015 relating to the sharing of contaminated needles and
People who inject drugs (PWID) are among the syringes. The available data are sparse but suggest
most marginalized and disadvantaged drug users. that, globally, new HIV infections among PWID
They experience poor health outcomes with a greater climbed from an estimated 114,000 in 2011 to
chance of premature death, high rates of potentially 152,000 in 2015.13 The joint UNODC/WHO/
life-threatening infectious diseases, such as HIV, UNAIDS/World Bank estimate for the prevalence
hepatitis and tuberculosis, and increased risk of both of HIV among PWID in 2015 is 13.1 per cent. This
fatal and non-fatal drug overdoses.9, 10 The situation suggests that roughly one in eight people who
is often made worse by a lack of access to relevant injected drugs in 2015 were living with HIV, which
evidence-based prevention and treatment services equates to 1.55 million PWID infected with HIV
for drug dependence and infectious diseases.11, 12 worldwide. This estimate is based on the reporting
Infectious diseases acquired through the sharing of of HIV prevalence by 118 countries, covering 95
injection equipment for drug use further impact on per cent of estimated PWID.
those who do not inject or use drugs through other By far the highest prevalences of HIV among PWID
modes of transmission (for example, sexual). are found in South-West Asia (28.5 per cent) and
The joint UNODC/World Health Organization Eastern and South-Eastern Europe (24.0 per cent),
(WHO)/Joint United Nations Programme on HIV/ where rates are approximately twice the global aver-
AIDS (UNAIDS)/World Bank estimate for the age (13.1 per cent). Together, China, Pakistan, the
number of people worldwide who injected drugs in Russian Federation, Ukraine and the United States
2015 is 11.8 million (range: 8.6 to 17.4 million), are home to one in three adults worldwide. How-
corresponding to 0.25 per cent (range: 0.18 to 0.36 ever, the same five countries account for 68 per cent
per cent) of the population aged 15-64 years. This of PWID living with HIV. Despite the steady
estimate is based on the reporting of injecting drug decline observed in the numbers of PWID in drug
use from 107 countries, covering 89 per cent of the dependence treatment institutions (registered drug
global population aged 15-64 years. users) in the Russian Federation, the prevalence of
HIV among registered PWID rose steadily over the
Subregions where the prevalence of injecting drug period 2009-2014, from 13.2 per cent to 19.9 per
use is above the global average are Eastern and cent.14
South-Eastern Europe, Central Asia and Transcau-
casia, North America, Oceania and South-West Asia. Hepatitis C is an infectious disease affecting the
More than half (53 per cent) of PWID worldwide liver, which is responsible for considerable mortality
reside in just four countries (China, Pakistan, Rus- and morbidity among PWID. The burden of disease
sian Federation and United States). among PWID, including people with a past history
of injecting drug use (important because the health
consequences might not be seen for many decades
9 Bradley M. Mathers and others, “Mortality among people after initial infection), is far greater for hepatitis C
who inject drugs: a systematic review and meta-analysis”, than HIV infection. The number of deaths is more
Bulletin of the World Health Organization, vol. 91, No. 2
(2013), pp. 102-123. than 3.5 times higher for hepatitis C and the number
10 Louisa Degenhardt and others, “Global burden of disease of years of “healthy” life lost (as measured by DALYs)
attributable to illicit drug use and dependence: findings
from the Global Burden of Disease Study 2010”, The
Lancet, vol. 382, No. 9904 (2013), pp. 1564-1574. 13 UNAIDS, Get on the Fast-Track: The Life-cycle Approach to
11 Joint United Nations Programme on HIV/AIDS HIV (Geneva, 2016).
(UNAIDS), The GAP Report 2014 (Geneva, 2014). 14 Russian Federation, Ministry of Health, Main Indicators of
12 UNAIDS, Do No Harm: Health, Human Rights and People Substance Abuse Services in the Russian Federation in 2013-
Who Inject Drugs (Geneva, 2016). 2014: Statistical Yearbook (Moscow, 2016).
19WORLD DRUG REPORT 2017
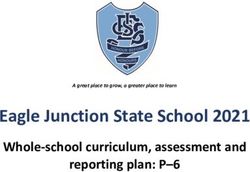
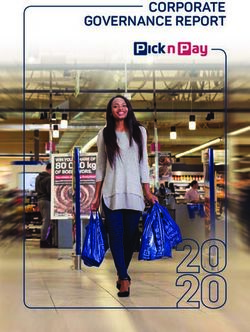
Fig. 6 Regional patterns in injecting drug use and HIV among people who inject drugs, 2015
(a) Prevalence of injecting drug use (b) Number of PWID and those among this group
living with HIV
Regional Subregional
Oceania
ESE
WC
Europe
WC ESE
S CAT ESE
Asia SW NME S
NME ESE SW CAT
5.0 million
Americas N LAC
LAC N
1.0
Africa 0.1
--- Global average
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4
Prevalence (percentage)
Source: Responses to the annual report questionnaire; progress reports of UNAIDS on the global AIDS response (various years);
the former Reference Group to the United Nations on HIV and Injecting Drug Use; published peer-reviewed articles and govern-
ment reports.
Notes: Unlabelled symbols are regional estimates. Subregions are denoted as follows: Europe — Western and Central (WC) and Eastern
and South-Eastern (ESE); Asia — Central Asia and Transcaucasia (CAT), East and South-East (ESE), South-West (SW), Near and Middle-East
(NME) and South (S); and the Americas — North America (N) and Latin America and the Caribbean (LAC). For Oceania, estimates are
based on data from Australia and New Zealand only.
Part (a): Percentage of population aged 15-64 years who inject drugs.
Part (b): Number of PWID (outer circle) and number of PWID living with HIV (inner circle).
is approximately 2.5 times higher. The vast majority is estimated at 7.4 per cent, suggesting that 880,000
of DALYs for both hepatitis C and HIV are the PWID are infected with the disease.
result of years of life lost as a result of premature
New, highly effective hepatitis C treatments (direct-
death.15 Hepatitis C is highly prevalent among
acting antivirals) have been shown to cure 90 to 95
PWID, with the joint UNODC/WHO/UNAIDS/
per cent of chronic hepatitis in 12 or 24 weeks. In
World Bank estimate of 51.5 per cent for 2015,
2015, WHO included direct-acting antivirals in its
suggesting that 6.1 million PWID are infected with
Model List of Essential Medicines18 and, in 2016,
hepatitis C. For PWID living with HIV, co-infection
launched the first global strategy on hepatitis.19
with hepatitis C is highly prevalent, at 82.4 per cent,
Despite the high burden of hepatitis C among
with hepatitis C among those living with HIV
PWID, treatment has occurred at very low levels,
becoming a major cause of morbidity and mortali-
which is related to the substantial barriers that exist
ty.16 The prevalence of hepatitis B17 among PWID
for PWID in accessing care.20 These include lack
15 Louisa Degenhardt and others, “Estimating the burden of of awareness, stigma and discrimination, limited
disease attributable to injecting drug use as a risk factor for access to hepatitis C testing and treatment and the
HIV, hepatitis C, and hepatitis B: findings from the Global cost of the medications. The median cost of a
Burden of Disease Study 2013”, The Lancet Infectious
Diseases, vol. 16, No. 12 (2016), pp. 1385-1398.
16 Lucy Platt and others, “Prevalence and burden of HCV 18 Model List of Essential Medicines: 19th List (Geneva, April
co-infection in people living with HIV: a global systematic 2015) (amended November 2015).
review and meta-analysis”, Lancet Infectious Diseases, vol. 16, 19 Global Health Sector Strategy on Viral Hepatitis 2016-2021:
No. 7 (2016), pp. 797-808. Towards ending viral hepatitis (Geneva, 2016).
17 The hepatitis B prevalence estimate is intended to refer to 20 Philip Bruggmann and Jason Grebely, “Prevention, treat-
active infection (HBsAg), rather than anti-HBc, which indi- ment and care of hepatitis C virus infection among people
cates previous exposure. However, it is not always possible who inject drugs”, International Journal of Drug Policy, vol.
to differentiate that in the data reported to UNODC. 26 (2015), pp. S22–S26.
20GLOBAL OVERVIEW OF DRUG DEMAND AND SUPPLY B. Health impact of drug use
2
Fig. 7 Comparison of burden of disease possible consequence of drug use. Ending the global
from hepatitis C and HIV attributable epidemic of tuberculosis is part of target 3.3. of the
to injecting drug use, including past Sustainable Development Goals and is the aim of
injecting, 2013 the WHO End Tuberculosis Strategy. However, evi-
300 9.0
Disability-adjusted life years (millions)
dence is required to understand how policy on drug
Number of deaths (thousands)
250 7.5 use can be an inclusive and integral part of the efforts
to achieve that goal. Tuberculosis is a potentially
200 6.0 life-threatening infectious disease that is spread from
150 4.5
person to person by breathing the same air as those
with active tuberculosis, particularly when they
Hepatitis C
Hepatitis C
100 3.0 cough, sneeze or spit. Despite being preventable and
curable in most cases, tuberculosis is one of the top
50 1.5
ten causes of death globally, and more people died
HIV
HIV
0 0.0 from tuberculosis in 2015 than from HIV/AIDS.
Deaths DALYs Tuberculosis is one of the leading causes of mortal-
ity among people who use drugs and are living with
Years of “healthy” life lost as a result of disability HIV.23 One of the high-risk groups for the spread
Years of life lost as a result of premature death of tuberculosis are people who use drugs. Based on
the limited data available from studies in Europe,
Source: Degenhardt and others, “Estimating the burden of Asia and the Americas,24 the prevalence of tuber-
disease attributable to injecting drug use as a risk factor for
HIV, hepatitis C, and hepatitis B.
culosis among PWID is estimated at approximately
Notes: DALYs comprise “healthy” years of life lost as a result of 8 per cent (median prevalence based on 23 studies)
both premature death and years lived with disability. with a range from 0.2 per cent to 66 per cent. The
prevalence of tuberculosis in the general population
12-week course of the medication (sofosbuvir) in at the global level is estimated at less than 0.2 per
26 OECD countries was $42,017, ranging from cent.25
$37,729 in Japan to $64,680 in the United States.21 People who use drugs are disproportionately affected
Only a few countries are taking steps towards uni- by risk factors for tuberculosis such as poor social
versal access to treatment for all people with chronic circumstances, infection with HIV and periods of
hepatitis C infections. Some examples where action incarceration. People who use drugs are often socio-
has been taken include Australia, which, since March economically disadvantaged and vulnerable to
2016, has offered universal access to hepatitis C poverty, homelessness and malnutrition. Infection
treatment and has identified prisoners and PWID with HIV is particularly serious because HIV dra-
as priority populations for the expansion of cover- matically increases the chance of latent tuberculosis
age of treatment. France has been providing universal infection progressing to active tuberculosis.26 Infec-
access to hepatitis C treatment under its national tion with HIV is a major reason for the high
health insurance system since September 2016. prevalence of tuberculosis among PWID.27 Without
Georgia and Morocco have launched hepatitis C
elimination programmes, and Portugal announced 23 WHO, Global Tuberculosis Report 2016 (Geneva, 2016).
universal access to hepatitis C treatment in 2015.22 24 Pippa Grenfell and others, “Tuberculosis, injecting drug use
and integrated HIV-TB care: A review of the literature”,
Drug use and tuberculosis Drug and Alcohol Dependence, vol. 129, No. 3 (2013), pp.
180-209, supplemented by responses to annual report ques-
In previous World Drug Reports, limited attention tionnaire.
had been devoted to tuberculosis, despite it being a 25 WHO, Global Tuberculosis Report 2015 (Geneva, 2015).
26 Helen McShane, “Co-infection with HIV and TB: double
trouble”, International Journal of STD and AIDS, vol. 16,
21 Swathi Iyengar and others, “Prices, costs, and affordability of No. 2 (2005), pp. 95-101.
new medicines for hepatitis C in 30 countries: an economic 27 European Centre for Disease Prevention and Control and
analysis”, Plos Medicine, vol. 13, No. 5 (2016), pp. 1-22. EMCDDA, Prevention and control of infectious diseases
22 WHO, Global Report on Access to Hepatitis C Treatment: among people who inject drugs. Joint publications series
Focus on Overcoming Barriers (Geneva, 2016). (Stockholm, ECDC, 2011).
21You can also read