Changing diabetes barometer - First report - changing diabetes
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

changing diabetes barometer First report changing diabetes

contents Foreword 4 Preface 5 Executive Summary 6 1. Time to work together 10 1.1 Diabetes – a story of missed opportunities 10 1.2 Meeting the challenge 11 1.3 The Changing Diabetes Barometer in context 12 2. Key Issues 14 2.1 Development of the Changing Diabetes Barometer concept 14 2.2 The economics of diabetes 14 2.3 Raising the capacity and competence of diabetes healthcare professionals 16 2.4 Expanding access to care 18 2.5 Improving self-management – assessing non-clinical indicators 20 2.6 Summary of key issues – improving quality of life for patients 22 3. The Changing Diabetes Barometer 24 3.1 What is the Changing Diabetes Barometer? 24 3.2 Inspiring and driving change 26 3.3 Organisation 28 3.4 The Changing Diabetes Barometer – the future 29 3.5 Countries included in the Changing Diabetes Barometer survey 30 2

Changing Diabetes at the national level
4. National examples of diabetes care 34
4.1 Learning from best practice 34
4.2 Case studies 35
4.3 Overview of case studies – what do they show us? 53
4.4 Novo Nordisk initiatives to improve control 54
4.5 Improving diabetes care in developing countries 55
5. Direct costs of diabetes 58
5.1 Controlling diabetes, controlling costs 58
5.2 Studying diabetes in the UK 58
5.3 Overview of the analysis 59
5.4 Economic costs of diabetes 63
5.5 Breaking even and moving into credit 64
5.6 Conclusion 66
6. Indirect costs of diabetes 68
6.1 What are the indirect costs? 68
6.2 The Danish example 69
6.3 Current study in Sweden 71
Appendix 72
References 74
3
foreword
It is my firm belief that we can beat diabetes. We all share the same and all people at risk of developing the disease in the future. As it mea
great goal – to reduce the impact of diabetes on individuals, families, sures the impact of diabetes care, it will provide essential information
communities and societies; to help the man, woman and child affected to support policy making and evaluation. It will communicate standards
by diabetes to live the very best life they can. Understanding the chal by which people will start measuring their actions to tackle and treat
lenge, and the effects of our efforts, is central to meeting the chal diabetes and, most importantly, inspire learning from others as efforts
lenge. Without measuring, we can’t improve anything. We need to set are compared with those in other countries and regions.
standards for ourselves, for patients, for nations and internationally to
improve our actions in the fight against this complex, chronic disease. Depending on where you live, diabetes care faces different pressures
This is what the Changing Diabetes Barometer does. and has different priorities. The priority may be improving quality of life
for people with diabetes, it may be cutting costs, or it may be increas
ing access to treatment. We need to understand these pressures but
also ensure that, whatever the local situation, we all constantly strive to
improve our response to diabetes.
The Changing Diabetes Barometer initiative is just a beginning but it
is my belief that it will constitute an important step following the UN
Resolution on diabetes, helping people and governments to respond
to the major challenge acknowledged by the UN. The response needs
leadership but also partnership. I look forward to continuing to support
the initiative, helping it to move forward and ensuring that it has a real
impact on diabetes care, and the lives of individuals everywhere.
By 2025 over 380 million people will live with diabetes. The challenge
presented by the diabetes pandemic is enormous. With the develo
ping world bearing the brunt of this burden, as well as a global health Jean-Claude Mbanya
problem, it is an international economic impediment and a barrier to Vice Dean and Professor of Medicine and Endocrinology,
development. University of Yaoundé, Member of Changing Diabetes Barometer
International Advisory Board
Concerted action from many players to promote healthier lifestyles is
vital to reduce the escalation of diabetes, and this must be combined
with provision around the world of the best care possible for people
already living with it.
The Changing Diabetes Barometer is an important new contribution to
ensuring that we do the very best we can for all people with diabetes,
4preface
As a global diabetes care leader, Novo Nordisk has much to offer as a is needed throughout the diabetes care path, from before a person is
partner in the fight against diabetes. We support many individual projects diagnosed, and even before they develop the disease, to spread best
around the world to combat diabetes, but our aim is larger. As a business practices and present the strongest challenge to diabetes.
and as a corporate citizen in a world heavily burdened by disease, we
want to change diabetes. We want to change the impact diabetes has Raising awareness of diabetes is, in itself, a challenge. The effects of this
on lives, change the amount of pain and suffering diabetes causes and devastating disease are complex and far reaching. All too often, how
change the burden of diabetes on economies around the world. ever, its impact is left to wreak havoc unnoticed. This lack of immediacy
has been mistranslated into a lack of urgency, and the lack of urgency
Change is essential if we are to break the curve of the pandemic of leads not only to the disease operating silently on the body, but also
diabetes. We believe in the critical role that innovation can play. This speaking too quietly in the world of health policy.
innovation is not limited to research into medicines. Instead, innovation
The importance of raising awareness of diabetes led Novo Nordisk to
be a strong partner in the Unite for Diabetes campaign which led to the
adoption of the 2006 UN Resolution on diabetes. Words are, however,
not enough. We need to continue to work together to put this resolu
tion into action.
In March 2007 we gathered a wide range of stakeholders, including
keynote speaker President Bill Clinton, to discuss how we can change
diabetes. At this forum we pledged to launch the Changing Diabetes
Barometer – a new tool to keep score of the fight against diabetes. If
we cannot measure diabetes then we cannot manage it. We need to be
able to compare interventions and outcomes, just as we do medicines,
to drive further innovation and ensure best practices are shared.
For too long the fight against diabetes has been conducted in the dark;
in many places spending great sums on care without knowing whether
the battle is being won or lost. Working with others on this initiative,
we intend to turn on the lights.
Lars Rebien Sørensen
CEO and President, Novo Nordisk A/S
5executive
summary
An innovative response to an urgent need The Changing Diabetes Barometer sets out to encourage just that. It
starts from very limited data and examples from several countries –
The Changing Diabetes Barometer is both a report and a concept: a India, Israel, Italy, Japan, Sweden and the USA, with accounts of further
framework for measuring progress in the fight against diabetes. The initiatives from a number of other countries and regions – and it is re
concept is both large and urgent – its aim is to inspire the change in stricted to published data. These countries’ experiences are analysed to
approach which is essential if there is to be any chance of bringing the develop an understanding of the potential for improved diabetes care,
diabetes pandemic under control. the difficulties that have been overcome, and the early indications of
success. After less than ten years’ experience, several of the countries
Diabetes is growing in its prevalence all over the world. The Interna already systematically collecting and analysing diabetes care data have
tional Diabetes Federation currently estimates that 246 million people been able to show significant improvements; not only in the supply of
worldwide have diabetes in 2007, which is almost 6% of the adult data, but in the medical outcomes reported. The Changing Diabetes
population. This number is expected to reach 380 million by 2025, or Barometer highlights their achievements and encourages other coun
7.3% of the adult population. Many of these people with diabetes will tries and regions to build their own data systems. More than that, it
develop serious medical complications, for which hospital treatment is encourages them to look at their data, find the weak points, learn from
costly. And as many as a third do not know that they have it so are not others and set about making the systems stronger.
taking any action or receiving any treatment.
The UN Resolution on diabetes, adopted on 20 December 2006,
The world has many excellent initiatives to provide care for people with focused public and political attention on diabetes in comparison with
diabetes, but only a minority are able to benefit from them fully. A the infectious diseases which had for so long been in the spotlight.
number of countries have recognised the scale of the pandemic and Only three months later, the Global Changing Diabetes Leadership
have put in place national strategies to address it, including steps to Forum, organised by Novo Nordisk with the support of the IDF, set out
train more healthcare professionals and improve access to medicines. to inspire participants from every aspect of diabetes care to make real
But only a few have documented the present level of diabetes care they improvements in their own countries. The Forum established that if a
can offer, or how effective that is in keeping this long-term condition situation is to be managed, we need to be able to measure it, and we
under control. need to know how well it is working. Out of this came the Changing
Diabetes Barometer.
An initial survey for this report reviewed the published data available
from 21 countries around the world. It suggested that, of the 21 coun
tries one third had no data on treatment indicators like mean blood Key objectives
glucose (HbA1c), blood pressure and lipid levels; one third did not have
data on incidence rates; and only a few had systems in place tracking The Changing Diabetes Barometer has three objectives; to
important key indicators in a dynamic registration database allowing • illustrate the link between quality of diabetes care, reduction in com
consistent follow up on a national scale. A major effort is needed to plications and socio-economic costs, thus providing all stakeholders
improve knowledge about progress in the fight against diabetes, where with the opportunity to make informed choices;
we are succeeding and where we are failing, and inform decision mak
ers at all levels where to look for inspiring examples of how they can
do better.
6• improve treatment through inspiring learning, based on measuring understood that investing in diabetes screening and more effective care
and comparing results as all stakeholders develop a clear picture of will, within a relatively short time, result in lower medical costs and less
the current quality of diabetes care in their country; and lost productivity. As populations’ age and diabetes incidence rises, it
• inspire others to follow best practice examples. is even more pressing to halt the loss of people’s skills and experience
from the working population.
At the international level, the Changing Diabetes Barometer aims to
inspire national stakeholders to measure the impact of their efforts and This First Changing Diabetes Barometer Report sets the foundation for
learn from international best practice examples. It will monitor progress this work with a computer simulation analysis of direct costs in one
across countries to encourage constructive competition, and in the fu country where the evidence is available: the UK (see Chapter 5). From
ture, create an international baseline on the prevention, progress and this it can be shown that better control of blood glucose can reduce life
treatment of diabetes. It will communicate this information and incour time healthcare costs by 13%. If early diagnosis is linked with enhanced
age dialogue between healthcare policy makers and payers. treatment then these costs are reduced by as much as 21%. This leads
to the finding that because of reduced spending on the complications
At the national level, the Changing Diabetes Barometer will stimulate of diabetes, up to 48% of the available funds used for enhanced treat
informed dialogue on the necessity of measuring the treatment pro ment of diabetes could be spent not on complications, but on improved
gress. Data resources will be developed on the results from countries care at an earlier stage of the disease. That would have enormous im
participating in the initiative. These will include the indicators of dia pact on maintaining and improving the patient’s quality of life.
betes prevention, progress and treatment, plus information on the ex
istence and scope of any national diabetes strategy. Comparing data The presence of sufficient numbers of adequately-trained healthcare
both between and within countries presents the idea of competition in professionals, and also of IT staff presents a challenge to data collection
healthcare, but one based on all stakeholders challenging themselves but also an opportunity for the Changing Diabetes Barometer initia
to do better within a culture of using measured results for learning and tive to be of assistance. Many Healthcare Ministries around the world
improving, rather than for penalising or rewarding. Based on the evi have supported initiatives to train more doctors, nurses and healthcare
dence, action plans and individual targets can be set locally to improve auxiliaries, particularly in identifying diabetes at an early stage, and in
diabetes care. It is hoped that as the Changing Diabetes Barometer treating it to limit development of complications. The Changing Diabe
initiative grows, and countries collect more and better data, it will also tes Barometer, presenting information based on data collected around
be possible to collect more qualitative information on issues relating to the world, will highlight the points of healthcare systems where the
the quality of life of the individual person with diabetes, as affected by need is greatest. Through encouraging efforts to make information
the care they receive (see Chapter 3). more readily available and comparable, the initiative will help build
competence through learning from others and the free exchange of
best practice examples.
Key issues
Many developing countries have very acute problems. These include
If it is to call for a higher quality of diabetes care, the Changing Dia lack of financial resources, availability of healthcare professionals, and
betes Barometer has to take full account of the many factors which availability of adequate and up-to-date training for them. Further chal
challenge diabetes care in different parts of the world. The economic lenges may include cultural attitudes, access to medicines and hospitals,
cost of diabetes is well documented, but still the message is not well and the sheer enormity of the size of populations and distances involving.
7Here, even though data on diabetes care may be even more limited, the opportunity is great to make a start in documenting what is done, so that steps can be taken to develop it. Other countries’ experiences can offer solutions, and there is no need to re-invent. Access to adequate care is, of course, also a challenge for the undiagnosed and poorly treated propor tions of the diabetes population in the developed world. Again, this needs to be measured, understood and successful ways to tackle the problems examined, shared and implemented. Finally, as effective self-management of diabetes is one of the keys to maintaining people with diabetes in greater comfort and better quality of life for more years, the elements influencing its success or oth erwise of this also need to be measured and tracked. The Changing Dia betes Barometer and it’s future use of DAWN-inspired surveys to gather information on unmet needs and ways to improve the procces of care can play a vital role. A call to action This is the first Changing Diabetes Barometer Report. It sets an agenda for change, addressed to everyone in the diabetes community. To make diabetes care more comprehensive and more effective, we first have to know what is already in place and we have to track how the fight against diabetes is progressing. But collecting data is not just an academic exercise. It must be studied and used, to learn from existing actions, encouraging constructive competition to build a better approach to diabetes care policy, clinical and personal decision making. The Changing Diabetes Barometer project is just beginning. Join it and together we will change diabetes. 8
9
1. time
to work
together
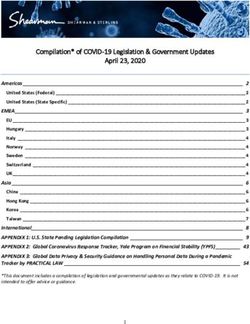
1.1 Diabetes – a story of missed opportunities Figure 1: The rule of halves
Diabetes is increasing at alarming rates worldwide, with devastating
effects on both the individual and society. The International Diabetes Among all
Federation (IDF) currently estimates that in 2007, 246 million people people with
diabetes
worldwide have diabetes1, representing 6% of the population aged
20-79. This number is expected to reach 380 million by 2025, or 7.3%
of the adult population. Many of these people with diabetes will develop
serious medical complications, for which costly hospital treatment can 50% are
only alleviate but never cure. diagnosed
only 6% would have
If 50% of them a succesful outcome
…a barrier between patients and their goal receive care …
… and 50% of those achieved
of ‘living normally’ treatment targets…
and 50% achived desired outcomes
The root of the problem of diabetes is our inability, throughout the
world, to offer truly adequate care. While many excellent healthcare The ‘rule of halves’ was developed in studies of hypertension2,3,4 and
professionals, care policies and treatments are available, the hard fact applies equally well to diabetes.
is that only a very small proportion of people with diabetes are able to
benefit fully from them. As a chronic disease, diabetes takes many years For diabetes, the rule of halves tells the story of missed opportunities
to run its course. During that time the availability of high quality treat along the care pathway and the diminishing effectiveness of current
ment, which is limited for a variety of reasons, means that many suffer a attempts to combat the disease. If, out of all people with diabetes, only
far worse quality of life than they could, facing a barrier between them 50% are diagnosed, many do not receive adequate care and many do
and their goal of ‘living normally’ and making their full contribution to not reach treatment targets, then only a tiny proportion manage to live
society. Earlier diagnosis could substantially reduce the proportion of well with their diabetes.
those whose diabetes has already caused other medical complications
by the time of diagnosis. A high proportion of people with diabetes are
not even diagnosed, so do not benefit from treatment at all and many
who are diagnosed fail to reach treatment targets.
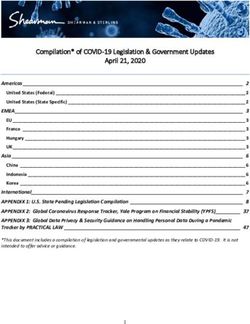
10Figure 2: Number of people with diabetes (PwD), worldwide, 2006 ...we are driving diabetes care in the dark
Because of the missed opportunities to keep people with diabetes liv
70 ing well for longer, society sustains massive losses, both through direct
60 costs to healthcare systems in treatment of the medical complications,
50 and through even greater indirect costs to national economies in terms
40
of lost productivity and social welfare. All this is in addition to the costs
to individuals and their supporters in terms of human suffering and loss
30
of earnings. The challenge is growing as the world’s population ages
20
and adopts less healthy lifestyles. It is particularly acute in developing
10
countries, which are estimated by the IDF to contain 300 million out of
0 a world total of 380 million people with diabetes by 2025.
Europe
North America
Latin America
Western Pacific
South East Asia
Sub-Saharan Africa
and North Africa
Middle East
Figure 3: World prevalence of diabetes and impaired glucose tole
rance*, 2007 and 2025 (ages 20-79)
Not diagnosed PwD (millions) 2007 2025
Diagnosed but not treated PwD (millions) Diabetes prevalence (%) 6.0 7.3
Treated PwD (millions) Number of people with diabetes (millions) 246 380
IGT prevalence (%) 7.5 8.0
Number of people with IGT (millions) 308 418
Source: IDF Diabetes Atlas 20061 and Novo Nordisk
*People with impaired glucose tolerance (IGT) have a significant risk of
In 2007 the actual proportions being diagnosed, receiving treatment, developing type 2 diabetes. Source: IDF Diabetes Atlas 20061
achieving targets and achieving desired outcomes in diabetes varies sig
nificantly between different parts of the world and different treatment
regimes. Calculating them is dependent on the level of confidence that 1.2 Meeting the challenge
is attached to the data at each stage. Published data from national
registers have the highest level of confidence, but in much of the world Diabetes care will not be improved significantly, especially in the face
data available is no more than anecdotal. Without reliable information of this growing pandemic, until a solid foundation of knowledge has
we do not know how we are progressing in the fight against diabetes, been built about the extent and effectiveness of care today. Only when
we are driving diabetes care in the dark. We need transparent measures outcomes are measured and compared can weaknesses in strategies,
to enable the weak points of the cycle of diabetes to be identified, treatment methods and care systems be diagnosed and improvements
prioritised and action taken – whether in prevention, diagnosis, or ef made. The achievements of countries or regions which have already
fective treatment. made a start can offer benchmarks to inspire change.
11…only when outcomes are measured and The UN Resolution was a major achievement for the IDF-led Unite for
compared can improvements be made Diabetes campaign, as for the first time, national governments had ac
knowledged the seriousness of the threat in comparison with infectious
The present collection of disparate national initiatives for data collec diseases like HIV/AIDS, which had for so long attracted more concern.
tion calls for a concerted approach to gather information and track
progress. The aim is, however, not solely to gather information; this Changing Diabetes is a global initiative of Novo Nordisk, dedicated to
is only the first step. Instead, an international consensus is needed on making a difference to people with diabetes – how it is treated, how it
how to develop measurable and comparable improvements through is viewed around the world, and how the future of this disease can be
out the whole cycle of diabetes care. Scrutinising and defining exactly controlled. As well as scientific and medical research, real change must
what data would best inform healthcare payers, and policy-makers, involve many participants and actions, through government, worldwide
decision-making will enable sound investment for the future. If national public health policy, healthcare professionals and industry.
initiatives can be encouraged, and results and best practices be shared
openly, it will make compelling information for decision-makers and A milestone Global Changing Diabetes Leadership Forum was organised
help bring diabetes out of the dark. People with diabetes would ex by Novo Nordisk with the support of the IDF in March 2007, just three
perience an improved quality of life, savings to the healthcare systems months after the adoption of the UN Resolution. It brought together
through avoidance of diabetes complications could be re-channelled almost 200 participants from politics, government, international organi
and the whole economy would benefit from a more productive work sations, patient organisations, healthcare, academia and the media. Its
force. objective was to spark a worldwide change, by inspiring all these dif
ferent participants in diabetes care to make real improvements in their
The Changing Diabetes Barometer initiative is a response to this urgent own countries.
and pressing need for concerted action.
As a result of the Leadership Forum, Novo Nordisk made a commitment
to publish annually a Changing Diabetes Barometer. The Changing
1.3 The Changing Diabetes Barometer Diabetes Barometer would gather information on global progress in
in context the fight against diabetes. It would also be a source of international
inspiration, as it would provide healthcare providers and policymak
Efforts to raise awareness of the serious potential of the diabetes pan ers with insight into the best practices which enable improvements in
demic are beginning to take effect. On 20 December 2006 the United diabetes care.
Nations (UN) General Assembly adopted a Resolution on diabetes which
called on all UN member states to take action, including developing
national policies for the prevention, treatment and care of diabetes in Starting point – scarce data
line with the sustainable development of their healthcare systems, and
taking into account the internationally agreed development goals. The Since the Forum, Novo Nordisk has collected information based on
Resolution was based on the recognition that diabetes, with its chronic available data on diabetes care from 21 countries, through its affiliates
nature and debilitating and costly complications, is a major threat to throughout the world. This survey suggested that, of the 21 countries
these goals, and that strengthening public health and healthcare delivery one third had no data on treatment indicators like HbA1c, blood pres
systems is critical to achieving them. sure and lipid levels one third did not have data on incidence rates and
12only a few had systems in place tracking important key indicators in a Novo Nordisk’s Commitment
dynamic registration database that enabled consistent follow-up on a
national scale. Reducing average HbA1c results in fewer severe cases and an increased
number of patients in good control. For example, reducing average
Working with others through the Changing Diabetes Barometer initiative, HbA1c from 7.5% to 7.0% by 2012 in Japan could result in 450,000
Novo Nordisk seeks to increase measuring, support learning and bring more patients in good control – saving up to 125,000 patient life years.
about improvements in diabetes care around the world. In the United States, where over 2.5 million people have HbA1c over
10%, reducing the average HbA1c of 11.8% to under 10% would save
Former Mexican Health Minister Dr Julio Frenk: up to 2 million patient life years by 2012.
“Ministers of Health need to tell Ministers of Finance that this is not just
a humanitarian issue… It’s a fundamental economic issue, since we will Novo Nordisk’s commitment to improving patient outcomes will
not grow our economies, we will not become competitive, we will not work through a three-part mechanism. First it will establish the facts
be able to participate in the global economy unless we have a healthy on not only the extent of diabetes worldwide – which is well known
workforce. This is much more than a public health crisis; it’s a security through the IDF and other sources – but also the extent, methods, ef
issue, because diabetes weakens the fabric of society.” ficiency and outcomes of diabetes healthcare interventions. Second, it
will communicate the information and encourage dialogue between
Professor Elizabeth Teisberg: healthcare policy-makers and payers. This will engage the support of
“The companies I have talked to have found that the cost of their em- healthcare providers and should also contribute to increased public
ployees“ poor health is 2.5 – 3 times higher than the direct cost of understanding and awareness. The third phase is to use the informa
health benefits. So not investing in quality care is a short-sighted view tion to stimulate and support national initiatives and projects which will
and will end up costing more.” improve diabetes care.
Professor Jean-Claude Mbanya:
“You can imagine how excited we are in the diabetes world to be part
of something that will meet the needs of our healthcare providers and
V E M
especially the patients. This Barometer is very timely because of the O
EA
IMPR
UN Resolution on diabetes passed in December 2006, which specifi-
SU R E
cally says that countries should develop national diabetes programmes
according to the level of their healthcare systems. If we can develop a
tool which countries can use to map their progress in developing and
implementing their programmes, that would be most welcome to the
E
national diabetes communities.” CO
MPAR
132. key
issues
2.1 Development of the Changing in life expectancy (average 18 years to 33 years) have been achieved
Diabetes Barometer concept in cystic fibrosis, when publication of results led to changes in care
practices1.
In September 2007, the Changing Diabetes Barometer Advisory Board
explored the key issues for the Changing Diabetes Barometer, including …publication of results led to changes
the challenges for the initiative and the opportunities it has and brings in care practices
to the diabetes community.
These suggestions lead to the idea of competition in healthcare, but this
The Advisory Board identified four main themes which intersect with must be constructive competition based on all stakeholders challenging
the Changing Diabetes Barometer initiative, and indeed with diabetes themselves to do better within a culture of using measured results for
care more broadly. These are: learning and improving, rather than for penalising or rewarding.
• Economics of diabetes care
• Capacity and competence of diabetes healthcare professionals Better diabetes care will generate an improved return on the invest
• Access to care ment constituted by spending on healthcare. Reliable, comparable re
• Empowering people with diabetes and improving self management. cording will provide the substance for analysis and drive learning, lead
ing to identification of the sections of the chain of care provision where
Central to the debate is the dual cost of diabetes – to the individual in improvements can be made. Improvement at these key points will then
terms of suffering, and to the economy in terms of the direct financial support primary prevention; support secondary prevention which re
costs of healthcare, social costs and the indirect losses to productivity. duces or delays complications, reduce hospital costs, reduce premature
The economics of care need to take full account of the value to the mortality, and release spending for other needs. The concept offers major
patient. Therefore, aiming to increase the value for patients means that advantages for everyone concerned – the payers and policy-makers, the
care delivery needs to be reorganised over the full cycle of care. Mak healthcare professionals, and most of all for the person with diabetes.
ing improvements throughout the cycle will contribute to improving
the quality of life of the person with diabetes – the equation between
a potentially long sentence of inconvenience, discomfort and pain, or 2.2 The economics of diabetes
a period of enjoyable and valuable life-years. This is after all the aim
of diabetes care, to ensure that people with diabetes live longer and The costs of diabetes are very significant to both the individual and to the
better-quality lives. wider economy, and they are growing. As a chronic, non-communicable
disease, diabetes places increasing burdens on both, in direct healthcare
Professor Elizabeth Teisberg: costs and the indirect costs of lost productivity, social care and financial
“The core issue in healthcare is improving the value of healthcare losses to the individual. Using new approaches to recording diabetes care
delivery – the value of health outcomes relative to the cost of achieving will contribute substantially to improving the care itself and reduce the
them.” costs, both financial and personal. The Changing Diabetes Barometer
will enable healthcare providers to benchmark their practices with those
Lessons can be learnt from other branches of medicine; for example, achieving better results, and help both payers and policy makers to opti
following publication of outcomes in coronary bypass surgery improve mise the use of resources and achieve better value.
ments mortality has been reduced by 41%; and spectacular increases
14…recording diabetes care will reduce the costs, Direct costs of healthcare
both financial and personal
In many countries healthcare spending has risen faster than the growth
in GDP per head of the population3 and is taking an increasing share
Diabetes prevalence is increasing rapidly in both developed and devel of governments’, employers’ and individuals’ budgets. Treatment and
oping countries; the IDF estimates a rise from 246 million people with strategies for prevention of diabetes worldwide in 2007 are estimated
diabetes worldwide in 2007 (6% of adults aged 20-79) to 380 million at US$ 232 billion; rising to US$ 302.5 billion by 20254. The grow
by 2025 (7.3%)2. The Western Pacific region has the highest number of ing prevalence of non-communicable diseases in relation to infectious
people with diabetes (67 million in 2007), while North America has the diseases means that the increasing call on governments’ healthcare
highest prevalence (9.2%). budgets may cause critical competition for finance within healthcare
and between that and other public services.
The ageing of populations in both the developed and developing world
is expected to result in increased prevalence of diabetes. Unless it is …the magnitude of expenditure should
matched by increased healthcare spending, ageing also increases the demand that progress be measured
development of the long-term complications of diabetes, with associat
ed high treatment costs. The other key factors for diabetes are by now While in low-income countries almost all diabetes expenditure goes
deeply entrenched – the trend towards Western-style processed diets toward drugs to lower blood glucose, in industrialised countries up to
and reduced physical exercise, which together contribute to overweight 75% of diabetes healthcare costs are spent on hospital treatment for
and obesity. These factors are involved even in developing countries, complications. The magnitude of expenditure and its variation should
where traditional lifestyles are receding as economic realities encourage demand that progress be measured and tracked, but this is currently
people to move from rural to urban areas in search of employment. not the case.
Industrialisation in the emerging economies of the world makes this
pattern likely to continue.
Indirect costs to productivity and to the individual
The social and economic consequences of diabetes take very different
forms in different parts of the world. The costs of professional treatment The medical and psychosocial effects of diabetes also give rise to costs
and care in the developed world can be estimated in market terms. But to society. Diabetes can involve sub-optimal performance of employees
in the developing world much of the cost is influenced by distorted prices at work, time off work through illness or treatment requirements, pre
in the health care sector, the fact that people cannot afford treatment mature retirement through disability and premature death. Its cost to
and care and therefore do not get it, and that a very large part of the national productivity depends on the state of evolution of the economy
economy takes place in the informal sector (unregistered economic activ and the size of the population of working age, as can be seen from
ity, bartering, subsistence farming, and home production of food and the example of five countries with differing characteristics. Comparing
services). The reason for taking this into consideration is that diabetes China and India, for example, very similar productivity losses in absolute
hits people at the very core of their ability to generate economic means terms have a much greater impact in India in relation to GDP.
to sustain their living standard.
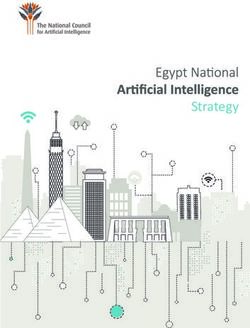
15Figure 4: Effect of diabetes on productivity in five countries Much evidence has amassed in the last 20 years7 that effective control
of blood glucose, coupled with control of blood pressure, prevents or
2007 China Denmark India UK USA reduces complications. New studies discussed in Chapter 5 of this report
Productivity loss, US $bn 20.5 1.3 20.4 3.3 41.4 are now demonstrating the potential gains in terms of life expectancy
Productivity loss, %GDP 0.6 0.4 1.9 0.1 0.3 and delayed development of the diabetes related complications which
can follow earlier diagnosis of diabetes and intensive control of blood
Source: Economist Intelligence Unit 5
glucose. The studies show the balance which can be achieved between
investment in more effective care at an early stage of diabetes, and
Diabetes also causes substantial indirect costs, which are widely agreed the return on that investment. The return is not only a vastly improved
to exceed by far those of healthcare provision. People with diabetes quality of life for the person with diabetes, for a longer time, but also
suffers lost earnings if they have to give up work; and also face the significant cost savings in both the direct and indirect costs outlined
prospect of a reduced pension. Their care may be provided by public- above, because of prevented or delayed incidence of complications.
sector services, or by family members, who may also incur loss of earn
ings to provide care. Professor Ashok Kumar Das:
“Treating diabetes appropriately is cheap, and not treating it is costly.”
…indirect costs far exceed those of
healthcare provision
2.3 R
aising the capacity and competence of
At this personal level, most industrialised countries have organised diabetes healthcare professionals
medical insurance schemes and/or government-supported healthcare
services, so financial strain is not added to the physical suffering caused The current capacity and competence of diabetes healthcare profes
by diabetes. But in many developing countries, people with diabetes sionals presents both a challenge and an opportunity to this initiative. In
are obliged to pay for their own medical treatment costs. For example, order for Changing Diabetes Barometer recording systems to document
up to 25% of household income in India is required to cover these the performance of diabetes care and to improve it, one of the main
costs, and 30% of poor households in China attributed their poverty concerns is ensuring the presence of sufficient numbers of adequately-
to healthcare costs6. trained healthcare professionals.
Numbers of doctors and nurses are far from adequate in many develop
Redressing the economic balance ing countries. In contrast, in developed regions, some of the case stud
ies in Chapter 4 show that some doctors have been initially resistant
Attention is focusing on how to contain the pattern of spiralling costs to change, and suspicious of collecting data which might be used to
and increasing suffering. The Changing Diabetes Barometer initiative criticise their performance.
to consolidate present efforts and improve recording of diabetes care
worldwide will clearly contribute. It will identify weak points in the Ensuring adequate numbers of healthcare professionals is an issue to
chain of primary prevention of diabetes ➤ diagnosis ➤ treatment of be addressed by national Finance and Health Ministries. In the specific
diabetes and prevention of complications ➤ treatment of complications context of diabetes, a number of initiatives are already under way, e.g.
so that steps can be taken to improve them. programmes to train doctors, nurses and healthcare auxiliaries in India
16and to provide extra diabetes expertise in Sweden (see Chapter 4). The The data system should encourage active participation on the basis that
Changing Diabetes Barometer initiative and the other efforts of the it will offer doctors improved insight into what is working well, and
international diabetes community, particularly of the IDF and its activi not so well, in their own procedures. Anonymity in data reporting will
ties related to World Diabetes Day and the UN Resolution, will help by probably be needed, at least initially - those setting up data registers
drawing the attention of the world’s governments to the diabetes pan will need to evaluate the national conditions to decide whether or not
demic and the need for the medical resources to curb it. it is essential, or possibly whether individual reporting centres can be
identified after a time lag.
…the Changing Diabetes Barometer will offer and
share solutions as well as raising awareness Dr Julio Frenk:
of problems “One challenge we shouldn’t minimize is the danger of data providers
feeling exploited, and the other is the failure to use the data.”
The medical profession will naturally ask for justification for collect
ing and sharing diabetes treatment data. The Changing Diabetes It is important, too, that the data they supply should show not just that
Barometer initiative must show that taking part will create benefits a measurement has been made, but its results. For example, the UK
rather than burdens. It must be explained and guaranteed that sharing Quality and Outcomes Framework (QOF8) requires measurement not
the results of their healthcare interventions is not intended to trigger only of the proportion of patients having HbA1c measured in the last
judgement. Instead it is intended as a source of reference, to show the 15 months, but of the proportion achieving HbA1c less than 7.5%.
achievements of other sister organisations / hospitals / primary care cen Only if outcomes are shown can others know what can be achieved.
tres against which each doctor or care centre can benchmark their own
achievement. The Changing Diabetes Barometer will offer and share There is evidence from countries which already have a national dia
solutions as well as raising awareness of problems, building on the ex betes register that doctors become keen to adopt the best practices
perience of those who have already met problems in their own national of their colleagues and compete actively to raise the standard of their
data systems and overcome them. own performance. This very genuine commitment among the medical
profession to deliver the best care possible for their patients, and their
In setting up these systems, the organisations which have already gone desire to address challenges of capacity either relating to number of
through the process are adamant that data collection should not in healthcare professionals or their knowledge, suggests potential for a
crease the workload of healthcare professionals, and that it should be powerful partnership with this initiative.
gathered in the process of normal routine consultations. Contributing
medical staff should be encouraged to analyse their own data and act …practitioners and patients will be able
on it, and not merely to supply it into a storage file. to drive up their own standards
Professor Soffia Gudbjörnsdottir: Through benchmarking, best practice sharing and open exchange
“The challenge is not so much to get the data collected, but to get the of knowledge and results, practitioners and patients will be able to
healthcare professionals to learn to look at their own data regularly, drive up their own standards. With the Changing Diabetes Barometer
and check its quality. This is a way to drive the process. We have re- providing an accepted framework for dialogue on diabetes care all
corded data for ten years but just doing that does not help.” stakeholders will be able to engage in debate about how to allocate
resources and prioritise attention.
17Information Technology 2.4 Expanding access to care
Barriers which could limit development of the Changing Diabetes Ba Special problems of developing countries
rometer is inadequacy of IT systems and suitably trained personnel to
support databases (particularly limited in some developing countries), Treatment of diabetes and its assessment in developing countries
and securing funding for data collection – again a case of early invest presents major problems: of financial resources, availability of health
ment bringing promise of a later return. Investment is also needed in care professionals and the infrastructure to support them, availability of
mechanisms to ensure data validity to remove any suggestion that it adequate and up-to-date training for them. Efforts may be challenged
could be manipulated. Where no IT systems were operating before the by cultural attitudes and resistance to change, face restricted access to
register, this can be taken as a great opportunity to set up systems using medicines and hospitals, and struggle with the sheer enormity of the
standardised file formats and software. The availability of information size of populations and distances involving unreliable supply chains. A
through technology including computing capacity, internet and mobile large majority of people in developing countries are forced to pay them
phones can now be used to increase greatly the empowerment of peo selves for some or all of their medicines, or simply not to have them.
ple with diabetes, and support the efforts of healthcare professionals,
especially in relation to monitoring self-management and compliance. For many years attention to helping developing countries has been
focused on controlling infectious diseases like HIV-AIDS, malaria and
Dr Jonathan Betz Brown: tuberculosis. Yet the growth of chronic diseases already imposes sub
“Some of the things we identify as barriers are actually opportunities. stantial costs and the World Bank estimates that they will become the
The fact that in most countries no outcome data and process data has leading cause of death in low-income countries by 20159. Rising life
been gathered, is a huge opportunity to do it in a standardised way expectancy for all age groups, lower fertility rates, better control of
so that there can be comparisons. ….The power of data to change infectious diseases, and changing lifestyles with more smoking, bad
behaviour seems partly related to whether an incentive is involved, but diet and lack of exercise, all indicate that non-communicable diseases
sometimes the data themselves are so embarrassing that they create will become a major problem to developing countries. Health systems
their own incentive.” will need to be adapted to cope with the growing numbers of elderly
people who will require long-term care alongside the present focus on
While it can be very hard for countries with no data to begin the process, addressing acute infectious diseases. About three-quarters of the dis
experience from Italy (see Chapter 4) has shown that data collection ability burden related to non-communicable diseases, including diabe
can in time win the support of healthcare policy-makers, for developing tes, in low- and middle-income countries occurs among those between
a culture of constructive competition and patient empowerment which the ages of 15 and 69, at the peak of their economic productivity.
will combine to improve patient care and eventually reduce costs.
Chronic illness in developing countries often forces families to finance
Professor Elizabeth Teisberg: treatment themselves, or to take family members out of employment
“Measuring and analysing outcomes does pay for itself, in time – we or school to care for relatives. The World Bank estimates that the di
can’t afford not to do it. Improvements in healthcare will drive down rect costs of diabetes are between 2.5 to 15.0% of annual health care
specific costs.” budgets, depending on local prevalence and the sophistication of
available treatments. Among low- and middle-income countries, total
diabetes-related costs are highest in Latin America and the Caribbean,
18where the economic burden of diabetes has been estimated at US$ 65 At a political level, the World Diabetes Foundation has also supported
billion annually. many initiatives to raise awareness of diabetes and its burden among
policy-makers and the healthcare community in developing countries –
The limited resources for diabetes care allocated by Health Ministries in including support for countries developing diabetes practice guidelines,
many developing countries has also led to limitations on glucose self- e.g. in sub-Saharan Africa, and mobilisation of multiple support for the
monitoring, which is advocated by current good practice guidelines. In UN Resolution on Diabetes.
many countries glucose meters and glucose testing strips are unavail
able or restricted to people on at least twice-daily insulin; urine test The relevance of the Changing Diabetes Barometer to these massive
ing strips are an alternative which could be made much more widely practical, financial and political problems in developing countries is two
available10. fold. At an international level it will be a powerful argument to convince
governments and policymakers of the vital urgency of confronting the
One of the major courses of action to improve this situation is to pro growing impact of diabetes. At a national level the initiative will present
vide education and other initiatives to promote lifestyle changes, in par practical counsel on how to build better care. Obviously not all the experi
ticular aimed at improving diet and exercise, and offered in a range of ences will be relevant or appropriate to all, but within the Changing Dia
settings e.g. in the community, workplaces and schools. A key opportu betes Barometer are best practices and ways to achieve improvements,
nity exists to screen people for diabetes and other non-communicable which can be selected to help in a wide variety of other countries.
diseases during normal medical checkups, and to provide appropriate
treatment at as early a stage as possible. The underlying, major ini
tiative to underpin these efforts is to encourage and achieve higher Early diagnosis, screening and prevention
incomes through economic growth. The Changing Diabetes Barometer
can contribute to these actions by measuring the scale of the problem, Access to appropriate care is, of course, also a major issue in the de
particularly in relation to identifying people with undiagnosed diabetes, veloped world for those who are at risk but unaware, undiagnosed, or
and those in need of secondary prevention steps to reduce the onset receiving inadequate treatment. The initial format for the Changing Dia
of complications. betes Barometer will include measures of BMI (as an indicator of preven
tion efforts), diabetes prevalence and average HbA1c (an indicator of the
Many relevant practical initiatives have been put in place under the Novo quality of diabetes treatment). These three first indicators are meant to be
Nordisk World Partnership Project to address the individual problems of a starting point for collection of data on the whole course of diabetes.
developing countries, using partnerships with concerned people and
organisations at the local level. These projects commonly faced an initial Against the background of the increasing prevalence of diabetes, and
lack of support and political will from governments towards diabetes its slow progression, attention has to be focused on the possibilities
prevention, and many countries had no national diabetes programme . 11
to intervene and delay or halt development of subsequent stages. In
Healthcare provision was often ineffective due to lack of equipment, particular, early diagnosis has been shown to reduce the development
facilities and infrastructure. The initiatives included a distance learning of the complications of diabetes. Primary prevention actions taken with
programme for doctors in Bangladesh, strengthening diabetes clinics people showing impaired glucose tolerance (IGT) can reduce or prevent
in Tanzania and training in insulin management for primary care physi its progression into diabetes. Intensive treatment after diagnosis can
cians in Malaysia. reduce or delay the appearance of complications – this is secondary
prevention. All of these possible interventions are clearly beneficial to
19overall quality of life for the individual12. Effective medical intervention 2.5 Improving self-management – assessing
is therefore essential in order to slow down or halt progression of the non-clinical indicators
disease at each of these stages.
Effective diabetes care requires a partnership between the healthcare
Eventually the Changing Diabetes Barometer should attempt to assess professional team and the person with diabetes. This involves offering
the important area of the undiagnosed and the population at risk of education to the patient so they can fully understand their disease, and
diabetes more fully, as well as those already being treated. the impact of their actions upon it; providing appropriate and timely
information; and shaping the encounter between doctor and patient
It is not considered economically feasible to screen whole populations so the patient is involved and empowered to take control of their dia
for signs of diabetes or IGT, but opportunistic screening targeted at betes, rather than allowing it to control them. The Changing Diabetes
those sections of the population which are likely to be at risk can be Barometer needs to develop ways to measure and communicate best
highly effective. practice on effective self-management and the provision of psychoso
cial support for people with diabetes.
Diabetes development can often be halted by simple lifestyle changes
and in particular control of overweight and obesity by diet, increased
physical activity, by drug treatment or a combination of these meth Patient self-management support
ods. However simply distributing information on healthy lifestyles is and the DAWN initiative
inadequate to change behaviour effectively unless other components in
society promote an active lifestyle and healthy eating. Less than half of the people with diabetes reach an optimal level of
health and quality of life despite availability of effective medicines.
The IDF has developed a large-scale population approach to the preven Based on a 2001 study of more than 5,000 people with diabetes and
tion of Type 2 diabetes, aiming to result in important health changes 3,000 diabetes healthcare professionals in 13 countries, the DAWN
for a large percentage of the population. Some countries have begun programme established new knowledge about the real-life barriers to
to develop and implement a national diabetes prevention plan in order optimal self-management. It also studied ways to address the deficits
to do just this and involve many groups including schools, religious and in the access to psychosocial support from the healthcare system and
ethnic communities, industry (marketing, investment policy, product community17. Successive international DAWN summits involving all key
development) and the workplace (health promotion within the work stakeholders in diabetes led to the DAWN Call to Action18, which is
ing environment). The first of these was Finland, whose Development used as a foundation for advancement of team-based patient-centred
Programme for the Prevention and Care of Diabetes in Finland 2000– self-management supportive diabetes care and more recently to a focus
201013 includes a population strategy aimed at promoting the health of on large-scale implementation initiatives.
the entire nation; an individualised strategy for those at high risk; and a
strategy of early diagnosis and management for those with new-onset Key to the process is increased education and information for people
Type 2 diabetes. It builds on the 58% reduction in the incidence of with diabetes, including the encouragement of ‘expert patients’ who
diabetes through dietary and exercise advices achieved in the Finnish can pass on their knowledge to others with diabetes, to healthcare
diabetes prevention study – where patients who met 80% of their diet, providers and the community in general – creating more general aware
exercise and weight loss goals did not develop diabetes14. ness and understanding. Many DAWN initiatives have explored the
most effective options in providing information for people with dia
20betes, including use of language-independent illustrations, IT systems Surveys
and computer software supporting the use of DAWN questionnaires in
everyday diabetes care. Surveys and questionnaires, as exemplified by DAWN surveys, can be
used to gather information from individuals on ‘non-clinical’ issues like
Psychosocial support is also vital to help people take on the task of man access to medicines and quality of self care. The Changing Diabetes
aging their long-term illness. The DAWN MIND translational research Barometer should consider the use of surveys to supplement hard bio
programme (Monitoring Individual Needs of people with Diabetes) is chemical data – especially to provide information on issues such as ac
working through 12 leading diabetes centres around the world to help cess to medicines, lifestyle, quality of life, and quality of self care.
support people with diabetes and their carers to cope with the psycho
logical issues that arise in developing individual care plans, and encour Dr Jonathan Betz Brown:
ages personal participation in the decision-making involved. Coaching “Most of those countries are quite poor, so survey methods are quite
in self-management is a critical area which can be taught both to medi inexpensive. Surveys give you control over how the indicators are de-
cal students and to expert patients. The original DAWN study of 2001 fined, how the data are gathered and how the population is defined.”
showed that many patients experience emotional stress related to their
diabetes, and that more than half of healthcare providers do not feel Access to insulin has been studied by IDF in three separate surveys since
equipped to adequately identify these issues in their practice17. 199219; which found very wide variation in its availability worldwide,
and also in the availability of blood glucose test strips. Urine testing
Experience from DAWN on the results of national surveys of patients’ strips are more available, but their use seems to be decreasing without
wishes and needs have been considered in the development of many a corresponding rise in blood testing strips, which suggests that increas
large scale diabetes care initiatives, e.g. Poland, Germany, Denmark, ing numbers may not be testing at all. The 1997 survey had shown that
Taiwan, Italy, Mexico, Colombia, Argentina, Greece, Japan, the insulin, syringes and needles were often not available because of price
Netherlands, Russia, Ukraine and the USA. The original surveys are be and transportation problems. Only 48 out of 120 countries surveyed
ing followed by expert analysis of how far the national healthcare sys could give access to insulin at all times to those who needed it. Access
tems are taking account of patients’ experiences and concerns. In Italy, to insulin was worst in Africa and best in Europe.
supervised by the Ministry of Health, national DAWN surveys in adults,
young people and migrating populations are providing the foundation Dr Julio Frenk:
for the national diabetes strategy. “There is a great value in international comparison, especially given the
huge differences we are going to find around the world, especially in
The DAWN programme 15
(Diabetes Attitudes, Wishes and Needs) prevalence and incidence. We can also find some overall indicators of
aims to improve patient outcomes by understanding patients the performance of the healthcare system, and apart from the actual
as individuals. DAWN was launched by Novo Nordisk in 2001 in outcomes, things like whether they’ve had blood pressure measured
partnership with the IDF and an international advisory panel16. As tells a lot about access to the healthcare system.”
it has already established worldwide the advisability of including
considerations of diabetes patients’ experiences and needs in na-
tional programmes for diabetes care, it is only natural to draw on
the knowledge acquired by the DAWN programme in developing
the Changing Diabetes Barometer.
21You can also read