Prediction of Coronary Artery Aneurysms in Children With Kawasaki Disease Before Starting Initial Treatment
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ORIGINAL RESEARCH
published: 30 September 2021
doi: 10.3389/fped.2021.748467
Prediction of Coronary Artery
Aneurysms in Children With
Kawasaki Disease Before Starting
Initial Treatment
Ching-Ying Huang 1,2,3*, Nan-Chang Chiu 1,2,3,4 , Fu-Yuan Huang 1,2 , Yen-Chun Chao 1,2 and
Hsin Chi 1,2,3,4*
1
Department of Pediatrics, MacKay Children’s Hospital, Taipei City, Taiwan, 2 Department of Pediatrics, MacKay Memorial
Hospital, Taipei City, Taiwan, 3 Department of Medicine, MacKay Medical College, New Taipei City, Taiwan, 4 MacKay Junior
College of Medicine, Nursing and Management, Taipei City, Taiwan
Background: Precisely predicting coronary artery aneurysms (CAAs) remains a clinical
challenge. We aimed to investigate whether coronary dimensions adjusted for body
Edited by: surface area (Z scores) on baseline echocardiography and clinical variables before
Ozgur Kasapcopur, primary treatment could predict the presence of late CAAs.
Istanbul University-Cerrahpasa, Turkey
Methods: We conducted a retrospective study including children hospitalized for
Reviewed by:
Amra Adrovic, Kawasaki disease and received intravenous immunoglobulin within 10 days of illness.
Istanbul University-Cerrahpasa, Turkey We defined late CAAs as a maximum Z score (Zmax) ≥2.5 of the left main, right, or left
Mikhail Kostik,
Saint Petersburg State Pediatric
anterior descending coronary artery at 11–60 days of illness. Associations between late
Medical University, Russia CAAs and clinical parameters and baseline maximum Z scores were analyzed.
Ovgu Kul Cinar,
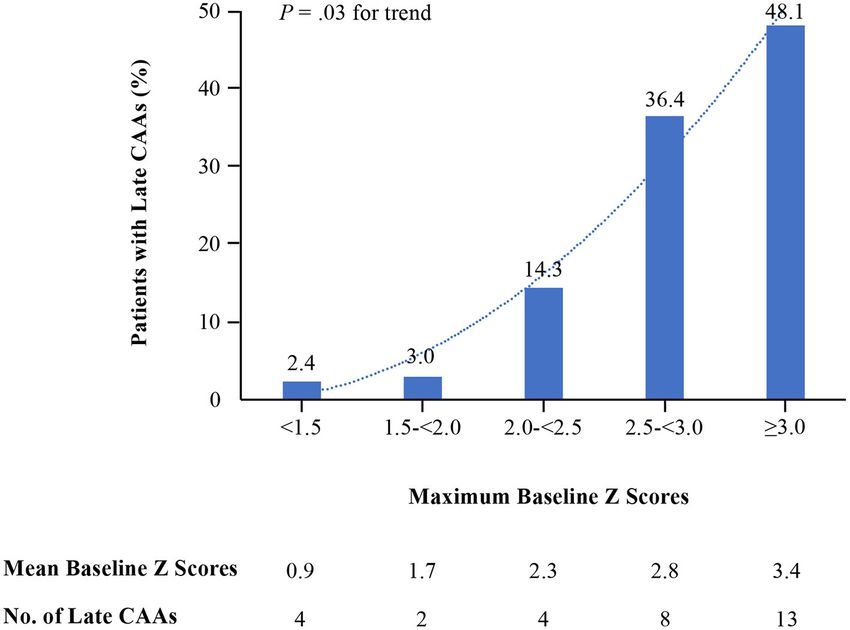
Great Ormond Street Hospital for Results: Among the 314 included children, 31 (9.9%) had late CAAs. Male, higher
Children NHS Foundation Trust, C-reactive protein, and higher baseline Zmax were risk factors of late CAAs. Late CAAs
United Kingdom
were significantly associated with baseline Zmax ≥2.0 vs.Huang et al. Coronary Z-Score and Kawasaki Disease shown to reduce the risk of coronary artery formation; the first IVIG infusion. Coronary artery internal diameters in nonetheless, despite the intervention, CAAs still occur in 2 to the left main coronary artery (LMCA), left anterior descending 6% of patients in the subacute and convalescent stages (8–10). artery (LAD), and right coronary artery (RCA) obtained by Adjuvant anti-inflammatory therapy, administered together with echocardiography were converted to Z scores using a model primary standard IVIG treatment in the acute stage, has been derived from body surface area-adjusted Z scores based on data shown to reduce the progression of coronary dilation (11, 12). from healthy Taiwanese children (25). Z scores were calculated at However, the time window in which to diagnose and treat KD baseline and for studies obtained 11–60 days after illness onset. with intensification is brief, as the primary therapy should be The maximum Z score (Zmax) was defined as the largest Z started within the first 10 days of illness to prevent long-term score of the LMCA, LAD, or RCA on echocardiography. Patients complications (13, 14). Therefore, a reliable method of promptly were defined as having late CAAs if they had a Z score ≥2.5 identifying children at a high risk of later CAAs is needed to tailor in the LMCA, LAD, or RCA at 11–60 days after illness onset. treatment (15). Small, medium, and giant (or large) aneurysms were classified Risk factors for CAAs include male sex (16), IVIG treatment according to 2017 American Heart Association guidelines as Z beyond 10 days of symptom onset (16, 17), increased C-reactive scores of ≥2.5 to
Huang et al. Coronary Z-Score and Kawasaki Disease
TABLE 1 | Comparisons between patients with and without coronary artery aneurysms at 11 to 60 days of illness.
Case No. With CAAs (N = 31) Without CAAs (N = 283) Univariate analysis
OR (95%) P
Age at illness 314 1.01 (0.98–1.03) 0.66
onset in months
Mean (SD) 22.1 (16.4) 16.9 (8.0–33.2)
Median (IQR) 20.8 (15.8) 17.4 (9.9–26.9)
5 Year 0 (0) 8 (2.8) — —
Male sex 314 25 (80.6) 153 (54.1) 3.54 (1.41–8.89) 0.007
Incomplete KD 314 7 (22.6) 32 (11.3) 2.29 (0.91–5.73) 0.08
WBC, x109 cells/L 313 1.0 (1.0–1.0) 0.61
Mean (SD) 15.1 (5.7) 14.5 (5.8)
Median (IQR) 13.8 (10.8–17.7) 13.8 (10.7–17.7)
% Neutrophile 314 1.02 (0.99–1.05) 0.11
Mean (SD) 64.2 (12.0) 59.9 (14.4)
Median (IQR) 61.0 (56.0–74.0) 61.5 (50.5-70.4)
Hemoglobin, g/dL 311 0.93 (0.66–1.31) 0.66
Mean (SD) 10.9 (1.1) 11.1 (1.0)
Median (IQR) 11.0 (10.4–12.0) 11.1 (10.4–11.8)
Platelet count, 310 1.0 (.99–1.0) 0.47
x109 /L
Mean (SD) 355.1 (108) 328.8 (118.1)
Median (IQR) 329 (275.3–422) 326.5 (274–386.7)
CRP, mg/dL 257 1.06 (1.0–1.12) 0.04
Mean (SD) 11.1 (6.6) 8.3 (6.4)
Median (IQR) 8.9 (6.4–15.1) 6.5 (3.6–11.4)
Sodium, mmol/L 190 0.98 (0.83–1.14) 0.75
Mean (SD) 135.2 (3.8) 135.5 (2.9)
Median (IQR) 135.0 (132.5–139) 135.5 (134–137)
Albumin, g/dL 214 0.48 (0.21–1.12) 0.09
Mean (SD) 3.7 (0.5) 3.9 (0.5)
Median (IQR) 3.8 (3.4–4.1) 4.0 (3.6–4.3)
AST, IU/L 276 1.0 (0.99–1.0) 0.83
Mean (SD) 84 (99) 79 (119)
Median (IQR) 44 (31–83) 42 (29–73)
ALT, IU/L 276 1.0 (0.99–1.0) 0.90
Mean (SD) 82 (95) 84 (99)
Median (IQR) 36 (15–124) 34 (19–104)
Maximum Z score 314 5.51 (3.26–9.31)Huang et al. Coronary Z-Score and Kawasaki Disease
and 3 (1%) received a combination of a second dose of IVIG TABLE 2 | Maximum Z score ≥2.0 on baseline echocardiography as a predictor
and corticosteroids. of late coronary artery aneurysms at 11 to 60 days of illness.
Overall, 31 patients (9.9%) had the presence of CAAs at Measure Value (95% CI) P
11–60 days of illness. Patients with or without the presence
of late CAAs had no differences in days from illness onset Sensitivity 0.81 (0.63–0.91)
to IVIG treatment (median [IQR]: 6 (5–8) vs. 6 (5–7), P = Specificity 0.82 (0.76–0.85)
0.24) and doses (mg/kg/day) of acetylsalicylic acid administration Positive predictive value 0.32 (0.23–0.44)
(median [IQR]: 57.1 [44.4–80.9] vs. 50.7 [37.6–80.0], P = 0.17), Negative predictive value 0.97 (0.95–0.99)
proportions of combination primary therapy (0 vs. 1.8%, P = False positive rate 0.18 (0.14–0.23)
1.0), and days of baseline echocardiograms (median [IQR]: 6 Accuracy 0.82 (0.77–0.86)
(5–8) vs. 6 (5–7), P = 0.74). The median time from the initial Positive likelihood ratio 4.39 (3.25–5.92)
treatment to second/third echocardiography was 15 (IQR: 11–22) Negative likelihood ratio 0.24 (0.12–0.49)
days/50 (IQR: 42–80) days. AUC of ROC 0.86 (0.78–0.98)Huang et al. Coronary Z-Score and Kawasaki Disease FIGURE 1 | Baseline maximum Z scores and rates of late coronary artery aneurysms. during the acute KD phase predicted persistent or progressive TABLE 3 | Comparisons of children with late coronary artery aneurysms by coronary aneurysms at one month after KD onset in more than maximum coronary Z score on baseline echocardiography. two-thirds of their patients (26). In addition, McCrindle et al. Baseline Zmax reported that if the Zmax was ≥2.5 in initial echocardiography, the Z score remained ≥2.5 over 5 weeks of follow-up in 78%
Huang et al. Coronary Z-Score and Kawasaki Disease
scores ≥2.5, meaning a significant abnormality of the coronary may spontaneously regress over time, a prospective study
artery. Our findings are also supported by a previous study in with more frequently repeated echocardiograms may better
which the authors concluded that patients with KD with coronary detect the occurrence of late CAAs. We may have missed
artery diameter variations in the LMCA and RCA were at an some less severe cases because follow-up echocardiography
increased risk of treatment failure and that those with increased for patients without baseline CAAs tends to be postponed,
systemic inflammatory parameters may be at a higher risk of and only patients with outcome data from echocardiograms
coronary artery events (31). Therefore, we calculated LMCA, during the study period were included. In addition, most of
RCA, and LAD Z scores and targeted the coronary lesions at the patients with IVIG resistance received additional therapy,
11–60 days after illness onset to maximize the detection of which would have biased our study towards less positive
late CAAs. results by improving coronary artery outcomes at 11–60
Sensitivity and specificity of baseline Zmax were good for the days of illness. Moreover, the relatively small number of
prediction of the later development of CAAs in our patients. patients with late CAAs restricted our ability to reach some
However, it had a low positive predictive value, which may be due comparative conclusions between those with baseline Zmax < 2.0
to the regression of coronary arteries from a higher to normal Z and ≥2.0.
score after IVIG treatment. Conversely, the negative predictive
value was 97 %, as patients with baseline ZmaxHuang et al. Coronary Z-Score and Kawasaki Disease
7. Dedeoglu R, Barut K, Oztunc F, Atik S, Adrovic A, Sahin S, et al. Evaluation from the American heart association. Circulation. (2017) 135:e927–e99.
of myocardial deformation in patients with Kawasaki disease using speckle- doi: 10.1161/CIR.0000000000000484
tracking echocardiography during mid-term follow-up. Cardiol Young. (2017) 25. Lin MT, Chang CH, Hsieh WC, Chang CE, Chang YM, Chen YC, et al.
27:1377–85. doi: 10.1017/S1047951117000580 Coronary diameters in Taiwanese children younger than 6 years old: Z-
8. Durongpisitkul K, Gururaj VJ, Park JM, Martin CF. The prevention of score regression equations derived from body surface area. Acta Cardiol Sin.
coronary artery aneurysm in Kawasaki disease: a meta-analysis on the efficacy (2014) 30:266–73.
of aspirin and immunoglobulin treatment. Pediatrics. (1995) 96:1057–61. 26. Liu MY, Liu HM, Wu CH, Chang CH, Huang GJ, Chen CA, et al. Risk factors
9. Ogata S, Tremoulet AH, Sato Y, Ueda K, Shimizu C, Sun X, et al. Coronary and implications of progressive coronary dilatation in children with Kawasaki
artery outcomes among children with Kawasaki disease in the United States disease. BMC Pediatr. (2017) 17:139. doi: 10.1186/s12887-017-0895-8
and Japan. Int J Cardiol. (2013) 168:3825–8. doi: 10.1016/j.ijcard.2013.06.027 27. McCrindle BW Li JS, Minich LL, Colan SD, Atz AM, Takahashi M,
10. Holve TJ, Patel A, Chau Q, Marks AR, Meadows A, Zaroff JG. Long-term et al. Coronary artery involvement in children with Kawasaki disease: risk
cardiovascular outcomes in survivors of Kawasaki disease. Pediatrics. (2014) factors from analysis of serial normalized measurements. Circulation. (2007)
133:e305–11. doi: 10.1542/peds.2013-1638 116:174–9. doi: 10.1161/CIRCULATIONAHA.107.690875
11. Dionne A, Burns JC, Dahdah N, Tremoulet AH, Gauvreau K, de Ferranti 28. Ma S, Choi SY, Ahn HJ, Siu AM, Melish ME, Bratincsak A. The importance of
SD, et al. Treatment intensification in patients with Kawasaki disease echocardiogram during the second week of illness in children with Kawasaki
and coronary aneurysm at diagnosis. Pediatrics. (2019) 143:e20183341. disease. J Pediatr. (2020) 218:72-7.e71. doi: 10.1016/j.jpeds.2019.10.067
doi: 10.1542/peds.2018-3341 29. Takahashi K, Oharaseki T, Naoe S, Wakayama M, Yokouchi Y. Neutrophilic
12. Chen S, Dong Y, Kiuchi MG, Tremoulet AH, Gauvreau K, de Ferranti SD, involvement in the damage to coronary arteries in acute stage of Kawasaki
et al. Coronary artery complication in Kawasaki disease and the importance disease. Pediatr Int. (2005) 47:305–10. doi: 10.1111/j.1442-200x.2005.02049.x
of early intervention: a systematic review and meta-analysis. JAMA Pediatr. 30. Ronai C, Hamaoka-Okamoto A, Baker AL, de Ferranti SD, Colan SD,
(2016) 170:1156–63. doi: 10.1001/jamapediatrics.2016.2055 Newburger JW, et al. Coronary artery aneurysm measurement and Z score
13. Anderson MS, Todd JK, Glodé MP. Delayed diagnosis of Kawasaki variability in Kawasaki disease. J Am Soc Echocardiogr. (2016) 29:150–7.
syndrome: an analysis of the problem. Pediatrics. (2005) 115:e428–433. doi: 10.1016/j.echo.2015.08.013
doi: 10.1542/peds.2004-1824 31. Dallaire F, Fournier A, Breton J, Nguyen TD, Spigelblatt L, Dahdah N. Marked
14. Ruan Y, Ye B, Zhao X. Clinical characteristics of Kawasaki syndrome and the variations in serial coronary artery diameter measures in Kawasaki disease:
risk factors for coronary artery lesions in China. Pediatr Infect Dis J. (2013) a new indicator of coronary involvement. J Am Soc Echocardiogr. (2012)
32:e397–402. doi: 10.1097/INF.0b013e31829dd45e 25:859–65. doi: 10.1016/j.echo.2012.05.019
15. Son MBF, Gauvreau K, Kim S, Tang A, Dedeoglu F, Fulton DR, et al. Predicting 32. Iemura M, Ishii M, Sugimura T, Akagi T, Kato H. Long term
coronary artery aneurysms in kawasaki disease at a north american center: consequences of regressed coronary aneurysms after Kawasaki disease:
an assessment of baseline z scores. J Am Heart Assoc. (2017) 6:e005378. vascular wall morphology and function. Heart. (2000) 83:307–11.
doi: 10.1161/JAHA.116.005378 doi: 10.1136/heart.83.3.307
16. Yan F, Pan B, Sun H, Tian J, Li M. Risk Factors of coronary artery abnormality 33. Orenstein JM, Shulman ST, Fox LM, Baker SC, Takahashi M, Bhatti TR, et al.
in children with Kawasaki disease: a systematic review and meta-analysis. Three linked vasculopathic processes characterize Kawasaki disease: a light
Front Pediatr. (2019) 7:374. doi: 10.3389/fped.2019.00374 and transmission electron microscopic study. PLoS ONE. (2012) 7:e38998.
17. Han RK, Sinclair B, Newman A, Silverman ED, Taylor GW, Walsh P, et al. doi: 10.1371/journal.pone.0038998
Recognition and management of Kawasaki disease. CMAJ. (2000) 162:807–12. 34. Gordon JB, Kahn AM, Burns JC. When children with Kawasaki disease grow
18. Belay ED, Maddox RA, Holman RC, Curns AT, Ballah K, Schonberger LB. up: myocardial and vascular complications in adulthood. J Am Coll Cardiol.
Kawasaki syndrome and risk factors for coronary artery abnormalities: (2009) 54:1911–20. doi: 10.1016/j.jacc.2009.04.102
United States, 1994-2003. Pediatr Infect Dis J. (2006) 25:245–9. 35. Fujiwara T, Fujiwara H, Nakano H. Pathological features of coronary
doi: 10.1097/01.inf.0000202068.30956.16 arteries in children with Kawasaki disease in which coronary arterial
19. Cameron SA, Carr M, Pahl E, DeMarais N, Shulman ST, Rowley aneurysm was absent at autopsy. Quant. Anal. Circ. (1988) 78:345–50.
AH. Coronary artery aneurysms are more severe in infants than in doi: 10.1161/01.CIR.78.2.345
older children with Kawasaki disease. Arch Dis Child. (2019) 104:451–5. 36. Tsuda E, Tsujii N, Hayama Y. Cardiac events and the maximum diameter of
doi: 10.1136/archdischild-2018-314967 coronary artery aneurysms in Kawasaki disease. J Pediatr. (2017) 188:70-4.e71.
20. Suzuki Y, Iijima M, Sasaki H, Muto T, Tanaka H, Kaneko K, et al. Tachycardia doi: 10.1016/j.jpeds.2017.05.055
as a potential risk indicator for coronary arterial lesions in Kawasaki disease.
Eur J Pediatr. (1999) 158:207–9. doi: 10.1007/s004310051050 Conflict of Interest: The authors declare that the research was conducted in the
21. Chbeir D, Gaschignard J, Bonnefoy R, Beyler C, Melki I, Faye A, et al. absence of any commercial or financial relationships that could be construed as a
Kawasaki disease: abnormal initial echocardiogram is associated with potential conflict of interest.
resistance to IV Ig and development of coronary artery lesions. Pediatr
Rheumatol Online J. (2018) 16:48. doi: 10.1186/s12969-018-0264-7 Publisher’s Note: All claims expressed in this article are solely those of the authors
22. Liu L, Luo C, Hua Y, Wu M, Shao S, Liu X, et al. Risk factors associated and do not necessarily represent those of their affiliated organizations, or those of
with progression and persistence of small- and medium-sized coronary artery
the publisher, the editors and the reviewers. Any product that may be evaluated in
aneurysms in Kawasaki disease: a prospective cohort study. Eur J Pediatr.
this article, or claim that may be made by its manufacturer, is not guaranteed or
(2020) 179:891-900. doi: 10.1007/s00431-019-03492-8
23. Friedman KG, Gauvreau K, Hamaoka-Okamoto A, Tang A, Berry endorsed by the publisher.
E, Tremoulet AH, et al. Coronary artery aneurysms in Kawasaki Copyright © 2021 Huang, Chiu, Huang, Chao and Chi. This is an open-access
disease: risk factors for progressive disease and adverse cardiac article distributed under the terms of the Creative Commons Attribution License (CC
events in the US Population. J Am Heart Assoc. (2016) 5:e003289. BY). The use, distribution or reproduction in other forums is permitted, provided
doi: 10.1161/JAHA.116.003289 the original author(s) and the copyright owner(s) are credited and that the original
24. McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, publication in this journal is cited, in accordance with accepted academic practice.
Gewitz M, et al. Diagnosis, treatment, and long-term management No use, distribution or reproduction is permitted which does not comply with these
of Kawasaki disease: a scientific statement for health professionals terms.
Frontiers in Pediatrics | www.frontiersin.org 7 September 2021 | Volume 9 | Article 748467You can also read