Opioid Prescribing to US Children and Young Adults in 2019
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Opioid Prescribing to US Children and
Young Adults in 2019
Kao-Ping Chua, MD, PhD,a Chad M. Brummett, MD,b,c Rena M. Conti, PhD,d Amy S. Bohnert, PhDb,e
BACKGROUND:Recent national data are lacking on the prevalence, safety, and prescribers of abstract
opioid prescriptions dispensed to children and young adults aged 0 to 21 years.
METHODS: We identified opioid prescriptions dispensed to children and young adults in 2019 in
the IQVIA Longitudinal Prescription Database, which captures 92% of US pharmacies. We
calculated the proportion of all US children and young adults with $1 dispensed opioid
prescription in 2019. We calculated performance on 6 metrics of high-risk prescribing and the
proportion of prescriptions written by each specialty. Of all prescriptions and those classified
as high risk by $1 metric, we calculated the proportion written by high-volume prescribers
with prescription counts at the $95th percentile.
RESULTS:Analyses included 4 027 701 prescriptions. In 2019, 3.5% of US children and young
adults had $1 dispensed opioid prescription. Of prescriptions for opioid-naive patients, 41.8%
and 3.8% exceeded a 3-day and 7-day supply, respectively. Of prescriptions for young
children, 8.4% and 7.7% were for codeine and tramadol. Of prescriptions for adolescents and
young adults, 11.5% had daily dosages of $50 morphine milligram equivalents; 4.6% had
benzodiazepine overlap. Overall, 45.6% of prescriptions were high risk by $1 metric. Dentists
and surgeons wrote 61.4% of prescriptions. High-volume prescribers wrote 53.3% of
prescriptions and 53.1% of high-risk prescriptions.
CONCLUSIONS:Almost half of pediatric opioid prescriptions are high risk. To reduce high-risk
prescribing, initiatives targeting high-volume prescribers may be warranted. However, broad-
based initiatives are also needed to address the large share of high-risk prescribing
attributable to other prescribers.
a
Division of General Pediatrics, Department of Pediatrics, Susan B. Meister Child Health Evaluation and Research
Center, University of Michigan, Ann Arbor, Michigan; bDivision of Pain Medicine, Department of Anesthesiology,
University of Michigan Medical School, Ann Arbor, Michigan; cMichigan Opioid Prescribing Engagement Network,
Ann Arbor, Michigan; dDepartment of Markets, Public Policy, And Law, Institute for Health System Innovation and
Policy, Questrom School of Business, Boston University, Boston, Massachusetts; and eVA Center for Clinical WHAT’S KNOWN ON THIS SUBJECT: Recent national data
Management Research, VA Ann Arbor Health System, Ann Arbor, Michigan
are lacking on the prevalence of dispensed opioid
Dr Chua conceptualized and designed the study, collected the data, analyzed and interpreted prescriptions among US children and young adults; the
the data, drafted the initial manuscript, and reviewed and revised the manuscript; Drs frequency of high-risk prescriptions that increase risk of
Brummett and Conti conceptualized and designed the study, analyzed and interpreted the data, adverse events, including overdose; and the prescribers
and reviewed and revised the manuscript; Dr Bohnert conceptualized and designed the study, who account for the most prescriptions.
analyzed and interpreted the data, reviewed and revised the manuscript, and provided study
supervision; and all authors approved the final manuscript as submitted and agree to be WHAT THIS STUDY ADDS: Of 4 million opioid prescriptions
accountable for all aspects of the work. dispensed to US patients aged 0 to 21 years in 2019, 46%
were high risk. Dentists and surgeons wrote 61% of
DOI: https://doi.org/10.1542/peds.2021-051539 prescriptions. High-volume prescribers with prescription
Accepted for publication May 18, 2021 counts at the $95th percentile wrote 53% of prescriptions.
Address correspondence to Kao-Ping Chua, MD, PhD, 300 N Ingalls St, SPC 5456, Room 6E18, Ann
Arbor, MI 48109. E-mail: chuak@med.umich.edu To cite: Chua K-P, Brummett CM, Conti RM, et al. Opioid
Prescribing to US Children and Young Adults in 2019.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Pediatrics. 2021;148(3):e2021051539
Copyright © 2021 by the American Academy of Pediatrics
Downloaded from www.aappublications.org/news by guest on September 22, 2021
PEDIATRICS Volume 148, number 3, September 2021:e2021051539 ARTICLE
Ensuring the safety and METHODS children and young adults aged 0 to
appropriateness of pediatric opioid 21 years who lived in one of the 50
prescribing, defined as prescribing to Data Source
US states or the District of Columbia.
children aged 0 to 17 years and In January 2021, we conducted a We chose this age range to capture
young adults aged 18 to 21 years, is cross-sectional analysis of the 2019 the population seen by pediatric
an important clinical and public IQVIA Longitudinal Prescription providers.16 We did not include
health goal. In the short-term, Database. This database contains a prescriptions from veterinarians. We
prescription opioid exposure record for every prescription excluded prescriptions for injectable
increases the risk of opioid-related dispensed in 2019 from 92% of US opioid formulations and
adverse events, including retail pharmacies (eg, chain pharmacies prescriptions with missing or
overdose.1–6 In the long-term, this and food store pharmacies), 70% of potentially invalid dosing
exposure is associated with mail-order pharmacies, and 70% of information, defined as days
increased lifetime risk of substance pharmacies in long-term care supplied #0, days supplied >90, or
use disorders in adolescents and facilities. In the database, quantity #0.
young adults.7–9 Pediatric opioid dispensing from pharmacies that
prescribing also has spillover effects serve only patients from specific Prevalence of Dispensed Opioid
because opioids prescribed to hospitals or health systems (eg, Prescriptions
children and young adults can be those affiliated with Kaiser On the basis of dispensing totals and
misused by relatives and friends.10–12 Permanente) is not captured. Data population denominators from the
elements include drug name, dosing 2019 American Community
Recent national data are lacking on Survey,17 we calculated the
(eg, days supplied), prescriber
the prevalence of dispensed opioid proportion of US children and young
identifiers and specialty, patient
prescriptions among US children
identifiers and characteristics, and adults with $1 dispensed opioid
and young adults, the frequency of
method of payment (commercial, prescription in 2019 (see Appendix
high-risk prescriptions that
Medicaid or other non-Medicare 2 for details). We repeated analyses
increase the risk of opioid-related
public insurance [eg, state public by age group, sex, and Census region
adverse events, and the prescribers
insurance programs], cash, and of patient residence.
who account for the most pediatric
Medicare). Data on patient income,
opioid prescriptions and high-risk Frequency of High-risk Prescribing
race, ethnicity, and prescription
prescriptions. In previous studies,
indication are not included. As We calculated performance on 6
researchers have reported recent
needed, we used data from 2018 metrics of high-risk prescribing:
trends in opioid prescribing to
children by using commercial when a 90-day look-back period
was required for prescriptions in Metrics 1 and 2: Proportion of
insurance claims and data from
early 2019. dispensed opioid prescriptions to
individual states,13–15 but the
opioid-naive patients exceeding a
generalizability of findings is
Analyses assessed dispensing of 3-day or 7-day supply. The Cen-
unclear. Timely national data on
opioid analgesics and ters for Disease Control and Pre-
pediatric opioid prescribing could
benzodiazepines included in IQVIA’s vention opioid prescribing
inform the design of initiatives to
market definition of these drug guidelines indicate a 3-day sup-
improve this prescribing. For
example, if a small group of classes (Appendix 1). The former ply usually suffices for acute
prescribers accounts for most high- excluded opioid cough-and-cold pain, whereas supplies exceeding
risk prescribing, initiatives medications and buprenorphine 7 days are rarely necessary.18
targeting these prescribers may be formulations approved for opioid These thresholds were largely
warranted. use disorder. Because data were based on data from older adults
deidentified, the Institutional but may also be reasonable for
Using a national prescription- Review Board of the University of children and young adults. For
dispensing database, we assessed the Michigan Medical School exempted example, in previous studies, opi-
prevalence, safety, and prescribers of this study from review. oid consumption after common
opioid prescriptions dispensed to US pediatric surgeries was typically
children and young adults in 2019.
Sample #3 days.11,19,20 Because data
To our knowledge, we provide the Analyses were conducted at the lacked information on indication,
most recent and complete data on US prescription rather than patient we used opioid-naive status as a
pediatric opioid prescribing to date in level. We included opioid surrogate for acute pain. In sup-
this study. prescriptions dispensed in 2019 to port of this approach, 75.4% of
Downloaded from www.aappublications.org/news by guest on September 22, 2021
2 CHUA et al
prescriptions to opioid-naive Metric 6: Proportion of opioid counts at the $95th percentile. We
patients in this study were writ- prescriptions dispensed to ado- calculated the proportion of all
ten by dentists, surgeons, or lescents and young adults that prescriptions and high-risk
emergency medicine physicians overlapped with a benzodiaze- prescriptions accounted for by these
(Appendix 3). Following a pine prescription for $1 day. We high-volume prescribers versus other
National Quality Forum–endorsed included this metric because con- prescribers. Among prescriptions
quality measure, we defined opi- current opioid and benzodiaze- from high-volume prescribers and
oid-naive status as the absence of pine exposure greatly increases other prescribers that were eligible
dispensed opioid prescriptions in overdose risk in adolescents and for each metric of high-risk
the 90 days before dispensing.21 young adults.3 To calculate the prescribing, we calculated the
Metrics 3 and 4: Proportion of metric, we converted opioid and proportion classified as high risk by
opioid prescriptions dispensed to benzodiazepine prescriptions to the metric. We compared proportions
young children aged 0 to 11 periods of exposure that would using x2 tests.
years that were for codeine and occur if patients took medica-
proportion of these prescriptions tions as prescribed.3 This period We calculated performance on
that were for tramadol. In 2017, began on the dispensing date and metrics by specialty and determined
the US Food and Drug Adminis- ended on the dispensing date which specialties accounted for the
plus days supplied minus 1. If most high-risk prescriptions. We
tration contraindicated codeine
the exposure period for an opioid present results in Appendix 4 for
and tramadol use in young chil-
prescription overlapped with interested readers but do not
dren owing to reports of fatal
that of a benzodiazepine pre- discuss them owing to limited space.
overdose in this age group.22
Metric 5: Proportion of opioid scription, the opioid prescription
Statistical Analysis
prescriptions dispensed to ado- was included in the numerator.
Analyses used SAS 9.4 (SAS Institute,
lescents and young adults aged
We calculated the proportion of all Inc, Cary, NC), Stata 15.1 (Stata Corp,
12 to 21 years with daily dosages
prescriptions classified as high risk College Station, TX), and 2-sided
of $50 morphine milligram
by $1 metric. For each metric, we hypothesis tests with a 5 .05.
equivalents (MMEs). MMEs are a
calculated performance by
standardized measure of opioid
demographic characteristics. Using RESULTS
dosage; 50 MMEs corresponds to
logistic regression with Huber-White
10 pills containing 5 mg hydroco- Sample
robust standard errors clustered at
done.23 We calculated daily
the patient level, we assessed which The database included 144 734 094
MMEs by multiplying strength,
characteristics were associated with opioid prescriptions dispensed in
quantity, and published MME 2019; 4 030 834 (2.8%) were for
performance. We calculated average
conversion factors,23 then divid- patients aged 0 to 21 years. Of these
marginal effects (AMEs), or the
ing by days supplied. The 50- prescriptions, 3133 (0.08%) were
difference in the probability of
MME threshold derives from the excluded. Of the remaining
outcomes if all patients were in a
Centers for Disease Control and 4 027 701 prescriptions in the
particular demographic category
Prevention guidelines.18 Although
versus the baseline category.26 sample, 3 487 263 (86.6%) were for
this specific threshold has not adolescents and young adults and
been tested in adolescents and Prescribers of Opioid Prescriptions 3 250 443 (80.7%) were for opioid-
young adults, overdose risk in and High-risk Prescriptions naive patients. Method of payment
this population increases as daily In prescriber analyses, we excluded was commercial insurance for
opioid dosage rises.3 We did not prescriptions with missing prescriber 2 447 863 (60.8%) prescriptions,
assess this metric for young chil- identifiers. Of the remaining followed by Medicaid and/or other
dren because we lacked informa- prescriptions, we calculated the public insurance (1 106 206; 27.5%),
tion on weight, which affects proportion written by each specialty. cash (330 225; 8.2%), and Medicare
risks associated with any given To assess the degree to which (143 407; 3.6%). Hydrocodone
dosage level.24 In contrast, most pediatric opioid prescribing and high- accounted for 2 120 784 (52.7%)
opioid prescriptions to adolescents risk prescribing is concentrated, we prescriptions, followed by
and young adults use weight- ranked prescribers by the number of oxycodone (857 641; 21.3%),
invariant adult dosing. For exam- opioid prescriptions dispensed to codeine (556 463; 13.8%), and
ple, mean weight of adolescents children and young adults in 2019 tramadol (395 829; 9.8%); 51 046
aged 14 years is 50 kg.25 and identified those with prescription (1.3%) prescriptions were for
PEDIATRICS Volume 148, number 3,Downloaded
September from
2021 www.aappublications.org/news by guest on September 22, 2021 3TABLE 1 Prevalence of Dispensed Opioid Prescriptions Among US Children and Young Adults Aged 0 to 21 Years in 2019
Proportion Of US
No. Patients in the Rate of Dispensed Children and Young
Database With $1 US Population Opioid Prescriptions Adults With $1
No. Prescriptions Dispensed Opioid Denominator From per 100 US Children Dispensed Opioid
(Percentage of Total) Prescription in 2019 2019 ACSa and Young Adults Prescription in 2019
Overall 4 027 701 (100.0) 3 131 759 90 657 309 4.4 3.5
Age group, y
0–11 540 438 (13.4) 427 241 47 552 304 1.1 0.9
12–21 3 487 263 (86.6) 2 704 518 43 105 005 8.1 6.3
Sex
Male 1 818 708 (45.2) 1 430 441 46 439 447 3.9 3.1
Female 2 203 232 (54.7) 1 696 980 44 217 862 5.0 3.8
Unknown 5761 (0.1) 4338 N/Ab N/Ab N/Ab
Census region
Northeast 452 473 (11.2) 364 360 14 426 616 3.1 2.5
Midwest 854 430 (21.0) 663 939 19 050 769 4.5 3.5
South 1 906 296 (47.3) 1 446 345 35 350 669 5.4 4.1
West 824 502 (20.5) 660 969 21 829 255 3.8 3.0
N/A, not applicable; ACS, American Community Survey.
a
See Appendix 2 for details on obtaining population denominators.
b
Population denominators for patients of unknown sex could not be calculated. Prevalence estimates for male and female patients would be slightly higher if patient sex were
known for these 5761 prescriptions.
extended-release and/or long-acting Prevalence of Dispensed Opioid children aged 0 to 11 years and
opioids. Median days supplied was 3 Prescriptions adolescents and young adults aged 12
days (25th–75th percentile: 3–5). In Table 1, we display prevalence to 21 years, this proportion was 0.9%
The 4 027 701 prescriptions were estimates overall and by demographic and 6.3%, respectively. The proportion
for 3 131 759 patients; 449 310 subgroup. Of all US children and of children and young adults with $1
(14.3%) patients had multiple young adults, 3.5% had $1 dispensed dispensed opioid prescription in 2019
dispensed prescriptions in 2019. opioid prescription in 2019. For young was highest in the south (4.1%).
TABLE 2 Performance on 2 Metrics Assessing Days Supplied in Opioid Prescriptions for Opioid-Naive Children and Young Adults
Proportion of Prescriptions for Opioid-Naive Patients Proportion of Prescriptions for Opioid-Naive Patients
With Days Supplied >3 With Days Supplied >7a
No. Prescriptions No. Prescriptions No. Prescriptions No. Prescriptions
Eligible for Metric in Numerator (%) Eligible for Metric in Numerator (%)
Overall 3 250 443 1 359 082 (41.8) 3 250 443 124 874 (3.8)
Age group, y
0–11 437 914 234 551 (53.6) 437 914 40 770 (9.3)
12–21 2 812 529 1 124 531 (40.0) 2 812 529 84 104 (3.0)
Sex
Male 1 478 677 619 295 (41.9) 1 478 677 60 193 (4.1)
Female 1 767 313 737 723 (41.7) 1 767 313 64 127 (3.6)
Unknown 4453 2064 (46.4) 4453 554 (12.4)
Census region
Northeast 374 372 121 781 (32.5) 374 372 9648 (2.6)
Midwest 687 665 283 918 (41.3) 687 665 23 110 (3.4)
South 1 504 480 656 505 (43.6) 1 504 480 64 119 (4.3)
West 683 926 296 878 (43.4) 683 926 27 997 (4.1)
Method of payment
Commercial 2 034 441 797 592 (39.2) 2 034 441 66 649 (3.3)
Medicaid or other 912 743 412 178 (45.2) 912 743 26 297 (2.9)
public insurance
Cash 271 669 129 039 (47.5) 271 669 25 834 (9.5)
Medicareb 31 590 20 273 (64.2) 31 590 6094 (19.3)
Opioid-naive patients were those without any dispensed opioid prescriptions during the 90 days to 1 day before the dispensing date of the index prescription.
a
By definition, all prescriptions for opioid-naive patients with days supplied >7 days were included among prescriptions for opioid-naive patients with days supplied >3 days.
b
Medicare covers children and young adults with end-stage renal disease and some children and young adults with disabilities.
Downloaded from www.aappublications.org/news by guest on September 22, 2021
4 CHUA et alTABLE 3 Performance on 4 Age-Specific Metrics of High-risk Prescribing
Proportion of Prescriptions to Young Children Proportion of Prescriptions to Young Proportion of Prescriptions to AYAs Proportion of Prescriptions to
for Codeine Children for Tramadol With Daily MME $50 AYAs With Benzodiazepine Overlap
No. Prescriptions No. Prescriptions in No. Prescriptions No. Prescriptions in No. Prescriptions No. Prescriptions in No. Prescriptions No. Prescriptions in
Eligible for Metric Numerator (%) Eligible for Metric Numerator (%) Eligible for Metric Numerator (%) Eligible for Metric Numerator (%)
Age group, y
0–11 540 438 45 494 (8.4) 540 438 41 619 (7.7) N/A N/A N/A N/A
12–21 N/A N/A N/A N/A 3 487 263 402 430 (11.5) 3 487 263 159 269 (4.6)
Sex
Male 298 003 24 340 (8.2) 298 003 21 146 (7.1) 1 520 705 187 403 (12.3) 1 520 705 65 001 (4.3)
Female 241 208 21 031 (8.7) 241 208 19 953 (8.3) 1 962 024 214 469 (10.9) 1 962 024 94 075 (4.8)
Unknown 1227 123 (10.0) 1227 520 (42.4) 4534 558 (12.3) 4534 193 (4.3)
Census region
Northeast 44 250 3012 (6.8) 44 250 3744 (8.5) 408 223 48 281 (11.8) 408 223 19 858 (4.9)
PEDIATRICS Volume 148, number 3,Downloaded
Midwest 115 571 7477 (6.5) 115 571 8703 (7.5) 729 859 81 814 (11.2) 729 859 27 899 (3.8)
September from
South 286 899 28 354 (9.9) 286 899 23 672 (8.3) 1 618 397 184 779 (11.4) 1 618 397 80 367 (5.0)
West 93 718 6651 (7.1) 93 718 5500 (5.9) 730 784 87 556 (12.0) 730 784 31 145 (4.3)
Method of
payment
Commercial 268 783 22 721 (8.5) 268 783 22 774 (8.5) 2 179 080 267 919 (12.3) 2 179 080 93 839 (4.3)
Medicaid 184 193 9252 (5.0) 184 193 2304 (1.3) 922 013 79 380 (8.6) 922 013 30 315 (3.3)
or other
public
insurance
Cash 55 311 11 320 (20.5) 55 311 8986 (16.2) 274 914 29 402 (10.7) 274 914 10 504 (3.8)
Medicare 32 151 2201 (6.8) 32 151 7555 (23.5) 111 256 25 729 (23.1) 111 256 24 611 (22.1)
Young children were those aged 0 to 11 years; AYAs were those aged 12 to 21 years. AYA, adolescent and young adult; N/A, not applicable.
5 2021 www.aappublications.org/news by guest on September 22, 2021Frequency of High-risk Prescribing opioid-naive patients were less demographic subgroups were
In Tables 2–3, we display performance likely to exceed a 3-day supply if generally modest.
on the 6 metrics of high-risk they were for adolescents and young
adults rather than young children Prescribers of Opioid Prescriptions
prescribing. Among 3 250 443 and High-risk Prescriptions
prescriptions for opioid-naive patients, (unadjusted difference: 13.6
percentage points; AME: 12.2; 95% Of 4 027 701 prescriptions in the
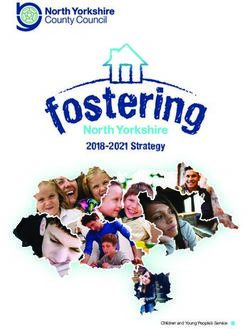
1 359 082 (41.8%) and 124 874 (3.8%)
exceeded a 3-day and 7-day supply, confidence interval [CI]: 12.4 to sample, 84 470 (2.1%) were
respectively (Fig 1). Among 540 438 12.1). The same pattern occurred excluded in prescriber analyses
prescriptions for young children, for prescriptions exceeding a 7-day owing to missing prescriber
45 494 (8.4%) and 41 619 (7.7%) were supply. Prescriptions to young identifiers. Of the remaining
for codeine and tramadol, respectively. children were less likely to be for 3 943 231 prescriptions, dentists
Among 3 487 263 prescriptions for codeine if the method of payment accounted for 1 504 370 (38.2%) and
adolescents and young adults, 402 430 was Medicaid and/or other public surgeons accounted for 918 154
(11.5%) had a daily MME of $50 and insurance rather than commercial (23.3%). These prescribers
159 269 (4.6%) had benzodiazepine insurance (unadjusted difference: collectively accounted for 2 422 524
overlap. Among all 4 027 701 3.4 percentage points; AME: 3.6; prescriptions (61.4%) (Table 4).
prescriptions, 1 834 776 (45.6%) were 95% CI: 3.7 to 3.4). The same Surgical subspecialties accounting
classified as high risk by $1 metric. pattern occurred for tramadol. For for the most prescriptions were
metrics assessing prescriptions to orthopedics (7.6% of the 3 943 231
For each metric, the AMEs of adolescents and young adults with a prescriptions) and otolaryngology
demographic characteristics on daily MME of $50 and opioid- (6.3%) (Appendix 6). Surgeons
performance are displayed in benzodiazepine overlap, (47.1%) accounted for a higher
Appendix 5. Prescriptions for performance differences between proportion of prescriptions for
FIGURE 1
Distribution of days supplied among dispensed opioid prescriptions for opioid-naive children and young adults. A total of 3 250 443 opioid prescriptions
were dispensed to such patients in 2019. Of these, 1 234 208 (38.0%) had days supplied between 4 and 7 days. Additionally, 2508 had days supplied exceeding
30 days; these prescriptions are not depicted in this graph owing to their small numbers.
Downloaded from www.aappublications.org/news by guest on September 22, 2021
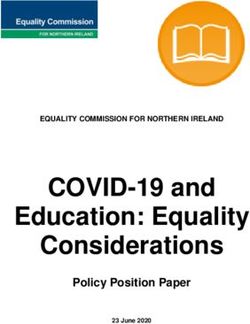
6 CHUA et alTABLE 4 Opioid Prescriptions Dispensed to Children and Young Adults In 2019, by Prescriber risk prescriptions (Figure 2). In
Specialty Appendix 8, we report results when
Specialty No. Prescriptions Percentage of All Prescriptions defining high-volume prescribers as
Dentista 1 504 370 38.2
those with prescription counts at the
Surgeryb 918 154 23.3 $99th percentile.
Physician assistant 282 194 7.2
Emergency medicinec 279 478 7.1 For each metric, we display the
Nurse practitioner 218 143 5.5 proportion of eligible prescriptions
Family medicined 194 316 4.9
from high-volume prescribers and
Obstetrics and/or gynecologye 138 889 3.5
Internal medicinef 85 539 2.2 other prescribers that were
General pediatrics 66 376 1.7 classified as high-risk in Figure 3.
Podiatry 59 830 1.5 This proportion was consistently
Pain medicine and anesthesiologyg 43 359 1.1 higher among prescriptions from
Hematology and/or oncologyh 37 655 1.0
Physical medicine and rehabilitationi 21 059 0.5
other prescribers (median
Hospice and/or palliative care 2599 0.1 difference: 2.9 percentage points;
All other prescribersj 81 434 2.1 P < .001 for all differences).
Unknown 9836 0.2
Totalk 3 943 231 100.0l
a DISCUSSION
Includes general dentists, dental subspecialists (anesthesiology, endodontics, orthodontics, pedodontists, periodon-
tics, and orthodontics), and oral and maxillofacial surgeons. In 2019, almost half of the 4 million
b
Includes cardiothoracic, colorectal, general, hand, neurosurgery, ophthalmology, orthopedic surgery, otolaryngology,
opioid prescriptions dispensed to US
pediatric, plastic, thoracic, transplant, urology, and vascular surgery.
c
Includes pediatric emergency medicine physicians and emergency medicine physicians in clinical informatics, medi- children and young adults were
cal toxicology, sports medicine, and underseas medicine. classified as high risk by at least 1
d
Includes family medicine physicians in clinical informatics, geriatric medicine, and sports medicine and those
dually boarded in family medicine and/or psychiatry.
of 6 metrics. Dentists and surgeons
e
Includes general obstetrics and/or gynecology, gynecologic oncology, maternal and fetal medicine, reproductive collectively accounted for 6 in 10
endocrinology and infertility, and female pelvic medicine and/or reconstructive surgery.
f
prescriptions. Approximately 20 000
Includes internists in sports medicine and geriatrics and physicians dually boarded in internal medicine and anes-
thesiology, family medicine, pediatrics, and preventive medicine.
high-volume prescribers (those with
g
Includes nonpain medicine anesthesiology and pain medicine physicians from anesthesiology, neurology, physical prescription counts at the $95th
medicine and/or rehabilitation, and psychiatry. percentile) accounted for 53% of all
h
Includes pediatric and nonpediatric hematology and/or oncology.
i
Includes pediatric and nonpediatric physical medicine and rehabilitation. Physical medicine and rehabilitation physi-
prescriptions and high-risk
cians in pain medicine were classified as pain medicine physicians. prescriptions.
j
Addiction, aerospace, allergy and/or immunology, anesthesiology, cardiology, chiropractic, critical care, dermatology,
endocrinology, gastroenterology, general practice, genetics, gastroenterology and/or hepatology, hospitalists, hygien-
In this study, we provide national
ist, infectious disease, legal medicine, microbiology, midwife, military, naturopath, neonatology, nephrology, neurology,
neuromuscular medicine, nuclear medicine, nurse, nurse anesthetist, occupational medicine, optometrist, osteopathy, data on the prevalence and
pathology, pharmaceutical medicine, pharmacist, preventive medicine, psychiatry, pulmonology, radiation oncology, demographic correlates of high-risk
radiology, rheumatology, sleep medicine, and toxicology. Also includes pediatricians in the following specialties: ado-
lescent medicine, child abuse, clinical informatics, developmental and/or behavioral, neurodevelopmental, medical
pediatric opioid prescribing. In
toxicology, sports medicine. These pediatricians accounted for just 673 pediatric opioid prescriptions. 2019, 41.8% and 3.8% of opioid
k
l
Sample for this analysis includes 3 943 231 prescriptions with nonmissing prescriber identifiers. prescriptions dispensed to opioid-
Values in the rows above do not add to 100% owing to rounding error.
naive children and young adults
exceeded a 3-day and 7-day supply,
young children than dentists prescribers with prescription counts of respectively, although many of these
(11.8%). In contrast, dentists $31, 7431 (35.6%) and 6684 (32.1%) prescriptions likely were for dental
(42.1%) accounted for a higher were dentists and surgeons; 10 579 and surgical procedures that do not
proportion of prescriptions for (50.7%) practiced in the south. Of the require long durations of opioid
adolescents and young adults than other 383 254 prescribers, 56 371 therapy.11,19,20,27 Investigators have
surgeons (19.7%) (Appendix 7). (14.7%) and 64 997 (17.0%) were substantially reduced opioid
General pediatricians accounted for dentists and surgeons; 154 852 quantities in perioperative
1.7% of the 3 943 231 prescriptions. (40.4%) practiced in the south. High- prescriptions for adult patients by
volume prescribers accounted for developing procedure-specific
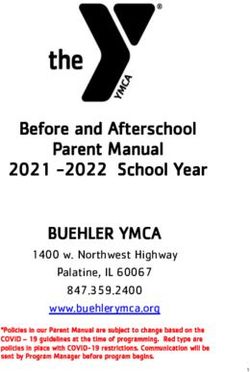
The 3 943 231 prescriptions were 2 100 283 prescriptions (53.3% of prescribing guidelines on the basis
written by 404 102 prescribers. The 3 943 231 prescriptions) and 950 137 of data on patient-reported
median prescriber accounted for 3 high-risk prescriptions (53.1% of postoperative opioid
prescriptions (25th–75th percentile: 1 787 721 high-risk prescriptions). consumption.28,29 Similar efforts
1–7). The 95th percentile was 31. Other prescribers accounted for 46.7% have begun in some pediatric
Among 20 848 (5.2%) high-volume and 46.9% of prescriptions and high- institutions30 but should be more
PEDIATRICS Volume 148, number 3,Downloaded
September from
2021 www.aappublications.org/news by guest on September 22, 2021 7FIGURE 2
Percent of pediatric opioid prescriptions and high-risk prescriptions accounted for by high-volume prescribers and other prescribers in 2019. High-volume
prescribers were the 20 848 prescribers with prescription counts at the 95th percentile or above among all clinicians who accounted for $1 dispensed opi-
oid prescription to children and young adults in 2019. Other prescribers were the 383 254 prescribers with prescriptions below the 95th percentile. Data
source: 2019 IQVIA Longitudinal Prescription Database.
widespread. Our findings highlight young children, electronic health anxiety, the most common
the importance of including young record systems and pharmacists indication for these medications.35
children in such efforts. In 2019, could prompt clinicians to consider Reducing low-value benzodiazepine
prescriptions for opioid-naive alternatives when this prescribing is prescribing may therefore be a
patients were more likely to exceed attempted. Additionally, insurers feasible method to reduce
a 3-day supply if they were for could refuse to cover codeine or concurrent opioid and
young children rather than for tramadol prescriptions for young benzodiazepine exposure.
adolescents and young adults, children.
potentially because the latter were The outsized role of dentists and
more likely to receive dental opioid Among opioid prescriptions surgeons in pediatric opioid
prescriptions, which are typically of dispensed to adolescents and young prescribing suggests that reductions
short duration.31 adults, 11.5% had daily opioid in prescribing by these clinicians
dosages of $50 MMEs. In the rare could substantially lower
Approximately 1 in 6 opioid instances in which such elevated prescription opioid exposure in
prescriptions dispensed to young dosages are required for children children and young adults. Evidence
children were for codeine or and young adults (eg, cancer pain), suggests such reductions could be
tramadol, both contraindicated in interventions to mitigate overdose achieved without compromising
this age group.22 The persistent use risk should be considered, such as pain control. For example, almost
of codeine is consistent with a study coprescribing naloxone.34 Moreover, 80% of dental opioid prescriptions
revealing incomplete reductions in 4.6% of opioid prescriptions for adolescents and young adults are
codeine prescribing to children dispensed to adolescents and young for tooth extraction,31 a procedure
undergoing tonsillectomy after a adults overlapped with a for which ibuprofen provides
2013 Food and Drug Administration benzodiazepine prescription. In this effective analgesia.36 As another
contraindication.32,33 To reduce population, benzodiazepines have example, randomized trials suggest
codeine and tramadol prescribing to limited evidence of efficacy for opioids and ibuprofen provide
Downloaded from www.aappublications.org/news by guest on September 22, 2021
8 CHUA et alFIGURE 3
Percent of eligible opioid prescriptions from high-volume prescribers and other prescribers that were classified as high-risk by 6 metrics. High-volume pre-
scribers were the 20 848 prescribers with prescription counts at the 95th percentile or above among all clinicians who accounted for $1 dispensed opioid
prescription to children and young adults in 2019. Other prescribers were the 383 254 prescribers with prescriptions below the 95th percentile. Data
source: 2019 IQVIA Longitudinal Prescription Database. AYA, adolescent and young adult; MME, morphine milligram equivalents.
equivalent analgesia for 53% of pediatric opioid High-volume prescribers also
tonsillectomy, a common pediatric prescriptions. The concentrated accounted for 53% of high-risk
surgery.37,38 Despite this, nature of pediatric opioid prescriptions. This finding suggests
researchers reported that 6 in 10 prescribing is consistent with a that initiatives to improve the safety
privately insured children previous study of opioid of pediatric opioid prescribing may
undergoing tonsillectomy from 2016 prescribing to privately insured be most efficient if they target high-
to 2017 had dispensed perioperative Americans, most of whom were volume prescribers. Importantly,
opioid prescriptions.39 Avoiding adults.41 Notably, high-volume however, other prescribers
opioid prescribing for surgical and prescribers may not necessarily collectively accounted for 47% of
dental procedures not only have high rates of opioid high-risk prescriptions and had
decreases the risk of misuse and prescribing. For example, slightly worse performance on
overdose but also decreases the risk surgeons whose patient volume is metrics of high-risk prescribing
of side effects, such as vomiting and higher than average may be high- compared with high-volume
constipation.40 Consequently, when volume prescribers even if their prescribers. Consequently, broad-
nonopioids provide effective prescribing rates are similar to based initiatives inclusive of all
analgesia, first-line use of these other surgeons. Nonetheless, the prescribers should also be
medications could improve safety outsized role of high-volume considered.
and patient experience. prescribers in pediatric opioid
prescribing suggests that We estimate that 6.3% of US
Approximately 20 000 high- their prescribing rates may adolescents and young adults had
volume prescribers accounted for warrant particular attention. dispensed opioid prescriptions in
PEDIATRICS Volume 148, number 3,Downloaded
September from
2021 www.aappublications.org/news by guest on September 22, 2021 92019. This estimate is markedly lower pharmacies. Second, dispensing from inform quality improvement
than the prevalence of past-year opioid hospital-specific pharmacies was not initiatives, unless the pandemic
use reported by adolescents and young observed. Some hospitals with such permanently alters practice.
adults participating in the National pharmacies may be affiliated with
Survey on Drug Use and Health academic medical centers, which CONCLUSIONS
(NSDUH). In the 2015–2016 NSDUH, may have prescribing practices that Reducing opioid prescribing by
17.2% and 24.4% of respondents aged differ from other settings. Third, the dentists and surgeons could
12 to 17 years and 18 to 25 years, role of surgical care in pediatric substantially lower prescription
respectively, reported past-year use of opioid prescribing is underestimated opioid exposure in children and
opioids prescribed to them but no in our analyses because physician young adults. To improve the safety
past-year misuse of their opioids or of assistants and nurse practitioners of pediatric opioid prescribing,
opioids prescribed to others.42 A account for one-fifth of initiatives targeting high-volume
caveat is that US opioid prescribing has perioperative opioid prescriptions.44 prescribers may be warranted.
declined since 2015, partly owing to
Fourth, because data lacked clinical However, broad-based initiatives are
heightened awareness of the opioid
details, the denominator for also needed to address the large
epidemic.43 Moreover, past-year opioid
estimates of the prevalence of share of high-risk prescribing
use could include use of leftover
dispensed opioid prescriptions could attributable to other prescribers.
opioids from prescriptions written
not be restricted to patients with
more than a year ago. Additional
potential indications for opioids (eg,
research is needed to reconcile our ABBREVIATIONS
estimates with the NSDUH. injuries). Finally, the outbreak of
coronavirus disease 2019 delayed AME: average marginal effect
Study strengths include our use of many dental and surgical CI: confidence interval
timely national data. However, procedures,45–47 the primary MME: morphine milligram
limitations exist. First, analyses indications for pediatric opioid equivalent
underestimate the prevalence of prescribing. Consequently, the rate NSDUH: National Survey on Drug
dispensed opioid prescriptions of this prescribing during the Use and Health
among US children and young adults pandemic is likely lower than in
because data do not include all 2019. However, findings will still
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported by the Susan B. Meister Child Health Evaluation and Research Center and the Janette Ferrantino Award (University of Michigan).
Further support was provided by the Substance Abuse and Mental Health Services Administration and the University of Michigan Precision Health Initiative.
Dr Chua is supported by a career development award from the National Institute on Drug Abuse (1K08DA048110). The funding sources played no role in the
design of the study; the collection, analysis, and interpretation of the data; and the decision to approve publication of the finished article. Funded by the
National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: Dr Brummett serves as a paid consultant for Heron Therapeutics, Vertex Pharmaceuticals, and Alosa Health and has
received fees for expert testimony. The other authors have indicated they have no potential conflicts of interest to disclose.
COMPANION PAPER: A companion to this article can be found online at www.pediatrics.org/cgi/doi/10.1542/peds.2021-052190.
REFERENCES overdose in adolescents and young 6. Gaither JR, Shabanova V, Leventhal JM.
1. Chung CP, Callahan ST, Cooper WO, et al. adults. JAMA Pediatr. US national trends in pediatric deaths
Outpatient opioid prescriptions for chil- 2020;174(2):141–148 from prescription and illicit opioids,
dren and opioid-related adverse events. 1999-2016. JAMA Netw Open. 2018;1(8):
4. Harbaugh CM, Lee JS, Hu HM, et al. Per-
Pediatrics. 2018;142(2):e20172156 e186558
sistent opioid use among pediatric
2. Groenewald CB, Zhou C, Palermo TM, patients after surgery. Pediatrics. 7. Miech R, Johnston L, O’Malley PM, Keyes
Van Cleve WC. Associations between opi- 2018;141(1):e20172439 KM, Heard K. Prescription opioids in
oid prescribing patterns and overdose adolescence and future opioid misuse.
among privately insured adolescents. 5. Gaither JR, Leventhal JM, Ryan SA, Pediatrics. 2015;136(5):e1169–e1177
Pediatrics. 2019;144(5):e20184070 Camenga DR. National trends in hospi-
8. McCabe SE, Boyd CJ, Evans-Polce RJ,
talizations for opioid poisonings among
3. Chua KP, Brummett CM, Conti RM, Boh- McCabe VV, Schulenberg JE, Veliz PT. Pills
children and adolescents, 1997 to 2012.
nert A. Association of opioid prescribing to powder: a 17-year transition from pre-
JAMA Pediatr. 2016;170(12):1195–1201
patterns with prescription opioid scription opioids to heroin among US
Downloaded from www.aappublications.org/news by guest on September 22, 2021
10 CHUA et aladolescents followed into adulthood. 20. Harbaugh CM, Vargas G, Streur CS, et al. 30. Freedman-Weiss MR, Chiu AS, Worhun-
J Addict Med. 2020;15(3):241–244 Eliminating unnecessary opioid exposure sky D, et al. An evidence-based guideline
after common children’s surgeries. JAMA supporting restricted opioid prescrip-
9. Quinn PD, Fine KL, Rickert ME, et al.
Surg. 2019;154(12):1154–1155 tion after pediatric appendectomy. J
Association of opioid prescription initia-
Pediatr Surg. 2020;55(1):106–111
tion during adolescence and young 21. Pharmacy Quality Alliance. PQA meas-
adulthood with subsequent substance- ures overview. 2020. Available at: 31. Chua KP, Hu HM, Waljee JF, Brummett
related morbidity. JAMA Pediatr. https://www.pqaalliance.org/assets/ CM, Nalliah RP. Opioid prescribing pat-
2020;174(11):1048–1055 Measures/PQA_Measures_Overview.pdf. terns by dental procedure among US
Accessed March 25, 2021 publicly and privately insured patients,
10. McCabe SE, West BT, Boyd CJ. Leftover
2013 through 2018. J Am Dent Assoc.
prescription opioids and nonmedical 22. Food and Drug Administration. FDA
2021;152(4):309–317
use among high school seniors: a restricts use of prescription codeine pain
multi-cohort national study. J Adolesc and cough medicines and tramadol pain 32. Chua KP, Shrime MG, Conti RM. Effect of
Health. 2013;52(4):480–485 medicines in children; recommends FDA investigation on opioid prescribing to
against use in breastfeeding women. children after tonsillectomy/adenoidec-
11. Voepel-Lewis T, Wagner D, Tait AR. Left- tomy. Pediatrics. 2017;140(6):e20171765
2017. Available at: https://www.fda.gov/
over prescription opioids after minor
downloads/Drugs/DrugSafety/UCM553814. 33. Food and Drug Administration. Safety
procedures: an unwitting source for
pdf. Accessed January 2, 2021 review update of codeine use in chil-
accidental overdose in children. JAMA
23. Centers for Disease Control and Preven- dren; new Boxed Warning and Contrain-
Pediatr. 2015;169(5):497–498
tion. Data resources: analyzing pre- dication on use after tonsillectomy
12. Chua KP, Brummett CM, Conti RM, Haffa- and/or adenoidectomy. 2013. Available
scription data and morphine milligram
jee RL, Prosser LA, Bohnert ASB. Assess- at: https://www.fda.gov/media/85072/
equivalents (MME). 2020. Available at:
ment of prescriber and pharmacy download. Accessed January 2, 2021
https://www.cdc.gov/drugoverdose/
shopping among the family members
resources/data.html. Accessed January 34. Guy GP Jr, Strahan AE, Haegerich T, et
of patients prescribed opioids. JAMA
2, 2021 al. Concurrent naloxone dispensing
Netw Open. 2019;2(5):e193673 among individuals with high-risk opioid
24. Basco WT Jr, Ebeling M, Garner SS, Hul-
13. Gagne JJ, He M, Bateman BT. Trends in prescriptions, USA, 2015-2019 [pub-
sey TC, Simpson K. Opioid Prescribing
opioid prescription in children and ado- lished online ahead of print March 9,
and Potential Overdose Errors Among
lescents in a commercially insured pop- 2021]. J Gen Intern Med. doi:10.1007/
Children 0 to 36 Months Old. Clin
ulation in the United States, 2004-2017. s11606-021-06662-3
Pediatr (Phila). 2015;54(8):738–744
JAMA Pediatr. 2019;173(1):98–99 35. Wang Z, Whiteside SPH, Sim L, et al.
25. Centers for Disease Control and Preven-
14. Brown KW, Carlisle K, Raman SR, et al. Comparative effectiveness and safety of
tion. Weight-for-age charts, 2 to 20
Children and the opioid epidemic: age- cognitive behavioral therapy and phar-
years, selected weight z-scores in kilo-
stratified exposures and harms. Health macotherapy for childhood anxiety dis-
grams, by sex and age. 2009. Available orders: a systematic review and meta-
Aff (Millwood). 2020;39(10):1737–1742
at: https://www.cdc.gov/growthcharts/ analysis. JAMA Pediatr. 2017;171(11):
15. Basco WT Jr, McCauley JL, Zhang J, et data/zscore/zwtage.xls. Accessed Janu- 1049–1056
al. Trends in dispensed opioid analgesic ary 2, 2021
prescriptions to children in South Caro- 36. Moore PA, Ziegler KM, Lipman RD, Ami-
26. Norton EC, Dowd BE, Maciejewski ML. noshariae A, Carrasco-Labra A, Mariotti
lina: 2010-2017. Pediatrics.
Marginal effects-quantifying the effect A. Benefits and harms associated with
2021;147(3):e20200649
of changes in risk factors in logistic analgesic medications used in the man-
16. Hardin AP, Hackell JM; COMMITTEE ON regression models. JAMA. agement of acute dental pain: an over-
PRACTICE AND AMBULATORY MEDICINE. 2019;321(13):1304–1305 view of systematic reviews. J Am Dent
Age limit of pediatrics. Pediatrics. Assoc. 2018;149(4):256–265.e3
27. Nalliah RP, Sloss KR, Kenney BC, et al.
2017;140(3):e20172151 Association of opioid use with pain and 37. Kelly LE, Sommer DD, Ramakrishna J, et
17. United States Census Bureau. American satisfaction after dental extraction. al. Morphine or ibuprofen for post-ton-
Community Survey (ACS). 2021. Available JAMA Netw Open. 2020;3(3):e200901 sillectomy analgesia: a randomized
at: https://www.census.gov/programs- 28. Vu JV, Howard RA, Gunaseelan V, Brum- trial. Pediatrics. 2015;135(2):307–313
surveys/acs. Accessed January 2, 2021 mett CM, Waljee JF, Englesbe MJ. State- 38. St Charles CS, Matt BH, Hamilton MM,
18. Dowell D, Haegerich TM, Chou R. CDC wide implementation of postoperative Katz BP. A comparison of ibuprofen ver-
guideline for prescribing opioids for opioid prescribing guidelines. N Engl J sus acetaminophen with codeine in the
chronic pain - United States, 2016. Med. 2019;381(7):680–682 young tonsillectomy patient. Otolaryngol
MMWR Recomm Rep. 2016;65(1):1–49 29. Michigan Opioid Prescribing Engage- Head Neck Surg. 1997;117(1):76–82
19. Monitto CL, Hsu A, Gao S, et al. Opioid ment Network. Opioid prescribing rec- 39. Chua KP, Harbaugh CM, Brummett CM,
prescribing for the treatment of acute ommendations. 2020. Available at: et al. Association of perioperative opi-
pain in children on hospital discharge. https://opioidprescribing.info. Accessed oid prescriptions with risk of complica-
Anesth Analg. 2017;125(6):2113–2122 January 2, 2021 tions after tonsillectomy in children.
PEDIATRICS Volume 148, number 3,Downloaded
September from
2021 www.aappublications.org/news by guest on September 22, 2021 11JAMA Otolaryngol Head Neck Surg. cation use and misuse subtypes in org/brief/asset/Dental%20Services%
2019;145(10):911–918 the United States. Addict Behav. 20and%20the%20Impact%20of%
40. Kelley-Quon LI, Kirkpatrick MG, Ricca RL, 2019;90:285–293 20COVID-19%20-%20An%20Analysis%20of
et al. Guidelines for opioid prescribing 43. Centers for Disease Control and Preven- %20Private%20Claims%20-%20A%20FAIR
in children and adolescents after sur- tion. U.S. opioid dispensing rate maps. %20Health%20Brief.pdf. Accessed
gery: an expert panel opinion. JAMA 2020. Available at: https://www.cdc.gov/ November 1, 2020
Surg. 2021;156(1):76–90 drugoverdose/maps/rxrate-maps.html. 46. Wolfson B. The pandemic is hurting
Accessed December 30, 2020 pediatric hospitals, too. Kaiser Health
41. Kiang MV, Humphreys K, Cullen MR,
Basu S. Opioid prescribing patterns 44. Cron DC, Lee JS, Dupree JM, et al. Pro- News. 2020. Available at: https://khn.
among medical providers in the United vider characteristics associated with org/news/the-pandemic-is-hurting-
States, 2003-17: retrospective, observa- outpatient opioid prescribing after sur- pediatric-hospitals-too/. Accessed July
tional study. BMJ. 2020;368:l6968 gery. Ann Surg. 2020;271(4):680–685 22, 2021
42. McCabe SE, Wilens TE, Boyd CJ, Chua 45. FAIR Health. Dental services and the 47. Meredith JW, High KP, Freischlag JA.
KP, Voepel-Lewis T, Schepis TS. Age- impact of covid-19: an analysis of pri- Preserving elective surgeries in the
specific risk of substance use disor- vate claims. 2020. Available at: https:// COVID-19 pandemic and the future.
ders associated with controlled medi- s3.amazonaws.com/media2.fairhealth. JAMA. 2020;324(17):1725–1726
Downloaded from www.aappublications.org/news by guest on September 22, 2021
12 CHUA et alOpioid Prescribing to US Children and Young Adults in 2019
Kao-Ping Chua, Chad M. Brummett, Rena M. Conti and Amy S. Bohnert
Pediatrics originally published online August 16, 2021;
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/early/2021/08/13/peds.2
021-051539
References This article cites 36 articles, 9 of which you can access for free at:
http://pediatrics.aappublications.org/content/early/2021/08/13/peds.2
021-051539#BIBL
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on September 22, 2021Opioid Prescribing to US Children and Young Adults in 2019
Kao-Ping Chua, Chad M. Brummett, Rena M. Conti and Amy S. Bohnert
Pediatrics originally published online August 16, 2021;
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/early/2021/08/13/peds.2021-051539
Data Supplement at:
http://pediatrics.aappublications.org/content/suppl/2021/08/13/peds.2021-051539.DCSupplemental
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2021
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
Downloaded from www.aappublications.org/news by guest on September 22, 2021You can also read