NHS Direct Booking Management Service - BMS Service Specification V2.0 September 2004
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
NHS Direct Booking Management Service BMS Service Specification V2.0 September 2004
NHS Direct Booking Management Service
BMS Service Specification
Owner Contact Details
For more information about the status Document owner:
of this document please contact the Linda.parker@nhsdirect.nhs.uk
NHS Direct Booking and Choice Team Linda Parker, Deputy Director –
Partnerships, NHS Direct Booking and 07990 650419
Choice Team
2Document Amendment History
Version Date Comment By Approved
0.1 15/3/2004 Version 0.1 for comment Elena Faraoni Dilip Chakrabarti
0.2 25/3/2004 Amended with comments from project team and Elena Faraoni Dilip Chakrabarti
MC for ICT section
0.3 30/3/2004 Formatting changes Elena Faraoni
0.4 07/04/2004 Minor Revisions – copy to NPfIT (MF) for Dilip Chakrabarti Dilip Chakrabarti
comment
0.5 13/05/2004 Amended with comments from NPfIT (MF and Linda Parker Dilip Chakrabarti
AF)
1.0 25/05/2004 Amended with comments from NHS Direct sites Linda Parker
1.1 9/8/2004 Revisions to reflect developments in Choose Linda Parker Dilip Chakrabarti
and Book programme
1.2 19/8/04 Amended after Booking and Choice Team Linda Parker Dilip Chakrabarti
comments
1.3 3/9/04 Amended in light of Choice Policy Framework Linda Parker Dilip Chakrabarti
document
1.4 6/9/04 Amended for comment by NPfIT Linda Parker
1.5 10/9/04 Amended with NPfIT comments Linda Parker
3TABLE OF CONTENTS
Page No.
1. Introduction 7
1.1 The Booking Management Service: Definition and the position of NHS Direct 7
1.2 Purpose of this document 7
1.3 Contact details for the NHS Direct Booking and Choice Team 9
2. NHS Direct BMS: The services that NHS Direct is able to provide 10
2.1 Overview 10
2.2 Booking Management Service definition 14
2.3 Delivering the service and meeting the standards 17
3. NHS Direct: Location of services 22
3.1 The approach and current provision 22
3.2 The process for preparing identified NHS Direct sites 23
4. NHS Direct BMS: Funding sources and mechanisms 25
4.1 Core services 25
4.2 Enhanced services 27
4.3 Invoicing procedures 27
5. NHS Direct: Support to local BMS solutions 30
5.1 The services provided to local BMS solutions 30
45.2 Joint working arrangements between NHS Direct and local BMS providers 31
during BMS implementation
6. Commissioning the BMS: Next Steps 33
6.1 Commissioning NHS Direct: Next Steps 33
6.2 Commissioning the BMS from non NHS Direct providers: Next Steps 34
7. Issues arising from Local Health Communities 36
7.1 Choice 36
7.2 Clinical assessment / triage 37
7.3 “Warm” call transfers 37
7.4 Proxy referrals on behalf of a Health Professional 38
7.5 TUPE 39
Glossary of Abbreviations 41
Appendices issued as part of this document:
A Initial planning template (45KB)
B Generic model Service Level Agreement (213KB)
C Summary of available Management Information reports (65KB)
5Appendices available on request (from linda.parker@nhsdirect.nhs.uk ):
D Appointment request / confirmation letters (generated by Choose and Book application) (43KB)
E Message Scripts (Welcome messages played to callers) (27KB)
F National Call Guidelines for BMS call handlers (283KB)
G Sample letters to non-bookers (46KB)
H Enhanced Services request / costing template (47KB)
I NHS Direct BMS Operational Policy (2.5MB)
61. INTRODUCTION
1.1 THE BOOKING MANAGEMENT SERVICE: DEFINITION AND THE POSITION OF NHS DIRECT
The Booking Management Service (BMS) is the telephone call centre function of the Choose and Book programme.
The BMS is a channel by which patients, clinicians and health and social care professionals can book appointments for
referrals made through Choose and Book (formerly known as Electronic Booking System – EBS). It will enable patients to
choose the date, time and service provider for their appointment, selectable from a short list agreed with their referring
clinician, in line with the Choice Policy Framework. The BMS performs only administrative functions and therefore does
not accept a duty of clinical care for the patient. This duty remains the preserve of the relevant clinicians.
Following a comprehensive options appraisal exercise, NHS Direct has been positioned as the preferred national
provider for the delivery of the BMS. However, “Where Strategic Health Authorities (SHAs) have already made previous
investment and arrangements, which have already gained clinical support and backing, they may choose to opt out of the
NHS Direct model, however, performance monitoring of the provision of BMS across the country will ensure that National
Standards, performance targets and value for money are achieved” 1.
1.2 PURPOSE OF THIS DOCUMENT
This document has been written to provide BMS commissioners with a clear understanding of the service proposition
being offered by NHS Direct in the context of its position as preferred national BMS provider.
1
Booking Management Resources Pack – Final Version 1.0
7The document has been updated to incorporate comments and queries raised by Local Health Communities that have
arisen during our early implementation discussions. Specifically, it includes:
• An outline of the services that are supported by NHS Direct within national BMS delivery (Section 2)
• The approach NHS Direct is taking in relation to the location of its BMS sites (Section 3)
• A description of the funding mechanisms that underpin the national development of BMS (Section 4)
• An outline of the support that NHS Direct will offer to Local Health Communities who
choose to develop local BMS solutions (Section 5)
• An outline of the steps that commissioners need to take to formally engage with NHS Direct (Section 6)
• A series of responses to issues that have been raised by Local Health Communities
e.g. Choice processes, support for clinical assessment mechanisms (Section 7)
This service specification has been developed on the basis of current functionality of Choose and Book. However, the
Booking and Choice programme is a rapidly emerging agenda and NHS Direct reserves the right to make adjustments to
this service specification in the light of future national programme developments.
81.3 CONTACT DETAILS FOR THE NHS DIRECT BOOKING AND CHOICE TEAM
Project Director Dilip Chakrabarti dilip.chakrabarti@nhsdirect.nhs.uk 07974 004798
Deputy Director – Operations Steve Kolodziej steve.kolodziej@nhsdirect.nhs.uk 07769 918279
Deputy Director – Partnerships Linda Parker linda.parker@nhsdirect.nhs.uk 07990 650419
National Systems Manager Linda Nelson linda.nelson@nhsdirect.nhs.uk 07769 918276
(Choose and Book)
IT & Telephony Lead Mike Cahill mike.cahill@nhsdirect nhs.uk 07769 918271
92. THE BMS: THE SERVICES THAT NHS DIRECT IS ABLE TO PROVIDE
This section of the document provides:
• An overview of how the BMS fits into the wider context of the Choose and Book programme
• A summary of the services the NHS Direct BMS is able to provide
• An overview of how NHS Direct will comply with the nationally defined service standards
2.1 OVERVIEW
The scope of the BMS is linked to the development of the Choose and Book software and can only offer services to
patients that have been referred using this system. Choose and Book has a planned release schedule and the BMS
functions will be able to develop in response to these releases. Choose and Book was launched in summer 2004 with
functional support for core services only. New releases of Choose and Book will expand the number of services
available.
• Core Services: Choose and Book will initially deliver the core service of referral and full booking from primary to
secondary care services in England for first outpatient appointment and day case bookings. This is the functionality
that will be supported by the BMS and for which funding support is available.
• Additional and Future Services: A number of additional services are named in the Electronic Booking Service
contract and, as these are taken up, the functionality will be available to the BMS.
In addition to the core and additional services that the BMS will support, commissioners may decide to enhance the
scope of the services offered to their patients. These enhanced services are likely to be outbound, telephony-based
functions, are outside the scope of Choose and Book core services and will be solely funded by the Local Health
10Community. The definition and procurement of any Enhanced Services will need to be the subject of discussions
between commissioners and NHS Direct.
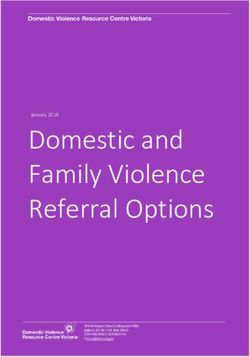
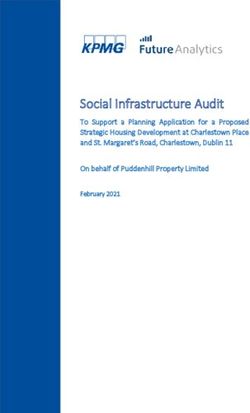
An overview of how the development of the BMS fits into the wider context of the development of the national Choose
and Book programme is provided in the diagram below.
Booking Management Service Choose and Book
Core Services
BMS to
provide call
Core services centre
Bookings & referrals into consultant and non-
support consultant led:
First outpatient appointments
Inbound: Booking, cancelling, queries, changing Day case bookings from primary care
Bookable mental health services
appointments for patients or health care
professionals
Outbound:Follow-up unmade appointments via
whitemail Additional & future services
BMS may Primary to primary bookings
Booking linked appointments
provide call Booking follow -up appointments
centre Recording patient transport requirements
support if Tertiary service booking
Booking into primary care services
required Bookings via DITV
Integration with call centre technology
Bookings into social care
Text message appointment reminders
Enhanced services : Transfer of EBS referral letters to the NCRS
to be defined on basis of local need between commissioners and
NHS Direct
Project Office .6
11The delivery of the core, additional / future and enhanced services depends on the interaction between different
stakeholders and funding streams. The framework for the delivery of these services is summarised in the table below.
Services Timescales for Service delivery Source of funding Source of funding Who is
delivery of dependant on for Choose and for supporting responsible for
Choose and Book Choose and Book Book application BMS the definition of
functionality application requirements?
Core services Summer 2004 Yes National National and Local NPfIT in
Delivery Plans consultation with
(LDPs) LHCs
Additional/ future Summer 2004- Yes National LDPs/ local benefits NPfIT in
services Summer 2008 on a realisation consultation with
“call off” basis LHCs
Enhanced Dependant on local No: Some services N/A LDPs LHCs with BMS
services health community are likely to only be provider
requirements practical when
Choose and Book
functionality offers
them e.g. follow-up
calls etc.
12The additional Choose and Book functionality planned in Releases 2 and 3, at the time of writing, is summarised in the
table below. However for the current position please visit the “Future Release” section of the Choose and Book website
http://chooseandbook.nhs.uk/implementation/future.asp
Release 2 Release 3
• Redirected referral • Tertiary referrals
• Clinical Assessment Service • Reminder letter generation function
• Primary – primary referrals (if clinic appears in
PAS)
• Inclusion of services which are not bookable via
Choose and Book on the Directory of Services
search
132.2 BOOKING MANAGEMENT SERVICE DEFINITION
The table below sets out what the BMS will provide nationally as core services, as well as summarising what additional /
future and enhanced services NHS Direct could potentially support.
Core Services Additional/ future Services Enhanced Services
Type of appointments dealt Type of appointments dealt with Type of appointments dealt with
with
Consultant and non consultant Primary Care Service appointments Potentially any appointments not
led first outpatient appointments (i.e. appointments with GPSIs) dealt with as part of the core,
additional or future services, as long
as they are supported by Choose
and Book
Consultant and non consultant GP appointments
led day case bookings referred
from Primary care
Consultant and non consultant Linked appointments (for the same
led bookable mental health clinical condition)
services
Tertiary care appointments
Follow-up appointments
Social care appointments
14Core Services Additional/ future Services Enhanced Services
BMS Services supported by Potential BMS Services that NHS Potential BMS Services that NHS
NHS Direct Direct could support Direct could support
Inbound: Patient books Health professional books, cancels, Outbound: BMS reminds patient of
appointment via BMS queries, changes appointments with appointment via white mail
patient present (for the types of
appointment defined above)
Inbound: Patient changes Outbound: BMS identifies reason for
appointment via BMS DNAs
Inbound: Patient queries Outbound: pre-assessment of
appointment via BMS referral
This is outside the scope of an
administrative BMS but please see
section 7.2 for further detail
Inbound: Patient cancels Outbound: post discharge follow-up
appointment via BMS call
Inbound: Health professional Inbound: provider changes, cancels
generates an appointment and queries appointment via BMS
request and then books
appointment with patient present The requirements of the Choice
via BMS Policy will need to be considered
where a provider cancels an
appointment
15Core Services Additional/ future Services Enhanced Services
Inbound: Health professional BMS makes a referral as a proxy for
changes the appointment with an authenticated NHS health care
patient present via BMS professional
The National Clinical Reference
Panel has confirmed that the
creation of an appointment request
carries clinical risk and is therefore
out of scope for BMS. Please see
Section 7.4 for more detail
Inbound: Health professional
cancels the appointment with
patient present via BMS
Inbound: Health professional
queries the appointment via BMS
Outbound: BMS follows-up
unmade appointments via
whitemail (post). The first
reminder letter will be sent within
2 postal days after the
appointment request appears on
the BMS worklist. An unbooked
appointment request will first
16Core Services Additional/ future Services Enhanced Services
appear on the BMS worklist after
7 days (system default). The
second and final letter will be
sent 7 days after that. (Copies of
the letters are available as
Appendix G)
Support Services offered by
NHS Direct
Management Information
Reporting against the 11 national
service standards
Customer satisfaction surveys
Call routing, load balancing, call
capacity management, out of
hours and Disaster Recovery
administration for LHCs with
local BMS solutions
2.3 DELIVERING THE SERVICE AND MEETING THE STANDARDS
NHS Direct will comply with all the service requirements set out in the Booking Management Resource Pack (NPfIT, Dec
2003). The majority of these standards are integral to shaping how the service is delivered, but several result in
measurable service outputs that will be reported to commissioners. The following table sets out how the 11 nationally-
defined service standards will be met.
17No. Standard How NHS Direct will meet the standard
1 HELA and DSE compliance for Call All BMS sites will be fully compliant with the relevant HELA and DSE
Centre Environments requirements and all members of staff will be trained appropriately.
2 National complaint handling and Following its formation as a Special Health Authority on April 1st 2004, NHS
escalation policies Direct has developed a single national complaints and escalation policy that
fully meets the national requirements.
3 Service availability and access BMS opening hours:
Call handlers staff rotas will be managed using validated call rostering tools, to
ensure that the BMS will be available from 7am to 10 pm, 365 days per year.
Handling planned and unplanned downtime/ peaks in demand:
Call escalation and business continuity procedures will be put in place across
BMS sites to ensure that the service can continue during periods of peaks in
demand or unexpected IT/ telephony downtime.
Intelligent Call Management (ICM) technology enables calls to the BMS to be
automatically routed and processed irrespective of the physical location of the
call centre. This process will not be apparent to the caller.
Providing equity in access:
NHS Direct BMS sites will provide access to interpretation services for non-
English speaking patients and text telephone facilities for hearing or speech-
impaired patients.
Providing single number access to the BMS:
NHS Direct is responsible for managing the three 0845 numbers that provide
national access to the BMS:
18No. Standard How NHS Direct will meet the standard
• 0845 60 88888 Patient telephone access
• 0845 8 50 11 50 Health care professional access
• 0845 8 50 22 50 TexBox user access
Callers will be charged at their normal local rate
Supporting LHCs with local BMS call centres:
Where LHCs wish to include a local BMS call centre as the preferred
answering location for their patients, Geographical Based Routing (GBR)
technology will allow calls from landlines, originating from within the agreed
geographical area representing their patients, to be offered to a local BMS. If
the local BMS is unavailable, or the call is not answered within 60 seconds, the
call will be answered by NHS Direct. Calls that cannot be determined as
originating from within the agreed geographical area (and under current
European regulations this includes calls from mobile telephones) will be
answered by NHS Direct.
4 Use of standard messaging NHS Direct will continue to work with representatives of LHCs, patient access
groups, the BMS telephony provider and the Booking and Choice programme
to develop, record and play national messaging to callers before their call is
connected to the local call centre. The current scripts are available as
Appendix E.
The BMS nationally will use identical call flow architectures and messaging
throughout the network of call centres.
5 Use of standard processes and NHS Direct has developed a standard operational manual, with training
dialogue courses to support the implementation of the manual and its procedures, for all
its BMS sites and associated staff (Appendix I). Staff will be using nationally
defined call structures and scripts and these are available as Appendix F.
19No. Standard How NHS Direct will meet the standard
6 Key Performance Indicators (KPIs) The performance of NHS Direct is already managed against a number of these
KPIs. Staff rostering tools and the use of ICM for call management purposes
will be actively managed to ensure that the BMS meets these targets. The
KPIs will be monitored on a daily basis at a national level and included in all
management information reports required by commissioners. Full use will be
made of technology to monitor demand.
7 Management Information A national framework of standard report forms has been developed and
appears as Appendix C. These will draw on information gathered via the
telephony system and data available from Choose and Book. NHS Direct will
work with its commissioners to agree any specific LHC requirements.
8 Compliance with Choice policy The BMS nationally will support the delivery of Choice at Point of Referral. The
service NHS Direct will offer will largely be driven by the Choice policy agreed
at Local Health Community level and the functionality of Choose and Book.
BMS staff will provide callers with objective information available either within
Choose and Book Directory of Services or nhs.uk but will not offer
interpretation of this information, nor will they offer support in clinical decision-
making. The BMS will direct the patient to talk to other health professionals to
gain the clinical advice they need, where appropriate.
In line with assumption 33 of the BMS Resource pack, the BMS will re-offer
patients the choice of provider, limited to those services short-listed by the
referring clinician, if their provider cancels the original appointment.
9 Referring callers The BMS will offer callers the telephone numbers of other NHS departments/
services for further detailed information, based on the data that local health
communities supply.
The BMS is currently not able to offer “warm” transfer of calls to other service
providers for technical reasons – please see section 7.4.
20No. Standard How NHS Direct will meet the standard
10 Cost per call The BMS will meet the cost per call requirement.
11 Promoting the use of other channels for In conjunction with NPfIT, LHCs, and its telephony provider, NHS Direct will
EBS use national messaging to promote the other ways of booking appointments.
Other Call recording All calls will be recorded and kept inline with current data retention
requirements. As an organisation, NHS Direct is moving towards national
infrastructure solutions
213. NHS DIRECT: LOCATION OF SERVICES
This section provides a description of the BMS site identification process, as an integral part of NHS Direct’s corporate
approach to a national organisational infrastructure.
3.1 THE APPROACH AND CURRENT PROVISION
As a result of its formation as a Special Health Authority in April 2004, NHS Direct is reviewing its operational approach in
order to maximise efficiency and support closer partnership working within the NHS. Services will move towards
organisation on a regional basis, with those regions mirroring the NPfIT clusters. This shift involves the review of current
estate, and the transition to new working arrangements will involve the development of existing and new sites, as well as
some rationalisation of existing delivery sites. The review provides an opportunity to take a strategic approach to the
siting of BMS delivery at an early stage in the national process.
When planning the location of BMS sites, the following fundamental working assumptions will be considered:
• The core functions of the BMS can be delivered from any location. If commissioners request enhanced services,
the NHS Direct Booking and Choice Team will evaluate whether these need to be locally provided and if so,
which is the best placed site to offer that provision
• Consolidating the service into fewer, larger call centres will reduce infrastructure and management overhead
costs and ensure best value for money (on a cost per call minute basis) for the NHS
Not all existing NHS Direct sites will provide BMS call centre functions, but careful consideration will be given to the
geographical spread across England.
22The North East London NHS Direct site in Ilford is currently delivering all BMS services for the Early Adopters who have
commissioned the service from NHS Direct, with the NHS Direct South West London site in Croydon offering business
continuity support. As the wider NHS Direct organisational “Blue Print” process2 develops and the Choose and Book
programme rollout schedule becomes clear, detailed modeling of call volumes will take place and new sites will be able
to be identified in a planned and structured manner.
3.2 THE PROCESS FOR PREPARING IDENTIFIED BMS SITES
The NHS Direct Booking and Choice Team and NPfIT are currently working together on detailed Choose and Book
rollout plans and timelines. These are taking into account the implications of hospital PAS upgrade / replacement
schedules and the development of SHA and PCT local BMS plans that are providing projected call volumes.
The National Booking and Choice Programme will agree the rollout of call volumes and staffing requirements with NHS
Direct. Sites will be identified and developed to support national BMS provision and an operational preparation process
will be started, as outlined in the table below.
Stage Stage Stage description
No.
1 Initial site selection The corporate Estates Review to identify those sites that will
deliver BMS, taking into account location, size and suitability
of physical and ICT infrastructure available at the site, as well
as development potential.
2
The Blue Print process involves consultation from October – December 2004 on the planned development of NHS Direct, its sites and
services with the rest of the NHS and other stakeholders
23Stage Stage Stage description
No.
2 Site state of readiness Sites will be audited against site readiness criteria. The audit
audit is a more detailed review of site suitability and its primary
objective is to identify any ICT or telephony developments
needed, in order to meet to the BMS service standards.
3 Modelling the demand The NHS Direct Booking and Choice Team will work with
forecasting against know NPfIT and LHCs to populate the data forecasting model, to
activity ensure that sufficient capacity is developed as needed.
4 Operational preparation The NHSD Booking and Choice Team will work with the
for go-live selected site to ensure it is ready for the set “go-live” date.
244. THE BMS: FUNDING SOURCES AND MECHANISMS
This section of the document describes:
• The funding mechanism for BMS provision
• The invoicing procedures between NHS Direct and PCTs
4.1 CORE SERVICES
Until December 2005 NHS Direct will invoice LHCs at the rate of £0.42 per call minute, capped at a maximum call length
of six minutes, for inbound calls to the BMS handled on behalf of their patients. LHCs will be entitled to reclaim 100% of
this cost from the Department of Health subject to the constraints of HM Treasury approved budgets. From December
2005 NHS Direct will invoice LHCs at actual cost of providing core BMS services to their patients. Funding support for
BMS will be allocated on a capitation basis to the LHCs, through their nominated lead PCT. Funding support for BMS will
be available until at least the end of Financial Year 2007/8
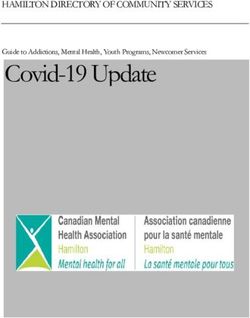
Until December 2005, due to anticipated low call volumes, the actual cost of providing the BMS (fixed set-up,
infrastructure and management costs) will not be covered by the amount NHS Direct invoices the LHCs. Therefore the
National Booking and Choice Programme has agreed to fund the difference between NHS Direct’s actual costs and the
monies invoiced to LHCs, subject to the constraints of HM Treasury approved budgets. This arrangement protects BMS
commissioners against disproportionate costs being levied during the rollout phase, prior to the service being able to
operate at scale.
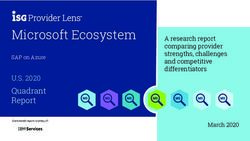
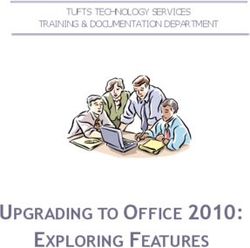
The diagram below shows how, as call volumes increase, the difference between the actual cost of providing the BMS
and the monies invoiced to the LHCs diminishes, eventually disappearing altogether. This point is predicted to be
25reached during the summer / early autumn 2005 but is dependent upon rate of rollout achieved. Once this point has been
reached the actual cost of providing the BMS will be funded solely by the LHCs.
BMS Funding until December 2005
100%
90%
80%
70%
actual cost of BMS
60%
Central funded
50%
LHC funded
40%
30%
20%
10%
0%
04
05
05
4
5
04
5
05
4
5
-0
-0
-0
-0
-0
n-
n-
b-
c-
c-
pr
ug
ug
ct
ct
Ju
Ju
Fe
De
De
O
O
A
A
A
26Early Adopters in cluster Anticipated funding for core services supported by central funding allocation to SHAs. Any
shortfalls to be supplemented by national funding until the cost of providing the service
equals the funding raised by actual calls
Full Roll-out in cluster Local allocations only
4.2 ENHANCED SERVICES
No central funding has been allocated for BMS support to the provision of enhanced services. If Local Health
Communities decide to opt for the provision of any enhanced services these will need to be funded locally and
commissioned separately.
Discussions about the provision of enhanced services will take place between local commissioners and NHS Direct, the
process being supported by a concise planning template, available as Appendix H.
4.3 INVOICING PROCEDURES
Until December 2005, NHS Direct is invoicing each PCT, via their nominated lead PCT, on a quarterly basis for
transactions processed through the Choose and Book application, at the end of each quarter. This avoids raising invoices
based on predicted call volumes and then adjusting subsequent invoices to reflect actual call volumes.
From December 2005 the intention is to raise invoices at the start of each quarter, or month, depending on the level of
funding and size of service involved.
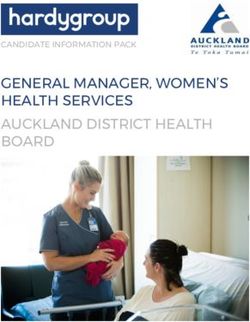
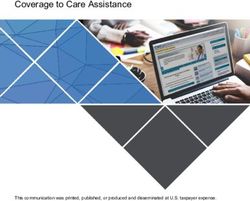
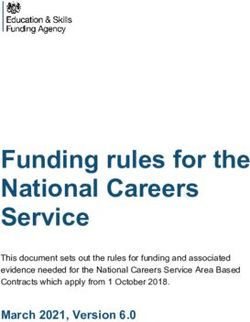
27Telephony switch data is not able to report calls on an individual PCT basis. Consequently, BMS usage will be calculated
from activity recorded through the Choose and Book application. All activity – bookings, amendments and cancellations –
will be used to apportion calls to PCTs for charging purposes and the diagram below shows the methodology to be used,
including the formula for calculating costs. The text telephone calls will be charged at the same rate as other calls, but
they are likely to be much longer calls.
There will inevitably be a difference between the level of Choose and Book activity reported from the software and the
actual number of calls logged by the telephony switch system but if, over time, this difference appears significant, NHS
Direct will examine the reasons for the divergence.
28NHS DIRECT – BMS PCT CALL CHARGING METHODOLOGY
At the end of each invoicing period all PCT’s will receive an invoice from NHS
PCT 1 23% Direct for any calls processed through Choose and Book. As the call telephony
switch cannot allocate call volumes by PCT (and this is illegal for mobile calls) the
PCT 2 17% total number of effective calls coming into NHS Direct will be apportioned to each
All BMS calls received PCT, based on the activity recorded against them from Choose and Book.
by NHSD
PCT 3 16% The number of text telephone calls is expected to be very low, but the calls may
10,000 be upto 30 minutes in duration.
(month 1) PCT 4 14%
The number of calls will be multiplied by the average call length for each call type,
multiplied by £0.42
PCT 5 26%
PCT 6 4% FORMULA =
(Total Call Vol) x (PCT Choose & Book Activity) x (Avg Call Length – capped at 6
mins until Dec 2005) x (£0.42)
Effective Calls received from
BT to NHS Direct % of monthly N.B This methodology will be reviewed in March 2005 in the light of actual call
activity put
activity data
through
Choose &
Book
application for
each PCT
295. NHS DIRECT: SUPPORT TO LOCAL BMS SOLUTIONS
This section of the document describes:
• The support NHS Direct will provide to Local Health Communities with local BMS solutions
• The joint working arrangements during BMS implementation
5.1 SUPPORT PROVIDED TO LHCs WITH LOCAL BMS SOLUTIONS
All patients will access the BMS via nationally-defined 0845 numbers (see P.19). These numbers have been set by the
National Programme for IT, are not NHS Direct numbers and will be the access numbers for all BMS delivery, irrespective
of provider.
NHS Direct will provide the following support to local BMS providers:
• Management of the national BMS call distribution platform
• Management of the infrastructure to support geographical-based call routing
NHS Direct will facilitate the creation of a call routing plan by liaising with all other BMS providers, or their
commissioners, and the call distribution platform provider. It should be noted that geographical routing areas
are defined by BT telephone exchange areas and may not always map directly onto PCT geographical
boundaries. All calls that are incorrectly routed to NHS Direct BMS will be answered and processed to
ensure compliance with e-government directives for UK public sector call centres. All callers who use a
mobile phone will be routed to NHS Direct BMS. These calls cannot be geographically routed as current
European regulations do not permit the use of mobile location information to route calls. It is estimated that
3020% of total calls to the BMS will come from mobile phones. NHS Direct will invoice PCTs for the handling of
their patients’ calls under these circumstances as defined in section 4.3
• Provision of raw data for management information purposes:
NHS Direct will provide the raw data relating to the calls received through the call distribution platform.
Details of the data are outlined in Appendix C. The analysis of this data for management information
purposes, and performance reporting to commissioners against the 11 service standards by non NHS Direct
BMS, however, will remain the responsibility of the local BMS.
Commissioners for local BMS solutions will be charged £0.01 per call minute for calls routed via the national call
distribution platform. This charge applies to all calls that are routed in line with the call routing plan agreed before go-live.
If calls are subsequently rerouted and handled by NHS Direct because of unavailability of the local site or failure to
answer the call within 60 seconds, NHS Direct will invoice PCTs for the handling of these calls at the standard rate of
£0.42 per minute, as set out in section 4.3
5.2 JOINT WORKING ARRANGMEENTS BETWEEN NHS DIRECT AND LOCAL BMS PROVIDERS DURING
IMPLEMENTATION
Where the BMS in any locality is not being delivered by NHS Direct, discussions will take place during implementation
between the local BMS provider and NHS Direct to understand:
• Proposed timelines for implementation
• The nature and extent of the service being provided and any business continuity / out of hours implications
for NHS Direct
• Detail of the requirements of the call routing plan
31• The respective operational processes of both NHS Direct and the alternative BMS provider
Should a local BMS provider wish NHS Direct to provide support around specific aspects of service development, for
example staff training, this can be the subject of local negotiation and associated service agreement.
326. COMMISSIONING THE BMS: NEXT STEPS
This section offers:
• Guidance on the next steps commissioners should take should they decide to choose this service
proposition
• Guidance on the next steps commissioners should take if they wish to develop their own BMS
6.1 COMMISSIONING NHS DIRECT: THE NEXT STEPS
In order to begin discussions with NHS Direct regarding the provision of the national BMS model, Local Health
Communities should contact a member of the NHS Direct Booking and Choice Team – whose details appear on Page 9.
NHS Direct will provide an information pack, comprising the current version of the BMS Service Specification (this
document), a generic Service Level Agreement document (Appendix B) - to offer an outline of what the respective
commitments are - and a spreadsheet template requesting the information needed to begin detailed operational planning
(Appendix A).
Using this information, commissioners will need to consider:
• Options for provision: Full NHS Direct or partial NHS Direct
• Whether the core service only is required, or whether local enhancements are needed
If the service is to be commissioned – wholly or partly – from NHS Direct, the spreadsheet within the pack gives full detail
of the information needed, but the table below summarises the information requirements and associated timescales.
33Information requirements Timescales for delivery of the
information
• Lead contact details in the LHC
• Planned go-live date and relevant
technical interdependencies Information required a minimum of 3
Local Health Community • Details of the PCTs / GP practices / months prior to planned go-live
Acute Trusts involved
• Planned specialties
• Expected call volumes for at least
the next 6-9 months
6.2 COMMISSIONING THE BMS FROM LOCAL PROVIDERS: THE NEXT STEPS
Local Health Communities have the opportunity of developing local BMS solutions. However, NHS Direct needs to be
aware of the planning of that provision in order to support the plans for national call routing and the management of the
call distribution platform. It is essential that commissioners contact a member of the NHS Direct Booking and Choice
Team (details on Page 9) at an early stage in BMS development. The table below sets out a summary of the information
that is required by NHS Direct.
34Information requirements Timescales for delivery of the
information
• Lead contact details in the LHC
• Planned go-live date and relevant
technical interdependencies Information required a minimum of 3
Non NHS Direct BMS • Details of postcodes, in order to months prior to planned go-live
develop the call routing plan
• Information about the line value of
the proposed call centre
• Proposed service model for
business continuity / disaster
recovery planning
357. ISSUES ARISING FROM LOCAL HEALTH COMMUNITIES
During the early phase of Choose and Book implementation, a number of recurring themes have emerged in discussion
with Local Health Communities. The answers to some of these are still emerging as experience develops, and
implementation approaches are being updated to take advantage of lessons learnt / best practice. This section offers the
current best practice response from NHS Direct to the issues raised, and indicates where further discussion needs to
take place.
7.1 CHOICE
The Choice Policy Framework states that the BMS will support Choice decisions based on
• Waiting times
• Location and convenience of appointment
• Patient experience
• Clinical quality
The Choose and Book application supports provision of information about waiting times and location for the patient.
Furthermore, both the Choose and Book Directory of Services and www.nhs.uk will contain information about the
convenience of hospitals and their facilities. The BMS, therefore, will support patients in making their choice, using these
two sources of information, as part of the core service, within core funding. This will, however, need to be kept under
review as experience develops, to assess the impact on the average call length of 4-6 minutes outlined in the HM
Treasury Full Business Case.
36Provision of information about patient experience and clinical quality needs to be examined in the light of shared
information systems, supporting Choice across multiple providers. The role and position of Clinical Assessment Services
in the process for the patient also needs to be considered (see 7.2).
Some commissioners have requested that the NHS Direct BMS directs patients to other specific information providers,
prior to a decision being made about choice of location. Processes will need to be developed in partnership with these
communities to ensure that offering a service to a limited group of patients neither affects the quality of service to other
patients, not puts their own patients at a disadvantage by increasing the complexity of their booking experience e.g.
offering patients a range of telephone numbers. The issues relating to the “warm” transfer of calls are addressed in 7.3
below.
In relation to the PCTs’ requirement to provide information for www.nhs.uk, pending further national direction on roles
and responsibilities, NHS Direct and its Health Information Service may be able to help PCTs and other organisations in
the development and maintenance of their local information systems, to enable them to meet their objectives.
7.2 CLINICAL ASSESSMENT / TRIAGE
The Clinical Assessment Service will be available in the Choose and Book application from Release 2. This offers Local
Health Communities the opportunity to triage referrals before a referral and booking are made, but is not part of the core
function of an administrative BMS. If LHCs wish to consider commissioning this clinical service from NHS Direct,
discussions should take place on an individual basis, as for other service enhancements.
7.3 “WARM” CALL TRANSFERS
Health Communities have expressed concern at NHS Direct’s decision not to undertake the “warm” transfer of calls to
other NHS sources of information. There are a number of reasons for this decision, including:
37• Warm transferred calls use two telephone lines at the original receiving site for the whole length of the
transferred call. This is known as “tromboning” and reduces the call handling capacity of the receiving site
• All calls received by NHS Direct arrive via BT’s advanced services platform (0808, 0845 etc.). For sound
technical reasons BT proscribes the transfer of these calls back through the advanced services platform i.e.
calls should not be transferred to another advanced service (0808, 0845 etc.) number
• Government requirements that state: “Where technology enables, all citizens [patients] must be dealt with
[supported] by the member of staff who first answers their call”
• It may not offer the patient the most efficient service, if the receiving service is busy
• There are significant resource implications in terms of time, staffing needs and additional telephony
infrastructure costs.
• There is currently no process for agreeing who is responsible for the cost of these outbound calls, for which
NHS Direct would be charged, and no mechanism for recovering the costs
Therefore, taking these issues into account, NHS Direct does not currently undertake “warm” call transfers. BMS call
handlers will, however, offer the patient any telephone numbers for further information that the Local Health Community
wishes to supply.
7.4 PROXY REFERRALS ON BEHALF OF A HEALTH PROFESSIONAL
Questions have been raised about the BMS undertaking proxy referrals on behalf of a health professional. There appear
to be several sets of circumstances when this may arise.
1. The GP generates the UBRN and password with the patient present but does not wish to take the
process any further in surgery time.
38In these circumstances, the BMS can accept the call to make a booking (not the appointment request)
but, equally, systems are already in place to enable other staff within GP Practices to carry out this work
on the basis of system permissions having been set by the GP
2. The GP has generated the UBRN and password, but wishes to dictate the referral letter over the phone to
a member of BMS staff.
The BMS will not accept this piece of work on the basis that BMS call handlers do not have the
appropriate level of skill. Additionally, complex processes would need to be in place for confirmation of
letter contents and the costs are likely to be disproportionately high.
3. The Choose and Book application may be unavailable. If the GP is not able to access the Choose and
Book application whilst the patient is present during the consultation, it has been suggested that it would
be helpful to be able to ring the BMS for the referral and booking to be “logged” for such time as the
system is again available. There may also be situations where the application is functioning but there is a
LAN or telephony problem for the GP Practice.
NHS Direct recognises that this facility would add value for GP Practices. However, as in 1. above, the
National Clinical Reference Panel has confirmed that the creation of appointment requests is out of scope
for the BMS due to the potential for clinical risk. Until there is a national resolution to this issue, the BMS
cannot accept these requests.
7.5 TUPE
Some Local Health Communities have asked whether NHS Direct would be prepared to accept the transfer of existing
non-NHS Direct call centre staff under TUPE arrangements. At the moment, this does not appear to be a universal issue,
given that many of the current processes undertaken by call centre staff in acute trusts and primary care will still be
39needed. However, changes in respective workloads resulting from the implementation of the Choice Policy Framework,
and the development of the Choose and Book software functionality mean that this may be a future discussion point.
There are some specific circumstances where it would be appropriate to have the discussions at an early stage:
• Where the Local Health Community has specific economic regeneration targets
• Where NHS Direct has chosen to deliver services from a site that “belongs” to a non-NHS Direct call
centre
• Where the local labour market conditions are adverse and NHS Direct would otherwise need to recruit
new staff, further damaging the market
Before discussions take place, the organisation wishing to transfer its staff will need to draw up a detailed migration plan,
including numbers and skill level of staff and proposals for timescales.
40GLOSSARY OF ABBREVIATIONS
Abbreviation Term
BMS Booking Management Service
DNA Did Not Attend
EA Early Adopter
GP General Practitioner
GwPSI General Practitioner with a Special Interest
ICT Information, Communications and Technology
LDP Local Delivery Plan
LHC Local Health Community
LSP Local Service Provider
NASP National Application Service Provider
NCRS National Integrated Care Record
NPfIT National Programme for Information Technology
PAS Patient Administration System
PCT Primary Care Trust
SHA Strategic Health Authority
41You can also read