Neonatal testing leading to the identification of Bh (para-Bombay) phenotype in the mother: case report with review of the literature - Exeley
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Case R ep ort
Neonatal testing leading to the identification
of Bh (para-Bombay) phenotype in the mother:
case report with review of the literature
G. Mohan, A. Vaidya, and S. Shastry
Para-Bombay is a rare phenotype with a homozygous nonfunc- case reports on the para-Bombay phenotype from India; what
tional FUT1 gene and a normal FUT2 gene leading to H-deficient makes this case unique is that we identified a para-Bombay
red blood cells (RBCs) with or without ABH substances,
phenotype in the mother because of her newborn’s blood type.
depending on inheritance of the ABO gene. This case is about a
5-day-old male baby suffering from sepsis who required a 45-mL
packed RBC transfusion. The baby’s sample tested as A1B, D+ and Case Report
mother’s sample tested as group O, D+ with group 4 discrepancy
due to ABO isoagglutinins. Further workup of the mother’s sample
with anti-H lectin was negative, which suggested the mother to be We received a request for 45-mL packed red blood cell
group Oh, D+. Antibody screening was panreactive with negative (PRBC) concentrate for a neonate on postnatal day 7 who
autocontrol, suggestive of anti-H. The titer of immunoglobulin was diagnosed with sepsis. The male baby was born after
(Ig)M anti-H was 64, IgG titer using dithiothreitol was 8, and anti-
a full-term normal delivery (weight 2300 g) at an outside
IH was absent. A negative adsorption and elution test suggested that
RBCs were devoid of A and B antigens. The father’s sample tested hospital and had been transferred to our center because of
clearly as group A1, D+; hence, the cis-AB blood group was ruled suspected sepsis, later confirmed as Klebsiella pneumoniae
out in the baby. The secretor study of the mother’s saliva revealed sepsis, on postnatal day 6. We performed blood grouping on
the presence of B and H substances that neutralized polyclonal B
AutoVue Innova (Ortho Clinical Diagnostics, Raritan, NJ)
and H antisera. Therefore, we concluded that the mother was of the
para-Bombay (Bh) phenotype. This case highlights the importance using column agglutination technology per departmental
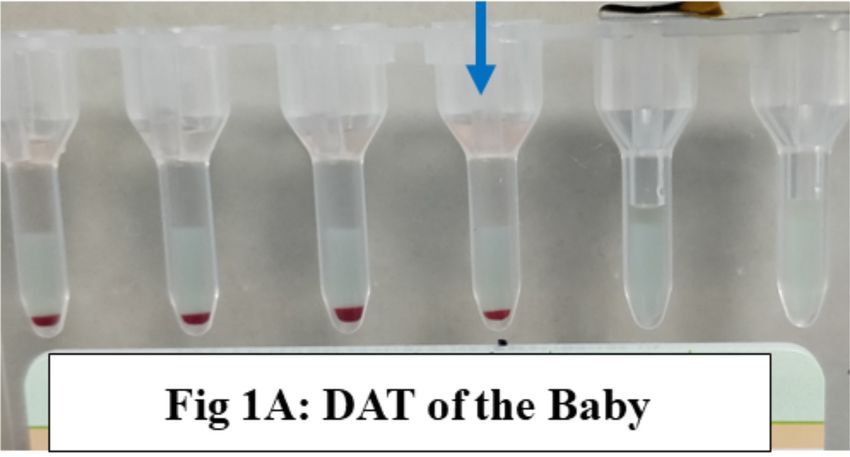
of reverse grouping and resolving blood grouping discrepancies standard protocol. The direct antiglobulin test (DAT) of the
between mother and child―in this case because of an incongruous baby (Fig. 1A) as well as the mother’s ABO grouping were
ABO blood type of the baby and the mother who was previously
tested as group O, D+. Immunohematology 2021;37:59–63. obtained (Table 1). The mother’s ABO grouping showed an
DOI:10.21307/immunohematology-2021-008. unexpected reaction in the pooled O RBC suspension on
serum testing, which led us to suspect a group 4 discrepancy
Key Words: blood groups, H antigen, anti-H, para-Bombay, (defined as an unexpected reaction in pooled RBCs because of
blood group discrepancy, secretor test, India ABO isoagglutinins or unexpected non-ABO alloantibodies),3
and hence anti-H lectin (Tulip Diagnostics, Goa, India)
The Bombay phenotype was identified in 1952 by as well as indirect agglutination testing was performed to
Bhende and colleagues.1 The Bombay phenotype results resolve the discrepancy. Antibody screening and identification
from a homozygous deficiency of the FUT1 gene along with showed panagglutination reactivity (Fig. 1B–D) with negative
a silenced mutation of the FUT2 gene. The incidence of the autocontrol (Bio-Rad, Hercules, CA); additional testing with
Bombay phenotype in the Indian population is approximately anti-H lectin was negative, thus implying the mother’s blood
1 in 10,000 and is most often due to a T725G mutation in the group/type to be Oh D+. The antibody reacted strongly with
FUT1 gene and a 10-kb deletion in the FUT2 gene.2 The para- cord group O RBCs (4+), similar to its reactivity with adult
Bombay phenotype is either due to a point mutation or a silence group O RBCs, thus ruling out anti-IH. However, we were not
mutation on the FUT1 gene with a normal FUT2 gene.2 As a able to perform a complete adsorption of the suspected anti-H
result, para-Bombay individuals have ABH substances in their and repeat the antibody identification to rule out other clinically
secretions and plasma (Type 1 precursor chain) depending significant antibodies due to the limited sample volume. Also,
on whether or not they inherit ABO genes. ABH substance in due to lack of H-deficient RBCs, we were not able to confirm
the plasma can be adsorbed onto the red blood cells (RBCs), the antibody specificity, thus concluding the antibody to be a
leading to a weak expression of ABH antigens. There are few ‘probable anti-H’. The antibody titer by serial dilution using
I M M U N O H E M ATO LO GY, Vo l u m e 37, N u m b e r 2, 2 0 21 59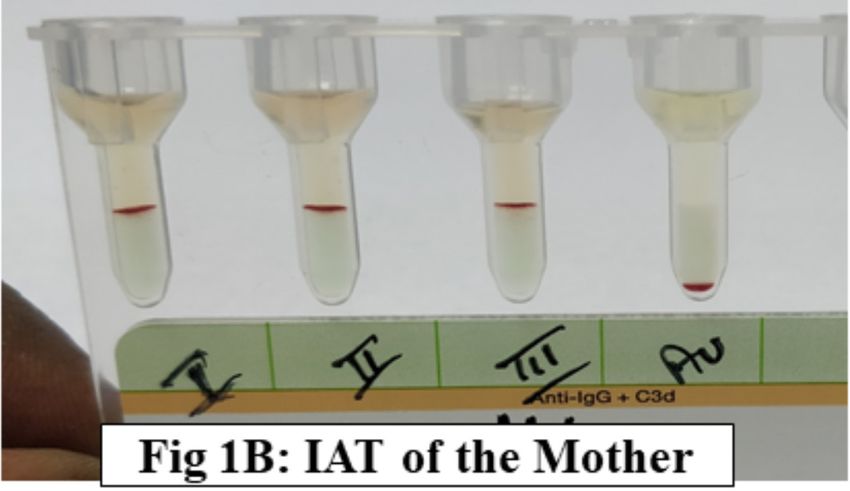
G. Mohan et al.
A B
D
C
Fig. 1 Direct antiglobulin test of the baby depicted by arrow (A); antibody screening (B) and identification (C, D) of the mother was performed
by the indirect antiglobulin test. Au = autocontrol; Ac = autocontrol.
conventional tube method showed 64 in immediate spin phase and hence we performed blood testing of the father—he was
(immunoglobulin [Ig]M) and 8 after dithiothreitol (DTT) group A1, D+ (Table 1). A thorough history from the parents
treatment of serum in the antihuman globulin (AHG) phase was obtained; this information ruled out in vitro fertilization/
using anti-IgG (Tulip Diagnostics). All workup was done after assisted reproductive methods and the possibility of another
obtaining informed consent from the parents. biological father. The other possibility was the mother being of
The mother was a primigravida; she had a normal vaginal the para-Bombay phenotype with offspring inheriting the ABO
delivery at 36 weeks of gestation with no history of previous gene. We collected saliva samples and performed the secretor
transfusions. Her sample was tested as group O, D+ in the test per the method given by AABB.4 The test revealed that the
referring hospital. Because the mother was Oh and baby was mother had B and H substances in her saliva that neutralized
A1B, we considered the possibility of a cis-AB blood group, polyclonal B and H antisera (Table 2). This finding was further
Table 1. Blood group testing results of the neonate, mother, and father
Anti-A Anti-A1 Anti-B Anti-A,B Anti-D1† Anti-D2† Anti-H A RBCs* B RBCs* O RBCs* Inference
Neonate +4 +4 +4 +4 +4 +4 +2 — — — A1B, D+
Mother 0 0 0 0 +4 +4 0 +4 +4 +4 ? Bombay
? AlloAb
Father +4 +4 0 +4 +4 +4 +4 0 +4 0 A1, D+
*Pooled red blood cell (RBC) suspensions, prepared in-house.
†
D1 and D2 denote D typing reagents from two different lots as per departmental standard operating procedure.
60 I M M U N O H E M ATO LO GY, Vo l u m e 37, N u m b e r 2, 2 0 21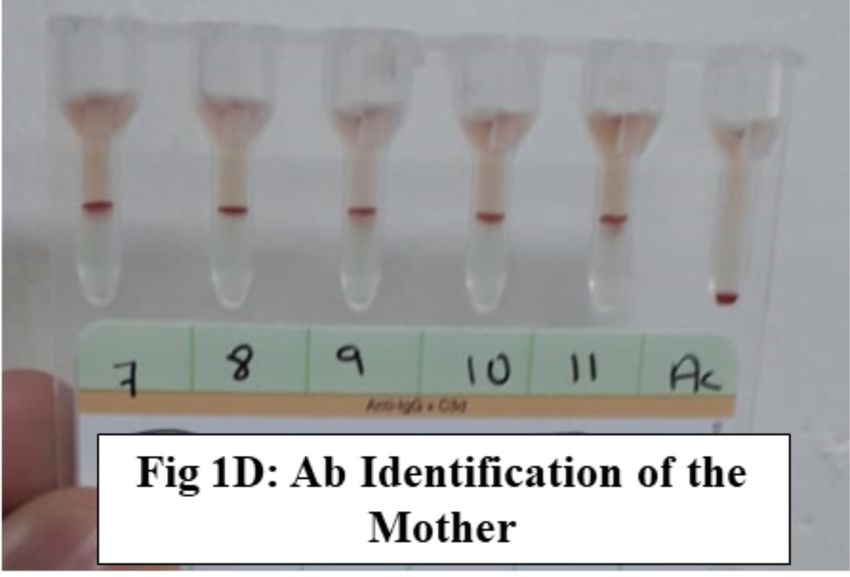
Probable anti-H in an H-deficient Bh para-Bombay mother
Table 2. Secretor status workup Discussion
Blood group/ Anti-A + Anti-B + Anti-H +
D type A RBCs* B RBCs* O RBCs* Interpretation The possible mechanisms of the para-Bombay phenotype
Known A, D+ 0 2+ 0 Group A are a mutated or a silenced FUT1 gene (H gene) with an active
secretor 1
FUT2 gene (secretor SE gene), resulting in expressing ABH
Known B, D+ 2+ 0 0 Group B
secretor 2 substances in secretions.2 These individuals are homozygous
Mother ? Oh, D+ 2+ 0 0 Bh para-Bombay
for a nonfunctional FUT1 gene. The common mutations
(patient) in FUT1 and FUT2 genes in a para-Bombay phenotype
Nonsecretor O, D+ 2+ 2+ 2+ Nonsecretor identified in recent years are summarized in Table 4. These
Saline NA 2+ 2+ 2+ No substances individuals may express weak ABH substances on their RBCs
*Pooled red blood cell (RBC) suspensions, prepared in-house. by adsorbing a Type 1 precursor chain from the plasma. The
NA = not applicable. negative results in the adsorption and elution in our case
suggested that the RBCs were devoid of antigen expression.
During the secretor status workup in this case, the anti-B and
supported by the Lewis phenotype of the mother, Le(a–b+), anti-H were neutralized by B and H substances, respectively,
which suggested that she is a secretor. These findings led to whereas anti-A was not inhibited. The immunohematologic
the determination of the mother to be an H-deficient secretor, workup concluded that the mother was an H-deficient secretor
probably Bh (para-Bombay), D+ phenotype. for B and H substances with probable anti-H, and she lacked
All the crossmatched PRBC units were incompatible antigen expression on RBCs, making a possible serologic
with the mother’s serum; hence, we crossmatched with the conclusion of the Bh para-Bombay secretor phenotype.
baby’s serum. A PRBC unit (group O, D+) that was ABO- Phenotyping the mother for Lewis antigens gave the result
compatible and AHG phase crossmatch–compatible with the of Le(a–b+), also revealing that the mother has the secretor
baby’s serum was issued, and the post-transfusion increase gene—because the Lewis phenotype of nonsecretors would
in hemoglobin and hematocrit was sufficiently achieved. be Le(a+b–), since they lack the Se allele needed for the
The laboratory parameters before and after transfusion are conversion of Type 1 precursor to Type 1H precursor, which is
provided in Table 3. The transfusion event was uneventful. then converted to Leb antigen by the LE gene.
The parents were counseled regarding the rare para-Bombay Anti-H found in a Bombay individual is a clinically
phenotype in the mother. significant antibody causing hemolytic transfusion reactions
Table 3. Laboratory parameters of the newborn
Parameters (normal lab range) Admission (PND 4) Before transfusion (PND 6) 24 hours after transfusion (PND 8)
Hemoglobin (14–22 g/dL) 11.4 9.8 11.1
Hematocrit (45–75%) 32.6 26 32.1
RBC count (5–7 × 10 /µL) 6
3.84 2.81 3.61
Reticulocyte (2–5%) 4.8 0.76 1.86
Reticulocyte absolute (0.02–0.11 × 10 /µL) 6
0.06 0.02 0.07
Platelet (100–400 × 103/µL) 151 118 138
Total leukocyte count (10–26 × 10 /µL) 3
4.5 14.6 15.5
Total bilirubin (≤8 mg/dL) 8.9 5.4 2.09
Direct bilirubin (0–0.6 mg/dL) 0.9 1.1 1.0
C-reactive protein (0–5 mg/L) 24.8 19.9 8.59
Peripheral smear Normocytic normochromic, Normocytic normochromic, Normocytic normochromic,
polychromasia, 2/100 nRBCs polychromasia polychromasia
pH 7.27 — —
sO2 (92–94%) 87 — —
PND = postnatal day; RBC = red blood cell; nRBCs = nucleated red blood cells; sO2 = saturated oxygen.
I M M U N O H E M ATO LO GY, Vo l u m e 37, N u m b e r 2, 2 0 21 61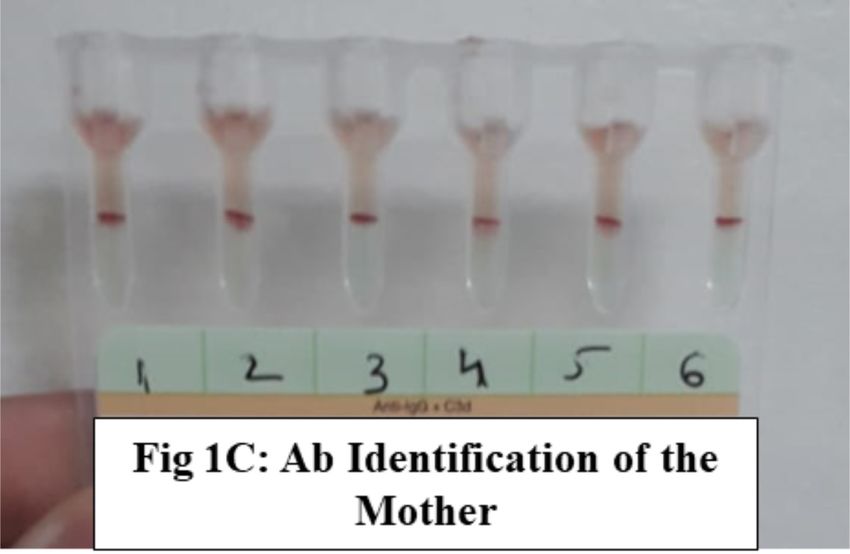
G. Mohan et al.
Table 4. Review of literature
Authors and year Country Cases (n) Blood group Mutation in FUT1 Mutation in FUT2
Xu et al., 2010
5
China 1 Bh 235C wild-type —
Cai et al., 2011
6
China 17 — 547delAG, 880delTT, c658T, Se 357, Se 357,716,
c649T, c35T, 423A Se 357,385
Luo et al.,7 2013 China 9 — 547delAG, 880delTT, C658T, Se 357, Se 357,716,
C35T, A980C Se 357,385
Lin et al.,8 2013 China 1 Bh 547delAG, 814A>G —
Townamchai et al.,9 2014 Taiwan 1 ABh NA —
Zhang et al.,10 2014 China 3 — 547delAG, 35C>T —
Zhang et al., 2015 11
China 7 — 547delAG, 880delTT, C658T, Se 357, Se 357,716,
C522A Se 357,385
Wang et al.,12 2017 China 1 Ah C958insG and c961G>A Se 357,385
Er et al., 2018
13
Taiwan 1 Ah 881delTT, 551delAG —
Song et al.,14 2018 China 1 Ah A328G and 58T —
Hong et al.,15 2018 China 1 ABh C49T>C —
Subrahmaniyan, 2018 16
India 1 ABh NA NA
Kim et al., 2019
17
South Korea 1 Ah c328G>A missense mutation c390>T
Lin et al.,18 2019 China 9 3 Ah and 6 Bh 547delAG, 814A>G, —
55G>Cc.755G>C
Lin and Er,19 2019 Taiwan 1 Ah 881delTT and c658T —
Patel et al.,20 2020 India 1 Ah NA NA
Matzhold et al., 2020 21
Austria 1 Aberrant Bh c551-552AG deletion —
MeSH search terms: para-Bombay, 2010–2020. NA = not applicable.
and hemolytic disease of the fetus and newborn (HDFN). It dominant B gene came from the mother—thus enabling him
is predominantly of the IgM type that reacts at 4–37°C and to express ABH substance on his RBCs. Because the family
agglutinates all reagent RBCs.22 Compared with the anti-H members refused any further testing, we could not perform
in the Bombay phenotype, anti-H found in para-Bombay is a the genotyping of the mother. The baby’s RBC testing (A1B,
weaker antibody with lower titers, whereas anti-IH, a complex D+) led to the identification of the mother, who was previously
antibody, is also found in rare hh individuals. In our case, typed as group O, D+, as para-Bombay (Bh, D+). This finding
the possibility of anti-IH was ruled out because of the strong highlights the importance of performing serologic grouping
reaction with cord group O RBCs. The baby did not have and investigating incongruous results, a basic step in any
laboratory findings characteristic of HDFN during the hospital immunohematology laboratory.
stay (Table 3). The IgM type of the antibody in the mother,
a weaker anti-H in para-Bombay individuals compared with References
Bombay individuals, and the fact that the baby’s sample tested
1. Bhende YM, et al. A “new” blood-group character related to the
as A1B (which has the least amount of H substance) played a ABO system. 1952. Natl Med J India 2008;21:264–6.
role in determining the clinical significance of this probable 2. Gorakshakar A, Donta A, Jadhav S, Vasanta K, Ghosh K.
anti-H and a lack of HDFN in the neonate.22,23 Para-Bombay Molecular analysis of Bombay phenotype cases seen in India.
Vox Sang 2015;10:100–5.
individuals can have anti-H, anti-IH, or both, as well as anti-A
3. Harmening DM, Manning BL. The ABO blood group system.
or anti-B depending on their ABO group.6 In: Modern blood banking and transfusion practices. 7th ed.
In this case, the father was group A, D+, meaning that Philadelphia, PA: F.A. Davis, 2018.
the father had at least one dominant A and H gene (AA/AO 4. Cohn SC, Delaney M, Johnson ST, Katz L, Eds. Method 2-8:
Testing saliva for A, B, H, Lea, and Leb antigens. In: AABB
and HH/Hh). The mother was identified as Bh, having at least
technical manual. 20th ed. Bethesda, MD: AABB, 2020.
one B gene (BB/BO and hh). The baby was A1B, D+, meaning
the A and H dominant genes came from the father and the
62 I M M U N O H E M ATO LO GY, Vo l u m e 37, N u m b e r 2, 2 0 21Probable anti-H in an H-deficient Bh para-Bombay mother
5. Xu X, Hong X, Liu Y, et al. Analysis of alpha-1,2-fucosyl- 17. Kim M, Kim JS, Park H, et al. The first case of para-Bombay
transferase gene mutations in a Chinese family with para- blood type encountered in a Korean tertiary hospital. J Korean
Bombay phenotype. Zhonghua Yi Xue Yi Chuan Xue Za Zhi Med Sci 2019;34:6–11.
2010;27:250–4. 18. Lin J, Chen R, Zhu S, Qiu X, Huang Y, Wang X. Sequence
6. Cai X, Jin S, Liu X, Fan L, Lu Q, Xiang D. Molecular genetic analysis of α-(1, 2)-fucosyltransferase gene in nine Chinese
analysis for the para-Bombay blood group revealing two novel individuals with para-Bombay phenotype. Gene 2019;685:
alleles in the FUT1 gene. Blood Transfus 2011;9:466–8. 21–3.
7. Luo G, Wei L, Wang Z, et al. The summary of FUT1 and FUT2 19. Lin C, Er T. Identification of a case with heterozygous mutations
genotyping analysis in Chinese para-Bombay individuals in the FUT1 gene leading to a para-Bombay phenotype. Clin
including additional nine probands from Guangzhou in China. Lab 2019;65.
Transfusion 2013;53:3224–9. 20. Patel JN, Donta AB, Patel AC, Pandya AN, Kulkarni SS. Para-
8. Lin J, Huang Y, Zhu S. Genetic analysis of an individual with Bombay phenotype: a case report from a tertiary care hospital
para-Bombay phenotype. Zhonghua Yi Xue Yi Chuan Xue Za from South Gujarat. Asian J Transfus Sci 2020;12:16–7.
Zhi 2013;30:165–7. 21. Matzhold E, Wagner T, Dexler C, Schonbacher M. Aberrant ABO
9. Townamchai N, Watanaboonyongcharoen P, Chancharoenthana B phenotype with irregular anti-B caused by a para-Bombay
W, Avihingsanon Y. A case of nearly mistaken AB para-Bombay FUT1 mutation. Transfus Medi Hemother 2020;47:94–7.
blood group donor transplanted to a group ‘O’ recipient. BMJ 22. Scharberg EA, Olsen C, Bugert P. The H blood group system.
Case Rep 2014:2014;bcr2014206374. Immunohematology 2016;32:112–8.
10. Zhang J, Zheng Y, Sun D. Formation of para-Bombay phenotype 23. Mak KH, Lubenko A, Greenwell P, Voak D, Yan K, Poole J.
caused by homozygous or heterozygous mutation of FUT1 Serologic characteristics of H-deficient phenotypes among
gene. Zhongguo Shi Yan Xue Ye Xue Za Zhi 2014;22:195–8. Chinese in Hong Kong. Transfusion 1996;36:994–9.
11. Zhang A, Chi Q, Ren B. Genomic analysis of para-Bombay
individuals in south-eastern China: the possibility of linkage
disequilibrium between FUT1 and FUT2. Blood Transfus Ganesh Mohan, MD (corresponding author), Associate Professor,
2015;13:472–7. Department of Immunohematology and Blood Transfusion, Kasturba
12. Wang L, Huang C, Wei Z, Tan J, Qin L, Tian L. Identification Medical College, Manipal, Manipal Academy of Higher Education,
of a novel FUT1 allele with two mutations in a Chinese para- Tiger Circle Road, Madhav Nagar, Manipal, Karnataka 576104,
Bombay individual. Transfusion 2017;57:93–6. India, ganesh.mohan@manipal.edu or drganeshmohan@gmail.
13. Er T, Yang T, Liu Y. Heterozygous FUT1 mutations causing a com; Ashwinkumar Vaidya, MBBS, Junior Resident, Department
para-Bombay phenotype. Clin Lab 2018;64:1787–9. of Immunohematology and Blood Transfusion, Kasturba Medical
14. Song M, Zhao S, Jiang T, Lu H. A very rare case with particular College, Manipal, Manipal Academy of Higher Education,
H-deficient phenotypes. Indian J Hematol Blood Transfus Karnataka, India; and Shamee Shastry, MD, Professor and Head,
2018;34:788–91. Available from https://doi.org/10.1007/ Department of Immunohematology and Blood Transfusion,
s12288-018-0915-3. Kasturba Medical College, Manipal, Manipal Academy of Higher
15. Hong X, Chen S, He J, Zhu F. c.49T>C mutation on the α-(1,2)- Education, Karnataka, India.
fucosyltransferase gene responsible for an individual with
para-Bombay phenotype. Transfusion 2018;58:1076–7.
16. Subramaniyan R. AB para-Bombay phenotype: a rare
blood group variant and its clinical significance. Hematol
Transfus Cell Ther 2018;40:96–7. Available from https://doi.
org/10.1016/j.htct.2017.11.003.
Notice to Readers Attention:
State Blood Bank Meeting Organizers
All articles published, including communications
and book reviews, reflect the opinions of the authors If you are planning a state meeting and would like copies of
and do not necessarily reflect the official policy of the Immunohematology for distribution, please send a request,
American Red Cross. 4 months in advance, to immuno@redcross.org.
I M M U N O H E M ATO LO GY, Vo l u m e 37, N u m b e r 2, 2 0 21 63You can also read