Mathematical Modeling of Epidemic Diseases; A Case Study of the COVID-19 Coronavirus - arXiv
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
DRAFT VERSION, SUBJECT TO MODIFICATION. FOLLOW THE UPDATES FROM: https://arxiv.org/abs/2003.11371 1
Mathematical Modeling of Epidemic Diseases; A
Case Study of the COVID-19 Coronavirus
Reza Sameni*
Grenoble, France
Revision: 19 May 2020
Abstract—The outbreak of the Coronavirus COVID-19 has shown by simulation, how social measures such as distancing,
taken the lives of several thousands worldwide and locked- regional lockdowns and public health vigilance, can influence
out many countries and regions, with yet unpredictable global the model parameters, which in turns change the mortality
arXiv:2003.11371v3 [q-bio.PE] 19 May 2020
consequences. In this research we study the epidemic patterns of
this virus, from a mathematical modeling perspective. The study rates and active contaminated cases over time.
is based on an extensions of the well-known susceptible-infected- It should be highlighted that mathematical models applied
recovered (SIR) family of compartmental models. It is shown to real-world systems (social, biological, economical, etc.) are
how social measures such as distancing, regional lockdowns, only valid under their assumptions and hypothesis. Therefore,
quarantine and global public health vigilance, influence the model
this research— and similar ones— that address epidemic pat-
parameters, which can eventually change the mortality rates and
active contaminated cases over time, in the real world. As with all terns, do not convey direct clinical information and dangers for
mathematical models, the predictive ability of the model is limited the public, but should rather be used by healthcare strategists
by the accuracy of the available data and to the so-called level of for better planning and decision making. Hence, the study of
abstraction used for modeling the problem. In order to provide this work is only recommended for researchers familiar with
the broader audience of researchers a better understanding of
the strength points and limitations of mathematical modeling
spreading patterns of epidemic diseases, a short introduction on
biological systems modeling is also presented and the Matlab of biological systems. The Matlab codes required for repro-
source codes for the simulations are provided online. ducing the results of this research are also online available in
the Git repository of the project [7].
In Section II, a brief introduction to mathematical modeling
I. I NTRODUCTION of biological systems is presented, to highlight the scope of
Since the outbreak of the Coronavirus COVID-19 in January the present study and to open perspectives for the interested
2020, the virus has affected most countries and taken the lives researchers, who may be less familiar with the context. The
of several thousands of people worldwide. By March 2020, proposed model for the outspread of the Coronavirus is
the World Health Organization (WHO) declared the situation a presented in Section III. The article is concluded with some
pandemic, the first of its kind in our generation. To date, many general remarks and future perspectives.
countries and regions have been locked-down and applied
strict social distancing measures to stop the virus propagation. II. A N INTRODUCTION MATHEMATICAL EPIDEMIOLOGY
From a strategic and healthcare management perspective, the AND COMPARTMENTAL MODELING
propagation pattern of the disease and the prediction of its
spread over time is of great importance, to save lives and to A. Mathematical modeling
minimize the social and economic consequences of the disease. A model is an entity that resembles a system or object in
Within the scientific community, the problem of interest has certain aspects, but is easier to work with as compared to the
been studied in various communities including mathematical original system. Models are used for the 1) identification and
epidemiology [1], [2], biological systems modeling [3], [4], better understanding of systems, 2) simulation of a system’s
signal processing [5] and control engineering [6]. behavior, 3) prediction of its future behavior, and ultimately
In this study, epidemic outbreaks are studied from 4) system control. Apparently, from item 1 to 4, the problem
an interdisciplinary perspective, by using an extension of becomes more difficult and although the ultimate objective is
the susceptible-exposed-infected-recovered (SEIR) model [2], to harness or control a system, this objective is not necessarily
which is a mathematical compartmental model based on the achievable. While modeling is the first and most important step
average behavior of a population under study. The objective in this path, it is highly challenging and nontrivial. The various
is to provide researchers a better understanding of the signif- issues that one faces in this regard, include:
icance of mathematical modeling for epidemic diseases. It is
• Models are not unique and different models can co-exist for
* R. Sameni is Associate Professor of Biomedical Engineering at School of a single system.
Electrical & Computer Engineering, Shiraz University, Shiraz, Iran, currently • A model is only a slice of reality and all models have a
on sabbatical leave as a visiting researcher at GIPSA-lab, Université Grenoble scope, outside of which, they are invalid.
Alpes, CNRS, Grenoble INP, 38000 Grenoble, France and a member of the
SEEPIA (Simulation & Estimation of Epidemics with Algorithms) project • Modeling can be done in different levels of abstraction,
working group (e-mail: reza.sameni@gmail.com). which corresponds to the level of simplification and theDRAFT VERSION, SUBJECT TO MODIFICATION. FOLLOW THE UPDATES FROM: https://arxiv.org/abs/2003.11371 2
specific aspects of the system that are considered by the exponentially spreads among the population, the infected
model. population tend to encounter each other and repeated healthy
ones (the healthy individuals already contacted by another
Example 1. The response of global stock markets with numer-
infected person). Hence, the stochastic model of infection
ous economic, political, industrial, social and psychological
propagation, somehow saturates1 . The probabilistic models
factors, to a high impact news can in cases be modeled with
used for modeling such epidemic spread are commonly based
a second-order differential equation, with a step-like over-
on the branching process and a Poisson distributions for the
damped behavior that reaches its steady state after a while.
probability of contact between infectious and healthy subjects.
Or in medicine, the response of the human body— with more
The stochastic perspective to epidemic modeling has been
that thirty-seven trillion cells— to medication can in many
extensively studied in the literature [2], [11]–[13]. Herein, we
cases be “resonably” modeled with a first order differential
adopt a more heuristic approach for model formation, which
equation.
is less rigorous, but is equally accurate in large populations
While various types of models are used for biological sys- (refer to the above references for the justification).
tems, we are commonly interested in mathematical models [8], Suppose that x(t) denotes the number of infected indi-
as they permit the prediction and possible control of biological viduals of a population at time t. Next, assuming that the
systems. In choosing among different available models, the chance of infection increases with the number of infected
widely accepted principle is the model parsimony, which sim- individuals, we assume that the variations in the population
ply means that “a model should be as simple as possible and of the number of infected between time t and t + ∆ (over
as complex as necessary!”. The model parsimony, is also an relatively small intervals ∆) is proportional to the number of
important factor for estimating the unknown model parameters infected individuals, i.e.,
using real data. A more accurate model with fewer number dx(t) x(t + ∆) − x(t)
of parameters is evidently preferred over a less accurate and ≈ = φ(t)x(t) (1)
dt ∆
more complex model. But how should one select between
Let us name φ(t) the reproduction function, which models
a more accurate complex model and a less accurate simpler
how the infected population evolves over time. This function
one? Measures such as the Akaike information criterion (AIC),
accounts for the expectation of various probabilistic factors,
the Bayesian information criterion (BIC) and the minimum
such as the rate of infection transmission, population density
description length (MDL), address the balance between the
and contact patterns. Note that although the x(t) on the right
number of observations and the model unknown parameters
hand side of (1) could have been unified in φ(t), the above
to select between competing models with variable number of
form has the advantages that φ(t) can be interpreted as the
parameters and different levels of accuracy [9], [10]. Finally,
exponential rate, with inverse time units.
the physical interpretability of the model parameters and the ∆
ability to estimate the parameters such that the model matches Denoting the kth generation of the infection spread by xk =
real-world data, is what makes the whole modeling framework x(k∆), (1) can be discretized as follows:
meaningful. xk+1 = [1 + ∆φ(k∆)]xk
∆
Now, defining the reproduction number rk = [1 + ∆φ(k∆)],
B. From stochastic infection propagation models to ordinary it is evident that the population at the discretized time index
differential (difference) equation modeling k can be recursively found from the initial condition x0 :
The outbreak of a contagious disease in a large population
xk = (rk−1 rk−2 · · · r0 )x0 (2)
is a stochastic event. Starting from a single infected individual,
the infection is transmitted to others in a stochastic manner, Apparently, if for all k, rk < 1 (or equivalently φ(t) < 0),
either by direct contact, proximity, or environmental traces (in- the infection would decay to zero; otherwise if rk > 1 (or
fected objects left over in the environment). The new infected φ(t) > 0) it spreads. In the simplest case, for which the
generation in turns transmits the infection (again probabilisti- reproduction function is a constant φ(t) = λ, we have a
cally) to the healthy individuals that they meet or encounter. constant reproduction number R0 = 1 + λ∆, resulting in an
During the primary stages of an epidemic outbreak, healthy- exponential growth/decay:
infected individual encounters are statistically independent. As
xk = x0 Rk0 , (3)
a result, the chance of multiple infected people meeting a
single healthy individual is probabilistically low. Therefore, or in the continuous case:
assuming that each infected individual contaminates R0 new
people on average (known as the reproduction number, more x(t) = x(0)eλt (4)
rigorously defined in Section II-E), if R0 > 1 the disease The equivalence of the discrete and continuous solutions is
spreads exponentially from one time step to another (for evident up to the first order approximation of the derivative,
example on a daily basis). However, in a finite population, as assumed in (1).
the exponential growth can not continue for ever. Depending
1 Another interpretation is that after a while, it becomes more and more
on the population size and contact patterns, the probability
difficult for the average infected person to meet R0 non-infected individuals,
of infected people encountering independent healthy indi- and therefore the reproduction number drops and the number of new infections
viduals decreases. Therefore, after the initial outbreak that decreases exponentially.DRAFT VERSION, SUBJECT TO MODIFICATION. FOLLOW THE UPDATES FROM: https://arxiv.org/abs/2003.11371 3
More generally, the reproduction function φ(t) (or rk in Compartmental modeling is also known as mass transport
the discrete case) can be a time-varying function of factors [15], or mass action [16], in other contexts. More technically, a
such as the total susceptible population, the population of compartmental model is a weighted directed graph represen-
the exposed individuals (carriers of the disease but without tation of a dynamic system. Each compartment corresponds
symptoms), contact patterns, and countermeasures such as to a node of the graph and the linking arrows are the graph
social distancing and lockdowns. As shown in the sequel, edges. From this perspective, for an n compartment system,
the notion of reproduction function (number) and its impact the compartment variables can be considered as state variables
on epidemic outbreak generalizes to eigen-analysis of vector- denoted in vector form as x(t) = [x1 (t), . . . , xn (t)]T . The
valued dynamic epidemic models (when the population is compartmental model provides a graphical representation of
divided into multiple groups of individuals known compart- the state-space model:
ments), enabling the stability analysis of such models.
As a reminder for later use, when λ < 0, the exponential ẋ(t) = f (x(t), w(t); θ(t), t)
(5)
law in (4) implies that the population of the infected cases y(t) = g(x(t); θ(t), t) + v(t)
drops 63%, 86%, 95%, 98%, 99%, and 99.75% from its initial where f (·) is the state dynamics function corresponding to
value, after λ−1 , 2λ−1 , 3λ−1 , 4λ−1 , 5λ−1 , and 6λ−1 time the compartmental model graph (which can be possibly time-
units, respectively. The latter indicates for example that after variant and nonlinear), w(t) = [w1 (t), . . . , wl (t)]T represents
6λ−1 time units, only 25 cases out of 10,000 would still be deterministic or stochastic external system inputs, y(t) =
infected. This property is later used to estimate the model [y1 (t), . . . , ym (t)]T is the vector of observable model vari-
parameters from clinical experimental results. It is good to note ables considered as outputs (the measurements), g(·) if the
that although the exponential law for infection spread is the function that maps the state variables to the observations
most common assumption, depending on the application, more (measurements), v(t) = [v1 (t), . . . , vm (t)]T is the vector of
accurate non-exponential models have also been considered measurement inaccuracies, considered as additive noise and
[14]. θ(t) = [θ1 (t), . . . , θp (t)]T is a vector of model parameters
to be set or identified. Researchers familiar with estimation
C. Compartmental modeling theory, have already guessed that the state-space form of
(5), implies that one may eventually be able to estimate and
Differential (difference) equations arise in many modeling
predict the compartment variables from noisy measurements,
problems. The major application of these equations is when
using state-space estimation techniques, such as the Kalman
the rate of change of a variable is related to other variables,
or extended Kalman filter [17].
as it is so in most physical and biological systems. Many
With this background, the basic steps of compartmental
powerful mathematical tools exist for the analysis and (nu-
modeling are:
merical) solution of models based on differential equations.
Despite their vast applications, differential equations are dif- 1) Identifying the quantities of interest as distinct compart-
ficult to conceive and interpret without visualization. In this ments and selecting a variable for each quantity as a
context, compartmental models are used as a visual means function of time. These variables are the state variables
of representing differential equations of dynamic systems. A of the resulting state-space equations.
compartment is an abstract entity representing the quantity 2) Linking the compartments with arrows indicating the rate
of interest (volume, number, density, etc.). Depending on the of quantity flow from each compartment to another (visu-
level of abstraction, each of the variables of interest (equivalent ally denoted over the arrows connecting the compartments).
to system states in dynamic systems) are represented by 3) Writing the corresponding first-order (linear or nonlinear)
a single compartment, conceptually represented by a box. differential equations for each of the state variables of the
Each compartment is assumed to be internally homogeneous, model. In writing the equations from the graph represen-
which implies that all entities assumed inside the compartment tation, the edge weights multiplied by the state variable
are indistinguishable. For example, depending on the model of their start node are added to (subtracted from) the rate
complexity selected for modeling a certain epidemic disease, change equation of the end node (start node). External
men and women at risk can be assumed to conform a single inputs can be considered to be originated from an external
compartment, or may alternatively be considered as different node with value 1.
compartments. A similar partitioning may be considered for 4) Setting initial conditions and solving the system of equa-
different age groups, ethnicities, countries, etc., at a cost of a tions (either analytically or numerically), which is in the
more complex (less parsimonious) model with additional states form of a first-order state-space model.
and parameters to be identified. Apparently, the available real- A compartmental model is linear (nonlinear), when its rate
world data may be insufficient for the parameter identification flow factors are independent (dependent) of the state variables.
of a more detailed (complex) model. A compartmental model is time-invariant (time-variant), when
The compartments interact with one another through a set its rate flow factors are independent (dependent) of time. Com-
of rate equations, visually represented by arrows between partmental models may be open or closed. In closed systems,
the compartments. Therefore, compartmental models can be the quantities are only passed between the compartments,
converted to a set of first order linear or nonlinear equations while in open systems the quantities may flow into or out
(and vice versa), by writing the net flow into a compartment. of the whole system. In a closed compartmental model, theDRAFT VERSION, SUBJECT TO MODIFICATION. FOLLOW THE UPDATES FROM: https://arxiv.org/abs/2003.11371 4
γ
γx
u ρ
x z s i r
α β αi β
y
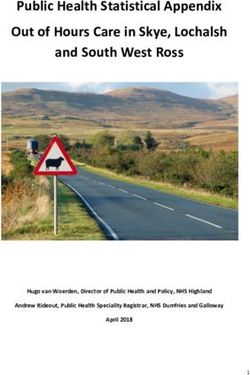
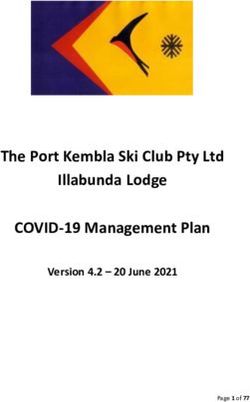
Fig. 2. The basic susceptible-infected-recovered (SIR) model
Fig. 1. A sample compartmental model corresponding to the set of dynamic
equations in (6)
in fact the fraction of each group’s population divided by N ).
Accordingly, the system is closed and we have
sum of all the differential equations of the system is zero (for
all t). s(t) + i(t) + r(t) = 1 (7)
Example 2. A three compartment model corresponding to the A compartmental model for the propagation of the disease is
following set of equations is shown in Fig. 1. shown in Fig. 2. The compartmental representation of Fig. 2
dx(t) is equivalent to the following set of differential equations:
= u − γx(t)2 − αx(t)
dt ds(t)
dy(t) = −αs(t)i(t) + γr(t)
= αx(t) − βy(t) (6) dt
dt
dz(t) di(t)
= γx(t)2 + βy(t) − ρz(t) = αs(t)i(t) − βi(t) (8)
dt dt
which can be put in the matrix form of (5). Due to the state- dr(t)
= βi(t) − γr(t)
dependency of the rate flow between x and z, the model is dt
nonlinear. It is also an open system, since the sum of rate Accordingly, moving from the susceptible group to the in-
changes is non-zero, i.e., there is net flow in and out of the fected group takes place at a rate that is proportional to the
whole system (due to u and ρ). population of the infected and susceptible groups, with pa-
rameter α. At the same time, infected individuals are assumed
D. Mathematical epidemiology to recover at a constant rate of β. Finally, considering that
In order to model the propagation of epidemic diseases in a the disease is not assumed to result in lifetime immunity
population, certain disease- and population-specific assump- of the subjects, the recovered individuals again return to the
tions are required. The most common assumptions in this susceptible group at a fixed rate of γ. From (8), it is evident
context include: that
ds(t) di(t) dr(t)
• The diseases are contagious and transfer via contact. + + =0 (9)
• A disease may or may not be fatal.
dt dt dt
• There may be births during the period of study, and the which is in accordance with (7) and the fact that the system
birth may (or may not) be congenitally transferred from the is assumed to be closed (no births or deaths have been
mother to the baby. considered).
• The disease can have an exposure period, during which the Assuming initial conditions for each group, the set of
contaminants carry and spread the disease, but do not have nonlinear equations (8) can be (numerically) solved to find the
visible symptoms. evolution of the population of each compartment over time.
• Catching the disease may or may not result in short-term or The numerical solution of a basic (non-fatal) SIR model is
long-term immunity. Depending on the case, the recovered shown in Fig. 3, with and without lifetime immunity. The time-
patients can again become susceptible to the disease. step for numerical discretizing of the differential equations of
• Interventions such as medication, vaccination, lockdown, this simulation has been chosen to be ∆=0.1 of a day. Notice
quarantine and social distancing can change the pattern of how the outbreak of a disease that does not cause lifetime
propagation. immunity (such as a typical flu), can result in a constant
Let us consider an example, which is the basic model that we rate of illness throughout time, after its transient period. For
later extend for the COVIC-19 virus propagation pattern. widespread epidemic diseases, the healthcare strategists are in-
1) The susceptible-infected-recovered model: A basic terested in the slopes of s(t), i(t) and r(t), rather than the total
model used for modeling epidemic diseases without lifetime number of infected individuals (as it is currently the case for
immunity is known as the susceptible-infected-recovered (SIR) the COVID-19 Coronavirus). The prolongation of the disease
model [2], [18], [19]. In this model, the total population of spread provides the better management of healthcare resources
N individuals exposed to an epidemic disease at each time such as hospitalization, medication, healthcare personnel, etc.
instant t is divided into three groups (each represented by a
compartment): the susceptible group fraction denoted by s(t), For later reference, it is interesting to study the fixed-point
the infected group fraction denoted by i(t), and the recovered of the SIR model (where ṡ(t) = i̇(t) = ṙ(t) = 0). Equating
group fraction denoted by r(t) (the compartment variables are the left sides of (8) with zero, it can be algebraically shownDRAFT VERSION, SUBJECT TO MODIFICATION. FOLLOW THE UPDATES FROM: https://arxiv.org/abs/2003.11371 5
replacing the perturbed point in (8) and neglecting second and
1
S(t) higher order terms containing ǫ, we obtain:
I(t)
0.8 R(t)
ds(t)
= −α(1 − ǫ)ǫ ≈ −αǫ < 0
Population Ratio
dt
0.6 di(t)
= α(1 − ǫ)ǫ − βǫ ≈ (α − β)ǫ (12)
dt
0.4 dr(t)
= βǫ > 0
dt
0.2
As a result, the first fixed-point is unstable, since due to the
sign of the derivatives of the perturbed system, the system’s
0
0 50 100 150 dynamics drives the state vector away from the fixed-point
days (since the population of the susceptible group has a negative
(a) Basic SIR with immunity derivative). However, depending on whether α > β or not, the
outbreak may or may not result in an increase in the infected
1 population. Simply put, if the infection rate is greater than
S(t)
I(t)
the recovery rate (α > β) the disease would lead into an
0.8 R(t) outspread; but if the recovery rate is faster than the infection
Population Ratio
rate (α < β) the percentage of the infected population
0.6 will remain close to zero. In either case, for a non-fatal
non-immunizing disease, all individuals that become infected
0.4 recover after a while and move to the recovered group and
again go back to the susceptible group at a rate of γ. Note
0.2 that a SIR model with a non-zero infected population fraction
in steady-state, indicates that there is a constant flow between
0
0 50 100 150 the compartments, i.e., people are constantly contaminated,
days recovered and again become susceptible to the disease.
(b) Basic SIR without immunity
Perturbing the second fixed-point results in
ds(t) β
Fig. 3. Simulation of a basic non-fatal SIR model with α=0.5 and β=0.05 = −α( − ǫ)(I0 + ǫ) + βI0 ≈ ǫ(αI0 − β)
in two cases: a) γ=0.0 (lifetime immunity) and b) γ=0.04 dt α
di(t) β
= α( − ǫ)(I0 + ǫ) − βI0 ≈ −ǫ(αI0 − β) (13)
dt α
that if α, γ 6= 0 (the non-immunizing case), the SIR model dr(t)
= β(I0 + ǫ) − β(I0 + ǫ) = 0
has only two fixed-points: dt
In this case, depending on whether (αI0 − β) > 0 or not, the
(s∗ (t), i∗ (t), r∗ (t)) = (1, 0, 0) fixed-point may be stable or unstable.
β β (10) For later use, we can show that during the outbreak of the
(s∗ (t), i∗ (t), r∗ (t)) = ( , I0 , I0 )
α γ SIR model (s(t) ≈ 1), the number of infected cases follows
an exponential pattern:
γ(α − β) ∆
where I0 = . The first fixed-point corresponds to the i(t) ≈ i(0) exp[(α − β)t] (14)
α(γ + β)
lack of any infected cases, and the second corresponds to a
2) The fatal SIR model: A fatal version of the SIR model
persistent disease in the population, as illustrated in Fig. 3(b).
with rates of birth µ∗ and with different death rates from the
This situation is only reachable if β < α, i.e., when the
susceptible (µs ), infected (µi ) and recovered (µr ) groups is
infection rate is greater than the recovery rate.
shown in Fig. 4. This system is no longer closed and its state
We can also verify whether or not the fixed-points are
equations can be written as follows:
stable. Various methods can be used for this purpose. Perhaps,
the most tangible approach is based on perturbation theory. ds(t)
= γr(t) − αs(t)i(t) − µs s(t) + µ∗
Simply stated, one can add small perturbations to the fixed- dt
points of the system and check whether or not the perturbations di(t)
= αs(t)i(t) − βi(t) − µi i(t) (15)
are compensated by the system’s dynamics by pushing the dt
state vector back to its fixed-point. Accordingly, the first fixed- dr(t)
= βi(t) − γr(t) − µr r(t)
point in (10) can be perturbed to: dt
(s(t), i(t), r(t)) = (1 − ǫ, ǫ, 0) (11)
E. The basic reproduction number (R0)
where 0 < ǫ ≪ 1 is a small perturbation (e.g., equivalent to As noted before, the outbreak threshold of epidemiology
a single case of disease outbreak in a large population). Now models is known as the basic reproduction number R0 . It isDRAFT VERSION, SUBJECT TO MODIFICATION. FOLLOW THE UPDATES FROM: https://arxiv.org/abs/2003.11371 6
γ Example 3. In the SIR model (8), if we replace r(t) = 1 −
µ∗ s(t) − i(t) from (7), the model reduces to:
αi β
s i r di(t)
= αs(t)i(t) − βi(t)
µs µi µr dt (20)
ds(t)
= −αs(t)i(t) + γ[1 − s(t) − i(t)]
Fig. 4. The susceptible-infected-recovered (SIR) model with birth and death dt
rates Therefore,
αs(t)i(t) −βi(t)
F= , V=
defined as the average number of secondary infections due 0 −αs(t)i(t) + γ[1 − s(t) − i(t)]
to an infected individual hosted by a completely susceptible (21)
population [20]–[22], [1, Ch. 7]. The R0 during epidemic and at the fixed-point x = (0, 1)
outbreak is generally greater than the average infections (R)
αs(t) αi(t)
at any other time other than the outbreak. ∇x F (x∗ ) =
0 0 i(t)=0,s(t)=1
From the mathematical modeling perspective, a formal
−β 0
definition of R0 was first presented in [23]. Consider the ∇x V(x ) =
∗
−αs(t) − γ −αi(t) − γ i(t)=0,s(t)=1
general dynamic representation of a compartmental model: (22)
which results in the reproduction number:
ẋ(t) = f (x(t)) (16)
α
R0 = ρ(−FV−1 ) = (23)
where x(t) = [x1 (t), x2 (t), . . . , xp (t), xp+1 (t), . . . , xn (t)]T β
is the state vector (compartment variables), such that where we can see that the epidemic stability condition R0 < 1
x1 (t), . . . , xp (t) correspond to the infected compartments (ex- is identical to the stability condition α < β, found for the SIR
posed, infected, etc.), and xp+1 (t), . . . , xn (t) are all the other model in Section II-D1.
variables (susceptibles, recovered, passed-away, etc.). We next
partition each row of f (·) as follows: Comparing (23) and (14) we notice that although the
epidemic stability condition found from R0 is related to the
f (x(t)) = F (x(t)) + V(x(t)) (17) outbreak exponent (slope of infection during outbreak), but
they are not the same quantities.
where F (·) groups all the terms of f (x(t)), which correspond In fact, a major drawback of the conventional definition
to new infections (the portion of the population, which are of R0 using the NGM is that the discretization time (or
either susceptible or had fully recovered, but are becoming generation period) is discarded in its definition and therefore,
exposed or infected due to contact with the exposed or there is no direct analogy between the discrete-time and
infected). On the other hand, V(·) groups all the other terms continuous-time outbreak behavior of the epidemic. Motivated
of the equations, including removals from the infected groups by this fact and based on the analogy between the discrete-
and other compartmental transitions. time and continuous-time models presented in Section II-B,
The Jacobian of F (·) and V(·) are next calculated at the no we hereby propose an alternative definition of the reproduction
infection fixed-point x∗ = [0, 0, . . . , 0, x∗p+1 , . . . , x∗n ]T : number:
Proposition: An alternative definition of the repro-
F 0 V 0 duction number is
∇x F (x ) =
∗
, ∇x V(x∗ ) = (18)
0 0 J3 J4
R̃0 = eλ1 ∆ (24)
Finally, the reproduction number is defined as the spectral where λ1 is the real-part of the dominant eigenvalue
radius (leading eigenvalue) of the negative of the so-called of the dynamic model’s Jacobian evaluated at the
next generation matrix (NGM) FV−1 : fixed-point of interest, and ∆ is the generation time
unit (or discretization period). Accordingly, for an
R0 = ρ(−FV−1 ) (19) irreducible dynamic model, R̃0 < 1 (or λ1 < 0)
and R̃0 > 1 (or λ1 > 0) correspond to stable and
which is proved to have the biological properties of the
unstable epidemic conditions, respectively.
reproduction number for epidemic studies.
In fact, while the threshold between stability and instability It is clear that for small generation time units ∆ (small as
of an epidemic can be defined in various forms, only the compared with the compartmental model “rate of variations”
definition based on R0 is biologically popular [22]. In [23], in time), we have:
it is also shown how different partitionings of the state-space R̃0 ≈ 1 + λ1 ∆ (25)
model can lead to different spectral radii; however, only the
choice described in (17) leads to the biologically meaningful The major advantage of the above definition for the reproduc-
definition of R0 . tion number is that the time unit between generations appears
in the definition. Therefore, the R̃0 of different epidemics thatDRAFT VERSION, SUBJECT TO MODIFICATION. FOLLOW THE UPDATES FROM: https://arxiv.org/abs/2003.11371 7
s γ
have been experimentally obtained from real-world data ac- ρ
quired with different generation time units become comparable αe e + αi i
with one another. Moreover, our studies on various epidemic κ β
e i r
models shows that the stability condition λ1 < 0 (or R̃0 < 1)
is exactly equivalent to the R0 < 1 condition obtained from µ
the common definition of the basic reproduction number using p
the NGM. The mathematical proof of equivalence of the two
conditions remains as future work. Fig. 5. Proposed Model I: the fatal susceptible-exposed-infected-recovered
(SEIR) model for Coronavirus modeling with a unique recovery group
III. P ROPOSED E PIDEMIC M ODEL I
Many infectious diseases are characterized by an incuba- In (27), similar to the classical SIR model, the interpretation
tion period between exposure and the outbreak of clinical of the nonlinear terms including s(t)e(t) and s(t)i(t) is that
symptoms. Subjects exposed to the infection are much more the rate of exposure to the virus is proportional the population
dangerous for the public as compared to the subjects showing of both the susceptible and exposed/infected subjects.
clinical symptoms. The condition becomes more and more Note that the system closure constraint (26) gives an excess
dangerous, with the increase of the isncubation rate. A well- degree of freedom, which can be used to reduce the model
known case is the HIV virus in its clinical latency stage. order by replacing s(t) = 1 − e(t) − i(t) − r(t) − p(t). This
The experience of the COVID-19 shows that a two-week simplifies the compartmental model as follows:
incubation period can spread a virus worldwide and almost de(t)
at any level of the society. Remember that any two of us = [1 − e(t) − i(t) − r(t) − p(t)][αe e(t) + αi i(t)]
dt
are only six handshakes apart!2 For this reason, an additional − κe(t) − ρe(t)
compartment is added between the susceptibility and infection di(t)
stages of the SIR model, which accounts for the asymptomatic = κe(t) − βi(t) − µi(t)
dt
exposed subjects. Moreover, since we are also interested in dr(t)
minimizing the mortality rate of the disease, a termination = βi(t) + ρe(t) − γr(t)
dt
compartment is dedicated to the passed-away population. The dp(t)
variables of the model are therefore: = µi(t)
dt
1) s(t): The susceptible population fraction (the number of (28)
individuals in danger of being infected, divided by the total
population). A. Measurements model
2) e(t): The exposed population fraction (the number of indi- Among the state variables of the proposed model, all
viduals exposed to the virus but without having symptoms, except e(t) are directly measurable (with potential errors). The
divided by the total population). measurements can be formulated in matrix form as follows:
3) i(t): The infected population fraction (the number of
e(t)
infected individuals with symptoms, divided by the total
I(t) 0 1 0 0 i(t) vi (t)
population).
R(t) = 0 0 1 0 + vr (t) (29)
4) r(t): The recovered population fraction (the number of r(t)
P (t) 0 0 0 1 vp (t)
recovered individuals, divided by the total population). p(t)
5) p(t): The number of individuals that pass away due to the
disease, divided by the total population). where I(t) is the fraction of reported infections, R(t) is
the fraction of reported recoveries (both symptomatic and
Keeping in mind that
asymptomatic), P (t) is the fraction of reported death tolls,
s(t) + e(t) + i(t) + r(t) + p(t) = 1 (26) and v(t) = [vi (t), vr (t), vp (t)]T is measurement noise. The
evident sources of measurement noises include: unavailable
the proposed model and its compartmental representation are information regrading the exact population, intentional and
shown in equations (27) and Fig. 5. unintentional misreported values, mis-classified reasons of
death (especially for the elderly or subjects suffering from
Model I: multiple health issues), and the marginal cases that may be
ds(t) unknown or misclassified for the healthcare system. Equation
= −αe s(t)e(t) − αi s(t)i(t) + γr(t)
dt (29) can be written in more compact form as follows:
de(t)
= αe s(t)e(t) + αi s(t)i(t) − κe(t) − ρe(t) y(t) = Cx(t) + v(t) (30)
dt
di(t) (27)
= κe(t) − βi(t) − µi(t) where x(t) = [e(t), i(t), r(t), p(t)]T is the reduced state-
dt
dr(t) vector. Although the variable e(t) is not directly measurable
= βi(t) + ρe(t) − γr(t)
dt from the available public data, we will show in Section V
dp(t)
= µi(t) 2 Cf. https://en.wikipedia.org/wiki/Six degrees of separation
dtDRAFT VERSION, SUBJECT TO MODIFICATION. FOLLOW THE UPDATES FROM: https://arxiv.org/abs/2003.11371 8
that under certain conditions, e(t) can be estimated from the noted 99.75% percentage as the target infection drop-out
measurements. threshold, and advised 14 days of quarantine for the whole
Note that in the above measurement model, it is assumed population. In that case, we can select κ = 6/14 = 0.43
that R(t) is the total recovery fraction of both the symptomatic (inverse days) in our model. Apparently, there is a lot of
and asymptomatic cases, assuming that the asymptomatic re- simplifications in this discussion; the age range, the subject-
coveries are measurable by (random or systematic) public tests specific body immune system features, the severeness of
over the population, such as the antibody tests that have been the virus and many more factors have been neglected. But
conducted by some nations during the COVID-19 outbreak. it gives an idea about how the parameters can be tuned
In Section IV, the model is modified to a more practical case, in practice, up to a reasonable order of magnitude. With
in which only the recoveries due to the symptomatic cases are this background, we now explain the interpretation of each
measured. parameter of the model.
We should add that wide screening policies adopted by
certain countries are external factors that can significantly
B. Model assumptions and level of abstraction
accelerate the identification of the infected cases. In this
The simplifying assumptions behind the proposed model case, screening is a factor that increases κ.
are: • αi : The contagion factor between the infected and suscepti-
1) The model variables are assumed to be continuous in both ble populations, which is related to the contagiousness of the
amplitude and time. virus and social factors such as personal hygiene, population
2) Birth and natural deaths have been neglected. Therefore, density and level of human interactions. In order to find the
other parameters leading to changes in the population are range (or order of magnitude) of this parameter, we can start
not considered. Neglecting the birth rate is also supported with the contagion factors of more known viruses, such as
by the current findings that babies are not susceptible to flu and influenza, which are more or less influenced by the
this virus and to the best of our knowledge, no congenital same spreading factors.
transmissions of the virus from mothers to fetuses have • αe : The contagion factor between the exposed and suscepti-
been reported. ble populations. This parameter is logically far greater than
3) In the current study, we do not distinguish between male αi , since in ordinary conditions (before lockdowns and quar-
and female subjects; although the current global toll of the antine), people rarely avoid contact with an asymptomatic
virus suggests that men have been more vulnerable to the individual; nor does the individual itself avoid interaction
virus than women. with others.
4) Age ranges have not been considered; although we known • γ: The reinfection rate, or the rate of returning from the
that higher aged subjects are more vulnerable to the virus recovered group to the susceptible group. This happens for
and countries have different population pyramids. the cases that the body does not develop lifetime immunity
5) Moreover, in this primary version, we have not yet consid- after recovery, or the virus itself starts to mutate over
ered the possibility of vaccination. time. This parameter is the inverse of the immunity rate
6) Geopolitical factors such as distance, country borders and of the virus. It is currently too early to comment about the
continental differences have also been ignored. But con- immunity characteristics of the Coronavirus3. Although at
sidering that different countries have adopted customized least one case of reinfection soon after recovery has been
countermeasures against the virus spread, the model pa- reported, preliminary research have suggested short-term
rameters are fitted over country-level data. immunity of up to four months.
• β: The recovery rate of the infected cases. By considering
the fourth equation in (27), we can denote the change in
C. Model parameters
the number of hospitalized recoveries (or under control
Having formed the model, we now explain its parameters in any form, e.g., under home-care) by rh , resulting in
and their relationship with real-world factors and clinical rh (t + ∆) − rh (t) ≈ ∆βi(t), where ∆ is the time unit of
protocols. The techniques for estimating and fitting these approximation (for example 1 day). Therefore, the parameter
parameters on real data is later detailed in Section VI. β can be approximated by dividing the daily recovery count
Note that all the model parameters have the dimension of of the population under study, by the total infected cases
inverse time, to balance the left and right side dimensions in the same day. In the real world, apart from the body
of (27), and that the studied model is essentially based on strength of the infected subject in resisting against the virus,
an exponential law assumption, as detailed in Section II-B. this parameter depends on the healthcare infrastructure of a
Therefore, we can find rules of thumb for selecting the model country (hospitalization facilities, availability of medication,
parameters based on clinical facts and protocols. number of intensive care units, etc.).
• κ: The rate at which symptoms appear in exposed cases, • ρ: The recovery rate of the exposed cases (the cases that
resulting in transition from the exposed to the infected are exposed, but recover without any symptoms). This
population. The selection of this parameter is according to
the exponential law detailed in Section II-B. Assume that we 3 Refer to:
are dealing with an extremely contagious disease for which https://www.who.int/docs/default-source/coronaviruse/
the healthcare decision makers have agreed on the above who-china-joint-mission-on-covid-19-final-report.pdfDRAFT VERSION, SUBJECT TO MODIFICATION. FOLLOW THE UPDATES FROM: https://arxiv.org/abs/2003.11371 9
parameter is not directly measurable from pure observations E. Model analysis during outbreak
and requires lab-based experiments. However, we logically Let us study the model during the initial outbreak of the
expect this parameter to be of the same order or greater than epidemic, when the infection toll is still much smaller than
the parameter β (the recovery rate of the infected population the total population. For instance, suppose that a country
with symptoms). has 100,000 of exposed or infected cases, which is indeed
• µ: The mortality rate of the infected cases. By approximat- significant for any country, as it is far beyond the available
ing the last equation in (27) by p(t + ∆) − p(t) ≈ ∆µi(t), number of intensive care unit beds of even the most developed
where ∆ is the time unit of approximation (for example countries4 . But for a 100 million population country, such an
1 day), the parameter µ can be approximated by dividing exposure/infection toll is only 0.1% of the total population.
the daily death toll by the total infected cases in the same Therefore, during the primary phases of the disease spread,
day. As with β, the mortality of the virus itself, the immune the model can be simplified by assuming that the susceptible
system of the subjects, and the medical infrastructure are population is almost constant (s(t) ≈ 1) and ds(t)/dt ≈ 0, re-
important factors that influence the parameter. gardless of the other parameters of the model. This assumption
• e0 : The initial exposed population (seed). practically implies that the total population is not important
By studying the above factors, we can see that the only during an epidemic outbreak (in low percentages of infection),
parameters of the model that can be changed in the short- resulting in
term (before the development of long-term solutions such
Result 1. In low percentages of infection, the per-
as vaccination, medication, improvement of hospitalization
formance of epidemic control policies of states,
facilities, etc.), is to reduce the infection rates by minimizing
countries, and regions should not be evaluated by
human contacts (social distancing), or to apply public screen-
normalizing the infection/recovery/death tolls to their
ing. These are the two policies, which have been adopted
total population; but rather the net values should be
worldwide.
compared.
This result has also been approved in previous research
D. Fixed-point analysis based on model fitting on data from several epidemic diseases,
As with the basic SIR model presented in Example II-D1, showing that the disease spread is considerably independent
the fixed-point(s) of the model can be sought by letting the left of the total population size [20].
hand sides of all equations in (27) equal to zero. Accordingly, Under this assumption, (27) is simplified to the linear set
assuming that all the model parameters are nonzero, the only of equations:
fixed-point is the no-disease case (i(t) = e(t) = r(t) = 0): de(t)
dt e(t)
(s∗ (t), e∗ (t), i∗ (t), r∗ (t), p∗ (t)) = (1 − p0 , 0, 0, 0, p0) (31) di(t) αe − κ − ρ αi 0 0
i(t)
κ −β − µ 0 0
dt
≈
where 0 ≤ p0 ≤ 1 is the steady-state total death fraction. The dr(t)
ρ β −γ 0 r(t)
stability of this fixed-point can be addressed by perturbing the 0 µ 0 0
dt p(t)
fixed-point with a minor exposure ǫ (which can correspond to
dp(t)
a single new exposed case in the real world): dt
(34)
(s(t), e(t), i(t), r(t), p(t)) = (1 − p0 − ǫ, ǫ, 0, 0, p0) (32) Defining x(t) = [e(t), i(t), r(t), p(t)]T , (34) can be written in
matrix form:
d
Putting this point in the state dynamics (27), we find: x(t) = Ax(t) (35)
dt
ds(t) where A is the 4×4 state matrix on the right hand side of (34).
= −αe (1 − p0 − ǫ)ǫ ≈ −αe (1 − p0 )ǫ < 0 Equation (35) can be solved for an arbitrary initial condition,
dt
de(t) such as x(0) = (e0 , 0, 0, 0). The characteristic function of this
= αe (1 − p0 − ǫ)ǫ − κǫ − ρǫ ≈ (αe − αe p0 − κ − ρ)ǫ linear system is:
dt
di(t) |λI − A| = λ(λ + γ)[λ2 + (β + µ − δ)λ − δ(β + µ) − καi ] = 0
= κǫ > 0
dt (36)
dr(t) ∆
where δ = (αe − κ − ρ). Therefore the system’s eigenvalues
= ρǫ > 0
dt are:
dp(t) p
=0 δ − β − µ + (δ + β + µ)2 + 4καi
dt λ1 =
(33) p 2
which is unstable, i.e., the system’s dynamics drives it away δ − β − µ − (δ + β + µ)2 + 4καi (37)
λ2 =
from the fixed-point in the direction of reducing the healthy 2
cases, resulting in further infection. A more rigorous study of λ3 = 0, λ4 = −γ
the system stability conditions is presented in the following 4 See for example:
sections using eigenanalysis. https://link.springer.com/article/10.1007/s00134-012-2627-8/tables/2DRAFT VERSION, SUBJECT TO MODIFICATION. FOLLOW THE UPDATES FROM: https://arxiv.org/abs/2003.11371 10
which are all real-valued. Moreover, it is straightforward to Result 2. During an exponential outbreak of an
check that λ1 > δ > λ2 . The eigenvectors corresponding to epidemic (λ1 > 0), the system is unstable and with-
each eigenvalue are: out enforcing temporary lockdowns, social distancing
and quarantine of the infected cases (resulting in the
λ1 − δ ραi + β(λ1 − δ) µ(λ1 − δ) T model parameter changes), the exponential increase
v1 = k1 [1, , , ]
αi αi (λ1 + γ) αi λ1 in the number of infected subjects continues to a
λ2 − δ ραi + β(λ2 − δ) µ(λ2 − δ) T (38) point where a significant percentage of the popula-
v2 = k2 [1, , , ]
αi αi (λ2 + γ) αi λ2 tion is infected.
v3 = [0, 0, 0, k3 ]T , v4 = [0, 0, k4 , 0]T
Using the method detailed in Section II-E, we can further
where k1 , k2 , k3 and k4 are arbitrary constants. The general show that for the epidemic model (27), the reproduction
form of the solution of the compartmental variables is a number (spectral radius of the NGM) is equal to:
summation of exponential terms with the above exponential
rates and eivenvectors: αe (β + µ) + καi
R0 = (42)
(κ + ρ)(β + µ)
4
Apparently, R0 < 1 exactly simplifies to the stability condition
X
x(t) = ak eλk t vk (39)
k=1 in (41), when λ1 < 0.
Specifically, after some algebraic simplifications, we can cal- Result 3. Under countermeasures, the model eigen-
culate the infected and exposed populations as follows: values change and λ1 (the dominant eigenvalue of the
linearized dynamic model) is the single parameter
e0 (λ1 − δ)(δ − λ2 ) that can be tracked as a score for evaluating how
i(t) = [exp (λ1 t) − exp (λ2 t)] good countermeasures such as social distancing and
αi (λ1 − λ2 )
e0 quarantine are performing.
e(t) = [(λ1 − δ) exp (λ2 t) + (δ − λ2 ) exp (λ1 t)]
λ1 − λ2
(40) Considering that the death toll p(t) is composed of the same
From the last equation in (27), it is clear that the death toll exponential terms as the infected cases in (40), the above result
will not stop before i(t) = 0. Also from (40), we can see that is indeed disturbing.
since λ1 is the dominant eigenvalue, the steady-state behavior It is also interesting to observe from (40 ) that the population
and whether or not i(t) and e(t) diverge from or converge to of the different compartments of the model is only linearly
zero, depends on the sign of λ1 . The necessary and sufficient proportional to the initial exposed population size e0 5 . There-
condition for the linearized system’s stability (stopping the fore, for a large population (at the level of a populated city or
death doll) is λ1 < 0, which simplifies to καi + δ(β + µ) < 0, country), the initial infected seed size is not as important as the
or: other model parameters that influence the exponential behavior
καi < (κ + ρ − αe )(β + µ) (41) of the model (such as the social contact rates). Therefore:
Result 4. The initial seed size is not the most critical
A sufficient condition that guarantees this property is when parameter for epidemic management. Regions with
αi = αe = 0. The condition αi = 0 implies that the smaller initial seeds of infected/exposed cases may
susceptible group avoids contact with the infected ones. How- end up with a higher infected and death toll depend-
ever, the second condition (αe = 0) is difficult to fulfill ing on their infection rates, defined by factors such
in the real-world, since the exposed group do not have any as human-contact rate and personal hygiene.
symptoms. This is why social distancing is required to enforce
αe ≈ 0 and to permit all the exposed subjects to move to the Another interesting property is to check the ratio between
infected group without infecting new individuals, after which the number of infected (which is measurable in the real world)
the asymptomatic group can be all considered clear of the and the number of exposed (which is not directly measurable).
disease. Another practical case is when αi ≈ 0 (healthy people From (40), we can find6 :
avoid contact with the infected) and κ + ρ > αe (the rate of
recovery of the exposed or the appearance of their symptoms i(t) exp(λ̃1 t) − exp(−λ̃2 t)
is faster than the rate of new exposures). This condition is = (43)
e(t) αi [λ̃1 exp(λ̃1 t) + λ̃−1
−1
2 exp(−λ̃2 t)]
fulfilled by social distancing and lockdown (isolation of even
the asymptomatic cases for a certain period). ∆ ∆
where λ̃1 = λ1 − δ and λ̃2 = δ − λ2 are both positive.
However, if none of the above conditions are fulfilled and Therefore, when the terms containing exp(−λ̃2 t), which is
λ1 > 0, the number of exposed and infected cases increases a decaying exponential, vanish and the epidemic model is still
exponentially at a rate of λ1 . In this case, with fixed system
parameters, the infection rate rises exponentially up to a point 5 Note that the COVID-19 is believed to have started from a single case.
at which the linear approximation does no longer hold. This 6 The numerator and denominator of (43) have been multiplied by exp(−δt)
practically translates into: to obtain the simplified form.DRAFT VERSION, SUBJECT TO MODIFICATION. FOLLOW THE UPDATES FROM: https://arxiv.org/abs/2003.11371 11
in its linear phase (i(t) ≪ s(t) or s(t) ≈ 1), the ratio can be observed and reported by the healthcare units. The dynamic
approximated by: system corresponding to this model is:
i(t) λ̃1 Model II:
→ for t ≫ λ̃−1
2 and i(t) ≪ s(t) (44)
e(t) αi ds(t)
= −αe s(t)e(t) − αi s(t)i(t) + γe re (t) + γi ri (t)
dt
which gives the following practical result: de(t)
= αe s(t)e(t) + αi s(t)i(t) − κe(t) − ρe(t)
dt
Result 5. During the primary phases of an epidemic di(t)
= κe(t) − βi(t) − µi(t)
outbreak (when the number of contaminated cases dt
dre (t)
has an exponential growth, but the percentage of = ρe(t) − γe re (t)
the infected individuals to the total population is dt
dri (t)
still small), the number of exposed subjects can be = βi(t) − γi ri (t)
dt
approximated by e(t) ≈ αi λ̃−1 1 i(t), permitting its dp(t)
estimation from i(t). = µi(t)
dt
(45)
subject to s(t)+e(t)+i(t)+re (t)+ri (t)+p(t) = 1, which can
F. Repeated waves of epidemic again be used to reduce the model order by omitting one of
the model variables (e.g., s(t)). In the latter case, we assume
The peaks of the infected group population, and its potential that the observed variables are I(t), Ri (t) and P (t), resulting
repetition in time, is important from the strategic viewpoint in the following observation model:
[24]. These points correspond to local or global extremums of
i(t), which mathematically correspond to where di(t)/dt = 0 e(t)
in (27), i.e., where i(t) = κe(t)/(β + µ). It can be shown
I(t) i(t) vi (t)
0 1 0 0 0
that this leads to a reduced order set of nonlinear dynamic
Ri (t) = 0 0 0 1 0 re (t) + vr (t) (46)
equations, which can be solved for the remaining variables
P (t) 0 0 0 0 1 ri (t)
vp (t)
[s(t), e(t), r(t), p(t)]T . The simulations demonstrated in the
sequel, show that the infected population can have multiple p(t)
local peaks over time, with recurrent behaviors, proving that:
which can be written in compact form, as in (30).
Result 6. The epidemic disease can repeat pseudo- Similar to the first model, under the assumption of low
periodically over time (in later seasons or years) fraction of infection (during epidemic outbreak) and omitting
and turn into a persistent disease in the long term. the variable s(t), (45) simplifies to:
The amplitude and time gap of the infection peaks
de(t)
depends on the model parameters. dt
di(t) e(t)
This behavior has been observed in previous pandemics, αe − κ − ρ αi 0 0 0
dt i(t)
such as the 1918 pandemic influenza, known as the Spanish flu, κ −β − µ 0 0 0
dre (t)
≈ ρ 0 −γe 0 0 re (t)
where three pandemic waves of infection have been observed
dt
0 β 0 −γi 0 r (t)
within an interval of a few months7 . A mathematical study dri (t) i
0 µ 0 0 0
p(t)
of sustained oscillations of similar compartmental models has dt
dp(t)
been studied in previous research [19], [25].
dt
(47)
Defining the state vector x(t) = [e(t), i(t), re (t), ri (t), p(t)]T ,
IV. P ROPOSED E PIDEMIC M ODEL II
(47) can be written in a matrix form similar to (35), where
The proposed model can be extended from various aspects. A is now the 5×5 state matrix on the right hand side of (47)
One such extension is to separate the recoveries from expo- and solved for an arbitrary initial condition. The characteristic
sure from the recoveries from infection. The advantage of function of this linear system is:
this separation is that in practice, the subjects that recover
without any symptoms may only be identified by broad public |λI−A| = λ(λ+γe )(λ+γi )[λ2 +(β+µ−δ)λ−δ(β+µ)−καi ]
screening, which is not very practical for a large population. (48)
∆
While the infected individuals that recover are already known where as in the first model δ = (αe − κ − ρ), resulting in the
for the healthcare system and are easy to monitor. Based on following eigenvalues:
this idea, the proposed extension of the model is as shown p
δ − β − µ + (δ + β + µ)2 + 4καi
in Fig. 6. Accordingly, the variables i(t), p(t) and ri (t) λ1 =
(the recoveries from infection) are the variables that can be p 2
δ − β − µ − (δ + β + µ)2 + 4καi (49)
λ2 =
7 Cf.
2
https://en.wikipedia.org/wiki/Spanish flu λ3 = 0, λ4 = −γe , λ5 = −γiYou can also read