Public Health Statistical Appendix Out of Hours Care in Skye, Lochalsh and South West Ross - Hugo van Woerden, Director of Public Health and ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Public Health Statistical Appendix
Out of Hours Care in Skye, Lochalsh
and South West Ross
Hugo van Woerden, Director of Public Health and Policy, NHS Highland
Andrew Rideout, Public Health Speciality Registrar, NHS Dumfries and Galloway
April 2018
1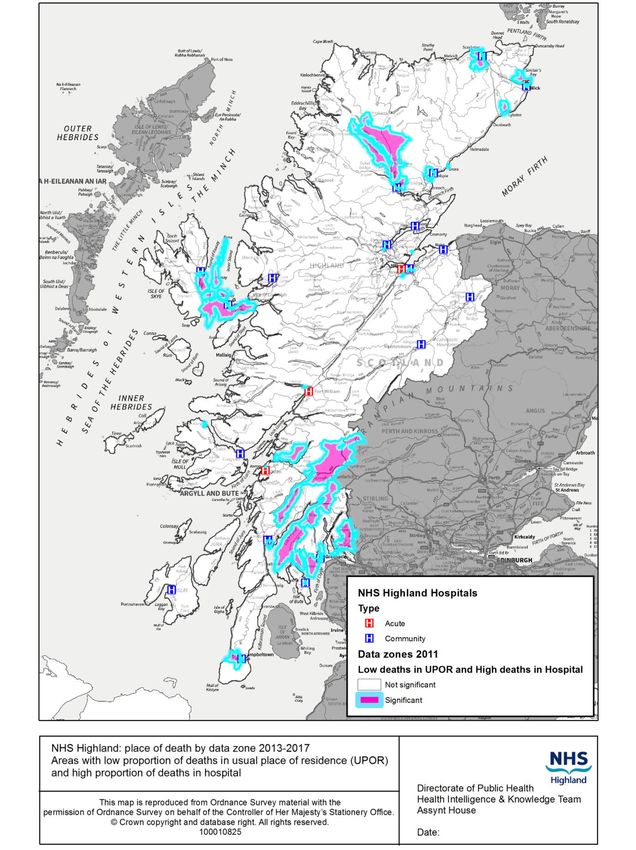
Executive Summary
The aim of the briefing is to present epidemiological information that will inform the
recommendations that the panel will make, whilst minimising any overlaps with sources of
epidemiological information that are provided by other reports to the panel.
The briefing considers: who receives care, who delivers care, what care is delivered, where is the
care delivered and when is care utilised?
The population of Skye is scattered with relatively long travel distances. It is an aging population,
with a falling proportion of working age, who can provide care services, although the elderly in Skye
place relatively low demands on Out of Hours services. There are areas of rural deprivation, which
may result in greater levels of Out of Hours care.
Out of Hours care has historically been provided by GPs and hospital based facilities including units
in both Portree and Broadford that did not fall into a typical description of emergency departments
or minor injury units. Unscheduled care is increasingly being provided by nurses, paramedics, NHS
24, other emergency services and first responders. Care is also provided for island populations on
Raasay and Eigg.
The delivery of care draws on community services, primary care, local intermediate care, NHS 24, a
general hospital in Fort William and a large general hospital1 in Inverness, which is the main source
of visiting outpatient services to the island. Service redesign plans around facilities in Broadford and
Portree are underway, with a new hospital planned in Broadford.
Out of Hours services display expected diurnal variation and an annual seasonal pattern associated
with the very large influx of tourists each summer. It is anticipated that complementary data on
ambulance and NHS 24 services will be provided by these services.
In conclusion, the Isle of Skye is a challenging environment in which to provide Out of Hours care,
given its geography. There is a need to build on emerging models of care to make Skye a place
which is internationally recognised as leading the way in providing solutions that work in such a
context. This is likely to require cross organisational working and increasing use of technology to link
local services with specialist input.
1
ISD Hospital classification: http://www.isdscotland.org/Health-Topics/Finance/Costs/Reference-Information.asp
2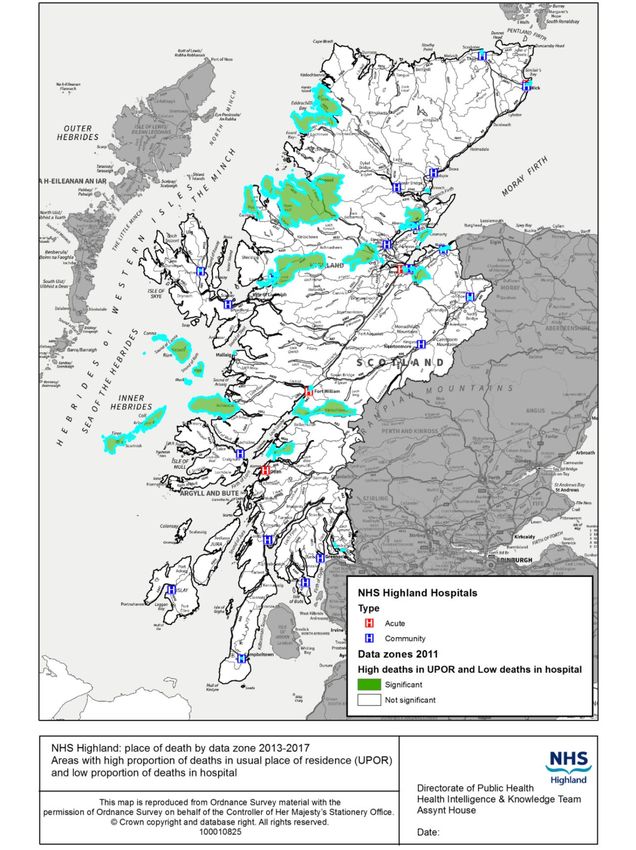
Table of Contents
1. Introduction 7
1.1 Defining Out of Hours Care 7
2. Who receives care? 8
2.1 Demography 8
2.2 Deprivation 11
2.3 Patients with Long Term Limiting Illness 19
2.4 End of Life Care 19
3. Who delivers care? 24
3.1 NHS staff 24
3.2 Unpaid carers 27
4. What care is delivered? 30
4.1 Historic changes to services 30
4.2 Out of Hours Services 34
4.3 Unscheduled care contact outcomes 36
4.4 Admission to hospital after unscheduled care contact 37
4.5 Outpatient Care 39
4.6 District Nursing 43
4.7 Allied Health Professionals 44
4.8 Hospital services 48
4.9 Midwifery Care 60
4.10 Ambulance Services 61
5. Where is the care delivered? 66
5.1 Travel 70
5.2 Care Homes 74
5.3 Projections of future need 76
6. When is care utilised? 78
7. Conclusion 85
7.1 Limitations 85
7.2 Main findings 85
8. Acknowledgements 86
9. References 87
3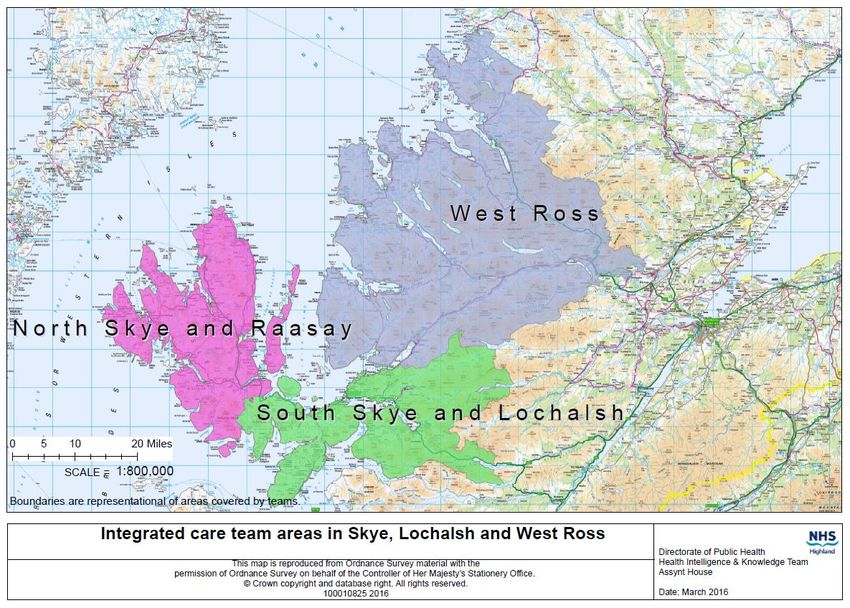
Tables
Table 1: Income deprivation in Skye, Lochalsh and South West Ross by data zone 17
Table 2: Proportion of deaths by Locality and District geographies and place of death, 2010-2012 (NHS
Highland residents only) 20
Table 3: Number of deaths by Locality and District geographies and place of death, 2010-2012 (NHS Highland
residents only / 3 year number of events) 21
Table 4: Unscheduled care contacts at Broadford and Portree by outcome, 2013- 2017 36
Table 5: Unscheduled care contacts at Broadford and Portree resulting in hospital admission, 2015- 2017 37
Table 6: Admission to hospital in the Out of Hours period after contact with the Out of Hours service 2017 38
Table 7: Summary of outpatient services at Portree Hospital and the MacKinnon Memorial Hospital 39
Table 8: Allied Health Professional Appointments, Portree Hospital 45
Table 9: Allied Health Professional Appointments, Mackinnon Memorial Hospital 46
Table 10: Allied Health Professional Appointments, other Skye and Lochalsh locations 47
Table 11: Summary of services in Portree Hospital and the Mackinnon Memorial Hospital, Broadford 48
Table 12: Mean and Median length of stay for Skye Hospitals, 2008/9 to 2012/13 55
Table 13: Pattern of delayed discharges by length of delay, Skye, Lochalsh and South West Ross, 2011-14 58
Table 14: Age specific delayed discharge rates per 1000 population, Skye, Lochalsh and South West Ross, 2011-
14 59
Table 15: Annual rates of SAS call-out attendances during 2014 by Ambulance station 61
Table 16: Annual rates and numbers of SAS call-out attendances during 2014 by area of attendance 62
Table 17: Patients transferred by ambulance from Portree Hospital/Medical Centre to Broadford Hospital
during 2014 by emergency status 62
Table 18: Community Health Index Practice list population of Skye and Lochalsh (excluding South West Ross)
within 60 minutes drive time from Portree and Broadford 71
Table 19: Summary of bus services to and from Broadford or Portree 73
Table 20: Summary of Ferry Services for Raasay-Sconser 74
Table 21: Number of unscheduled care patient contacts at Broadford and Portree by calendar year by time of
day 79
Table 22: Number of unscheduled care patient contacts at Broadford and Portree combined, by calendar year
by time of day 82
Table 23: Number of contacts with unscheduled care services at Broadford and Portree by Data Zone of
residence by time of contact, during 2017 82
Table 24: Percentage of contacts by type and time at Portree, 2017 83
Table 25: Percentage of contacts by type and time at Broadford, 2017 83
Table 26: Service access to unscheduled care services at both Broadford and Portree by time period for
residents of SLsWR and non-residents by method of contact, 2017 84
4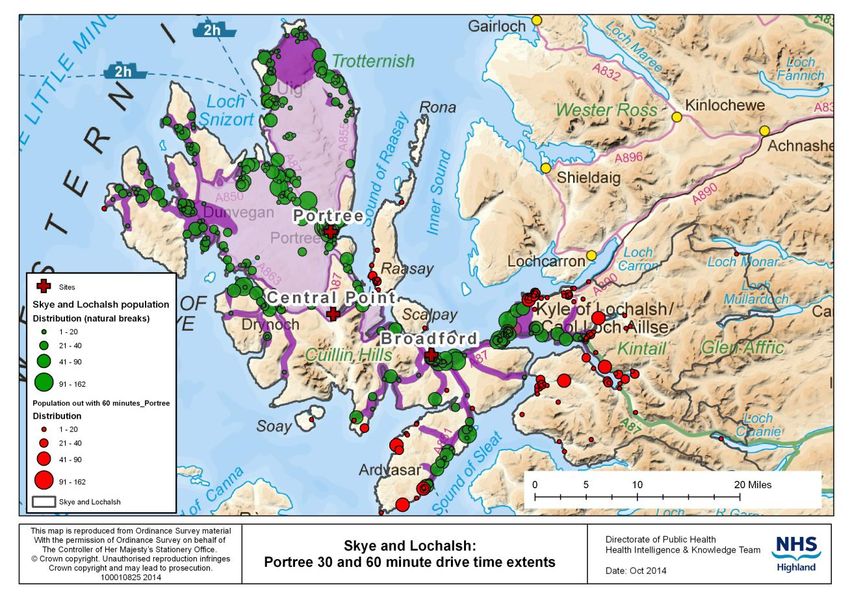
Figures
Figure 1: Trend in population estimates (2003 to 2013) and projections to 2037 by age band, Skye, Lochalsh
and South West Ross 8
Figure 2: Population over time – Skye, Lochalsh & West Ross 9
Figure 3: Community Health Index population distribution in the Skye, Lochalsh and South West Ross area 10
Figure 4: Population pyramid for Skye and Lochalsh, 2013 and 2026 11
st nd
Figure 5: Overview of the NHS Highland Board 1 and 2 Quintiles of deprivation using SIMD 2012 12
Figure 6: Model of potentially fragile areas in Scotland 14
Figure 7: Economically fragile areas in Scotland 16
Figure 8: Distribution of income deprivation by data zone area in Skye, Lochalsh and South West Ross 18
Figure 9: Age and sex specific rates of Long Term Limiting Illness, Skye and Lochalsh, 2001 & 2012 19
Figure 10: Place of death by data zone, combined years 2013-17 (hospital deaths) 22
Figure 11: Place of death by data zone, combined years 2013-17 (deaths at home) 23
Figure 12: Proportion of Out of Hours cases seen by different professionals, Skye, 2013 to 2017 24
Figure 13: Summary of current Whole Time Equivalent (WTE) establishments in Skye, Lochalsh and South West
Ross Workforce Plan 25
Figure 14: Provision of unpaid care by category by Highland geography 2011 27
Figure 15: Unpaid care and formal care provision in Highland at 2011 Census 28
Figure 16: Estimated and projected number of older people in Highland receiving informal care 29
Figure 17: Location of Out of Hours Care, Skye and Lochalsh, 2018 34
Figure 18: Percentage of unscheduled care activity at Portree and Broadford (combined) by age group and
residence, Jan-Dec 2017 34
Figure 19: Directly age standardised rate per 1000 population of unscheduled care at Broadford and Portree by
Data Zone of residence in SLsWR, 2017 35
Figure 20: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all
specialties and all locations, 2010-2011 – 2012-2013 40
Figure 21: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all
specialties at MacKinnon Hospital, 2010-2011 – 2012-2013 41
Figure 22: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all
specialties at Portree Hospital, 2010-2011 – 2012-2013 42
Figure 23: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all
specialties at Raigmore Hospital, 2010-2011 – 2012-2013 43
Figure 24: Number of inpatient admissions and available beds at Portree Hospital, 2011-18 49
Figure 25: Number of inpatient discharges and length of stay at Portree Hospital, 2011-18 49
Figure 26: Percentage occupancy and available beds at Portree Hospital, 2011-18 50
Figure 27: Number of inpatient admissions and available beds, MacKinnon Memorial Hospital, 2012-18 51
Figure 28: Number of inpatient discharges and length of stay, MacKinnon Memorial Hospital, 2012-18 51
Figure 29: Occupancy and number of available beds, MacKinnon Memorial Hospital, 2012-18 52
Figure 30: Trends in admissions and bed day rates for Skye hospitals, 2003 - 13 53
Figure 31: Summary of bed changes identified in the Mackinnon Memorial Hospital, Broadford, 2006/07 to
2013/14 54
Figure 32: Summary of bed changes identified in the Portree Hospital, 2006/07 to 2013/14 54
Figure 33: Monthly percentage bed occupancy at Skye Hospitals, 2009/10 to 2013/14 55
Figure 34: Length of stay in Skye Hospitals, including inter-quartile data, maximum and minimum data,
2008/09 to 2012/13 (GP beds only) 56
Figure 35: Trends in admission rates per 1000 population by GP practice, Skye Hospitals, 2009-13 57
Figure 36: Top 25 primary diagnoses for admissions to Skye Hospitals, 2009-13 58
Figure 37: Reasons for delayed discharges, Skye, Lochalsh and South West Ross, 2011-14 60
5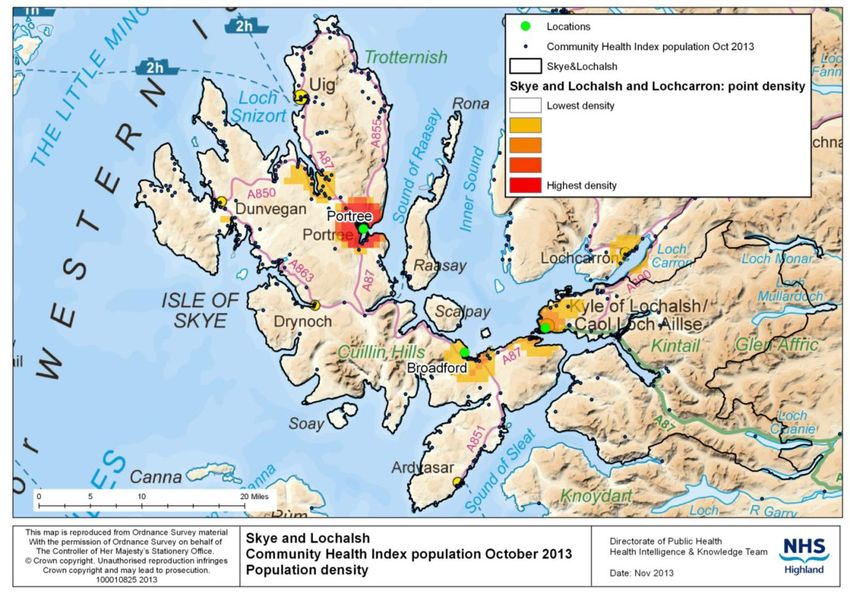
Figure 38: Births to mothers resident in Skye and Lochalsh in calendar years 2006 - 2016 60
Figure 39: Number of patients conveyed from Skye and Lochalsh in 2017 by receiving hospital 63
Figure 40: Average time spent conveying patients to Raigmore Hospital, 2017 64
Figure 41: Average time spent on incidents in Inverness, when ambulances were detained in Inverness, by
home despatch point, 2017 65
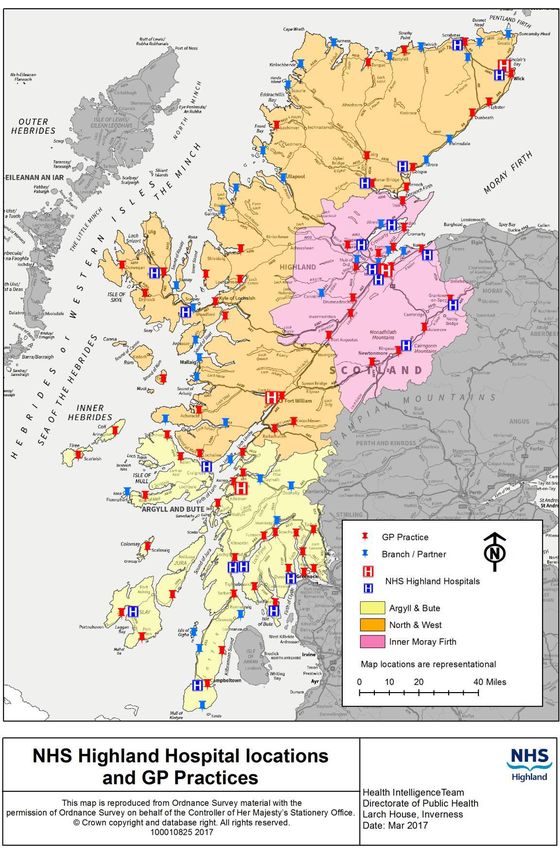
Figure 42: Health Services across NHS Highland 66
Figure 43: Health care facilities in Skye and Lochalsh and South West Ross 67
Figure 44: Geography covered by Integrated Care teams (nursing and social care) 68
Figure 45: GP practices in Skye and Lochalsh 69
Figure 46: Population registered with General Practices in April 2014 and October 2017 70
Figure 47: Area within 30 and 60 minutes drive from Portree Hospital 71
Figure 48: Area within 30 and 60 minutes drive from MacKinnon Memorial Hospital 72
Figure 49: Care home places in Skye, Lochalsh and South West Ross 75
Figure 50: Care Home places and Hospital beds per 1000 population aged 75+, NHS Highland 76
Figure 51: Summary of bed models using Skye, Lochalsh and South West Ross population projections and 85%
bed occupancy 77
Figure 52: Cumulative number of Out of Hours cases seen per hour over a week, totalled over 12 months 78
Figure 53: Percentage of unscheduled care patient contacts at Broadford and Portree combined by calendar
year by time of day 78
Figure 54: Percentage of unscheduled care patient contacts at Broadford and Portree by calendar year by time
of day 79
Figure 55: Unscheduled care activity at Portree and Broadford (combined), Jan 2013 to Dec 2017 80
Figure 56: Unscheduled care activity at Broadford from January 2013 to December 2017 81
Figure 57: Unscheduled care activity at Portree from January 2013 to December 2017 81
Figure 58: Out of Hours contacts at both Broadford and Portree and Highland by method of contact, 2013-
2017 84
6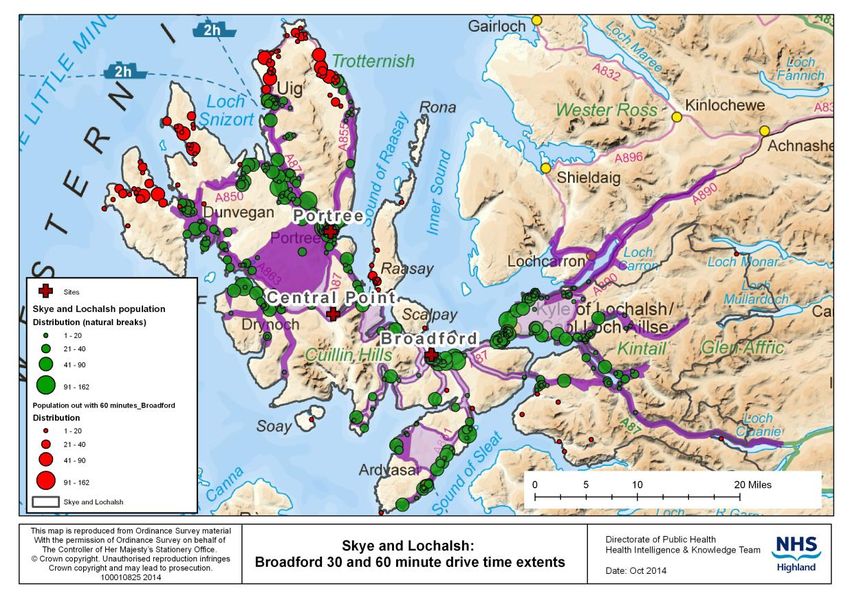
1. Introduction
The terms of reference for the Out of Hours work being led by Sir Lewis Ritchie state that, “The
specific remit is to assess the resilience of urgent primary care out-of-hours provision” and “to
provide an external professional view of the urgent care services in the area”2 . This briefing is
designed to support that review and provide epidemiological information for consideration by the
Panel who are supporting the review.
The aim of the briefing is, therefore, to present epidemiological information that will inform the
recommendations that the panel will make, whilst minimising any overlaps with sources of
information that are provided by other reports to the panel. It is anticipated that any
recommendations that the panel may make may wish to take into consideration: who receives
care?; who delivers care?; what care is delivered?; where is the care delivered?, and when is care
utilised? Available evidence which addresses these questions is provided below.
The primary focus of this briefing is the Isle of Skye. Data related to Lochalsh & South West Ross is
also provided where it is thought that this may be relevant and is easily available. Given the tight
timescale, the briefing draws primarily on available data, as opposed to undertaking fresh analyses.
This briefing has not been underpinned by a literature review, as relevant literature on Out of Hours
services and models of care are available as part of the recent Scottish Government National Review
on Out of Hours care published in 2015 by Sir Lewis Ritchie, ‘Pulling together: transforming urgent
care for the people of Scotland. The Report of the Independent Review of Primary Care Out of Hours
Services’.3
1.1 Defining Out of Hours Care
Out of Hours care can be defined in a recent review as “care provided between 18.30 and 08.00 on
weekdays, all weekend and Bank Holidays”4. The review goes on to say, “Care provided in the OOH
time period is unscheduled, i.e. there has been no forward planning (either by patient or professional)
or appointment made in advance. However, such care may or may not be regarded as urgent care.”
The report also states that, “in practice, out-of-hours care provision often starts at 6pm.” This is the
standard hand over time in NHS Highland.
2
NHS Highland, 2018. Terms of Reference, External view of arrangements for Unscheduled Care (urgent primary care out-
of-hours provision) in Skye, Lochalsh and South West Ross. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/1%20OOHs%202018/SkyeNHS%20HighlandReviewTOR160118_Final.pdf
3
Ritchie, L., 2015. Pulling together: Transforming Urgent Care for the People of Scotland. The Report of the Independent
Review of Primary Care Out of Hours Services. Edinburgh: Scottish Government. Available online:
http://www.gov.scot/Resource/0049/00490526.pdf
4
O’Donnell, C., Foster, H., Macdonald, S., Burns, N. & Gannon, M., 2015. Out-of-Hours Primary Medical Care: What Can
Research Tell Us? Findings From a Rapid Systematic Review and Qualitative Study. University of Glasgow. Available online:
http://www.gov.scot/Resource/0049/00492082.pdf [Accessed 9 April 2018].
7
2. Who receives care?
A range of information describing the population of Skye is provided below in relation to
demography, deprivation, long term limiting illness and end of life care.
In summary, although the total population numbers in Skye are expected to be stable over the next
twenty years (Figure 1), the proportion of older people has increased since 2001 (Figure 4) and this
trend is expected to continue (Figures 1 & 2). People across Skye also experience significant
deprivation (Figures 5 and 8), with just over 1,000 individuals (10%) being regarded as ‘income
deprived’. Both increasing age and greater deprivation are also associated with having one or more
long term limiting illnesses (Figure 9).
2.1 Demography
The trend in population by age is shown below.
Figure 1: Trend in population estimates (2003 to 2013) and projections to 2037 by age band, Skye,
Lochalsh and South West Ross
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
p.25. Figure 2. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
Slightly older data is provided below, which is useful in that it demonstrates the percentage changes
in different age groups.
8
Figure 2: Population over time – Skye, Lochalsh & West Ross
Source: NHS Highland Public Health Intelligence, 2017. Highland Community Partnership Profile – Skye,
Lochalsh & Wester Ross. Data source: National Records of Scotland Small Area Population Estimates; Best fit of
data zones 2001 and 2011 to Highland Community Partnership area.
The graph above demonstrates that the population between birth and 15 years fell by 17% between
2001 and 2015, whereas the population aged 65 years and over rose by 40.2% within the same
timeframe. An aging population is likely to place additional pressure on Out of Hours services over
the medium to long term.
9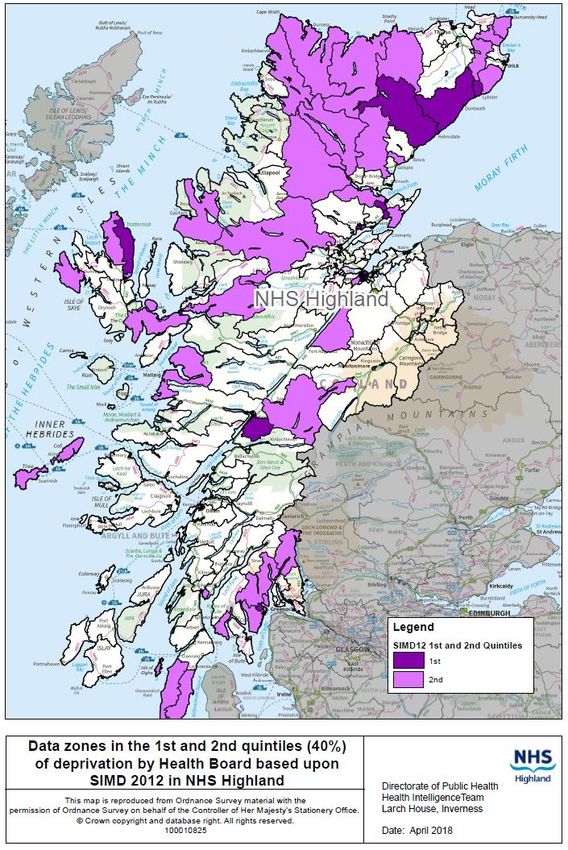
Figure 3: Community Health Index population distribution in the Skye, Lochalsh and South West
Ross area
Source: Douglas, I., 2013. Population drive time access to Community Hospitals in Skye & Lochalsh and South
West Ross, NHS Highland, Public Health Intelligence and Knowledge Team. p.6. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Drive%20time%20access%20SLSWR%20Nov%202013.pdf
Also included in: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of
community and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement -
Version 26. p.19, map2. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The map demonstrates that the greatest population density is around Portree, Broadford, and Kyle
of Lochalsh, although there are significant clusters of population elsewhere.
A population pyramid is provided below for 2013 and 2026. The predicted trend is a significant
growth in the very old and a fall, in particular, in the female population around their twenties and
thirties.
10Figure 4: Population pyramid for Skye and Lochalsh, 2013 and 2026
Source: Marshall, A., 2017. Projections of health care usage for Skye and Lochalsh. University of St Andrews.
p.11, figure 6.
Figure 4 should be interpreted with caution, as the date labelling in the source document is unclear.
However, the key message from the population pyramid is that there are relatively few individuals of
working age, compared to the population of very elderly who are may require care.
2.2 Deprivation
Deprivation is known to affect Out of Hours service utilisation.
Deprivation within communities not only relates to income (Table 1), but also factors such as
population density and access to services, and using these indices the population in parts of Skye,
along with other parts of Highland Region, experiences the highest levels of community ‘fragility’
(Figure 6).
The figure below provides information using the standard deprivation measure used in Scotland.
11Figure 5: Overview of the NHS Highland Board 1st and 2nd Quintiles of deprivation using SIMD 2012
Data source: NHS Highland, Public Health Intelligence, Scottish Government SIMD 2012 indicators. Available
online: http://www.gov.scot/Topics/Statistics/SIMD/DataAnalysis/Background-Data-2012/Background2SIMD2012
12The map above indicates that a number of data zones in the Skye, Lochalsh and South West Ross
area are in the 40% of most deprived areas within NHS Highland. One data zone, representing Skye
North East, is in the 20% of most deprived areas in the study area. If the national rather than health
board ranks of deprivation are considered, no areas in Skye, Lochalsh and South West Ross are
ranked in the 20% of most deprived areas.
Deprivation in remote and rural areas is poorly reflected in standard deprivation indices and,
therefore, two models which use alternative approaches5 are shown below, based on the concept of
fragility. In rough outline the first model included the following factors:
1. Depopulation related to young working age adults
2. Population density
3. Rates of claim for Department of Work and Pensions benefits
4. Estimated median gross total household income £ per week
5. Access to nine core services
6. Drive time to a major retail centre
5
Douglas, I. and Thomas, C., 2015. Supporting the Highland Community Planning Partnership to identify areas of rural
population need. NHS Highland and Highland Council. Published within: Highland Community Planning Partnership (CPP)
Board meeting 3 June 2015 – Item 8: Deprivation and Inequalities – Rural Analysis; Annex 2. Available online:
https://www.highland.gov.uk/meetings/meeting/3466/highland_community_planning_partnership_board
13Figure 6: Model of potentially fragile areas in Scotland
Source: Douglas, I. and Thomas, C., 2015. Supporting the Highland Community Planning Partnership to identify
areas of rural population need. NHS Highland and Highland Council. Published within: Highland Community
Planning Partnership (CPP) Board meeting 3 June 2015 – Item 8: Deprivation and Inequalities – Rural Analysis;
Annex 2, .p6. Available online:
https://www.highland.gov.uk/meetings/meeting/3466/highland_community_planning_partnership_board
14Fragile areas were “characterized by a number of factors including weakening of communities
through population loss; low incomes; limited employment opportunities; poor infrastructure;
inadequate housing and remoteness”, based on four indicators:
1. Population decline 2001 to 2005, three bands identified (Small Area Population Estimates)
2. Population density 2005, two bands identified (Small Area Population Estimates)
3. Drive time to a mid-sized service centre, three bands identified (SNS, Google Maps
4. Income per household, two bands identified (CACI Paycheck).
Although the map above and map below produce quite distinct patterns, both maps indicate that
parts of Skye, Lochalsh and South West Ross include economically fragile areas.
15Figure 7: Economically fragile areas in Scotland
Source: Douglas, I. and Thomas, C., 2015. Supporting the Highland Community Planning Partnership to identify
areas of rural population need. NHS Highland and Highland Council. Published within: Highland Community
Planning Partnership (CPP) Board meeting 3 June 2015 – Item 8: Deprivation and Inequalities – Rural Analysis;
Annex 2, p.6. Available online:
https://www.highland.gov.uk/meetings/meeting/3466/highland_community_planning_partnership_board
16The map above indicates that the whole of the north-west coastline of the north of Scotland is
economically fragile. If it is assumed that this is potentially associated with an aspect of rural
deprivation, it would confirm the fact that north Skye is an area which would be of importance in
terms of public sector planning.
The data below relate to income deprivation, which is arguably the single domain that is most
generalisable as a marker of deprivation.
Table 1: Income deprivation in Skye, Lochalsh and South West Ross by data zone
Source: Douglas, I., 2014. Income deprivation in Skye, Lochalsh and West Ross. NHS Highland Public Health
Intelligence and Knowledge Team. p.6. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Skye_incomedep.pdf
There are clearly areas of low income in Skye, which are likely to impact on the need for Out of
Hours services. The most deprived areas by this metric are Portree North and Portree West.
The map below provides a graphical description of income, which is one of the indices included in
many assessments of deprivation.
17Figure 8: Distribution of income deprivation by data zone area in Skye, Lochalsh and South West
Ross
Source: Douglas, I., 2014. Income deprivation in Skye, Lochalsh and West Ross. NHS Highland Public Health
Intelligence and Knowledge Team. p.7. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Skye_incomedep.pdf
The map above indicates that north east Skye is the area with the highest level of deprivation on the
island, using this particular metric; although Table 1 indicates greater proportions in Portree West
and Portree North, and greater numbers of deprived individuals in Portree West, Portree North, Uig,
Broadford, and Skye South East, which may have an impact on service use.
182.3 Patients with Long Term Limiting Illness
There is a clear relationship between age and long term limiting illness and between both of these
factors and the use of Out of Hours services6. Age specific rates of Long Term Limiting Illness
prevalence in this area is therefore shown below.
Figure 9: Age and sex specific rates of Long Term Limiting Illness, Skye and Lochalsh, 2001 & 2012
Source: Marshall, A., 2017. Projections of health care usage for Skye and Lochalsh. University of St Andrews. p.9.
There is a strong relationship between age and Long Term Limiting Illness in both men and women.
This is relevant to Out of Hours services, where the population is aging, as is the case in Skye, as it is
likely to affect need for health services.
2.4 End of Life Care
End of life care can have a significant impact on Out of Hours services. Some information on the
pattern of death across NHS Highland is therefore provided below.
In West Highland area a larger proportion of people die in settings where they may require Out of
Hours care (at home or in care homes) compared to Highland Region as a whole (Table 2). In Skye,
Lochalsh and West Ross over a three year period this meant that every week an average of between
1 and 2 people (74 people per year) died at home, with a significant proportion presumably dying in
the Out of Hours period.
6
Ritchie, L., 2015. Pulling together: Transforming Urgent Care for the People of Scotland. The Report of the Independent
Review of Primary Care Out of Hours Services. Edinburgh: Scottish Government. Available online:
http://www.gov.scot/Resource/0049/00490526.pdf
19Table 2: Proportion of deaths by Locality and District geographies and place of death, 2010-2012
(NHS Highland residents only)
Source: Douglas, I., 2013. Place of death in NHS Highland. NHS Highland, Public Health Intelligence &
Knowledge Team. p.20, Figure 15
The proportion of deaths in hospital for Skye, Lochalsh and West Ross, at 43.4%, is higher than some
comparable areas.
20Table 3: Number of deaths by Locality and District geographies and place of death, 2010-2012
(NHS Highland residents only / 3 year number of events)
Source: Douglas, I., 2013. Place of death in NHS Highland. NHS Highland, Public Health Intelligence &
Knowledge Team. p.19, Figure 14
The above table gives the numbers of deaths, to give an indication of the size of the end of life
population requiring end of life care and comparisons with other areas in NHS Highland. There were
664 deaths over the three year period, 2010-12 in Skye, Lochalsh and West Ross (SLWR). From Table
3 this indicates an annual average of 96 deaths in hospital, 2 deaths in a hospice, 74 deaths at home,
and 49 deaths in care homes in SLWR during this period.
The two maps below provide blue and pink shading of data zones to indicate two and three standard
deviations from the mean. The aim of these maps is to help identify areas that have unusual
patterns of place of death. The southern half of Skye is an area that relies heavily on hospital beds
as the place of death, and presumably end of life care, compared to NHS Highland as a whole.
21Figure 10: Place of death by data zone, combined years 2013-17 (hospital deaths)
Source: NHS Highland, 2017. The Annual Report of the Director of Public Health – Realistic Medicine. p32.
Available online: http://www.nhshighland.scot.nhs.uk/Publications/Documents/DPH-Annual-Report-2017_(web-version).pdf
22The map below examines the same topic but from the point of view of areas where a high
proportion of residents die at home. The Isle of Skye is not somewhere which stands out as a place
where a high proportion of patients die at home.
Figure 11: Place of death by data zone, combined years 2013-17 (deaths at home)
Source: NHS Highland, 2017. The Annual Report of the Director of Public Health – Realistic Medicine. p32.
Available online: http://www.nhshighland.scot.nhs.uk/Publications/Documents/DPH-Annual-Report-2017_(web-version).pdf
233. Who delivers care?
This section provides information on the workforce who deliver care. Some information is also
provided around informal carers.
3.1 NHS staff
In recent decades Out of Hours patients have been seen by GPs. However, parts of NHS Highland
are increasingly using a range of health professionals as is shown in the graph below.
Figure 12: Proportion of Out of Hours cases seen by different professionals, Skye, 2013 to 2017
Source: NHS Highland, 2017. Urgent Care – Data Summary for Skye. p.7.Prepared by Project Lead, Out of Hours
and Acting Primary Care Manager North & West (GMS) from ADASTRA patient management system.
The graph demonstrates the increasing use of nurses and paramedics to provide Out of Hours
services, with 40% of cases being seen by a professional other than a doctor by mid-2017. It is
anticipated that this trend will continue.
Several tables are provided below, which present available data on staff groups.
24Figure 13: Summary of current Whole Time Equivalent (WTE) establishments in Skye, Lochalsh and
South West Ross Workforce Plan
Data source: Extracted from Skye, Lochalsh and South West Ross Workforce Plan: version 8 within NHS
Highland, 2017. OUTLINE BUSINESS CASE, The Modernisation of Community and Hospital Services in Badenoch
& Strathspey (B&S) and Skye, Lochalsh and South West Ross (SLSWR). Appendix 11, pp 155-168. Available
online:http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/November%202017/4.5%20Outline%20Business%20C
ase%20BS%20and%20SLSWR.pdf.
25Figure (cont): Summary of current Whole Time Equivalent (WTE) establishments in Skye, Lochalsh and South West Ross Workforce Plan
Data source: Extracted from Skye, Lochalsh and South West Ross Workforce Plan: version 8 within NHS Highland, 2017. OUTLINE BUSINESS CASE, The Modernisation of
Community and Hospital Services in Badenoch & Strathspey (B&S) and Skye, Lochalsh and South West Ross (SLSWR). Appendix 11, pp 155-168. Available
online:http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/November%202017/4.5%20Outline%20Business%20Case%20BS%20and%20SLSWR.pdf.
Some of these teams appear to be relying on small numbers of staff and are probably fragile, as recruitment in this area is known to be challenging. Teams
such as those providing radiography and MacMillan nurses have some of the smallest whole time equivalent numbers (WTE).
263.2 Unpaid carers
The 2011 Census indicated that there were 2,054 people living in Skye, Lochalsh and West Ross
(SLWR) who were involved in providing unpaid care and support to a family member, friend or
neighbour to enable that person to continue to live in their own community.
The provision of unpaid care makes a vital contribution to the supply of care and this will be
increasingly important factor as the Highland population continues to age. The number providing
unpaid care in SLWR has grown by 3.6 percent between 2001 and 2011.
Figure 14: Provision of unpaid care by category by Highland geography 2011
Source: NHS Highland Public Health Intelligence. Census 2011 Snapshots: Unpaid care in Highland. Data
source: Census 2011: KS301SCA
The above graphic shows a higher percentage of the population providing unpaid care in Skye,
Lochalsh and West Ross compared to other areas in Highland.
27Figure 15: Unpaid care and formal care provision in Highland at 2011 Census
Source: NHS Highland Public Health Intelligence. Census 2011 Snapshots: Unpaid care in Highland. Data
source: Census 2011: KS301SCA
The above figure suggests that there is relatively little relationship between inpatient and care
establishment places, per 1000 population, and unpaid care at local level across Highland.
The sustainability of long-term care to older people relies heavily on the supply of informal care. As
the number of older people increases in future years, demand for informal care is also likely to
increase. Most informal care for older people is provided either by spouses or adult children.
The trends in population ageing and changes in the structure of families have led to forecasters
projecting a “tipping point” for care, where the numbers of older people needing care will begin to
exceed the numbers of family members available to provide the care7.
The following figure illustrates the projected increase in provision of unpaid, informal care over the
next 20 years in Highland.
7
Carers UK, 2010. Tipping point for care: time for a new social contract. Available from:
http://www.carersuk.org/professionals/resources/research-library/item/495-tipping-point-for-care-time-for-a-new-social-contract. Accessed
11 April 18.
28Figure 16: Estimated and projected number of older people in Highland receiving informal care
Source: NHS Highland Public Health Intelligence, 2018. Appendix 1: Assessing the needs of individuals with high
levels of dependency in NHS Highland. Data source: Family Resource Survey (2017) and NRS population
estimate for Highland 2016.
As has previously been demonstrated, the growth in numbers is particularly marked in those aged 85
years and over.
294. What care is delivered?
A number of aspects around what care is delivered is provided below including: historic aspects of
services, Out of Hours services, outpatient services, services delivered by Allied Health Professionals
in the community, and hospital services.
4.1 Historic changes to services
Some of the key changes to services that have happened in Skye are provided in box 1 and 2 below.
These are taken from the Full Public Consultation document for service redesign and provide a
snapshot of the services around 2014.
30Box 1 Local context
The opening of the Skye Bridge in 1995, and removal of tolls in 2004, eased access onto
and off the island.
Development of the Rural Practitioner Team based in Dr MacKinnon’s Memorial Hospital
in Broadford. Rural Practitioners are mostly GPs with enhanced training in emergency
care for rural settings. The team was established in 2004 to meet community needs
following the withdrawal of local surgical consultant and anaesthesia cover (for safety
reasons) plus the need to provide out-of-hours medical cover.
In May 2006, Gesto Hospital in Edinbane was closed.
New health centres were opened in Sleat in 2005, Kyle in 2008, and Broadford in 2012.
Broadford Health Centre replaced the existing Broadford Medical Practice and serves
patients from communities in Broadford, Strath, Kyleakin and Kyle Rhea communities. It
is co-located with Dr MacKinnon’s Memorial Hospital.
There have been Care home closures – Staffin, Hilton (Broadford) and Graham House
(Dornie).
An Acarsaid Care Home in Broadford was re-developed in 2010/11. There has been new
supported housing in Dornie.
Teleneurology clinics, Telediabetes clinics and Telecardiac rehabilitation clinics got
underway in both Portree and Broadford in 2011.
Various developments to community teams include redesign of community nursing
team, community midwifery team and community midwifery Unit in Dr MacKinnon
Memorial Hospital in Broadford.
A new dental clinic opened in Portree in 2012.
NHS Highland took on responsibility for adult social care (care-at-home, care homes, day
care services) in April 2012, as part of integration.
The Broadford Ambulance station closed in 2013 and was re-located to Dr MacKinnon
Memorial Hospital
Development of South Skye Practice (Broadford/Sleat/Carbost) – ongoing
Source: NHS Highland, 2014. Full public consultation document - Proposed modernisation of community and
hospital services in Skye, Lochalsh and South West Ross. p.14. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20%20FINAL%20FULL%2019%20May%2014.pdf
31A description of services, as included in the Public Consultation document, is provided below.
Box 2 Summary of some of the current services
Local GPs, nurses, allied health professionals8, community staff and others have been
working with an independent health care planner. They have been looking at current
services which are summarised below:
GP Practice
There are 14,680 registered patients in the area who are served by ten GP Practices
District General Hospital
The nearest district general hospital is Raigmore Hospital which is 120 miles away from
Portree, approximately three hours by road ambulance.
Dr MacKinnon Memorial Hospital, Broadford
This is a 20-bedded, intermediate care community hospital providing assessment,
resuscitation and stabilisation of acutely ill patients, supported by a small team of salaried
Rural Practitioners (RPs).
RPs are like GPs but with additional emergency training, allowing the hospital to function at
a higher level than most community hospitals. The hospital has 24-hour on-site medical and
nursing cover and 24 hour A&E and Primary Care Emergency Services (PCEC).
A small amount of planned day case surgery is carried out.
Radiology services, including ultrasound, are also on site.
There are a range of visiting specialist out-patient services from Raigmore (Inverness), New
Craigs Hospital (Inverness) and Belford Hospital (Fort William).
Portree Community Hospital
12-bedded community Hospital is located adjacent to the Portree Medical Centre. It is
supported by 24-hour nursing cover and access to 24-hour medical cover. The medical cover
is provided by GPs from the Portree Medical Centre from 0800-2300 every day, delivered by
GPs and during the out-of-hours period by Rural Practitioners; after 2300 there is no on-site
medical cover but is provided from Broadford RPs supported by a North Skye second on call
doctor.
8
Allied Health Professionals or AHPs include a number of health care workers such as physiotherapists,
occupational therapists, podiatrists, dieticians, speech & language therapists and radiographers.
32Box 2 Summary of services (contd.)
Portree Hospital (contd.)
Radiology services are available four days per week to support out-patient clinics which
include Orthopaedics, Ear, Nose and Throat, Ophthalmology, General Medicine, Renal,
Chest, Rehabilitation and Psychiatry.
Other services
Midwifery services cover Skye and Lochalsh with a base in both hospitals and one
community bed in Dr MacKinnon Memorial Hospital supporting 15-25 births per year.
Multi-disciplinary teams (social workers, care-at-home workers, physiotherapists,
occupational therapists, community nurses, and community mental health teams), currently
work out of a number of different bases.
Adult social care provided by NHS Highland includes care-at-home service, one Care Home
(An Acarsaid) in Broadford, Day Care Services (Tigh na Drochaidh) in Portree and (Airdferry)
in Dornie.
There are also two privately run Care Homes (Budh Mhor) in Portree and (The Haven) in
Idrigill, Uig. There is one private Nursing Home (Home Farm) in Portree.
The Howard Doris Unit in Lochcarron is a privately run facility, providing residential and day
services.
Source: NHS Highland, 2014. Full public consultation document - Proposed modernisation of community and
hospital services in Skye, Lochalsh and South West Ross. pp15-16. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20%20FINAL%20FULL%2019%20May%2014.pdf
334.2 Out of Hours Services
A variety of analyses of Out of Hours data is provided below. The first map shows the locations of
different types of Out of Hours care.
Figure 17: Location of Out of Hours Care, Skye and Lochalsh, 2018
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.3.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
A number of first responder and community response units locations are shown, as well as urgent
care facilities in Broadford and Portree. The age profile of unscheduled care activity is provided
below.
Figure 18: Percentage of unscheduled care activity at Portree and Broadford (combined) by age
group and residence, Jan-Dec 2017
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.7.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
34There is a notable difference in the age profile of those with out of area postcodes using
unscheduled care services at Broadford and Portree compared to those with resident postcodes. The
largest numbers of users in both groups are aged between 25 and 64. This activity makes up 60% of
the overall volume of the out of area group contacts compared with 42% of those with resident
postcodes in Skye, Lochalsh and South West Ross (SLsWR). The SLsWR resident activity has a
younger and older age profile. Utilisation by the very elderly is lower than might be expected. A
more detailed analysis of utilisation by area is provided below. A datazone is the key small area
statistical geography that is used in Scotland. They were introduced in 2004, to provide stable and
consistent small area geography, as other metrics, such as postcode or electoral ward can change
over time. There are 6,505 datazones covering the whole of Scotland.
Figure 19: Directly age standardised rate per 1000 population of unscheduled care at Broadford
and Portree by Data Zone of residence in SLsWR, 2017
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.10.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
After adjusting for population age, the highest rates of unscheduled care contacts with services are
found in Data Zones that are geographically close to service locations. In particular, the populations
of Broadford and Portree have the highest rates of service use. The rate in the Portree East & Rural
Data Zone is nearly twice as high as the overall rate.
There are very few contacts with patients who have home postcodes in South West Ross. Resident
of Lochalsh and the South of Skye almost exclusively use services only at Broadford. Residents of the
north of Skye access services at both Portree and Broadford. From the data extract used for this
analysis, it is not possible to understand the nature of the injury or illness involved in individual
35contacts. However, the pattern of use of Broadford by residents of the north Skye data zones may
reflect prioritisation of care to a location with an urgent care facility.
4.3 Unscheduled care contact outcomes
The outcome for unscheduled care contacts is provided below for the two main Skye hospitals.
Table 4: Unscheduled care contacts at Broadford and Portree by outcome, 2013- 2017
Broadford Contacts Portree Contacts
2013 2014 2015 2016 2017 2013 2014 2015 2016
Patient to Contact Surgery 971 1169 1205 1570 1840 1078 1201 1099 922
No Follow Up 2174 1950 1745 1587 1293 1392 1338 1157 1465
Surgery Follow Up in Morning 117 117 126 150 111 164 149 121 141
Admitted to Hospital 289 300 169 175 300 60 61 22 12
Refer to Ward 933 961 1115 1050 886 223 255 192 75
Outpatient Review Arranged 653 609 575 672 635 213 273 220 228
Refer to A&E 119 102 109 113 121 212 266 232 212
Transfer 12 5 18 26 48 14 19 16 19
Patient to Contact Dental Helpline 13 19 17 19 12 10 14 12 17
District Nurse Attended 7 10 9 14 10 8 11 14 5
Other 21 5 7 5 7 23 9 11 10
Total 5309 5247 5095 5381 5263 3397 3596 3096 3106
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.23.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
The available Adastra data extract provided no indication of the acuity of the patient workload.
However, an outcome field has been used to illustrate what happens to patients contacting
unscheduled care services. At Broadford in 2017, 25% of activity results in no follow up. As a
proportion of all activity the no follow up outcome has decreased in every year since 2013 with
more patients being instructed to contact their General Practice.
In 2017 6% of activity resulted in admission to hospital. However, the category ‘refer to ward’ also
appears to be used to capture admission related activity and 6 percent will be an underestimate of
admission. Very few consultations at the location are formerly recorded as resulting in a transfer
and again ‘refer to ward’ appears to be used to capture some of this activity.
The data suggests that 60-65% of unscheduled care contacts at Broadford end either with no follow
up or potential for a further contact with Primary Care and that 12% go on to an outpatient review.
About a quarter of all the contacts result in further direct engagement with hospital based services
either as an admission or a ward referral.
The pattern of patient care is very different at Portree. 40 percent of activity ends in no follow up. A
further 33-40 percent of activity results in a potential contact with Primary Care. Seven percent of
activity is referred to A&E and a further 7 percent results in an outpatient review. Very few people
are recorded as being admitted directly to hospital through unscheduled care services at Portree.
364.4 Admission to hospital after unscheduled care contact
It is useful to consider the proportion of cases that are admitted after contact with Out of Hours
services. The number of contacts with an associated hospital admission has been calculated by
linking Adastra data and an extract of hospital admission data from the local TrakCare patient
management system. The first hospital admission within a day of the recorded Adastra contact was
included in the table below.
Table 5: Unscheduled care contacts at Broadford and Portree resulting in hospital admission, 2015-
2017
Broadford Contacts No. per year
2015 2016 2017
Belford Hospital 2 5 2
Mackinnon Memorial Hospital 325 267 355
New Craigs Hospital 6 1 -
Portree Hospital 2 - -
Raigmore Hospital 127 161 137
Total 462 434 494
Portree Contacts No. per year
2015 2016 2017
Mackinnon Memorial Hospital 140 106 105
New Craigs Hospital 4 2 -
Portree Hospital 36 6 -
Raigmore Hospital 45 49 45
Total 225 163 150
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.24.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
At Broadford the data linkage suggests that 9 percent of contacts result in an admission. The
majority of these occur at the location. The analysis of the informational outcome data in the section
above suggested that about 6% of activity at Broadford resulted in further direct engagement with
hospital care.
From the data linkage there was an average of 141 direct admissions to Raigmore from Broadford a
year.
The data linkage suggests that about 6 percent of unscheduled care contacts at Portree result in an
admission to hospital. This is a larger proportion than identified in the admitted category of the
‘informational outcomes’. The majority of the admissions identified by the data linkage were
recorded as being ‘referred to A&E’ or ‘referred to ward’ in the informational outcomes recorded on
Adastra.
Information on admission to hospital, by Out of Hours period, is shown below.
37Table 6: Admission to hospital in the Out of Hours period after contact with the Out of Hours
service 2017
Out of Hours locations Number of admissions* Number of admissions as a % of all contacts at
the location
Tongue/Armadale 32 17.7
Lochcarron/Torridon 22 13.3
Wick 131 11.3
Thurso 108 10.1
Islay 10 9.6
Broadford 305 9.5
Fort William 237 8.8
Oban 232 8.4
Raigmore 1058 8.2
Dingwall 209 7.8
West Lochaber 11 7.8
Ullapool 27 7.3
Golspie 162 7.2
Invergordon 313 7
West Sutherland 10 7
Mull - Tobermory and Salen 13 6.6
Aviemore 220 6.3
Gairloch/Aultbea 20 6.3
Campbeltown 13 6.2
Portree 107 5.7
Cowal Rural 11 5.4
Rothesay 16 4.7
Lochgilphead 21 4.2
Dunoon 31 2.8
1
Nairn 25 0.7
Total 3360 7.2
*table excludes sites with less than 10 admissions; Activity between 6pm - 8am Monday to Friday, weekends
and Bank Holidays recorded on Adastra.
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.26.
1
Activity at Nairn is only very partially captured on Adastra.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS).
The above table is based upon the first hospital admission within a day of an Out of Hours contact at
a location recorded on Adastra.
The percentage of admissions at Broadford is higher than the Highland average; whereas the rate at
Portree is lower than average. 224 of the 305 (73%) admissions from Out of Hours contacts which
were at Broadford Hospital were to the Broadford Hospital and 80 (26%) to Raigmore Hospital. 84 of
the 107 (79%) admissions from Out of Hours contacts at Portree were to the Broadford Hospital and
23 (21%) to the Raigmore Hospital.
384.5 Outpatient Care
The two hospitals in Skye have a number of outpatient services. Many of these are provided by
visiting Consultants, primarily from Raigmore Hospital. Although outpatient care is less relevant to
Out of Hours care, the review has requested as full information as possible on local services and
details have therefore been provided. Much of the information presented below is from the Service
Redesign Outline Business Case and related Public Consultation documents.
Table 7: Summary of outpatient services at Portree Hospital and the MacKinnon Memorial
Hospital
Source: McVicar, G., 2014. Summary presentation used at public meetings – Skye hospitals, summary of
current and possible future arrangements. NHS Highland. p.4. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Skye%20Hospitals%20-
%20Summary%20of%20current%20and%20future.pdf
Local clinics are also run in both locations, although only shown on the left of the above table.
The pattern of outpatient care is summarised in the following maps, in relation to both hospitals in
Skye and Raigmore Hospital, Inverness.
39Figure 20: Directly age standardised outpatient attendance rates by data zone of residence in
SLsWR, all specialties and all locations, 2010-2011 – 2012-2013
Source: Douglas, I., 2014. Outpatient activity in Skye, Lochalsh and South West Ross, 2011-2013. NHS Highland
Public Health Intelligence and Knowledge Team. p.13. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Outpatient%20activity%20in%20Skye.pdf
The map above indicates that the north west of Skye appears to have a relatively low rate of use of
outpatients.
40Figure 21: Directly age standardised outpatient attendance rates by data zone of residence in
SLsWR, all specialties at MacKinnon Hospital, 2010-2011 – 2012-2013
Source: Douglas, I., 2014. Outpatient activity in Skye, Lochalsh and South West Ross, 2011-2013. NHS Highland
Public Health Intelligence and Knowledge Team. p.16. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Outpatient%20activity%20in%20Skye.pdf
The map above indicates that, as expected the highest users of services in the hospital in Broadford
live in the south of Skye and in the vicinity of the hospital.
41Figure 22: Directly age standardised outpatient attendance rates by data zone of residence in
SLsWR, all specialties at Portree Hospital, 2010-2011 – 2012-2013
Source: Douglas, I., 2014. Outpatient activity in Skye, Lochalsh and South West Ross, 2011-2013. NHS Highland
Public Health Intelligence and Knowledge Team. p.19. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Outpatient%20activity%20in%20Skye.pdf
The map above indicates that, as expected, the population that make the most use of the hospital in
Portree live north of that hospital, or in the vicinity of Portree.
42Figure 23: Directly age standardised outpatient attendance rates by data zone of residence in
SLsWR, all specialties at Raigmore Hospital, 2010-2011 – 2012-2013
Source: Douglas, I., 2014. Outpatient activity in Skye, Lochalsh and South West Ross, 2011-2013. NHS Highland
Public Health Intelligence and Knowledge Team. p.22. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Outpatient%20activity%20in%20Skye.pdf
The map above appears to indicate that utilisation of outpatient appointments at Raigmore Hospital
falls progressively as the travel distance increases, with residents of Skye making less use than
residents in Lochalsh. This pattern may also be related to a higher proportion of appointments being
delivered locally.
4.6 District Nursing
The level of community care and the hours that service is available can impact on more formal Out
of Hours services.
The District Nursing teams for Skye, Lochalsh and West Ross do not routinely provide a 24 hour per
day service, but arrangements are in place via an overnight on call service for End of Life care, by the
day team, as and when this is possible and as it is required. This service can be accessed through
NHS 24 or the Out of Hours team.
NHS Highland is piloting the principles developed by the Buurtzorg model in Holland across a
number of sites and is increasingly recognising the need to consider the optimal level of provision of
Out of Hours district nursing and community care services, within available funding envelopes9.
There may be the possibility of extending some district nursing services into the evening in the
9
https://buurtzorg.org.uk/ Accessed 11 April 18.
43future10. The ongoing review of district nursing services in the north and west operational unit
builds on the Scottish Government report, ‘Transforming Nursing, Midwifery and Health
Professionals Roles – Paper 3 - The district nursing role in integrated community nursing teams,11‘
published in December 2017, and on the ‘The Report of the Independent Review of Primary Care Out
of Hours Services’.12 Both of these documents highlight the challenges and opportunities for District
Nursing and Advanced Nurse Practitioners in remote and rural areas.
Virtual community wards are planned for Integrated Health and Social Care Teams in the North &
West NHS Highland unit. The aim of such virtual wards is to provide a high level of care in people’s
own homes for those most at risk from unscheduled hospital admissions. Work is also underway to
integrate Care at Home staff into such arrangements13.
4.7 Allied Health Professionals
Data on community services is generally poorly collected in Scotland and should be interpreted with
caution. Available data on Allied Health Professionals is provided below.
10
NHS Highland, 2017. Draft North Highland District Nursing Service Review.
11
http://www.gov.scot/Resource/0052/00529738.pdf
12
http://www.gov.scot/Resource/0049/00490526.pdf
13
North & West Operational Unit, Service Description, Virtual Community Ward (personal communication from Director of
Transformation and Quality Improvement to DPH 9/4/18)
44Table 8: Allied Health Professional Appointments, Portree Hospital
2013/2014 2014/2015 2015/2016 2016/2017
Occupational Therapy
Occupational Therapy
Occupational Therapy
Occupational Therapy
Speech & Language
Speech & Language
Speech & Language
Speech & Language
Multi-Profession
Multi-Profession
Multi-Profession
Multi-Profession
Physiotherapy
Physiotherapy
Physiotherapy
Physiotherapy
Dietetics
Dietetics
Dietetics
Dietetics
Podiatry
Podiatry
Podiatry
Podiatry
Total
Total
Total
Total
Month
APR 49 24 241 85 12 411 14 13 250 75 4 356 30 15 319 91 9 1 465 74 272 107 453
MAY 42 30 268 69 11 420 33 23 250 103 14 423 41 12 207 88 4 3 355 77 1 220 79 377
JUN 51 40 226 108 19 1 445 46 29 246 132 17 470 13 13 216 89 1 332 79 12 182 104 1 1 379
JUL 58 19 277 103 16 1 474 40 12 230 72 11 365 22 14 232 110 2 3 386 80 1 112 72 265
AUG 25 16 189 82 9 321 21 19 223 121 1 385 50 6 272 114 442 67 138 102 307
SEP 81 15 151 97 3 347 47 11 296 82 5 441 50 8 287 49 1 10 405 52 76 104 232
OCT 40 27 257 41 12 4 381 39 2 307 104 3 2 457 61 13 209 109 8 400 63 190 113 366
NOV 43 25 200 118 21 407 34 12 305 105 3 2 461 42 4 228 113 1 7 395 56 1 129 113 299
DEC 35 15 151 59 4 264 33 15 319 88 4 459 50 8 202 93 3 356 53 137 93 283
JAN 44 12 270 106 7 439 40 8 265 89 1 403 47 6 249 116 1 1 420 25 169 80 274
FEB 39 14 277 86 4 420 52 7 245 118 3 425 80 5 219 143 1 448 46 138 79 263
MAR 33 34 220 79 14 380 11 244 112 10 10 387 66 1 198 108 373 44 204 96 344
TOTAL 540 271 2727 1033 132 6 4709 399 162 3180 1201 73 17 5032 552 105 2838 1223 19 37 4777 716 15 1967 1142 1 1 3842
Source: NHS Highland Planning & Performance, 2017. Requested by Project Lead, Skye & Lochalsh Service Redesign Project
The numbers suggest a well utilised service in this population. There is marked variation in physiotherapy appointments over time. Relatively little of the
activity is multi-profession. The numbers seen are generally higher than in Broadford (see below). This suggests that future provision of this nature should
be considered in any future model of care for north Skye residents.
45You can also read