MANAGEMENT OF PATIENTS WITH SARS-COV-2 INFECTIONS AND OF PATIENTS WITH CHRONIC LUNG DISEASES DURING THE COVID-19 PANDEMIC (AS OF 9 MAY 2020)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
main topic
Wien Klin Wochenschr
https://doi.org/10.1007/s00508-020-01691-0
Management of patients with SARS-CoV-2 infections and
of patients with chronic lung diseases during the COVID-19
pandemic (as of 9 May 2020)
Statement of the Austrian Society of Pneumology (ASP)
Holger Flick · Britt-Madelaine Arns · Josef Bolitschek · Brigitte Bucher · Katharina Cima · Elisabeth Gingrich ·
Sabin Handzhiev · Maximilian Hochmair · Fritz Horak · Marco Idzko · Peter Jaksch · Gabor Kovacs ·
Roland Kropfmüller · Bernd Lamprecht · Judith Löffler-Ragg · Michael Meilinger · Horst Olschewski ·
Andreas Pfleger · Bernhard Puchner · Christoph Puelacher · Christian Prior · Patricia Rodriguez · Helmut Salzer ·
Peter Schenk · Otmar Schindler · Ingrid Stelzmüller · Volker Strenger · Helmut Täubl · Matthias Urban ·
Marlies Wagner · Franz Wimberger · Angela Zacharasiewicz · Ralf Harun Zwick · Ernst Eber
© The Author(s) 2020
Summary The coronavirus disease 2019 (COVID-19) has to be adapted during the pandemic but must still
pandemic is currently a challenge worldwide. In Aus- be guaranteed.
tria, a crisis within the healthcare system has so far
been prevented. The treatment of patients with com- Keywords SARS-CoV-2 · COVID-19 · Community
munity-acquired pneumonia (CAP), including SARS- acquired pneumonia · ARDS · Chronic lung disease
CoV-2 infections, should continue to be based on ev-
idence-based CAP guidelines during the pandemic; Introduction
however, COVID-19 specific adjustments are useful.
The treatment of patients with chronic lung diseases The Austrian healthcare system is currently con-
fronted with the challenge of the coronavirus disease
H. Flick · G. Kovacs · H. Olschewski F. Horak
Division of Pulmonology, Department of Internal Medicine, Allergy Center Vienna West, Vienna, Austria
Medical University of Graz, Graz, Austria
M. Idzko
B.-M. Arns Division of Pulmonology, Department of Internal Medicine
Department of Internal Medicine I, Hanusch Krankenhaus, II, Medical University of Vienna, Vienna, Austria
Vienna, Austria
P. Jaksch
J. Bolitschek · F. Wimberger Division of Thoracic Surgery, Department of Surgery,
Elisabethinen Hospital Linz, Linz, Austria Medical University of Vienna, Vienna, Austria
B. Bucher · K. Cima · H. Täubl G. Kovacs · H. Olschewski
Department of Pulmonology, Tirol Kliniken, Hospital Ludwig Boltzmann Institute for Lung Vascular Research,
Hochzirl-Natters, Natters, Austria Graz, Austria
E. Gingrich R. Kropfmüller · B. Lamprecht · H. Salzer
Private Practice in Pulmonology, Vienna, Austria Department of Pulmonology, Kepler University Hospital,
Medical Faculty, Johannes Kepler University, Linz, Austria
S. Handzhiev
Department of Pulmonology, University Hospital Krems, J. Löffler-Ragg
Krems, Austria Department of Internal Medicine II (Infectious Diseases,
Pneumology, Rheumatology), Medical University of
M. Hochmair
Innsbruck, Innsbruck, Austria
Respiratory Oncology Unit, Karl Landsteiner Institute of
Lung Research and Pulmonary Oncology, Department M. Meilinger · M. Urban
of Internal and Respiratory Medicine, Krankenhaus Department of Internal and Respiratory Medicine,
Nord—Klinik Floridsdorf, Vienna, Austria Krankenhaus Nord—Klinik Floridsdorf, Vienna, Austria
K Management of patients with SARS-CoV-2 infections and of patients with chronic lung diseases during the. . .main topic
2019 (COVID-19) pandemic. Since March 2020, inci- In order to attain all three of the aforementioned
sive adaptations to the thus far well-established med- goals, as far as the current resources (which are lim-
ical care structures and procedures have been rapidly ited due to the pandemic) allow, alignment of medical
implemented in order to be prepared for a high num- activities with existing evidence-based and well-im-
ber of acutely and severely ill patients suffering from plemented guidelines and their adaptation to the
COVID-19. Simultaneously, the speed of the spread currently difficult situation, as might be required in
of SARS-CoV-2 in Austria could be effectively reduced individual cases, should be continued. Especially
by radical, preventive social measures and a critical with respect to chronic diseases, acting with good
overburdening of the medical care centres has so far judgement and open communication with patients
been successfully prevented. and relatives are required to find feasible solutions.
In the current situation, there are three goals for
pneumologists: Management of patients with SARS-CoV-2
1. Optimal medical care for severely ill patients suffer- infections
ing from COVID-19 in order to achieve the lowest
possible SARS-CoV-2 mortality rate. The current epidemiological situation
2. Guarantee of an unchanged best possible medical
General facts on COVID-19
acute care of patients with other severe pulmonary
diseases (infections, asthma, chronic obstructive Since January 2020, the COVID-19 pandemic has
pulmonary disease (COPD), interstitial lung dis- spread rapidly worldwide. According to the World
ease (ILD) or cystic fibrosis (CF) exacerbations, pul- Health Organization (WHO) up to now 3,759,967
monary embolism, probable malignant pulmonary COVID-19 cases have been confirmed worldwide and
lesions, etc). 259,474 patients have already died [1].
3. Continuation of important medical treatment of Epidemiological information on and study results
people with underlying severe chronic diseases from COVID-19 must still be interpreted with cau-
(lung cancer, asthma, COPD, pulmonary hyperten- tion. They are subject to powerful dynamics and mul-
sion, ILD, CF, status post lung transplantation, sleep tifactorial influences, display a variable data quality
associated breathing disorders, etc.). These patients and due to differences in healthcare structures and
require special attention, because they could be epidemiological features allow only limited interna-
further threatened by a SARS-CoV-2 infection. tional comparisons. Therefore, as is common practice
in antibiotic stewardship, national and regional data
A. Pfleger · P. Rodriguez · V. Strenger · M. Wagner · should be systematically gathered and regularly ana-
E. Eber, Professor of Paediatrics, MD, ATSF, FERS () lyzed. This is the only way in which the current local
Division of Paediatric Pulmonology and Allergology, situation can be adequately assessed.
Department of Paediatrics and Adolescent Medicine, Like influenza, COVID-19 is a viral infectious dis-
Medical University of Graz, Auenbruggerplatz ease with a variable course (from asymptomatic to
34/2, 8036 Graz, Austria mild to severe to fatal). In Europe, most of the people
ernst.eber@medunigraz.at
positively tested show mild symptoms. Conversely,
B. Puchner more than 80% of the hospitalized patients suffered
Division of Pulmonology, Reha Zentrum Münster, Münster, from fever, cough and respiratory distress (Table 1;
Austria [2, 3]). In particular, older and comorbid patients are
C. Puelacher severely affected and present with severe community
Interdisciplinary Outpatient Sleep Laboratory, Telfs, Austria acquired pneumonia (CAP) with resulting hypoxia. In
C. Prior addition, possible COVID-19 specific phenomena are
Private Practice in Pulmonology, Innsbruck, Austria described, such as a reduced sensation of dyspnea,
whereby a respiratory deterioration may not be sub-
P. Schenk
jectively perceived for a long time, a lack of increase
Department of Pulmonology, Landesklinikum Hochegg,
Grimmenstein, Austria of the respiratory rate despite severe oxygenation dis-
turbance, and a temporary loss of smell and taste.
O. Schindler Due to the infectiousness of the pathogen, hospi-
Department of Internal, Respiratory and Critical Care
tal-associated SARS-CoV-2 pneumonia can also be ex-
Medicine, State Hospital II, Location Enzenbach,
Gratwein-Straßengel, Austria pected in the future.
According to the European Centre for Disease
I. Stelzmüller Prevention and Control (ECDC), severe COVID-19
Private Practice in Pulmonology, Salzburg, Austria
courses (need for hospitalization) have so far been
A. Zacharasiewicz observed in Europe in 28% of all cases; however, due
Department of Paediatrics, Teaching Hospital of the Medical to undetected mild courses, a high number of unre-
University of Vienna, Wilhelminen Hospital, Vienna, Austria ported cases and a higher rate of mild courses can be
R. H. Zwick assumed.
Therme Wien Med, Vienna, Austria
Management of patients with SARS-CoV-2 infections and of patients with chronic lung diseases during the. . . Kmain topic
Table 1 Symptoms of a SARS-CoV-2 infection [2, 3] Table 2 Hospital and ICU mortality rates for COVID-
Symptoms Positively tested people Hospitalized 19 worldwide as compared to other CAP-associated
(including mild cases) COVID-19 patients pathogens from solely European and North American stud-
ies
Fever/chills 49% 85%
Cough 24% 86% Hospital mortality ICU mortality
Shortness of – 80% CAP in general [7, 15–19] 12.9–14.1% 17.0–29.5%
breath S. pneumoniae [18, 20, 21] 8.0–12.0% 17.5–26.0%
Myalgia – 34% L. pneumonia [22–25] 3.9–18.5% 21.6%
Diarrhea 2% 27% Viral CAP in general [26, 27] 14.8% 22.0%
Nausea/vomiting – 24% Influenza A/B [10, 19, 28–31] 12.6% 17.1–41.2%
Sore throat 12% 18% COVID-19
Headache – 16% China (Wuhan)a [32–36] 10.7–21.9% 61.5%
Nasal congestion, 4% 16% USA (New York)b [37] 21.0% 78.0%
rhinorrhea
Europe (ECDC) [2] 14% –
Chest pain – 15% a
United Kingdom [26] – 34.8–46.8%
Abdominal pain – 8%
Spaina [38] – 29.2%
Fatigue 8% –
Italy (Lombardy)a [39] – 25.6%
Aching 7% – a
COVID-19 pandemic epicenters
b
Epicenter New York: on 23 April 2020 approx. tenfold more SARS-CoV-2
An average of 16% of hospitalized patients suffered infected people/100,000 inhabitants and 20-fold more COVID-19
deaths/100,000 inhabitants than in Austria at the same time [40]
from a very serious illness course (need for intensive CAP community acquired pneumonia, COVID-19 coronavirus disease 2019,
care or respiratory support) and COVID-19 hospital ECDC European Centre for Disease Prevention and Control, ICU intensive
mortality in Europe is currently at 14% [2]. care unit
There are relevant differences in Europe with re-
spect to COVID-19 deaths per 100,000 inhabitants.
With a comparable COVID-19 incidence (175–250 Hospitalization and mortality risk for COVID-19
cases/100,000 inhabitants), 7–9 deaths/100,000 have and community-acquired pneumonia due to other
been registered in Austria, Denmark, Germany, and pathogens
Liechtenstein and 31–39 deaths/100,000 in France, In order to realistically classify the current COVID-19
Sweden, and the Netherlands [4]. In Europe, the high- data, they must also be compared with the incidence
est burden of COVID-19 is currently reported from and course of other severe respiratory infections as
Belgium (455 cases/100,000 and 75 deaths/100,000 they occurred before the COVID-19 pandemic. In
inhabitants). In line with these figures, the European principle, pathogen-induced CAP which requires hos-
monitoring of excess mortality for public health action pitalization (hCAP) is frequent. With an incidence
(EuroMOMO) network has recorded an exceptionally of 296 hCAP per 100,000 inhabitants, an estimated
high pandemic-associated excess mortality rate in 26,222 patients with hCAP are treated in Austria ev-
certain European countries (UK, France, Spain, Bel- ery year and 2185 patients every month [7]. With an
gium, the Netherlands, Italy, and Switzerland), but average hospital mortality rate of 13% (Table 2) Austria
a significantly lower one in Austria and other coun- has 3409 (39/100,000) hCAP deaths per year and 284
tries, such as Denmark, Germany, Greece, Norway, hCAP deaths per month whereas COVID-19 caused
and Ireland [5]. 491 deaths per month during the peak phase of the
In Austria, 15,735 persons have so far been tested pandemic (27 March–27 April 2020). It can therefore
positive for SARS-CoV-2 and 615 (3.9%) have died be assumed that in Austria the pandemic caused at
from or with COVID-19. At present, 230 COVID-19 least a transient doubling of hCAP deaths/100,000 in-
patients are hospitalized (peak at the beginning of habitants.
March with 1010 hospitalized patients) and 79 are be- Influenza must be considered separately as the in-
ing treated in intensive care units (peak at the begin- fluenza case fatality rate is only partly caused by in-
ning of March with 267 ICU patients) (24–34% more fluenza pneumonia but 400,000 influenza-associated
than the European average). Thus, at the beginning of deaths are annually expected worldwide [8, 9].
March 26% (currently only 8%) of all available inten- The incidence of inpatient influenza cases in Eu-
sive care beds in Austria were occupied by COVID-19 rope ranges between 12–95/100,000 depending on the
patients [6]. Primary data on the number of patients season of the year and the effective vaccination cov-
previously treated in hospitals or intensive care units erage rate of the population, and for children in Aus-
and the mortality rates are currently unavailable in tria between 2002 and 2018 was 50/100,000 [10–13].
Austria. If this incidence is applied to Austria, assuming an
ICU rate of 7% and a hospital mortality rate of 4%,
during each influenza season there will be 1152–8416
inpatients, 81–589 cases requiring ICU, and 46–337
K Management of patients with SARS-CoV-2 infections and of patients with chronic lung diseases during the. . .main topic
Table 3 Comparison of comorbidities of patients who care. The significance of typical cardiopulmonary,
died from COVID-19 or other pneumonia pathogens (pneu- renal and metabolic comorbidities for the course of
mococcus, influenza, etc.) [41–44] CAP is well-known from influenza, pneumococcal
Comorbidities of deceased pa- COVID-19 Other CAP pathogens and legionella infections, and plays a decisive role in
tients (%) (%)
SARS-CoV-2 CAP to the same extent. Consequently,
Arterial hypertension 40–75 54 as is the case with other CAP pathogens, the risks
Diabetes 20–31 31 of hospitalization and mortality of SARS-CoV-2 CAP
Heart diseases 23–49 38 increase significantly from the age of 60 years and
Neurologic disorders 13 16–19 with the number of concomitant diseases (Table 3; [7,
Carcinomas 2–18 28 10, 15, 29, 41]).
Chronic renal insufficiency 23 13–27 Furthermore, the COVID-19 pandemic has clearly
Chronic lung diseases 8–19 6–24 demonstrated that the mortality rate of an acute in-
Dementia 18 28
fection is always determined by social and structural
factors (e.g. timely public health interventions to slow
CAP community acquired pneumonia, COVID-19 coronavirus disease 2019
the spread of a pandemic infection, prompt and flex-
ible structural adjustments to the healthcare system,
inpatient deaths in Austria. For the period from De- the number of immediately available intensive care
cember to April (influenza season), for Austria this or mechanical ventilation beds, capacity for isolation
means that there are 288–2104 inpatients and 20–147 and protection in the outpatient and inpatient area,
influenza cases requiring ICU per month. Due to short-term and effective medical staff training).
a very low influenza vaccination rate as compared to In some countries and regions there were acute
other European countries, higher rather than lower supply emergencies and therefore it can be assumed
rates can be expected for Austria. This assumption is that in these critical and partly catastrophic medi-
supported by calculations of the Agentur für Gesund- cal situations, not all acutely and severely ill patients
heit und Ernährungssicherheit (AGES), which based could be provided with the required timely and ade-
on the statistical model FluMOMO, supposes an aver- quate medical care. For example, the mortality rate
age of 2326 influenza deaths per year in the last 4 years in the primarily unprepared epicenter (Wuhan city
and thus 582 influenza deaths per month during the in Hubei province) was initially 12% and later in the
influenza season (COVID-19: currently approximately other Chinese provinces only about 1% [45]. This is
450 deaths per month, as of 19 April 2020) [14]. Ac- substantiated by excess mortality rates recorded by
cordingly, the annual wave of influenza in Austria is EuroMOMO in some countries that were severely af-
very likely to lead to a burden on the healthcare sys- fected by the pandemic.
tem comparable to that of the current COVID-19 pan-
demic. Therefore, systematic recording like that cur- SARS-CoV-2 in children
rently established for COVID-19 should also be intro- In an analysis of the first approximately 45,000 labo-
duced in Austria with respect to influenza-associated ratory-confirmed COVID-19 cases in China, children
deaths amongst hospitalized patients. 39.0 °C. Cough-
pathogens, and depending on the functionality of the ing and tachypnea are described in about 30–50%
healthcare system hospital mortality would appear to and pharyngitis (5–45%), rhinitis (10–30%), diar-
be comparable to that of other pathogen-induced CAP rhea (10–30%) and vomiting (6%) are significantly
(Table 2). less frequent [48–51]. Similarly to adults, laboratory
The CAP mortality risk is determined by the extent tests showed an increase in C-reactive protein (CRP)
of immediate lung parenchyma damage, secondary (moderate), transaminases, lactate dehydrogenase,
infections/complications, age and pre-existing co- D-dimer and creatine kinase, as well as leukopenia
morbidities, and the quality of the available medical (primarily lymphopenia) [51].
Management of patients with SARS-CoV-2 infections and of patients with chronic lung diseases during the. . . Kmain topic
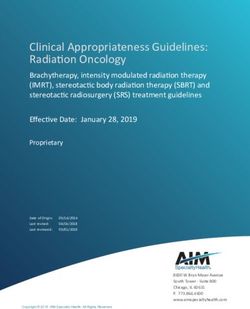
Fig. 1 Guidance for pa-
Acute respiratory symptoms (cough, shortness of breath, possibly fever) during the COVID-19 pandemic
tients regarding the severity
of a possible SARS-CoV-2
infection Mild symptoms Severe symptoms
• Previously healthy paents: • Previously healthy paents:
only light coughing, no shortness of breath severe coughing and shortness of breath
• Co-morbid paents (ComoP) with chronic • Co-morbid paents (ComoP) with chronic
cough/dyspnea: minor increase in coughing or cough/dyspnea: significant increase in coughing or
shortness of breath shortness of breath
9 Observe course of disease at home (a rapid 9 Call the 24h-hotline 1450 and follow the
deterioraon may occur 7-10 days aer the onset instrucons given
of symptoms; in this case immediate presentaon 9 In the case of ComoP, if necessary, addional
to hospital) telephone consultaon with the responsible
9 Seek informaon about current instrucons doctor‘s office/department
(Ministry of Social Affairs, AGES) and call the 24h- 9 When suspecng a life threatening situaon,
hotline 1450 present to hospital immediately
9 In the case of ComoP addional telephone
consultaon with the responsible doctor’s
office/department
Due to the less specific symptoms in children, it is Epidemiological outlook
difficult to make a reliable clinical diagnosis. Accord- As soon as the governmental pandemic prevention
ingly, especially in pediatric patients it is important to measures are eased, the Austrian healthcare system
test extensively for SARS-CoV-2 and to implement ap- must be further prepared for more than a renewed
propriate protective measures for medical personnel. increase in the number of COVID-19 cases. All other
Severe courses of respiratory insufficiency, or the respiratory infections (e.g. influenza, RSV, Pneumo-
need for intensive care constitute the exception [47]. coccus, Mycoplasma and Bordetella infections), the
Severe COVID-19 infections have been repeatedly sus- spread of which as in the case of SARS-CoV-2 was
pected in infants; however, these were mostly only concomitantly suppressed by the pandemic preven-
suspected cases (without SARS-CoV-2 testing). The tion measures, will also increase again.
authors assume that other viruses (especially respira- Within this context, the increased public awareness
tory syncytial virus [RSV]) might have caused a con- of potentially threatening infectious diseases created
siderable percentage of the severe courses of the in- by the COVID-19 pandemic is to be welcomed. As
fection [52]. Only a few pediatric COVID-19 deaths a next step, targeted reasonable, individual and social
have been reported in the literature so far [46, 47, 53]. preventive measures have to be developed and sup-
Due to the often milder disease course in children, ported. For example, these could not only include
it has been discussed whether oligosymptomatic and the individual willingness for protective vaccination
asymptomatic children could play an essential role in against influenza and other relevant pathogens but
the transmission, without this hypothesis ever having also a deeper understanding among the population of
been confirmed scientifically [52]. On the contrary, how to autonomously differentiate between harmless
a recent study from Iceland showed that when screen- infections that should be cured at home and serious
ing asymptomatic individuals, the proportion of virus acute illnesses that must be treated by a general prac-
excretion is threefold higher in 40–50 year-olds (ap- titioner or in hospital (Fig. 1).
prox. 1.5%) than in children/young people between
the ages of 10 and 20 years (approx. 0.5%). In a group Management of SARS-CoV-2 pneumonia
of more than 800 children under 10 years of age, not
a single child was tested positive [54]. Basic management of SARS-CoV-2 CAP
The SARS-CoV-2 infections in children with risk Serious SARS-CoV-2 pneumonia is a severe viral CAP
factors and underlying diseases (chronic respiratory (svCAP), the clinical presentation of which (acute on-
diseases such as cystic fibrosis, severe asthma, bron- set, bilateral pneumonia, progressive respiratory fail-
chopulmonary dysplasia as well as cardiac diseases, ure, high risk of mortality) is comparable to that of se-
primary and secondary immunodeficiencies, underly- vere influenza CAP (Table 2). In the current pandemic
ing malignant diseases, malnutrition, etc.) are rarely situation, the guarantee of sufficient medical care for
reported in pediatric analyses [46, 52]. Whether or such severe medical conditions is of crucial impor-
not it can be derived that these children are less at tance. Due to the frequency of svCAP (especially dur-
risk than adults with risk factors, or whether children ing the annual influenza season), the medical centers
from risk groups have more effectively been protected in Austria are familiar with the clinical management
against infection, remains unclear. of svCAP.
K Management of patients with SARS-CoV-2 infections and of patients with chronic lung diseases during the. . .main topic
Fig. 2 Guidance for physi-
Acute respiratory symptoms (cough, shortness of breath, possibly fever) during the COVID-19 pandemic
cians regarding the de-
gree of severity of a prob-
able SARS-CoV-2 infec- Mild disease (outpaent treatment possible) Severe disease (inpaent treatment required)
tion (adapted from [55,
a • So far healthy, or minor ComoP (ComoP/1a) • So far healthy, or minor ComoP (ComoP/1a)
pp. 151–200]). Robert
(prior confinement in bedmain topic
Fig. 3 Guidance for the
Indicaons for immediate intensive care management (ICU)
identification of critically
ill CAP patients during the o Severe O2-refractory hypoxia with imminent respiratory exhauson
COVID-19 pandemic (CAP
as an emergency) (adapted o Volume-refractory hypotension
from [55, pp. 151–200]).
a
Robert Koch Institute 9 Adherence to strict hygienic measuresa
guidelines on hygienic mea- 9 Mechanical venlaon (NIV or invasive venlaon)
sures within the framework 9 Vasopressive therapy and extended shock therapy
of the treatment and care
of patients with a SARS- 9 Anbioc therapy
CoV-2 infection: https://
www.rki.de/DE/Content/ An indicaon for intensified therapy and close monitoring exists, if ≥3 of 9 of the modified IDSA/ATS minor
InfAZ/N/Neuartiges_ criteria are met (increased risk for decompensaon requiring ICU):
Coronavirus/Hygiene.html.
CAP community-acquired o PaO2 ≤55 mmHg in room air or PaO2/FIO2 -rao ≤250
pneumonia, UD underlying o Respiratory rate ≥30/min
disease, IDSA/ATS Infec- o Mullobar infiltrates in the chest x-ray
tious Diseases Society of
o Newly developed disturbance of consciousness
America/American Thoracic
Society, NIV non-invasive o Systolic blood pressuremain topic
general more sensitive than those from nasopharyn- are available and that these drugs should be further
geal smears [57]; however, for reasons of hygiene nei- tested in RCTs. Nevertheless, the FDA has approved
ther sputum induction nor diagnostic bronchoscopy the use of chloroquine and hydroxychloroquine for
should be solely performed for confirming COVID-19. hospitalized COVID-19 patients (body weight >50 kg)
In intubated patients with an initially negative PCR outside of studies. For remdesevir, the FDA deci-
from the upper respiratory tract, further PCR testing sion was based on unpublished topline data from
in a lower respiratory tract specimen (e.g. tracheal se- a randomized, double-blind, placebo-controlled trial
cretions via closed suction system) is recommended. (NCT04280705) and from another open-label trial
This increases the diagnostic sensitivity and reduces (NCT04292899). At present, the European Medicines
the false negative test rate [58, 59]. Agency (EMA) has not granted approval for chloro-
A chest x-ray is neither sufficiently sensitive nor quine, hydroxychloroquine, remdesivir or any other
precise enough for the diagnosis of SARS-CoV-2 CAP; specific SARS-CoV-2 therapy or vaccination.
however, if the clinical signs and symptoms are spe-
cific and the PCR result is positive, x-ray findings typ- Systemic steroids
ical for COVID-19 (bilateral mostly ground glass-like With a few exceptions, a large number of studies
peripheral and basal consolidations) are sufficient. and meta-analyses showed no benefit and even an
In justified cases (as mentioned), severe cases, or increased fatality rate for systemic steroids in svCAP
for better differentiation of alternative diagnoses or or viral acute respiratory distress syndrome (vARDS)
complications, a chest CT scan is indicated [60]. Typ- [66–68]. Accordingly, the routine use of systemic
ical COVID-19 chest CT findings are bilateral, mul- steroids for the treatment of svCAP/vARDS includ-
tifocal, peripheral/subpleural and dorsobasal ground ing COVID-19 is not recommended [62]; however, in
glass opacities with or without consolidations. In the exceptional circumstances, systemic steroids may be
course of the disease, consolidation areas may in- considered in cases of viral CAP:
crease and a crazy paving pattern may occur. Sensitiv- According to the septicemia guidelines, hydrocorti-
ity, specificity, negative and positive predictive values sone is indicated for refractory shock with massive
of chest CT scans were described in a larger study hemodynamic instability [69, 70].
as 97%, 25%, 65% and 83%, respectively [61]. Thus, Severe COPD exacerbation: 0.5 mg prednisolone/
SARS-CoV-2 CAP can be detected sensitively by chest kg/day for 5–7 days, then stop.
CT, but the radiological changes may also result from Severe asthma exacerbation: 0.5 mg prednisolone/
other infections or diseases, or complications. kg/day for a maximum of 7 days, then slowly taper-
ing over a further 7 days.
Specific SARS-CoV-2 CAP therapy In the course of svCAP, systemic steroids may be
In general, treatment of a SARS-CoV-2 CAP, as of considered in suspected individual cases of or-
another bacterial or viral pneumonia, should follow ganizing pneumonia, postpneumonic interstitial
relevant guidelines (see above). Currently, there is pneumonia, hemophagocytic lymphohistiocytosis,
broad discussion about antiviral and anti-inflamma- or exacerbation of pre-existing pulmonary fibrosis.
tory treatment approaches that have yet to be suf-
ficiently validated (remdesivir, chloroquine, hydrox- Respiratory intensive care
ychloroquine, tocilizumab, recombinant angiotensin Patients requiring intensive care and ventilation
converting enzyme 2 and others). They should there- should be treated according to generally accepted
fore not be used as standard therapy in clinical rou- national and international recommendations. Thus,
tine. According to the WHO recommendations, their for the usually predominant severe oxygenation dis-
efficacy, safety and tolerability should first be tested order, an escalation from a ventilation mask with
in clinical trials, preferably randomized controlled reservoir (non-rebreather mask) via high-flow nasal
trials (RCT) [62, 63]. Until results from RCTs are oxygenation (HFNO) to non-invasive ventilation (NIV)
available, experimental therapies outside clinical tri- is recommended. In all international recommenda-
als must be extremely well justified and considered tions, special focus is placed on the protection of the
solely in selected individual cases (compassionate practitioner, in particular during measures such as
use). They should not be used uncritically, potentially intubation, NIV, HFNO, bronchoscopy or nebuliza-
harmful side effects must be considered and wherever tion [69, 71, 72]. Aerosol production is probably not
possible, their application should be documented in significantly increased with oxygen therapy, HFNO,
registers [64]. nebulization and NIV with non-vented systems, and
On 28 March 2020, the U.S. Food and Drug Ad- a significantly increased risk for personnel is presently
ministration (FDA) issued an emergency use autho- not assumed. In contrast, an increased risk for per-
rization for chloroquine/hydroxychloroquine, and sonnel has been shown for intubation, bronchoscopy,
on 1 May 2020 for remdesivir for the treatment of endotracheal aspiration and the use of vented sys-
COVID-19 [65]. The FDA points out that only in tems, or in the absence of a virus filter in the expi-
vitro or anecdotal clinical data and case series on ratory part of ventilation systems. A recent COVID-
the efficacy of chloroquine and hydroxychloroquine 19 position paper of the German Respiratory Society
Management of patients with SARS-CoV-2 infections and of patients with chronic lung diseases during the. . . Kmain topic provided a good overview of aerosol production and cruitment maneuvers and deterioration when exces- the resultant risk for practitioners [73]. sively high positive end-expiratory pressure (PEEP) is If available, HFNO and NIV of COVID-19 patients used (>10 cm H2O). The frequent severe oxygenation should be performed in negative pressure rooms. impairment is primarily due to vasoplegia with an In clinical practice, however, the number of nega- altered ventilation-perfusion ratio and microthrom- tive pressure rooms is limited in Austria, and HFNO botic events. and NIV are also acceptable in other facilities; how- In the L-type, O2/HFNO application, NIV or inva- ever, personal protection measures must be strictly sive ventilation with lower PEEP (6–10 cm H2O) and adhered to. prone positioning are usually effective. Higher tidal Since aerosol formation increases with augmented volumes are well tolerated without lung injury (venti- HFNO flow rate, the flow rate should be set as low as lator induced lung injury, VILI). possible and an oronasal mask (FFP1 mask) should be The H-type (high elastance) is characterized by applied to the patient’s face to reduce aerosol release. poor compliance (15 cm H2O), delay. but frequently low plateau pressures is useful. It can Irrespective of the type of ventilation, the use of be assumed that COVID-19 ARDS patients also benefit a respirator with a double-hose system and bacteria/ significantly from prone positioning according to the virus filter at the expiratory section of the breathing ProSEVA protocol [62, 75]. Recruitment maneuvers circuit is recommended. Ventilation with a single- (Lachmann maneuvers) can also be tried in patients hose system and vented systems should be avoided with the H-type [76]. due to aerosol formation. Ventilators for home venti- A transition from the L-type to the H-type is pos- lation, including obstructive sleep apnoea syndrome sible and may be recognized early due to increased (OSAS) therapy, should therefore not be used in the in- breathing effort (esophageal manometry, change in patient setting for SARS-CoV-2 positive patients, but CVP, assessment of the work of breathing). should be replaced by suitable ventilators, or an ap- According to present experience and autopsy re- propriate mask construction with a filter at the expira- ports, euvolemia is recommended because overhydra- tory valve. Air humidifiers of home ventilators should tion disproportionately worsens the respiratory situa- not be used [74]. If only ventilators with a single- tion. hose system and distal flow measurement are avail- To date, there is no substantial evidence for the ap- able, a filter must be installed at the patient side, with plication of the aforementioned experimental COVID- the resultant increase in airway resistance to be taken 19 therapies for patients in intensive care. Based on into account. If a continuous positive airway pressure the principle primum nil nocere, the use of insuffi- (CPAP) helmet is used, a filter must be attached to the ciently validated and unapproved medications is only expiratory part. recommended in clinical trials, or in compassionate For intubation, video laryngoscopy and rapid se- use programs. Moreover, potential side effects and quence induction with full relaxation are recom- possible interactions with standard intensive care mended to prevent aerosol formation, possible cough- medication have to be considered [77]. Equally, the ing of the patient and close proximity of the airway evidence for efficacy of a supportive therapy with operator to the patient’s head. Nebulization should be zinc, ascorbic acid or selenium is also insufficient. avoided in favor of the use of metered dose inhalers. The WHO guidelines for the treatment of COVID- According to the severity of the oxygenation impair- 19 incorporate the subject of intensive care and we ment, intubation and invasive ventilation are often recommend the regular updates to be followed and recommended for an oxygenation index (PaO2/FiO2) accounted for [62]. ≤200 [72]. Whether in such a case NIV is still feasi- Microcirculatory disturbances on a thrombotic ble as an alternative has to be individually assessed basis are assumed, and after a risk-benefit analy- for each patient. Depending on the underlying pul- sis a pharmacologic thrombosis prophylaxis is also monary disease and the clinical condition, with spe- indicated for the frequently occurring (moderate) cial regard to the load of the respiratory muscles, thrombocytopenia [78, 79]. the cooperation of the patient, strict protective mea- As occurs during other serious infections, COVID- sures for the medical staff, and the user’s experience 19 ARDS patients may develop a form of secondary with NIV are particularly important. In the presence hemophagocytic lymphohistiocytosis (sHLH). There- of ARDS and no improvement with NIV, intubation fore, a close watch must be kept for signs of a massive should not be delayed. hyperinflammatory response. Specific and adequately Two phenotypes of COVID-19 lung disease are dis- evaluated diagnostic criteria for COVID-19 sHLH are tinguished (Fig. 4): the L-type (low elastance) is char- not yet available [80, 81]. Diagnosis and classification acterized by good compliance, a poor response to re- of sHLH so far have been based on the practice-ori- K Management of patients with SARS-CoV-2 infections and of patients with chronic lung diseases during the. . .
main topic
COVID-19 with SpO260 mmHg
• pH >7.35
• Clinical improvement
a
Special consideraons for NIV: Protecve staff clothing! Tight-fing masks! Double-hose system with bacteria/virus filter! When using single-hose
systems, place filters at the proximal end close to the paent! Helmets only for isolated oxygenaon impairment and with a double-hose system.
Fig. 4 Guidance for the respiratory management of severe SARS-CoV-2 CAP
ented and evaluated HScore [82, 83]. A freely available NIV and aerosol therapy, this therapy increases virus
calculator can be found at http://saintantoine.aphp. transmission to the environment. In this case, an in-
fr/score/. There is no gold standard for the therapy dividual risk-benefit assessment must be performed;
of sHLH; the current evidence is based on case se- however, if possible, PAP should be continued under
ries, and RCTs have yet to be conducted. As with strict hygiene and isolation measures. According to
other non-COVID-19 associated sHLH, in individual current evidence, PAP does not exacerbate COVID 19
cases especially systemic corticosteroids, but also cy- infections. When single-hose systems and vented
closporine, intravenous immunoglobulins, anakinra, masks have been used so far, for the protection of
tocilizumab or other therapies may be considered the practitioner it is recommended to not use air hu-
[84]. midifiers if possible and change to non-vented masks
with a special exhalation valve and filter. If avail-
Aerosol therapy able, switching to a two-hose system is an alternative
During any form of inhalation or respiratory sup- option.
port therapy (nebulization, O2 via nasal cannula/
mask, HFNO, NIV), aerosol formation and thus an Bronchoscopy in COVID-19 patients
increased risk of infection for healthcare profession- Bronchoscopy is not recommended for the exclusion
als and patients must be expected (see also section or verification of COVID-19 (lack of therapeutic con-
on “Cardiorespiratory physiotherapy”) [85]. These sequence, unnecessary risk for personnel, and possi-
treatment forms should only be used if indicated, and ble risk of clinical deterioration due to bronchoscopy);
in view of the possible risk of contamination of the however, in exceptional situations, bronchoscopy may
surroundings by aerosols should either be applied be indicated in confirmed or suspected COVID-19 pa-
in a relatively restrictive manner or even avoided. tients (e.g. in immunosuppressed patients to exclude
Preferably, bronchodilators or corticosteroids should Pneumocystis pneumonia).
be inhaled with dry powder inhalers or (also with NIV Bronchoscopy involves the risk of aerosol forma-
or invasive ventilation) metered dose inhalers [86]. tion and thus a significantly increased risk of SARS-
For further details see the sections on “Respiratory CoV-2 infection for personnel present during the pro-
intensive care” and “Cardiorespiratory physiotherapy”. cedure. Bronchoscopy in intubated patients probably
has a lower transmission risk.
Hospitalized COVID-19 patients with sleep-related In accordance with international recommenda-
breathing disorders tions, if SARS-CoV-2 infection is suspected or con-
If a patient treated with positive airway pressure firmed, the following should be considered during the
(PAP) for a sleep-related breathing disorder devel- COVID-19 pandemic [87–89]:
ops COVID-19, it may be assumed that analogous to
Management of patients with SARS-CoV-2 infections and of patients with chronic lung diseases during the. . . Kmain topic
Fig. 5 Guidance on limi-
Resources for the medical care of seriously ill paents are sll largely available:
tations/withdrawal of ther-
• Decisions on medical care are generally made on the basis of the individual needs of each paent (paent-
apy (DNE, DNI, DNR etc.) oriented)
during the COVID-19 pan- • Intensive care is principally not indicated (applies generally without a pandemic situaon), if
demic. DNE do not esca- 9 the dying process has begun irreversibly,
late, DNI do not intubate, 9 from a medical point of view therapy is hopeless (no improvement or stabilisaon to be expected),
DNR do not resuscitate 9 survival would be linked to a permanent stay on an ICU,
9 the paent refuses intensive care.
If resources are increasingly exhausted, disaster medicine aspects have to be considered:
• Priorisaon takes place due to the obligaon to enable as many paents as possible to benefit from medical
care with the resources available
• Priorisaon is based on the criterion of clinical success (who has the higher probability of survival, or a beer
overall prognosis)
• Priorisaon is not jusfiable due to the principle of equality only within the COVID-19 paent group
• The mulple eye principle is applied in decision making (if possible, two experienced physicians and one
representave of the nursing staff)
See also:
• Österreichische Gesellscha für Anästhesiologie, Reanimaon und Intensivmedizin: hps://www.anaesthesie.news/wp-
content/uploads/gari_checkliste_triage_icu_final_26.3.2020.pdf und hps://www.anaesthesie.news/wp-content/uploads/gari_sop_triage_covid-
19_arge_ethik_final_26.3.2020.pdf
• Deutsche Interdisziplinäre Vereinigung für Intensiv- und No allmedizin u.a.: hps://pneumologie.de/fileadmin/user_upload/Aktuelles/2020-03-
25_COVID-19_Ethik_Empfehlung_Endfassung_2020-03-25.pdf
• Naonal Instute for Clinical Excellence: hps://www.eugms.org/fileadmin/user_upload/NICE_crical-care-admission-algorithm-pdf-8708948893.pdf
• Österreichische Palliavgesellscha:
hps://www.palliav.at/index.php?eID=tx_securedownloads&p=17&u=0&g=0&t=1588259787&hash=2327ddccbb3591eacb289a5f33267eb2eedca37c&fil
e=/fileadmin/redakteur/images/news/OPG.DokumentCOVID19.final.2020.03.20.pdf
Extremely restrictive indications for a bronchoscopy. Routine bronchoscopies in non-COVID-19 patients
Primary use of other sensitive diagnostic proce- (e.g. for the evaluation of pulmonary nodules/lesions
dures (e.g. obtaining tracheal secretions via a closed or interstitial lung diseases) should only be performed
suction system for microbiological testing including during the current pandemic if strictly indicated, with
SARS-CoV-2 PCR). increased personal protection measures (including
Bronchoscopy is indicated in emergency situations the use of FFP2 or FFP3 masks) and strict adherence
(e.g. life-threatening hemoptoe, high-grade airway to hygiene protocols.
stenosis, or foreign body aspiration), or if an alter-
native diagnosis can be verified, which would lead Therapeutic goals, treatment limitations and withdrawal
to a significant change in therapeutic management. of treatment in COVID-19 patients
Reduction of staff (bronchoscopist, bronchoscopy The ethical principles of intensive and palliative care
assistance, if necessary an anesthesia team) to apply equally to COVID-19 patients. Since in sev-
a core team. No students, basic or advanced trainees eral countries even increased intensive care resources
in the bronchoscopy suite. have been completely exhausted, guidelines for the
Strict personal protection for the entire team (dis- allocation of intensive care beds, triage and palliative
posable protective gown, disposable gloves, FFP3 care have been established in Austria [90, 91]. Based
mask, protective glasses/visor, hair protection). on the patient’s present state of health and the sever-
Strict attention to correctly putting on and taking ity of the infection and respect for the will of the pa-
off protective clothing. tient, capacities should be kept available for patients
If justifiable, rigid bronchoscopies with jet venti- for whom a higher probability of survival is predicted
lation should not be performed; however, should [92]. Not only is this a difficult undertaking due to
a rigid bronchoscopy be unavoidable, it should be the lack of validated predictive scores for COVID-19,
performed in an intubated patient with conven- but it also ignores the problem that patients without
tional ventilation and reduced aerosol escape, e.g. SARS-CoV-2 infection, or those with clinically silent
using a FLUVOG attachment (KARL STORZ SE & Co. infection, may require intensive care for other reasons
KG, Tuttlingen, Germany). (e.g. COPD exacerbation, myocardial infarction, poly-
Bronchial lavage should be performed as fraction- trauma, etc.) (Fig. 5). The German and British pro-
ated procedure (10 ml NaCl 0.9% for each fraction; fessional societies have developed recommendations
to reduce the transmission risk, the suction device regarding clinical-ethical decision-making [93, 94].
should be clamped after sampling or before discon-
nection).
Bronchoscopes are to be cleaned and disinfected in
a validated manner; there is no evidence that these
processes have to be changed for SARS-CoV-2.
K Management of patients with SARS-CoV-2 infections and of patients with chronic lung diseases during the. . .main topic
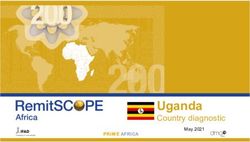
Fig. 6 Patient information:
The following measures are recommended to all paents with comorbidies and certain paents with chronic
preventive measures to pro-
lung diseases to prevent infecons, or in the case of an infecon, to reduce the risk of a severe course of the
hibit COVID-19 and/or a se- disease:
vere course of the disease
(recommendations for pa- 9 Adherence to recommended hygiene measures and restricon of social contacts for chronically ill paents (see
tients with underlying dis- RKI recommendaons regarding hygiene measures within the framework of the treatment and care of paents
eases) with a SARS-CoV-2 infecon: hps://www.rki.de/DE/Content/InfAZ/N/Neuarges_Coronavirus/Hygiene.html)
9 In the case of symptoms of an infecon contact with the health care system in due me (see figure 1)
9 Connuaon of the previous treatment of the chronic lung disease (no disconnuaon of medicaon due to
fears regarding SARS-CoV-2, confer with physician)
9 Cessaon of smoking
9 Connuaon of physical acvies in order to prohibit muscular decondioning
9 Compleon of the vaccinaon status with regard to pneumococcus at the next opportunity
9 As from November, vaccinaon against influenza
General management of patients with chronic – FEV1main topic
reslizumab, benralizumab, and dupilumab) should porarily worsen the respiratory symptoms of patients
also remain unchanged. According to present knowl- with chronic lung diseases, but the patients usually
edge a negative influence on the immune defence recover without consequences, including a complete
against SARS-CoV-2 is not expected from these bio- recovery of lung function.
logicals, but from oral corticosteroids (the therapeutic
alternative). Lung cancer
Under no circumstances should the drugs be dis-
continued on the assumption that they could impair There is currently no evidence to suggest that discon-
the immune system; a well-controlled asthma is the tinuing or interrupting anti-tumor therapy, such as
best provision for a mild course of a SARS-CoV-2 in- chemotherapy and/or immunotherapy is necessary.
fection. In addition, patients with asthma should pay Diagnosis and therapy should be continued according
close attention to any marked changes in their symp- to current standards; however, an individual decision
toms, especially to a sudden increase in breathless- should always be reached between the physician and
ness and newly occurring cough and fever. While the patient. For further details we suggest consulting
shortness of breath and cough are common in pa- the current ASCO, ESMO and DGHO/ÖGHO recom-
tients with asthma, fever may possibly indicate an mendations [96–98].
infection and should be taken seriously and further
assessed. Cystic fibrosis (CF)
COPD Adult CF patients are at risk of a possibly severe dis-
COPD patients should also adhere strictly to their ease course with SARS-CoV-2 infection. Apart from
regular therapy in order to prevent exacerbations. adherence to the generally valid prevention measures
If in the current situation an exacerbation occurs (hand hygiene, social distancing) adult CF patients
and requires medical consultation or hospitalization should stay at home and not seek social contacts in
(Fig. 1), patients cannot follow the most important professional or other types of social environment.
recommendations for the prevention of a SARS-CoV-2 Third parties should undertake shopping for food and
infection, namely staying at home and keeping at supplies of medications or respiratory physiotherapy
a distance to other people. In general, regularly ap- devices and the purchases should be placed in front
plied medication contributes to good disease control of the door.
and this also applies to COPD; thus, a high degree Furthermore, with respect to routine appointments
of adherence to therapy is of advantage especially in in outpatient clinics, contact should be made with the
this pandemic. Dyspnea and cough are typical COPD respective center in order to clarify which examina-
signs and symptoms; a sudden worsening of dysp- tions can be postponed, and which outpatient visits
nea and increased body temperature should prompt might take place under special conditions in the re-
suspicion of SARS-CoV-2 infection in these patients spective unit, or whether in individual cases the visit
(Fig. 1); however, fever could also be due to a COPD can be replaced by telephone consultations and in-
exacerbation. While systemic corticosteroids are cur- structions.
rently not recommended for COVID-19, their use for The CF centers are making every effort to suspend
the treatment of a common COPD exacerbation is outpatient visits that are not absolutely necessary
justified. as long as this does not cause disadvantages for the
patients. The usual therapeutic measures such as
Asthma and COPD patients with probable or confirmed chest physiotherapy, medical, and nutritional therapy
SARS-CoV-2 infection should be continued in a particularly careful man-
Patients with chronic respiratory diseases and a SARS- ner. In the case of clinical deterioration, signified by
CoV-2 infection have an equal chance of a mild fever and increased cough with or without respiratory
course of the disease that can be treated in domes- distress, it is advisable to contact the responsible CF
tic isolation. High grade fever should be avoided, centre by telephone, especially if a visit to the center
and sufficient hydration is recommended. Even in has already been scheduled.
stable phases of their disease, many COPD patients Clearly indicated inpatient i.v. antibiotic treatment
control oxygen saturation independently with finger courses should be administered in any case. If inpa-
pulse oximetry. If the oxygen saturation falls below the tient treatment of a SARS-CoV-2 infection is necessary,
usual range, medical care should be sought. If it is not a tailored antibiotic therapy adapted to the respective
possible to control oxygen saturation at home, breath- microbial spectrum will be initiated.
ing should be closely monitored. If dyspnea at rest A recently published article reported on ten SARS-
or during minimal physical activity increases, med- CoV-2 infected CF patients in Lombardy (out of a to-
ical care should be sought. Asthma patients should tal of 42,161 infected people in Lombardy and 101,739
document their symptoms and peak flow values in in Italy on 31 March 2020). In each case, the in-
the usual manner. Marked changes require medical fection had been transmitted by a family member.
attention. Generally speaking, COVID-19 can tem- In addition, five patients were reported from France,
K Management of patients with SARS-CoV-2 infections and of patients with chronic lung diseases during the. . .main topic
seven from the UK, five from Germany and three (in- Pulmonary hypertension
cluding one transplantation patient) from Spain (all
of them adults) [99]. In this limited number of pa- Patients with pulmonary hypertension, and in partic-
tients, the SARS-CoV-2 infection did not lead to a no- ular pulmonary arterial hypertension (PAH), belong
ticeable worsening of the underlying disease. The to the risk patient group; however, there are no data
CF centers are encouraged to report patients infected on the clinical course of COVID-19 in patients with
with SARS-CoV-2 to the European CF registry (ser- PAH. We are also unaware of any recent publications
vicedesk@ecfregistry.eu). that have investigated specific correlations between
this viral disease and pulmonary vascular disease.
Interstitial lung diseases As with other lung diseases, infection prevention
is of general importance in patients with PAH. De-
Due to structural lung changes, immunosuppressive pending on the severity of the underlying disease,
therapy, diffusion impairment with a frequently ex- even mild respiratory infections have been reported
isting need for supplemental oxygen and advanced to cause a temporary increase in the pressure load of
age, patients with interstitial lung disease (ILD) are the right heart up to clinical decompensation. A pneu-
a COVID-19 risk group. In order to minimize the risk monia caused by SARS-CoV-2 leads to a deterioration
of infection, ILD patients should adhere rigorously to of oxygenation, and the accompanying local and sys-
social distancing and other recommended protective temic inflammatory reactions also suggest the possi-
measures. Support from family members, neighbors bility of a worsening of the right ventricular function.
and aid organizations with respect to the organiza- In an autopsy study, an accumulation of marked right
tion of supplies of food and medication is essential, ventricular dilatation in deceased COVID-19 patients
although at the same time direct contact with people was described [100].
not living in the same household should be strictly As a consequence, the officially recommended
avoided. measures for social distancing appear to be of signifi-
Scheduling of appointments in ILD outpatient clin- cant importance for patients with pulmonary vascular
ics should be optimized in order to avoid long wait- diseases; however, this should not result in delayed
ing times and patient crowding. With written consent diagnostics. Suspected cases of acute pulmonary em-
and by means of technical support, alternatives such bolism should continue to be assessed and treated
as video chats can be considered for routine follow- according to guidelines as soon as possible in or-
ups. To minimize direct contact between physicians der that patients with a potentially fatal acute illness
and thus the risk of infection transmission, alternative are not harmed. Patients with suspected severe pul-
(e.g. digital) forms of communication should also be monary hypertension should also be subjected to
considered for multidisciplinary case discussions (ILD examinations including right heart catheterization
boards). without delay and treatment should be initiated in
For a timely diagnosis of a SARS-CoV-2 infection, accordance with the guidelines.
it is necessary to perform PCR testing as soon as new Patients with PAH therapy should adhere to the
signs and/or symptoms of illness develop. This allows generally recommended hygiene and other measures
the early detection of other causes of the symptoms and, if there are signs and/or symptoms of a SARS-
or an acute exacerbation and appropriate treatment CoV-2 infection, depending on the severity of the
can be initiated without delay. symptoms, they should contact their general practi-
Many ILD patients are treated with immunosup- tioner, consultant or specialist at the centre and start
pressive agents. Thus, in the case of a viral infection antibiotic therapy early.
more severe disease courses can be expected. Antifi- The need for a regular outpatient visit at the PAH
brotic therapy in fibrosing ILD and immunosuppres- centre should be assessed on an individual basis. Pa-
sive therapy in inflammatory ILD should be continued tients should take precautionary measures with regard
in ILD patients, who are not suffering from COVID-19, to their specific PAH medication (supplies for at least
in order not to risk ILD exacerbation. If a SARS-CoV-2 8 weeks) and, if necessary, in the case of supply short-
infection is confirmed, an individual assessment must ages duly contact the PAH centre. Close telephone
be made as to whether immunosuppressive therapy contacts with patients are recommended and should
should be reduced or temporarily discontinued. be practiced by the centers.
Treatment of patients with advanced ILD and
COVID-19 is likely to generate ethical concerns and Pulmonary rehabilitation and smoking cessation
difficult therapeutic decisions may be required. An therapy
open discussion of the issues with patients and their
families and the definition of treatment goals may The Pension Insurance Fund (Pensionsversicherungs-
be necessary. For patients with advanced ILD and anstalt, PVA) is classified as being part of the criti-
COVID-19, palliative measures should also be consid- cal infrastructure of Austria. It is legally obliged to
ered. maintain services and in particular those of its own
rehabilitation centers. In the health service area, the
Management of patients with SARS-CoV-2 infections and of patients with chronic lung diseases during the. . . KYou can also read