Leucemie Secondarie Maria Teresa Voso Dipartimento di Biomedicina e Prevenzione Università di Roma Tor Vergata Rome, Italy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Leucemie Secondarie
Maria Teresa Voso
Dipartimento di Biomedicina e Prevenzione
Università di Roma Tor Vergata
Rome, Italy
30 min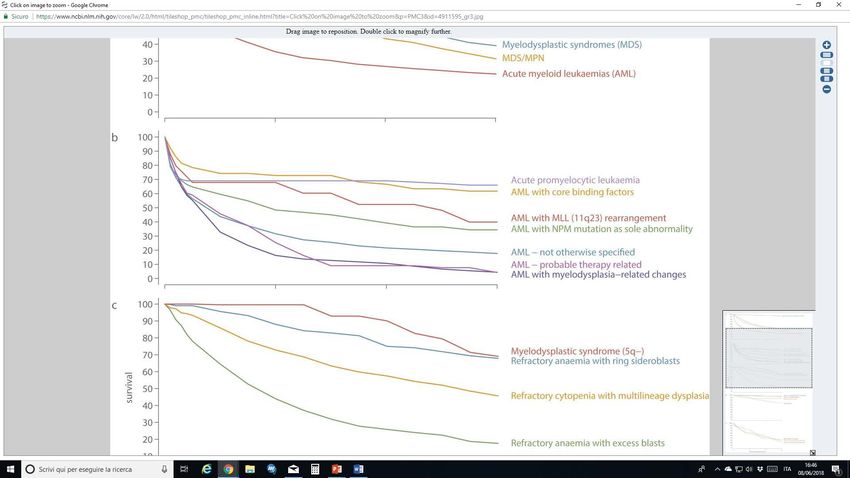
Learning objectives
ü Definition and prevalence of secondary leukemias
ü Clinical characteristics
ü Pathogenesis
ü Treatment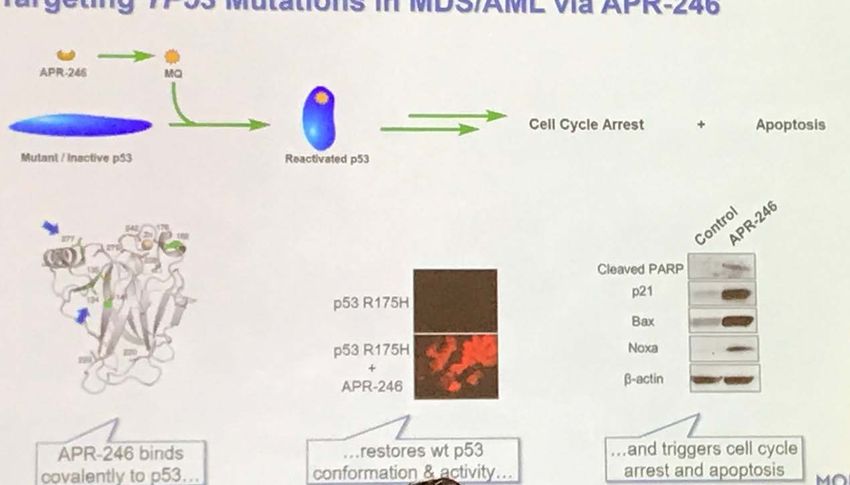
Who has Secondary Leukemia?
Patient
Definition
• Elderly Disease
• Evolution of a previous
• Inherited risk factors (SNV, • AML-MRC
myeloid neoplasia
• MDS germ-line mutations) • Complex karyotype
• MPN • Frequent CHIP • -7 or del(7q)
• Frail (previous CHT/RT) • -5 or del(5q)
• AML with myelodysplasia-
• Organ dysfunction • Isochromosome 17p
related changes (MRC)
• Remission status of previous • 11q23
• Therapy-related myeloid disease • TP53 mutations
neoplasms
• Time from previous disease
Prevalence of s-AML
German/Austrian AMLSG Registry (2012-2014)
n=3525 AML
inv(16)
t(8;21) * CEBPA-mut
t(15;17) t-AML
* About 1%: s-AML and t-AML 28%
t(9;11) Secondary
t(11q23)
t(6;9)
inv(3)/t(3;3)
NOS
NPM1-mut
Nagel et al, Ann Hematol 2017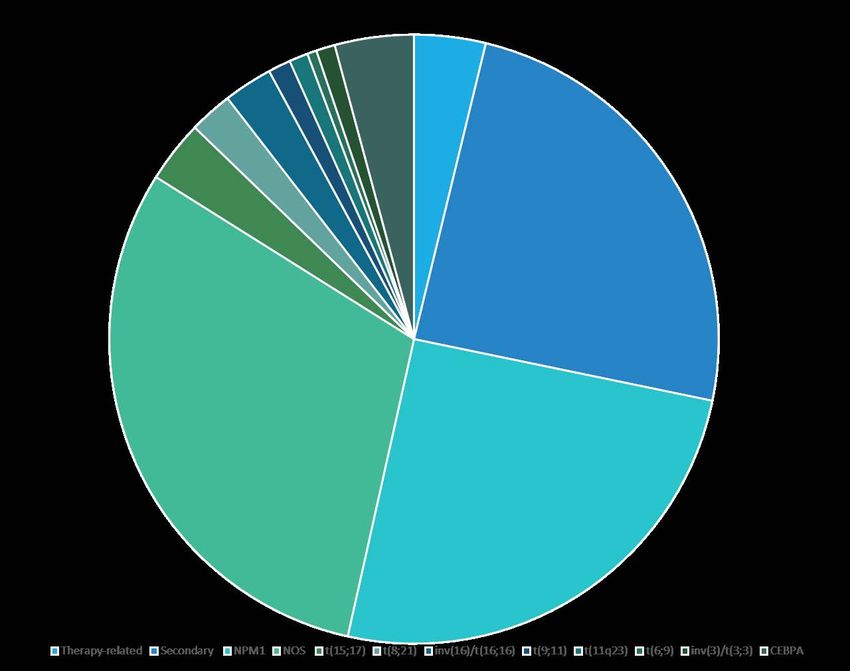
AML with MRC Cytogenetic abnormalities sufficient to diagnose
AML with MRC
(>20% BM or PB blasts and no prior therapy)
ü Detection of multilineage dysplasia (defined as the
presence of 50% or more dysplastic cells in at least 2 cell lines)
ü History of MDS
ü Presence of an MDS-related cytogenetic abnormality
with 1 exception: del(9q) because of its association with NPM1
or biallelic CEBPA mutations (and its apparent lack of prognostic
significance in those settings)
ü Absence of NPM1 or CEBPA bi-allelic mutations
Arber et al, Blood 2016
Le alterazioni “mielodisplasia relate” nelle leucemie acute MRC devono essere presenti in : A) > 15% dei progenitori midollari B) > 50% dei progenitori midollari in almeno 2 linee C) >20% dei progenitori midollari D) > 30% dei progenitori midollari
Therapy-related Myeloid Neoplasms
Karyotype
Italian Multicenter Registry
May 2009- Sep 2013
277 t-MN
57% WHO-defined AML, 43% MDS
Fianchi et al, Am J Hematol 2015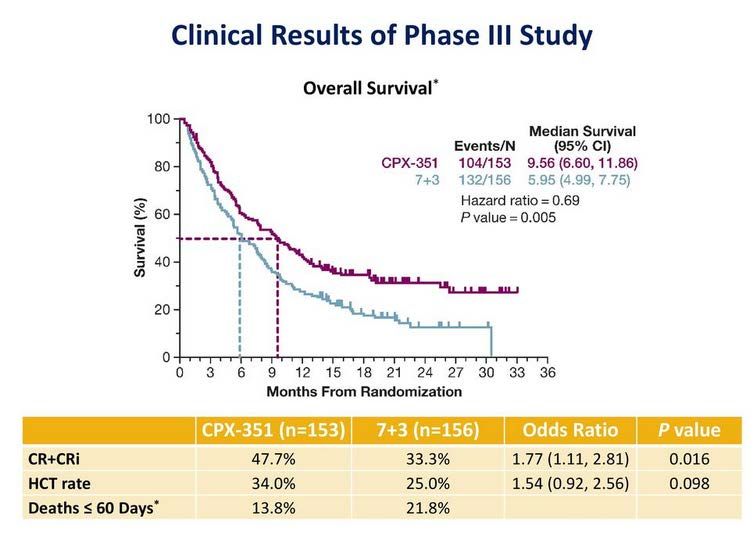
Primary Diseases
SEER Registry
n = 801 t-MN
Italian Registry
n = 277 t-MN
GI Ca
Others
Lymphoma
Autoimmune
diseases
Genito-Urin.Ca
Breast Ca
Mc Kerney et al., Nature Rev Cancer 2017 Fianchi L et al, Am J Hematol 2015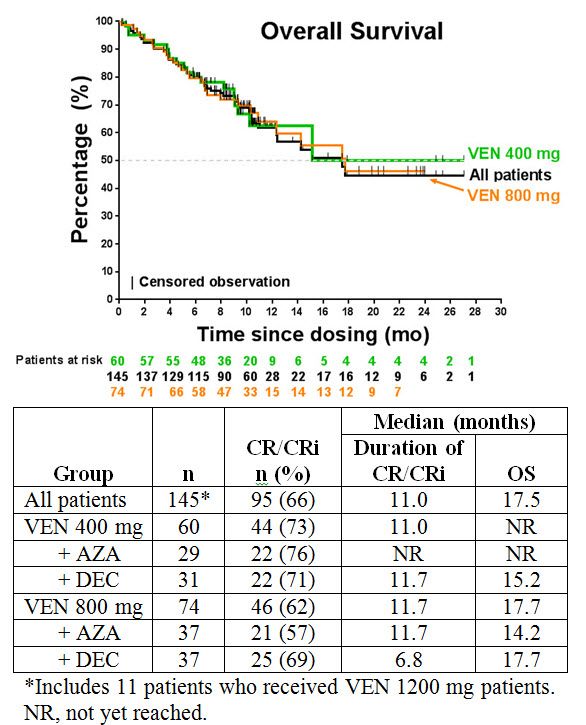
Characteristics of t-MDS
(n= 1245 pts from IWG)
Type of primary Tumor Time from primary DG Type of treatment Type of CHT received
to MDS (years) received (83% of pts)
Data from Kuendgen et al (IWG), Leukemia 2020 (in press)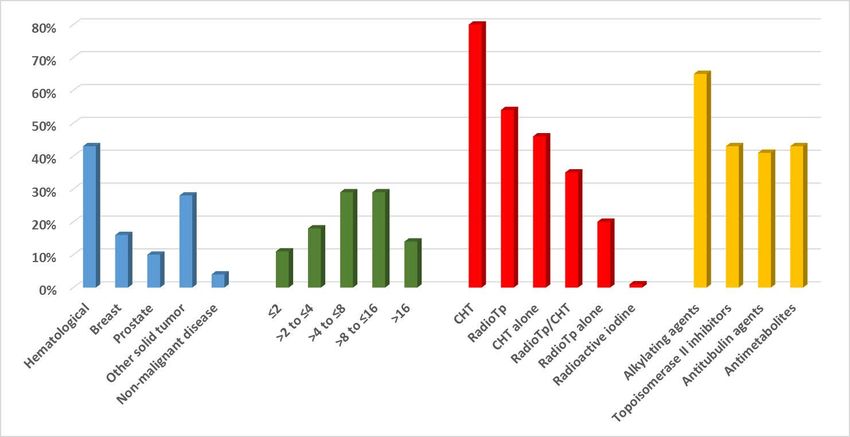
Differences between t-related and dn-MDS
(n= 1245 t-MDS* vs 4593 dn-MDS, all pPrognostic scores in t-MDS
ü Patients with t-MDS are characterized by a higher-proportion of high/very-high R-IPSS
ü Largely due to a higher prevalence of poor-very-poor karyotypes
Kuendgen et al (IWG), Leukemia 2020 (in press)Survival of t-MN according to IPSS-R
ü Survival in t-MDS patients is inferior to that of de novo MDS in the same
prognostic subgroup
ü Particularly for very-low/low/intermediate R-IPSS categories
Kuendgen et al (IWG), Leukemia 2020 (in press)Type of Treatment and prevalence of t-MN
in Lymphomas
Non-Hodgkin
Hodgkin lymphoma
lymphoma
ABVD (< 1%) R-CHOP (5%) HDT (2-3%)
Flud+RadioIT (>5%)
Bendamustine (about
2%)Update from large studies
Time from
Patients (n) primary DG to t- Association with
t-MN Reference
Median F-up MN t-MN onset
(Median)
11952 pts Age at HL DG: Eichenauer et al.,
0.9% 31 months
F-Up: 72 mos 43 vs 34 yrs (p=0,001) Blood 2014
Hodgkin
lymphoma 16 trials, 9498 pts Eichenauer et al.,
RT/CHT vs CHT (p=0.037)
(1994-2007), 0.7% Haematologica
Std Dose vs Intensified (p=0.0028) 2017
F-up: 7.4 yrs
460 pts Len vs Holstein et al,
8% vs About 60
placebo after HSCT Lenalidomide for SM CALGB, Lancet
1% months Hematol 2017
Multiple (231 Len)
Myeloma 3.1% Palumbo et al,
7 Trials : 3218 pts Cum Incidence Lenalidomide plus Melphalan (vs
vs Lancet Oncol
(2620 len vs 598) at 5 yrs other combinations 2014
1.4%
CHT, HR = 1.38
RT/CHT, HR = 1.77 Calip et al, Breast
Breast Cancer 56251 pts 1.2% 3.2 yrs RT alone, HR = 1.08 Cancer Res Treat
G-CSF, HR= 1,47 2015
Alkyl/Cycloph + G-CSF, HR= 1,86t-MN in Multiple Myeloma
All t-MN
Gertz et al., Blood 2014t-AML with Recurrent Translocations
Therapy-related Acute Promyelocytic Leukemia
Italian Multicenter Registry
on Secondary Leukemias PETHEMA Registry
16 t-APL of 157 t-AML (10%)
146 sAPL of 1616 APL (8%)
May 2009 - Sep 2013
Fianchi et al. Am J Hematol 2015 Courtesy of Sanz, Montesinos et al, unpublishedOutcome of t-APL
Treatment Response Intensively treated patients,
excluding treatment with ATRA only
CTX/ATRA ATO/ATRA CTX/ATO ATRA ATRA only
% (N)
n=53 n=24 n=19 n=7
Event-free survival (%)
CR 78% (40) 100% (23) 95% (18) 57% (4)
P=0.045
PR 10% (5) – – –
ED 12% (6) – 5% (1) 43% (3)
v Like t-APL, inv(16)/t(16;16) or t(8;21) t-AML have outcomes similar to
de novo counterpart when intensive treatment is feasible.
Kayser et al, Leukemia 2017Le neoplasie mieloidi therapy-related secondarie a farmaci inibitori delle topoisomerasi presentano frequentemente: A) una fase MDS B) Traslocazioni ricorrenti C) cariotipo complesso D) delezioni del 5q
Pathogenesis
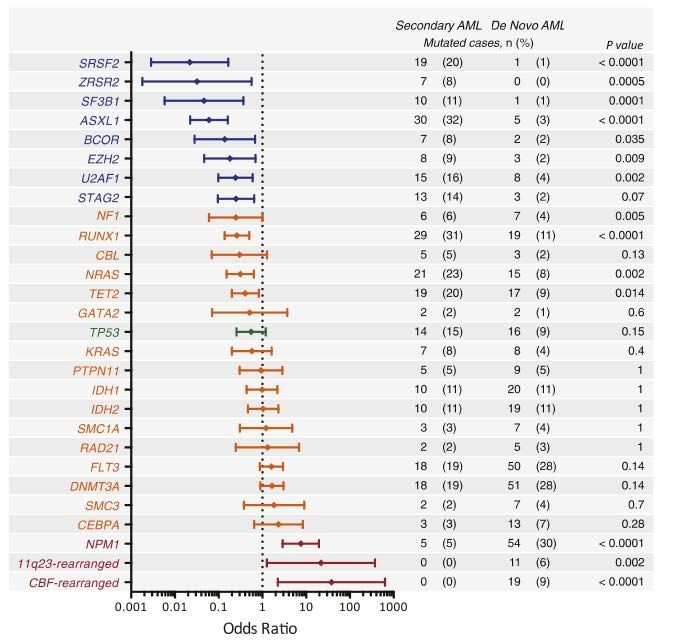
Prevalence of Somatic Mutations
AML MDS
Secondary De novo p
Epigenetic / Splicing
Secondary De novo Primary Therapy-related
Lindsley et al, Blood 2015 Lindsley et al, NEJM 2017CHIP is a predisposing factor for t-MN
Primary disease t-MN (n) CHIP at DG (%) Reference
7 Lymphoma 7 4 TP53-mut (57%) Wong, Nature 2014
9 Lymphoma, 3 APL, 2 AML 14 3 (21%) Fabiani, Oncotarget 2017
8/13 (62%) vs 15/56
6 Hemat and 7 Solid T. 13 Gillis, Lancet Oncol 2017
(27%) controls
10/14 (71%) vs Takahashi, Lancet Oncol
14 Lymphomas 14 2017
17/54 (31%)
18 HSCT (13 lymphoma, 5
18 7/10 in PBSC Berger, Blood 2018
PC diseases)Model of Therapy-related Leukemogenesis
Germ-line Variant
(Cancer susc. Gene, SNP?)
Second - Third hit
Chemotherapy / Genetic / Epigenetic
Radiotherapy Environment
t-MN
Environmental
Factors
CHIP
22Treatment and Outcome
Survival in Acute Myeloid Leukemias
UK’s population-based Haematological Malignancy (2004-2015)
3-year Survival Estimates
Roman et al, Cancer Epidemiol 2016Survival in s-AML
Swedish AML Registry
Overall Survival (N=3363) Survival by s-AML Group
De novo De novo
vs vs
t-AML (p) AHD (p)
Intensive treatment All agesTreatment Options in t-MN
Overall survival
BSC (58)
CHT (83)
AZA (50)
Allo-SCT (42)
Auto-SCT (11)
Fianchi et al, Am J Hematol 2015 Ok et al, Leukemia 2014Hypomethylating Treatment
Azacitidine in t-MN
Response %
Survival proportion(%)
CR 21
PR 4
HI 17
SD 31
Progression 27
Time from AZA start (months)
v Survival with Decitabine in t-MN similar to de novo MDS/AML
Fianchi et al, J Hematol Oncol 2012Hypomethylating Treatment
Azacitidine in AML-MRC
* Overall survival analyses not performed for «prior history of MDS only» cohort due to small sample size
Seymour et al, BMC Cancer 2017CPX-351
v100 nM bilamellar liposomes
v5:1 molar ratio of cytarabine to daunorubicin
vDrug exposure maintained for 7 days, selective uptake by leukemic cells vs normal cells in mice
Phase II trial of CPX-351 randomized vs 3+7 in Phase III trial of CPX-351 randomized vs 3+7 in
older adults with untreated AML (n=126) secondary AML (n=309)
v No significant differences in CR, EFS and v Significantly improved CR + CRi with CPX-351
OS in the whole cohort
Lancet et al, Blood 2014 Lancet et al, JCO 2018New Drugs for Pts Unfit for Intensive Treatment: ABT-199
ü Phase 1 study: dose escalated ABT-199 combined with AZA SD or DEC 5 days
ü AML, ineligible for STD CHT, intermediate or adverse cytogenetics
ü Major SAE: febrile neutropenia and hematologic toxicity
Di Nardo et al, Lancet Oncol 2018Prognostic Factors for ABT-199 Response and Survival
Evaluable for Median Duration of
Response/OS CR/CRi CR/CRi, Mos Median OS, Mos
Subgroup n (%) n (%) (95% CI) (95% CI)
All patients 145 97 (67) 11.3 (8.9, NR) 17.5 (12.3, NR)
Cytogenetic risk *
Intermediate 74 (51) 55 (74) 12.9 (11, NR) NR (17.5, NR)
Poor 71 (49) 42 (60) 6.7 (4.1, 9.4) 9.6 (7.2, 12.4)
Age
≥75 years 62 (43) 40 (65) 9.2 (6.4, 12.5) 11 (9.3, NR)Targeting TP53 mutations in AML via APR-246 Apr-246 binds Restores TP53 Triggers cell cycle arrest covalently to TP53 conformation and activity and apoptosis
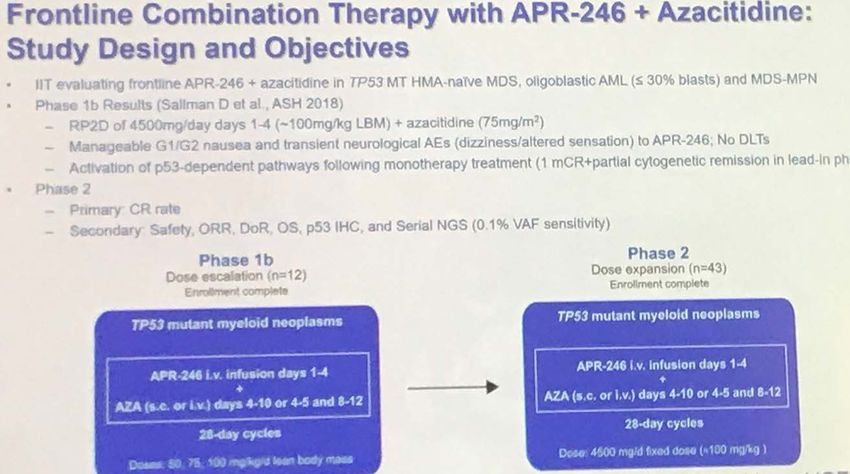
Phase 2 Results of APR-246 and Azacitidine (AZA) in Patients with TP53 mutant
Myelodysplastic Syndromes (MDS) and Oligoblastic Acute Myeloid Leukemia (AML)
Sallman et al. ASH 2019v 40 pts had MDS, 11 AML-MRC and 4 CMML/MDS-MPN;
v 85% had complex cytogenetics and 33% TR-MDS/AML, all TP53 mutated.
ORR (n= 45 pts, median follow-up: 10.5 months) Tx-related adverse events
G1/G2
v Median time to response: 2.1 months (0.1-5.4), median duration of response: 6.5 months.
v ORR rate: 88% for MDS/AML and 75% for MDS/MPN
v Complete and partial cytogenetic response: 41% (n=18) and 18% (n=8) of pts
Sallman et al. ASH 2019Key messages ü Le neoplasie mieloidi therapy-related presentano elevata complessita’ genetica, con mutazioni distintive rispetto alle forme de novo ü Fra i fattori predisponenti troviamo frequentemente mutazioni associate alla CHIP ü Possono insorgere in seguito a chemio- o a radioterapia, anche se la chemioterapia ha un ruolo dominante ü Le t-MN sono caratterizzate da prognosi avversa rispetto alla controparte de novo, ad eccezione delle t-AML con traslocazioni ricorrenti, che trattate adeguatamente, hanno andamento clinico favorevole (es: APL) ü La chemioterapia non risulta efficace, ma nuovi farmaci quali il CPX-351, la combinazione di Azacitidina/ ABT-199, e l’inibitore di TP53 APR-246 mostrano risultati molto incoraggianti
You can also read