Issue XIV. November 2017 - Col legi de Fisioterapeutes de ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Issue XIV. November 2017 PHYSIOTHERAPY UPDATES

PHYSIOTHERAPY UPDATES
Table of contents
Edited by TABLE OF CONTENTS
EDITORIAL Page 4
Col·legi
de Fisioterapeutes
Scientific evidence and art in physiotherapy. Are they compatible?
de Catalunya
Ramon Aiguadé, treasury manager
ADMINISTRATION BOARD and responsible for the Scientific Journal
Dean: Mr Manel Domingo
Vice-dean: Ms Mònica Rodríguez
Secretary: Mr Gabriel Liesa
ORIGINAL ARTICLES Page 5 to 16
Vice-secretary: Ms Eva Cirera
Treasury manager: Mr Ramon Aiguadé Results of exercise in breast cancer survivors
Chairpersons: Mr Juanjo Brau, Ms Eva
Hernando, Mr Francesc Rubí, Ms Marta Jiménez Montes M
Sala, Ms Patricia Vidal, Ms Núria Coral
Fascial treatment in sports. A bibliographical review
SCIENTIFIC COMMITTEE Navarro R, Simon M, Casasayas O, Miguel M, Ortiz S,
Mr Manel Domingo, Mr Ramon Aiguadé, Blasi M, Álvarez P, Pérez-Bellmunt, A
Mr Francesc Rubí, Ms Mercè Sitjà
COORDINATOR AND TRANSLATED ARTICLES Page 17 to 31
LANGUAGE ADVISOR
Ms Marta Bordas
Assessment of electromyography activity of pelvic floor muscles
SCIENTIFIC TRANSLATOR
during postural exercises using Wii Fit Plus© virtual video games.
Ms Carme Sanahuges
Analysis and perspectives in re-education.
DESIGN AND LAYOUT Steenstrup B, Giralte F, Bakker E, Grise P
Mr Jordi Rodríguez Ramos
Balance and Mobility in Community-Dwelling Older Adults: Effect of
El Col·legi de Fisioterapeutes de
Catalunya does not necessarily agree Daytime Sleepiness
with the opinions expressed in the Tyagi S, Perera S, S. Brach J
signed articles whose responsibility
lays exclusively on their authors.
ABSTRACTS Page 32 to 41
Main office
C/Segle XX, 78. 08032 Barcelona
Tel. 93 207 50 29 Fax. 93 207 70 22 Effects of an ischiosural elasticity programme on the activation and
www.fisioterapeutes.cat fatigue of posterior stabilizing muscles in the lumbopelvic region
cfc@fisioterapeutes.cat Monné-Guasch L, Girabent-Farrés M, Germán-Romero A,
Herrera-Pedroviejo E, Moizé-Arcone L, Rodríguez-Rubio PR
Manuscripts sent to:
Col·legi de Fisioterapeutes de
Catalunya. Revista Científica. Interaction of stabilizing muscles in the
C/Segle XX, 78. 08032 Barcelona pathophysiology of stress urinary incontinence
revistacientifica@fisioterapeutes.cat Fayt C, Bakker E
LD: B-16049-2012
ISSN: 2014-6809
The validity of O’Sullivan’s classification system (CS) for a sub-group
for a sub-group of NS-CLBP with motor control impairment (MCI):
Overview of a series of studies and reviewof the literature
Dankaerts W, O’Sullivan P
Stakeholder involvement in the design of a patient-centered compa-
rative effectiveness trial of the “On the Move” group exercise
program incommunity-dwelling older adults
S. Brach J, Perera S, Gilmore S, VanSwearingen JM,
Brodine D, Wert D, Nadkarni NK, Ricci E
Col·legi de Fisioterapeutes de Catalunya
EC-5221 / 10 MA-1681 / 10
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
2
PHYSIOTHERAPY UPDATES
Table of contents
Neurodynamic treatment improves leg pain, back pain,
function and global perceived effect at 4 weeks
in patients with chronic nerve-related leg pain
Hall T, Coppieters MW, Nee R, Schäfer A, Ridehalgh C
Effects of standing programmes in abduction on the prevention
of hip dysplasia in children with spastic diplegic cerebral palsy
Macias Merlo L
Open kinetic chain versus closed kinetic chain
therapeutic exercises after anterior cruciate ligament
ligamentoplasty: an evidence-based approach
Calvo Sanz J, Rodriguez Rubio PR, Garcia Tirado JJ,
Girabent Farrés M, Monné Guasch L, Monné Cuevas P
LEARN HOW TO DO RESEARCH Page 42 to 49
Bibliographical citations and bibliographical reference managers
Sánchez Aldeguer J, Esquirol Caussa J, Dalmau i Santamaria I,
Bayo Tallón V, Sánchez Padilla M
Critical appraisal of scientific texts
Bayo Tallón V, Sánchez Padilla M, Sánchez Aldeguer J,
Esquirol Caussa J, Dalmau i Santamaria I
POSTERS Page 50 and 51
Bibliographical review of electrical stimulation
in sleep apnoea-hypopnoea syndrome
Bagué Cruz, A
CONGRESS REVIEW Page 52
XXII SEPAR Joint Winter Meeting
Castillo Sánchez, I
FINAL YEAR PROJECT Page 53 to 59
Treatment of spasticity in cerebral palsy: a systematic review
Biosca Sellarès M, Muñoz Benito C
AGENDA Page 60
Col·legi de Fisioterapeutes de Catalunya
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
3Col·legi
de Fisioterapeutes
de Catalunya
PHYSIOTHERAPY UPDATES
EDITORIAL
SCIENTIFIC EVIDENCE
AND ART IN PHYSIOTHERAPY.
ARE THEY COMPATIBLE?
Ramon Aiguadé
Treasury manager and responsible
for the Scientific Journal
Some days ago, I tweeted that physiotherapy is a form why it is important to join physiotherapy and art. Becau-
of art based on scientific evidence. Some colleagues se we must base our treatment on what scientific evi-
commented on the incompatibility of the two concepts: dence shows to be the most effective way of treating our
scientific evidence and art. In my view, healthcare patients but we cannot forget about our communication
sciences have to be applied with art. If we base our pro- skills, we cannot forget to transmit what we are doing.
fessional practice only on scientific evidence, we run the
risk or falling into an impersonal and cold practice. We Our profession is constantly growing and scientific evi-
know that this human touch is essential. Several factors dence in physiotherapy is growing exponentially. The
would influence this: future is ours. Let’s grab it!
• We spend more time with our patients than other This new issue of our journal presents some origi-
healthcare providers. nal articles on breast cancer and fascial treatment
in sports; translated articles and abstracts by some
• The duration of the processes that we treat tend to of the participants in the International Physiotherapy
last several weeks or months. Congress #FTP18 that will be held in Barcelona on
4th and 5th May. You will also find the section “Learn
• The personal contact involved in the treatments how to do research”, little information capsules on re-
we provide. search methodology. There is a very interesting poster
on electrical stimulation in sleep apnoea-hypopnoea
Physiotherapy is a form of art because it is closely re-
syndrome, a physiotherapy degree final project (TFG)
lated to communication and to the capacity of doing
about the treatments to improve spasticity in patients
things and doing them well. Art is perceived differently
with cerebral palsy, and a summary of the SEPAR Con-
by each and every one of us. A work of art some of us
ference. As usual, you can have a look at the agenda
love is rejected or not understood by others.
of conferences and meetings that will take place in the
Physiotherapy is not detached from this reality. When next months, which are really interesting and engaging.
we treat our patients, we establish a relationship with
If you have done a master’s course and would like to
them, we communicate with our hands, we transmit our
send us your master’s degree final project (TFM), do not
mood… and this is something we physiotherapists do
hesitate to send it to us so that we can help you to dis-
quite well. A physiotherapy treatment can be, for many
seminate your work, which will surely contribute signifi-
of us, a fully justified action but a colleague may think
cantly to the improvement of our profession. Let’s go on!
this treatment could be improved complementing it with
a different manoeuvre or technique. This is the reason
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
4Col·legi
de Fisioterapeutes
de Catalunya
PHYSIOTHERAPY UPDATES
ORIGINAL ARTICLE
RESULTS OF EXERCISE IN BREAST CANCER SURVIVORS
Magdalena Jiménez Montes
Master’s degree in chest physiotherapy. Degree in physiotherapy
ABSTRACT
Aim. Evaluating the results of exercise in breast cancer Conclusion. The results obtained are published in a
survivors, taking the following variables into accou- table, observing a significant improvement in terms of
nt: quality of life, fatigue, depression, anxiety, and quality of life, fatigue, as well as in other parameters.
adherence to exercise.
Discussion. Some limitations have been found such as
Search strategy. The Pubmed archive was searched unspecified adjuvant therapies as well as important as-
using the search equation: physical therapy and adjuvant pects like the greater health benefits derived from exer-
therapy and breast neoplasm. cise in breast cancer survivors.
Study selection. The search produced 47 articles
within the established framework, based on the inclu-
sion and exclusion criteria 14 articles were selected.
KEYWORDS: Physical therapy. Adjuvant therapy. Breast neoplasm.
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
5PHYSIOTHERAPY UPDATES
Results of exercise in breast cancer survivors
STATE OF THE ART To select the articles obtained in the search, the following
inclusion and exclusion criteria were used:
Breast cancer is currently the most common type of
cancer affecting women (1). In Spain, in 2012, there The inclusion criteria were:
were 25,215 new cases, with an incidence of 11.7% (1).
In the same year, it was published that breast cancer • Studies including physical exercise in their inter-
was the type of cancer with the highest five-year preva- ventions.
lence with 17.9% and a mortality rate of 9% per 100,000 • Experimental studies.
inhabitants/year (1). These figures confirm the impor- • Studies on patients treated with adjuvant
tance of this disease in our society. treatments.
The treatment of breast cancer can be divided into di- • Studies including information about their inter-
fferent variants and will depend on the characteristics ventions, comparisons and results in their des-
of the tumour. Taking into account the patient’s cha- criptions.
racteristics, we can summarise them into: surgery,
radiotherapy, chemotherapy and/or hormonal therapy. The exclusion criteria were:
The treatment will be different depending on the sta- • Study protocols.
ge of the disease, neodajuvant treatment before sur-
gery, adjuvant treatment after surgery, and palliative • Observational studies.
treatment in case of metastasis (2). If we focus on the • Studies out of the previously established limits.
adjuvant treatment, we must stress it increases survival • Studies with non-adjuvant treatments.
rates and decreases the risk of relapses. At this stage
• Studies with adjuvant pre-treatment interven-
of the treatment, we can distinguish different types of
tions.
radiotherapies (depending on the approach and type of
carcinoma), hormone treatment, chemotherapy and/or Out of the 47 studies, 14 met the selected criteria.
monoclonal medication (Herceptin) (2).
DATA EXTRACTION
Mortality rates show the efficiency of the medical
treatment but it is essential to know the consequences The results of the obtained studies are shown in the ta-
and complications that it has on patients. The litera- ble below:
ture on the subject provides evidence of its psycholo-
gical effects (such as anxiety and/or depression, body In order to summarise the results, from the 14 reviewed
image and self-esteem problems (3,4), and physiolo- studies, 5 articles with no significant results and 8 ar-
gical effects (such as fatigue (described by 80% of pa- ticles with significant improvement in some of the stu-
tients) (5), muscle weakness, lymphedema, shoulder died variables were obtained.
and postural disorders, heart and lung complications,
According to the articles shown in the table, we can
etc.). All of them affect and are detrimental to the quali-
see the different outcomes of physical exercise on
ty of life of sufferers and reduce their tolerance to exer-
breast cancer survivors like benefits in terms of qua-
cise (6). Physiotherapy can improve this situation (7).
lity of life (4), reduced fatigue4 (4,5,13,18), increased
AIM strength (8,15,18), increased muscular endurance (8)
and less pain (13). The intervention periods of these
The main aim of this review was to know the effects results vary from 8 weeks to a year and the sample size
of physical exercise on breast cancer survivors based varies from 41 to 230 patients.
on the variables of quality of life, fatigue, depression,
anxiety, and adherence. Although other variables inclu- Moreover, we also found non-significant results when
ded in the reviewed articles were also registered. analysing the same variables (6,12,14,16,17).
DATA SOURCES OUTCOME ANALYSIS
The review in Pubmed was done in January 2016 using the When doing the search, it was quite limiting not to know
physical therapy and adjuvant therapy and breast neoplasm, exactly the adjuvant treatment that the patient had re-
equation and using the following limitations: studies pu- ceived, which could affect the different results. That is
blished prior to the previous five years, studies done on why it is important to specify precisely what the admi-
humans, and randomized controlled trials. A total of 47 nistered treatment was. This may be due to the fact of
studies were found. trying to get as many patients as possible but it would
be necessary to know more about the treatment in or-
STUDY SELECTION der to better understand the effects of exercise. Another
limiting factor when doing this review was the lack of in-
The population in the articles were breast cancer survi- formation in some articles regarding the patient’s basal
vors who had been treated with adjuvant therapy either state, regarding the amount of exercise that that person
before or during the study intervention period.
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
6PHYSIOTHERAPY UPDATES
Results of exercise in breast cancer survivors
did before starting the oncologic treatment, since this 2. Senkus E, Kyriakides S, Penault-Llorca F, Poort-
could also affect outcome variability. mans P, Thompson A, Zackrisson S, Cardoso F;
ESMO Guidelines Working Group. Primary breast
It must be emphasised that there is currently a consi- cancer: ESMO Clinical Practice Guidelines for
derable interest in the field of exercise and breast can- diagnosis, treatment and follow-up. Ann Oncol.
cer survivors, resulting in several articles on this topic. 2013 Oct;24 Suppl 6:vi7-23.
Considering this, we can see greater importance being
3. Luoma ML, Hakamies-Blomqvist L, Blomqvist C,
placed on the survival rate of these patients and the
Nikander R, Gustavsson-Lilius M, Saarto T. Expe-
physical and psychological effects resulting from the
riences of breast cancer survivors participating in
treatment. Taking the results into account, it would be
a tailored exercise intervention -a qualitative stu-
interesting to know more about the patient’s adherence
dy. Anticancer Res. 2014Mar;34(3):1193-9.
to the exercise programme since only Cournueya et al.’s
study (16) includes this variable, which is essential for 4. Hayes SC, et al. Exercise for health: a randomized,
the long-term benefits in these patients’ life. It would controlled trial evaluating the impact of a prag-
also be necessary to know about the minimum required matic, translational exercise intervention on the
time to find improvements related to the variables, since quality of life, function and treatment-related side
there are interventions of minimum 8 weeks up to a year. effects following breast cancer. Breast Cancer
Res Treat. 2013 Jan;137(1):175-86.
Regarding clinical practice, regular physical exercise 5. Reis D, Walsh ME, Young-McCaughan S, Jones T.
should be a part of the treatment given to these patients Effects of Nia exercise in women receiving radia-
because, as we can see in the treatments described in tion therapy for breast cancer. Oncol Nurs Forum.
the reviewed studies, they are informed of its benefits 2013 Sep;40(5):E374-81.
(1,4,5,7,10,14) but quite often this is not done. Clarifying
6. Saarto T, et al. Effectiveness of a 12-month exer-
the cause of this (lack of information, lack of motivation,
cise program on physical performance and quality
etc.) would help us find a solution and ensure its imple-
of life of breast cancer survivors. Anticancer Res.
mentation. In addition, this could improve the relation-
2012 Sep;32(9).
ship between the healthcare providers and the patient,
who sometimes feels neglected after the drug treatment. 7. Hanuszkiewicz J, Malicka I, Stefańska M, Bar-
czyk K, Woźniewski M. Body postureand trunk
Scientific research must continue investigating within muscle activity in women following treatment of
this field to demonstrate how the physical and psycho- breast cancer. OrtopTraumatol Rehabil. 2011 Jan-
logical state of these survivors can be improved, and Feb;13(1):45-57.
consequently improving their quality of life. 8. Winters-Stone KM, Leo MC, Schwartz A. Exercise
effects on hip bone mineral density in older, post-
In this article review, we can find the results of the 14
menopausal breast cancer survivors are age de-
studies with 5 articles presenting non-significant outco-
pendent. Arch Osteoporos. 2012;7:301-6.
mes and 9 articles presenting significant improvements
in some of the analysed variables. Nevertheless, further 9. Hornsby WE, et al. Safety and efficacy of aerobic
studies in this field are needed. training in operable breast cancer patients recei-
ving neoadjuvant chemotherapy: a phase II rando-
Thus, after reviewing the articles, we can learn the mized trial. Acta Oncol. 2014 Jan;53(1):65-74.
psychological and physical benefits of exercise on breast 10. Goodwin PJ,et al. Randomized trial of a telephone-
cancer survivors treated with an adjuvant treatment. based weight loss intervention in postmenopausal
women with breast cancer receiving letrozole: the
Ethical responsibilities LISA trial. J Clin Oncol. 2014 Jul 20;32(21):2231-9.
L'autora declara que s'han pres les mesures correctes 11. Husebø AM, Dyrstad SM, Mjaaland I, Søreide JA,
de sobre protecció de persones i animals, confidencia- Bru E. Effects of scheduledexercise on cancer-
litat de dades i dret a la privacitat i consentiment infor- related fatigue in women with early breast cancer.
mat durant la realització d'aquest article. ScientificWorldJournal. 2014 Jan 19;2014:271828.
12. Schmidt ME, Wiskemann J, Armbrust P, Sch-
Conflict of interests neeweiss A, Ulrich CM, Steindorf K. Effects of re-
sistance exercise on fatigue and quality of life in
The author of this manuscript declares no conflict of in-
breast cancerpatients undergoing adjuvant che-
terests related to this article.
motherapy: A randomized controlled trial. Int J
BIBLIOGRAPHY Cancer. 2015 Jul 15;137(2):471-80.
13. Steindorf K, et al. Randomized, controlled trial of
1. Ferlay J, Soerjomataram I, Ervik M, Dikshit R, resistance training in breast cancer patients re-
Eser S, Mathers C, Rebelo M, Parkin DM, Forman ceiving adjuvant radiotherapy: results on cancer-
D, Bray, F. GLOBOCAN 2012 v1.0, Cancer Inciden- related fatigue and quality of life. Ann Oncol. 2014
ce and Mortality Worldwide: IARC. Nov;25(11):2237-43.
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
7PHYSIOTHERAPY UPDATES
Results of exercise in breast cancer survivors
14. Taso CJ, Lin HS, Lin WL, Chen SM, Huang WT, 17. Courneya KS, et al. A multicenter randomized
Chen SW. The effect of yogaexercise on improving trial of the effects of exercise dose and type on
depression, anxiety, and fatigue in women with psychosocial distress in breast cancer patients
breast cancer: a randomized controlled trial. J undergoing chemotherapy. Cancer Epidemiol Bio-
Nurs Res. 2014 Sep;22(3):155-64. markers Prev. 2014 May;23(5):857-64.
15. Travier N, et al. Effects of an 18-week exercise 18. Van Waart H, et al. Effect of Low-Intensity Physi-
programme started early during breast cancer cal Activity and Moderate- to High-Intensity Phy-
treatment: a randomised controlled trial. BMC sical Exercise During Adjuvant Chemotherapy
Med. 2015 Jun 8;13:121. on Physical Fitness, Fatigue, and Chemotherapy
16. Courneya KS, et al. Subgroupeffects in a randomi- Completion Rates: Results of the PACES Ran-
sed trial of different types and doses of exercise domized Clinical Trial. J Clin Oncol. 2015 Jun
during breast cancer chemotherapy. Br J Cancer. 10;33(17):1918-27.
2014 Oct 28;111(9):1718-25.
Table I: Result table
Author/s Year N Intervention Comparison Results
Saarto, T 2012 573 12-month supervised domici- Quality of life, fati- Non- significant although
et al. (6) liary exercise programme for gue, and depression. there is a relative increase in
breast cancer survivors com- the intervention group in terms
pared to a control group doing of physical activity and quality
exercise without supervision. of life.
Hayes, S 2012 194 Physical exercise intervention Quality of life, Significant increase pPHYSIOTHERAPY UPDATES
Results of exercise in breast cancer survivors
Author/s Year N Intervention Comparison Results
Husebø AM, 2014 54 Study on patients during Comparison of the Significant increase in physical
Dyrstad SM, breast cancer treatment and effects of the pro- activity level in the interven-
Mjaaland I, 6-month post-chemotherapy. gramme on fatigue, tion group compared to the
Søreide JA, The intervention group had a physical activity control group.
Bru E (11) home-based exercise inter- level or physical
vention during chemotherapy; condition.
the control group had their
usual routine.
Schimdt, M, 2014 95 The study compared an Fatigue and quality Non-significant improvements.
Wiskeman, J, intervention group following of life.
Armbrust, P, a resistance exercise training
Ulrich, C, programme and a control
Steindorf, K group having a group relaxa-
(12) tion programme for 12 weeks
during chemotherapy.
Steindorf, K 2014 155 Resistance exercise training in Comparison of Significant difference (p=0.004)
et al. (13) the intervention group versus fatigue and quality in the reduction of physical fa-
a relaxation programme in the of life. tigue in the intervention group
control group for 12 weeks compared to the control group,
during adjuvant radiotherapy. as well as those items regar-
ding quality of life, function
(p=0.0035) and pain (0.040).
Taso, C, 2014 60 The intervention group had a Depression, anxiety No significant results were
Lin, H, yoga programme for 8 weeks and fatigue were obtained.
Lin, W, and the control group had their analyzed.
Chen, S, usual care.
Huang, W,
Chen, S (14)
Courneya, K 2014 301 Patients with breast cancer Adherence to exer- Non-significant results.
et al. (16,17) receiving chemotherapy were cise in the different
assigned to three exercise pro- programmes.
grammes: STAN (30’ of aerobic
exercise), HIGH (60’ of aerobic Depression, self- Regarding baseline levels,
exercise), COMB (60 of aerobic esteem, stress, and there was a significant impro-
exercise + resistance exercise). anxiety. vement in the COMB and HIGH
groups (p = 0.027).
Travier, N 2015 204 The intervention group had an Quality of life, Significant reduction in physi-
et al. (15) aerobic and resistance exer- anxiety, depression, cal fatigue in the intervention
cise programme versus the physical condition, group compared to the control
control group with usual care. fatigue. group. Significant increase in
For 18 weeks, measures were submaximal cardiorespiratory
taken at 18 and 36 weeks du- fitness in the intervention
ring breast cancer treatment. group compared to the control
group at 18 weeks but not at
36 weeks.
Waart, H 2015 230 Three intervention program- Fatigue, quality The exercise groups obtai-
et al. (18) mes in women with breast of life, physical ned significant outcomes for
cancer during chemotherapy: functioning and cardiorespiratory fitness (p
low-intensity physical activity condition.Col·legi
de Fisioterapeutes
de Catalunya
PHYSIOTHERAPY UPDATES
ORIGINAL ARTICLE
FASCIAL TREATMENT IN SPORTS. A BIBLIOGRAPHICAL REVIEW
Navarro R1,+, Simon M1,+, Casasayas O1, Miguel M2,3, Ortiz S2,3, Blasi M2,3, Álvarez P1, Pérez-Bellmunt, A1,3,4,*
1
Area of structure and function of the human body. Universitat Internacional de Catalunya.
2
Faculty of medicine and healthcare (Bellvitge Campus). Universitat de Barcelona.
3
Human Anatomy and MSK Ultrasound Lab. Faculty of medicine and healthcare (Bellvitge Campus).
4
SARX (Research Group in the Anthropology of Corporality). Universitat Internacional de Catalunya.
+
Equal contribution
.*
C/Josep Trueta s/n, 08195 Sant Cugat del Vallès, email: aperez@uic.es
Fascial tissue is a structure of mesenchymal tissue of done by two independent reviewers and the opinion of
mesodermic origin, which develops together with mus- another reviewer was taken into account when there
cular tissue (1). It forms a viscoelastic, functional and were any discrepancies. Research selection was based
three-dimensional type of tissue, mainly made up of co- on the information analysis provided by the abstract,
llagen fibres (2,3) and surrounding nervous tissue (neu- title, and key words. Finally, 12 articles were selected
rofascia), viscera (viscerofascia), and muscular tissue for this study, which were carefully studied, taking the
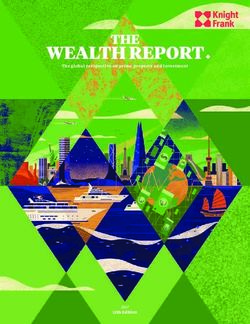
(myofascia). Some of its main functions are the absorp- whole text, for the assessment stage. Figure 1 shows
tion and dissemination of tensions (4), movement coor- the flow diagram of this article research. The last day
dination (5,6) and compartmentalization and division of the research was carried out was 10th February 2017.
both, anatomical regions and tissues (forming the epi-,
endo-, and peri- structures). The inclusion criteria were the following:
This close interconnection between fascial tissue and 1. Clinical studies related to fascial tissue.
the rest of anatomical structures gives fascia a central 2. Studies in which the therapeutic intervention is
importance within the field of sports and movement. managed within the field of physiotherapy.
Fascial restrictions or adhesions can cause movement 3. Articles with their full text available, published in
of flexibility limitations (7,8), take part in inflamma- a language the authors understood.
tory and painful processes (9-11) and lead to certain
muscular or tendinous lesions (12), neuropathies and The exclusion criteria were the following:
nerve compressions (13,14). However, it has also been
demonstrated that manipulation of fascial tissue has 1. Anatomical, histological, or biomechanical research
many positive effects in the therapeutic and physiolo- on fascial tissue.
gical fields like, for example, vascular plasticity, tissue 2. Systematic reviews.
restoration (15-17) and muscle tone reduction (18). 3. Studies whose full text was not available.
Taking into account the close relationship between fas- Methodology for assessing the studies and their
cia, muscular tissue and sports, the aim of the current scientific evidence
study is to do a systematic review of the literature to
determine the type of fascial treatments applied in the In order to assess the methodological quality of the stu-
field of sports, the pathologies studied and the variables dies the Jadad Scale was used, as it is a reference (19),
analysed. one of the oldest scales, and shows a good interrater
reliability (20). According to this scale, clinical trials are
MATERIALS AND METHODS
described along an interval from 0 to 5. Good quality cli-
Research methodology and inclusion criteria nical trials score 3 or more and low quality clinical trials
score under 3.
The bibliographic search was done using the MEDLINE
and PEDro databases. The terms used for the search A scale developed by the Canadian Task Force on the Pe-
derived from the combination of the words: fascia AND riodic Health Examination, ubsequently adapted by the
manual therapy AND sport. The search resulted in 22 same group (21), was used to assess the level of scien-
potential articles. The first information analysis was tific evidence of the studies.
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
10PHYSIOTHERAPY UPDATES
FASCIAL TREATMENT IN SPORTS. A BIBLIOGRAPHICAL REVIEW
Two independent reviewers, using the same methodo- ve traction of the connective tissue on the medial as-
logy, carried out both assessments. Any disagreement pect of the tibia (35). In the analysed article, the applied
between the reviewers was resolved including a third treatment intended to have a direct incidence on the
reviewer, who helped to achieve a consensus. crural fascia and used the Fascial Distortion Model® de-
veloped by Stephen Typaldos.
RESULTS AND DISCUSSION
In some other publications, what was analysed was
We found 12 articles to be analysed. The reading of the whether the influence of soft tissue stretching could
bibliography in these articles did not increase the total. improve function and relieve pain in patients with ace-
Table 1 describes the descriptive analysis of the publi- tabular problems (36) or soccer players with inguinal
cations and journals where the articles were published. hernias (37). In both cases, the results were positive in
terms of pain relief and movement but not in compari-
The methodological quality and scientific evidence of
son to a control group and when combining fascial and
the analysed publications are low. Some of the articles
muscular therapies, the observed improvement could
could not be assessed as they were not clinical trials or
not be assigned to the treatment on the fascia.
did not use any of the designs intended by the scales.
Table 1 shows the scores obtained. Two studies analysed the effects of self-myofascial re-
lease in healthy patients. One of the publications exa-
The pathology with the highest incidence in this review
mined whether the use of a foam roller before a sports
is plantar fasciitis (in 3 out of the 12 articles). This con-
performance test improved the results and reduced
dition is due to the inflammation, thickening, and mi-
fatigue (38), the results showed only a reduction in the
crodegeneration of the plantar aponeurosis (22) and
sportsperson’s fatigue. The other publication examined
affects 10% of the population (23). The specific fascial
the effects of using a foam roller on arterial physio
treatments used in the articles were: stretching, mo-
logy (39), observing significant results in arterial rigidity
bilization of connective tissue and fascial treatment
and endothelial vascular function.
of trigger points. The treatments that these specific
treatments complemented or were compared to were Table 2 shows the pathologies and treatments used in
shock waves and ultrasounds. The outcome analysis each of the studies, the characteristics of the samples
shows that there was an improvement in movement and and the results obtained.
in pain relief when either using a method with a higher
incidence in fascial tissue (24) or when combining di- CONCLUSIONS
fferent types of treatments specifically working on the
fascia. No significant differences were observed when The most commonly used therapies in the analysed
the fascial treatment was complemented with flexion- trials were Fascial Manipulation®, general techniques
extension ankle mobilizations (26). of soft tissue manual therapy, and self-myofascial re-
lease. Although the analysed trials do not show a high
Another pathologic entity that was quite present in this level of evidence and methodological quality, the results
review was back problems, found in 3 articles. In these presented in this review suggest that fascial techniques
studies, both the posture adopted by the hyperkyphotic can be effective in the treatment of pain and the impro-
patient (27) and the presence of pain in patients with uns- vement of mobility, both in healthy and unhealthy sub-
pecific back pain (28). In one of the publications, there is jects in sports and clinical settings.
reference to the treatment of spinal canal stenosis in a
patient with hypocondroplasia (29). In all the studies, the The review shows that the parts of the body mostly re-
treatment used was specific for fascial tissue and the presented in this study are those in which fascial tissue
methods used were: nonspecific soft tissue techniques, has a major role in tension transmission such as the
myofascial massage and Fascial Manipulation® (MF). plantar aponeurosis and lumbosacral aponeurosis. The
Whereas the first two treatments do not strictly stick to most commonly observed pathologies in this review are,
any particular method, MF, developed by Luiggi Stecco, by far, plantar fasciitis and back problems. We were qui-
focuses on treating deep fascia, its three-dimensions te surprised not to find any pathology directly related to
and interconnections (30). Regardless of the treatment the muscle or tendon, which are very frequent problems
being more or less protocolised, applying fascial therapy in sports.
improved the assessed variables in all cases.
Future clinical trials in which manual fascial treatments
In one of the publications, the medial tibial stress syn- are applied must determine, in a more precise way, the
drome (MTSS) is studied. MTSS is described as a syn- methodology of the fascial technique used in order to
drome characterised by complex pain suffered by some improve the replication of the study and the results. The
athletes on the medial aspect of the tibia. Its incidence methodological quality of the studies should also be im-
varies between 4% and 35% (31,32), although it seems proved so that the publication of future research has a
to be more frequent in runners or jumpers (33,34). Even greater impact. It is also important to highlight the fact
though the aetiology of MTSS is not very clear, some that there are unspecified treatments like fascial thera-
researchers suggest that it can be caused by repetiti- py that directly work on this tissue.
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
11PHYSIOTHERAPY UPDATES
FASCIAL TREATMENT IN SPORTS. A BIBLIOGRAPHICAL REVIEW
BIBLIOGRAPHY 15. Sucher BM. Myofascial manipulative release of
carpal tunnel syndrome: documentation with
1. Blasi M, Blasi J, Domingo T, Pérez-Bellmunt A, magnetic resonance imaging. J Am Osteopath
Miguel-Pérez M. Anatomical and histological stu- Assoc 1993 Dec;93(12):1273-1278.
dy of human deep fasciae development. Surgical
16. Arroyo-Morales M, Olea N, Martinez M, Moreno-
and Radiologic Anatomy 2012:1-8.
Lorenzo C, Daz-Rodrguez L, Hidalgo-Lozano A.
2. Yahia L, Pigeon P, DesRosiers E. Viscoelastic pro- Effects of myofascial release after high-intensity
perties of the human lumbodorsal fascia. J Bio- exercise: a randomized clinical trial. J Manipula-
med Eng 1993;15(5):425-429. tive Physiol Ther 2008;31(3):217-223.
3. Stecco A, Macchi V, Stecco C, Porzionato A, 17. Kraemer WJ, Flanagan SD, Comstock BA, Fra-
Ann Day J, Delmas V, et al. Anatomical study of gala MS, Earp JE, Dunn-Lewis C, et al. Effects
myofascial continuity in the anterior region of of a whole body compression garment on mar-
the upper limb. J Bodywork Movement Ther kers of recovery after a heavy resistance workout
2009;13(1):53-62. in men and women. J Strength Cond Res 2010
4. Benjamin M, Kaiser E, Milz S. Structure-function Mar;24(3):804-814.
relationships in tendons: a review. J Anat 2008 18. Delaney J, Leong KS, Watkins A, Brodie D. The
Mar;212(3):211-228. short-term effects of myofascial trigger point
5. Vleeming A, Pool-Goudzwaard AL, Stoeckart R, massage therapy on cardiac autonomic tone in
van Wingerden J, Snijders CJ. The Posterior La- healthy subjects. J Adv Nurs 2002;37(4):364-371.
yer of the Thoracolumbar Fascia| Its Function 19. Jadad AR, Moore RA, Carroll D, Jenkinson C,
in Load Transfer From Spine to Legs. Spine Reynolds DJM, Gavaghan DJ, et al. Assessing
1995;20(7):753-758. the quality of reports of randomized clinical
6. Huijing PA, Baan GC. Extramuscular myofas- trials: is blinding necessary? Control Clin Trials
cial force transmission within the rat anterior 1996;17(1):1-12.
tibial compartment: proximo-distal differen- 20. Interrater agreement of Jadad’s scale. Annual Co-
ces in muscle force. ActaPhysiolScand 2001 chrane Colloquium Abstracts. Lyon, October; 2001.
Nov;173(3):297-311.
21. Guide to Clinical Preventive Services: An As-
7. Barnes MF. The basic science of myofascial re- sessment of the Effectiveness of 169 Interven-
lease: morphologic change in connective tissue. tions. Mayo Clinic Proceedings: Elsevier; 1989.
J Bodywork Movement Ther 1997;1(4):231-238.
22. Berkowitz JF, Kier R, Rudicel S. Plantar fasciitis:
8. Peacock CA, Krein DD, Silver TA, Sanders GJ, von MR imaging. Radiology 1991 Jun;179(3):665-667.
Carlowitz KA. An acute bout of self-myofascial
23. Pfeffer G, Bacchetti P, Deland J, Lewis A, Ander-
release in the form of foam rolling improves per-
son R, Davis W, et al. Comparison of custom and
formance testing. International journal of exerci-
prefabricated orthoses in the initial treatment of
se science 2014;7(3):202.
proximal plantar fasciitis. Foot & Ankle Interna-
9. Stecco C, Stern R, Porzionato A, Macchi V, Masie- tional 1999;20(4):214-221.
ro S, Stecco A, et al. Hyaluronan within fascia in
24. Rompe JD, Furia J, Cacchio A, Schmitz C, Maffulli
the etiology of miofascial pain. Surg Radiol Anat
N. Radial shock wave treatment alone is less effi-
2011 Dec;33(10):891-896.
cient than radial shock wave treatment combined
10. Stecco A, Gesi M, Stecco C, Stern R. Fascial compo- with tissue-specific plantar fascia-stretching in
nents of the myofascial pain syndrome. Curr Pain patients with chronic plantar heel pain. Interna-
Headache Rep 2013 Aug;17(8):352-013-0352-9. tional Journal of Surgery 2015;24:135-142.
11. Klingler W, Velders M, Hoppe K, Pedro M, Schleip 25. Renan-Ordine R, Alburquerque-Sendín F, Ro-
R. Clinical relevance of fascial tissue and dys- drigues De Souza, Daiana Priscila, Cleland JA,
functions. Curr Pain Headache Rep 2014;18(8):1-7. Fernández-de-las-Peñas C. Effectiveness of
12. Perez-Bellmunt A, Miguel-Perez M, Brugue MB, myofascial trigger point manual therapy combi-
Cabus JB, Casals M, Martinoli C, et al. An ana- ned with a self-stretching protocol for the ma-
tomical and histological study of the structures nagement of plantar heel pain: a randomized
surrounding the proximal attachment of the hams controlled trial. Journal of orthopaedic & sports
tring muscles. Man Ther 2015 Jun;20(3):445-450. physical therapy 2011;41(2):43-50.
13. Young IJ, van Riet RP, Bell SN. Surgical release 26. Shashua A, Flechter S, Avidan L, Ofir D, Melayev
for proximal hamstring syndrome. Am J Sports A, Kalichman L. The effect of additional ankle and
Med 2008 Dec;36(12):2372-2378. midfoot mobilizations on plantar fasciitis: a ran-
14. Puranen J, Orava S. The hamstring syndro- domized controlled trial. Journal of orthopaedic
me--a new gluteal sciatica. Ann Chir Gynaecol & sports physical therapy 2015;45(4):265-272.
1991;80(2):212-214.
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
12PHYSIOTHERAPY UPDATES
FASCIAL TREATMENT IN SPORTS. A BIBLIOGRAPHICAL REVIEW
27. Ćosić V, Day JA, Iogna P, Stecco A. Fascial Mani- 34. Lassus J, Tulikoura I, Konttinen YT, Salo J, Santa-
pulation® method applied to pubescent postural virta S. Bone stress injuries of the lower extremi-
hyperkyphosis: A pilot study. J Bodywork Move- ty. ActaOrthopScand 2002;73(3):359-368.
ment Ther 2014;18(4):608-615. 35. Moen MH. Aetiology, imaging and treatment of
28. Branchini M, Lopopolo F, Andreoli E, Loreti I, medial tibial stress syndrome. Utrecht Universi-
Marchand AM, Stecco A. Fascial Manipulation® ty; 2012.
for chronic aspecific low back pain: a single 36. Cashman GE, Mortenson WB, Gilbart MK. Myo-
blinded randomized controlled trial. F1000Re- fascial treatment for patients with acetabular
search 2015;4. labral tears: a single-subject research design
29. Hanson AA. Improving mobility in a client with study. Journal of orthopaedic & sports physical
hypochondroplasia (dwarfism): A case report. J therapy 2014;44(8):604-614.
Bodywork Movement Ther 2010;14(2):172-178. 37. Yuill EA, Pajaczkowski JA, Howitt SD. Conser-
30. Stecco L, Stecco C. Fascial manipulation. Piccin, vative care of sports hernias within soccer pla-
Italy 2004. yers: a case series. J Bodywork Movement Ther
31. Bennett JE, Reinking MF, Pluemer B, Pentel A, 2012;16(4):540-548.
Seaton M, Killian C. Factors contributing to the 38. Healey KC, Hatfield DL, Blanpied P, Dorfman LR,
development of medial tibial stress syndrome in Riebe D. The effects of myofascial release with
high school runners. Journal of Orthopaedic & foam rolling on performance. J Strength Cond
Sports Physical Therapy 2001;31(9):504-510. Res 2014 Jan;28(1):61-68.
32. Yates B, White S. The incidence and risk factors 39. Okamoto T, Masuhara M, Ikuta K. Acute effects
in the development of medial tibial stress syndro- of self-myofascial release using a foam roller
me among naval recruits. Am J Sports Med 2004 on arterial function. J Strength Cond Res 2014
Apr-May;32(3):772-780. Jan;28(1):69-73.
33. Arendt EA, Griffiths HJ. The use of MR imaging
in the assessment and clinical management of
stress reactions of bone in high-performance
athletes. Clin Sports Med 1997;16(2):291-306.
Figure 1. Flux diagram
22 articles
2 systematic reviews
3 anatomical studies
2 biomechanical studies ica
1 no clinical study
14 articles
1 demographical study
1 article in a language authors did not know
12 articles
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
13PHYSIOTHERAPY UPDATES
FASCIAL TREATMENT IN SPORTS. A BIBLIOGRAPHICAL REVIEW
Table 1
Jadad US Preventi-
Authors Title Publication Year scale ve Task Force
Branchini, M.; Lopopolo, F.; Fascial manipulation for chronic F1000Re- 2015 4 I
Andreoli, E.; Loreti, I.; aspecific low back pas : a single search
Marchand, A. Stecco, A. blinded randomized controlled trial
Shashua, A.; Fletcher, S.; The effect of additional ankle Journal of 2015 4 I
Avidan, L.; Ofir, D.; Melayev, A.; and midfoot mobilizations on Orthapaedic&
Kalichman, L. plantar fasciitis: a randomized Sports Physi-
controlled trial cal Therapy
Rompe, J.; Furia, J.; Cacchio, A.; Radial shock wave treatment International 2015 4 I
Schmitz, C.; Maffulli, N. alone is less efficient than radial Journal of
shock wave treatment combined Surgery
with tissue-specific plantar fascia-
stretching in patients with chronic
plantar heel pain
Cashman, G.; Mortenson, B.; Myofascial treatment for patients Journal of 2014 - II-3
Gilbart, M. with acetabular labral tears: Orthapaedic&
a single-subject research Sports Physi-
design study cal Therapy
Schulze, C.; Finze, S.; Bader, R.; Treatment of Medial Tibial Stress The Scientific 2014 - II-2
Lison, A. Syndrome according to the Fascial World Journal
Distortion Model: A Prospective
Case Control Study
Okamoto, T.; Masuhara, M.; Acute effects of self-myofascial Journal of 2014 1 I
Ikuta, K. release using a foam roller on Strength and
arterial function Conditioning
Research
Ćosić, V.; Day,J.; Iogna, P.; Fascial Manipulation method Journal of 2013 - II-3
Stecco, A. applied to pubescent postural Bodywork and
hyperkyphosis : a pilot study Movement
Therapies
Healey, K.; Hatfield, D.; The Effects of Myofascial Release Journal of 2013 1 I
Blanpied, P.; Dorfman, L.; With Foam Rolling on Performance Strength and
Riebe, D. Conditioning
Research
Yuill, E.; Pajaczkowski, J.; Conservative care of sports her- Journal of 2012 - II-3
Howitt, S. nias within soccer players: A case Bodywork &
series Movement
Therapies
Renan-Ordine, R.; Alburquer- Effectiveness of Myofascial Tigger Journal of 2011 1 I
que-Sendin, F.; Rodrigues point Manual Therapy Combined Orthapaedic&
de souza, D.; Cleland, J.; With a self-stretching protocol for Sports Physi-
Fernandez-de-las-peñas, C. the management of plantar heel cal Therapy
pain : a randomized controlled trial
Hanson, A. Improving mobility in a client with Journal of 2010 - -
hypocondroplasia (dwarfism) : a Bodywork and
case report Movement
Therapies
Wang, H.; Shih, T.; Lin, K.; Real-time morphologic changes of Manual 2008 - II-3
Wang, T. the iliotibial band during thera- Therapy
peutic stretching; an ultrasono-
graphic study
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
14PHYSIOTHERAPY UPDATES
FASCIAL TREATMENT IN SPORTS. A BIBLIOGRAPHICAL REVIEW
Table 2
Authors Subjects Physiotherapy treatment and analysed variable Results
Branchini 24 subjects Each subject had 8 sessions over 4 weeks. The treatment The subjects who received
et al. with uns- was administered based on the groups. the combined treatment
pecific low Control group: physiotherapy programme including re- (study group) obtained better
back pain laxation, control of diaphragmatic breathing, stretching, results in all the variables at
postural and functional rehabilitation, etc. the end of the treatment and
Study group: the same programme combined with FASCIAL 1 month afterwards.
MANIPULATION®.
The analysed variables were pain, function, and the most
significant outcome for each individual patient.
Shashua 50 subjects The experimental and control groups had a total of 8 Both groups had positive
et al. with plantar sessions, two sessions a week, of stretching exercises and results in all the variables
fasciitis ultrasounds. but there were no significant
In addition, the intervention group received mobilization of differences between them.
the ankle and midfoot joints in the first sessions.
Dorsiflexion range of motion, pain, and lower limb function
were measured.
Rompe 152 sub- Group 1: three sessions of shock wave therapy at weekly The combined treatment of
et al. jects with intervals. shock waves + stretching
chronic Group 2: a stretching programme with specific exercises programme is more effective
plantar for the plantar fascia for 8 weeks, 3 times a day; three ses- than just the shock wave
fasciitis sions of shock wave therapy at weekly intervals. therapy in all the variables
Variables: pain (nine-item pain subscale of the validated after 8 weeks.
Foot Function Index) and outcomes (subject-relevant outco-
me questionnaire).
Cashman 4 subjects The patients were treated for 6 to 8 weeks. Therapy consis- Significant improvement of
et al. with aceta- ted of a combination of soft tissue therapy, stretching, and hip pain, particularly in the
bular labral strengthening of the hip muscles. posterolateral area, and
tears The analysed variables were hip pain and function. better hip function.
Schulze 32 subjects The subjects received fascial treatment using the Typal- Significant improvement of
et al. with medial dos® fascial distortion model and they were not allowed to pain and tolerated exercise.
tibial stress perform any sport activity on the days the treatment was
syndrome administered.
They received therapy every day until the symptoms disap-
peared (6 days of treatment on average).
Okamoto 10 healthy The subjects had two sessions with different treatments in A foam roller reduces ar-
et al. subjects random order at intervals of 3 days. terial stiffness and impro-
One of the treatments consisted of myofascial therapy with ves vascular endothelial
a foam roller on the thigh muscles and trapezius. The other function.
treatment (control) had the patients resting supine.
The variables used were: brachial-ankle index, blood pres-
sure, heart rate, and plasma nitric oxide concentration.
Ćosić 17 adoles- The subjects received between 2 and 4 weekly sessions of Significant improvement
et al. cents with FASCIAL MANIPULATION®. in all the parameters after
postural hy- All the subjects were evaluated for psychological aspects, the treatment and 7 months
perkypho- sport, pain; anteposition of shoulders, head, and pelvis, dis- afterwards.
sis tance between C7 and L3 from plumb-line, distance from
fingers to floor on forward bend.
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
15PHYSIOTHERAPY UPDATES
FASCIAL TREATMENT IN SPORTS. A BIBLIOGRAPHICAL REVIEW
Authors Subjects Physiotherapy treatment and analysed variable Results
Healey 26 healthy he treatment was divided into 2 different sessions with an There were no significant
et al. subjects interval of 5 days. The subjects had to do a series of exer- differences between the two
cises and some athletic performance tests whose results treatments for the athletic
were used to determine the analysed variables. performance tests but there
The exercises were planking exercises in one of the ses- was a reduction in post-
sions and foam rolling exercises in the other session. exercise fatigue for those
Fatigue, soreness, and exertion were also measured. who had the foam rolling
session.
Yuill et al. 3 soccer The subjects were treated 1-2 times a week for 6-8 weeks. Significant reduction of pain
players with The treatment consisted of soft tissue therapy, six joules 8 weeks after treatment.
inguinal of laser at the site of the chief complaint, microcurrents
hernia. applied to the area of chief complaint, acupuncture, Wo-
benzyme for the pain and inflammation, hip rehabilitative
exercises, and plyometric training.
The analysed variables included pain (AS) and muscular
resistance.
Renan- 60 subjects The subjects had 4 sessions a week for 4 weeks with different The outcomes were sig-
Ordine with plantar treatments for each group. nificantly better in all the
et al. fasciitis Group 1: lower limb self-stretching exercises. variables for the group that
Group 2: lower limb self-stretching exercises + soft tissue received the combined the-
trigger point manual therapy. rapy programme (group 2).
The analysed variables were function, pain and pain thresholds.
Hanson A sub- The subject had 8 sessions in which he received myofascial The patient showed positive
ject with massage, from less to more specific techniques as the results in reducing adhe-
hypochon- treatment progressed. sions in the thigh, improving
droplasia She also had stretches of the iliopsoas and specific massa- circulation, and increasing
(dwarfism) ge for the muscle. the distance the client could
and spinal walk before resting.
stenosis
Wang 44 healthy The subjects were treated with the Ober maneuver in three There was significant reduc-
et al. subjects positions: neutral, adducted and adducted with weight. tion in iliotibial band width in
Iliotibial band width was measured. neutral position.
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
16Col·legi
de Fisioterapeutes
de Catalunya
PHYSIOTHERAPY UPDATES
TRANSLATED ARTICLE
ASSESSMENT OF ELECTROMYOGRAPHY ACTIVITY OF PELVIC FLOOR MUSCLES
DURING POSTURAL EXERCISES USING WII FIT PLUS© VIRTUAL VIDEO GAMES.
ANALYSIS AND PERSPECTIVES IN RE-EDUCATION
B. Steenstrup,a,*, F. Giralteb, E. Bakkerc, P. Griseb
a
Médipôle du Rouvray, 76800 Saint-Etienne-du-Rouvray, França, França; b Urology department, CHU de Rouen, 76000 Rouen, France;
c
HE L de Vinci — IES Parnasse-deux Alice, 1200 Brussels, Belgium
*
Corresponding author: Email address: b.steenstrup@wanadoo.fr (B. Steenstrup)
http://dx.doi.org/10.1016/j.purol.2014.09.046
1166-7087/© 2014 Elsevier Masson SAS. All rights reserved.
Received on 18 July 2014. Accepted on 23 September 2014. Available online on 23 October 2014.
ABSTRACT
Introduction. The aim of this work was to evaluate the traction the SEMG activity raised at a mean of 14.43 mV
effect of postural awareness by using the Wii Fit Plus© (7.87—21.89). In the first set of exercises on the WBB
on the quality of the baseline (automatic) activity of the without any visual feedback, the automatic activity of the
pelvic floor muscles (PFM) measured by intravaginal PFM increased from 2.87 mV to 8.75 mV (7.96—9.59). In
surface electromyography (SEMG). the second set, with visual postural and SEMG control,
mean baseline SEMG activity even raised at 11.39 mV
Methods. Four healthy continent female subjects, all (10.17—11.58).
able to perform a voluntary contraction, undertook 2
sets of 3 various exercises offered by the software Wii Conclusion. Among women able of a voluntary contrac-
Fit Plus© using the Wii balance board© (WBB): one tion of PFM, visualisation of posture with the help of the
set without any visual control and the second set with WBB and of SEMG activity of the PFM during static and
postural control and SEMG visual feedback. Simulta- dynamic Wii Fit Plus© activities, may improve the auto-
neously, we recorded the SEMG activity of the PFM. matic activation of the PFMs.
Results. Mean baseline activity of PFM in standing posi- Level of evidence. 4.
tion at start was 2.87 mV, at submaximal voluntary con-
KEYWORDS: Pelvic floor muscle. Electromyography. Biofeedback.
Posture. Wii Fit Plus©. Awareness.
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
17PHYSIOTHERAPY UPDATES
ASSESSMENT OF ELECTROMYOGRAPHY ACTIVITY OF PELVIC FLOOR MUSCLES DURING POSTURAL EXERCISES
USING WII FIT PLUS© VIRTUAL VIDEO GAMES. ANALYSIS AND PERSPECTIVES IN RE-EDUCATION
INTRODUCTION control of PFM activity with a surface electromyography
(SEMG) and control of COP of postural activity. We ex-
The perineal muscular complex is mainly made up of pect that this visualisation while doing the re-education
type-I muscle fibres of a small diameter, resistant to exercises stimulates the awareness process of a better
fatigue, and characterised by low amplitude voluntary postural activity of PFMs and the muscles in the lumbo-
contractions. These muscle cells present a long period pelvic region in general.
of post-activity hyperpolarization that limits their maxi-
mum discharge rate (1). These anatomical and histo- METHOD
logical specificities provide pelvic floor muscles (PFMs)
with a key role in the control of micturition (2) and defe- This is a preliminary observational study, done in Sept-
cation, in sex (3), and in the maintenance of lumbopelvic ember 2013 at CHU in Rouen, France.
stability (4,5), In order to preserve these functions, the
PARTICIPANTS
PFMs are activated by the somatic and emotional motor
systems (SMS and EMS) (6). These different activation Four continent nulliparous female volunteers who
pathways permit voluntary contractions through the were verbally recruited: aged between 28 and 50 years
lateral SM whereas the medial SMS permits postural (mean = 42.7), weighing from 48 to 68 kg (mean = 60
adjustments (feedback) during axial movements. The la- kg), between 1.58 and 1.68 m tall (mean = 1.62 m) with
teral EMS, in turn, controls contractions in preparation a BMI between 19.5 and 24.1 (mean = 22.6), number
for imminent perturbation (feedforward) or anticipated of births ranging from 1 to 3 (mean = 2)), all vaginal
postural adjustment (APA). If the relationship between births, episiotomy 3, forceps 2, and no urogynecologi-
the loss of these anticipatory postural activations and cal surgery. They all filled in a questionnaire on gene-
chromic low back pain has been widely described in the ral health that is routinely used in our service. They
literature by Hodges et al., it was Smith in 2007 who first did not have any history of neurological, psychiatric or
showed the role of APAs in the context of stress urinary gastroenterological problems.
incontinence (SUI) (7). Based on this new evidence in the
field of pathophysiology, Bakker et al. (2008) proposed a EXPERIMENTAL PROTOCOL
functional model of incontinence for the management
of SUI (8). This hypothesis is supported by Capson et al. All the participants completed an informed consent form
(2011), who observed an improved automatic response to take part in a biomedical study following the French gui-
of PFMs to postural changes in the lumbopelvic region delines for public health. Each participant had a BFB (Pe-
if the subject is standing (self adjustment position) risize 4+©) vaginal probe inserted vaginally with the use
through lumbopelvic stabilization (9). of some hypoallergenic gel. The probe has 4 independent
hemispherical electrodes in backward and lateral position,
Virtual reality video games offer potentially innovative connected with 4 2-mm banana plugs. This is a non-obtu-
approaches that still need to be further examined. The ration probe used to limit the artefacts caused by the in-
concept of the Wii Fit Plus© gaming software is based crease of endocavitary pressure during the exercises (14).
on ideas that could affect re-education (10): mirror Several studies have demonstrated the reliability of SEMG
images, reward and stimuli presented as scores du- activity recordings of PFMs with surface electrodes (15,16).
ring outcome progression. This game also involves an Junginger found a strong correlation between bladder
interesting cognitive workload fractionated into a pho- neck elevation assessed with ultrasound and a SEMG of
nological loop and a visuospatial sketchpad (11). We can PFMs (17). A snap Dura Stick Plus® reference surface
find numerous conditions that will favour a progressive electrode was placed on the osseous rim of the pelvis. The
recruitment of static or dynamic postural activity. The vaginal probe and reference electrode were connected to
activity of mirror neurons could be strongly promoted an SEMG device: Myotrack® (Thought Technology Ltd.) as-
with the concept in which a virtual trainer shows you, sisted by INFINITY® software (18) with an automatic recor-
throughout the exercise, what the ideal posture and ding measurement of SEMG output of PFMs in microvolts
right movements are (take-off pose and tree pose). In RMS (root mean square) (19). The acquisition frequency of
the third proposed exercise, it is an avatar (hula-hoop). Myotrack® is 1Khz and the chosen acquisition gain, 0.5%.
During the exercises, the patient visualises her centre For the assessment, the first second of SEMG activity was
of pressure (COP) or her avatar’s activity, which, in turn, excluded. In this study, we calculated the mean of the 10
is based on COP recordings. At the end of each exercise, RMS of the reference submaximal contractions in order
the software presents numerical results, using a reward to compare them with the mean of SEMG activity during
system of points and feedback stimuli that favour per- postural exercises. We used a Wii Balance Board© (WBB),
formance. We know that PFMs are modulated by the a platform for the general public assessing COP assisted
emotional motor system (6) and that there is great co- by Nintendo© Wii and Wii Fit Plus© software. The WBB
hesion in the virtual concept of motor learning. Leisure allows a right-left and back-forth control of COP. Users
activities like hula-hoop involve a dynamic activity of the can therefore modify their postural activity (20) visualising
pelvis and lumbar region and help a dynamic postural their COP on a screen of considerable dimensions (640 ×
activity of the PFMs (12,13). We have examined the con- 400 mm). The Wii Fit Plus© software proposes postural
tribution of visualisation through double biofeedback:
PHYSIOTHERAPY UPDATES Issue XIV, Year 2017
18You can also read