Infection Prevention Updates for Acute Care and Outpatient Settings
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Guidance and responses were provided based on information known on
5/25/2022 and may become out of date. Guidance is being updated
rapidly, so users should look to CDC and NE DHHS guidance for updates.
Infection Prevention Updates for
Acute Care and
Outpatient Settings
May 25, 2022
Questions and Answer Session
Presenters today are:
Gary Anthone, MD gary.anthone@nebraska.gov
Lacey Pavlovsky, RN, MSN, CIC lpavlovsky@nebraskamed.com
Panelists today are:
Margaret Drake, MT(ASCP), CIC margaret.drake@nebraska.gov
M. Salman Ashraf, MBBS salman.ashraf@nebraska.gov
Richard Starlin, MD rick.starlin@unmc.edu
Rebecca Martinez, BA, BSN, RN, CIC remartinez@nebraskamed.com
Jody Scebold, EdD, MSN, RN, CIC jodscebold@nebraskamed.com
Chris Cashatt RN, BSN, CIC ccashatt@nebraskamed.com
Moderated by Margaret Deacy mdeacy@nebraskamed.com
Please use the Q&A box in the webinar platform to type a question. Questions will
be read aloud.
If your question is not answered during the webinar, please e-mail it to
nebraskaicap@nebraskamed.com or call Monday – Friday 8:00 am – 4:00 pm CST to speak
with one of our Infection Preventionists.
Slides and a recording of this presentation will be available on the Nebraska ICAP website
https://icap.nebraskamed.com/covid-19-webinars/
Learning Objectives During this series, participants should be better able to: 1. Recognize infection prevention and control issues for application of the recommendations to mitigate these issues. 2. Identify resources on infection prevention and control that will be helpful to mitigate infection prevention and control challenges. 3. Describe latest updates on COVID-19 pandemic related to infection prevention and control practices in acute and outpatient settings. Target Audience Healthcare professionals working in acute and outpatient settings. To include medical directors, nursing staff, directors of nursing, infection preventionists, quality program leaders, administrators, consultant pharmacists or other staff working in Acute and Outpatient settings.

Mission and Goals To provide an educational venue that connects infection preventionists and providers from acute and outpatient facilities across Nebraska with the objective of promoting the latest research and best practices in infection prevention and control. These educational webinars are aimed to help promote and strengthen the Nebraska infection prevention and control infrastructure. The goals for this educational activity include: 1. Increase knowledge of infection control processes for acute and outpatient settings. 2. Increasing awareness of specific infection prevention and control issues that may be confronted in acute and outpatient settings. 3. Provide resources to attendees to help them with infection prevention and control efforts in their own facilities. 4. Provide resources to attendees on the most up to date COVID-19 pandemic related guidance and recommendations.

Continuing Education
1.0 Nursing Contact Hour is awarded for the LIVE viewing of this webinar
Nebraska Medicine is approved as a provider of nursing continuing
professional development by the Midwest Multistate Division, an accredited
approver by the American Nurses Credentialing Center’s Commission on
Accreditation.
In order to obtain either contact hour, you must be present for the entire live
webinar and complete the post webinar survey
No conflicts of interest were identified for any member of the planning committee,
presenters or panelists of the program content
This CE is hosted by Nebraska Medicine and UNMC along with Nebraska ICAP and
Nebraska DHHS
Continuing Education
1.0 AMA PRA Category 1 Credit™ for Physicians offered by UNMC is awarded
for the live viewing of this webinar
In support of improving patient care, University of Nebraska
Medical Center is jointly accredited by the Accreditation Council
for Continuing Medical Education (ACCME), the Accreditation
Council for Pharmacy Education (ACPE), and the American
Nurses Credentialing Center (ANCC), to provide continuing
education for the healthcare team.
The University of Nebraska Medical Center designates this live
activity for a maximum of 1 AMA PRA Category 1 Credit™.
Physicians should claim only the credit commensurate with the
extent of their participation in the activity.
Disclosure Declaration As a jointly accredited provider, the University of Nebraska Medical Center (UNMC) ensures accuracy, balance, objectivity, independence, and scientific rigor in its educational activities and is committed to protecting learners from promotion, marketing, and commercial bias. All faculty, planner and others in a position to control continuing education content participating in an accredited continuing education activity are required to disclose all financial relationships with ineligible companies. Ineligible companies are organizations whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients. The accredited provider is responsible for mitigating all relevant financial relationships in accredited continuing education. Disclosure of these commitments and/or relationships is included in these activity materials so that participants may formulate their own judgments in interpreting its content and evaluating its recommendations. This activity may include presentations in which faculty may discuss off-label and/or investigational use of pharmaceuticals or instruments not yet FDA-approved. Participants should note that the use of products outside currently FDA-approved labeling should be considered experimental and are advised to consult current prescribing information for FDA-approved indications. All materials are included with the permission of the faculty. The opinions expressed are those of the faculty and are not to be construed as those of UNMC. The accredited provider has mitigated and is disclosing identified relevant financial relationships for the following faculty, planners, and others in control of content prior to assuming their roles: FACULTY The faculty have nothing to disclose: Gary Anthone, MD Lacey Pavlovsky, RN, MSN, CIC PLANNING COMMITTEE The planning committee members have nothing to disclose: Margaret Drake, MT Rebecca Martinez, BSN, Daniel Brailita, MD M. Salman Ashraf, MBBS (ASCP), CIC BA, RN, CIC
Nebraska DHHS Updates
Gary Anthone, MD
Chief Medical Officer, DHHS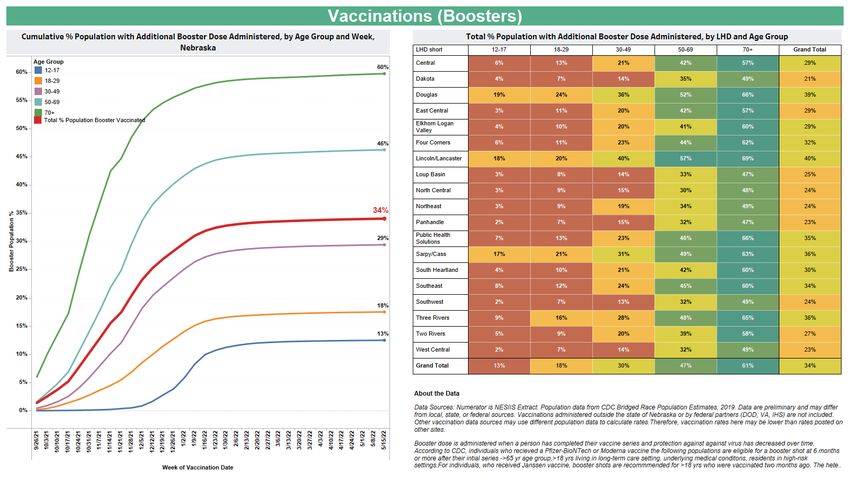
• Increase of 16pts (+16; +5; -3; +1) • 7 Day rolling average of 2.1% (1.7; 1.3; 1.2; 1.4) • 15% of hospitalized COVID pts in ICU (10; 4; 14; 8) • 25% of COVID ICU pts on Vents (29; 0; 43; 50) • 3% of statewide ICU pts are COVID pts (2; 1; 2; 1) • Average of 11 new covid pts admitted per day (8; 7; 5; 7) • 2 ped admits last week (3; 4; 2; 9;)
Infection Prevention
Risk Assessment
Presented by Lacey Pavlovsky, RN, MSN, CIC
Nebraska ICAP Infection PreventionistJoint Commission Requirements IC.01.03.01: The hospital identifies risks for acquiring and transmitting infections. The hospital identifies risks for acquiring and transmitting infections based on the following: • Its geographic location, community, and population served • The care, treatment, and services it provides • The analysis of surveillance activities and other infection control data The hospital reviews and identifies its risks at least annually and whenever significant changes occur with input from, at a minimum, infection control personnel, medical staff, nursing, and leadership. The hospital prioritizes the identified risks for acquiring and transmitting infections. These prioritized risks are documented. The Joint Commission E-dition (jcrinc.com)
Joint Commission Requirements
IC.01.04.01: Based on the identified risks, the hospital sets goals to minimize
the possibility of transmitting infections.
The organization’s written infection prevention and control goals include the
following
1. Addressing its prioritized risks.
2. Limiting unprotected exposure to pathogens.
3. Limiting the transmission of infections associated with procedures.
4. Limiting the transmission of infections associated with the use of medical
equipment, devices, and supplies.
5. Improving compliance with hand hygiene guidelines
Joint Commission Resources, Using the Risk Assessment to Set Goals and Develop the Infection Prevention and Control Plan.
Available at http://www.jcrinc.com/using-the-risk-assessment-to-set-goals-and-develop-the-infection-prevention-and-control-
plan/Joint Commission Requirements The Joint Commission’s Infection Prevention and Control (IC) standards require organizations to use the risk assessment process to set goals for a comprehensive infection control plan. Specifically, Standard IC.01.04.01 states, “Based on the identified risks, the [organization] sets goals to minimize the possibility of transmitting infections.” “The results of the hospital’s infection risk assessment should be prioritized, ideally in order of level of probability and potential for harm. The hospital can then set goals for reducing the risks of infections that pose the greatest threat to patients and the community. These goals should lead to focused activities, based on relevant professional guidelines and sound scientific practices.” Joint Commission Resources, Using the Risk Assessment to Set Goals and Develop the Infection Prevention and Control Plan. Available at http://www.jcrinc.com/using-the-risk-assessment-to-set-goals-and-develop-the-infection-prevention-and-control- plan/
Purpose of an Infection Prevention
(IP) Risk Assessment
1 2 3 4
Enable committees Prioritize the most Develop response to Develop a plan,
and work groups to important work healthcare concerns strategy, and
focus resources on to improve patient evaluation for
the most compelling and/or facility safety highest risk areas.
infection prevention
issue at your facilityFrequency of an IP Risk
Assessment
– Beginning of year and/or beginning of fiscal year
– Anytime circumstances change or significant changes occur
• New services
• New programs
• Response to external events
• New risk identified and there may be a need to
reprioritize
• Change in regulations
– Review risk assessment periodically (annually at a
minimum)The Team Who should be a member of the team – Infection Preventionist(s) – Administration – Nursing Leadership – Medical staff – Pharmacy – Environmental Services – Safety/Risk Officer – Engineering/Facilities – Nursing Staff – Quality Director – Employee Health – Lab – PT/OT This Photo by Unknown Author is licensed under CC BY-NC – Respiratory Therapy – Education
Risk Assessment Team Sport
Do as a group or one-
Input from everyone on-one with key
personnel
You’ll guide the
First time is most
process, but everyone
difficult
contributesSteps
–Identify the risks
• Sources to consider when trying to identify the risks
–Unusual occurrences
–Potentially compensable events
–Significant/sentinel events
–Medical/legal claims
–Regulatory complaints
–Audits
–Surveys
–Community standards of care/practice
–Risks may have subcategories
• e.g., SSI (list individual procedures performed)Areas to Score
Probability- Likelihood this event will occur/fail
Impact- How severe/harm if the event does
occur
Preparedness – Infection Prevention Systems in
place/Quantity of supplies/Staff awarenessScoring Key Example 1
Several different tools available for you to use.
Probability Impact Preparedness
3 2 1 3 2 1 1 2 3
High Medium Low High Medium Low High Medium Low
None or
Much Some very Very Nothing
will happen Maybe rare Prepared
harm harm little Prepared in place
harm
Probability Impact Preparedness
3 2 1 0 3 2 1 3 2 1 0
High Medium Low Never High Moderate Minimal Poor Fair Good ExcellentScoring Key Example 2
Probability Impact Preparedness
5 4 3 2 1 5 4 3 2 1 1 2 3 4 5
Frequent Probable Occasional Rare Improbable Catastrophic Major Moderate Minor No impact Extremely high High Moderate Low Extremely Low
Staff
Severe or severly Trivially extremely well
aware
Not likely Life exacerbated injury or Mildly exacerbated exacerbated prepared/ staff Staff Staff know
Almost Quite there is a No awareness
May occur but Not likely threatening, illness or significantly injury or illness, injury or illness, No harm have drilled have policy and
certain likely procedur by staff
possible Death reduced life temporary harm may require first and know drilled procedure
e or
expectancy aid response
policyScoring Key Example 3
Example Risk Assessment
Risk assessment template courtesy of CHI Health Infection PreventionAdmission Risks
Ventilators Urinary Tract Infection Events
• VAP • CAUTI ICU
• CAUTI-Other units
• Vent Bundle non-compliance
• Foley Bundle non-compliance
Central lines PIV related HAI
• CLABSI-ICU • Blood Stream Infections This Photo by Unknown
Author is licensed under
• CLABSI-NICU CC BY
• CLABSI-Other Inpatient Locations Surgical Site Infections
• SSI-Ortho
• Central Line Bundle non- • SSI-C-Section
compliance
• SSI-Hyster
• SSI-Colon
Healthcare-acquired Drug Resistant • SSI-Neuro
Organisms/Communicable Diseases
• MRSA
• VRE
• CRE
• COVID-19
• C-diff
This Photo by Unknown
Author is licensed under
CC BY-SA-NC
This Photo by Unknown Author is licensed under CC BY-SA-NCHealthcare Worker (HCW) Risks
• Hand Hygiene non-compliance
• Transmission based precautions non-
compliance
• Standard Precautions non-compliance
• Aseptic technique non-compliance
• Infection Prevention Policy and Procedures
staff knowledge deficit This Photo by Unknown Author is licensed under CC BY-ND
• Sharps/Splash occupational exposure
• Delayed recognition of employee outbreak
(I.E. Pertussis or COVID-19)
• Influenza immunization not received
• Annual PPD/N-95 Fit test not complete
• HCW immunizations not up to date
• Universal Masking non-compliance
• Social distancing non-compliance
• HCW working while infectious
This Photo by Unknown Author is licensed under
CC BY-SAEnvironmental Associated Risks
• Cleaning & Disinfection of Environment inadequate
• Sterilization of Equipment inadequate
• PPE available for surge of infectious patients
inadequate
• Improper disposal of Sharps
• Improper disposal of Medical Wastes
• Failure of negative ventilation
• Incomplete preconstruction ICRA
Image from ICRA 2.0 Assessment.pdf
This Photo by Unknown
Author is licensed under CC
(ashe.org)
BY-SA
This Photo by Unknown Author is licensed under CC BY-NDCommunity Tab
• Epidemic/Pandemic (i.e., COVID-19)
• Bioterrorism
• Respiratory illness outbreak
This Photo by Unknown Author is licensed under CC BY
• Food-borne/Gastrointestinal illness outbreak
• Waterborne illness outbreak
• Mycobacterium Tuberculosis
• Weather related event
• Large public/entertainment events
• Day Care related outbreaks
• Academic Dormitories-related outbreaks (I.E. Mumps) This Photo by
Unknown Author is
• Immigrant population licensed under CC BY-
SA
• Community MDRO
• Transportation/travel related event This Photo by
Unknown Author is
licensed under CC BY-
SA
This Photo by Unknown Author is licensed under CC
BY-NDExample
The higher the
final score, the
higher the risk
Risk assessment template courtesy of CHI Health Infection PreventionNext Steps
Priority # Priority Goal Objective Strategies Progress/Analysis Evaluation
1.
2.
3.
4.
5.
Based on the scoring of your risk assessment
and the consensus of your team, you will
prioritize the elements you will need to
work on in the coming year.Creating Goals for your
Program
Prioritize pressing goals for coming Program Year
• Some will probably be determined by your organization
• Some are universal to all IP Programs
– Hand hygiene
– Prevention of InfectionsGoals
Priority # Priority Goal
1. SSI Hysterectomy Decrease NHSN SIR by the end of
FY2023
2. HCW working while Employees will use/understand
infectious infectious symptoms and COVID
testing policies if symptomatic
3. Hand Hygiene non- Improve hand hygiene compliance
compliance
Goals:
• May not be strictly measurable or tangible
• Outcome to achieve Long-termObjectives
Priority # Priority Goal Objectives
1. SSI Hysterectomy Decrease NHSN SIR by the • Reduce NHSN SIR by 10% in FY23
end of FY2023 • SIR Rate in FY22 was 2.53
• Target: NHSN SIR of 2.28 or less for FY23
2. HCW working while Employees will 10% reduction in incident reports of employees
infectious use/understand infectious working while infectious from FY22
symptoms and COVID testing
policies if symptomatic
3. Hand Hygiene non- Improve hand hygiene Overall Hand Hygiene compliance will be 90% or
compliance compliance better for FY2023
Objectives:
• What you want to accomplish
• Specific action supports the goal
• Measurable and tangible
• Mid to short termStrategies
Priority # Priority Goal Objective Strategies
1. SSI Hysterectomy Decrease NHSN SIR by • Reduce NHSN SIR Q1
the end of FY2023 by 10% in FY23 1. Perform analysis of
current HYST SSI, and
• SIR Rate in FY22 look for trends
was 2.53 2. Develop SSI
• Target: NHSN SIR of Team/Subcommittee
2.28 or less for to review analysis
FY23
2. HCW working while Employees will 10% reduction in Q1
infectious use/understand incident reports of 1. Survey employees as
to why Incidents are
infectious symptoms employees working occurring
and COVID testing while infectious from 2. Audit the incident
policies if FY22 reports for FY22 to
symptomatic determine trends
Strategies
• Action Plans/steps to achieve the objective
• The HOW and WHAT
• Assign responsibility – don’t try to do all by yourselfStrategies
• Break down into steps
• Assign who is responsible for each part of the plan
• Involve others
For example: Survey staff
IP develop survey by 5/1/2022
Unit directors hand out survey during May unit meetings
Unit directors will return survey to IP by 6/2/2022Progress/Analysis
Priority # Priority Goal Objectives Strategies Progress/Analysis
1. SSI Hysterectomy Decrease NHSN SIR • Reduce NHSN SIR Q1 Q1 (as of *Date)
by the end of FY2023 by 10% in FY23 1. Perform analysis of current 1. Analysis complete on
HYST SSI, and look for 5/1/2022 done
• SIR Rate in FY22 trends 2. SSI Team developed,
was 2.53 2. Develop SSI and first meeting on
• Target: NHSN SIR Team/Subcommittee to 5/15/2022
of 2.28 or less for review analysis
FY23
2. HCW working Employees will 10% reduction in Q1 Q1 (as of *Date)
while infectious use/understand incident reports of 1. Survey employees as to 1. Surveys completed
why Incidents are 2. Audit completed
infectious symptoms employees working occurring
and COVID testing while infectious 2. Audit the incident reports
policies if from FY22 for FY22 to determine
symptomatic trends
Progress/Analysis-
Update and analyze your progress on at least
on a quarterly basis.Progress/Analysis
• Use visuals to present your progress and analysis to the IP committee
(e.g., charts, graphs)
• Keep administration updated on progress
• Keep staff updated on how they are doing- share success and failures with
the department involvedEvaluation
Priority Priority Goal Objective Strategies Progress/Analysis Evaluation
#
1. SSI Decrease • Reduce NHSN Q1 Q1 (as of *Date) Q1
Hysterectomy NHSN SIR by SIR by 10% in 1. Perform 1. Analysis 1. Analysis shared with SSI
the end of FY23 analysis of complete on Team on 7/15/2022
FY2023 • SIR Rate in current HYST 7/1/2022 done 2. SSI Team scheduled to
FY22 was 2.53 SSI, and look 2. SSI Team meet monthly and
• Target: NHSN for trends developed, and develop Q2 strategies
SIR of 2.28 or 2. Develop SSI first meeting
less for FY23 Team/Subcom on 7/15/2022
mittee to
review analysis
Q2. Q2. Q2.
1. Staff to 1. Unit managers 1. 3West with new staff;
complete verified staff need to have
education on completion of education available
CHG pre-op education on upon hire/orientation
bathing 10/3/2022Final Evaluation Written text document Address the specific goals you prioritized Address the organizational goals Address the universal IP goals Continuing with the goals for the new plan year
References Fulton, Teresa , RN, MSN, CIC,CCMSCP. Risk Assessment, IP Plan and QAPI. 4th Annual Wyoming Infection Prevention Conference. Available at www.health.wyo.gov/Media.aspx?mediald=15694 Risk Assessment for Infection Prevention and Control Programs. APIC, n.d. Available at https://higherlogicdownload.s3.amazonaws.com/APIC/eb3f0499-9134-44a-9b14- f1d9f3915c3f/UploadedImages/IPCRiskAssessment.pdf Joint Commission Resources, Using the Risk Assessment to Set Goals and Develop the Infection Prevention and Control Plan. Available at http://www.jcrinc.com/using-the-risk-assessment-to-set-goals-and-develop-the- infection-prevention-and-control-plan/ Association for Professionals in Infection Control and Epidemiology, Inc. Fourth edition, June 2014 Infection Control during Hospital Renovation and Construction; Policies, Procedures and Strategies to Protect Patients and Workers. Laborers’ Health and Safety Fund of North America https://tools.niehs.nih.gov/wetp/public/Course_download2.cfm?tranid=9803
Updates Presented by NE ICAP
COVID-19 Booster Updates CDC - COVID-19 Vaccine Boosters
51
What Clinicians Need to Know about
Monkeypox in the United States and
Other Countries
CDC Image
• On 5/24/22, CDC held a Clinical Outreach and Community Activity (COCA) webinar about
monkeypox including guidance about the typical clinical presentation, treatment options,
pre- and post-exposure prophylaxis, and reporting to public health authorities.
• As of 5/24/22 there were 8 confirmed orthopox (OPX) cases. Of these, 1 is confirmed
monkeypox (Massachusetts), the others are considered monkeypox until proven
otherwise, confirmation testing is only available at CDC.
• Signs and Symptoms:
• Historically: characteristic rash preceded by prodromal symptoms (e.g., fever,
lymphadenopathy, flu-like symptoms)
• Current cases: atypical features with reason for unusual presentation currently
unknown
• Rash still characteristic; but often starting in genital and perianal areas
• Rash sometimes not disseminating to other parts of body
• Being recognized at outpatient clinics because easily confused with sexually
transmitted infections
• Prodromal symptoms mild or not occurring52
Monkeypox Infectiousness &
Transmission
• Patient infectious once symptoms begin (whether prodromal or rash symptoms) until lesions scab
and scabs fall off
• Transmission – (Good News is Not Easily Transmitted)
• Direct or indirect contact with body fluids or lesion materials
• Contact with fomites
• Exposure to respiratory secretions
• Examples of high and intermediate risk exposures
• Shared towels and bedding (infectious body fluids and scabs may be present)
• Skin-to-skin contact with a patient who has monkeypox
• Being inside the patient's room or within 6 feet of a patient during any procedures that
may create aerosols from oral secretions, skin lesions, or resuspension of dried exudates,
without wearing an N95 or equivalent respirator (or higher) and eye protection
• Outpatient clinics and acute care facilities and providers are highly encouraged to read the CDC HAN
and review the slides and video once available if you missed the webinar.
• 5/20/22 CDC HAN Advisory
• 5/24/22 CDC COCA WebinarSHEA/IDSA/APIC Compendium
2022 Update: CLABSI and VAE
• SHEA/IDSA/APIC Compendium of Strategies to Prevent Healthcare-
Associated Infections in Acute Care Hospitals is a nationally and globally
utilized resource that continues to provide up-to-date, concise, and
practical recommendations for essential infection prevention practices
and guidance on how to build them into the delivery of care.
• The compendium was first published in 2008 and then updated in 2014.
• Two of the seven guidance documents have been updated so far and
the others will be released in 2022. You are encouraged to review.
• Strategies to prevent central line-associated bloodstream
infections (CLABSIs) in acute-care hospitals
• Strategies to prevent ventilator-associated pneumonia, ventilator-
associated events (VAEs), and non-ventilator healthcare-associated
pneumonia (NV-HAP) in acute-care hospitalsUpcoming Webinars & Requests
Join us for our next webinar on June 8th
to discuss interpreting susceptibility and the NE ASAP program
If you have suggestion(s) for future webinar topics or an IP
ENIGMA to discuss include them in the continuing education
(CE) survey or contact us with your requests!
Image by rawpixel.com
Call us at 402.552.2881
Email us at nebraskaICAP@nebraskamed.com
You can also be added to our setting specific mailing lists, receive
webinar and training invites and be connected to an Infection
Preventionist that specializes in your area by filling out the contact form
at: https://nebraskamed.formstack.com/forms/icap_questionQuestions and Answer Session Please use the QA box in the webinar platform to type a question Attendees also have the option to upvote other attendee’s questions Questions will be read aloud by the moderator A recording of the discussion will be made available on the Nebraska ICAP website Panelists: Gary Anthone, MD Lacey Pavlovsky, RN, MSN, CIC Margaret Drake, MT (ASCP), CIC M. Salman Ashraf, MBBS Richard Starlin, MD Rebecca Martinez, BA, BSN, RN, CIC Jody Scebold, EdD, MSN, RN, CIC Chris Cashatt RN, BSN, CIC
ICARs for Acute & Outpatient Settings
• Infection Control Assessment and Response (ICAR) tools are used to
systematically assess a healthcare facility’s infection prevention and
control practices and guide quality improvement activities (e.g., by
addressing identified gaps)
o ICAP is offering on-site and tele (virtual) assessments to both
acute and outpatient settings
• Call NE ICAP at 402.552.2881 to be connected with
an Infection Preventionist
o Or scan the QR code
• Ask to be added to the ICAP email distribution list
o https://nebraskamed.formstack.com/forms/add_me_to_email_distribution_listListen to New ICAP Podcasts!
Twitter: @Mouthy_IP
Apple Podcasts: https://podcasts.apple.com/us/podcast/the-mouthy-
ip/id1573465413
Spotify: https://open.sp
otify.com/show/2evXIrvZFiZFP2VZBq9cVK?si=DVhPEewJSL2xXIrDi0Y2Bg&dl_bra
nch=1
Amazon Music: https://music.amazon.com/podcasts/2bc794ab-59af-4bbe-a8df-
6a72309fa024/THE-MOUTHY-IP
Podchaser: https://www.podchaser.com/podcasts/the-mouthy-ip-1955086
Twitter: @dirty_drinks
Amazon Music: https://music.amazon.com/podcasts/769c29a8-1e71-46a5-9ab3-
94020d7af1f7/DIRTY-DRINKS
Apple Podcasts: https://podcasts.apple.com/us/podcast/dirty-drinks/id1574937193
Podchaser: https://www.podchaser.com/podcasts/dirty-drinks-1963455
Spotify:
https://open.spotify.com/show/3Y8w2YVedZYnX8ZS897mU9?si=lyBNetUTTSGtlg3PmBH3
Tg&dl_branch=1ICAP Contact Info
Call 402-552-2881
Office Hours are Monday – Friday
8:00 AM - 4:00 PM Central Time
Weekends and Holidays 8:00-4:00
On-call hours are available for emergencies only
Scan the QR Code to be taken to our website
contact form. You can request a call back
from an IP, Sign up for newsletters and reminders
and request an ICAR Review for your facility.Webinar CE Process
1 Nursing Contact Hour is awarded by NE Medicine *
* Nebraska Medicine is approved as a provider of nursing continuing
professional development by the Midwest Multistate Division, an accredited
approver by the American Nurses Credentialing Center’s Commission on
Accreditation.
1 AMA PRA Category 1 CreditTM for Physicians offered by UNMC
CNE Nursing Contact Hours: AMA PRA Category 1 Credit™
➢ Completion of survey is required. Completion of survey is required.
➢ The survey must be specific to the ➢ The survey must be specific to the individual
individual obtaining credit. (i.e.: 2 people
obtaining credit. (i.e.: 2 people cannot be
cannot be listed on the same survey)
listed on the same survey)
➢ One certificate is issued monthly for
all webinars attended ➢ One certificate is issued monthly for
➢ Certificate comes directly from ICAP all webinars attended
via email ➢ Certificate can be downloaded from
➢ Certificate is mailed by/on the 15th the UNMC CCE system directly, they
of the next month will email you access
➢ Survey functionality is lost on ➢ Survey functionality is lost on mobile
mobile devices devicesYou can also read