DERMATOLOGY FOR THE NON-DERMATOLOGIST - 4/30/2021 Megan N. Landis, MD Clinical Associate Professor of Dermatology University of Louisville ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

DERMATOLOGY
FOR THE
NON-DERMATOLOGIST
4/30/2021
Megan N. Landis, MD
Clinical Associate Professor of Dermatology
University of Louisville, Division of Dermatology
Dermatology and Skin Cancer Center of Southern Indiana
Corydon, IN
Information presented is
based on evidence-based
recommendations and well
DISCLOSURES designed published studies
• Investigator and/or Consultant: Abbvie, Celgene, Cutanea, Dermira,
Foamix, Galderma, Incyte, Kadmon, Novartis, Novum, Ortho Dermatology,
Pfizer, Regeneron, Sanofi Genzyme, Symbio
•
OBJECTIVE • To Make Your Life Easier! • Skin issues frequently seen in primary care, common conundrums, pitfalls to avoid • High yield clinical pearls
ACUTE ALLERGIC CONTACT DERMATITIS • Linear vesicles in rash (poison ivy) • Localized: topical corticosteroids • Diffuse: long, slow prednisone taper over ~21 days (avoid rebound)

RECURRENT OR CHRONIC ALLERGIC CONTACT DERMATITIS • Patch testing

CASE #2 Which treatment is absolutely contraindicated for this patient? A. Topical clobetasol 0.05% ointment B. Oral corticosteroids C. Phototherapy (nbUVB) D. Cyclosporine
PSORIASIS:
TOPICAL THERAPIES
• Topical Anti-inflammatories
• Topical steroids
• Topical tacrolimus or pimecrolimus (face, underarms, groin)
• Keratinocyte Proliferation Modulators
• Vitamin D analogues (calcipotriene)
• Tazarotene (palmar/plantar involvement)
PSORIASIS:
SYSTEMIC THERAPIES
• NO ORAL/SYSTEMIC STEROIDS: severe flare upon withdraw
• Phototherapy
• Cyclosporine
• Methotrexate
• Biologics
• LOOK for joint involvement: permanent destruction (nails = greater risk PsA)
AAD.org
PSORIASIS
• Chronic disease, primarily of skin and joints; may wax and wane
• ~2% of US population
• 30% have family history
• Onset most commonly ages 20-30 and 50-60yrs
• 80% of patients have mild to moderate disease (5% BSA OR affecting crucial body areas – hands, feet, face,
scalp, or genitals)
AAD.org
PSORIASIS:
TYPES
• Plaque (most common)
• Inverse/flexural/genital
• ErythrodermicPSORIASIS:
TYPES
• Guttate (often preceded by strep pharyngitis)
• Palmoplantar pustular
• Generalized pustular (von Zumbusch variant) – severe, life-threatening, often due to
systemic steroid withdrawal
• Nail psoriasisPSORIASIS:
COMORBIDITIES
IMPORTANT:
-Screen psoriasis patients for
joint involvement (30%)
-Monitor psoriasis patients
for comorbidities routinely
Aurangabadkar SJ. Comorbidities in psoriasis. Indian J Dermatol Venereol Leprol
2013;79:10-17PSORIASIS • Localized plaque type often managed by PCP • All other types of psoriasis often referred to derm
MOLLUSCUM
• BOTE sign: Beginning Of The End
• Inflammatory phenomenon, often precedes resolution
• Tender, inflamed, painful
• 8 patients – cultures with only skin flora
• Symptomatic management only
• No antibiotics needed (unless red streaking
or abscess formation) Forbat E, et al. Peditr Dermatol 2017;34(5): 504-515.
Image: Butala N, et al. Pediatrics 2013;131:5.MOLLUSCUM
• Pox virus: skin contact and fomites
• Self-limited, resolves ~6-24mo without treatment
• Watchful waiting
• Cantharidin, podophyllin, cryo, curettage, topical retinoid,
hydrogen peroxide, 2.5-15% KOH
• Imiquimod: NOT effective and potential for high systemic Forbat E, Al-Niaimi F, Ali FR. Peditr Dermatol 2017;34(5): 504-515.
Katz KA. JAMA Dermatol. 2015;151:125-126.
absorption and hematologic abnormalities Van der Wouden JC et al. Cochrane Database Syst Rev 2017;5:CD004767.
Myhre PE, Levy ML, Eichenfield, et al. Pediatr Dermatol. 2008;25:88-95.
Romiti, et al. Pediatr Dermatol. 2000;17:495.
Romiti, et al. Pediatr Dermatol. 1999;16:228-231.
Teixido C, et al. Pediatr Dermatol 2018;35:336-342.ATOPIC DERMATITIS (AD)
• Chronic, pruritic inflammatory skin disease; wide range of severity
• Up to 20% of children and 4-10% of adults
• Onset ~3-6mo; 90% diagnosed by age 5
• ~30% persist into adulthood
• Eczema: nonspecific reference to group of inflammatory skin diseases with itching,
redness, and scale
• Atopic dermatitis is a type of eczematous dermatitis
• Also included in eczematous dermatitis: seborrheic dermatitis, allergic contact dermatitis, irritant
dermatitis, etcATOPIC DERMATITIS (AD)
• “the itch that rashes”: primary symptom is pruritus
• Scratching to relieve AD-associated itch results in “itch-scratch” cycle
that exacerbates the disease
• Infants/Toddlers: Scalp, forehead, cheeks, & extensor arms/legs
• Older children: Flexures of neck, arms, legs, cheeks
Eichenfield LF, et al. J Am Acad Dermatol. 2014
Jul;71(1):116-32ATOPIC DERMATITIS (AD)
• Cause: not completely known, multifactorial with factors including:
• Skin barrier dysfunction
• Immune dysregulation
• Genetics
• Environment
• Usually not food relatedATOPIC DERMATITIS (AD):
TREATMENT
• Puts water in the skin
• But, it will evaporate and take more water with it from skin, UNLESS:
SEAL in the moisture
• Water is GOOD as long as you moisturize afterwards
• Gentle, fragrance-free bar soap at end of bath
• Medicine to rash and moisturize everywhere immediately Eichenfield LF, et al. J Am Acad Dermatol. 2014
Jul;71(1):116-32ATOPIC DERMATITIS (AD):
TREATMENT
• Topical anti-inflammatories: topical corticosteroids, topical calcineurin inhibitors
• Narrow band UVB treatment
• Immunosuppressive meds: cyclosporine, methotrexate, etc
• Dupilumab (DUPIXENT): 1st biologic for AD, approved 2017, monoclonal antibody
directed against IL-4 and IL-13
• 6yrs and above
Eichenfield LF, et al. J Am Acad Dermatol. 2014
Jul;71(1):116-32SEVERE ATOPIC DERM
• NO SYSTEMIC STEROIDS
• Makes disease worse in the long run
• Consensus statement from Peds Derms
• Wet wraps
• DIET: VERY RARELY MATTERS. STRICT DIET RESTRICTIONS NOT recommended
Eichenfield LF, et al. J Am Acad Dermatol. 2014
Jul;71(1):116-32ATOPIC DERMATITIS: WHEN TO REFER • Severe or extensive disease • Symptoms poorly controlled with topical therapy • Recurrent skin infections
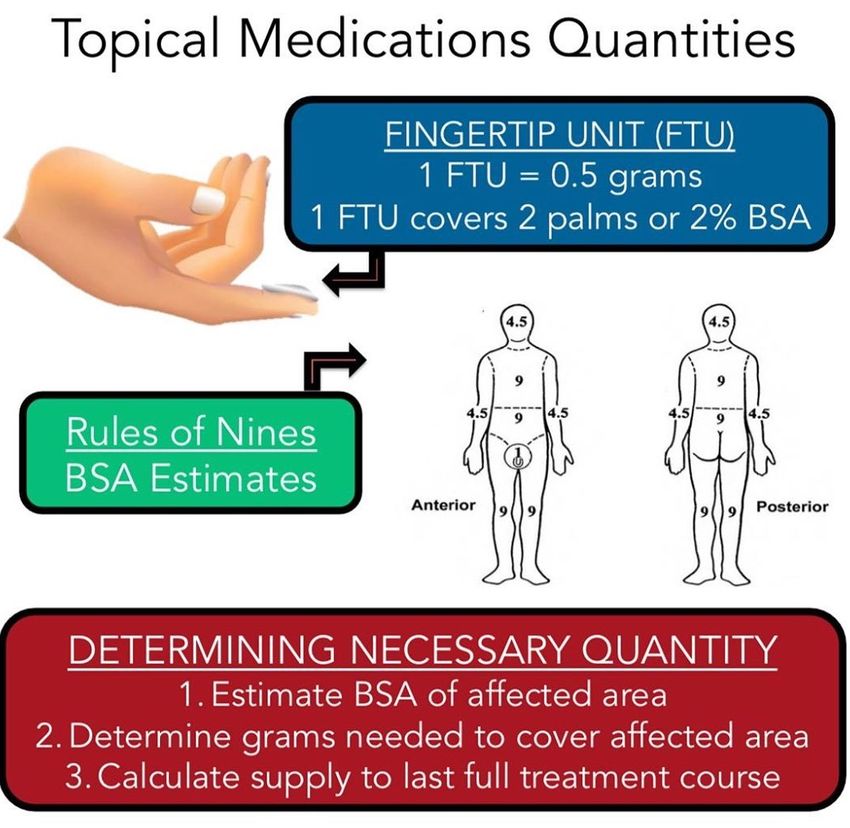
CORTICOSTEROID QUANTITIES
• Commonly available in:
• 15g
• 30g
• 45g
• 60g
• 120g
• 240g
• 454g (1LB jar)Keys:
-prescribe enough but not too much to get
them in trouble
-~30g to cover adult body once
-reassess quantity at follow up
Image: Grepmed.com
https://image.slidesharecdn.com/seminarpresentation0n04-01-
2014-140219112401-phpapp01/95/seminar-principles-of-
topical-therapy-10-638.jpg?cb=1392809584TOPICAL MEDICATIONS:
VEHICLE/BASE
• What topical medications are prepared in
Vehicles
• Can optimize for various sites on body and to optimize penetration
Foams
Creams
Gels
Sprays
Lotion
(Not Shown) Oils
Image: AAD.org
Solutions OintmentsTOPICAL MEDICATIONS:
VEHICLES
• Ointments (Vaseline): lubricating, greasy, semi-occlusive
• BEST for AD, but sometimes not tolerated
• Cream (vanishes when rubbed in): may sting and irritate open skin areas, more
preservatives/fragrances
• Useful when can’t tolerate ointment
• Lotion (pourable liquid): may burn or sting
• Helpful for larger and some hair bearing areas
Indian J Dermatol. 2016 May-Jun; 61(3):
279–287.TOPICAL MEDICATIONS:
VEHICLES
• Foam: more elegant, easy to spread, good for scalp/hair bearing areas, $$$
• Gel: may sting, least occlusive, dries quickly
• Good for acne, hair bearing areas
• Oil: less stinging or burning than solution
• Good for scalp
• Solution: water or alcohol-based lotion containing a dissolved powder
• Good for scalp
Indian J Dermatol. 2016 May-Jun; 61(3):
279–287.TOPICAL MEDICATIONS:
VEHICLE RECOMMENDATIONS
• For eczema (AD): for the body ointment if tolerated, cream if not
• For scalp: oil, solution, or foam
• Acne: cream, gel, foam (for large surfacer area, on back)Potency Class Example Agent
TOPICAL CORTICOSTEROIDS Super high I Clobetasol propionate 0.05%
Fluocinonide 0.05%
High II
Mometasone furoate ointment 0.1%
Mometasone furoate cream 0.1%
Medium III – V Triamcinolone acetonide ointment 0.1%
• Do NOT look at percentage: strength Triamcinolone acetonide cream 0.1%
depends on class
Fluocinolone acetonide 0.01%
• Recommendation: get familiar and Low VI – VII Desonide 0.05%
Department of Dermatology Hydrocortisone 1% 13
comfortable with a few in a few different
classes
• High: clobetasol 0.05% (body: severe areas only; DO NOT USE
ON FACE OR. FOLDS)
• Medium: triamcinolone 0.1% (body, NO NOT USE ON FACE OR
FOLDS)
• Low: hydrocortisone 2.5% (face and folds)RECOMMENDATION • Use twice daily until itch free and smooth • If not improved in 2 weeks, patient to call • Reassess at follow up • Transition to nonsteroidal (crisaborale, tacrolimus, pimecrolimus) for maintenance • If not improving as expected: biopsy or refer (other diagnosis? cutaneous T cell lymphoma? Allergic contact dermatitis?)
AMELANOTIC MELANOMA
• Small minority of melanomas do not have clinically apparent pigment
• All subtypes of melanoma can be amelanotic
• Differential diagnosis:
• Basal cell carcinoma (#1)
• Squamous cell carcinoma or verruca when on acral surfaces
• Pyogenic granuloma
• Angioma / angiokeratoma
• Prognosis is same whether melanotic or amelanoticMELANOMA A = Asymmetrical B = Irregular Borders C = Multiple Colors D = Diameter > 6 mm E = Evolving (changing)
MELANOMA
• ABCDEs
• “Ugly Duckling” sign
• Early detection: 99% 5-year survival rate for patients whose melanoma is detected
early.
• survival rate drops to 66% if the disease reaches the lymph nodes
• 27% if it spreads to distant organs
Skincancer.orgBUT, BEWARE
CANDIDA INTERTRIGO
• Satellite pustules
• Tinea spares scrotum
• Skin cancers occur EVERYWHERE – if doesn’t respond - biopsy
Bowenoid papulosis, aka squamous cell carcinoma-in-situCANDIDA INTERTRIGO
• Erythematous and macerated plaques, peripheral scale,
often with peripheral satellite lesions
• Skin folds below the breasts, under the abdomen, axilla,
and groin
• Tx:
• decrease moisture to area (powder qAM, loose clothing,
sweat wicking material),
• topical ketoconazole (+hydrocortisone), iodoquinolTINEA CRURIS
• Tinea spares scrotum
• KOH
• Localized: topical terbinafine or clotrimazole bid x 2 weeks (check feet and toenail)
• Generalized: terbinafine 250mg daily x 2 weeks
• Skin cancers occur EVERYWHERE – if doesn’t respond - biopsyPYODERMA GANGRENOSUM • Painful, sterile pustule >>> rapidly ulcerates with neutrophilic infiltrate • Punch biopsy from edge of ulcer to aid diagnosis, with tissue culture • Association with IBD, RA, some leukemias • Rule out infection (NOT necrotizing fasc – results in erroneous debilitating amputations!!) • DO NOT DEBRIDE!!!! • Treatment: Topical and/or intralesional steroids, immunosuppressive meds/TNF-a-Inhibitors
BIOPSY TECHNIQUE
• Pigmented lesions and moles/nevi: NEVER cryo
• Always send for pathology
• Pathologists need to see entire lesion to fully evaluate
• Site documentation – the more detailed, the better
• Photos
• Triangulate
MayoClinic.orgBIOPSY TECHNIQUE • How to biopsy: Punch? Shave? Excision? Incision? • Where to biopsy? (ex: LCV - newest lesion, pyoderma gangrenosum – edge of ulcer)
PATHOLOGY REQUISITION FORM
• Specimen location
• Biopsy technique: tangential (shave), punch, excision
• Clinical description of lesion or rash (size, appearance)
• Prior and/or current treatments
• Clinical differential diagnosis (what you think it could be)
Image: dermpathdiagnostics.comSHAVE BIOPSY SUPPLIES • Persona blade • Lidocaine with epi • Alcohol swab • Cotton tip applicators • Hyfrecator ands/or aluminum chloride • Vaseline and bandage
PUNCH BIOPSY SUPPLIES • Lido w/ epi • Alcohol swab • Punch biopsy blade • Forceps • Iris Scissors • Needle driver • Suture • Vaseline and bandage
CARE FOR BIOPSY SITE • Fold 2 x 2 gauze to make mini pressure dressing • Paper tape or Coban for sensitive skin • Keep covered and dry for 24hrs, then gently wash with soap and water, pat dry and recover with Vaseline and bandage until healed • Erythema around shave and punch biopsy sites is expected
Any time something doesn’t respond as expected = BIOPSY Differential Diagnosis: • Seborrheic dermatitis • Contact dermatitis • Actinic keratosis • Basal cell carcinoma • Squamous cell carcinoma
BASAL CELL CARCINOMA (BCC)
• Most common type of skin cancer
• Most commonly: sun-exposed areas with history excess sun exposure, burns
• 85% occur on head and neck, BUT found EVERYWHERE
• Additional risk factors: male, increased age
Rogers HW, et al. JAMA Dermatol 2015;151: 1081-1086.BASAL CELL CARCINOMA:
TYPES
• Nodular (most common)
• Superficial
• Sclerosing/morpheaform
• Ill-defined border, more aggressive
• Pigmented
AAD.orgBCC TREATMENT:
SURGICAL AND NON-SURGICAL OPTIONS
• Head and neck, sclerosing subtype: Mohs surgery
• Fellowship trained, Board certified dermatologist
• Real time evaluation of margins for tissue conservation to minimize defect
• Other areas: depends on type, size, location
• Mohs surgery
• Excision
• Electrodessication and curettage
• Non-surgical options (superficial and/or poor surgical candidate): Imiquimod 5% cream, 5-
Fluorouracil 5% cream, photodynamic therapy (PDT), radiation AAD.orgBASAL CELL CARCINOMA • History of one skin cancer = likely to get more • NEEDS ROUTINE full body skin checks • Sun protection • Once monthly self skin exams
ACTINIC KERATOSES
• Slow growing rough, scaly macules/papules on sun damaged skin
• From years of sun exposure
• Face, lips, ears, forearms, scalp, neck or back of the hands
• Usually ages 40 and above
• Reduce your risk by minimizing sun exposure and protecting skin from
ultraviolet (UV) rays
• Left untreated, the risk of actinic keratoses turning into a squamous cell
carcinoma is about 5% to 10%.
MayoClinic.orgACTINIC KERATOSES • Many treatment options • For few focal lesions: cryotherapy (scar) • Field treatments: 5-fluorouracil, imiquimod, PDT
PITYRIASIS ALBA • Mild, often asymptomatic type of atopic dermatitis of the face • Ill-defined, hypopigmented mildly scaly patches on bilateral cheeks • Often younger children, spring and summer when skin begins to tan with sun • Skin care: moisturizer twice daily • +/-low potency topical corticosteroids or topical calcineurin inhibitors • Sun protection • Will fade with time once inflammation resolves
CHERRY ANGIOMAS • Common, acquired vascular proliferation • Highest concentration on torso • Increase in number starting at age 40 • May bleed or thrombose and mimic melanoma • When in doubt – BIOPSY or REFER it out
NEVI (AKA MOLES)
• Often appear sun exposed areas
• Most commonly acquired nevi begin to appear in early childhood
• New lesions over age ~50: biopsy or refer
• Appearance changes with time
• Brown macule(s)/papule(s) > brown papule(s) > skin-colored soft papule(s)
• Children & adolescents: change in nevi common, doesn’t necessarily indicate
malignancyNEVI (AKA MOLES) • Increased risk of melanoma: (refer to dermatology) • Personal history melanoma (5-8% chance of 2nd) • Family hx melanoma (first degree family members) • More than 100 nevi •
NEVI (AKA MOLES)
• Evaluate nevi in context of individual patient
• Nevi in one patient tend to resemble one another
• Melanoma often has a different pattern: ”ugly duckling” sign
• ABCDE’s of melanoma
• NEVER use cryotherapy on a pigmented lesion
• If uncertain of what lesion is: biopsy or refer to dermatology
• Biopsy goal: get the breadth and depth of entire lesionSTASIS DERMATITIS
VS
CELLULITIS
• Stasis Dermatitis
• Erythema, scale, pruritus, erosions, exudate
• Typically lower third of legs
• Often with pitting edema
• Bilateral or unilateral (previous vascular injury, etc.)
• +/-varicose veins and orange-red-brown discoloration (hemosiderin deposition)
• Cellulitis
• Acute, often fever and pain, more erythema, well-demarcated, without pruritus or scaleCELLULITIS
VERSUS
STASIS DERMATITIS
• 30-75% of pts admitted for cellulitis actually had stasis
dermatitis
• Skin cultures, blood cultures, and leukocytosis: NOT reliable
indicators of cellulitis
• Antibiotic prescriptions written for cellulitis shown to be
unnecessary for 67% of patients
J Am Acad Dermatol 2015; 73: 70-75
JAMA Dermatol 2014; 150: 1056-1061.VERRUCA VULGARIS (WART) • Scaly, hyperkeratotic, exophytic (growing upwards and outwards) plaques (also flat variants) • Small black dots: thrombosed capillaries at base of lesion • HPV infection of keratinocytes or mucosal epithelial cells • HPV ubiquitous in environment • Skin contact and fomites • COMMON! • At least 20% overall prevalence in US
DIFFERENTIAL DIAGNOSIS • Epidermal Nevus
DIFFERENTIAL DIAGNOSIS • Lichen Planus
DIFFERENTIAL DIAGNOSIS • Squamous cell carcinoma
VERRUCA VULGARIS:
TREATMENT
• Necessary?
• Spontaneous resolution in 2 yrs: >75%
• Based on placebo groups in trials with cure rate (20-70%)
• Indications for treatment
• No specific anti-HPV therapy
• Prevent self-inoculation:
• Discourage picking, biting, touching: risk spreading to lips,
faceVERRUCA VULGARIS: TREATMENTS
• Cryotherapy
• Cure rates rate from 31-52% after 3 treatments. Pain, blistering,
scarring
• Tretinoin 0.025-0.05% cream
• Facial flat warts
• 5-FU cream (5-fluorouracil)
• +/-Irritating to uninvolved skin
• +/- salicylic acid
• Imiquimod
• 3 times weekly, cure rate around 44%
• Intralesional Candida Ag
Bolognia
SA Ringin. J Cutan Aesthet Surg. 2020 Jan-Mar; 13(1): 24–30.SALICYLIC ACID 40% PLASTER: WARTS
• 25 pads for ~$20
• Up to 75% cure rate at 12 weeks with daily use
• Clean skin - Gently pare with nail file (don’t
use elsewhere) to remove dead skin – apply
plaster cut to fit over wart
• May apply tape over
• Repeat daily
• Good adjunctive home treatment
Madan RK and Levitt J. J Am Acad Dermatol 2014;70:788-92.LIQUID NITROGEN:
-196℃
• Pare, then two 10-15 sec freeze-thaw cycles, allowing
to thaw between cycles; 1-3 week intervals
• Margin around lesion correlates to depth of freeze
• Spray until “ice-ball” (white freeze color change)
formation spreads from center of wart with a 2mm
margin
• Produces most damage to koilocytes (keratinocytes
infected with HPV)
• CAUTION in periungual area to avoid nail dystrophy BologniaCRYOTHERAPY: POST-OP • Pain • Post-inflammatory hyper-/hypo- pigmentation • Blister formation • Scarring • Recurrence • Multiple treatments likely necessary
HPV VACCINE AND WARTS • Case reports: resolution of refractory skin warts after receiving HPV vaccination • Vaccine targets: • 6, 11, 16, 18, 31, 33, 45, 52, 58 • Common HPV types for skin warts: • Common: 1, 2, 4, 7 • Plantar: 1 • Flat: 3, 10, • Anogenital: 6, 11
IMPACT OF ACNE
• 85% of teens, at least 12% of adult women
• Lower self-confidence and self-esteem
• More likely to employ a teen without acne
• PCPs likely to be the first the patient sees and
may open up to. Patients often ashamed to
mention
• Successful treatment improves psychological
Cotterill J, Cunliffe W. Br. J Dermaotl 1997;137:246-50.
factors Dreno B et al. Dermatol Ther 2016;6(2):207-218.ACNE: TREAT AND/OR REFER SOONER RATHER
THAN LATERLESION TYPES
• Comedones: open
and closed
• Papules and pustules
• Cysts and nodulesACNE SEVERITY
• Mild (topical retinoid, +/-topical Abx, BP)
• Mostly comedones • Severe (ISOTRETINOIN)
• < 10 papules/pustules • Comedones
• Many papules/pustules
• Moderate (topical retinoid, +/-doxycycline, BP, OCPs, • +/- nodules/cysts (deeper)
spironolactone, topical Abx) • Active scarring
• Comedones • **recalcitrant to treatment
• >10 papules/pustules
• Consider: duration, backTREATMENT • Combinational almost always • CHRONIC disease – set patient expectations • Timing of results • Inflammatory/non-inflammatory lesions? • Mild/moderate/severe? • Scarring? Chronicity? Previous treatments?
TREATMENT: MILD ACNE
• Topical retinoids
• Mainstay of treatment: EVERYONE
• Comedolytic and anti-inflammatory
• Concentration & vehicle impact tolerability
• Adapalene tends to be better tolerated • +/-BP
(**OTC**) • +/-topical antibiotic
• Older formulations inactivated by sunlight and • +/-topical dapsone
benzoyl peroxide (BP) Eichenfeld LF, et al. Pediatr 2013;131(3): S163-S186.
Leyden JJ. J Am Acad Dermatol 2003;49(3): S200-S210.
• Patient counseling Bolognia 2018WHO GETS A RETINOID?
TREATMENT: MODERATE ACNE
• “Many” inflammatory papules
• Oral antibiotic (x3mo MAX)
• Evidence supports use of doxycycline, minocycline, erythromycin, TMP-SMX,
TMP, and azithromycin
• + BP (ALWAYS)
• + topical retinoid
• NO NEED for both oral and topical Abx simultaneously
• Female patients: OCPs, spironolactone
Thiboutot D et al. Arch Dermatol 2006;142:597-602
Zaenglein et al. J Am Acad Dermatol 2016;74:945-73BENZOYL PEROXIDE • Bactericidal: prevents/eliminates C. acnes resistance • ALWAYS use in patients on oral or topical antibiotics • Available in strengths of 2.5-10% • Concentration dependent irritation • Contact time can affect efficacy: leave-on vs wash-off – location dependent • Bleaching and staining of fabric
TREATMENT: MODERATE ACNE (CONT’D) • Follow-up at 3mo, ideally skin cleared and transition to only topical tx • +/- inc retinoid strength pending tolerability
SEVERE ACNE • Scarring • Nodules, cysts • Unable to maintain clearance on topical regimen • *the back • Treatment: ISOTRETINOIN
ISOTRETINOIN
• Reverses retention hyperkeratosis, reducing comedone
formation
• Decreases sebum levels
• Reduces C. acnes
• Decreases inflammation
• Remission and “cure” possible
Layton AM. J Dermatol Treat 4: S2-S5,1993ISOTRETINOIN
• LIFE-CHANGING
• Baseline labs and repeat at 2mo
• Liver, lipid profile, +/-CK
• I-pledge and birth control or abstinence
• Goal dose
• Controversies
Timothy J, et al. J Am Acad Dermatol. 2016;75(2)323—328.ACNE TOP 5 PEARLS
1. NEVER use antibiotics (topical or oral) as monotherapy. Limit oral antibiotics to 3
months
2. ALWAYS use topical benzoyl peroxide when using an antibiotic
3. EVERYONE gets a retinoid
4. It takes a good 3 months of consistent use to see the full effects of acne meds
5. Isotretinoin is life-changing and typically well tolerated in patients who are good
candidatesCASE: #22 What is this condition? A. Scarring from overuse of steroids B. Lichen planus C. Hidradenitis suppurativa D. Deep fungal infection E. Skin cancer
HIDRADENITIS SUPPRATIVA • Recurrent painful subcutaneous nodules and draining cysts • Double comedone(s), sinus tracts, and abscesses • Occurs in axilla*, inguinal, perianal, perineal, mammary, and inframammary regions
HIDRADENITIS SUPPURATIVA • Begins ages 20s-30s • Estimated prevalence 1-4% of population • Women > Men • Clinical diagnosis • Time from disease on set to diagnosis: 7-12 years
HIDRADENITIS SUPPRATIVA • Painful • Malodorous discharge, soiling of cloths • Under-diagnosed • High incidence of depression • Negative impact on work and social life
HIDRADENITIS SUPPRATIVA:
TREATMENT
• Oral and topical antibiotics
• Biologics: TNF-alpha inhibitor, adalimumab, shown to be effective for moderate to severe HS
• Important: Identify disease early and start appropriate treatment
• Underdiagnosed – patients reluctant to mention and/or seek care
Kimball AB, et al. Ann Intern Med. 2012; 157(12):846-855.SUMMARY: THE IMPORTANT THINGS • Any skin lesion or condition that doesn’t respond as expected or diagnosis uncertain: biopsy or refer • When doing a skin biopsy, clarify (and photo ideally) site, use best technique, know which area is best to sample • Encourage sun protection and monthly self skin checks • Don’t underestimate acne and its potential long term impacts. No need for scarring
INTERESTED IN LEARNING MORE DERMATOLOGY?
We have a few spots remaining for the CME/CE course: 9/17/21 @ Huber’s in southern IN
Skinternal Medicine: Dermatology for the Non-Dermatologist
www.skinternalmedicineconference.comTHANK YOU!!
meganlandis08@yahoo.comADDITIONAL REFERENCES
Zaenglein et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol 2016;74:945-73.
Layton AM, et al. Clin Exp Dermatol 1994; 19: 303-308
Goulden V et al. Prevalence of facial acne in adults. J Am Acad Dermatol.1999; 41: 577-8
Levin J. Dermatol Clin 2016(34): 133-145.
Gastroenterol 93:606
Br J Dermatol 123: 653
Cutis 64: 106
Dupre A, et a;. Vitamin B-12 induced acne. Cutis 1979;24(2):210-11.
Layton AM. J Dermatol Treat 4: S2-S5,1993
Timothy et al. JAAD 2016.
Simonart T. Acne and whey protein supplementation among body builders. Dermatol 2012;225:256-8
Huang et al. Isotretinoin treatment for acne and risk of depression: a systematic review and meta-analysis. J Am Acad Dermatol
2017;76:1068-76.ADDITIONAL REFERENCES Halioau et al. Feelings of stigmatization in patients with rosacea. J Eur Acad Dermatol Venereol. 2017;31:163-8 Bewley et al. Erythema of rosacea impairs quality of life: results of a meta-analysis. Dermatol Ther 2016;6:237-47 Egeberg et al. Patients with rosacea have increased risk of depression and anxiety disorders: a Danish nationwide cohort study. Dermatol 2016;232:208-13 Van Zuuren. Rosacea. New Engl J Med. 2017;377,18:1754-64* Fowler et al. Efficacy and safety of once daily topical brimonidine tartrate gel 0.5% for the treatment of moderate to severe facial erythema of rosacea: results of two randomized, double-blind, and vehicle-controlled pivotal studies. J Drugs Dermatol 2013;12:650-6 Rhofade cream prescribing information. Irvine, CA: Allergan, 2017 (https://www.allergan.com) Deckers and Kimball. The Handicap of Hidradenitis Suppurativa. Dermatol Clin 2016;34:17-22 Alikhan et al. J Am Acad Dermatol 2009;60: 539-61 Woodruff et al. Mayo Clin Proc. 2015:90(12): 1679-1673* Kimball AB, et al. Adalimumab for the treatment of moderate to severe Hidradenitis supprativa: a parallel randomized trial. Ann Intern Med. 2012; 157(12):846-855.
You can also read

















































